
Abstract
This study addresses the long-term trends in heat-related mortality across 29 US metropolitan areas from 1975 to 2004 to discern the spatial patterns and temporal trends in heat vulnerability. Mortality data have been standardized to account for population trends, and seasonal and interannual variability. On days when a city experienced an “oppressive” air mass, mean anomalous mortality was calculated, along with the likelihood that oppressive days led to a mortality response at least one standard deviation above the baseline value. Results show a general decline in heat-related mortality from the 1970s to 1990s, after which the decline seems to have abated. The likelihood of oppressive days leading to significant increases in mortality has shown less of a decline. The number of oppressive days has stayed the same or increased at most metropolitan areas. With US homes near saturation in terms of air-conditioning availability, an aging population is still significantly vulnerable to heat events.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
1 Introduction
Heat has long been recognized and studied as a major hazard to public health (e.g., Kovats and Hajat 2008; Kalkstein et al. 2008). Much work has examined the relative vulnerability of subsets of the population, and has identified age, sex, social isolation, preexisting medical conditions, health status, and poverty as critical determinants of vulnerability (e.g., Curriero et al. 2002; Borrell et al. 2006; Bouchama et al. 2007), although there are significant differences between developed and developing nations (Hajat et al. 2005). Spatially, mid-latitude metropolitan areas with greater summertime temperature variability show stronger responses to heat than desert and semi-tropical cities, where variability is less (e.g., Medina-Ramon and Schwartz 2007; Gosling et al. 2007). More detailed spatial analysis of vulnerability within urban areas has identified neighborhoods with older housing, larger heat islands, and poorer residents as being collectively more vulnerable (Harlan et al. 2006; Smoyer 1998).
Interest in heat impacts has increased over recent years following dramatic heat wave events. Events such as the ‘Chicago heat wave’ in 1995 (Palecki et al. 2001) and the prolonged heat event over much of Europe in 2003 (Pirard et al. 2005, Schär et al. 2004) have identified problems within the infrastructure to deal with such events (Klinenberg 2002). This interest will likely continue to increase, as demographic and likely climate changes substantially increase the potentially vulnerable population over the course of the twenty first century (Confalonieri et al. 2007; Meehl et al. 2007).
Heat watch-warning systems (HWWS), which are becoming more widespread in developed nations, represent an important component in programs to reduce heat-related vulnerability (e.g., Sheridan and Kalkstein 2004; Pascal et al. 2006; Kovats and Ebi 2006). These systems, based on a variety of methodologies that identify hot weather events, typically include some sort of heat-response plan aimed at the most vulnerable subsets of the population. There is little doubt that new, sophisticated HWWSs, and more proactive and elaborate intervention activities, have contributed to reduce heat-related mortality in a number of large urban locales (e.g., Ebi et al. 2004; Palecki et al. 2001). Programs to increase awareness about the negative health impacts of heat have contributed to this reduction as well.
One of the means to evaluate the effectiveness of heat-response plans is to examine the temporal variability in the heat-health relationship. Some research has shown a significant decrease in heat-related mortality over time (Davis et al. 2003; Donaldson et al. 2003; Carson et al. 2006), a trend attributed to increased air-conditioning and improved health care, especially in developed nations. In particular, the research of Davis et al. (2003) has received much attention, particularly because it suggests that heat-related mortality has become less of a problem in most cities. However, the data analysis in this manuscript ends in 1998; several more years’ data have since become available. In addition, Davis’ manuscript evaluates data on a decadal scale; a finer temporal scale may be useful to evaluate these mortality trends in further detail. Understanding changes in vulnerability, along with the potential effectiveness of the HWWSs and associated intervention activities, are particularly important given the projected climate changes which will likely lead to increased heat events over the coming decades (Meehl et al. 2007; Meehl and Tebaldi 2004).
In this research, we examine changes in spatial and temporal patterns of acute heat-related mortality in the United States from 1975 to 2004, utilizing a synoptic climatological method for determining “oppressive” weather. A total of 29 metropolitan areas across the US, representing many different climate types, are analyzed (Table 1; Fig. 1). In addition to assessing changes in heat vulnerability over time, we also address the contribution of the potential factors listed above to these pattern changes.

The 29 cities whose metropolitan areas were studied in this research
2 Materials and methods
2.1 Mortality data
For each of the 29 locations in Fig. 1, daily mortality totals over the 30-year period of study were calculated. These specific cities were selected based upon geographic location and data completeness to permit an evaluation of spatial differences that may exist in mortality trends. Nearest neighbor analysis was conducted to ensure that cities were not geographically clustered in any one location, and the nearest neighbor statistic was 1.31, indicating that the selected cities are randomly to uniformly distributed across the US.
All deaths that occurred in each primary city’s metropolitan area (as defined by the 2000 US Census) were included. As it has long been acknowledged that counting only ‘official’ (coroner-determined) heat-related deaths leads to a significant undercount of the effects of heat (Dixon et al. 2005; Whitman et al. 1997), more broadly defined counts are used in nearly all studies. Additionally, while some studies exclude deaths of those under 65, or deaths due to unnatural causes, it has been found that using totals of all-cause deaths produces results similar to any of these subdivisions, when assessed with regard to meteorological variability (Sheridan and Kalkstein 2004).
Using a common procedure employed by epidemiologists, these daily mortality counts were first age-adjusted to the population distribution of the United States in 2000 across ten distinct age segments. This is accomplished by “weighting” every death based upon each location’s unique age structure. For example, if a metropolitan area has a disproportionate number of elderly compared to the US population in 2000, each elderly death will receive slightly less weight compared to other age groups. On the other hand, if a specific locale has relatively few elderly compared to the US population in 2000, each elderly death will be given additional weighting. To adjust for population changes throughout the period of record, population totals for each age group were compiled from the United States Census for 1970, 1980, 1990, and 2000. A linear interpolation was then used to estimate population counts for the intervening years, a methodology consistent with previous studies (Davis et al. 2004). This methodology allows for direct comparisons between metropolitan areas regardless of age structure, and the final mortality counts are presented as daily deaths per standardized million. For a complete description of the age-standardization procedure, refer to Anderson and Rosenberg (1998). Additionally, there were instances in which known disasters unrelated to heat (e.g., plane crash) had a profound impact on daily mortality totals. In all, there were 25 such days across the 29 metropolitan areas, and these outliers, defined as having a daily adjusted mortality total for injury and poisoning deaths with a z-score of over 10, were removed from analysis.
Once daily mortality counts were age-adjusted, data were then further standardized to account for the seasonal cycle in mortality along with interannual variability. From the age-adjusted data, the mean season cycle was calculated by averaging 11-day centered-mean mortality over the entire period of record (e.g., the mean mortality for June 6 would be the average mortality over June 1–11 for the entire period). Seven-, 9-, 13- and 15-day centered means were also evaluated for several cities, with little change to the significance of the results. This centered-mean mortality value for each day would then be subtracted from the age-adjusted daily mortality to create a new value, with seasonal trend removed, for each day. To account for variability over time, these anomalous values are then subsequently adjusted according to 3-year running mean daily mortality. Thus, to follow the example above, the standardized anomalous mortality used in this analysis for June 6, 2000, after seasonal de-trending, would be adjusted further by subtracting the mean anomalous daily mortality over all days from 1999 to 2001. This final anomalous mortality value, still expressed in deaths per standardized million (DSM), is what is used in this study.
2.2 Weather data
The Spatial Synoptic Classification (SSC) classifies each day at a weather station into one of a number of air masses or weather types, based on temperature, dew point, pressure, wind speed and direction, and cloud cover opacity; for more information, see http://sheridan.geog.kent.edu/ssc.html or Sheridan (2002). In this research, the SSC is utilized to identify “oppressive air masses” (air masses or weather types for which mean mortality is statistically significantly above the summer baseline). There are several reasons for utilizing this method. First, the heat watch-warning systems on which the authors have worked are based on these air masses. Second, the air masses are designed to change in character both spatially and temporally; that is, a typical ‘Dry Tropical (DT)’ day will vary from place to place and month to month (e.g., Table 2). Thus, seasonal patterns can readily be accounted for, and weather’s impact is determined in a relative, rather than absolute, way. Third, these air masses represent holistic and realistic representations of the impact of an entire weather situation upon the human body. The “synoptic approach” has now been used successfully in dozens of analyses of weather/human health interactions, and continues to serve as a benchmark procedure for such studies around the world.
Two of the SSC’s primary air masses—Moist Tropical (MT) and Dry Tropical (DT)—are most frequently correlated with statistically significant increases in heat-related mortality (Sheridan and Kalkstein 2004). MT is warm and very humid, with frequent convective showers and high overnight temperatures, whereas DT is dryer but hotter and sunnier during the daytime. Across much of the US, especially during the summer, at least one of these two air masses becomes quite common, with a frequency of over 80% across parts of Florida. Where a particular air mass is very common, a plus subset (MT+, DT+) has been developed to extract only those days at least one standard deviation (1sd) above weather—type seed-day means for apparent temperature. Thus, MT+ would represent the warmest, most humid subset of MT days. The selection of whether to utilize the plus subsets or the entire air mass is based largely upon their usage in the authors’ heat watch-warning systems, and corresponds to a frequency threshold of 10%. Thus, where mean summertime (defined here as May–August) frequency of MT (DT) is greater than 10% of all days, only MT+ (DT+) is examined. In this study, for all eastern and central metropolitan areas which demonstrate high frequencies of MT incursions—effectively all metropolitan areas east of the Rocky Mountains—only MT+ is examined. Only in the four analyzed ‘Desert’ metropolitan areas is DT frequency above 10%, and hence DT+ only is considered ‘oppressive’ in these locales. Mean frequencies of these oppressive air masses are shown for each city in Table 3. For each city examined, the airport closest to downtown for which the SSC was available was utilized.
2.3 Analysis
Much research has shown that the strongest relationships between heat and health outcomes are at shorter lags (0–3 days; Basu and Samet 2002). To correspond with our heat watch-warning system research, a 0-day lag is used here. The mean anomalous mortality on all oppressive days is calculated, and its difference from zero is tested using a one-sample t-test. To assure a robust sample size, the mean anomalous mortality (in DSM) was tested for the aggregate of both oppressive air masses, not each air mass individually. For the temporal trend analysis, 3-year running subsets were chosen (i.e., 1975–1977, 1976–1978, … 2002–2004) during which mean oppressive air mass mortality was calculated for the entire summer. For this research, summer is considered to be May 1–August 31. This includes typical ‘meteorological summer’ as well as the month of May. This shift to include earlier portions of the heat season is based on research that suggests a greater importance of early season heat events (e.g., Hajat et al. 2005; Sheridan and Kalkstein 2004).
In addition to calculating the mean response, the frequency with which oppressive air masses lead to above-baseline mortality was also assessed. The threshold for “above-baseline mortality” was set at +1sd above the baseline; to accommodate the decreased variability in mortality over time, the standard deviation of mortality was calculated for the summers of each moving 3-year period (1975–1977, 1976–1978, etc.) to correspond with the analyses described above.
3 Results
3.1 Mean mortality response
The mean response across the entire period of study varies significantly from city to city, from a low of 0.1 DSM (deaths per standardized million) in Phoenix, to a high of 2.3 DSM in Portland (Table 3). In general, higher values are observed in the generally cooler locations, areas with high daily summer temperature variability, and northeastern and midwestern metropolitan areas with older housing stock; most of the lower mortality values are observed across warmer, more recently developed southern and western metropolitan areas. A moderately strong negative correlation (r = −0.59) is observed between the mean number of days that are in an oppressive air mass category and the mean mortality response, suggesting a possible dose-response relationship.
In support of previous research, there is a clear decrease in the mean mortality response on oppressive days over the 30-year study period. In terms of linear trends, 23 of the 29 metropolitan areas studied have a negative slope in mean response (17 of those statistically significant at α = 0.05), suggesting decreased vulnerability (Table 3). When grouped into the six regions of study, spatial and temporal patterns become clearer (Fig. 2). Rates have fallen most significantly across the Northeast, Midwest, and Central regions, where mortality rates in the 1970s averaged as high as 2.0–3.0 DSM, and in recent years have been between 0.5 and 1.0 DSM. Across the Pacific region, rates have fallen somewhat less significantly, with greater year-to-year variability observed (likely a function of the lower mean number of oppressive days in this region). Interestingly, across the two least heat-sensitive regions, the Desert and Southeast regions, mortality rates have remained remarkably consistent over time between 0.5 and 1.0 DSM. It thus appears that by the end of the study period, regional variability in mortality responses have become much less apparent across much of the US.

Mean anomalous mortality (in deaths per standardized million) on oppressive air mass days by region. Year listed is middle year in 3-years running mean (e.g., 1976 = 1975–1977)
It is also noteworthy that in most of the metropolitan areas in which heat mortality has decreased, the majority of the downward trend is apparent from the beginning of the study period to the mid-1990s, and the decline has abated over the past 10 years. Since 1996, linear slopes show an increase in mortality response in 20 of 29 metropolitan areas; while most are not statistically significant, it does strongly suggest the decline in heat vulnerability has largely stopped, and may show preliminary signs of reversing.
Despite this general decrease, mortality rates during oppressive air mass episodes are still statistically significantly above expected values in many metropolitan areas (Table 4). In fact, with the exception of several years in the late 1990s, heat-related mortality is still statistically significant in at least 10 of the 29 metropolitan areas, only slightly lower than the number of statistically significant metropolitan areas in the 1970s (Fig. 3). Moreover, especially in the Desert and Southeast regions, statistically significant increases in the number of oppressive days per year (discussed further below) have also been noted, suggesting the potential for increased vulnerability there.

The number of analyzed metropolitan areas for which the increase in mortality on oppressive days is statistically significant (P < 0.05). Year listed is middle year in 3-years running mean (e.g., 1976 = 1975–1977)
3.2 Evaluation of very high mortality days
As the temperature-mortality relationship has been observed to be heteroscedastic (e.g., Sheridan and Kalkstein 2004) with increasing variability in mortality as temperatures reach high levels, there is concern that mean mortality increases could be the result of several notable outlier days. To test the robustness of the results, the percentage of oppressive days on which mortality is “very high”—more than one standard deviation (+1sd) above the baseline—was calculated. Assuming that the data are normally distributed with μ = 0, one would expect approximately 16% of days to exceed this threshold.
Across all metropolitan areas studied, the mean mortality is more than 1sd above the baseline on about 23% of oppressive days, suggesting that there are approximately 50% (23 vs. 16) more days with very high mortality than would be expected if the days were normally distributed with a mean of zero. In comparing metropolitan areas (Table 3), percentages range from 16% in Phoenix (suggesting there is no increased likelihood of significantly elevated mortality) to 34% in New York City, with percentages between 25 and 30% common across the Northeast, Midwest, and Pacific regions, and lower values elsewhere.
In comparison with the mean mortality response, a more consistent pattern emerges in the time trends of the percentage of oppressive days that lead to very high mortality (Fig. 4). A similar general decline in vulnerability is observed, as 19 of the 29 metropolitan areas still exhibit negative slopes; however, in only seven metropolitan areas are the trends statistically significant. Similar to the mean mortality response, there is a general inter-regional convergence through the period of study, and by the early 2000s the percentage of oppressive days with mortality of at least 1sd above the mean has generally remained between 20 and 28%.

Percentage of oppressive air mass days during which mortality totals are at least one standard deviation above the mean, by region. Year listed is middle year in 3-years running mean (e.g., 1976 = 1975–1977)
3.3 Number of oppressive days
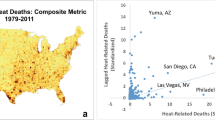
Across the 29 metropolitan areas, corresponding with the general decrease in mortality, there has been a mean increase in the frequency of oppressive days at the rate of 1.2 days/10 years, with the slopes at 10 metropolitan areas statistically significantly upward, though it should be acknowledged that year-to-year variability is far more readily observable than any underlying trend (e.g., Fig. 5). The trend in oppressive days is most significantly upward (Table 3) across Southeast metropolitan areas (Miami, Houston, and New Orleans), desert locations (particularly Las Vegas), and several urban Northeast and Central locales (New York, Philadelphia, and St. Louis). At most other metropolitan areas, small decreases to small to moderate increases (on the order of 1 day/10 years) are observed. A significant trend discrepancy is observed between San Diego and Los Angeles. Much of this can be attributed to the period from 1978 to 1985, when mean summer minimum temperatures at San Diego averaged more than 3°C warmer than Los Angeles, a difference that has since significantly declined.

Number of oppressive days (MT+, DT) for Miami, Florida, by year
Interestingly, despite the positive correlation noted above between the mean number of oppressive days and mean anomalous mortality, when comparing temporal trends in these two variables across each of the 29 metropolitan areas, no correlation (r = .00) is observed. Indeed, for some of the southern metropolitan areas such as Miami for which the increases in oppressive days are greatest, mean mortality on such days is steady. Thus, much of the oppressive day/mortality response may actually be due to the increased variability in oppressive days, rather than the increased numbers of oppressive days.
4 Discussion and conclusions
The results presented above suggest that the heat-mortality relationship has indeed changed significantly over the past 30 years across the US. Improvements in health care and air-conditioning prevalence have likely contributed to the general broad decline. However, the decline has abated across the majority of metropolitan areas since the mid-1990s. In many major US cities, air-conditioning has reached near-saturation; nationwide the percentage of homes without air-conditioning has fallen from 47% in 1978 to 15% in 2005; across the South, only 2% of houses have no air-conditioning availability, and across the Midwest, this figure is less than 10% (US Census 2008). Moreover, rising energy costs are for some a limiting factor in the use of air-conditioning even if a unit is owned (Sheridan 2007), and it is recognized that widespread air-conditioning use in urban areas contributes to increased urban temperatures for those outdoors or without access to air-conditioning.
Considering these statistics, there is little reason to believe that further future drops in heat-related mortality should be expected considering that increased availability of air-conditioning is considered to be a major factor in the downward trend of the 1970s–1990s. Further, since the data suggest that the number of very high mortality days has remained rather constant over much of the evaluated period (between 20 and 28% of the oppressive air mass days exhibit mortality at least 1sd above the mean), much of the decrease in heat-related mortality over the past 30 years can be connected with the general decrease in day-to-day mortality variability (e.g., Carson et al. 2006).
The relationship between the level of vulnerability, and the frequency and interannual variability of oppressive days is clearly complex. In support of previous research (e.g., Kalkstein et al. 2008), there is in general a greater response to heat in locales where there are fewer oppressive days, and these are also generally the locales with the greatest summer climate variability. However, some of this inverse correlation between mortality and frequency of oppressive days may be a result of the method used; that is, if a different definition were used for a city (e.g., evaluating only days with maximum or minimum temperatures greater than 1sd above the mean, rather than using the air mass-based approach), the response rate might be different. However, some of the hottest metropolitan areas used in this study have operational heat-watch warning systems (HWWS) developed by the authors (e.g., Phoenix, Houston), and no statistically significant stratification among ‘oppressive’ days has been identified; that is, above the air-mass threshold the days are not deadlier even as temperatures increase. This suggests that a more rigid climatological definition of oppressive days would not increase vulnerability in some of the warmer metropolitan areas. Indeed, the general increase in the number of oppressive days, with little decrease in mean mortality response, has resulted in potential increases in heat-related vulnerability across many of the warmer metropolitan areas.
There are uncertainties regarding the future direction of heat-related mortality, even if this research supports the notion that the decline has abated. First, the role of “harvesting” or “mortality displacement” needs further investigation. Is elevated mortality during an excessive heat event merely a function of vulnerable people dying a few days earlier than they would have anyway (e.g., Hajat et al. 2005), or do most of these people represent unique deaths that would not have occurred if the heat event did not happen (e.g., Kalkstein 1998)? Are mortality displacement proportions changing through time? Also, what is the impact of the new and more sophisticated HHWS upon heat-related mortality? These new systems have frequently been associated with more elaborate intervention activities by stakeholders; there have been a few studies evaluating their efficacy (Ebi et al. 2004; Sheridan 2007; Kalkstein and Sheridan 2007), but more study is needed and now potentially feasible, as many of these systems have now been running for 3 years or more.
Finally, the results suggest that there is little reason to believe that the decline in heat-related mortality observed from the 1970s to 1990s will proceed in earnest again in the foreseeable future. It is quite possible that, in individual metropolitan areas with newly developed heat health warning systems, some declines will hopefully occur, emphasizing the importance of proper alert methodologies and intervention procedures during extreme heat events. However, with the number of oppressive air-mass days increasing, the approaching air-conditioning saturation, and the increasing population of vulnerable age groups as the US population ages, we suggest that heat will remain the most important weather-related killer in the US for many years to come.
References
Anderson RN, Rosenberg HM (1998) Age standardization of death rates: implementation of the year 2000 standard. Technical report 47. National Vital Statistics Reports, Hyattsville, MD
Basu R, Samet JM (2002) Relation between elevated ambient temperature and mortality: a review of the epidemiologic evidence. Epidemiol Rev 24:190–202. doi:10.1093/epirev/mxf007
Borrell C, Mari-Dell’Olmo M, Rodriguez-Sanz M, Garcia-Olalla P, Caylà JA, Benach J, Muntaner C (2006) Socioeconomic position and excess mortality during the heat wave of 2003 in Barcelona. Eur J Epidemiol 21:633–640. doi:10.1007/s10654-006-9047-4
Bouchama A, Dehbi M, Mohamed G, Matthies F, Shoukri M, Menne B (2007) Prognostic factors in heat wave-related deaths. Arch Intern Med 167:E1–E7. doi:10.1001/archinte.167.20.ira70009
Carson C, Hajat S, Armstrong B, Wilkinson P (2006) Declining vulnerability to temperature-related mortality in London over the 20th century. Am J Epidemiol 164:77–84. doi:10.1093/aje/kwj147
Confalonieri U, Menne B, Akhtar R, Ebi KL, Hauengue M, Kovats RS, Revich B, Woodward A (2007) Human health. In: Parry ML, Canziani OF, Palutikof JP, van der Linden PJ, Hanson CE (eds) Climate change 2007: impacts adaptation and vulnerability. Contribution of working group II to the fourth assessment report of the intergovernmental panel on climate change. Cambridge University Press, Cambridge, UK, pp 391–431
Curriero FC, Heiner KS, Samet JM, Zeger SL, Strug L, Patz JA (2002) Temperature and mortality in 11 cities of the eastern United States. Am J Epidemiol 1555:80–87. doi:10.1093/aje/155.1.80
Davis RE, Knappenberger PC, Novicoff WM, Michaels PJ (2003) Decadal changes in summer mortality in U.S. cities. Int J Biometeorol 47:166–175
Davis RE, Knappenberger PC, Michaels PJ, Novicoff WM (2004) Seasonality of climate-human mortality relationships in US cities and impacts of climate change. Clim Res 26:61–76. doi:10.3354/cr026061
Dixon PG, Brommer DM, Hedquist C, Kalkstein AJ, Goodrich GB, Walter JC, Dickerson CCIV, Penny SJ, Cerveny RS (2005) Heat mortality versus cold mortality: a study of conflicting databases in the United States. Bull Am Meteorol Soc 86:937–943. doi:10.1175/BAMS-86-7-937
Donaldson GC, Keatinge WR, Nayha S (2003) Changes in summer temperature and heat-related mortality since 1971 in North Carolina, South Finland, and Southeast England. Environ Res 91:1–7. doi:10.1016/S0013-9351(02)00002-6
Ebi KL, Teisberg TJ, Kalkstein LS, Robinson L, Weiher RF (2004) Heat watch/warning systems save lives: estimated costs and benefits for Philadelphia 1995–1998. Bull Am Meteorol Soc 85:1067–1074. doi:10.1175/BAMS-85-8-1067
Gosling SN, McGregor GR, Páldy A (2007) Climate change and heat-related mortality in six cities. Part 1: model construction and validation. Int J Biometeorol 51:525–540. doi:10.1007/s00484-007-0092-9
Hajat S, Armstrong BG, Gouveia N, Wilkinson P (2005) Mortality displacement of heat-related deaths. Epidemiology 16:613–620. doi:10.1097/01.ede.0000164559.41092.2a
Harlan SL, Brazel AJ, Prashad L, Stefanov WL, Larsen L (2006) Neighborhood microclimates and vulnerability to heat stress. Soc Sci Med 63:2847–2863. doi:10.1016/j.socscimed.2006.07.030
Kalkstein LS (1998) Climate and human mortality: relationships and mitigating measures. In: Auliciems A (ed) Advances in bioclimatology, vol 5. Springer, New York, pp 161–177
Kalkstein AJ, Sheridan SC (2007) The social impacts of the heat-health watch/warning system in Phoenix, Arizona: assessing the perceived risk and response of the public. Int J Biometeorol 52:43–55. doi:10.1007/s00484-006-0073-4
Kalkstein LS, Greene JS, Mills DM, Perrin AD, Samenow JP, Cohen J-C (2008) Analog European heat waves for U.S. cities to analyze impacts on heat-related mortality. Bull Am Meteorol Soc 88:75–85. doi:10.1175/BAMS-89-1-75
Klinenberg E (2002) Heat wave: a social autopsy of disaster. University of Chicago Press, Chicago
Kovats RS, Ebi KL (2006) Heatwaves and public health in Europe. Eur J Public Health 16:592–599. doi:10.1093/eurpub/ckl049
Kovats RS, Hajat S (2008) Heat stress and public health: a critical review. Annu Rev Public Health 29:41–55. doi:10.1146/annurev.publhealth.29.020907.090843
Medina-Ramon M, Schwartz J (2007) Temperature, temperature extremes, and mortality: a study of acclimatization and effect modification of 50 US cities. Occup Environ Med 64:827–833
Meehl GA, Tebaldi C (2004) More intense, more frequent, and longer lasting heat waves in the 21st century. Science 305:994–997. doi:10.1126/science.1098704
Meehl GA, Stocker TF, Collins WD, Friedlingstein P, Gaye AT, Gregory JM, Kitoh A, Knutti R, Murphy JM, Noda A, Raper SCB, Watterson IG, Weaver AJ, Zhao Z-C (2007) Global climate projections. In: Solomon S, Qin D, Manning M, Chen Z, Marquis M, Averyt KB, Tignor M, Miller HL (eds) Climate change 2007: the physical science basis. Contribution of working group I to the fourth assessment report of the intergovernmental panel on climate change. Cambridge University Press, Cambridge, UK
Palecki MA, Changnon SA, Kunkel KE (2001) The nature and impacts of the July 1999 heat wave in the midwestern United States: learning from the lessons of 1995. Bull Am Meteorol Soc 82:1353–1367. doi:10.1175/1520-0477(2001)082<1353:TNAIOT>2.3.CO;2
Pascal M, Laiidi K, Ledrans M, Baffert E, Caserio-Schönemann C, Le Tertre A et al (2006) France’s heat health watch warning system. Int J Biometeorol 50:144–153. doi:10.1007/s00484-005-0003-x
Pirard P, Vandentorren S, Pascal M, Laiidi K, Le Tertre A, Cassadou S, Ledrans M (2005) Summary of the mortality impact assessment of the 2003 heat wave in France. Eurosurveillance 10:153–156
Schär C, Vidale PL, Lüthi D, Frei C, Häberli C, Liniger MA, Appenzeller C (2004) Variability in European summer heat waves. Nature 427:332–336. doi:10.1038/nature02300
Sheridan SC (2002) The redevelopment of a weather-type classification scheme for North America. Int J Climatol 22:51–68. doi:10.1002/joc.709
Sheridan SC (2007) A survey of public perception and response to heat warnings across four North American cities: an evaluation of municipal effectiveness. Int J Biometeorol 52:3–15. doi:10.1007/s00484-006-0052-9
Sheridan SC, Kalkstein LS (2004) Progress in heat watch-warning system technology. Bull Am Meteorol Soc 85:1931–1941. doi:10.1175/BAMS-85-12-1931
Smoyer KE (1998) A comparative analysis of heat waves and associated mortality in St. Louis, Missouri-1980 and 1995. Int J Biometeorol 42:44–50. doi:10.1007/s004840050082
US Census (2008) American Housing Survey. Available: http://www.census.gov/hhes/www/housing/ahs/ahs.html. Accessed 26 Aug 2008
Whitman S, Good G, Donoghue ER, Benbow N, Shou W, Mou S (1997) Mortality in Chicago attributed to the July 1995 heat wave. Am J Public Health 87:1515–1518
Acknoweldgments
The authors wish to express their appreciation to the US National Weather Service and Environmental Protection Agency for their continued financial support of our heat/health research; and to the two anonymous reviewers for their prompt and thorough reviews.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sheridan, S.C., Kalkstein, A.J. & Kalkstein, L.S. Trends in heat-related mortality in the United States, 1975–2004. Nat Hazards 50, 145–160 (2009). https://doi.org/10.1007/s11069-008-9327-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11069-008-9327-2