
Abstract
An ecosystem approach was adopted to investigate the interactions among anthropogenic habitat alterations, overcrowding, water insecurity, and enteric diseases in young children in Mexico City. A geographic information system (GIS) was used to define eligible wells and surrounding homesteads. Water quality was obtained from previously published investigations, and bacterial indicators included fecal coliforms and fecal streptococci. A cross-sectional survey was conducted during the rainy season 2002. A total of 1250 eligible households were visited on a random sample basis, and only those with children younger than 5 years of age were interviewed. Data on diarrheal disease (with a recall period of the last 2 weeks) were obtained from 950 children, and their guardians also provided information on housing, water supply, sanitation, and socioeconomic variables. The study found that the risk of diarrheal diseases was higher in children from the households that received drinking water from contaminated wells than from clean wells (odds ratio [OR], 1.7; 95% confidence interval [CI], 1.00–2.86). The final analysis showed that the rate of diarrhea was higher in children from nonowned homes than in those living in owned dwellings (OR, 1.7; 95% CI, 1.04–2.77); the risk was also higher in children from houses with poor sanitation facilities (e.g., latrines or septic tank) than in those from houses connected to a sewage disposal system (OR, 1.7; 95% CI, 1.00–2.93). Children from households perceiving unpleasant characteristics of drinking water showed a higher risk than those without complaints (OR, 2.2; 95% CI, 1.28–3.76). This approach underlines the benefits of interdisciplinary research and may contribute to environmental health protection policy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
When we saw all those cities and villages built on the water, and that straight and level causeway leading to Mexico, we were astounded... It was so wonderful that I do not know how to describe the first glimpse of things never heard of, seen or dreamed before... But today all that I then saw is overthrown and destroyed; nothing is left standing.
—Bernal Díaz del Castillo, The Conquest of New Spain (circa 1568)
Contemporary Mexico City is nested in a naturally closed valley surrounded by a series of mountains. Three thousand years ago, this valley included a lake system that covered approximately 1500 km2. Over the centuries, Aztec groups settled around the shores and developed a highly efficient agricultural system based on man-made terraces (chinampas) constructed with mud recovered from the bottom of the lake and retained with interwoven wooden stick and rods (Rojas, 1995). The combination of terraces, surrounding irrigation canals, and dikes constituted an effective flooding control and crop production ecosystem that supported the large population and allowed the splendor of ancient Mexico City (Soustelle, 1975).
The Spanish arrival (1519) and its sociocultural consequences was one of the earlier waves of globalization. In most of Latin America, the effect from that wave (there were others, of course, e.g., from Asia) resulted in deep land use changes and the introduction of different farming technologies, as well as decline of the indigenous population and natural resources (e.g., gold and silver). In central México, in particular, the “Conquest” meant widespread hydraulic disruption, agricultural decline, and famine; the lakes were gradually drained and practically disappeared throughout the following centuries (Simon, 1995). A long history of drought, floods, and epidemics simply reflects the conflict between ongoing waves of “new” human settlements and the local ecosystems.
The population of the Mexico City metropolitan area (MCMA) is forecasted to be 23.5 million by the year 2015 (Instituto Nacional de Geografía e Informática [National Institute of Statistics, Geography and Informatics; INEGI], 2000). Water supply depends mostly on groundwater reserves (i.e., extraction wells) and is already showing symp-toms of overexploitation, including soil subsidence, clay fractures, and potential downward migration of pollutants. Groundwater contamination may occur if cracked sewers and aging water pipes mix their contents (Ezcurra and Mazari, 1996; Jimenez et al., 2004). Low-income groups, overcrowded in marginal municipalities and slums, carry the heaviest health burden of inadequate shelter, water insecurity, and poor standards of personal hygiene and sanitation (Ezcurra, 1992; World Health Organization, 2002). Exposure to fecal pollution is increasing as a result of economic driving forces, urban sprawl, and weak institutions (Cifuentes et al., 2002, 2004).
Official information on groundwater pollution and health risk in MCMA is scarce and hardly credible (Cifuentes et al., 1999). Available data fail to give a holistic picture of the effect of human activities on both the health of the ecosystem itself and the people who inhabit it. Although the precise definition of an ecosystem still is a matter of debate, in this investigation we adopted the working definition of ecosystem proposed by the Canadian Council of Ministers of the Environment, which states that “for purposes of planning and information gathering, the intrinsic characteristics of a given ecosystem may be better defined by the user, according to the task at hand and the scope of the process. While in general, the limits selected will circumscribe an ecological space such as a watershed or a region, we can also designate a farm, a rural community or an urban subdivision” [Hancock, 1990, unpublished data]. The study described herein was based on the ecosystem approach (Constanza et al., 1998; Yassi et al., 1999; Forget and Lebel, 2001) and addressed the interactions among human health, groundwater resources, the built environment, and sociocultural factors (e.g., lifestyles). As illustrated below, our investigation required the use of complementary research skills, methods, and disciplines.
METHODS
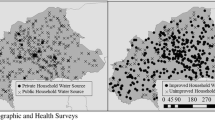
The boundaries of the MCMA were first framed within basic geographic areas. The use of a geographic information system (GIS) allowed overlapping different layers of data, e.g., geologic, hydraulic, and demographic. Spatial data were sourced from municipal information (INEGI, 2000), and a GIS was generated by using Map Info software version 4.0 (Map Info Corp., New York, NY) (Figs. 1 and 2). Eligible basic geographic areas were characterized according to demographic variables, as provided by National Census tracts (INEGI, 2000).

Mexico City metropolitan area (MCMA) hydrologic areas and sampled wells.

Perceived tap water attributes within a basic geographic area (AGEB).
Groundwater Microbiology
A multistage stratified sampling technique was used (Kirkwood, 1988) to select 40 wells from a previous investigation by Mazari et al. (2000; Fig. 1). The number of wells selected allowed for equal representation (probability proportional to size). Water quality indicators included fecal coliforms and fecal streptococci, as reported in previous investigations (Mazari et al., 2000).
Population
“Sentinel” study sites (i.e., homesteads and compounds) were eligible on the basis of housing-related variables, water supplies, and sanitation status, which allowed assessment of heterogeneity. Eligible units were restricted to those situated less than 0.5 km around the 40 selected wells (see the use of GIS, described previously). Initial site visits allowed for the detection of nonresidential blocks (e.g., farming plots, public buildings, and schools), which were discharged from further consideration. A total of 1250 selected dwellings were visited by following a two-stage sample selection technique, which consisted of taking a random sample of homesteads first and then taking a random sample of households (Kirkwood, 1988). Upon previous informed consent, only households with children younger than 5 years of age were fully interviewed (n = 950) during a cross-sectional survey conducted in the rainy season 2002 (June to October). Trained field workers used structured questionnaires to gather data on diarrheal diseases among young children, and the recall period was the previous 2 weeks, as recommended by the World Health Organization (1984). The guardian (i.e., mother) also provided information on housing, water supply, sanitation, and hygiene-related variables.
Statistical Analysis
Data were entered twice, and errors were removed. Whereas the sampling unit was the dwelling, the unit of analysis was the individual (i.e., diarrheal disease episodes). A well was designated as “contaminated” when the presence of bacterial indicators (either fecal coliforms per 1000 ml or fecal streptococci per 5 liters) was reported in water samples. Each child was allocated to one water-quality category, and such exposure was kept throughout the analysis. An episode of diarrhea was defined as three or more lose stools in 24 hours. Potential confounding factors (e.g., maternal literacy) were included in the analysis; every independent variable that showed a statistically significant association with the health outcome was included in the final model. Variables that showed no statistical association with enteric disease throughout the bivariate analyses were discharged from further consideration. Statistical analysis was performed by using multiple logistic regression techniques (Hosmer, 1989). Disease prevalence rates, odds ratios (ORs), 95% confidence intervals (CIs), and P values were derived by using Stata (Stata Corp., College Station, TX). The environmental and health outcome data were overlapped by using a GIS (Map Info).
RESULTS
Table 1 illustrates the overall characteristics of the study population. Nearly 25% of these children lived in crowded homes (three or more individuals per bedroom). One of five relied on water supply from a backyard tap; half of households interviewed declared frequent purchasing of commercially bottled water. Data showed that 13% of the dwellings did not have a connection with municipal sewers. When household guardians (i.e., mother) were asked about perceived features of the water they received from public supplies, approximately 10% complained of unpleasant taste and odor (Table 1).
Figure 2 presents an example of combined of GIS and qualitative data relating to the perception of taste and odor of tap water, as reported by 22 guardians within a single basic geographic area. The figures depicts three positive findings (three of the 22 guardians reported an unpleasant odor in the water). This finding is consistent with the 11.4% of household guardians who reported an unpleasant odor in the study overall (Table 1). The remaining findings regarding the perception of tap water in this basic geographic area were negative; i.e., 19 of the 22 household guardians did not report an unpleasant water odor or taste.
Table 2 shows the results from the multivariate analysis. The final model shown here included only statistically significant associations between the health outcome (i.e., diarrheal diseases) and independent variables. After adjusting for potential confounding factors (e.g., age, sex, and mother’s literacy), we observed that the risk of diarrheal diseases was statistically higher in children from households in the category of polluted wells than those from the group in the clean wells category (OR, 1.7; 95% CI, 1.00–2.86). The final analysis showed an increased risk of diarrheal disease for children living in single-bedroom dwellings (OR, 1.7; 95% CI, 1.04–2.77). A similarly high risk was observed among children from houses with poor standards of sanitation (e.g., septic tank) compared with those living in dwellings connected to the municipal sewage disposal system (OR, 1.7; 95% CI, 1.00–2.93). The highest health risk, however, was detected in children from households describing unpleasant attributes of tap water (i.e., taste and odor; OR, 2.2; 95% CI, 1.28–3.76) when compared with children from households without complaints.
DISCUSSION
For the common citizen and occasional visitor, the most evident environmental hazard in Mexico City may be the smoggy sky, rather than the contamination of soil and groundwater resources. Yet even local environmental health professionals are not fully aware of the extent of the underground water crisis. In the traditional environmental health disciplines, soil and water issues are often seen as belonging to separate domains; fragmentation and increasing specialization have resulted in intellectual myopia and a lack of thorough protection policies. The ecosystem approach used in this investigation allowed for assessment of the complexity of four broad components: public health, the biophysical setting, social factors, and behavior (i.e., lifestyles).
The main results confirmed that the so-called waterborne diseases in Mexico City can be traced to a variety of factors, rather than to a single cause. In particular, structural socioeconomic inequities (e.g., differences in the provision of waste-water infrastructure) were associated with an increased risk of otherwise preventable ill health. As our data showed, children with the heaviest burden of diarrheal diseases were those living in dwellings plagued with fecally polluted water. Thus, waterborne disease provides an ongoing example of the environmental injustice issues that prevail in this society.
The Mexico City ecosystem is showing symptoms of distress as a result of economic activities and dramatic population growth. The more we try to stabilize ecosystems by external measures, the more we restrict their capacity to regenerate themselves (Lebel, 2003). In the 21st century, water supply will depend on increasingly fragile underground reserves and will pose an ongoing challenge to governance and equity measures that affect particularly vulnerable groups (e.g., children and the elderly).
Furthermore, the effects of the ecologic, economic, and public health hazards shown in this study extend far beyond the geographic boundaries of a megacity. Nowadays, the links among enteric disease, poverty, and ecosystem degradation represent a constant catastrophe and send profound and crystal-clear messages to the global community as examples of environmental health problems exacerbated by denial and neglect (Guerrant, 1994). If we define ecohealth in global terms, we may understand why and how endemic diseases and poverty are intimately linked. These health risks, however, are not restricted to developing countries. Industrialized societies (most of which already have sophisticated water treatment technology in place) are facing an increasing number of waterborne outbreaks, and this has fueled debate about environmental health protection measures (Hancock et al., 1977; Levy et al., 1998).
CONCLUSIONS
It is worth quoting Thomas Friedman (1999), when he was questioned about these issues: “... the best way for us to deal with the brutalities of globalization, is by first understanding the logic of the system and its moving parts, and then by figuring out how this system can benefit the most people while inflicting the least amount of pain” (p. 36). The integrated ecosystem approach adopted in this study helps to fulfill Friedman’s recommendation. Needless to say, the ecosystem approach to human health is far from a second-rate research strategy appropriate for use only in poorer countries of the south. Transforming the paradigm entails recognizing that the quality of the human environment and socioeconomic development are inextricably related. It involves transforming traditional and fragmented models and implies a grand convergence of the natural sciences, engineering, social sciences, health sciences, policy analysis, and, of course, the local population.
References
E Cifuentes J Hernández L Venczel M Hurtado (1999) ArticleTitlePanorama of acute diarrheal diseases in Mexico Health & Place (UK) 5 247–255
E Cifuentes L Suarez M Espinoza L Juárez-Figueroa A Martínez-Palomo (2004) ArticleTitleThe risk of Giardia intestinalis infection in children from an artificially recharged groundwater site in Mexico City American Journal of Tropical Medicine & Hygiene 71 65–70
E Cifuentes L Suarez M Solano R Santos (2002) ArticleTitleDiarrheal disease in children from a water reclamation site in Mexico City Environmental Health Perspectives 110 619–624
R Constanza M Mageau B Norton BC Patten (1998) Predictors of ecosystem health D Rapport R Constanza PR Epstein C Gaudet R Levins (Eds) Ecosystem Health Blackwell Science Malden, MA 240–250
E Ezcurra (1992) ArticleTitleCrecimiento y colapso en la cuenca de Mexico Ciencias 25 13–27
E Ezcurra M Mazari (1996) ArticleTitleAre mega cities viable? A cautionary tale from Mexico City Environment 38 6–35
G Forget J Lebel (2001) ArticleTitleAn ecosystem approach to human health International Journal of Occupational and Environmental Health 7 IssueID2 S1–S38
T Friedman (1999) The Lexus and the Oliver Tree First Anchor Books New York
R Guerrant (1994) ArticleTitleTwelve messages from enteric infections American Journal of Tropical Medicine & Hygiene 51 26–35
Hancock CM, Rose JB, Callaham M (1977) The Prevalence of Giardia and Cryptosporidum, in US Groundwater. Proceedings of the International Symposium on Waterborne Cryptosporidum, Denver, CO: American Water Works Association, pp 147–152
DW Hosmer S Lemeshow (1989) Applied Logistic Regression John Wiley and Sons New York
InstitutionalAuthorNameInstituto Nacional de Geografía e Informática (2000) Información Estadísticay Geografía Municipal, Vol 6, INEGI Mexico City, Mexico
B Jimenez M Mazari R Dominguez E Cifuentes (2004) El agua en el Valle de Mexico B Jiménez D Moran O Escolero (Eds) El Agua en Mexico vista desde la Academia Academia Mexicana de Ciencias Mexico City, Mexico 15–32
B Kirkwood (1988) Essentials of Medical Statistics Blackwell Scientific Oxford
J Lebel (2003) Health: An Ecosystem Approach International Development Research Centre Ottawa, Canada
DA Levy MS Bens CF Craun RB Calderon BL Herwaldt (1998) ArticleTitleSurveillance for waterborne-disease outbreaks—United States, 1995–1996 MMWR CDC Surveillance Summaries 47 1–33
M Mazari E Cifuentes E Velazquez J Calva (2000) ArticleTitleMicrobiological groundwater quality in Mexico City Urban Ecosystems 4 91–103
M Rojas (1995) Presente, Pasado y Futuro de Las Chinampas Centro de Investigaciones y Estudios Superiores en Antropología Social Mexico City, Mexico
J Simon (1995) Mexico’s Environment on the Edge, Sierra Club San Francisco, CA
J Soustelle (1975) La vida cotidiana de los Aztecas Fondo de Cultura Económica Mexico City, México
InstitutionalAuthorNameWorld Health Organization (1984) Guidelines for a Sample Survey of Diarrhoeal Disease Morbidity, Mortality and Treatment Rates. WHO Diarrheal Control Program Document WHO/CDD/SER Geneva 84–86
InstitutionalAuthorNameWorld Health Organization (2002) The World Health Report: Environmental Risks WHO Geneva 68–73
A Yassi P Mas M Bonet RB Tate N Fernandez J Spiegel et al. (1999) ArticleTitleApplying an ecosystem approach to the determinants of health in Centro Havana Ecosystem Health 5 3–19 Occurrence Handle10.1046/j.1526-0992.1999.09902.x
Acknowledgments
We thank the Conserva funding agency, the Conacyt research program (Mexico), and the staff of hydraulics (DGCOH) for their support during field work; M. Parkes for her constructive comments; and R. Santos during GIS final work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cifuentes, E., Rodriguez, S. Urban Sprawl, Water Insecurity, and Enteric Diseases in Children from Mexico City. EcoHealth 2, 70–75 (2005). https://doi.org/10.1007/s10393-004-0117-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10393-004-0117-3