
Abstract
This study investigated the association of flood/stagnant water (FSW) with various health outcomes among respondents living in urban slums of Dhaka and adjacent rural areas. We also assessed the differences of individual-, household- and area-level characteristics between the FSW-affected and non-affected areas. Bangladesh as a whole and slums in the megacity of Dhaka in particular are severely affected by the FSW. Data were collected from 3,207 subjects (aged 10+ years) through baseline surveys conducted in March 2008 and 2009. Twelve big slums in Dhaka and three adjacent villages were selected as study areas. Face-to-face interviews using a multidimensional pre-tested questionnaire were conducted by the trained university graduates. We performed various types of analyses ranging from the simple frequency analysis to the multivariable-adjusted logistic regression modelling. Our empirical findings suggest that slums were more affected by the FSW as compared to the rural areas. People living in the FSW-affected areas were more vulnerable in terms of individual-, household- and area-level characteristics than non-affected people. Age was also significantly associated with various health outcomes. According to multivariable analyses controlled for various factors, the FSW-affected people reported significantly higher likelihoods of health symptoms (namely fever, cold/cough, weakness), communicable diseases (namely diarrhoea and gastric disease) and poor mental well-being as compared to the non-affected people. Only the burden of non-communicable diseases was lower in the FSW-affected areas than the non-affected areas. Our findings lead us to conclude that the FSW-affected area is an independent risk factor for various physical and mental health problems. Urban slums are more affected than rural areas by the FSW. Therefore, we underscore the necessities of well-designed and comprehensive public health interventions focusing on individual, community and higher levels of interventions to reduce the FSW-related health and other consequences among the people living in the FSW-affected areas and urban slums in the rapidly growing city of Dhaka, Bangladesh.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Global climate change increases extreme weather and climate events (IPCC 2012) including losses and consequences (IPCC 2012; ICSU 2008; Jonkman et al. 2008). The overall consequences of global climate change are more in the low- and middle- income countries of Asia and Africa, because of high population growth, widespread poverty, greater dependence on climate-sensitive ecosystems, lack of institutional and economical capacities and poor governance (Campbell-Lendrum and Corvalán 2007; Costello et al. 2009; Haines et al. 2006; Keim 2008; Khan et al. 2011; Nath and Behera 2011; Shahid 2010). Flooding is one of the most common hazards in the world (Ahern et al. 2005; Keim 2008), which counts about 40 % of the total natural hazards (Keim 2008). Worldwide around 800 million people live in flood-prone areas (IPCC 2012). Unfortunately, Bangladesh, one of the biggest delta regions in the world (Chowdhury and Ward 2007), is the worst victim of increasing floods (Ahmed and Ahmed 1999). It is a regular event there and inundates a substantial part of the country every year (Mirza 2002; Shaw 2006). This country naturally receives high precipitation during the monsoon season leading to the regular flooding. Climate change-related factors such as heightened snow melt in the Himalayas due to increasing temperature, increasing rainfall and river bank erosion in the upstream areas, growing siltation in the downstream and sea-level rise as well as anthropogenic factors such as excessive development and growing population in the floodplain and coastal areas without adequate drainage system, poor river management, construction of flood dykes and barrages in the upstream areas outside the territory of Bangladesh, a lack of coordination among different stakeholders as well as a lack of regional cooperation sharing the catchment areas of common rivers are responsible for flooding in Bangladesh (Karim 1995; Khalequzzaman 1994; Khalil 1990; Mirza et al. 2001; Shaw 2006; Tingsanchali and Karim 2005).
Coastal areas, megacities and cities are prone to damaging and costly flooding (Alam and Rabbani 2007; Braun and Aßheuer 2011; Khan et al. 2011; Rashid et al. 2007; Wenzel et al. 2007). Dhaka, the capital and the largest megacity in Bangladesh, is a typical example in this regard. This is one of the fasted growing megacities in the world, with an estimated population of 15.4 million in 2011 (United Nations, 2012). The elevation of greater Dhaka is about 2–13 metres above the sea level, although most of the urbanised areas are at the elevation of 6–8 metres (Huq and Alam 2003). The megacity is surrounded by four rivers and one canal namely by the Buriganga River to the south, the Balu and Shitalakshya rivers to the east, the Tongi canal to the north and the Turag River to the west (Alam and Rabbani 2007). Dhaka city experiences floods during the monsoon season as a regular basis (Dewan et al. 2007), which are mainly caused by the overflow of surrounding rivers and internal water logging. Some of the major floods in Dhaka occurred in 1954, 1955, 1970, 1974, 1980, 1987, 1988, 1998 and 2004 (Alam and Rabbani 2007; Huq and Alam 2003). Although overall livelihood of the city dwellers and functionality of the city are disturbed by floods (Alam and Rabbani 2007; Braun and Aßheuer 2011; Dewan et al. 2007), people living in slums and marginal settlements are more vulnerable than the well-off people (Rashid et al. 2007; Wenzel et al. 2007).
There are about 5,000 slums in the megacity of Dhaka that accommodate over one-third of its total population (Khan et al. 2009). Slums in the Dhaka megacity and other cities of developing countries are generally characterised by various risk factors such as low socio-economic status, poor housing, lack of sanitation and drinking water supply, high population density, lack of healthcare services, water logging and poor drainage and other environmental services (Cifuentes and Rodriguez 2005; CUS et al. 2006; Isunju et al. 2011; Khan et al. 2009; Kimani-Murage and Ngindu 2007). All these factors make slums highly conducive for different communicable diseases (e.g. diarrhoea). Moreover, the majority of the new migrants and their families from the rural parts of Bangladesh—one of the most important driving forces for rapid urbanisation in Dhaka—initially settle down in urban slums due to insufficient income and low house rent. Since slum dwellers have limited economic capacity and face multiple healthcare barriers, often they receive inadequate treatment and healthcare for their diseases (Khan et al. 2012). In contrast, families with a higher socio-economic status and higher income may possess better education, higher-paid jobs and improved awareness regarding hygiene and health care. Therefore, they may live in better housing and use clean water sources and sanitary facilities, which in turn can contribute positively to the family’s hygiene and overall health situation (Dasgupta 2008).
Floods can significantly affect the health and well-being of the population directly (e.g. mortality, injuries) and indirectly. The indirect effects of floods are mainly caused by various environmental problems. For instance, floods can increase the scarcity of safe drinking water due to contamination of water and sanitation as well as can increase the water logging due to poor drainage system (Ahmed and Ahmed 1999; Harris et al. 2008; Mirza 2011; Rashid et al. 2007; Shahid 2010). These negative aspects of floods generally create conducive environment for communicable diseases, which ultimately increase the burden of water-, rodent- and vectorborne diseases (Costello et al. 2009) including acute respiratory and eye infections, skin diseases, malnutrition and poor mental health. Particularly, diarrhoea is a waterborne communicable disease which is highly prevalent in urban slums. This disease can be transmitted through direct contact and/or through contaminated food, water and environmental surfaces. More occurrences of diarrhoea during and after floods can be attributed to various factors like contamination of water, poor drainage, changing transport and dissemination of infectious agents, poor economic status, lack of sanitation, food scarcity, overcrowding and subsequent faecal-oral spread of gastrointestinal pathogens (Ahern et al. 2005; Ahmed and Ahmed 1999; Ivers and Ryan 2006; Khan et al. 2011; Kunii et al. 2002; Schwartz et al. 2006; Shahid 2010). For example, a lack of sanitation may increase the risk of diarrhoea because infected faecal matters can be transported to the digestive tract of uninfected persons through hands, water and foods (Buttenheim 2008). Unhygienic behaviours (e.g. lack of hand washing with soap) among people living in affected areas due to lack of education and knowledge may also influence diarrhoeal diseases (Cairncross et al. 2010; Henry and Rahim 1990; Luby et al. 2006).
Although various studies concerning floods in Bangladesh are available, to our knowledge, epidemiological studies that focused on the associations between various health outcomes (physical and mental) and flood/stagnant water (FSW) (coded yes/no) are scarce. Particularly, this is the case for the rapidly growing slum communities in Dhaka. Therefore, the present study primarily aimed to report (1) how strongly individual-, household- and area-level characteristics were associated with the FSW variable and (2) how the risks of various health outcomes reflecting health symptoms, diseases, mental well-being, self-perceived health status (SPHS) and malnutrition differed by the dichotomous categories of the FSW variable. Moreover, (3) differences of respondent’s satisfaction regarding neighbourhood facilities and other individual- /family-level characteristics between affected and non-affected areas, (4) differences of health outcomes among various age groups and (5) differences of area affectedness by the FSW between rural areas and urban slums were reported.
2 Methods
The data used in this study were collected through baseline surveys (designed for a one-year cohort study) conducted in March 2008 and 2009. A total of 3,207 respondents (aged 10+ years) were selected from the equal number of systematically mapped households located in 12 large slums in the Dhaka megacity and 3 adjacent rural villages (see Khan et al. 2012 for detailed information). Only one respondent from each household was interviewed. In this study, a large slum was defined as a slum with a minimum of 500 households and six acres of land. As our study mainly aimed to focus on urban slum dwellers, we included more slums than rural villages in the sample. It should be noted that same criteria for selecting villages and households were applied in rural areas.
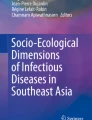
The selected slums were well-distributed throughout the city (Fig. 1). After selecting the slums, our research team (headed by a geographer) prepared an individual household map (using Google Satellite Maps as a base) for each slum by extensive field visits and then marked all the households (families) in the map with unique identification numbers. Next, the research team again visited all the households in the selected slums and collected basic information (e.g. number of household members, age and sex) from each household. Global positioning system (GPS) was used to show the location of each interviewed household in the slum. The map of each slum along with household unique identification number was considered as the sampling frame for this study. Since the total population varies from slum to slum, we used two-step formulae proposed by Bartlett et al. (2001). Based on their recommendations, at first, we used the Cochran’s sample size formula which is shown in Eq. 1 (Cochran 1997).
Where
-
t = the value of t-test when α = 0.5 which was 1.96;
-
p = 0.5 (assumed prevalence);
-
q = 1 − p = 0.5;
-
d = an acceptable margin of error which was 6 %, i.e. d = 0.06; and
-
n 0 = an estimated sample size for categorical data based on Cochran’s formula.

Maps showing study sites (urban slums) in Dhaka
Then, we applied the equation 2 to estimate different sample sizes depending on the number of households in each slum.
Because of the equation 2, we got the highest sample size for the slum with the highest number of households. In contrast, the sample size was the lowest for the slum with the lowest number of households. This particular feature increases the representativeness of the study. Slum-specific household numbers (total) and sample sizes (estimated) allowed us to calculate the sampling rate “r” by dividing the total number of households in a particular slum by its estimated sample size. To explain more about the selection of households for interview, let us consider the number of households is 1,000 (where each household was given an identification number from 1 to 1000) and the estimated sample size is 200 (based on above-mentioned formulae) in a particular slum. It gives a sampling rate (r) of five. Now, we have 200 small blocks with equal number of households. Only from the first block (with identification number 1–5) we will randomly select a number. If the number is 3, then other selected households will be 8, 13, 18, 23, 28,…, 993 and 998 based on sampling rate. After selecting households, our research team purposively selected only one respondent from each household to make our sample representative for gender and age groups. Because non-purposive (i.e. random) selection of respondents could produce biased results in terms of gender and non-response rate (Khan et al. 2009). Normally, the prevalence of respondent working outside home is higher among men than women, and among adults than elderly; therefore, it is more difficult to catch randomly selected men and adults during interview than women and elderly. It should be mentioned that our sample size was not adjusted for non-response rate as we achieved our target by replacing the non-respondent household by the next available household at the baseline survey. A pre-tested questionnaire was used to collect information by face-to-face interviews, which were conducted by the trained university graduates. At the beginning of the interview, the aims of the survey were explained and verbal consent from each of the respondents was obtained.
2.1 Dependent variables
In total, we used 10 dependent variables which are listed below. These variables can be grouped as health symptoms (namely fever, cold/cough and weakness), diseases, namely communicable (diarrhoea and gastric disease) and non-communicable (combined) diseases, and other health problems reflecting SPHS, the WHO-5 Well-being, and malnutrition (i.e. underweight). For collecting the information of health symptoms and diseases, each respondent was asked to report “whether the respondent suffered from (symptoms or diseases) during the last 3 months preceding the survey”. Although there were five answers for the SPHS variable in the original question, we converted it as a dichotomous variable for our analysis. The WHO-5 Well-being Index had five questions with Likert scale from 0 to 5. First, we added them and got the total scores from 0 to 25. Then, we divided these scores into two groups using cut-off point 13, where the score 13 and above was an indicator of good well-being. It should be noted that the WHO-5 Well-being Index is a quick, reliable and valid means for assessing psychological well-being. The index is quick because it contains only five questions, which are fewer than other available tools. It is also successfully applied in both developed and developing countries (Gruebner et al. 2011). The body mass index (BMI) was first calculated using the self-reported height and weight and then converted to underweight (BMI < 18.5) and else (BMI ≥ 18.5).
Health symptoms
-
a. Suffered from fever (yes = 1, no = 0).
-
b. Suffered from cold/cough (yes = 1, no = 0).
-
c. Suffered from weakness (yes = 1, no = 0).
Diseases
-
d. Suffered from diarrhoea (yes = 1, no = 0).
-
e. Suffered from gastric disease (yes = 1, no = 0).
-
f. Suffered from any of the three non-communicable diseases (combined due to small numbers) namely from diabetes, high blood pressure and heart disease (yes = 1, no = 0).
Any symptoms/diseases
-
g. Suffered from any symptoms/diseases (yes = 1, no = 0).
Other health outcomes
-
h. SPHS (fair/poor = 1, excellent/good/so so = 0).
-
i. The WHO-5 Well-Being Index (poor: total score below 13 = 1, good: total score 13–25 = 0).
-
j. BMI (Underweight = BMI < 18.5 = 1, else = 1).
2.2 Independent variables
From a large number of variables, only a subset which seemed to be relevant was used in this study. The selected variables were further grouped as individual-, household- and area-level characteristics (below). The main independent variable was “whether the study area was affected by the FSW (yes/no)”.
The individual characteristics (with categories in parentheses) were age of the respondent in years (continuous or categorical: 10–19, 20–29, …, 60 +), sex (male, female), education in years (no, 1–5 years called primary, 6+ called secondary+) and marital status (unmarried, married, divorced/widow/separated). These variables were used as control variables in the multivariable logistic regression analyses.
The household-level characteristics were sex of the household head (male, female), ownership of TV (yes/ no) and availability of the electricity in the house (yes/ no), structure of the house (permanent, provisional), whether the house got enough light from outside (yes/ no), whether the house had window (yes/ no), whether the kitchen was sufficient for the family (yes/ no), the number of families sharing the same water source (1–5 families; 6+ families), the number of families sharing the same toilet (1–5 families; 6+ families), the type of toilets in the house (hygienic and non-hygienic) and whether the family members got sufficient food (yes/ no).
The area-level characteristics were the area of residence (rural or urban), whether the respondent could reach their house through lorry, car, baby taxi, rickshaw and on foot (on foot, else), whether the area had proper drainage system (yes/ no), whether the garbage was collected on a regular basis (yes/ no), whether the neighbourhood environment affected the health of respondent negatively (yes/ no) and whether the area was good to see a medical doctor for treatment (very bad/bad, moderate, very good/good).
In addition to the above-mentioned variables, a set of variables representing respondent’s satisfaction of different neighbourhood facilities (e.g. water supply, health facilities and working facilities) and other individual- /family-level characteristics (e.g. own income, family income) (categorised as satisfied, moderately satisfied, dissatisfied) were analysed (based on the total sample) to show the differences between two categories of the FSW variable.
2.3 Statistical analysis
We performed various statistical analyses ranging from the descriptive analysis to the multivariable logistic regression modelling. Most of the analyses were performed using SPSS 20.0. First, bivariable analyses were performed to assess the associations of individual-, household- and area-level characteristics with the FSW variable (objective i). Then, we performed both bivariable and multivariable analyses to estimate the risks of various health outcomes based on the dichotomous categories of the FSW variable (objective ii). Specifically, multivariable logistic regression analyses (controlled for above-mentioned factors) were performed to estimate the odds ratio (OR) and 95 % confidence intervals (CI) for each outcome variable. p value based on either chi-square test (for categorical variables) or t-test (only for age—a continuous variable) was reported for most of the analyses. All associations with p < 0.05 were considered as significant, whereas p values of <0.001 were considered as highly significant. It should be noted that we used the total sample for 1–4 objectives and used the stratified sample (rural areas versus urban slums) for the last objective (5).
3 Results
Over 65 % of the total respondents reported that their areas were affected by the FSW. The affectedness was significantly higher (73.5 %) in urban slums as compared to rural areas (43.0 %) (Fig. 2). Table 1 is used to present the comparative results of individual-, household- and area-level characteristics by FSW along with p values to indicate the significance levels of the bivariable associations. Educational level was found to be higher in the non-affected areas than the affected areas. In the FSW-affected areas, the ownership of TV and availability of household electricity were significantly lower than the non-affected areas. Over 80 % of the houses were provisional in the affected areas, which was only 58 % in the non-affected areas. More than 70 % of the houses did not get enough light from outside in the FSW-affected areas as compared to 61 % in the non-affected areas. Similarly, prevalence of houses without any window and with insufficient kitchen was higher in the FSW-affected areas than the non-flood-affected areas. Sharing same water source and toilet facility by 6 or more families and use of non-hygienic toilet were more prevalent in the affected areas than the non-flood-affected areas. Area-level characteristics namely road accessibility to the household, drainage system, garbage management, environment in the house and neighbourhood, and availability of medical doctor to consult also revealed poorer conditions in the FSW-affected areas than non-affected areas.

Percentage of the FSW-affected area in rural areas, urban slums and total sample
The prevalence of health problems (Table 2) except cold/cough and diarrhoea varied from one age group to another. Age was significantly positively associated with any disease or symptom (ADS), weakness, gastric, non-communicable diseases, fair/poor health status and poor well-being. For instance, the prevalence of any disease or symptom (ADS) during the last 3 months preceding the survey was lowest (61.4 %) in the lowest age group (10–19 years) and highest (87.5 %) in the highest age group (60+ years). Similarly, the prevalence of poor well-being was lowest (48.8 %) in the age group of 10–19 years and highest (78.3 %) in the age group of 60+ years. Fever and underweight provided mixed associations (no trend) with age. The prevalence of fever of was highest in the age group of 20–29 years (40.9 %) and lowest in the age of 60+ years (29.2 %). The highest (37.1 %) and lowest (25.8 %) prevalence of underweight was found in the age of group of 10–19 and 30–39 years, respectively.
Figure 3 shows the percentage differences of respondent’s satisfaction regarding different neighbourhood facilities (e.g. water supply, educational facilities, healthcare facilities and working facilities) and individual- /family-level characteristics (e.g. own income, family income) by two categories of the FSW variable. For all these facilities and characteristics, respondent’s satisfaction was significantly lower (p < 0.001) in the FSW-affected areas than the non-affected areas. For example, the percentages of respondent’s satisfaction regarding water supply, water drainage, garbage management, recreation facility, health services and area environment were 9.4, 8.2, 7.8, 5.4, 11.3 and 8.8 % in the FSW-affected areas, respectively, whereas these percentages were 32.2, 28.8, 19.7, 15.3, 23.1 and 23.3 % in the non-affected areas, respectively.

Percentage of respondent’s satisfaction concerning different neighbourhood facilities and individual- /family-level characteristics
Area affectedness by the FSW was also strongly associated with health problems (Table 3) in both bivariable and multivariable analyses. Respondents living in the FSW-affected areas reported more from health symptoms, communicable diseases (like diarrhoea and gastric disease) and poor mental well-being than the respondents living in the non-affected areas. In contrast, the prevalence of non-communicable diseases was remarkably lower in the affected (2.7 %) than the non-affected areas (4.8 %). All associations between the FSW variable and health outcomes (except underweight and self-perceived health status) remained significant in both bivariable and adjusted multivariable analyses. For instance, the likelihood of suffering from diarrhoea in the FSW-affected areas was 1.8 times higher (OR = 1.8, 95 % CI = 1.13–2.87, p = 0.014) as compared to the non-affected areas in the multivariable adjusted analyses. Similarly, the likelihood of reporting poor well-being in the FSW-affected areas was 2.0 times higher (OR = 2.0, 95 % CI 1.69–2.37, p < 0.001) as compared to the non-affected areas.
4 Discussion
Our study clearly demonstrated that respondents living in the FSW-affected areas are more vulnerable than their non-affected counterparts from health and other (e.g. neighbourhood facilities) perspectives. Because these people reported higher prevalence of health symptoms, communicable diseases and poor well-being as well as expressed significantly lower levels of satisfactions concerning neighbourhood facilities and individual- /family-level characteristics. Most of the epidemiological findings in our study are supported by other studies. For instance, our findings concerning communicable diseases (e.g. diarrhoea) are found to be consistent with the findings of other studies (Ahmed and Ahmed 1999; Harris et al. 2008; Ivers and Ryan 2006; Kunii et al. 2002; Mirza 2011; Schwartz et al. 2006; Shahid 2010). As some of the possible explanations concerning the higher burden of communicable diseases in the FSW-affected areas are already given in the introduction, we skip these explanations here. The higher burden of health symptoms may be attributed to the existing differences of individual-, household- and area-level characteristics between the FSW-affected and non-affected areas. The poorer condition of well-being in affected areas could be attributed to various factors like crowding, poor housing and living environment, higher competition on the limited services and facilities, lack of tenure of land, lack of health facilities, violence and crime (Khan et al. 2009; Krämer et al. 2011).
Some of the possible implications based on our findings will be outlined below. It is already mentioned that Dhaka megacity is rapidly growing mainly due to the rural to urban migration and new settlements. This city is frequently affected by the flood and water logging mainly due to poor drainage, poor garbage management and elevation of the surrounding river beds and encroachments. Most of the new comers to the city generally settle down in environmentally poor and low land areas (like in slums), which are frequently affected by floods and post-flood problems. Since a large part of the city dwellers live in the FSW-affected areas and they suffer more from health problems, they should get proper attention and basic services from the city authorities, health sectors and other stakeholders. When we address the issues of urban and environmental health in developing countries, we should provide more attention on some vulnerable groups such as rural to urban migrants, slum dwellers and flood-affected people because they are the most challenging groups in the cities who can influence the urban health remarkably. These people suffer more from the higher level of poverty, environmental pollution, poor infrastructure, discrimination, social exclusion and crowding (Khan 2012). Without improving their settlements in terms of environment (e.g. garbage management, drainage) and basic facilities (e.g. water, sanitation), it would be difficult to improve their physical and mental health. Moreover, growing population in slums and flood-affected areas may hinder achieving one of the Millennium Development Goals concerning the improvement of lives among slum dwellers by 2020 (Khan 2012). In order to improve the health situations in the FSW-affected areas, some possible strategies are outlined below under different sub-sections.
4.1 Hygiene-related strategies
Bangladesh definitely needs timely and well-designed strategies and interventions to reduce the general and health consequences of floods in cities. Particularly, multidimensional attempts to minimise the health problems in the FSW-affected areas or in the urban slums are necessary in Dhaka. What interventions could be offered by the public health professionals and relevant authorities? Here, some of them are highlighted. Raising awareness concerning diseases and their transmissions during and after flood and benefits of maintaining personal hygiene is important (Khalil 1990). Encouraging people to wash their hands with soap might be an important and easy intervention to prevent waterborne communicable diseases. Because various studies reported the effectiveness of hand-washing practices—especially after defecation—to significantly reduce the transmission of the pathogens and emergence of diarrhoea (Cairncross et al. 2010; Henry and Rahim 1990; Luby et al. 2006). Apart from the interventions to promote hand-washing practices with soap in low-income settings, a proper disposal of faecal material and the use of modern toilets (instead of using open areas) are some strategies that could remarkably reduce the waterborne diseases and further infections (Curtis and Cairncross 2003).
4.2 Community-based or higher-level strategies
Community-based actions and interventions are also reported to be effective (Hunter et al. 2010; Pahwa et al. 2010) to reduce the burden of flood-related health risks. Some of the useful community-level actions may include the following: strengthening community-based primary health care outreach activities for the flood victims (Keim 2008) and strengthening the health education about flood consequences (Kunii et al. 2002). Moreover, health communications should be intensified at the community level to increase health prevention activities like preparedness at home, in schools, work places and at healthcare facilities (Keim 2008). For this purpose, overall manpower including public health personnel, who are particularly involved with the flood-related management, should be adequately trained. Public health strategies may include various options such as development and implementation of flood-specific surveillance programmes (Keim 2008; Shahid 2010), rapid actions from health authorities, strengthening hospital services and environmental risk management, improving drainage and sanitation systems in flood-prone settlements, and availability of medicines in flood-affected areas. Availability of essential equipment such as power generators and water pumps during flood is necessary to maintain critical health at hospitals, nursing homes, schools and outpatient clinics (Keim 2008). Vulnerable groups such as children, women, elderly and sick people should get more attention to reduce the health consequences. Affected people should be motivated to elevate their dwellings above the normal flood level and to use house materials resistant to water, as housing condition is one of the important determinants for health. In the FSW-affected areas, construction of embankments with adequate drainage systems is also useful (Ali 1999; Douglas 2009; Dove and Khan 1995; Khalil 1990; Shahid 2010). Since Dhaka city is surrounded by four rivers and low lands, restoration and excavation of water bodies (e.g. large tanks, canals) to hold more water and dredging of rivers are necessary (Islam 2001; Khalil 1990). Moreover, governments should implement policies to discourage new settlements in flood-prone areas by allocating alternative places (Mirza et al. 2001). The last but not least option might be the implementation of an integrated action combining housing, sanitation and other facilities for improving the health of the socially vulnerable people (Khan 2012).
4.3 Strengths and limitations
According to our knowledge, this study is an important contribution to the literature since it deals one of the most vulnerable groups of people living in the urban slums in a rapidly growing megacity. Another advantage of the study is the utilisation of a large sample, which may provide reliable results. It is one of the leading studies which addressed various health outcomes and estimated risks with respect to the FSW variable. Such a study is also important in the context of rapid urbanisation and slum growth in developing countries for urban planners, epidemiologists and other health personnel. However, our findings are not free from weaknesses. Generally, self-reporting is a problem because research participants have tendencies to respond in socially desirable ways. They tend to under-report socially undesirable and sensitive behaviours (e.g. weight, smoking) and tend to over-report appropriate and desirable behaviours (e.g. height) (Donaldson and Grant-Vallone 2002; Wang et al. 2002). Similarly, recall bias may lead to differential misclassifications of the related variable (e.g. health problems occurred within the last three months preceding the survey) (Hassan 2006). The cross-sectional nature of the data precludes us to comment on causal associations between independent variables and health outcomes. Disease information without subtypes (e.g. gastric disease) and combining three non-communicable diseases together due to small frequencies also limit our findings. Lastly, our findings should be used and generalised with cautions for other settings, since it was confined to some slums in Dhaka and adjacent rural areas (Khan et al. 2009).
5 Conclusions
Our study revealed significant differences between the FSW-affected and non-affected areas in terms of various health outcomes in both bivariable and multivariable analyses. Particularly, poorer health outcomes were observed in the FSW-affected areas than non-affected areas. These findings lead us to conclude that the FSW-affected area is an independent risk factor for various physical and mental health problems. Furthermore, we observed significant differences in almost all the potential determinants (except age) reflecting individual-, household- and area-level characteristics between the FSW-affected and non-affected areas. Significant differences were also found for neighbourhood facilities and individual/family characteristics by two categories of the FSW variable. Slums were more affected by the FSW as compared to rural areas, which implies higher health risks in slums and underscores the necessities of more public health interventions there. Some of the above-mentioned strategies could help reduce the health consequences and increase the satisfaction of urban livelihoods among the vulnerable groups, particularly who live in the FSW-affected areas in Dhaka, Bangladesh.
References
Ahern M, Kovats RS, Wilkinson P, Few R, Matthies F (2005) Global health impacts of floods: epidemiologic evidence. Epidemiol Rev 27:36–46
Ahmed SM, Ahmed HS (1999) Experiences of deluge: flood 1998. Research and Evaluation Division, BRAC, Dhaka
Alam M, Rabbani MG (2007) Vulnerabilities and responses to climate change for Dhaka. Environ Urban 19(1):81–97
Ali A (1999) Climate change impacts and adaptation assessment in Bangladesh. Climate Res 12:109–116
Bartlett JE, Kotrlik JW, Higgins CC (2001) Organizational research: determining appropriate sample size in survey research. Informat Technol Learning Perform J 19:43–50
Braun B, Aßheuer T (2011) Floods in megacity environments: vulnerability and coping strategies of slum dwellers in Dhaka/Bangladesh. Nat Hazards 58:771–787
Buttenheim AM (2008) The sanitation environment in urban slums: implications for child health. Popul Environ 30:26–47
Cairncross S, Hunt C, Boisson S et al (2010) Water, sanitation and hygiene for the prevention of diarrhoea. Inter J Epidemiol 39(suppl 1):i193–i205
Campbell-Lendrum D, Corvalán C (2007) Climate change and developing-country cities: implications for environmental health and equity. J Urban Health 84(1):i109–i117
Centre for Urban Studies (CUS), National Institute of Population Research and Training (NIPORT), Measure Evaluation (2006) Slums of urban Bangladesh: mapping and census, 2005. Dhaka, Bangladesh and Chapel Hill
Chowdhury MR, Ward MN (2007) Seasonal flooding in Bangladesh–variability and predictability. Hydrol Process 21:335–347
Cifuentes E, Rodriguez S (2005) Urban sprawl, water insecurity, and enteric diseases in children from Mexico city. EcoHealth 2:70–75
Cochran WG (1977) Sampling techniques, 3rd edn. Wiley, New York
Costello A, Abbas M, Allen A et al (2009) Managing the health effects of climate change. Lancet 373:1693–1733
Curtis V, Cairncross S (2003) Effect of washing hands with soap on diarrhoea risk in the community: a systematic review. Lancet Infect Dis 3:275–281
Dasgupta R (2008) Exploring intra-household factors for diarrhoeal diseases: a study in slums of Delhi, India. J Water Health 6:289–299
Dewan AM, Islam MM, Kumamoto T, Nishigaki M (2007) Evaluating flood hazard for land-use planning in greater Dhaka of Bangladesh using remote sensing and GIS techniques. Water Resources Manag 21:1601–1612
Donaldson SI, Grant-Vallone EJ (2002) Understanding self-report bias in organizational behavior research. J Bus Psychol 17(2):245–260
Douglas I (2009) Climate change, flooding, and food security in south Asia. Food Sec 1:127–136
Dove MR, Khan MH (1995) Competing constructions of calamity: the April 1991 Bangladesh cyclone. Popul Environ
Gruebner O, Khan MMH, Lautenbach S, Müller D, Krämer A, Lakes T, Hostert P (2011) A spatial epidemiological analysis of self-rated mental health in the slums of Dhaka. Int J Health Geogr 10:36
Haines A, Kovats RS, Campbell-Lendrum D, Corvalan C (2006) Climate change and human health: impacts, vulnerability, and mitigation. Lancet 367:2101–2109
Harris AM, Chowdhury F, Begum YA et al (2008) Shifting prevalence of major diarrheal pathogens in patients seeking hospital care during floods in 1998, 2004, and 2007 in Dhaka Bangladesh. Am J Trop Med Hyg 79(5):708–714
Hassan E (2006) Recall bias can be a threat to retrospective and prospective research designs. Internet J Epidemiol 3:26
Henry FJ, Rahim Z (1990) Transmission of diarrhoea in two crowded areas with different sanitary facilities in Dhaka, Bangladesh. J Trop Med Hyg 93:121–126
Hunter PR, Toro GIR, Minnigh HA (2010) Impact on diarrhoeal illness of a community educational intervention to improve drinking water quality in rural communities in Puerto Rico. BMC Public Health 10:219
Huq S, Alam M (2003) Flood management and vulnerability of Dhaka City. In: Kreimer A, Arnold M, Carlin A (eds.) Building safer cities: the future of disaster risk. DC: The World Bank, Washington, p 121–135
ICSU (2008) A science plan for integrated research on disaster risk: addressing the challenge of natural and human-induced environmental hazards. Paris
IPCC (2012) Summary for policymakers. In: Field et al. (eds) Managing the risks of extreme events and disasters to advance climate change adaptation. A special report of working groups I and II of the IPCC. Cambridge University Press, UK, p 1–19
Islam N (2001) The open approach to flood control: the way to the future in Bangladesh. Futures 33:783–802
Isunju JB, Schwartz K, Schouten MA, Johnson WP, van Dijk MP (2011) Socio-economic aspects of improved sanitation in slums: a review. Public Health 125:368–376
Ivers LC, Ryan ET (2006) Infectious diseases of severe weather-related and flood-related natural disasters. Curr Opin Infect Dis 19:408–414
Jonkman SN, Vrijling JK, Vrouwenvelder ACWM (2008) Methods for the estimation of loss of life due to floods: a literature review and a proposal for a new method. Nat Hazards 46:353–389
Karim N (1995) Disasters in Bangladesh. Nat Hazards 11:247–258
Keim ME (2008) Building human resilience: the role of public health preparedness and response as an adaptation to climate change. Am J Prev Med 35(5):508–516
Khalequzzaman M (1994) Recent floods in Bangladesh: possible causes and solutions. Nat Hazards 9:65–80
Khalil GM (1990) Floods in Bangladesh: a question of disciplining the rivers. Nat Hazards 3:379–401
Khan MMH (2012) Urban health in megacities of developing countries. Public Health Forum 75:29–30
Khan MMH, Krämer A, Gruebner O (2009) Comparison of health-related outcomes between urban slums, urban affluent and rural areas in and around Dhaka Megacity Bangladesh. Die ERDE 140(1):69–87
Khan MMH, Kraemer A, Pruefer-Kraemer L (2011) Climate change and infectious diseases in megacities of the Indian subcontinent. In: Krämer A, Khan MMH, Kraas F (eds) Health in megacities and urban areas. Springer, Heidelberg, pp 137–154
Khan MMH, Grübner O, Krämer A (2012) Frequently used healthcare services in urban slums of Dhaka and adjacent rural areas and their determinants. J Public Health. doi:10.1093/pubmed/fdr108
Kimani-Murage EW, Ngindu AM (2007) Quality of water the slum dwellers use: the case of a Kenyan slum. J Urban Health 84:829–838
Krämer A, Khan MMH, Jahn HJ (2011) Public health in megacities and urban areas: a conceptual framework. In: Krämer A, Khan MMH, Kraas F (eds) Health in megacities and urban areas. Springer, Heidelberg, pp 3–20
Kunii O, Nakamura S, Abdur R, Wakai S (2002) The impact on health and risk factors of the diarrhoea epidemics in the 1998 Bangladesh floods. Public Health 116:68–74
Luby SP, Agboatwalla M, Painter J et al (2006) Combining drinking water treatment and hand washing for diarrhoea prevention, a cluster randomised controlled trial. Trop Med Int Health 11:479–489
Mirza MMQ (2002) Global warming and changes in the probability of occurrence of floods in Bangladesh and implications. Global Environ Change 12:127–138
Mirza MMQ (2011) Climate change, flooding in South Asia and implications. Reg Environ Change 11(Suppl 1):S95–S107
Mirza MMQ, Warrick RA, Ericksen NJ, Kenny GJ (2001) Are floods getting worse in the Ganges, Brahmaputra and Meghna basins? Environ Hazards 3:37–48
Nath PK, Behera B (2011) A critical review of impact of and adaptation to climate change in developed and developing economies. Environ Dev Sustain 13:141–162
Pahwa S, Kumar GT, Toteja GS (2010) Performance of a community-based health and nutrition-education intervention in the management of diarrhoea in a slum of Delhi, India. J Health Popul Nutr 28:553–559
Rashid H, Hunt LM, Haider W (2007) Urban flood problems in Dhaka, Bangladesh: slum residents’ choices for relocation to flood-free areas. Environ Manag 40:95–104
Schwartz BS, Harris JB, Khan AI et al (2006) Diarrheal epidemics in Dhaka, Bangladesh during three consecutive floods: 1988, 1998, and 2004. Am J Trop Med Hyg 74(6):1067–1073
Shahid S (2010) Probable impacts of climate change on public health in Bangladesh. Asia Pac J Public Health 22(3):310–319
Shaw R (2006) Critical issues of community based flood mitigation: examples from Bangladesh and Vietnam. J Sci Culture 72(1–2):1–17
Tingsanchali T, Karim MF (2005) Flood hazard and risk analysis in the southwest region of Bangladesh. Hydrol Process 19:2055–2069
United Nations (2012) World urbanization prospects: The 2011 revision. United Nations, New York
Wang Z, Patterson CM, Hills AP (2002) A comparison of self-reported and measured height, weight and BMI in Australian adolescents. Asut N Z J Public Health 26:473–478
Wenzel F, Bendimerad F, Sinha R (2007) Megacities-megarisks. Nat Hazards 42:481–491
Acknowledgments
Both surveys were financially supported by the German Research Foundation under its priority programme 1233 “Megacities- Megachallenge: Informal Dynamics of Global Change (KR 947/9-1,2,3 and HO 2568/5-1,2,3)”.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Khan, M.M.H., Gruebner, O. & Krämer, A. Is area affected by flood or stagnant water independently associated with poorer health outcomes in urban slums of Dhaka and adjacent rural areas?. Nat Hazards 70, 549–565 (2014). https://doi.org/10.1007/s11069-013-0829-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11069-013-0829-1