
Abstract
In this study, we aim to determine the relationship between methylation level of an inflammatory-related gene, SOCS-1 in serum samples of patients with ankylosing spondylitis (AS) and their degree of inflammation as well as serum cytokine level. Quantitative real time methylation specific PCR was performed to examine the promoter methylation of SOCS-1 in serum samples of 43 HLA-B27+ AS patients and 6 B27+ healthy controls. Degree of inflammation was accessed by spondylopathy, sacroiliitis as well as acute phase reactant, erythrocyte sedimentation rate and C-reactive protein (CRP). Serum IL-6 and TNF-α level was determined by ELISA assay. SOCS-1 methylation can only be found in serums samples from patients but not normal control. Methylation of SOCS-1 significantly associated with severity of patient’s spondylopathy (P < 0.005), sacroiliitis (P < 0.005) and acute phase reactant CRP (P = 0.0278). AS patients also exhibited higher serum IL-6 (P < 0.001) and TNF-α level (P < 0.001). Importantly, patients with high serum IL-6 or TNF-α level demonstrated a significantly higher SOCS-1 methylation (P < 0.001). In conclusion, this proof-of-principle study suggested that methylation of SOCS-1 can be detected in serum of HLA-B27+ AS patients but not in B27+ controls. The pathogenic potential of SOCS-1 methylation in AS deserves further investigation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ankylosing spondylitis (AS) is a chronic systemic inflammatory disorder that causes axial bony ankylosis, enthesopathy and peripheral arthritis [1, 2]. The class I major histocompatibility complex (MHC) gene HLA-B27 is strongly associated with this disease [3]. More than 90 % of the AS patients are HLA-B27 positive, yet around 1–2 % of the B27 carriers will develop this disease. This observation suggests that factors other than HLA-B27 may be responsible for the development of AS [4].
Several reports demonstrated that increased expression of several cytokines such as IL-6 and TNF-α are observed in AS patients thus suggesting that activation of these signaling pathways may be crucial in the activation of AS [5–8]. Studies including ours have demonstrated that aberrant activation of these signaling pathways can induce epigenetic alterations of its downstream target in several human diseases [9–11]. However, the role of epigenetic alterations in AS have never been explored.
Epigenetic modifications such as DNA methylation play a crucial role in controlling gene expression in the genome [12]. DNA methylation which takes place at the 5′ position of cytosine of a CpG dinucleotide with the formation of 5-methylcytosine is a well-recognized epigenetic modification resulting in gene silencing [13]. Moreover, aberrant gene promoter hypermethylation resulting in gene inactivation has been linked to a number of human diseases [14, 15]. We along with the others have previously demonstrated aberrant DNA hypermethylation of multiple tumor suppressor genes in several human cancer [16–18]. This aberrant DNA methylation in the form of free circulating DNA can also be readily detected in serum samples of cancer patients in which increased apoptotic or necrotic tumor cells are observed [19–21]. Given such aberrant DNA hypermethylation plays an important role in human disease, it is of interest to examine if such aberrant DNA methylation also plays a role in AS.
In this study, we examined promoter methylation of the STAT3 target gene, SOCS-1 in serum samples of AS patients. Our result showed that methylation of SOCS-1 is associated with disease progression as well as cytokine expression. This proof-of-principle study suggests that epigenetic alteration may play a role in the pathogenesis of AS.
Materials and methods
Patient samples
Forty-three HLA-B27 positive AS patients and six B27 positive healthy controls were included in the study. The clinical-pathological data of these 43 AS patients is summarized in Table 1. Patients were evaluated and diagnosed according to the modified New York criteria. Serum samples were obtained by the standard methods from peripheral venous blood samples. Radiographs of sacroiliac joint and T-L (thoracolumbar) spine were examined independently by two radiologists blinded to patient identification. The sacroiliac grade of joints was determined as followed: grade I: cortex erosion with subchondral sclerosis; grade II: pseudowidening; grade III: fibrosis, calcification and interosseous bridging; grade IV: complete bony ankylosis of sacroiliac joint. T and L-spine lesion grade were determined as followed: grade I: osteitis of vertebral corner; grade II: cortex erosion with squareal vertebral body; grade III; bony bridges between vertebral body; grade IV: total ossification with bamboo spine. Patients were well explained and informed consents were obtained before the study. All human experiments conducted were in accordance with the ethical standards of the Institution Review Board (IRB) at Buddhist Dalin Tzu Chi General Hospital and with the Helsinki Declaration of 1975, as revised in 2000.
DNA extraction and bisulphite modification
DNA was extracted from 0.5 ml of serum samples by the QIAamp DNA blood mini kit (Qiagen, Valenica, CA) and bisulphite-modified using the EZ DNA methylation Kit (Zymo research, Orange, CA) which converts all genomic DNA with unmethylated cytosine into uracil, whereas methylated cytosine remains unaltered. These differential changes in nucleotide sequences enable the use of PCR-based methods to detect gene promoter methylation [22]. In brief, genomic DNA was denatured by sodium hydroxide and then chemically modified by sodium bisulfite for 16 h. Modified DNA was resuspended in 50 μl of TE buffer (10 mM Tris, 1 mM EDTA pH 7.5) [20].
Methylation detection of serum SOCS-1
To quantify the methylation of SOCS-1 gene in serum samples, bisulphite-modified DNA was subjected to real time quantitative methylation specific PCR with Taqman technology in ABI Stepone real time PCR system as previously described [20, 23]. The primers and probe sequences were listed in Table 2. Each reaction contained 12.5 μl universal PCR master mix (without UNG), 1.5 μl of 10 μM forward and reverse primers, and 4 μl of DNA template in a total volume of 25 μl. The amount of methylated DNA was determined by the threshold cycle number (Ct) for each sample against a standard curve generated by SssI-treated DNA (Chemicon, Temecula, CA, USA) and expressed as the amount of methylated DNA/0.5 ml of serum.
Bisulphite pyrosequencing
Bisulphite-modified DNA was subjected to PCR amplification strategy using a tailed reverse primer in combination with a biotin-labeled universal primer as described [24]. PCR and sequencing primers were designed using PyroMark Assay Design 2.0 (Qiagen GmbH, Hilden, Germany). SOCS-1 promoter (+690 to +954) was PCR-amplified in a 25 μl reaction containing 12.5 μl of 2× RBC Sensizyme Hotstart Taq premix (RBC Bioscience, Taiwan) 0.5 μM of each primer and 6.8 μl (around 35 ng) of bisulphite-modified DNA for 95 °C for 5 min followed by 50 cycles of 95 °C for 30 s, 62 °C for 1 min, and 72 °C for 45 s and a final extension at 72 °C for 7 min. 1.5 μl of each PCR reaction were analysed on a 1 % agarose gel before pyrosequencing. Pyrosequencing was performed on the PyroMark Q24 (Qiagen) using the Pyro Gold Reagents (Qiagen) according to the manufacturer’s protocol. The methylation level of eleven CpG sites from +884 to +935 with respective to transcriptional start site (TSS) was measured. The methylation percentage of each cytosine was determined by the light intensity of cytosines divided by the sum of light intensity of cytosines and thymines at each CpG site. In-vitro methylated DNA (Millipore) was included as positive control for pyrosequencing. All primer sequences were listed in Table 2.
Serum level of IL-6 and TNF-α
Serum level of IL-6 and TNF-α were measured with sensitive ELISA Quantikine HS Immunoassay Kits (R&D Systems, Minneapolis, MN) in accordance with the manufacturer’s instructions. Briefly, 100 μl (IL-6) or 200 μl (TNF-α) of serum samples were incubated with specific antibody for 2 h (IL-6) or 3 h (TNF-α) at room temperature. After several wash steps, the plates were incubated with secondary antibody for 2 h at room temperature. The plates were finally incubated with 50 μl of amplifier solution and incubated for 30 min at room temperature. The cytokine level was assessed by using a MRXII 96-well ELISA plate reader (Dynex Technologies, Chantilly, Virginia) at 490 nm.
Statistical analysis
Mann–Whitney U test was used to compare parameters of different groups. All statistical calculations were done using statistical package SPSS version 13.0 for windows (SPSS, Inc., Chicago, IL). P < 0.05 was considered significant.
Results
SOCS-1 methylation can be found in the serum samples of AS patients
To examine if epigenetic modifications play any role in AS, we analyzed promoter methylation of an inflammation-related gene, SOCS-1 in the serum samples of forty-three AS patients as well as six HLA-B27 positive healthy controls. By using quantitative real time methylation specific PCR (qMSP), the samples from healthy controls did not detect any SOCS-1 methylation. In contrast, AS patients showed various level of SOCS-1 methylation which was significantly higher than that of normal (Fig. 1a). Bisulphite pyrosequencing of selected samples also confirmed these results. To exclude the possibility that the undetectable level of SOCS-1 methylation obtained from normal control is not due to the absence of DNA, we performed gel-based MSP analysis on a house-keeping gene COL2A1 using bisulphite-converted DNA extracted from serum sample (Fig. 1b). Both samples from patients and normal healthy controls demonstrated the presence of COL2A1 MSP products in the serum samples thus confirming that normal healthy control is devoid of SOCS-1 methylation.

Methylation of SOCS-1 in serum samples of 43 HLA-B27+ AS patients and 6 B27+ normal healthy controls. a Methylation of SOCS-1 was quantified by real time quantitative MSP analysis. Values in dot plot represented amount of copy number of methylated SOCS-1 DNA in 0.5 ml of serum samples. AS patients have significantly higher level of methylated SOCS-1 than normal control. The horizontal line represented median value. b Bisulphite pyrosequencing result from selected patients samples and normal control. Serum samples from patients with high (5, 6) and low (8, 19) level of methylated SOCS-1 as well as from normal control (C54, C55) were selected for bisulphite pyrosequencing. The methylation level of each CpG sites are depicted in a blue color scale. The genomic location for pyrosequencing and qMSP analysis was indicated in the schematic diagram above. c Representative gel electrophoresis image of COL2A1 MSP result from serum samples of AS and normal control. IVD (in vitro methylated DNA) was used as positive control for methylation and water (H2O) was used as PCR control. COL2A1 can be amplified from all the samples. Sample numbers were also indicated. **Denotes P < 0.01 by Mann–Whitney U. (Color figure online)
Methylation of SOCS-1 associates with the degree of inflammation in AS patients
Having demonstrated that AS patients have higher methylation of SOCS-1, it is of interest to investigate if the methylation of SOCS-1 associates with the degree of inflammation in AS. We therefore analyze the correlation between methylation of SOCS-1 and the degree of inflammation in terms of spondylopathy, sacroiliitis, as well as the amount of acute phase reactant, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Significant higher methylation of SOCS-1 was observed in patients with higher spondylopathy (P < 0.005, Fig. 2a) and sacroiliitis (P < 0.005, Fig. 2b). For acute phase reactant, a positive trend between the level of SOCS-1 methylation and ESR (R 2 = 0.08054, P = 0.0652, Fig. 2c) or CRP (R 2 = 0.1127, P = 0.0278, Fig. 2d) was observed. These result suggested that SOCS-1 methylation correlates with the degree of inflammation in AS.

Association between SOCS-1 methylation and degree of inflammation in 43 AS patients. Dot plot showing increased SOCS-1 methylation with a spondylopathy or b Sacroiliitis. Values in dot plot represented amount of copy number of methylated SOCS-1 DNA in 0.5 ml of serum samples. Scatter plot showing the association between SOCS-1 methylation and c erythrocyte sedimentation rate (ESR) or d C-reactive protein (CRP). The horizontal line represented median value. **Denotes P < 0.01 by Mann–Whitney U
Methylation of SOCS-1 associates with serum cytokine level in AS patients
Previously studies demonstrated that AS is associated with increased serum level of IL-6 and TNF-α [25]. To further examine if there is any relationship between these serum cytokines and SOCS-1 methylation, we first examined serum IL-6 and TNF-α level in our patients cohort as well as control. As expected, AS patients demonstrated significantly higher serum IL-6 and TNF-α level than that of healthy control (P < 0.001, Fig. 3a, b). Serum IL-6 level significantly correlated with that of TNF-α in AS patients (R 2 = 0.2052, P = 0.0023, Fig. 3c) which is in accordance to the previous study that IL-6 is one of the target of the TNF-α signaling pathway [26]. Interestingly, the patients with serum IL-6 above median showed a significantly higher SOCS-1 methylation than the patients with serum IL-6 below median (P < 0.001, Fig. 4a). Similar results can also be observed in the patients with serum TNF-α above median (P < 0.001, Fig. 4b).

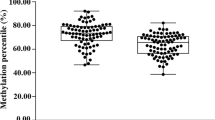
Cytokine level in 43 AS and 6 normal serum samples. Dot plot showing the amount of a IL-6 and b TNF-α in serum samples of AS patient or normal healthy control. Values in dot plot represented the amount of cytokine in pg/ml. The horizontal line represented median value. **Denotes P < 0.01 by Mann–Whitney U. c Scatter plot of serum IL-6 and TNF-α level in AS patients. The cytokine level correlates with each other (P = 0.0023). The regression line is also indicated

Correlation between cytokine level and SOCS-1 methylation in 43 AS patient. Dot plot showing patients with serum a IL-6 or b TNF-α above median (high) demonstrated a significantly higher SOCS-1 methylation than that with serum cytokine below median (low). Values in dot plot represented amount of copy number of methylated SOCS-1 DNA in 0.5 ml of serum samples. The horizontal line represented median value. **Denotes P < 0.01 by Mann–Whitney U
Discussion
In the present study, we examined the methylation of an inflammatory-related gene, SOCS-1 in serum samples of HLA-B27+ AS patients and B27+ normal healthy control. Methylation of SOCS-1 can only be detected in the serum samples of HLA-B27+ AS patients but not any of the B27+ healthy controls. Furthermore, significant association between methylation of SOCS-1 and degree of inflammation was also observed.
Aberrant DNA methylation plays an important role in several human diseases. Previous reports demonstrated that aberrant DNA methylation can be observed in chronic inflammatory [27, 28] and autoimmune rheumatic diseases [29]. This is the first report showing that aberrant DNA methylation can also be observed in AS thus further supporting the notion that aberrant DNA methylation is associated with chronic inflammatory disease. Recently, we have demonstrated that promoter methylation of SOCS-1 can be observed in the serum samples of chronic hepatitis C (CHC) patients and that CHC patients with higher serum SOCS-1 methylation level had better sustained virologic response [23]. Although the cellular source of methylated SOCS-1 in serum is currently unknown, we suspect that it is released from the cells undergoing inflammation which has increased rate of apoptosis [23, 30]. This hypothesis is supported by the observation that the amount of methylated SOCS-1 DNA is significantly associated with the degree of inflammation in AS patients. However, further experiments need to be performed to investigate the source as well as the mechanism of how the methylated DNA gets into systematic circulation.
SOCS-1 is an important negative regulator in JAK/STAT signaling pathway [31]. Although the mechanism leading to epigenetic silencing of SOCS-1 is currently unknown, it is plausible to originate from highly inflammatory cell with persistent cytokine signaling. Recent hypothesis suggest that persistent activation of signaling may lead to epigenetic silencing of its down-stream target [32]. For example, SHP-1 phosphatase which is a STAT3 target and negative regulator of intracellular signaling is found to be epigenetically silenced by promoter methylation in T cell lymphomas with persistent STAT3 activation [33]. Knock-down of STAT3 in the malignant T- cell induced DNA demethylation and re-expression of SHP-1. Moreover, we have previously observed promoter methylation of SOCS-1 in a gastric cancer cell line with persistent STAT3 activation [34]. Further, previous study demonstrated that TNF-α can lead to overexpression of IL-6 through activation of NF-κB and JAK/STAT signaling [26, 35]. Taken together, we propose that abnormal expression of TNF-α in AS patients [36] would activate these signalings thus leading to subsequent over-expression of IL-6. The activation of JAK/STAT signaling may result in the epigenetic silencing of SOCS-1, a STAT3 target and negative regulator of JAK/STAT signaling. This epigenetic event may further intensify the JAK/STAT signaling and subsequent expression of IL-6 thus perpetuating a vicious cycle.
NSAIDs have been considered as the standard treatment for AS patients for a long time [37]. Moreover, the effectiveness of TNF blockers [38] and monoclonal antibody against IL-6 receptor [39] in AS patients had been well demonstrated. Recently, the use of epigenetic modifiers in the treatment of autoimmune disease had been investigated [40, 41]. Whether modulation of SOCS-1 by hypomethylating agent alone or together with TNF blockers are effective in disease control deserves further investigation.
Another intriguing hypothesis is that patients with AS or other autoimmune rheumatic diseases may have increased incidence of malignancies [42]. Previous epidemiological observation suggested that AS patients had increased risk of acute leukemia [43]. This phenomenon may be explained by the fact that chronic inflammation-induced promoter methylation such as SOCS-1 tumor suppressor may contribute to carcinogenesis in the affected cell. In this regards, we surveyed the cancer incidence among all AS patients in our locality. Among 529 AS patients from rheumatology out-patient clinic at Dalin Tzu Chi General hospital, seven of them (1.3 %) have malignant tumor which is about 5 fold higher than the age-standardized cancer incidence in Taiwan [44].
As a preliminary observation, the correlation between SOCS-1 methylation and disease status of AS such as BASDAI (Bath Ankylosing Spondylitis Disease Activity Index), BASFI (Bath Ankylosing Spondylitis Functional Activity) and HAQ-S (Health Assessment Questionnaire-Spondylitis) were not determined in the current study. In assessment of disease severity and efficacy of treatment in AS, the ASAS (Assessment of SpondyloArthritis international Society) was formed and established a cure set of domain and individual instruments for evaluation of AS [45]. The potential of SOCS-1 methylation in AS assessment requires further investigations.
In conclusion, we have demonstrated that methylation of SOCS-1 can be detected in serum of HLA-B27+ AS patients. Methylation level of SOCS-1 correlated with the degree of inflammation as well as cytokine level. The prognostic potential of SOCS-1 methylation in predicting clinical outcome in AS patients deserves further investigation.
References
Dougados M, van der Linden S, Juhlin R, Huitfeldt B, Amor B, Calin A, Cats A, Dijkmans B, Olivieri I, Pasero G et al (1991) The European Spondyloarthropathy Study Group preliminary criteria for the classification of spondyloarthropathy. Arthritis Rheum 34:1218–1227
Khan MA, van der Linden SM (1990) Ankylosing spondylitis and other spondyloarthropathies. Rheum Dis Clin North Am 16:551–579
Brewerton DA, Hart FD, Nicholls A, Caffrey M, James DC, Sturrock RD (1973) Ankylosing spondylitis and HL-A 27. Lancet 1:904–907
van der Linden SM, Valkenburg HA, de Jongh BM, Cats A (1984) The risk of developing ankylosing spondylitis in HLA-B27 positive individuals. A comparison of relatives of spondylitis patients with the general population. Arthritis Rheum 27:241–249
Gratacos J, Collado A, Filella X, Sanmarti R, Canete J, Llena J, Molina R, Ballesta A, Munoz-Gomez J (1994) Serum cytokines (IL-6, TNF-alpha, IL-1 beta and IFN-gamma) in ankylosing spondylitis: a close correlation between serum IL-6 and disease activity and severity. Br J Rheumatol 33:927–931
Tutuncu ZN, Bilgie A, Kennedy LG, Calin A (1994) Interleukin-6, acute phase reactants and clinical status in ankylosing spondylitis. Ann Rheum Dis 53:425–426
Grom AA, Murray KJ, Luyrink L, Emery H, Passo MH, Glass DN, Bowlin T, Edwards C 3rd (1996) Patterns of expression of tumor necrosis factor alpha, tumor necrosis factor beta, and their receptors in synovia of patients with juvenile rheumatoid arthritis and juvenile spondyloarthropathy. Arthritis Rheum 39:1703–1710
Canete JD, Llena J, Collado A, Sanmarti R, Gaya A, Gratacos J, Blay M, Munoz-Gomez J (1997) Comparative cytokine gene expression in synovial tissue of early rheumatoid arthritis and seronegative spondyloarthropathies. Br J Rheumatol 36:38–42
Chan MW, Huang YW, Hartman-Frey C, Kuo CT, Deatherage D, Qin H, Cheng AS, Yan PS, Davuluri RV, Huang TH, Nephew KP, Lin HJ (2008) Aberrant transforming growth factor beta1 signaling and SMAD4 nuclear translocation confer epigenetic repression of ADAM19 in ovarian cancer. Neoplasia 10:908–919
Zuo T, Liu TM, Lan X, Weng YI, Shen R, Gu F, Huang YW, Liyanarachchi S, Deatherage DE, Hsu PY, Taslim C, Ramaswamy B, Shapiro CL, Lin HJ, Cheng AS, Jin VX, Huang TH (2011) Epigenetic silencing mediated through activated PI3K/AKT signaling in breast cancer. Cancer Res 71:1752–1762
Papageorgis P, Lambert AW, Ozturk S, Gao F, Pan H, Manne U, Alekseyev YO, Thiagalingam A, Abdolmaleky HM, Lenburg M, Thiagalingam S (2010) Smad signaling is required to maintain epigenetic silencing during breast cancer progression. Cancer Res 70:968–978
Baylin SB, Jones PA (2011) A decade of exploring the cancer epigenome: biological and translational implications. Nat Rev Cancer 11:726–734
Jones PA, Baylin SB (2007) The epigenomics of cancer. Cell 128:683–692
Herman JG, Merlo A, Mao L, Lapidus RG, Issa JP, Davidson NE, Sidransky D, Baylin SB (1995) Inactivation of the CDKN2/p16/MTS1 gene is frequently associated with aberrant DNA methylation in all common human cancers. Cancer Res 55:4525–4530
Merlo A, Herman JG, Mao L, Lee DJ, Gabrielson E, Burger PC, Baylin SB, Sidransky D (1995) 5′ CpG island methylation is associated with transcriptional silencing of the tumour suppressor p16/CDKN2/MTS1 in human cancers. Nat Med 1:686–692
Esteller M, Corn PG, Baylin SB, Herman JG (2001) A gene hypermethylation profile of human cancer. Cancer Res 61:3225–3229
Chan MW, Chan LW, Tang NL, Tong JH, Lo KW, Lee TL, Cheung HY, Wong WS, Chan PS, Lai FM, To KF (2002) Hypermethylation of multiple genes in tumor tissues and voided urine in urinary bladder cancer patients. Clin Cancer Res 8:464–470
Chou JL, Su HY, Chen LY, Liao YP, Hartman-Frey C, Lai YH, Yang HW, Deatherage DE, Kuo CT, Huang YW, Yan PS, Hsiao SH, Tai CK, Lin HJ, Davuluri RV, Chao TK, Nephew KP, Huang TH, Lai HC, Chan MW (2010) Promoter hypermethylation of FBXO32, a novel TGF-beta/SMAD4 target gene and tumor suppressor, is associated with poor prognosis in human ovarian cancer. Lab Invest 90:414–425
Laird PW (2003) The power and the promise of DNA methylation markers. Nat Rev Cancer 3:253–266
Chan MW, Chu ES, To KF, Leung WK (2004) Quantitative detection of methylated SOCS-1, a tumor suppressor gene, by a modified protocol of quantitative real time methylation-specific PCR using SYBR green and its use in early gastric cancer detection. Biotechnol Lett 26:1289–1293
Lee TL, Leung WK, Chan MW, Ng EK, Tong JH, Lo KW, Chung SC, Sung JJ, To KF (2002) Detection of gene promoter hypermethylation in the tumor and serum of patients with gastric carcinoma. Clin Cancer Res 8:1761–1766
Clark SJ, Statham A, Stirzaker C, Molloy PL, Frommer M (2006) DNA methylation: bisulphite modification and analysis. Nat Protoc 1:2353–2364
Tseng KC, Chou JL, Huang HB, Tseng CW, Wu SF, Chan MW (2013) SOCS-1 promoter methylation and treatment response in chronic hepatitis C patients receiving pegylated-interferon/ribavirin. J Clin Immunol 33(6):1110–1116
Colella S, Shen L, Baggerly KA, Issa JP, Krahe R (2003) Sensitive and quantitative universal pyrosequencing methylation analysis of CpG sites. Biotechniques 35:146–150
Bal A, Unlu E, Bahar G, Aydog E, Eksioglu E, Yorgancioglu R (2007) Comparison of serum IL-1 beta, sIL-2R, IL-6, and TNF-alpha levels with disease activity parameters in ankylosing spondylitis. Clin Rheumatol 26:211–215
Squarize CH, Castilho RM, Sriuranpong V, Pinto DS Jr, Gutkind JS (2006) Molecular cross-talk between the NFkappaB and STAT3 signaling pathways in head and neck squamous cell carcinoma. Neoplasia 8:733–746
Kang GH, Lee HJ, Hwang KS, Lee S, Kim JH, Kim JS (2003) Aberrant CpG island hypermethylation of chronic gastritis, in relation to aging, gender, intestinal metaplasia, and chronic inflammation. Am J Pathol 163:1551–1556
Kaneto H, Sasaki S, Yamamoto H, Itoh F, Toyota M, Suzuki H, Ozeki I, Iwata N, Ohmura T, Satoh T, Karino Y, Toyota J, Satoh M, Endo T, Omata M, Imai K (2001) Detection of hypermethylation of the p16(INK4A) gene promoter in chronic hepatitis and cirrhosis associated with hepatitis B or C virus. Gut 48:372–377
Ballestar E (2011) Epigenetic alterations in autoimmune rheumatic diseases. Nat Rev Rheumatol 7:263–271
Baud V, Karin M (2001) Signal transduction by tumor necrosis factor and its relatives. Trends Cell Biol 11:372–377
Nicola NA, Greenhalgh CJ (2000) The suppressors of cytokine signaling (SOCS) proteins: important feedback inhibitors of cytokine action. Exp Hematol 28:1105–1112
Chou JL, Chen LY, Lai HC, Chan MW (2010) TGF-beta: friend or foe? The role of TGF-beta/SMAD signaling in epigenetic silencing of ovarian cancer and its implication in epigenetic therapy. Expert Opin Ther Targets 14:1213–1223
Zhang Q, Wang HY, Marzec M, Raghunath PN, Nagasawa T, Wasik MA (2005) STAT3- and DNA methyltransferase 1-mediated epigenetic silencing of SHP-1 tyrosine phosphatase tumor suppressor gene in malignant T lymphocytes. Proc Natl Acad Sci USA 102:6948–6953
To KF, Chan MW, Leung WK, Ng EK, Yu J, Bai AH, Lo AW, Chu SH, Tong JH, Lo KW, Sung JJ, Chan FK (2004) Constitutional activation of IL-6-mediated JAK/STAT pathway through hypermethylation of SOCS-1 in human gastric cancer cell line. Br J Cancer 91:1335–1341
Tanabe K, Matsushima-Nishiwaki R, Yamaguchi S, Iida H, Dohi S, Kozawa O (2010) Mechanisms of tumor necrosis factor-alpha-induced interleukin-6 synthesis in glioma cells. J Neuroinflammation 7:16
Lu MC, Yang KL, Tung CH, Huang KY, Yu HC, Liu SQ, Lai NS (2008) Higher LPS-stimulated TNF-alpha mRNA levels in peripheral blood mononuclear cells from Chinese ankylosing spondylitis patients with –308G/A polymorphism in promoter region of tumor necrosis factor: association with distinct A33/B58/Cw10 haplotypes. Rheumatol Int 29:189–195
Braun J, Sieper J (2007) Ankylosing spondylitis. Lancet 369:1379–1390
Heiberg MS, Nordvag BY, Mikkelsen K, Rodevand E, Kaufmann C, Mowinckel P, Kvien TK (2005) The comparative effectiveness of tumor necrosis factor-blocking agents in patients with rheumatoid arthritis and patients with ankylosing spondylitis: a six-month, longitudinal, observational, multicenter study. Arthritis Rheum 52:2506–2512
Shima Y, Tomita T, Ishii T, Morishima A, Maeda Y, Ogata A, Kishimoto T, Tanaka T (2011) Tocilizumab, a humanized anti-interleukin-6 receptor antibody, ameliorated clinical symptoms and MRI findings of a patient with ankylosing spondylitis. Mod Rheumatol 21:436–439
Vishwakarma S, Iyer LR, Muley M, Singh PK, Shastry A, Saxena A, Kulathingal J, Vijaykanth G, Raghul J, Rajesh N, Rathinasamy S, Kachhadia V, Kilambi N, Rajgopal S, Balasubramanian G, Narayanan S (2013) Tubastatin, a selective histone deacetylase 6 inhibitor shows anti-inflammatory and anti-rheumatic effects. Int Immunopharmacol 16:72–78
Motegi K, Azuma M, Tamatani T, Ashida Y, Sato M (2005) Expression of aquaporin-5 in and fluid secretion from immortalized human salivary gland ductal cells by treatment with 5-aza-2′-deoxycytidine: a possibility for improvement of xerostomia in patients with Sjogren’s syndrome. Lab Invest 85:342–353
Bernatsky S, Ramsey-Goldman R, Clarke A (2006) Malignancy and autoimmunity. Curr Opin Rheumatol 18:129–134
Au WY, Hawkins BR, Cheng N, Lie AK, Liang R, Kwong YL (2001) Risk of haematological malignancies in HLA-B27 carriers. Br J Haematol 115:320–322
Chiang CJ, Chen YC, Chen CJ, You SL, Lai MS (2010) Cancer trends in Taiwan. Jpn J Clin Oncol 40:897–904
van der Heijde D, Bellamy N, Calin A, Dougados M, Khan MA, van der Linden S (1997) Preliminary core sets for endpoints in ankylosing spondylitis. Assessments in Ankylosing Spondylitis Working Group. J Rheumatol 24:2225–2229
Acknowledgments
This study was supported by research Grant from Dalin Tzu Chi General Hospital (98-2-2); College of Science, National Chung Cheng University and National Science Council, Taiwan (NSC100-2320-B-194-002).
Conflict of interest
The authors have declared no conflicts of interest
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lai, NS., Chou, JL., Chen, G.C.W. et al. Association between cytokines and methylation of SOCS-1 in serum of patients with ankylosing spondylitis. Mol Biol Rep 41, 3773–3780 (2014). https://doi.org/10.1007/s11033-014-3242-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11033-014-3242-2