
Abstract
Repetitive transcranial magnetic stimulation (rTMS) is a technique protecting neurons against diverse neurodegenerative disorders by delivering magnetic stimuli into the brain through the intact scalp. In the current study, the protection effect of rTMS on Parkinson’s disease (PD) and the associated mechanism driving the treatment were explored. The PD symptoms were induced using 6-OHDA in mice, and the effect of rTMS of two frequencies (1 Hz and 10 Hz) on the cognitive behaviors and neuron viability was detected. Afterwards, the level of Aβ1–42 and activity of MKK7-ERK-Fos-APP axis under the administration of rTMS were recorded as well. The intracranial injection of 6-OHDA impaired the cognitive behaviors of the mice in the test of Morris water maze as well as reducing the viability and number of neurons in PD mice. After the treatment of rTMS of both frequencies, the cognitive function of mice was improved and the neuron viability and number were restored in mice brain tissues. The administration of rTMS also increased the cerebrospinal fluid (CSF) level of Aβ1–42 in PD mice, which was accompanied by the suppressed levels of p-MKK7, p-ERK1/2, p–c-Fos, and APP. Moreover, the effect of rTMS on mice nerve system was all exerted in a frequency-dependent manner. In conclusion, the findings outlined in the current study affirmed the protection effect of rTMS against PD. The anti-PD function of rTMS was associated with the suppression of MKK7-ERK-Fos-APP axis, which subsequently resulted in the increased CSF Aβ1–42 level and decreased brain Aβ1–42 level.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Parkinson’s disease (PD) is a major neurodegenerative disorder occurring as a result of cell death of dopaminergic (DA) neurons. The disease is characterized by bradykinesia, resting tremor, muscular rigidity, and gait disturbance in elderly population [1, 2]. Currently, the diagnosis of PD is primarily based on clinical criteria [3]. However, given the fact that the neurodegenerative process of PD begins several years before the associated symptoms can be diagnosed, the current criteria themselves bring some limitations. According to the review of Hardy and Revesz, the early diagnosis of PD was a priority for the development of disease-modifying therapies for this disorder [3]. Thus, increasing attentions have been paid to the exploration of novel biomarkers to predict the progression of PD [4].
Emerging evidence shows that molecular changes in the brain tissues can be reflected in cerebrospinal fluid (CSF) composition [5]. Thus, CSF may represent a promising source for discovering biomarkers of neurodegenerative diseases. For example, recent studies have highlighted the potential of CSF biomarkers in the early diagnosis of AD: molecules such as amyloid β1–42 (Aβ1–42), total tau (t-tau), and phosphorylated tau (p-tau) are all biomarkers reflecting the pathology of AD [6]. Regarding the biomarkers for PD, it is recognized in the recent years that classical CSF biomarkers of AD can also be utilized in the diagnosis and treatment of PD [5, 7], of which Aβ1–42 has drawn a lot of interest [8]. The peptide is a typical member of Aβ peptides generated from amyloid precursor protein (APP) that is an integral membrane protein [9]. For a quite long time, the level of Aβ1–42 has been related to the progression of AD [10] and is being increasing descripted as a factor participating in the onset and progression of PD [8]. Numerous proteins are involved in post-transcription cleavage of APP into Aβs. For example, ADAM10 is important to the APP cleavage that does not form Aβs [11,12,13,14,15]. In another pathway, APP is underwent cleavage of BACE1 or BACE2, which subsequently produces amyloidogenic Aβ peptide in a γ-secretase cleavage manner [16,17,18,19,20]. Except for the above-mentioned molecules, presenilin, nicastrin (NCSTN), APH1B, and PEN2 are also uniquely involved in the cleavage of APP based on the tissue specificity [21,22,23]. Taken together, the levels of Aβ peptides are evidently reflecting the function of multiple pathways involved in the pathogenesis of neurodegenerative disorders such as PD. Thus, it is reasonable to develop treatment strategies for PD by targeted regulating the level of Aβ, which will restore the function of neurons in multi-pronged ways.
Noninvasive repetitive transcranial magnetic stimulation (rTMS) is a method of delivering magnetic stimuli into the brain through the intact scalp. In the recent years, the technique has been applied to manage neurodegenerative disorders in clinic and contributes to the up-regulation of endogenous neurotrophins in brains tissues [24, 25]. Since the clinical manifestations of PD are characterized by the abnormal neuronal activity within the basal ganglia, several studies have employed rTMS to protect brain tissues against progression of PD. For example, in the study of Miranda et al., the authors demonstrated that the patients receiving 25 Hz rTMS treatment for 4 weeks showed a gradual improvement in walking and hand movements [26]. The treatment effect of rTMS on PD was also proved in the meta-analysis of Fregni et al.: the pooled effect size across the studies significantly favored the rTMS stimulation when compared with sham stimulation [27]. However, even with comprehensive application of rTMS in clinic, the mechanism driving the effect of rTMS on neurodegenerative disorders stays partially revealed. Given the ubiquitous influence of rTMS on nerve system, the understanding of the molecular basis of the treatment will promote the application of the technique for more disorders. In 2013, Tan et al. reported that low-frequency (1 Hz) rTMS could reverse the abnormal level of Aβ1–42 in memory deficit rats [28]. The results were inspirable in that it linked the level of Aβ1–42 to the treatment effect of rTMS, which reminded us of the possibility that the anti-PD effect of rTMS might be also related to its interaction with brain Aβ1–42.
To verify the possibility, PD symptoms were induced in mice using 6-OHDA method. Then the PD mice were subjected to the treatment of rTMS of two frequencies (low frequency: 1 Hz; high frequency: 10 Hz) and the effect of rTMS administrations on the cognitive behaviors and brain structures of mice was assessed. Additionally, by focusing on the Aβ1–42 levels and MKK7-ERK-Fos-APP pathway that regulates the generation of Aβ1–42 [29], we also attempted to explain the pathways mediating anti-PD function of rTMS.
Methods
Induction of Parkinson’s disease using 6-OHDA
C57BL/6 mice (10-week-old) were provided by Changsheng Company (Jilin, Changchun) and housed at 25 ± 1 °C with a constant humidity of 45–55% with food and water available. For 6-OHDA lesions induction, mice were anesthetized using 50 mg/kg body weight phenobarbital sodium and were positioned within a stereotaxic apparatus. The left striatum was exposed by opening the brain skin along the sagittal suture. Afterwards, 2 μl 6-OHDA (4 μg/μl) (162,957–50 mg, Sigma, China) was injected into the left striatum. 10 min after the injection, the lesion was sutured and mice were housed routinely for 2 weeks before the rTMS treatment (Figure S1). For mice in Sham group, 6-OHDA was replaced by 0.02% vitamin C solution (A103534-100 g, Aladdin, China). This study was carried out in accordance with the recommendations of the Animal Care Guidelines for the Care and Use of Institutional Animal Ethics Committee of China Medical University and was ethically approved by the Institutional Animal Ethics Committee of China Medical University.
Administration of rTMS
The rTMS treatment was performed following previous study of Ma et al.: briefly, the mice in low-frequency rTMS group (PD + L rTMS) were exposed to low-frequency rTMS (1 Hz) with magnetic stimulation intensity set at 30% maximum output (1.26T). Two sessions of rTMS consisting of 1000 pulses in 10 trains were performed for 14 consecutive days. An interval of 2 min was between the two sessions to cool down the coil, and the interval between each train was 20 s. For administration of high-frequency rTMS (PD + H rTMS), the frequency was set to 10 Hz.
Morris water maze
MWM was used to test the learning and memorizing abilities. The assays were performed routinely as reported previously with two investigators blind to the experiment designs. The test included including a 5-day visible platform trial and a 1-day probe trial and. In brief, for visible platform trail in 60 s, mice were allowed to swim for 60 s before getting to the platform for four times each day. If the mice failed, investigator would help the mice to stay on the platform for 10 s before another test. For probe trial in the 6th day, the platform was removed, and then the time of mice staying in the quadrant in 60 s as well as the number of penetrating through the quadrant of the former platform position in 60 s in each test were measured.
Nissl staining
The substantia nigra (SN) sections were firstly subjected to dehydration, dimethylbenzene, and alcohol administration of different concentrations. Afterwards, the sections were incubated with 0.5% cresol purple for 10 min at room temperature. After being washed using ddH2O, the sections were sequentially administrated with 0.25% glacial acetic acid-alcohol solution, alcohol of different concentrations, and dimethylbenzene. The results of the staining were detected using a Microscope (BX53, OLUMPUS, Japan) at 100×.
Immunochemistry detection
Brain tissues were dehydrated using alcohol in different concentrations and embedded in paraffin. Then 5-μm sections were administrated with alcohol in different concentrations and washed with PBS for three times. Primaries antibody against tyrosine hydroxylase (TH) (1:200) (25859-1-AP, Proteintech, China), brain derived neurotrophic factor (BDNF) (1:200) (25699-1-AP, Proteintech, USA), and Aβ1–42 (1:200) (ab2539, Abcam, UK) were then added on sections and incubated at 4 °C overnight. After three cycles of PBS washing, secondary Cy3-labled antibodies (A0277, goat anti-rabbit, Beyotime Biotechnology, China) were incubated with sections at 37 °C for 30 min. Afterwards, the sections were labeled with horseradish peroxidase-labeled avdin at 37 °C for 30 min and incubated with DAB solution (DA1010, Solarbio, China). Finally, the sections were subjected to re-stain using hematoxylin for 3 min and dehydrated using alcohol of different concentrations. Images were captured using a fluorescence microscope (BX53, Olumpus, Japan) at 400× magnification.
Enzyme-linked immuno sorbent assay (ELISA)
The CSF level of Aβ1–42 was detected using Aβ1–42 Detection Kit following instruction for manufacturer (CEA946Mu, USCN, China). The results was represented by OD value at 450 nm using a Microplate Reader (ELX-800, BIOTEK, USA).
Western blotting
Brain tissues were lysed using RIPA lysis buffer (P0013B, Beyotime Biotechnology, China). The concentrations of protein samples were determined using BCA Protein Concentration Kit (P0009, Beyotime Biotechnology, China). After being separated by sodium dodecyl sulfatepolyacrylamide gel electrophoresis (SDS-PAGE) at 80 V for 2.5 h, protein samples were transferred to PVDF membranes and blocked using 5% skim milk powder for 1 h. Then the membranes were incubated with primary antibodies against MKK7 (1:10,000) (ab52618, Abcam, UK), phosphorylated MKK7 (p-MKK7) (1:1000) (Bioss, bs-3277R, China), ERK1/2 (1:1000) (#4695, CST, USA), p-ERK1/2 (1:1000) (#4370, CST, USA), p–c-Fos (1:1000) (ab27793, Abcam, UK), and β-actin (1:1000) (bsm-33036M, Bioss, China) at 4 °C overnight. Then secondary IgG-HRP antibodies (1:5000) (A0208, goat-anti rabbit; A0216, goat anti-murine, Beyotime Biotechnology, China) were added onto membranes and incubated at 37 °C for 45 min. Bands were developed using ECL Plus reagent (P0018, Beyotime Biotechnology, China), and the relative expression levels of proteins were calculated by Gel-Pro-Analyzer (Media Cybernetics, USA).
Statistical analysis
The data were represented by mean ± standard deviation (SD). One-way analysis of variance and post hoc multiple comparisons using Fisher’s Least Significance Difference (LSD) method were performed using GraphPad Prism version 6.0 (GraphPad Software, Inc., San Diego, CA) with a significant level of 0.05 (two tailed).
Results
Administration of rTMS improved cognitive behaviors of PD mice
As shown in Fig. 1, the injection of 6-OHDA dramatically impaired the cognitive function of mice when compared with mice in Sham group. The induction of PD significantly increased the latency of escaping time, suppressed the proportion of mice’s penetrating path in platform area, and shortened the time of mice staying in the platform quadrant (Fig. 1). For PD mice treated with rTMS, the data showed that both frequencies significantly improved the cognitive function of the mice (Fig. 1). Moreover, the improvement effect of rTMS increased with frequency, with rTMS of 10 Hz showing a better treatment outcome than rTMS of 1 Hz (Fig. 1).

Administration of rTMS improved cognitive function of PD mice (mean ± SD). a Quantitative analysis results of escaping latency. b Quantitative analysis results of the proportion of platform area in the pathway of mice traveling. c Quantitative analysis results of the number of mice penetrating former platform. *P < 0.05 vs. Sham group. #P < 0.05 vs. PD group. Each assay was represented by six replicates
Administration of rTMS protected SN neurons against 6-OHDA-induced damages
The results of Nissl staining showed that the number of SN neurons (stained blue) in PD group was lower than that in Sham group (Fig. 2), but the administration of rTMS of both frequencies restored the SN number in PD mice, evidently supporting the protection effect of the technique on neuron viability. Additionally, we also detected the expression and distribution of TH and BDNF that are two classical neurotrophic factors. The results of immunochemistry detection showed that although the injection of 6-OHDA dramatically suppressed the expression and distribution of both factors (stained brown), the administration of rTMS counteracted the effect of 6-OHDA and increased the levels of both indicators in SN tissues (Fig. 2). Similar to the effect on cognitive behaviors, the protection effect of rTMS on SN neurons also increased with frequency (Fig. 2).

Administration of rTMS increased neuron viability and number in the SN of PD mice (mean ± SD). Magnification for Nissl staining, ×100. Magnification for immunochemistry detection of TH, ×100. Magnification for immunochemistry detection of BDNF, ×400. Each assay was represented by six replicates
Administration of rTMS increased CSF Aβ1–42 level while suppressed the brain Aβ1–42 level in PD mice
The abnormally low CSF Aβ1–42 level associated with abnormally high brain Aβ1–42 level has been gradually recognized as a symptom of PD. The theory was verified in the current study: the CSF Aβ1–42 level was decreased in mice after 6-OHDA injection, while the brain Aβ1–42 level was increased (Fig. 3a, b). Nevertheless, the administration of rTMS reversed the levels of Aβ1–42 in CSF and brain tissues in a frequency-dependent manner (Fig. 3), which was a representative of attenuation of PD symptoms in mice. The results further supported our hypothesis that the protection effect of rTMS against PD was associated with its effect on the brain levels of Aβ1–42.

Administration of rTMS increased CSF Aβ1–42 level while suppressed brain tissue Aβ1–42 level in PD mice (mean ± SD). a Quantitative analysis results of ELISA detection of the CSF Aβ1–42 level. b Representative images of immunochemistry detection of the brain tissue Aβ1–42 level. Magnification ×400. *P < 0.05 vs. Sham group. #P < 0.05 vs. PD group. Each assay was represented by six replicates
Influence of rTMS on brain Aβ1–42 level was associated with the suppression of MKK7-ERK-Fos-APP axis
The generation of Aβ1–42 is closely related to the expression of APP. Thus, we also detected the activity of MKK7-ERK-Fos-APP axis in the current study. The injection of 6-OHDA increased the protein levels of p-MKK7, p-ERK1/2, p–c-Fos, and APP (Fig. 4), which would result in further deposition of Aβ1–42 in brain tissues. After being subjected to rTMS administration of both frequencies, the tissue levels of all the four indicators were suppressed (Fig. 4), evidently indicating the inhibition effect of rTMS on MKK7-ERK-Fos-APP axis. Moreover, the effect of rTMS administration on molecule expressions also strengthened with frequency (Fig. 4).

Administration of rTMS inhibited activity of MMK7-ERK-c-Fos-APP axis (mean ± SD). *P < 0.05 vs. Sham group. #P < 0.05 vs. PD group. Each assay was represented by six replicates
Discussion
In recent years, with the emerging evidence indicating the treatment role of electric current in multiple disorders, electromagnetic phenomena has been applied to induce electric current in human bodies [30]. Of types of diseases handled by magnetic stimulation, nerve disorders have shown extra sensitivity to the technique [31]. The reports regarding the protection effect of magnetic stimulation against neurodegenerative have drawn the sufficient development of the so-called rTMS technique [32]. Based on these previous studies, we attempted to provide a complementary explanation to the treatment mechanism driving the neuroprotection effect of rTMS on PD patients. With a series of in vivo assays, our findings supported the effect of rTMS in improving the cognitive function of PD mice. Moreover, we also indicated that the treatment effect of rTMS against PD was associated with the inhibition of MKK7-ERK1/2-c-Fos-APP, which finally resulted in Aβ1–42’s suppression in brain tissues and induction in CSF. The changes in Aβ1–42 level detected in the current evidently represented the amelioration of PD [8].
Aβ1–42 is one of the major components of Aβ oligomers that are the typical endogenous neurotoxic substance [28]. In a quite long period, the component has been conceived as a major factor causing synaptic dysfunction in the early stage of AD. For example, in the study of Colaianna et al., Aβ1–42 suppressed endogenous neurotrophin contents in vitro [33]. Moreover, the AD promoting function of Aβ1–42 was further verified with in vivo model [34]. As multiple disease processes might coexist in PD, scientists infer that the combination of different biomarkers that reflect each pathogenic mechanism is likely to be an appropriate approach to develop novel treatment strategies for both diseases [35]. Such hypothesis has been solidly proved with Aβ1–42. The association between CSF Aβ1–42 level and cognition decline in PD patients has been extensively reported [9]. Similar results were also verified in the current study: rTMS administrations of both frequencies showed considerable effect in inducing CSF Aβ1–42 level, which was accompanied by the improvements in cognitive function and neuron viability in PD mice.
The application frequency of rTMS has been long debated in that the results regarding the treatment effect of rTMS were viable. Meta-analysis of indicated that high-frequency rTMS improved motor symptoms in PD patients while low-frequency rTMS had shown little benefit [36, 37]. However, in the studies of Wagle-Shukla et al. and Chen et al., the authors inferred that the applications of low-frequency rTMS (1 Hz) could improve dyskinesia [38, 39]. Additionally, in the study of Tan et al., rTMS of 1 Hz attenuated Aβ1–42-induced memory deficits in rats [28]. To determine the influence of administration frequency on the treatment outcome of rTMS, we employed two frequencies in the current study. Our results showed that the treatment effect of rTMS on the cognitive behaviors and CSF Aβ1–42 level in PD mice was exerted in a frequency-dependent pattern. Nevertheless, even rTMS of 1 Hz showed evidently amelioration effect on the PD symptoms in mice. The results might be a complementary to the long-term controversy on the effective frequency of rTMS.
The application of rTMS has been gradually accepted by patients with neurodegenerative patients and clinicians, but the mechanism driving the treatment effect of the technique remains partially explained. Thus, we also detected the impact of rTMS treatment on MKK7-ERK1/2-c-Fos-APP axis. As being described by Huang et al., MKK7 and ERK1/2 activated by ApoE induced c-Fos phosphorylation, which then stimulated transcription factor AP-1. The stimulated AP-1 in turn enhanced the transcription of APP and subsequently increased brain Aβ1–42 level [29]. In the current day, the injection of 6-OHDA induced the activation of the axis as expected. After the treatment of rTMS, the activities of all the members involved the signaling transduction were suppressed, which resulted in the suppressed level of Aβ1–42 in brain tissues. The results proved the association between the axis and treatment effect of rTMS. However, no further modulation was performed to determine whether the treatment function of rTMS critically depended on the activity of the axis.
Collectively, the findings outlined in the current study affirmed the protection effect of rTMS against PD, and the effect could be strengthened with rTMS frequency. Contrary to some previous reports, our results showed that even low-frequency (1 Hz) rTMS could evidently relieve mice from PD impairments. At molecular level, we found that the treatment effect of rTMS was associated with the suppression of MKK7-ERK1/2-c-Fos-APP axis, which finally resulted in the decreased Aβ1–42 level in brain tissues and increased Aβ1–42 level in CSF. However, the conclusions were merely based on in vivo animal models and no further validation was performed to determine the key role of MKK7-ERK1/2-c-Fos-APP in the anti-PD function of rTMS. To elucidate the effect and mechanism of technique, more comprehensive work with clinical cohort and targeted modulation will be performed.
References
Driver JA, Logroscino G, Gaziano JM, Kurth T (2009) Incidence and remaining lifetime risk of Parkinson disease in advanced age. Neurology 72(5):432–438. https://doi.org/10.1212/01.wnl.0000341769.50075.bb
Buchman AS, Shulman JM, Nag S, Leurgans SE, Arnold SE, Morris MC, Schneider JA, Bennett DA (2012) Nigral pathology and parkinsonian signs in elders without Parkinson’s disease. Ann Neurol 71(2):258–266
Lees AJ, Hardy J, Revesz T (2004) Parkinson’s disease. Lancet 363(Suppl):1783–1793
Marras C, Lang A (2013) Parkinson’s disease subtypes: lost in translation? J Neurol Neurosur Ps 84(4):409–415. https://doi.org/10.1136/jnnp-2012-303455
van Dijk KD, Teunissen CE, Drukarch B, Jimenez CR, Groenewegen HJ, Berendse HW, van de Berg WD (2010) Diagnostic cerebrospinal fluid biomarkers for Parkinson’s disease: a pathogenetically based approach. Neurobiol Dis 39(3):229–241. https://doi.org/10.1016/j.nbd.2010.04.020
Dubois B, Feldman HH, Jacova C, Cummings JL, Dekosky ST, Barberger-Gateau P, Delacourte A, Frisoni G, Fox NC, Galasko D (2010) Revising the definition of Alzheimer’s disease: a new lexicon. Lancet Neurol 9(11):1044–1045
Nyhlén J, Constantinescu R, Zetterberg H (2010) Problems associated with fluid biomarkers for Parkinson’s disease. Biomarkers Med 4(5):671–681
Parnetti L, Castrioto A, Chiasserini D, Persichetti E, Tambasco N, El-Agnaf O, Calabresi P (2013) Cerebrospinal fluid biomarkers in Parkinson disease. Nat Rev Neurol 9(3):131–140
Bekris LM, Tsuang DW, Peskind ER, Yu CE, Montine TJ, Zhang J, Zabetian CP, Leverenz JB (2015) Cerebrospinal fluid Aβ42 levels and APP processing pathway genes in Parkinson’s disease. Movement Disord 30(7):936–944
Zetterberg H, Lunn MP, Herukka SK (2012) Clinical use of cerebrospinal fluid biomarkers in Alzheimer’s disease. Biomarkers Med 6(4):371–376
Postina R (2008) A closer look at alpha-secretase. Curr Alzheimer Res 5(2):179–186
Deuss M, Reiss K, Hartmann D (2008) Part-time alpha-secretases: the functional biology of ADAM 9, 10 and 17. Curr Alzheimer Res 5:2
Postina R, Schroeder A, Dewachter I, Bohl J, Schmitt U, Kojro E, Prinzen C, Endres K, Hiemke C, Blessing M (2004) A disintegrin-metalloproteinase prevents amyloid plaque formation and hippocampal defects in an Alzheimer disease mouse model. J Clin Invest 113(10):1456
Colciaghi F, Borroni B, Pastorino L, Marcello E, Zimmermann M, Cattabeni F, Padovani A, Di LM (2002) [alpha]-Secretase ADAM10 as well as [alpha]APPs is reduced in platelets and CSF of Alzheimer disease patients. Mo Med 8(2):67
Qin W, Ho L, Wang J, Peskind E, Pasinetti GM (2009) S100A7, a novel Alzheimer’s disease biomarker with non-amyloidogenic alpha-secretase activity acts via selective promotion of ADAM-10. PLoS ONE 4(1):e4183
Zetterberg H, Andreasson U, Hansson O, Wu G, Sankaranarayanan S, Andersson ME, Buchhave P, Londos E, Umek RM, Minthon L (2008) Elevated cerebrospinal fluid BACE1 activity in incipient Alzheimer disease. Arch Neurol-Chicago 65(8):1102–1107
Wu G, Sankaranarayanan S, Tugusheva K, Kahana J, Seabrook G, Shi XP, King E, Devanarayan V, Cook JJ, Simon AJ (2008) Decrease in age-adjusted cerebrospinal fluid beta-secretase activity in Alzheimer’s subjects. Clin Biochem 41(12):986–996
Ewers M, Zhong Z, Bürger K, Wallin A, Blennow K, Teipel SJ, Shen Y, Hampel H (2008) Increased CSF-BACE 1 activity is associated with ApoE-epsilon 4 genotype in subjects with mild cognitive impairment and Alzheimer’s disease. Brain 131(5):1252–1258
Sun X, Wang Y, Qing H, Christensen MA, Liu Y, Zhou W, Tong Y, Xiao C, Huang Y, Zhang S (2005) Distinct transcriptional regulation and function of the human BACE2 and BACE1 genes. FASEB J 19(7):739–749
Stockley JH, O’Neill C (2007) The proteins BACE1 and BACE2 and beta-secretase activity in normal and Alzheimer’s disease brain. Biochem Soc Trans 35(3):574–576
Zhang J (2002) aph-1 and pen-2 are required for Notch pathway signaling, gamma-secretase cleavage of betaAPP, and presenilin protein accumulation. Dev Cell 3(1):85–97
Baulac S, Lavoie MJ, Kimberly WT, Strahle J, Wolfe MS, Selkoe DJ, Xia W (2003) Functional gamma-secretase complex assembly in Golgi/trans-Golgi network: interactions among presenilin, nicastrin, Aph1, Pen-2, and gamma-secretase substrates. Neurobiol Dis 14(2):194–204
Kimberly WT, Lavoie MJ, Ostaszewski BL, Ye W, Wolfe MS, Selkoe DJ (2003) γ-secretase is a membrane protein complex comprised of presenilin, nicastrin, aph-1, and Pen-2. Proc Natl Acad Sci USA 100(11):6382–6387
Gersner R, Kravetz E, Feil J, Pell G, Zangen A (2011) Long-term effects of repetitive transcranial magnetic stimulation on markers for neuroplasticity: differential outcomes in anesthetized and awake animals. J Neurosci 31(20):7521–7526
Wang HY, Crupi D, Liu J, Stucky A, Cruciata G, Di RA, Friedman E, Quartarone A, Ghilardi MF (2011) Repetitive transcranial magnetic stimulation enhances BDNF-TrkB signaling in both brain and lymphocyte. J Neurosci 31(30):11044–11054
Miranda PC, Lomarev M, Hallett M (2006) Modeling the current distribution during transcranial direct current stimulation. Clin Neurophysio 117(7):1623–1629
Fregni F, Simon D, Wu A, Pascual-Leone A (2005) Non-invasive brain stimulation for Parkinson’s disease: a systematic review and meta-analysis of the literature. J Neurol Neurosur Psychiatry 76(12):1614
Tan T, Xie J, Liu T, Chen X, Zheng X, Tong Z, Tian X (2013) Low-frequency (1 Hz) repetitive transcranial magnetic stimulation (rTMS) reverses Aβ(1–42)-mediated memory deficits in rats. Exp Gerontol 48(8):786–794
Huang YA, Zhou B, Wernig M, Südhof TC (2017) ApoE2, ApoE3, and ApoE4 differentially stimulate app transcription and Aβ secretion. Cell 168(3):427
Ridding MC, Rothwell JC (2007) Is there a future for therapeutic use of transcranial magnetic stimulation? Nat Rev Neurosci 8(7):559–567
Ni Z, Chen R (2015) Transcranial magnetic stimulation to understand pathophysiology and as potential treatment for neurodegenerative diseases. Transl Neurodegener 4(1):22
Oscar AC (2008) Basic mechanisms of rTMS: implications in Parkinson’s disease. Int Arch Med 1(1):2
Colaianna M, Tucci P, Zotti M, Morgese MG, Schiavone S, Govoni S, Cuomo V, Trabace L (2010) Soluble βamyloid1–42: a critical player in producing behavioural and biochemical changes evoking depressive-related state? Br J Pharmacol 159(8):1704
Holsinger RM, Schnarr J, Henry P, Castelo VT, Fahnestock M (2000) Quantitation of BDNF mRNA in human parietal cortex by competitive reverse transcription-polymerase chain reaction: decreased levels in Alzheimer’s disease. Mol Brain Res 76(2):347–354
Parnetti L, Chiasserini D, Bellomo G, Giannandrea D, De CC, Qureshi MM, Ardah MT, Varghese S, Bonanni L, Borroni B (2011) Cerebrospinal fluid Tau/α-synuclein ratio in Parkinson’s disease and degenerative dementias. Mov Disord 26(8):1428–1435
Elahi B, Chen R (2010) Effect of transcranial magnetic stimulation on Parkinson motor function–systematic review of controlled clinical trials. Mov Disord 24(3):357–363
Zanjani A, Zakzanis KK, Daskalakis ZJ, Chen R (2015) Repetitive transcranial magnetic stimulation of the primary motor cortex in the treatment of motor signs in Parkinson’s disease: a quantitative review of the literature. Mov Disord 30(6):750–758
Nielsen NS, Jacobsen C (1997) Depression of motor cortex excitability by low-frequency transcranial magnetic stimulation. Neurology 48(5):1398–1403
Wagleshukla A, Angel MJ, Zadikoff C, Enjati M, Gunraj C, Lang AE, Chen R (2007) Low-frequency repetitive transcranial magnetic stimulation for treatment of levodopa-induced dyskinesias. Neurology 68(9):704–705
Acknowledgements
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors disclose no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
11010_2019_3531_MOESM1_ESM.tif
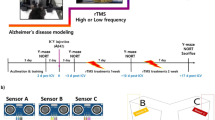
Supplementary material 1 (TIFF 83 kb) Figure S1. Schematic diagram of the experiment schedule. 10-week old mice were intracranially injected with 2 μl 6-OHDA (4 μg/μl) and housed routinely for 2 weeks before rTMS treatment of 2 weeks.
Rights and permissions
About this article

Cite this article
Ba, F., Zhou, Y., Zhou, J. et al. Repetitive transcranial magnetic stimulation protects mice against 6-OHDA-induced Parkinson’s disease symptoms by regulating brain amyloid β1–42 level. Mol Cell Biochem 458, 71–78 (2019). https://doi.org/10.1007/s11010-019-03531-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11010-019-03531-w