
Abstract
Background
Immune checkpoint inhibition (ICI) is an emerging immunotherapy for metastatic brain disease (MBD). Current management options include stereotactic radiosurgery (SRS), which has been shown to confer prognostic benefit in combination with ICI. However, the effect, if any, of ICI timing on this benefit is currently unclear. The aim of this study was to evaluate the effect of concurrent ICI with SRS on survival outcomes in MBD compared to non-concurrent ICI administered before or after SRS.
Methods
Searches of 7 electronic databases from inception to April 2018 were conducted following the appropriate guidelines. 1210 articles were identified for screening. Kaplan Meier estimation of 12-month overall survival (OS), local progression free survival (LPFS) and distant progression free survival (DPFS) were pooled as odd ratios (ORs) and analyzed using the random effects model.
Results
A total of 8 retrospective observational cohort studies satisfied selection criteria. Compared to non-concurrent ICI, concurrent ICI with SRS conferred a significant 12-month OS benefit (OR = 1.74; p = 0.011), and comparable 12-month LPFS (OR = 2.09; p = 0.154) and DPFS (OR = 0.88; p = 0.839). These significances were reflected in the subgroup of melanoma metastases.
Conclusion
Based on the trends of our findings, there appears to exist an optimal time window around SRS of which ICI may confer the most survival benefit. However, current literature is limited by a number of clinical parameters requiring further delineation which limits the certainty of these findings. Larger, prospective, and randomized studies will assist in identifying the time period for which ICI can provide the best outcome in MBD managed with SRS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The incidence of Metastatic Brain Disease (MBD) in the general cancer population is approximately 10% [1, 2]. Depending on primary type, prognosis can vary from poor to dismal. Of the most devastating, the historical overall survival (OS) of melanoma MBD is 3–5 months, with up to 95% of mortality events in these patients is attributed to the brain metastases [3, 4]. Thus, optimization of MBD management is important in order to improve survival outcomes.
The rise of immunotherapy in recent years has shown great promise in treating many of the MBD-prone primary cancers such as melanoma, non-small cell lung cancer (NSCLC) and renal cell carcinoma, in particular by immune checkpoint inhibition (ICI) [5,6,7,8,9]. ICI aims to boost antitumor immune responses by preventing the down-regulation of T-cell activation. Currently there are two classes of ICI that have been approved by the Federal Drug and Administration (FDA) for use in treating MBD: anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) monoclonal antibody ipilimumab, and the anti-programmed cell death protein 1 receptor (PD-1) checkpoint inhibitors nivolumab and pembrolizumab [10,11,12].
There is emerging data that describes that synergistic combination of ICI with stereotactic radiosurgery (SRS) confers greater survival prognosis in MBD patients compared to SRS alone [13,14,15,16]. This is in part believed to be attributed to what is termed the ‘abscopal effect’. First reported in 1953, it describes the phenomenon of metastatic tumor regression outside the field of radiation focus, and has been linked functionally to the immune system [17, 18]. It is believed that the use of ICI may provide an avenue to enhance this effect, and improve overall metastatic control, thus improving survival outcomes. However, as the use of ICI in MBD management involving SRS continues to garner interest, it is currently unclear as to if the timing of ICI administration in relation to SRS can affect the survival outcomes of MBD.
The aim of this systematic review and meta-analysis (SRMA) was to evaluate the current literature investigating the pooled effect and quality of evidence regarding the timing of ICI administration in relation to SRS to manage MBD, in particular focusing on whether or not concurrent ICI administration affords different survival outcomes compared to ICI administered non-concurrently, either before or after with SRS management. There were no funding sources used in this study.
Methods
Search strategy
The strategy was designed around the PICOS question format—Do MBD patients who are managed by SRS (population) and concurrent ICI (intervention: concurrent group) when compared to those who received ICI before or after SRS (comparator: non-concurrent group), differ in survival metrics (outcome) based on comparative studies (study type)? The present review was conducted according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines and recommendations [19]. Electronic searches were performed using Ovid Embase, PubMed, SCOPUS, Cochrane Central Register of Controlled Trials (CCTR), Cochrane Database of Systematic Reviews (CDSR), American College of Physicians (ACP) Journal Club and Database of Abstracts of Review of Effectiveness (DARE) from their dates of inception to April 2018. The literature was searched by using the following string of MeSH terms to detect all possible studies: (brain metastases) AND (ipilimumab OR nivolumab OR pembrolizumab OR immunotherapy OR checkpoint) AND (radiosurgery OR radiation OR radiotherapy). Translations of search terms are provided in the Supplementary. The reference lists of all retrieved articles were reviewed independently by two investigators (V.M.L. and A.G.) for further identification of potentially relevant studies. All identified articles were then systematically assessed against the inclusion and exclusion criteria.
Selection criteria
The inclusion criteria used to screen all identified articles were (1) MBD patients, (2) treated by SRS, (3) and received immunotherapy targeting the checkpoint of cell cycle by CTLA-4 or PD-1 inhibition either concurrently or non-concurrently, (4) with reported survival outcomes in (5) patients > 18 years. Concurrent administration was defined as within 4 weeks (or less) of SRS management, and included cases where immunotherapy was interdigitated between multiple SRS cycles. The exclusion criteria applied to all identified articles were (1) case series, (2) involvement of immunotherapy targeting BRAF, and other non-checkpoint targets, (3) primary treatment radiation in the form of whole brain radiation therapy, and (4) no quantitative definition of concurrent administration.
When institutions published duplicate studies with accumulating numbers of patients or increased lengths of follow-up, or when studies reported multiple time courses of the same treated cohort, only the most complete reports were included for quantitative assessment at each time interval. All publications were limited to those involving human patients and in the English language. Reviews, abstracts, case reports, conference presentations, editorials and expert opinions were excluded to minimize potential publication bias and duplication of results.
Data extraction
All survival outcome data were extracted from article texts, tables and figures. Our primary outcome of interest was the OS metric at 12-months as inferred by Kaplan–Meier estimation specific to each study. Other outcomes of interest included local and distal progression free survival, local progression free survival (LPFS) and distant progression free survival (DPFS) respectively, at 12-months, obtained in a similar manner to the OS metric. The LPFS and DPFS were defined as the new progressive enhancement involving and exclusive to the treated intracranial metastatic regions respectively.
Meta-analysis
Odds ratio (OR) was the primary summary statistic of this study, with concurrent administration used as the reference cohort. The outcomes of the included studies were pooled together by meta-analysis of non-integer proportions using a random-effects (RE) model to provide an overall summary statistic. These were presented as forest plots, with the overall heterogeneity statistics provided in-graphic. The I2 statistic was used to estimate the percentage of total variation across studies, owing to heterogeneity rather than chance, with values > 50% considered as substantial heterogeneity [20].
Meta-regression was performed to analyze potential effect modification on overall prognostic trend by a number of study covariates when the outcome was reported by ≥ 4 studies: study year, study size, study duration, mean age, proportion of females, MBD histology (melanoma only vs other combinations), ICI choice (ipilimumab only vs other combinations) and definition of concurrent use (2 vs. 4 weeks). All p values were 2-sided with significance set at p < 0.05. Statistical analyses were conducted with STATA 14.1 (StataCorp, College Station, Texas).
Quality assessment
The strength of evidence for each outcome was evaluated by two independent assessors (V.M.L. and A.G.) using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach and presented as a summary of findings table to identify the certainty of all pooled outcomes [21]. Each study was then assessed against the Newcastle–Ottawa Scale (NOS) [22] which accounted for criteria such as selection, comparability, and outcome to evaluate the quality of its design.
Bias assessment
Publication and small-study biases were assessed through the generation of a funnel plot and assessed for asymmetry. Egger’s linear regression test and Begg’s correlation test were used to investigate suspect asymmetry for small-study bias [23, 24]. Sensitivity analysis by exclusion was performed for all outcomes to evaluate the risk of single-study bias. Finally, a trim-and-fill approach was used to recalculate pooled effect size if any bias was suspected [25].
Results
Search strategy
The search strategy identified 1210 articles for evaluation (Fig. 1). Removal of 321 duplicates resulted in title and abstract screening of 889 articles, which yielded 48 articles for full-text evaluation. The full-text of these were then assessed against the selection criteria, which identified 8 single-institution retrospective observational cohort studies [16, 26,27,28,29,30,31,32] for inclusion into this systematic review and meta-analysis (Table 1). Of these 8 studies, Schapira et al. [32] described outcomes for NSCLC metastases only and Chen et al. [16] described outcomes for a combination of NSCLC, melanoma and RCC metastases—these 2 studies were allocated to the Mixed subgroup for secondary analysis. The remaining 6 studies [26,27,28,29,30,31] described melanoma metastases only, and were allocated to the Melanoma subgroup for secondary analysis.

Results of the preferred reporting items for systematic reviews and meta-analyses (PRISMA) search strategy
Of the excluded 40 studies, the three studies require mentioning: Ahmed et al. [33] did not quantify OS proportion of their cohorts; An et al. [34] evaluated early ICI with the definition of ≤ 5.5 months of SRS management which was too broad for our purposes; and quantitative data by Skrepnik et al. [35] could not be clarified.
Demographics and clinical features
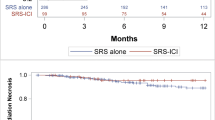
The pooled cohort included 408 MBD patients with 105/408 (26%) female, an average age of 60.8 years, and median of 2 metastases treated (Table 1). There were 181 (44%) patients who received ICI concurrent with their SRS management (67 within 2 weeks, 114 within 4 weeks), and 227 (56%) patients who received ICI either before or after their SRS management (Table 2). The most common metastatic primary and ICI agent reported was melanoma and ipilimumab (3 mg/kg for 4 doses) respectively. SRS was most commonly dosed at 20 Gy in a single fraction. Concurrent ICI was considered to be within 2 weeks of SRS in 3 studies [16, 26, 29], and the remaining 5 studies [27, 28, 30,31,32] a period of 4 weeks was used as the definition.
Overall survival
The median Kaplan Meier estimates for 12-month OS were 62% in the concurrent group and 50% in the non-concurrent group when all study data was pooled (Table 2). Overall, in the pooled cohort of all 8 studies, the 12-month OS was better in the concurrent ICI group, and this was statistically significant (OR = 1.74; 95% CI 1.13–2.69; I2 = 0.0%; p = 0.011, Fig. 2a). Meta-regression of study covariates did not detect any significant modifying trend on the observed pooled outcome (Supplementary).

Forest plots of the odd ratios (ORs) derived from Kaplan–Meier estimates and their corresponding 95% confidence intervals (95% CIs) of all studies investigating concurrent vs non-concurrent immune checkpoint inhibition (ICI) in metastatic brain disease (MBD) for outcomes (a) 12-month overall survival (OS), (b) 12-month local progression free survival (LPFS) and (c) 12-month distant progression free survival. The summary statistic, the 95% CI, and the relative weightings are represented by the middle of the square, the horizontal line, and the relative size of the square respectively. The heterogeneity and its significance of included studies is provided as an overall statistic for each plot
Furthermore, in the Mixed subgroup (n = 2), the trend and significance were maintained (OR = 2.71; 95% CI 1.06–6.91; I2 = 0.0%; p = 0.037), whereas in the Melanoma subgroup (n = 6), the trend was maintained, however significance was not (OR = 1.55; 95% CI 0.95–2.52; I2 = 0.0%; p = 0.070).
Local progression free survival
The median Kaplan Meier estimates for LPFS were 88% vs. 77% for concurrent vs non-concurrent cohorts respectively (Table 2). Overall, in a pooled cohort of 5 studies, superior 12-month LPFS trended in favor of concurrent ICI, however this was not statistically significant (OR = 2.09; 95% CI 0.76–5.73; I2 = 40.8%; p = 0.154) as shown in Fig. 2b. Meta-regression of study covariates did not detect any significant modifying trend on the observed pooled outcome (Supplementary).
In the Melanoma subgroup (n = 3), the trend and lack of significance were maintained (OR = 2.14; 95% CI 0.37–12.45; I2 = 67.1%; p = 0.399), and in the Mixed subgroup (n = 2), a similar result was obtained (OR = 2.30; 95% CI 0.69–7.72; I2 = 0.0%; p = 0.177).
Distal progression free survival
The median Kaplan Meier estimates for DPFS were 32.5% vs. 55.5% for concurrent vs non-concurrent cohorts respectively (Table 2). Overall, in a pooled cohort of 4 studies, superior 12-month DPFS trended in favor of non-concurrent ICI, however this was not statistically significant (OR = 0.88; 95% CI 0.23–3.29; I2 = 64.1%; p = 0.839) as shown in Fig. 2c. Meta-regression of study covariates identified study year (slope = 0.16; p = 0.039) as a covariate that exerted significant effect on overall trend (Supplementary). As slope < 1, it implied that newer studies were less likely to favor concurrent ICI compared to older studies. All other covariates did not significant modify the overall trend.
In the Melanoma subgroup (n = 3), the lack of significance was maintained, however, the trend was reversed in favor of concurrent ICI (OR = 1.34; 95% CI 0.27–6.69; I2 = 67.5%; p = 0.723). The resulting trend mirrored the overall one in the Mixed subgroup (n = 1) in term so trend favoring non-concurrent ICI (OR = 0.25; 95% CI 0.05–1.53; I2 = NA; p = 0.09).
Quality assessment
The certainty of effect estimates for pooled outcomes were evaluated by GRADE assessment. The certainty of the 12-month OS outcome was deemed to be low (+ 2), and very low for 12-month LPFS (+ 1), and 12-month DPFS (0) (Table 3). According to the NOS criteria, all included studies were of good quality with a median score of 8 (Supplementary).
Bias assessment
Funnel plots were generated for each outcome described to assess for publication bias via asymmetry (Supplementary). Asymmetry and bias was suspected in the 12-month OS outcome, despite negative results of Egger’s (p = 0.217) and Begg’s (p = 0.266) tests, as well as a negative sensitivity analysis for single-study bias. A trim-and-fill analysis by RE modelling was performed to validate this concern, which resulted in 2 filled studies (Supplementary), however both trend and significance were maintained in favor of concurrent ICI (OR = 1.56; 95% CI 1.04–2.34; p = 0.030; n = 10). In the Melanoma subgroup (n = 6), sensitivity analysis detected one study [36] upon exclusion which resulted in a significant 12-month OS trend. Yet, trim-and-fill analysis resulted in 1 filled study, and maintained the lack of significance in the trend favoring concurrent ICI (OR = 1.40; 95% CI 0.88–2.24; p = 0.153; n = 7).
The funnel plot for 12-month LPFS outcome (n = 5) was suspected of asymmetry despite negative Egger’s test (p = 0.348) and Begg’s test (p = 0.308) results. Sensitivity analysis by leave-one-out approach identified one study [36] which upon its individual exclusion, significance of the pooled trend was achieved. However, trim-and-fill analysis was negative. The symmetry of the funnel plot for 12-month DPFS (n = 4) was unclear, with Egger’s test (p = 0.201) and Begg’s test (p = 0.308) non-significant. However, sensitivity analysis did not identify any outlying studies to affect significance, and trim-and-fill analysis was negative.
Discussion
The aim of this SRMA was to determine if the timing of ICI relative to SRS has the potential to influence survival metrics in MBD patients. Based on the current literature, pooled analysis indicates that, compared to non-concurrent ICI, concurrent ICI results in significantly better 12-month OS (OR = 1.75; p = 0.011), and comparable 12-month LPFS (OR = 2.09; p = 0.154) and DPFS (OR = 0.88; p = 0.839) outcomes. The trend and significance of the LPFS finding was reflected in the Melanoma subgroup. However bias assessment identified a number of concerns in current studies which limits the certainty of these results.
To date, the largest study reporting concurrent ICI with SRS outcomes is by Chen et al. [16], who investigated outcomes of 79 NSCLC, melanoma and RCC MBD patients managed by ICI. They found with multivariate Cox regression modelling that concurrent ICI conferred a significant OS benefit for MBD, compared to non-concurrent ICI (HR = 2.69; p < 0.01), and SRS alone (HR = 2.69; p < 0.01). This conclusion aligns with the overall finding of this study. Despite this finding, we did not observe corresponding significant trends with respect either LPFS or DPFS. The leading view on this finding is that concurrent ICI with SRS affords greater systemic, extracranial control of MBD, rather than superior intracranial control [31, 36]. Additionally, it may be possible that the number of metastases present at treatment can dictate the propensity for progression independent to that of OS [16]. There is need for enhanced clinical course reporting to assist in clarifying this further in the future.
From the analysis by Chen et al. [16], melanoma histology was identified to significantly correlate with worse OS outcome compared to NSCLC and RCC (p = 0.043). A large portion of the current literature in fact focuses on melanoma outcomes specifically, with the most recent study by Rahman et al. [31] the largest to date. Their conclusions were slightly more tempered however, with OS survival not significantly different between concurrent vs noncurrent ICI (p > 0.05), despite median OS being 17.8 vs. 11.6 months respectively. This correlates with the non-significant trend in 12-month OS in favor of concurrent ICI seen in our melanoma subgroup. Of clinical interest, is that with regards to DPFS, the melanoma subgroup trended in favor of concurrent ICI (OR = 1.34, > 1; n = 3), compared to the other subgroup which favored non-concurrent ICI (OR = 0.25, < 1; n = 1)—the possibility that melanoma achieves better DPFS with different ICI timing compared to other MBD histology is a novel concept, potentially related to superior biological abscopal effect which has been postulated [37], however this remains speculative at best until more studies are published given it is extremely underreported. Nonetheless, it is plausible that MBD histology may be a delineating factor when evaluating optimal time frame for defining concurrent administration of ICI with SRS.
There is evidence that demonstrates melanoma histology carries worse OS and PFS prognosis in MBD patients managed by SRS when compared to other histologies [38,39,40]. It is highly possible then that the addition of ICI to treatment does not change this [16]. The lack of 12-month OS significance with concurrent ICI in the Melanoma subgroup (p = 0.070) compared to the significance in the Mixed subgroup (p = 0.037) would support this notion. We attempted to investigate the effect of histology by means of meta-regression, and although the results were negative for trend modifying effect across all outcomes, we acknowledge that the analysis was most likely underpowered due to low study numbers, and lack of non-melanoma cohorts for control. Should a difference between MBD histology be validated in the future, it may necessitate different inclusion criteria for concurrent ICI with SRS based on histology.
Another potential delineation factor for concurrent ICI is the agent of choice. To date there remains a paucity of data directly comparing different ICI agents administered concurrently in MBD. Chen et al. [16] reported that anti-PD-1 inhibition resulted in a significantly superior OS compared to anti-CTLA-4 inhibition based on their multivariate Cox regression (HR = 0.24; p < 0.01). However, this was not taking into consideration the timing of ICI with respect to SRS, nor was there any separation of this outcome based on MBD histology. Pasquali et al. [41] calculated a similar significant trend favoring anti-PD-1 over anti-CTLA-4 inhibition with respect to PFS in metatastic melanoma, however this was not delineated by timing either. We note that our meta-regression did not detect trend modifying effect by ICI choice reported by each study for all outcomes, however this is compromised by the fact studies were designated as either ‘ipilimumab only’ or ‘mixed ICI’ studies, wherein the latter group involved other ICI agents as well as ipilimumab.
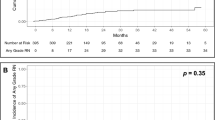
Whether concurrent ICI alters the risk of immune- or SRS-related complications after SRS in the treatment of MBD compared to non-concurrent ICI is currently underreported. The acceptable safety profile of ICI for MBD with SRS is discussed elsewhere in the literature [10,11,12], but whether or not concurrent ICI modulates this profile is unclear. Chen et al. [16] observed comparable incidence rates of immune-related adverse events between their concurrent vs non-concurrent cohorts (32% vs 30%). With respect to SRS-related complications, Diao et al. [36] reported radionecrosis (RN) incidences of 2/23 (9%) and 2/28 (7%) in their concurrent and non-concurrent ipilimumab cohorts with SRS for melanoma MBD respectively, with an overall median time to event of 6.6 months after SRS. Rahman et al. [31] delineated further, noting that between concurrent and non-concurrent ICI cohorts, rates of symptomatic RN were 4/35 (11%) vs. 5/39 (13%) respectively, and rates of pathological RN were 1/35 (3%) and 2/39 (5%) respectively. This anecdotal evidence would appear to advocate for the negligible modification to RN risk with concurrent ICI vs non-concurrent, however additional studies will be helpful in this regard.
Strengths and limitations
This SRMA adhered strictly to PRISMA guidelines and its selection criteria. We obtained ORs for survival metrics based on presented data in individual studies modelled by Kaplan–Meier estimation. The strength of this approach is that it accounts for potential loss by 12-month follow-up via censoring, to provide more consistent, comparable metrics across studies [42]. Finally, in all analyses, a random-effect (RE) model was tested in an attempt to minimize statistical interference by the possible clinical diversity and methodological variation between studies, as it assumes unequal variance between studies and distributes statistical weighting more conservatively [43]. This includes the use of various systemic therapies used prior/concurrently with the SRS and ICI combination, as well as the unique disease biology of different histology types, duration of follow-up, use of different ICI agents, baseline differences, and disease burden at presentation, all of which would be better accounted for by prospective study [16, 27, 31].
We applied a strict definition of ≤ 4 weeks within SRS for ‘concurrent’, which did exclude one study [34]. Although yet to be completely elucidated, it has been suggested that an optimal window within which ICI can be added to SRS exists, possibly within 6–15 days of SRS for ipilimumab [35]. This is based on the upregulation of SRS-induced cell death mechanisms within 7 days, and the half-life of ipilimumab being 14.9 days [44, 45]. Current studies are limited by their retrospective nature in this regard, which limits the scope for investigation of when exactly an OS ‘advantage’ of concurrent ICI diminishes in BM managing. In other words, after SRS, there may be a therapeutic window by which administration ICI has optimal effect. This may or may not be within 4 weeks, as An et al. [34] observed significant LPFS benefit of concurrent ICI within 5.5 months of SRS compared to outside that time period. Evaluation of this therapeutic window will prove clinically useful in the future, as it may widen the utility of ICI in the management of prolonged, complex MBD cases.
The number of studies in the literature is small. This is not particularly surprising given the novel nature of this topic, however limits the certainty by which we can advocate our findings due to the potential for underpowered analysis, as well as over-weighted, outlying studies. For example, our DPFS outcome appears to be affected by year of publication (slope = 0.16; p = 0.039), yet with n = 4 studies, it cannot be claimed that this trend is in fact clinically relevant until more studies are published.
Of particular note is the study by Diao et al. [27], whose exclusion in both 12-month OS and LPFS resulted in statistical significance in favor of concurrent ICI in the Melanoma subgroup, which was not the case with its inclusion. They noted that more frequent prior chemotherapy and higher doses of ipilimumab in the non-concurrent ICI cohort may have contributed to their inconsistent findings with the rest of the literature. This highlights that while it is attractive to assume concurrent ICI affords greater survival outcome benefits in theory, we must be wary that this does not guarantee effective translation into clinical practice.
Furthermore, potential selection bias cannot be controlled for in non-randomized studies. For example, patients into the non-concurrent ICI cohorts may have been recruited after insufficient outcomes following SRS were observed, predisposing these cases to poorer survival outcomes. Additionally, it is unclear if non-concurrent ICI administration before vs. after the SRS window may affect survival outcomes differently. Schapira et al. [32] reported that non-concurrent nivolumab/pembrolizumab before SRS trended towards superior OS and DPFS in NSCLC MBD compared to non-concurrent inhibition after SRS. Kiess et al. [28] reported a similar trend in their cohort of melanoma BM with ipilimumab. Greater factorial control by larger, randomized studies will assist in overcoming these limitations in the future.
Conclusion
It appears that ICI administration within 4 weeks of SRS for MBD confers a statistically significant superior 12-month OS when compared to administration outside that time period. However, the biological heterogeneity of MBD and ICI, and small number of retrospective clinical studies to date, limits the certainty of these results. The results of this systematic review and meta-analysis illustrate that it is conceivable there exists an optimal therapeutic window for ICI in MBD management to yield greatest OS, LPFS and DPFS benefit; when that is, and by what sequence, requires intensive delineation based on clinical parameters in future studies.
References
Cagney DN, Martin AM, Catalano PJ, Redig AJ, Lin NU, Lee EQ, Wen PY, Dunn IF, Bi WL, Weiss SE, Haas-Kogan DA, Alexander BM, Aizer AA (2017) Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: a population-based study. Neuro Oncol 19(11):1511–1521. https://doi.org/10.1093/neuonc/nox077
Barnholtz-Sloan JS, Sloan AE, Davis FG, Vigneau FD, Lai P, Sawaya RE (2004) Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol 22(14):2865–2872. https://doi.org/10.1200/jco.2004.12.149
Sampson JH, Carter JH Jr, Friedman AH, Seigler HF (1998) Demographics, prognosis, and therapy in 702 patients with brain metastases from malignant melanoma. J Neurosurg 88(1):11–20. https://doi.org/10.3171/jns.1998.88.1.0011
Staudt M, Lasithiotakis K, Leiter U, Meier F, Eigentler T, Bamberg M, Tatagiba M, Brossart P, Garbe C (2010) Determinants of survival in patients with brain metastases from cutaneous melanoma. Br J Cancer 102(8):1213–1218. https://doi.org/10.1038/sj.bjc.6605622
Larkin J, Hodi FS, Wolchok JD (2015) Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med 373(13):1270–1271. https://doi.org/10.1056/NEJMc1509660
Robert C, Schachter J, Long GV, Arance A, Grob JJ, Mortier L, Daud A, Carlino MS, McNeil C, Lotem M, Larkin J, Lorigan P, Neyns B, Blank CU, Hamid O, Mateus C, Shapira-Frommer R, Kosh M, Zhou H, Ibrahim N, Ebbinghaus S, Ribas A (2015) Pembrolizumab versus Ipilimumab in advanced melanoma. N Engl J Med 372(26):2521–2532. https://doi.org/10.1056/NEJMoa1503093
Gettinger S, Rizvi NA, Chow LQ, Borghaei H, Brahmer J, Ready N, Gerber DE, Shepherd FA, Antonia S, Goldman JW, Juergens RA, Laurie SA, Nathan FE, Shen Y, Harbison CT, Hellmann MD (2016) Nivolumab monotherapy for first-line treatment of advanced non-small-cell lung cancer. J Clin Oncol 34(25):2980–2987. https://doi.org/10.1200/jco.2016.66.9929
McDermott DF, Drake CG, Sznol M, Choueiri TK, Powderly JD, Smith DC, Brahmer JR, Carvajal RD, Hammers HJ, Puzanov I, Hodi FS, Kluger HM, Topalian SL, Pardoll DM, Wigginton JM, Kollia GD, Gupta A, McDonald D, Sankar V, Sosman JA, Atkins MB (2015) Survival, durable response, and long-term safety in patients with previously treated advanced renal cell carcinoma receiving Nivolumab. J Clin Oncol 33(18):2013–2020. https://doi.org/10.1200/jco.2014.58.1041
Ahmed KA, Abuodeh YA, Echevarria MI, Arrington JA, Stallworth DG, Hogue C, Naghavi AO, Kim S, Kim Y, Patel BG, Sarangkasiri S, Johnstone PAS, Sahebjam S, Khushalani NI, Forsyth PA, Harrison LB, Yu M, Etame AB, Caudell JJ (2016) Clinical outcomes of melanoma brain metastases treated with stereotactic radiosurgery and anti-PD-1 therapy, anti-CTLA-4 therapy, BRAF/MEK inhibitors, BRAF inhibitor, or conventional chemotherapy. Ann Oncol 27(12):2288–2294. https://doi.org/10.1093/annonc/mdw417
Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel JC, Akerley W, van den Eertwegh AJ, Lutzky J, Lorigan P, Vaubel JM, Linette GP, Hogg D, Ottensmeier CH, Lebbe C, Peschel C, Quirt I, Clark JI, Wolchok JD, Weber JS, Tian J, Yellin MJ, Nichol GM, Hoos A, Urba WJ (2010) Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med 363(8):711–723. https://doi.org/10.1056/NEJMoa1003466
Long GV, Atkinson V, Lo S, Sandhu S, Guminski AD, Brown MP, Wilmott JS, Edwards J, Gonzalez M, Scolyer RA, Menzies AM, McArthur GA (2018) Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: a multicentre randomised phase 2 study. Lancet Oncol 19(5):672–681. https://doi.org/10.1016/s1470-2045(18)30139-6
Gauvain C, Vauleon E, Chouaid C, Lerhun E, Jabot L, Scherpereel A, Vinas F, Cortot AB, Monnet I (2018) Intracerebral efficacy and tolerance of nivolumab in non-small-cell lung cancer patients with brain metastases. Lung Cancer 116:62–66. https://doi.org/10.1016/j.lungcan.2017.12.008
Gaudy-Marqueste C, Dussouil AS, Carron R, Troin L, Malissen N, Loundou A, Monestier S, Mallet S, Richard MA, Regis JM, Grob JJ (2017) Survival of melanoma patients treated with targeted therapy and immunotherapy after systematic upfront control of brain metastases by radiosurgery. Eur J Cancer 84:44–54. https://doi.org/10.1016/j.ejca.2017.07.017
Knisely JP, Yu JB, Flanigan J, Sznol M, Kluger HM, Chiang VL (2012) Radiosurgery for melanoma brain metastases in the ipilimumab era and the possibility of longer survival. J Neurosurg 117(2):227–233. https://doi.org/10.3171/2012.5.JNS111929
Mathew M, Tam M, Ott PA, Pavlick AC, Rush SC, Donahue BR, Golfinos JG, Parker EC, Huang PP, Narayana A (2013) Ipilimumab in melanoma with limited brain metastases treated with stereotactic radiosurgery. Melanoma Res 23(3):191–195. https://doi.org/10.1097/CMR.0b013e32835f3d90
Chen L, Douglass J, Kleinberg L, Ye X, Marciscano AE, Forde PM, Brahmer J, Lipson E, Sharfman W, Hammers H, Naidoo J, Bettegowda C, Lim M, Redmond KJ (2018) Concurrent immune checkpoint inhibitors and stereotactic radiosurgery for brain metastases in non-small cell lung cancer, melanoma, and renal cell carcinoma. Int J Radiat Oncol Biol Phys 100(4):916–925. https://doi.org/10.1016/j.ijrobp.2017.11.041
Mole RH (1953) Whole body irradiation; radiobiology or medicine? Br J Radiol 26(305):234–241. https://doi.org/10.1259/0007-1285-26-305-234
Ngwa W, Irabor OC, Schoenfeld JD, Hesser J, Demaria S, Formenti SC (2018) Using immunotherapy to boost the abscopal effect. Nat Rev Cancer 18:313. https://doi.org/10.1038/nrc.2018.6
Moher D, Liberati A, Tetzlaff J, Althman D (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. PLoS Med 6(7):e1000097
Higgins JPT, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327(7414):557–560
Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, Guyatt GH, Harbour RT, Haugh MC, Henry D, Hill S, Jaeschke R, Leng G, Liberati A, Magrini N, Mason J, Middleton P, Mrukowicz J, O’Connell D, Oxman AD, Phillips B, Schunemann HJ, Edejer T, Varonen H, Vist GE, Williams JW Jr, Zaza S (2004) Grading quality of evidence and strength of recommendations. BMJ 328(7454):1490. https://doi.org/10.1136/bmj.328.7454.1490
Wells G, Shea B, O’connell D, Peterson J, Welch V, Losos M, Tugwell P (2016) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hospital Research Institute, Ottawa
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315(7109):629–634
Begg CB, Mazumdar M (1994) Operating characteristics of a rank correlation test for publication bias. Biometrics 50(4):1088–1101
Duval S, Tweedie R (2000) Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 56(2):455–463
Cohen-Inbar O, Shih HH, Xu Z, Schlesinger D, Sheehan JP (2017) The effect of timing of stereotactic radiosurgery treatment of melanoma brain metastases treated with ipilimumab. J Neurosurg 127(5):1007–1014. https://doi.org/10.3171/2016.9.JNS161585
Diao K, Bian SX, Routman DM, Yu C, Kim PE, Wagle NA, Wong MK, Zada G, Chang EL (2018) Combination ipilimumab and radiosurgery for brain metastases: tumor, edema, and adverse radiation effects. J Neurosurg. https://doi.org/10.3171/2017.7.jns171286
Kiess AP, Wolchok JD, Barker CA, Postow MA, Tabar V, Huse JT, Chan TA, Yamada Y, Beal K (2015) Stereotactic radiosurgery for melanoma brain metastases in patients receiving ipilimumab: safety profile and efficacy of combined treatment. Int J Radiat Oncol Biol Phys 92(2):368–375. https://doi.org/10.1016/j.ijrobp.2015.01.004
Patel KR, Shoukat S, Oliver DE, Chowdhary M, Rizzo M, Lawson DH, Khosa F, Liu Y, Khan MK (2017) Ipilimumab and STEREOTACTIC RADIOSURGERY VERSUS STEREOTACTIC RADIOSURGERY ALONE FOR NEWLY DIAGNOSED MELANOMA BRAIN METASTASES. Am J Clin Oncol Cancer Clin Trials 40(5):444–450. https://doi.org/10.1097/COC.0000000000000199
Qian JM, Yu JB, Kluger HM, Chiang VL (2016) Timing and type of immune checkpoint therapy affect the early radiographic response of melanoma brain metastases to stereotactic radiosurgery. Cancer 122(19):3051–3058. https://doi.org/10.1002/cncr.30138
Rahman R, Cortes A, Niemierko A, Oh KS, Flaherty KT, Lawrence DP, Sullivan RJ, Shih HA (2018) The impact of timing of immunotherapy with cranial irradiation in melanoma patients with brain metastases: intracranial progression, survival and toxicity. J Neuro-Oncol. https://doi.org/10.1007/s11060-018-2795-7
Schapira E, Hubbeling H, Yeap BY, Mehan WA Jr, Shaw AT, Oh K, Gainor JF, Shih HA (2018) Improved Overall Survival and Locoregional Disease Control With Concurrent PD-1 Pathway Inhibitors and Stereotactic Radiosurgery for Lung Cancer Patients With Brain Metastases. Int J Radiat Oncol Biol Phys. https://doi.org/10.1016/j.ijrobp.2018.02.175
Ahmed KA, Kim S, Arrington J, Naghavi AO, Dilling TJ, Creelan BC, Antonia SJ, Caudell JJ, Harrison LB, Sahebjam S, Gray JE, Etame AB, Johnstone PA, Yu M, Perez BA (2017) Outcomes targeting the PD-1/PD-L1 axis in conjunction with stereotactic radiation for patients with non-small cell lung cancer brain metastases. J Neuro Oncol 133(2):331–338. https://doi.org/10.1007/s11060-017-2437-5
An Y, Jiang W, Kim BYS, Qian JM, Tang C, Fang P, Logan J, D’Souza NM, Haydu LE, Wang XA, Hess KR, Kluger H, Glitza IC, Mahajan A, Welsh JW, Lin SH, Yu JB, Davies MA, Hwu P, Sulman EP, Brown PD, Chiang VLS, Li J (2017) Stereotactic radiosurgery of early melanoma brain metastases after initiation of anti-CTLA-4 treatment is associated with improved intracranial control. Radiother Oncol 125(1):80–88. https://doi.org/10.1016/j.radonc.2017.08.009
Skrepnik T, Sundararajan S, Cui H, Stea B (2017) Improved time to disease progression in the brain in patients with melanoma brain metastases treated with concurrent delivery of radiosurgery and ipilimumab. OncoImmunology. https://doi.org/10.1080/2162402X.2017.1283461
Diao K, Bian SX, Routman DM, Yu C, Ye JC, Wagle NA, Wong MK, Zada G, Chang EL (2018) Stereotactic radiosurgery and ipilimumab for patients with melanoma brain metastases: clinical outcomes and toxicity. J Neuro Oncol. https://doi.org/10.1007/s11060-018-2880-y
Ribeiro Gomes J, Schmerling RA, Haddad CK, Racy DJ, Ferrigno R, Gil E, Zanuncio P, Buzaid AC (2016) Analysis of the abscopal effect with anti-PD1 therapy in patients with metastatic solid tumors. J Immunother 39(9):367–372. https://doi.org/10.1097/cji.0000000000000141
Sia J, Paul E, Dally M, Ruben J (2015) Stereotactic radiosurgery for 318 brain metastases in a single Australian centre: the impact of histology and other factors. J Clin Neurosci 22(2):303–307. https://doi.org/10.1016/j.jocn.2014.07.019
Caballero JA, Sneed PK, Lamborn KR, Ma L, Denduluri S, Nakamura JL, Barani IJ, McDermott MW (2012) Prognostic factors for survival in patients treated with stereotactic radiosurgery for recurrent brain metastases after prior whole brain radiotherapy. Int J Radiat Oncol Biol Phys 83(1):303–309. https://doi.org/10.1016/j.ijrobp.2011.06.1987
Sperduto PW, Kased N, Roberge D, Xu Z, Shanley R, Luo X, Sneed PK, Chao ST, Weil RJ, Suh J, Bhatt A, Jensen AW, Brown PD, Shih HA, Kirkpatrick J, Gaspar LE, Fiveash JB, Chiang V, Knisely JP, Sperduto CM, Lin N, Mehta M (2012) Summary report on the graded prognostic assessment: an accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol 30(4):419–425. https://doi.org/10.1200/jco.2011.38.0527
Pasquali S, Chiarion-Sileni V, Rossi CR, Mocellin S (2017) Immune checkpoint inhibitors and targeted therapies for metastatic melanoma: a network meta-analysis. Cancer Treat Rev 54:34–42. https://doi.org/10.1016/j.ctrv.2017.01.006
Rich JT, Neely JG, Paniello RC, Voelker CC, Nussenbaum B, Wang EW (2010) A practical guide to understanding Kaplan-Meier curves. Otolaryngol Head Neck Surg 143(3):331–336. https://doi.org/10.1016/j.otohns.2010.05.007
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Controlled Clinical Trials 7(3):177–188
Kim S, Ramakrishnan R, Lavilla-Alonso S, Chinnaiyan P, Rao N, Fowler E, Heine J, Gabrilovich DI (2014) Radiation-induced autophagy potentiates immunotherapy of cancer via up-regulation of mannose 6-phosphate receptor on tumor cells in mice. Cancer Immunol Immunother 63(10):1009–1021. https://doi.org/10.1007/s00262-014-1573-4
Weber JS, O’Day S, Urba W, Powderly J, Nichol G, Yellin M, Snively J, Hersh E (2008) Phase I/II study of ipilimumab for patients with metastatic melanoma. J Clin Oncol 26(36):5950–5956. https://doi.org/10.1200/jco.2008.16.1927
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no funding sources or conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lu, V.M., Goyal, A., Rovin, R.A. et al. Concurrent versus non-concurrent immune checkpoint inhibition with stereotactic radiosurgery for metastatic brain disease: a systematic review and meta-analysis. J Neurooncol 141, 1–12 (2019). https://doi.org/10.1007/s11060-018-03020-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-018-03020-y