
Abstract
To evaluate the efficacy of cognitive rehabilitation therapies (CRTs) for mild cognitive impairment (MCI). Our review revealed a need for evidence-based treatments for MCI and a lack of a theoretical rehabilitation model to guide the development and evaluation of these interventions. We have thus proposed a theoretical rehabilitation model of MCI that yields key intervention targets–cognitive compromise, functional compromise, neuropsychiatric symptoms, and modifiable risk and protective factors known to be associated with MCI and dementia. Our model additionally defines specific cognitive rehabilitation approaches that may directly or indirectly target key outcomes–restorative cognitive training, compensatory cognitive training, lifestyle interventions, and psychotherapeutic techniques. Fourteen randomized controlled trials met inclusion criteria and were reviewed. Studies markedly varied in terms of intervention approaches and selected outcome measures and were frequently hampered by design limitations. The bulk of the evidence suggested that CRTs can change targeted behaviors in individuals with MCI and that CRTs are associated with improvements in objective cognitive performance, but the pattern of effects on specific cognitive domains was inconsistent across studies. Other important outcomes (i.e., daily functioning, quality of life, neuropsychiatric symptom severity) were infrequently assessed across studies. Few studies evaluated long-term outcomes or the impact of CRTs on conversion rates from MCI to dementia or normal cognition. Overall, results from trials are promising but inconclusive. Additional well-designed and adequately powered trials are warranted and required before CRTs for MCI can be considered evidence-based.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Broadly speaking, the term mild cognitive impairment (MCI) is used to describe an older population with cognitive deficits not severe enough to warrant a diagnosis of dementia (Petersen 2004). It has been viewed as an intermediate stage between normal aging and dementia (Mariani et al. 2007) and as the prodromal stage for a variety of dementing neurodegenerative disorders, including Alzheimer’s disease (AD), frontotemporal dementia, dementia with Lewy bodies, and vascular dementia (Petersen 2004). Cognitive impairment associated with MCI can affect virtually all domains including memory, language, attention, visuospatial functioning, and executive functions (Arnaiz and Almkvist 2003). Depending on the study, prevalence rates of MCI within older adult populations have been estimated at 3–42 % (Ward et al. 2012). Estimated conversion rates of MCI to dementia have ranged from 2 to 31 %, with a mean annual conversion rate of 10.2 % (Bruscoli and Lovestone 2004). Studies indicate that 14–40 % of those with MCI return to normal cognitive function over time (Ganguli et al. 2004; Koepsell and Monsell 2012; Larrieu et al. 2002; Manly et al. 2008; Tschanz et al. 2006), and many individuals also exhibit a persistent form of MCI without converting to dementia (Manly et al. 2008; Schonknecht 2011).
Historically, many diagnostic criteria were proposed to describe the early cognitive changes that occur in older adults (Ward et al. 2012). Due to lack of adequate diagnostic criteria, approximately 13 years ago Petersen et al. (1999) developed an MCI diagnostic and classification system which is now widely adopted. This classification system yields four MCI subtypes and categorizes cognitive deficits as either amnestic or non-amnestic, and as either single cognitive domain or multiple cognitive domains (Petersen 2004). More recently, the National Institute on Aging and the Alzheimer’s Association put together a workgroup that recommends two sets of criteria for MCI due to AD, one set of criteria for healthcare providers without access to neuroimaging or cerebrospinal fluid analysis, and another for researchers and clinical trials that incorporate these biomarkers (Albert et al. 2011). This workgroup recommends almost identical criteria as did Petersen et al. (1999) for the establishment of a clinical diagnosis of MCI: 1) a subjective cognitive complaint whereby the patient, an informant, or a clinician report a decline over time, 2) objective evidence of cognitive impairment in one or more cognitive domains using formal or bedside testing, 3) the impact of cognitive impairments on daily functioning does not preclude independence, 4) the person does not meet criteria for dementia. Based on whether biomarkers have been tested and whether results are informative, this workgroup’s proposed system also yields research diagnostic categories that indicate the likelihood of underlying AD (i.e., MCI–Core Clinical Criteria; MCI due to AD–Intermediate Likelihood; MCI due to AD–High Likelihood; MCI–Unlikely due to AD).
Although the cognitive impairments associated with MCI do not preclude independent functioning, research suggests that individuals with MCI nevertheless experience changes in their psychological and daily functioning as well as quality of life (QOL) (Albert et al. 2011; Gold 2012; Winblad et al. 2004; Teng et al. 2012). A recent review article noted that neuropsychiatric symptoms are very common in individuals with MCI, with prevalence rates of at least one neuropsychiatric symptom ranging from 35 to 85 % (Monastero et al. 2009). The most common neuropsychiatric issues associated with MCI include depression, anxiety, irritability, agitation, apathy, euphoria, disinhibition, delusions, hallucinations, and sleep disorders (Apostolova and Cummings 2008; Bomboi et al. 2010; Ellison et al. 2008; Monastero et al. 2009). Areas of daily functioning most frequently impacted by MCI include appointment scheduling/attendance, transportation issues, and financial management (Gold 2012). Individuals with multi-domain MCI tend to demonstrate greater functional limitations than those with single domain MCI (Gold 2012). Individuals with MCI additionally report a reduced QOL relative to older adults without cognitive impairment, and this reduced QOL is associated with increased neuropsychiatric symptoms and reduced daily functioning (but not with objective cognitive performance) in older adults with MCI (Teng et al. 2012). The hypothesis that MCI is a transitional stage between normal aging and dementia implies that individuals with MCI are at risk for significant functional impairment and an eventual inability to live independently which would further decrease their QOL (Petersen et al. 2009).
MCI likely stems from multiple etiologies. In addition to neurodegenerative conditions like AD, Dementia with Lewy Bodies, and Parkinson’s disease, other possible etiologies for MCI include cardiovascular, metabolic, endocrine, traumatic, and psychiatric origins (Etgen et al. 2011; Mariani et al. 2007; Winblad et al. 2004). Likewise, numerous demographic, genetic, disease, and lifestyle factors have been associated with increased or decreased risk for diagnosis with MCI. Although a thorough discussion of each of these risk and protective factors is beyond the scope of this paper, a non-exhaustive list has been provided in Table 1. Notably, the risk and protective factors associated with MCI are similar to those associated with conversion to dementia (Gomar et al. 2011; Li et al. 2011a, b; Ravaglia et al. 2008; Schmand et al. 2012; Yu et al. 2012). The modifiable risk and protective factors that are associated with lifestyle habits are of particular interest to clinicians working with individuals with MCI since they can serve as the focus of preventative interventions and rehabilitation efforts. For example, some cognitive rehabilitation therapies (CRTs) for MCI involve lifestyle interventions, which for the purposes of this review, are defined as behavioral interventions designed to decrease the frequency of negative lifestyle behaviors (i.e., smoking, heavy alcohol consumption) and/or increase the frequency of positive lifestyle behaviors (i.e., Mediterranean diet, physical activity, cognitively-stimulating activities) known to impact risk of MCI.
Both pharmacological and non-pharmacological interventions have been recommended for the treatment of MCI. Although a number of pharmacological strategies have been evaluated (e.g., acetylcholinesterase inhibitors such as donepezil, rivastigmine, and galantamine, Vitamin E, rofecoxib, piracetam, memantine) or are under current investigation, these are reviewed elsewhere (Jelic et al. 2006; Karakaya et al. 2013; Popp and Arlt 2011) and are beyond the scope of the present paper. Instead, the current paper evaluates the efficacy of non-pharmacological interventions for MCI, specifically CRTs, by reviewing randomized controlled trials of such interventions (see Tables 2 and 3). Although terminology varies across settings and publications, for the purposes of this review, CRT is defined as any systematic behavioral therapy specifically designed to improve cognitive performance, help individuals to compensate for impaired cognitive performance, or enable individuals to adapt to impaired cognitive performance. As described in the next section, CRTs include lifestyle interventions, psychotherapy, and/or traditional cognitive training approaches as long as they are specifically implemented as a treatment to address cognitive impairments.
Theoretical Rehabilitation Model of MCI: Course, Risk and Protective Factors, and Treatment Targets
A theoretical rehabilitation model of MCI can provide a conceptual framework to inform development of CRTs for MCI as well as to guide selection of appropriate outcome measures for clinical trials that evaluate the impact of these interventions. Here we offer a provisional theoretical rehabilitation model based on the available literature that was reviewed and summarized in the “Introduction”, as well as the clinical trials that were systematically reviewed in the “Results” section below. In this model (Fig. 1), MCI is viewed as an intermediate stage between healthy age related cognitive decline (i.e., normal cognition) and dementia, though potential outcomes of MCI can also include chronic MCI without conversion to dementia or a return to normal cognition. The etiology of MCI and dementia are viewed as multifactorial; risk factors contribute toward an increased risk of MCI and dementia, while protective factors contribute toward a reduced risk. Thus, brain function and dysfunction are mediated and moderated by multiple risk and protective factors, including those listed in Table 1. In some individuals, the cumulative and interactive impact of these factors on the brain results in the behavioral manifestation known as MCI which, as depicted in Fig. 1, is characterized by three types of symptoms : (a) mild cognitive compromise (measured by objective neuropsychological tests), (b) mild functional compromise not yet precluding independent living (evaluated by measures of daily functioning and QOL), and (c) commonly associated neuropsychiatric symptoms such as depression, anxiety, fatigue, and sleep difficulties (measured by neuropsychiatric symptom severity scales).

Theoretical rehabilitation model of mild cognitive impairment (MCI) to guide the development and evaluation of cognitive rehabilitation therapies (CRTs) for MCI. In this provisional rehabilitation model, MCI is viewed as an intermediate stage between normal cognition and dementia. Individuals with MCI may alternatively return to normal cognition or present with a persistent MCI that does not convert to dementia. The etiology of MCI and dementia are viewed as multifactorial, and a range of risk and protective factors, including those listed in Table 1, contribute toward increased or decreased risk, respectively. In some individuals, the cumulative and interactive impact of these factors on the brain results in the behavioral manifestation known as MCI which is characterized by three types of symptoms: (a) mild cognitive compromise (measured by objective neuropsychological tests), (b) mild functional compromise not yet precluding independent living (evaluated by measures of daily functioning and quality of life), and (c) commonly associated neuropsychiatric symptoms such as depression, anxiety, fatigue, and sleep difficulties (measured by neuropsychiatric symptom severity scales). Based on this model, the figure identifies the key intervention targets that CRTs for MCI are likely to address. Specifically, CRTs can target the symptoms of MCI (i.e., cognitive compromise, functional compromise, or associated neuropsychiatric symptoms). Or, they may target modifiable risk and protective factors, particularly the lifestyle factors that are highlighted in the figure because they are known to increase (depicted as arrows with plus signs) or decrease (depicted as arrows with negative signs) risk for MCI and dementia. In a clinical trial, appropriate intervention outcomes would include reducing MCI symptoms (i.e., symptom management), reducing the conversion rate from MCI to dementia (i.e., preventing dementia), or increasing the conversion rate from MCI to normal cognition (i.e., curing MCI)
This theoretical rehabilitation model yields a number of plausible intervention targets for individuals with MCI, which are highlighted in Fig. 1 and include the symptoms of MCI (i.e., cognitive compromise, functional compromise, and neuropsychiatric symptoms) as well as modifiable risk and protective factors, particularly the lifestyle factors known to be associated with risk of MCI. Although CRTs are heterogeneous in terms of content and methods, integration of the literature with our model indicates that they can be designed to include any combination of four broad approaches, each directly or indirectly targeting different aspects of the model. Regardless of the combination of approaches used, all CRTs aim to reduce the symptoms of MCI (i.e., symptom management), delay or prevent progression to dementia (i.e., prevention of dementia), or increase the rate of conversion to normal cognition (i.e., curing MCI): 1) Restorative cognitive training most directly targets cognitive compromise (a). It aims to enhance or restore cognitive abilities, potentially through neuroplastic mechanisms. A common restorative approach utilizes structured and repeated practice of specific cognitive tasks and mental exercises that may or may not be computerized as a means of improving abilities in specific cognitive domains. 2) Compensatory cognitive training most directly targets functional compromise (b). It teaches individuals skills and strategies to compensate for cognitive impairments so that the impact of these deficits on daily function and QOL can be reduced. Compensatory strategies can include internal strategies (e.g., using visual imagery, chunking or acronyms to compensate for memory difficulties, using structured problem-solving and planning methods to compensate for executive dysfunction), external strategies (e.g., using day planners, timers, and navigation devices), or environmental strategies (e.g., setting up a quiet work space devoid of visually distracting stimuli). 3) Lifestyle interventions most directly target modifiable risk and protective factors, namely the positive and negative lifestyle factors highlighted in Fig. 1, that are associated with MCI or dementia. Lifestyle interventions educate individuals about the cognitive benefits of healthy lifestyle practices and the negative consequences of unhealthy lifestyle practices and encourage individuals to make changes to their life to improve the balance of these risk and protective factors. Lifestyle strategies can include regular physical exercise, healthy nutrition (i.e., Mediterranean diet), frequent participation in cognitively-stimulating activities, and reduction of other modifiable risk factors such as smoking and heavy alcohol consumption. Lifestyle approaches either directly engage individuals in healthy lifestyle practices (e.g., through an exercise, diet, or leisure time program) or they aim to change lifestyle practices and behaviors through education, encouragement, and other behavioral strategies (e.g., motivational interviewing) with the goal of improving MCI outcomes. Lifestyle interventions do not include interventions that are restricted to basic MCI psychoeducation (e.g., definitions of MCI, prognosis, etiology) or administration of specific dietary supplements (e.g., Vitamin B, folic acid, omega-3 fatty acids) or medications. 4) Psychotherapeutic interventions most directly target neuropsychiatric symptoms (c) that are common among individuals with MCI (e.g., depression, anxiety, fatigue, poor sleep). Unlike lifestyle interventions, this approach incorporates more traditional psychotherapy techniques to address accompanying neuropsychiatric symptoms and thus can include relaxation exercises, mindfulness techniques, skills to manage stress, fatigue, and poor sleep, and cognitive behavioral techniques such as cognitive restructuring to address negative thoughts and feelings related to MCI.
It should be noted that comprehensive treatment for MCI is likely to include services other than CRTs. Indeed, based on this rehabilitation model, other risk factors not highlighted in Fig. 1, such as many of the disease factors listed in Table 1, are likely best addressed through referral to other specialty providers for medications and/or other interventions besides CRT (e.g., diabetes, renal failure, polypharmacy). Some risk factors like cardiovascular disease or sleep disorders could benefit from both medical and behavioral interventions, and some risk factors may be addressed through both elements of CRT as well as other specialty providers (e.g., depression, smoking).
Lastly, it is worth acknowledging that there can be some overlap between the four CRT approaches described above. For example, restorative cognitive training contrasts with compensatory cognitive training by focusing on extensive repetition of carefully designed cognitive tasks (usually specific to an individual’s deficits, such as N-back tasks to enhance attention) as a way of strengthening neural circuits and improving performance on similar tasks through generalization. Compensatory cognitive training instead focuses on teaching a range of compensatory strategies (i.e., internal, external, and environmental) that an individual then practices throughout their daily life (e.g., using a planning worksheet to facilitate completion of important home and work projects). An individual may nevertheless employ certain compensatory skills while engaging in restorative exercises (e.g., chunking information). Moreover, while compensatory cognitive training focuses on application of strategies to improve daily functioning, use of these skills may also improve an individual’s objective cognitive performance on certain tests (e.g., categorizing during list learning tests). Similarly, although a lifestyle intervention aims to increase or decrease the frequency of a lifestyle behavior associated MCI risk (i.e., exercise, cognitively-stimulating activities, heavy alcohol consumption), certain psychotherapeutic strategies could be employed to achieve this aim (e.g., motivational interviewing). Likewise, although psychotherapeutic interventions use more traditional psychotherapeutic techniques to target neuropsychiatric symptoms associated with MCI (e.g., mindfulness to address depression and anxiety), lifestyle interventions can also reduce neuropsychiatric symptoms (e.g., exercise). Despite this overlap, the distinctions are offered as part of the proposed provisional rehabilitation model to aid in the development, evaluation, and comparisons of future CRTs. While some providers clearly identify with and employ only one approach, others integrate several. Thus, these distinctions may help the field ultimately determine which elements most effectively treat which aspects of MCI.
Objectives
The primary objective of this review is to evaluate the evidence for the efficacy of CRTs for older adults with MCI. As with other forms of rehabilitation (e.g., physical, occupational), CRTs aim to enhance an individual’s daily functioning and QOL, rather than to treat disease per se. Thus, our review will evaluate the efficacy of CRTs for older adults with MCI in terms of their short-term (<1 month following the intervention) and long-term (≥1 month following the intervention) impact on objective cognitive performance, with a focus on attention/information processing, memory, executive function, and global cognition. Additionally, we will evaluate efficacy in terms of CRTs impact on subjective cognitive complaints, daily functioning/everyday functioning, QOL, neuropsychiatric symptom severity, and other related constructs. Lastly, we will evaluate whether CRTs reduce conversion rates to dementia.
Based on our theoretical model and in an attempt to elucidate which approaches are most effective, we will distinguish between interventions that are Focused on one approach (i.e., restorative cognitive training, compensatory cognitive training, lifestyle interventions, psychotherapeutic interventions) versus Comprehensive interventions that entail multiple approaches. Because interventions that entail either restorative or compensatory cognitive training approaches can target one or more cognitive domains, we will also distinguish between Single Domain and Multi-Modal CRTs.
Methods
A systematic review of peer-reviewed journal articles was conducted on 10/25/12 using Pub Med. The following search terms were applied to all fields: (mild cognitive disorder OR MCI OR mild cognitive decline) AND (cognitive rehabilitation OR cognitive intervention OR cognitive training OR cognitive stimulation OR attention rehabilitation OR attention training OR information process training OR memory rehabilitation OR memory intervention OR memory training). Filters included publication dates between 1/1/1990 and 10/25/12, clinical trial, and published in English.
Articles included in the final review met the following criteria: 1) The study primarily evaluated the effects of a CRT intervention for MCI. 2) The study was a randomized controlled trial that quantitatively assessed outcomes at both pre- and post-intervention. 3) The study included at least one intervention group meeting criteria for MCI, and at least one demographically similar group of non-treated adults meeting criteria for MCI, AND the study employed adequate statistical analyses to compare change from pre- to post intervention across groups (e.g., repeated measures ANOVA, mixed effects model, slope analysis). If the study did not employ a repeated measures between group analysis or slope analysis, at a minimum the study compared change across time within each group, and then also compared results across groups at both pre- and post- intervention. 4) If individuals with dementia were included in the study, the results from individuals with MCI were reported separately from those with dementia. 5) Samples included community dwelling adults. 6) Sample sizes were ≥5/group. 7) The study included pre- and post-intervention outcome measures that evaluated objective cognitive performance using neuropsychological tests AND/OR self-report outcome measures that assessed subjective cognitive complaints, daily functioning/everyday functioning, QOL, neuropsychiatric symptom severity, or another related construct. We excluded studies which primarily focused on neuroimaging results.
Results: Efficacy of CRTs for MCI
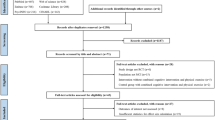
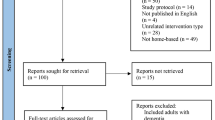
293 articles were initially identified through PubMed using the search terms described. After scanning titles and abstracts from these 293 articles, 34 articles were identified as potentially meeting our review criteria. The other 259 articles were rejected because it was clear from the abstracts that they did not meet one or several of the seven review criteria outlined in the “Methods”. The most common exclusions were that the study did not include a CRT intervention (e.g., the study was a medication trial) or that it did not include a group with MCI (e.g., the groups included only healthy older adults or adults with dementia). The complete manuscripts of the 34 remaining articles were then reviewed, and 20 additional articles were rejected because they did not meet all seven criteria outlined in the “Methods”. The most common exclusion at this stage was that the study was not a randomized controlled trial. In the end, 14 articles were found eligible for final review based on all seven criteria described in our “Methods”.
A summary of key findings and design characteristics/outcomes from the studies that were selected for final review can be found in Tables 2 and 3, respectively. Results are also described by intervention type below. Only results from studies with p ≤ 0.050 were deemed significant and are described as such in the tables and text. In terms of focused interventions (i.e., using only one approach), we identified seven lifestyle interventions, and one compensatory cognitive training intervention (single-domain, focused on memory). In terms of comprehensive interventions that utilized multiple approaches, we identified two single-domain interventions focused on memory, and three multi-modal interventions focused on multiple domains.
Focused Lifestyle Interventions
Over the past decade there has been a substantial increase in the scientific literature examining lifestyle interventions as a means to stave off negative cognitive aging outcomes. The bulk of the evidence suggests that exercise and cognitively stimulating activities are effective behavioral interventions for improving cognition and lowering risk of dementia (Jak 2012). However, to date, most evidence has come from epidemiological and cross sectional studies (Sofi et al. 2011; Verghese et al. 2006; Wilson et al. 2002, 2007, 2012); randomized trials have been less common. Furthermore, most existing studies have targeted normally aging populations while fewer have evaluated the ability of these strategies to positively impact outcomes in those who already have MCI.
Our search produced seven randomized controlled trials investigating lifestyle interventions in individuals with MCI. Rather than relying on lifestyle education and encouragement, all of these studies directly engaged participants in a program of cognitively stimulating activity (Kwoz et al. 2011), physical activity (Baker et al. 2010; Lam et al. 2011; Nagamatsu et al. 2012; Scherder et al. 2005; van Uffelen et al. 2008), or diet (Bayer-Carter et al. 2011). As a whole, these studies demonstrated that lifestyle interventions can significantly improve objective cognitive performance in those with MCI. Specifically, significant (p ≤ 0.050) improvements in executive functioning were noted following aerobic exercise interventions of at least 30 min per day, at least 3 days per week for a minimum of 6 weeks (Scherder et al. 2005). Aerobic activity for at least 45 min per day, 4 to 5 days per week for at least 12 weeks produced significant improvements in more than one cognitive domain (Baker et al. 2010; van Uffelen et al. 2008). Non-aerobic activity, namely resistance training and tai chi, was significantly associated with improvements in executive functioning and memory (Nagamatsu et al. 2012) and attention (Lam et al. 2011) in individuals with MCI. Following a lower fat and glycemic index diet for 4 weeks resulted in significant increases in visual memory (Bayer-Carter et al. 2011). Practicing a single cognitively stimulating activity, namely calligraphy with a trained instructor, 30 min daily, 5 days a week for 8 weeks led to significant increases in global cognition as compared to a no-intervention control (Kwoz et al. 2011).
These studies in aggregate had several significant limitations. Only one of the seven studies included extended follow-up and did not identify sustained benefits of lifestyle interventions (Scherder et al. 2005). Only one study evaluated the risk of progression to AD and did not find a significant effect (Lam et al. 2011). Other weaknesses of this literature included questionable diagnosis of MCI, relying strongly or exclusively on cognitive screening measures (e.g., Kwoz et al. 2011; Nagamatsu et al. 2012), poor compliance with the prescribed intervention (e.g., Nagamatsu et al. 2012; van Uffelen et al. 2008), and too much of the intervention period working toward criterion and therefore fewer weeks exercising at the prescribed intensity level. The neuropsychological measures examined in the lifestyle intervention trials were largely time-based with no adjustment for processing speed; it is therefore difficult to tease apart whether gains on executive functioning measures were simply increased speed or actual improvements in higher level thinking. The use of no-intervention control groups (e.g., Kwoz et al. 2011) was a significant methodological weakness of several of the studies and limited confidence that any cognitive gains were due to the specific lifestyle intervention (e.g., physical exercise) rather than added social contact or a general increase in daily activity. Finally, objective cognitive performance was the predominant outcome measure in this literature. There was little examination of daily functioning, QOL, or neuropsychiatric symptom changes following lifestyle interventions.
Focused Restorative Cognitive Training Intervention–Single Domain, Attention/Information Processing
Only one trial (Barnes et al. 2009) focused on improving attention through restorative cognitive training, with the notion that improvements in auditory attention and discrimination would yield downstream effects on other cognitive domains, such as memory. Using an intensive computerized cognitive training intervention (100 min/day, 5 days/week for 6 weeks), compared to a robust computer activities control group, the authors found that the experimental group significantly improved on a spatial span task, but not on any other cognitive tests from a comprehensive battery. It is unclear from their design if significant treatment effects would have been found relative to a no intervention or a less cognitively stimulating control group. This study did not examine long-term outcomes or impact on conversion rates from MCI to cognitive normalization or dementia.
Focused Compensatory Cognitive Training Intervention–Single Domain, Memory
One study focused on improving memory through compensatory cognitive training (Greenaway et al. 2012). Greenaway et al. (2012) emphasized training in calendars and notebooks 2 h/week for 6 weeks, including setting appointments, adding “to do” items, and journaling. Compared to controls, the experimental group significantly improved in their daily functioning and memory self-efficacy, and the improvements in daily functioning (but not memory self-efficacy) were sustained 6 months post-intervention. Treatment-associated changes on measures of objective global cognition, QOL, or neuropsychiatric symptom severity did not reach significance, perhaps because these were not the targets of treatment. This study did not examine impact on conversion rates to cognitive normalization or dementia.
Comprehensive Interventions–Single Domain, Memory
The two comprehensive interventions that targeted memory as a single domain (Rapp et al. 2002; Troyer et al. 2008) both provided training in compensatory memory skills, and both employed no-contact control groups. Rapp and colleagues’ (2002) intervention entailed six 2-h sessions spaced across 6 weeks and included training in compensatory memory skills along with psychoeducation and relaxation (breathing) training. Compared to controls, experimental subjects showed no significant improvement on objective memory test performance, but they did endorse significantly better memory abilities at post-test and 6-month follow-up, as well as significantly increased control over memory at post-test and significantly greater use of mnemonic strategies at follow-up. Troyer and colleagues’ (2008) intervention entailed ten 120-min sessions spaced across 6 months, 1 h devoted primarily to compensatory memory training, and the other hour devoted to intensive lifestyle education as well as psychotherapeutic techniques. Although aspects of the intervention were commendable (e.g., inclusion of specialists such as dieticians in the lifestyle component, connecting participants with community resources to increase their activity level, spacing the sessions over many months to potentially extend the benefits of the intervention), most results were non-significant. Compared to the control group, the experimental group reported significantly increased knowledge and use of compensatory memory strategies as well as a significantly stronger belief in the importance of lifestyle factors, which were sustained 3 months post-intervention; however, the experimental group did not evidence significant improvement on measures of objective memory performance, subjective memory complaints, or daily functioning. Because the outcome measures were created by the authors and the psychometric properties of the objective memory measures have not been previously reported, the non-significant results are difficult to interpret (i.e., was the intervention ineffective or were the measures inadequate?). Neither study examined conversion rates to cognitive normalization or dementia.
Comprehensive Interventions–Multi-Modal
Three eligible studies were identified (Kinsella et al. 2009; Buschert et al. 2011; Tsolaki et al. 2011). Two studies included restorative training (Buschert et al. 2011; Tsolaki et al. 2011), two compensatory training (Kinsella et al. 2009; Buschert et al. 2011), two lifestyle approaches (Kinsella et al. 2009; Buschert et al. 2011), and two psychotherapeutic techniques (Kinsella et al. 2009; Tsolaki et al. 2011). Kinsella and colleagues’ (2009) intervention entailed five 90-min sessions spaced across 5 weeks. Like Troyer and colleagues’ (2008) intervention, sessions primarily focused on compensatory memory training and included lifestyle education as well as psychotherapeutic techniques; the intervention also included some training in organization and attention skills to improve learning and memory. Using the same measures as used in the Troyer et al. (2008) study, this intervention was similarly associated with significantly increased knowledge and use of compensatory memory strategies but not with significant improvements in subjective memory complaints, calling into question the sensitivity of this latter measure. Compared with the control group, the experimental group evidenced significant improvements on two objective measures of prospective memory [different from the memory measures used in the Troyer et al. (2008) study] that were sustained 3 months post-intervention.
Buschert and colleagues’ (2011) intervention entailed twenty 120-min sessions spaced over 6 months and employed restorative and compensatory cognitive training in attention, memory and executive function as well as intensive lifestyle interventions that increased participants’ cognitive and physical activity levels through inclusion of reminiscence, psychomotor, recreational, creative, and social activities in class. Relative to the non-treated control group, this intensive intervention was associated with only modest to questionable improvements on well-validated measures of objective cognitive performance, though these results are difficult to interpret because of insufficient statistical power (n = 12/group). Specifically, relative to the control group, the experimental group evidenced improvements on measures of memory (i.e., RBANS story recall) and attention/executive function (i.e., TMT B) that appeared promising but only trended near significance (p < 0.100). Moreover, relative to the experimental group, the control group evidenced significant decline on one measure of global cognition (ADAS-cog), but this pattern only trended toward significance on another measure of global cognition (i.e., MMSE). Although the intervention was not associated with improvements on a QOL measure designed for individuals with AD, it is conceivable that this measure was not sensitive to the issues that individuals with MCI (rather than dementia) encounter. Interestingly, this was the only comprehensive intervention to include a measure of neuropsychiatric symptom severity (i.e., MADRS); the intervention was associated with significant improvements on this measure, suggesting that comprehensive CRTs may effectively target MCI-associated neuropsychiatric symptoms. This study did not evaluate long-term outcomes.
Tsolaki and colleagues’ (2011) intervention entailed sixty 60-min sessions spaced across 6 months, focused on restorative cognitive training in attention, memory, and executive function, and also included psychotherapeutic techniques. Whereas previously described multi-modal studies had sample sizes <25/group, this study was notable for its large sample size (treatment group, n = 104; control group, n = 72). Significant improvements from pre- to post-intervention were observed in the experimental group on objective measures of global cognition, attention, memory, executive function, visuomotor construction, language and daily functioning, whereas the only significant change noted in the control group was a decline in daily functioning. Groups did not differ on any measures pre-intervention, and between group comparisons post-intervention reached significance on one measure of daily functioning and on some but not all objective measures of cognition. However, interpretation of results was limited by a failure to include a repeated measures between group analysis of change over time (e.g., repeated measures ANOVA, mixed effects model, slope analysis). This study did not evaluate long-term outcomes.
Discussion: Summary and Future Directions
Overall, the results of randomized controlled trials evaluating the efficacy of CRTs for MCI can be categorized as encouraging but inconclusive. Perhaps because research on interventions for MCI is only in a very early stage, common design limitations (e.g., small sample size, inclusion of measures without established psychometric properties, less than optimal statistical analyses, failure to include long-term outcomes) hamper interpretation of study findings, particularly non-significant results. Although larger, well-designed randomized controlled trials are required before CRTs for MCI can be considered evidence-based, relevant trends from existing randomized controlled trials are discussed below.
Importantly, the three studies that included measures of compensatory strategy use and knowledge (Troyer et al. 2008; Kinsella et al. 2009; Rapp et al. 2002) and the one study that included a measure of the degree to which individuals rate lifestyle strategies as important (Troyer et al. 2008) found that interventions were associated with significant improvements on these measures. Consistent with research showing that individuals with MCI show learning potential and cognitive plasticity (Akhtar et al. 2006; Schreiber and Schneider 2007), these findings indicate that CRTs can effectively change targeted behaviors, knowledge, and beliefs in older adults with MCI, that adults with MCI are teachable, and that additional CRT trials are warranted with this population.
In terms of effects on objective cognitive performance, all of the seven focused lifestyle interventions and the three comprehensive multi-modal interventions were associated with significant improvements in at least one cognitive domain, suggesting that these approaches are perhaps the most promising (yet difficult to implement). The one single domain intervention that used restorative training to focus on attention found significant improvements in attention. None of the three single domain interventions that focused on memory found significant improvements in any cognitive domain, including memory. However, these latter three studies included only very brief neuropsychological batteries assessing either memory or global cognition. In contrast, most of the other studies employed comprehensive batteries and found one or more effects. Thus, the bulk of the evidence indicates that CRTs for MCI are associated with some improvements in objective cognitive performance, but the pattern of effects on specific cognitive domains is inconsistent across studies.
Other important outcomes were only infrequently assessed across studies and require further investigation. Three of the four studies that included measures of subjective cognitive complaints did not find significant treatment-associated improvements, and results on subjective cognitive complaint measures did not correspond with results on objective cognitive performance measures (i.e., one study found subjective improvement but not objective improvement, two found objective improvement but not subjective improvement, and one found neither objective nor subjective improvement). Although patients’ subjective cognitive complaints are important to understand and warrant further investigation in future trials, the present results suggest that general measures of subjective cognitive complaints may not prove optimal or sensitive to change (e.g., “To what extent would you rate your memory as poor?”). In contrast, two of the three studies that included measures of daily functioning found significant treatment-associated improvements on these measures. This suggests that that individuals with MCI may be better able to perceive changes in their ability to perform daily tasks related to cognition than to assess general cognitive ability per se, and that these more specific self-report measures may be more appropriate for clinical trials (e.g., “How often do memory problems interfere with your ability to follow through with important responsibilities, tasks, or roles in your family life?”). The only study that included a collateral measure of daily functioning (Greenaway et al. 2012) found a significant treatment-associated effect on this measure, raising the possibility that collateral measures of daily functioning might prove more sensitive and reliable than self-report measures. Only two studies examined QOL and neither found significant treatment-associated effects on these measures. Because both of these studies employed QOL measures designed for individuals with AD, it is possible these measures were not sensitive to MCI specific concerns. Of the studies that examined neuropsychiatric symptom severity, two did not find significant treatment-associated effects on these measures, one did, and one did not employ adequate analyses to determine effects. However, since none of the studies that incorporated psychotherapeutic techniques as part of their intervention assessed neuropsychiatric symptom severity, it is unclear whether inclusion of such an approach would more effectively target this outcome. Only two studies examined long-term outcomes, one finding sustained effects, the other not. Only one study evaluated conversion rates to dementia and found non-significant treatment effects.
The studies that were reviewed varied markedly in terms of their intervention design and selected outcome variables, with no clear pattern regarding which intervention approaches were more or less effective. One of the obstacles contributing to the variation in approaches to this research has likely been the lack of a theoretical rehabilitation model of MCI to guide the development of these interventions and the selection of appropriate outcome measures. We have thus proposed a theoretical rehabilitation model (see “Introduction” and Fig. 1) based on the literature that yields four key treatment targets–cognitive compromise, functional compromise, associated neuropsychiatric symptoms, and modifiable risk and protective factors. Based on this model, well-designed clinical trials would, therefore, include outcome measures that assess objective cognitive performance, daily functioning, and neuropsychiatric symptom severity. It will also be important for future studies to ultimately evaluate whether interventions are associated with a reduced conversion rate to dementia or an increased conversion rate to normal cognition, as it remains to be seen whether CRTs have more potential as an intervention to maintain cognitive status (i.e., prevention of dementia) versus an intervention to reverse cognitive decline (i.e., treatment of MCI). Similar to research on other chronic or progressive diseases, it will be difficult and expensive to adequately power such analyses given a mean annual conversion rate from MCI to dementia of 10.2 % (Bruscoli and Lovestone 2004) and the need to follow patients many years, even decades, to establish whether conversion occurs. Because reduced daily functioning and increased neuropsychiatric symptoms have been associated with reduced QOL in adults with MCI (Teng et al. 2012), trials should also include QOL measures, as has been previously recommended (Scholzel-Dorenbos et al. 2007). Given the potentially progressive nature of MCI, concerns have been raised that cognitive impairment might eventually impact an individual’s ability to complete or fully comprehend self-report questionnaires while lack of insight might lead to an inaccurate representation of an individual’s experience (Frank et al. 2011). Thus, clinical trials should include a combination of objective measures, collateral report measures, and self-report measures. They should evaluate both short-term as well as long-term treatment outcomes (e.g., 3 to 6 months post intervention), including an evaluation of whether individuals continue to implement or adhere to a treatment once the intervention has been discontinued (e.g., use of compensatory strategies, use of lifestyle strategies). They should also examine whether, relative to untreated control groups, interventions are associated with improvements on outcome measures or less decline on outcome measures.
Our provisional theoretical rehabilitation model (see “Introduction” and Fig. 1) also defines specific cognitive rehabilitation approaches that may directly or indirectly target key outcomes–restorative cognitive training, compensatory cognitive training, lifestyle interventions, and psychotherapeutic techniques. If well-designed studies are first able to definitively establish the overall efficacy of CRTs for MCI, more detailed studies can later be conducted to evaluate which approaches are associated with the largest effects on which outcomes (even though they may impact several outcomes), and which specific mechanisms operate to produce these improvements. For example, one could hypothesize that in a restorative cognitive training intervention, neuroimaging changes [e.g., increased cortical activation during functional magnetic resonance imaging (fMRI) tasks, increased white matter integrity on diffusion tensor imaging (DTI)] would mediate improvements in objective cognitive performance, and, in a compensatory cognitive training intervention, increased use of compensatory strategies would mediate improvements in daily functioning. Moreover, use of psychotherapeutic techniques in one’s daily life (e.g., relaxation exercises, sleep hygiene principles, cognitive restructuring) could be hypothesized to mediate improvements in neuropsychiatric symptom severity, and increased use of lifestyle strategies (e.g., increased physical activity or cognitively stimulating activity levels, healthier diet, reduced use of tobacco and alcohol) could be hypothesized to mediate cognitive improvements. Future studies could also evaluate the extent to which other intervention characteristics (e.g., number, length and frequency of sessions; lifestyle education versus in-class activities that increase cognitive and physical activity levels; educating about the benefits of external aids versus providing participants with these aids) and patient characteristics (e.g., demographics; premorbid IQ/cognitive reserve; baseline cognitive performance, daily functioning, and neuropsychiatric symptom severity; current and lifetime health and psychiatric status, engagement in cognitively stimulating activities, physical activity level, diet, tobacco and alcohol use) moderate outcomes.
In summary, our review of the literature on CRTs for MCI revealed the need for evidence-based treatments for MCI and the lack of a theoretical model to guide both the development and evaluation of such interventions. Data from existing studies are promising but inconclusive and indicate that additional trials are warranted if they are adequately powered and well-designed. Lastly, the development of standardized “manualized” cognitive rehabilitation interventions are recommended as they would facilitate replication studies, as well as the establishment and dissemination of evidence-based CRTs for MCI.
References
Akhtar, S., Moulin, C. J. A., & Bowie, P. C. W. (2006). Are people with mild cognitive impairment aware of the benefits of errorless learning? Neuropsychological Rehabilitation, 16(3), 329–346.
Albert, M. S., DeKosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., et al. (2011). The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association, 7(3), 270–279.
Anttila, T., Helkala, E., Viitanen, M., Kareholt, I., Fratiglioni, L., Winblad, B., et al. (2004). Alcohol drinking in middle age and subsequent risk of mild cognitive impairment and dementia in old age: a prospective population based study. British Medical Journal, 329(7465), 539.
Apostolova, L. G., & Cummings, J. L. (2008). Neuropsychiatric manifestations in mild cognitive impairment: a systematic review of the literature. Dementia and Geriatric Cognitive Disorders, 25(2), 115–126.
Arnaiz, E., & Almkvist, O. (2003). Neuropsychological features of mild cognitive impairment and preclinical Alzheimer’s disease. Acta Neurologica Scandinavica, 107(s19), 34–41.
Arntzen, K. A., Schirmer, H., Wilsgaard, T., & Mathiesen, E. B. (2011). Impact of cardiovascular risk factors on cognitive function: the Tromso study. European Journal of Neurology, 18(5), 737–743.
Baker, L. D., Frank, L. L., Foster-Schubert, K., Green, P. S., Wilkinson, C. W., McTiernan, A., et al. (2010). Effects of aerobic exercise on mild cognitive impairment. Archives of Neurology, 67(1), 71–79.
Barnes, D. E., Alexopoulos, G. S., Lopez, O. L., Williamson, J. D., & Yaffe, K. (2006). Depressive symptoms, vascular disease, and mild cognitive impairment: findings from the Cardiovascular Health Study. Archives of General Psychiatry, 63(3), 273–279.
Barnes, D. E., Yaffe, K., Belfor, N., Jagust, W. J., DeCarli, C., Reed, B. R., et al. (2009). Computer based cognitive training for mild cognitive impairment: results from a pilot randomized, controlled trial. Alzheimer’s Disease & Associated Disorders, 23(3), 205–210.
Bayer-Carter, J. L., Green, P. S., Montine, T. J., VanFossen, B., Baker, L. D., Watson, S., et al. (2011). Diet intervention and cerebrospinal fluid biomarkers in amnestic mild cognitive impairment. Neurology, 68(6), 743–752.
Beydoun, M. A., Beason-Held, L. L., Kitner-Triolo, M. H., Beydoun, H. A., Ferrucci, L., Resnick, S. M., et al. (2011). Statins and serum cholesterol’s associations with incident dementia and mild cognitive impairment. Journal of Epidemiology and Community Health, 65(11), 949–957.
Bickel, H. (2006). Smoking, alcohol consumption, and dementia. Zeitschrift fur Wissenshcaft und Praxis, 52(1), 48–59.
Bomboi, S., Derambure, P., Pasquier, F., & Monaca, C. (2010). Sleep disorders in aging and dementia. The Journal of Nutrition, Health & Aging, 14(3), 212–217.
Boot, B. P., Boeve, B. F., Roberts, R. O., Ferman, T. J., Geda, Y. E., Pankratz, V. S., et al. (2012). Probably rapid eye movement sleep behavior disorder increases risk for mild cognitive impairment and Parkinson disease: a population-based study. Annals of Neurology, 71(1), 49–56.
Bruscoli, M., & Lovestone, S. (2004). Is MCI really just early dementia? a systematic review of conversion studies. International Psychogeriatrics, 16, 129–140.
Buchman, A. S., Tanne, D., Boyle, P. A., Shah, R. C., Leurgans, S. E., & Bennett, D. A. (2009). Kidney function is associated with the rate of cognitive decline in the elderly. Neurology, 73(12), 920–927.
Buschert, V. C., Friese, U., Teipel, S. J., Schneider, P., Merensky, W., Rujescu, D., et al. (2011). Effects of a newly developed cognitive intervention in amnestic mild cognitive impairment and mild Alzheimer’s disease: a pilot study. Journal of Alzheimer’s Disease, 25, 679–694.
Ceresini, G., Lauretani, G., Maggio, M., Ceda, G. P., Morganti, S., Usberti, E., et al. (2009). Thyroid function abnormalities and cognitive impairment in elderly people: results of the Invecchiare in Chianti study. Journal of the American Geriatrics Society, 57(1), 89–93.
Cheng, G., Huang, C., Deng, H., & Wang, H. (2012). Diabetes as a risk factor for dementia and mild cognitive impairment: a meta analysis. Internal Medicine Journal, 42(5), 484–491.
Clarke, R., Birks, J., Nexo, E., Ueland, P. M., Schneede, J., Scott, J., et al. (2007). Low vitamin B-12 status and risk of cognitive decline in older adults. The American Journal of Clinical Nutrition, 86(5), 1384–1391.
Ellison, J. M., Harper, D. G., Berlow, Y., & Zeranski, L. (2008). Beyond the “C” in MCI: noncognitive symptoms in amnesic and non-amnestic mild cognitive impairment. CNS Spectrums, 13(1), 66–72.
Etgen, T., Bronner, M., Sander, D., Bickel, H., Sander, K., & Forstl, H. (2009). Somatic factors in cognitive impairment. Fortschritte der Neurologie-Psychiatrie, 77(2), 72–82.
Etgen, T., Sander, D., Bickel, H., & Forstl, H. (2011). Mild cognitive impairment and dementia: the importance of modifiable risk factors. Deutches Arzteblatt International, 108(44), 743–750.
Frank, L., Lenderking, W. R., Howard, K., & Cantillon, M. (2011). Patient self-report for evaluating mild cognitive impairment and prodromal Alzheimer’s disease. Alzheimer’s Research & Therapy, 3(6), 35.
Ganguli, M., Dodge, H. H., Shen, C., & DeKosky, S. T. (2004). Mild cognitive impairment, amnestic type: an epidemiologic study. Neurology, 63(1), 115.
Gardener, S., Gu, Y., Rainey-Smit, S. R., Keogh, J. B., Clifton, P. M., & Mathieson, S. L. (2012). Adherence to a Mediterranean diet and Alzheimer’s disease risk in an Australian population. Translational Psychiatry, 2, e164.
Gold, D. A. (2012). An examination of instrumental activities of daily living assessment in older adults and mild cognitive impairment. Journal of Clinical and Experimental Neuropsychology, 34(1), 11–34.
Goldstein, F. C., Levey, A. I., & Steenland, N. K. (2013). High blood pressure and cognitive decline in mild cognitive impairment. Journal of the American Geriatric Society, 61(1), 67–73.
Gomar, J. J., Bobes-Bascaran, M. T., Conejero-Goldberg, C., Davies, P., & Goldberg, T. E. (2011). Utility of combinations of biomarkers, cognitive markers, and risk factors to predict conversion from mild cognitive impairment to Alzheimer disease in patients in the Alzheimer’s disease neuroimaging initiative. Archives of General Psychiatry, 68(9), 961–969.
Greenaway, M.C., Duncan, N.L., Smith, G.E. (2012). The memory support system for mild cognitive impairment: randomized trial of a cognition rehabilitation intervention. International Journal of Geriatric Psychiatry.
Hai, S., Dong, B., Liu, Y., & Zou, Y. (2012). Occurrence and risk factors of mild cognitive impairment in the older Chinese population: a 3-year follow-up study. International Journal of Geriatric Psychiatry, 27(7), 703–708.
Hin, H., Clarke, R., Sherliker, P., Atoyebi, W., Emmens, K., Kirks, J., et al. (2006). Clinical relevance of low serum vitamin B-12 concentrations in older people: the Banbury B12 Study. Age and Ageing, 35(4), 416–422.
Jak, A. J. (2012). The impact of physical and mental activity on cognitive aging. Current Topics in Behavioral Neurosciences, 10, 273–291.
Jelic, V., Kivipelto, M., & Winblad, B. (2006). Clinical trials in mild cognitive impairment: lessons for the future. Journal of Neurology, Neurosurgery, and Psychiatry, 77, 429–438.
Kalmijn, S., Mehta, K. M., Pols, H. A., Hofman, A., Drexhage, H. A., & Breteler, M. M. (2000). Subclinical hyperthyroidism and the risk of dementia: the Rotterdam study. Clinical Endocrinology, 53(6), 733–737.
Karakaya, T., Fusser, F., Schroder, J., & Pantel, J. (2013). Pharmacological treatment of mild cognitive impairment as a prodromal syndrome of Alzheimer’s disease. Current Neuropharmacology, 11(1), 102–108.
Khatri, M., Nickolas, T., Moon, Y. P., Paik, M. C., Rundek, T., Elkind, M. S., et al. (2009). CKD associates with cognitive decline. Journal of the American Society of Nephrology, 20(11), 2427–2432.
Kinsella, G. J., Mullaly, E., Rand, E., Ong, B., Burton, C., Price, S., et al. (2009). Early intervention for mild cognitive impairment: a randomised controlled trial. Journal of Neurology, Neurosurgery, and Psychiatry, 80, 730–736.
Koepsell, T. D., & Monsell, S. E. (2012). Reversion from mild cognitive impairment to normal or near-normal cognition: risk factors and prognosis. Neurology, 79(15), 1591–1598.
Kurella, M., Chertow, G. M., Fried, L. F., Cummings, S. R., Harris, T., Simonsick, E., et al. (2005). Chronic kidney disease and cognitive impairment in the elderly: the health, aging, and body composition study. Journal of the American Society of Nephrology, 16(7), 2127–2133.
Kwoz, T. C., Bai, X., Kao, H. S., Li, J. C., & Ho, F. K. (2011). Cognitive effects of calligraphy therapy for older people: a randomized controlled trial in Hong Kong. Clinical Interventions in Aging, 6, 269–273.
Lam, L. C. W., Chau, R. C. M., Wong, B. M. L., Fung, A. W. T., Lui, V. W. C., Tam, C. C. W., et al. (2011). Interim follow-up of a randomized controlled trial comparing Chinese style mind body (Tai Chi) and stretching exercises on cognitive function in subjects as risk of progressive cognitive decline. International Journal of Geriatric Psychiatry, 26, 733–740.
Larrieu, S., Letenneur, L., Orgogozo, J. M., Fabriquole, C., Amieva, H., Le Carret, N., et al. (2002). Incidence and outcome of mild cognitive impairment in a population-based prospective cohort. Neurology, 59(10), 1594–1599.
Lee, H. B., Richardson, A. K., Black, B. S., Shore, A. D., Kasper, J. D., & Rabins, P. V. (2012). Race and cognitive decline among community-dwelling elders with mild cognitive impairment: findings from the Memory and Medical Care Study. Aging & Mental Health, 16(3), 372–377.
Li, J., Wang, Y. J., Zhang, M., Xu, Z. Q., Gao, C. Y., Fang, C. Q., et al. (2011). Vascular risk factors promote conversion from mild cognitive impairment to Alzheimer disease. Neurology, 76(17), 1485–1491.
Li, H., Li, J., Li, N., Li, B., Wang, P., & Ting, Z. (2011). Cognitive interventions for persons with mild cognitive impairment: a meta-analysis. Ageing Research Reviews, 10, 285–296.
Lopez, O. L., Jagust, W. J., Dulberg, C., Becker, J. T., DeKosky, S. T., Fitzpatrick, A., et al. (2003). Risk factors for mild cognitive impairment in the Cardiovascular Health Study Cognition Study: part 2. Archives of Neurology, 60(10), 1394–1399.
Luck, T., Luppa, M., Briel, S., Matschinger, H., Konig, H. H., Bleich, S., et al. (2010). Mild cognitive impairment: incidence and risk factors: results of the Leipzig Longitudinal Study of the aged. Journal of American Geriatrics Society, 58(10), 1903–1910.
Luck, T., Luppa, M., Briel, S., & Riedel-Heller, S. G. (2010). Incidence of mild cognitive impairment: a systematic review. Dementia and Geriatric Cognitive Disorder, 29(2), 164–175.
Manly, J. J., Tang, M. X., Schupf, N., Stern, Y., Ronsattel, J. P., & Mayeux, R. (2008). Frequency and course of mild cognitive impairment in a multiethnic community. Annals of Neurology, 63(4), 494–506.
Mariani, E., Monastero, R., & Mecocci, P. (2007). Mild cognitive impairment: a systematic review. Journal of Alzheimer’s Disease, 12, 23–35.
Monastero, R., Palmer, K., Qiu, C., Winblad, B., & Fratiglioni, L. (2007). Heterogeneity in risk factors for cognitive impairment, no dementia: population-based longitudinal study from the Kungsholmen Project. The American Journal of Geriatric Psychiatry, 15(1), 60–69.
Monastero, R., Mangialasche, F., Camarda, C., Ercolani, S., & Camarda, R. (2009). A systematic review of neuropsychiatric symptoms in mild cognitive impairment. Journal of Alzheimer’s Disease, 18(1), 11–30.
Nagamatsu, L. S., Handy, T. C., Hsu, C. L., Voss, M., & Liu-Ambrose, T. (2012). Resistance training promotes cognitive and functional brain plasticity in seniors with probable mild cognitive impairment. Archives of Internal Medicine, 172(8), 666–668.
Petersen, R. C. (2004). Mild cognitive impairment as a diagnostic entity. Journal of Internal Medicine, 256, 183–194.
Petersen, R. C., Smith, G. E., Waring, S. C., Ivnik, R. J., Tangalos, E. G., & Kokmen, E. (1999). Mild cognitive impairment: clinical characterization and outcome. Archives of Neurology, 56(3), 303–308.
Petersen, R. C., Doody, R., Kurz, A., Mohs, R. C., Morris, J. C., Rabins, P. V., et al. (2001). Current concepts in mild cognitive impairment. Archives of Neurology, 58(12), 1985–1992.
Petersen, R. C., Knopman, D. S., Boeve, B. F., Geda, Y. E., Ivnik, R. J., Smith, G. E., et al. (2009). Mild cognitive impairment: 10 years later. Archives of Neurology, 66(120), 1447–1455.
Popp, J., & Arlt, S. (2011). Pharmacological treatment of dementia and mild cognitive impairment due to Alzheimer’s disease. Current Opinion in Psychiatry, 24(6), 556–561.
Rapp, S., Brenes, G., & Marsh, A. P. (2002). Memory enhancement training for older adults with mild cognitive impairment: a preliminary study. Aging & Mental Health, 6(2), 5–11.
Ravaglia, G., Forti, P., Lucicesare, A., Rietti, E., Pisacane, N., Mariani, E., et al. (2008). Prevalent depressive symptoms as a risk factor for conversion to mild cognitive impairment in an elderly Italian cohort. The American Journal of Geriatric Psychiatry, 16(10), 834–843.
Roberts, R. O., Geda, Y. E., Knopman, D. S., et al. (2008). The Mayo Clinic Study of Aging: design and sampling, participation, baseline measures and sample characteristics. Neuroepidemiology, 30(1), 58–69.
Sachdev, P. S., Lipnicki, D. M., Crawford, J., Reppermund, S., Kochan, N. A., Trollor, J. N., et al. (2012). Risk profiles of subtypes of mild cognitive impairment: the Sydney Memory and Ageing Study. Journal of the American Geriatric Society, 60(1), 24–33.
Scarmeas, N., Stern, Y., Mayeux, R., Mannly, J. J., Schupf, N., & Luchsinger, J. A. (2009). Mediterranean diet and mild cognitive impairment. Archives of Neurology, 66(2), 216–225.
Scherder, E. J. A., Van Paaschen, J., Deijen, J. B., Van Der Knokke, S., Orlebeke, K., Burgers, I., et al. (2005). Physical activity and executive functions in the elderly with mild cognitive impairment. Aging & Mental Health, 9(3), 272–280.
Schmand, B., Eikelenboom, P., & van Gool, W. A. (2012). Value of diagnostic tests to predict conversion to Alzheimer’s disease in young and old patients with amnestic mild cognitive impairment. Journal of Alzheimer’s Disease, 29(3), 641–648.
Scholzel-Dorenbos, C. J., van der Steen, M. J., Engels, L. K., & Olde Rikkert, M. G. (2007). Assessment of quality of life as outcome in dementia and MCI intervention trials: a systematic review. Alzheimer’s Disease & Associated Disorders, 21(2), 172–178.
Schonknecht, P. (2011). Neurobiological and psychological aspects of mild cognitive impairment – bridging the gap. GeroPsych, 24(2), 63–64.
Schreiber, M., & Schneider, R. (2007). Cognitive plasticity in people at risk for dementia: optimising the testing the-limits-approach. Aging & Mental Health, 11(1), 75–81.
Sofi, F., Valecchi, D., Bacci, D., Abbate, R., Gensini, G. F., Casini, A., et al. (2011). Physical activity and risk of cognitive decline: a meta-analysis of prospective studies. Journal of Internal Medicine, 269(1), 107–117.
Steenland, K., Karnes, C., Seals, R., Carnevale, C., Hermida, A., & Levey, A. (2012). Late-life depression as a risk factor for mild cognitive impairment or Alzheimer’s disease in 30 US Alzheimer’s disease centers. Journal of Alzheimer’s Disease, 31(2), 265–275.
Teng, E., Tassniyom, K., & Lu, P. H. (2012). Reduced quality of life ratings in mild cognitive impairment: analyses of subject and informant responses. The American Journal of Geriatric Psychiatry, 20(12), 1016–1025.
Troyer, A. K., Murphy, K. J., Anderson, N. D., Moscovitch, M., & Craik, F. I. M. (2008). Changing everyday memory behavior in amnestic mild cognitive impairment: a randomised controlled trial. Neuropsychological Rehabilitation: An International Journal, 18(1), 65–88.
Tschanz, J. T., Welsh-Bohmer, K. A., Lyketsos, C. G., Corcoran, C., Green, R. C., Hayden, K., et al. (2006). Conversion to dementia from mild cognitive disorder: the Cache County Study. Neurology, 67(2), 229–234.
Tsolaki, M., Kounti, F., Agogiatou, C., Popsti, E., Bakoglidou, E., Zafeiropoulou, M., et al. (2011). Effectiveness of nonpharmacological approaches in patients with mild cognitive impairment. Neurodegenerative Diseases, 8, 138–145.
Unverzagt, F. W., Ogunniyi, A., Taler, V., Gao, S., Lane, K. A., Baiyewu, O., et al. (2011). Incidence and risk factors for cognitive impairment no dementia and mild cognitive impairment in African Americans. Alzheimer’s Disease and Associated Disorders, 25(1), 4–10.
van Uffelen, J. G. Z., Chinapaw, M. J. M., van Mechelen, W., & Hopman-Rock, M. (2008). Walking or vitamin B for cognition in older adults with mild cognitive impairment? a randomised controlled trial. British Journal of Sports Medicine, 42, 344–351.
Verghese, J., LeValley, A., Derby, C., Kuslansky, G., Katz, M., Hall, C., et al. (2006). Neurology, 66(6), 821–827.
Ward, A., Arrighi, H. M., Michels, S., & Cedarbaum, J. M. (2012). Mild cognitive impairment: disparity of incidence and prevalence estimates. Alzheimer’s & Dementia, 8(1), 14–21.
Wilson, R. S., Mendes De Leon, C. F., Barnes, L. L., Schneider, J. A., Bienias, J. L., Evans, D. A., et al. (2002). Participation in cognitive stimulating activities and risk of incident Alzheimer disease. Journal of the American Medical Association, 287(6), 742–748.
Wilson, R. S., Scherr, P. A., Schneider, J. A., Tang, Y., & Bennett, D. A. (2007). Relation of cognitive activity to risk of developing Alzheimer disease. Neurology, 69(20), 1911–1920.
Wilson, R. S., Segawa, E., Boyle, P. A., & Bennett, D. A. (2012). Influence of late-life cognitive activity on cognitive health. Neurology, 78(15), 1123–1129.
Winblad, B., Palmer, K., Kivipelto, M., Jelic, V., Fratiglioni, L., Wahlund, L. O., et al. (2004). Mild cognitive impairment–beyond controversies, towards a consensus: report of the International Working Group on mild cognitive impairment. Journal of Internal Medicine, 256, 240–246.
Yu, P., Dean, R. A., Hall, S. D., Qi, Y., Sethuraman, G., Willis, B. A., et al. (2012). Enriching amnestic mild cognitive impairment populations for clinical trials: optimal combination of biomarkers to predict conversion to dementia. Journal of Alzheimer’s Disease, 32(2), 373–385.
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Portland Veterans Affairs Medical Center, Portland, Oregon and Oregon Health & Science University, Portland Oregon. This work is in part supported by VA Merit Review awards to DS and JK, a grant from the National Institute on Drug Abuse to MH (2P50DA018165-06A1), and grants from the National Institute on Aging to JK (P30AG08017; P30AG024978). All authors read and approved the final contents of the manuscript.
Conflict of interest statement
The authors have declared that there are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Huckans, M., Hutson, L., Twamley, E. et al. Efficacy of Cognitive Rehabilitation Therapies for Mild Cognitive Impairment (MCI) in Older Adults: Working Toward a Theoretical Model and Evidence-Based Interventions. Neuropsychol Rev 23, 63–80 (2013). https://doi.org/10.1007/s11065-013-9230-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11065-013-9230-9