
Abstract
Migraine is a multifactorial disease with various factors, such as genetic polymorphisms and personality traits, but the contribution of those factors is not clear. To clarify the pathogenesis of migraine, the contributions of genetic polymorphisms and personality traits were simultaneously investigated using multivariate analysis. Ninety-one migraine patients and 119 non-headache healthy volunteers were enrolled. The 12 gene polymorphisms analysis and NEO-FFI personality test were performed. At first, the univariate analysis was performed to extract the contributing factors to pathogenesis of migraine. We then extracted the factors that independently contributed to the pathogenesis of migraine using multivariate stepwise logistic regression analysis. Using the multivariate analysis, three gene polymorphisms including monoamine oxidase A (MAOA) T941G, methylenetetrahydrofolate reductase (MTHFR) C677T, and tumor necrosis factor beta (TNF-β) G252Α, and the neuroticism and conscientiousness scores in NEO-FFI were selected as significant factors that independently contributed to the pathogenesis of migraine. Their odds ratios were 1.099 (per point of neuroticism score), 1.080 (per point of conscientiousness score), 2.272 (T and T/T or T/G vs G and G/G genotype of MAOA), 1.939 (C/T or T/T vs C/C genotype of MTHFR), and 2.748 (G/A or A/A vs G/G genotype of TNF-β), respectively. We suggested that multiple factors, such as gene polymorphisms and personality traits, contribute to the pathogenesis of migraine. The contribution of polymorphisms, such as MAOA T941G, MTHFR C677T, and TNF-β G252A, were more important than personality traits in the pathogenesis of migraine, a multifactorial disorder.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Migraine is the most common type of neurovascular headache. In Japan, approximately 8.4% of people experience migraine headaches [1], which are usually characterized by severe pain on one or both sides of the head and at times disturbed vision. Serotonin (5-hydroxytryptamine, 5-HT) is an important neurotransmitter that regulates brain vascular constriction, release of neurotransmitter, and platelet aggregation [2, 3]. Between attacks, migraine patients had lower plasma levels of 5-HT and higher plasma levels of 5-hydroxyindoleacetic acid (5-HIAA), a 5-HT metabolite, than controls and patients with a tension-type headache [4]. Nagata et al. [5] also suggested that plasma 5-HT levels during attack free-periods in patients with migraine with an aura (MA) were significantly lower than in controls and patients with a migraine without an aura (MO). Moreover, intravenous injection of 5-HT aborted reserpine-induced and spontaneous migraine headaches [6, 7]. Thus, 5-HT has an important role in the pathophysiology of migraine; therefore, genetic association studies have been performed on 5-HT-related gene polymorphisms by many investigators [8–15]. However, recent reports have suggested that the pathogenesis of migraine is related not only to 5-HT-related gene polymorphisms but also to 5-HT-unrelated gene polymorphisms, such as angiotensin-converting enzyme (ACE) [16], methylenetetrahydrofolate reductase (MTHFR) [17, 18], estrogen receptor 1 (ESR1) [19, 20], and tumor necrosis factor beta (TNF-β) [21].
Although migraine is a multifactorial disease, most previous studies have focused on the contribution of a single factor. Interestingly, Park et al. [14] investigated a harm avoidance personality dimension and polymorphisms in 5-HT transporter protein gene in MO patients, and reported that two factors, including the harm avoidance personality and a variable number of tandem repeats polymorphism within intron 2 (VNTR) of 5-HT transporter (5-HTTVNTR) independently contributed to MO patients. To clarify the pathogenesis of migraine, more genetic factors including 5-HT-related and 5-HT-unrelated gene polymorphisms and personality traits need to be analyzed simultaneously. In addition, migraine and psychiatric disorders are known to associate with the some of commonness personality traits [22] and genetic factors [23]. Therefore, to show independent factors for pathogenesis of migraine, it is very important to exclude subjects with depression and other co-morbid psychiatric disorders.
In this study, using subjects without depression and other co-morbid psychiatric disorders, we simultaneously analyzed the contributions of gene polymorphisms and personality traits in the pathogenesis of migraine, and extracted independent contributing factors by multivariate stepwise logistic regression analysis.
Methods
Subjects
We enrolled 91 Japanese migraine patients who were admitted to the Department of Neurology, Showa University Fujigaoka Rehabilitation Hospital, Kanagawa (Japan), Pain Clinic in Showa University East Hospital, Tokyo (Japan), and Neurosurgery Clinic/Institute, Tokyo (Japan), between June 2006 and December 2010. Migraine was diagnosed according to the international classification of headache disorders, 2nd edition (ICHD-II) in 2004 [24]. Ninety-one patients with migraine were divided into patients with migraine with aura (MA, n = 24), and without aura (MO, n = 67). Non-headache healthy volunteers comprised the control group (n = 119). Controls were matched for age and sex with patients and recruited in the same geographic areas. Moreover, controls were checked by interview to be healthy. We also confirmed it using the ID migraine screener Japanese version [25], which included a four-item (headache exacerbation in daily performance, nausea, photophobia, and osmophobia). Patients and controls with depression and other co-morbid psychiatric disorders were excluded by their history. All patients and controls were Japanese and gave their informed consent to this study.
The clinical study was approved by the Ethics Committee for Genome Research of Showa University.
NEO-FFI
Personality traits were assessed by the NEO Five-Factor Inventory (NEO-FFI) personality questionnaire, including neuroticism, extraversion, openness, agreeableness, and conscientiousness [26]. Scores are summed totals and have a range of 0–48 for each of five personality traits.
Genotyping
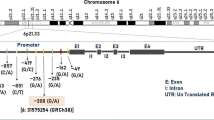
The gene polymorphisms of serotonin (5-HT) transporter 5-HTTLPR (NG_011747) [27] and 5-HTTVNTR (NG_011747) [28], 5-HT2A receptor T102C (rs6313) [29], 5-HT1B receptor G861C (rs6296) [30], monoamine oxidase A (MAOA) VNTR (NG_008957) [31, 32] and MAOA T941G (rs6323) [33], methylenetetrahydrofolate reductase (MTHFR) C677T (rs1801133) [34], angiotensin-converting enzyme (ACE) insertion/deletion (I/D) (NG_011648) [35], estrogen receptor 1 (ESR1) G325C (rs1801132) [36] and G594A (rs2228480) [37], dopamine receptor 2 (DRD2) C939T (rs6275) [38], and tumor necrosis factor-β (TNF-β) G252A (rs909253) [21] were studied. Genomic DNA was extracted from whole blood using NucleoSpin® Blood QuickPure (NIPPON Genetics Co., Ltd, Tokyo, Japan). The polymorphism of each gene was determined according to previous reports [21, 27–38]. Primer sequences, restriction enzymes, and expected fragment sizes of about 12 gene polymorphisms are shown in Table 1; Fig. 1.

PCR or PCR-restriction fragment length polymorphism (PCR–RFLP)-based genotyping of 5-HT-related and 5-HT-unrelated gene polymorphisms. PCR and digestion products were loaded on 3% agarose gel and stained with ethidium bromide (see Table 1)
The PCR products or restriction enzyme-treated PCR fragments with positive controls were run on 3% agarose gels and stained with ethidium bromide.
Statistical analysis
The genotype frequencies were tested using the public statistical web-tool http://www.oege.org/software/hwe-mr-calc.shtml for Hardy–Weinberg equilibrium (HWE). P > 0.05 was considered not deviate from the equilibrium. A power analysis was performed with the use of the Website (http://www.dssresearch.com/toolkit/spcalc/power_a1.asp). In this power analysis, we determined according to Cohen’s criteria [39] the following: small effect size of ≥0.2 and <0.5, and medium effect size of ≥0.5 and <0.8, and large effect size of ≥0.8, alpha = 5%. Results are expressed as mean ± SD. We applied univariate analysis using Student’s t-test for continuous variables, and χ2 test or Fisher’s exact test for categorical variables. Next, multivariate stepwise logistic regression analysis was performed to determine independent factors associated with the pathogenesis of migraine. Variables with P < 0.1 on univariate analysis were included in the multivariate model [40–42]. Odds ratio (OR) and its 95% confidence intervals (CI) were calculated to evaluate the effects of factors. Values of P < 0.05 were considered statistically significant. The analysis was performed using SPSS 11.0 J (SPSS, Tokyo, Japan).
Results
Characteristics of patients
The study population consisted of 91 migraine patients (age: 42.4 ± 10.2 years) including MA (n = 24) and MO (n = 67) (20 (22%) male and 71 (78%) female). One hundred and nineteen non-headache healthy Japanese controls (age: 40.7 ± 10.4 years) consisted of 31 (26%) men and 88 (74%) women. The migraine patients and healthy controls were age and sex matched.
Univariate analysis
Personality traits
As shown in Table 2, the neuroticism score was significantly higher in migraine patients (26.9 ± 8.0, P = 0.001) than in controls (23.4 ± 7.2). The conscientiousness score was higher in migraine patients (29.3 ± 6.6, P = 0.068) than in controls (27.7 ± 6.2). Extraversion, openness, and agreeableness scores were not different between migraine patients and controls.
In sub-group analysis, the neuroticism score was significantly higher in MA patients (28.6 ± 8.7, P = 0.002) and in MO patients (26.3 ± 7.8, P = 0.011) than in controls (23.4 ± 7.2). The extraversion score was lower in MA patients (21.3 ± 6.4, P = 0.052) than in controls (24.3 ± 7.0). The conscientiousness score was higher in MO patients (29.3 ± 6.4, P = 0.096) than controls (27.7 ± 6.2).
Gene polymorphisms
Table 3 shows the genotypic distributions in subjects. Only the genotype distribution of ESR1 G594A polymorphism was not consistent with HWE in controls (P < 0.001). It may be due to methodological reasons (e.g., non-population-based study and small sample size).
The genotypic distributions of MAOA T941G (T (male) plus T/T (female) plus T/G (female) vs G (male) plus G/G (female), P = 0.048), MTHFR C677T (C/C vs C/T plus T/T, P = 0.026), ACE I/D (I/I plus I/D vs D/D, P = 0.082), ESR1 G594A (G/G plus G/A vs A/A, P = 0.001), and TNF-β G252A (G/G vs G/A plus A/A, P = 0.074) were different between migraine patients and controls. On the other hand, no significant differences in genotypic distributions between migraine patients and controls were observed in the polymorphisms of 5-HTTLPR, 5-HTTVNTR, 5-HT2A T102C, 5-HT1B G861C, MAOAVNTR, ESR1 G325C, and DRD2 C939T.
In the results of sub-group analysis, between MA patients and controls, the genotypic distributions of 5-HTTLPR (s/s plus s/l plus s/xl vs l/l plus l/xl, P = 0.004), 5-HTTVNTR (12/12 vs 12/10 plus 12/9 plus 10/10, P = 0.029), 5-HT1B G861C (G/G vs G/C plus C/C, P = 0.040), MAOAVNTR (s (male) plus s/s (female) plus s/l (female) vs l (male) plus l/l (female), P = 0.077), ACE I/D (I/I plus I/D vs D/D; P = 0.025) and TNF-β G252A (G/G vs G/A plus A/A, P = 0.007) were different. Between MO patients and controls, the genotypic distributions of MAOA T941G (T (male) plus T/T (female) plus T/G (female) vs G (male) plus G/G (female), P = 0.068), MTHFR C677T (C/C vs C/T plus T/T, P = 0.008), and ESR1 G594A (G/G plus G/A vs A/A, P = 0.001) were different.
Multivariate analysis
The multivariate stepwise logistic regression was performed with neuroticism score, conscientiousness score, MAOA T941G, MTHFR C677T, ACE I/D and TNF-β G252A; and neuroticism score (P < 0.001), conscientiousness score (P = 0.004), MAOA T941G (P = 0.010), MTHFR C677T (P = 0.034), and TNF-β G252A (P = 0.027) were selected as significant factors that independently contributed to the pathogenesis of migraine. ESR1 G594A was excluded from multivariate analysis, because the genotype distribution of ESR1 G594A polymorphism was not consistent with HWE in controls. Table 4 lists each OR and 95% CI. The ORs (per unit increase) were 1.099 (95% CI = 1.050–1.149), 1.080 (95% CI = 1.025–1.139), 2.272 (95% CI = 1.215–4.250), 1.939 (95% CI = 1.051–3.576) and 2.748 (95% CI = 1.121–6.736).
Using an alpha error of 5%, post hoc analysis, for neuroticism score and conscientiousness score in personality traits, and for MAOA T941G, MTHFR C677T, and TNF-β G252A polymorphisms, showed that our sample size had the power of 0.91 (large), 0.43 (small), 0.48 (small), 0.61 (medium), and 0.49 (small), respectively.
Discussion
In this report not only gene polymorphisms but also personality traits are involved in the pathophysiology of migraine using multivariate stepwise logistic regression analysis. The personality traits, neuroticism and conscientiousness, and gene polymorphisms, such as MAOA T941G, MTHFR C677T, and TNF-β G252A, were selected as factors that independently contributed to the pathogenesis of migraine in Japanese population.
Previous reports have shown the association between migraine and neuroticism [22, 43]. The neuroticism score of NEO-FFI in this study was significantly high in migraine patients. The harm avoidance (HA) score in the Temperament and Character Inventory (TCI), another personality test, was elevated in migraine patients [14, 44]. Since the HA score is known to be correlated with the neuroticism score of NEO-FFI [45], neuroticism is an important personality trait in migraine. Moreover, in this study, we found for the first time that the conscientiousness is independently related with the pathogenesis of migraine. Thus, these personality traits including neuroticism and conscientiousness contributed to the pathogenesis of migraine.
The low level of plasma 5-HT seems to promote vasodilation, which is known to be one of the origins of headache. Oxidase deamination of 5-HT is known to be catalyzed by monoamine oxidase A (MAOA). MAOA is located on the X chromosome at Xp.11.3-Xp11.4 [46]. Several polymorphisms, including MAOA T941G and MAOAVNTR, have been identified in the MAOA coding sequence [31, 47]. Although the T941G polymorphism did not express the change in coding protein, it was reported to be significantly associated with low (T) and high (G) catalytic activity [31]. MAOA T941G polymorphism has been shown to be related with mood disorders, including major depressive or bipolar disorders [48]; however, we could not find a report showing the relation of MAOA T941G polymorphism in migraine. Hotamisligil and Breakfield [33] showed that MAOA activity is lower in T941 MAOA polymorphism than in G941 MAOA polymorphism. Our study was shown that G and G/G polymorphisms are higher in migraine patients than controls; therefore, it is possible that the plasma 5-HT levels in migraine patients, especially MO patients, are lower than in controls.
High plasma levels of homocysteine are related to a high risk for cardiovascular disease, cerebrovascular disease, and peripheral vascular disease [49, 50]. MTHFR is a key enzyme in homocysteine metabolism, catalyzing the production of 5-methylenetetrahydrofolate from 5,10-methylenetetrahydrofolate [51–53]. The T/T genotype of MTHFR C677T polymorphism, which changes an alanine to a valine residue in the catalytic domain, has been shown to decrease enzyme activity [53]. Moreover, the reduction of MTHFR leads to increased homocysteine levels [53]. In a Japanese study, Kowa et al. [17] reported that the T/T genotype of MTHFR is increased in MA patients. Moschiano et al. [54] suggested that homocysteine plasma levels were higher in MA patients than in healthy controls. Recent meta-analysis showed that the MTHFR T/T genotype may be a marker of MA [55]; however, a German study of 656 MA patients and 625 controls [56], and a Finnish study of 898 MA patients and 900 controls did not confirm an association [57]. On the other hand, Schurks et al. [18] suggested that the risk of MA is reduced among carriers of the T/T genotype of MTHFR C677T polymorphism. Oterino et al. [58] also reported that the genetic distribution of the C/C genotype of MTHFR C677T is higher in MO patients than in controls. In the present study, we found that the C/C genotype of MTHFR C677T may be one of the contributing factors of MO. Interestingly, the T/T genotype at MTHFR C677T polymorphism [59] is known to be a risk factor for depression. Since most previous studies did not exclude the subjects with depression and other co-morbid psychiatric disorders, it seems to be one of the reasons for the difference of results between previous studies and ours. MTHFR activities are known to be involved in the activity of dihydropteridine reductase [60], which has a key role in recycling tetrahydrobiopterin, a coenzyme for the rate-limiting enzymes of monoamine and nitric oxide (NO) biosynthesis [61]. Miwa et al. [62] reported that the increase of tetrahydrobiopterin content in the brain enhances 5-HT biosynthesis. Since plasma 5-HT levels during migraine attacks were substantially higher than during attack-free periods, it is possible that the reduction of activity in C/C carriers of MTHFR may stimulate not only the recycling of tetrahydrobiopterin but also 5-HT biosynthesis during migraine attacks. In C/C carriers of the MTHFR C677T polymorphism, vasocontraction and platelets aggregation, in response to 5-HT which is a major trigger of migraine may be stimulated.
This is the first report from Japan on genetic association of the G allele for TNF-β G252A polymorphism with migraine, especially MA. On the other hand, Trabace et al. [63] suggested that carrying the A allele for TNF-β G252A polymorphism is a risk factor for the development of MO, but not MA. Asuni et al. [21] also reported that the G allele for G252A TNF-β gene polymorphism is associated with MO. Ghosh et al. [64] showed that no association of TNF-β G252A polymorphism is determined between patients with migraine and controls. Since these researches were performed in Europe and India, racial differences may have caused this discrepancy. Interestingly, Abraham et al. [65] showed that the G allele is associated with higher TNF-α production in lymphoblastoid cell lines. On the other hand, the A/A genotype for TNF-β G252A polymorphism is known to be associated with higher TNF-α production [66]. Moreover, Messer et al. [67] reported that the A allele is related to increased TNF-β production. Thus, the association between TNF- β G252A polymorphism and TNF production is controversial. Cytokines are important mediators of inflammatory pathways, and the serum levels of cytokines such as TNF-α during attacks are higher than their levels upon outside attacks in patients with migraine [68]. Since the G252A polymorphism of TNF-β is a silent mutation, it can be stated that the TNF-β G252A gene polymorphism may have linkage disequilibrium with other functional mutations.
Genetic polymorphisms in the voltage-dependent P/Q-type Ca2+ channel alpha 1A subunit (CACNA1A) [69] and the alpha 2 subunit of the sodium/potassium pump (ATP1A2) caused migraine [70], and these familial hemiplegic migraines are rare. Almost all migraine types are caused by multifactorial factors, including genetic factors and environmental factors. In our study, by excluding the subjects with depression and other co-morbid psychiatric disorders, we could select purely many independent contributing factors, including personality traits and gene polymorphisms, to the pathogenesis of migraine using logistic regression analysis. However, because of small sample size, we did not have enough power for conscientiousness score, MAOA T941G and TNF-β G252A.
Although the sample size is the biggest limitation of the study, we could provide that the multiple factors, such as gene polymorphisms and personality traits, contribute to the pathogenesis of migraine. The contributions of polymorphisms, such as MAOA T941G, MTHFR C677T, and TNF-β G252A, seem to be more important than personality traits in the pathogenesis of migraine, a multifactorial disorder. Future studies are needed to collect more subjects and determine the pathogenesis of MA and MO, since the contributing factors differed between controls and MA or MO patients by univariate analysis.
References
Sakai F, Igarashi H (1997) Prevalence of migraine in Japan: a nationwide survey. Cephalalgia 17:15–22
Mohammad-Zadeh LF, Moses L, Gwaltney-Brant SM (2008) Serotonin: a review. J Vet Pharmacol Ther 31:187–199
Ishii M, Kobayashi S, Ohkura M et al (2009) Inhibitory effect of lomerizine, a prophylactic drug for migraines, on serotonin-induced contraction of the basilar artery. J Pharmacol Sci 111:221–225
Ferrari MD, Odink J, Tapparelli C et al (1989) Serotonin metabolism in migraine. Neurology 39:1239–1242
Nagata E, Shibata M, Hamada J et al (2006) Plasma 5-hydroxytryptamine (5-HT) in migraine during an attack-free period. Headache 46:592–596
Kimball RW, Friedman AP, Vallejo E (1960) Effect of serotonin in migraine patients. Neurology 10:107–111
Lance JW, Anthony M, Hinterberger H (1967) The control of cranial arteries by humoral mechanisms and its relation to the migraine syndrome. Headache 7:93–102
Nyholt DR, Curtain RP, Gaffney PT et al (1996) Migraine association and linkage analyses of the human 5-hydroxytryptamine (5-HT2A) receptor gene. Cephalalgia 16:463–467
Erdal ME, Herken H, Yilmaz M et al (2001) Association of the T102C polymorphism of 5-HT2A receptor gene with aura in migraine. J Neurol Sci 188:99–101
Yilmaz M, Erdal ME, Herken H et al (2001) Significance of serotonin transporter gene polymorphism in migraine. J Neurol Sci 186:27–30
Juhasz G, Zsombok T, Laszik A et al (2003) Association analysis of 5-HTTLPR variants, 5-HT2A receptor gene 102T/C polymorphism and migraine. J Neurogenet 17:231–240
Borroni B, Brambilla C, Liberini P et al (2005) Functional serotonin 5-HTTLPR polymorphism is a risk factor for migraine with aura. J Headache Pain 6:182–184
Marziniak M, Mössner R, Schmitt A et al (2005) A functional serotonin transporter gene polymorphism is associated with migraine with aura. Neurology 64:157–159
Park JW, Han SR, Yang DW et al (2006) Serotonin transporter protein polymorphism and harm avoidance personality in migraine without aura. Headache 46:991–996
Gonda X, Rihmer Z, Juhasz G et al (2007) High anxiety and migraine are associated with the s allele of the 5HTTLPR gene polymorphism. Psychiatry Res 149:261–266
Kowa H, Fusayasu E, Ijiri T et al (2005) Association of the insertion/deletion polymorphism of the angiotensin I-converting enzyme gene in patients of migraine with aura. Neurosci Lett 374:129–131
Kowa H, Yasui K, Takeshima T et al (2000) The homozygous C677T mutation in the methylenetetrahydrofolate reductase gene is a genetic risk factor for migraine. Am J Med Genet 96:762–764
Schurks M, Zee RY, Buring JE et al (2010) MTHFR 677C– > T and ACE D/I polymorphisms and migraine attack frequency in women. Cephalalgia 30:447–456
Colson NJ, Lea RA, Quinlan S et al (2004) The estrogen receptor 1 G594A polymorphism is associated with migraine susceptibility in two independent case/control groups. Neurogenetics 5:129–133
Oterino A, Pascual J, Ruiz de Alegría C et al (2006) Association of migraine and ESR1 G325C polymorphism. Neuroreport 17:61–64
Asuni C, Stochino ME, Cherchi A et al (2009) Migraine and tumour necrosis factor gene polymorphism. An association study in a Sardinian sample. J Neurol 256:194–197
Breslau N, Andreski P (1995) Migraine, personality, and psychiatric comorbidity. Headache 35:382–386
Moschiano F, D’Amico D, Canavero I et al (2011) Migraine and depression: common pathogenetic and therapeutic ground? Neurol Sci 32(suppl 1):S85–S88
Headache Classification Subcommittee of the International Headache Society (2004) The international classification of headache disorders: 2nd edition. Cephalalgia 24(suppl 1):9–160
Aiba S, Tatsumoto M, Saisu A et al (2010) Prevalence of typical migraine aura without headache in Japanese ophthalmology clinics. Cephalalgia 30:962–967
Costa PT Jr, McCrae RR (1992) Revised NEO personality inventory (NEO-PI-R) and NEO five-factor inventory (NEO-FFI) professional manual. Psychological Assessment Resources, Odessa
Murakami F, Shimomura T, Kotani K et al (1999) Anxiety traits associated with a polymorphism in the serotonin transporter gene regulatory region in the Japanese. J Hum Genet 44:15–17
Kaiser R, Muller-Oerlinghausen B, Filler D et al (2002) Correlation between serotonin uptake in human blood platelets with the 44-bp polymorphism and the 17-bp variable number of tandem repeat of the serotonin transporter. Am J Med Genet 114:323–328
Joober R, Benkelfat C, Brisebois K et al (1999) T102 polymorphism in the 5-HT2A gene and schizophrenia: relation to phenotype and drug response variability. J Psychiatry Neurosci 24:141–146
MaassenVanDenBrink A, Vergouwe MN, Ophoff RA et al (1998) 5-HT1B receptor polymorphism and clinical response to sumatriptan. Headache 38:288–291
Deckert J, Catalano M, Syagailo YV et al (1999) Excess of high activity monoamine oxidase a gene promoter alleles in female patients with panic disorder. Hum Mol Genet 8:621–624
Guo G, Ou XM, Roettger M et al (2008) The VNTR 2 repeat in MAOA and delinquent behavior in adolescence and young adulthood: associations and MAOA promoter activity. Eur J Hum Genet 16:626–634
Hotamisligil GS, Breakefield XO (1991) Human monoamine oxidase a gene determines levels of enzyme activity. Am J Hum Genet 49:383–392
Frosst P, Blom HJ, Milos R et al (1995) A candidate genetic risk factor for vascular disease: a common mutation in methylenetetrahydrofolate reductase. Nat Genet 10:111–113
Rigat B, Hubert C, Corvol P et al (1992) PCR detection of the insertion/deletion polymorphism of the human angiotensin converting enzyme gene (DCP1) (dipeptidyl carboxypeptidase 1). Nucleic Acids Res 20:1433
Colson NJ, Lea RA, Quinlan S et al (2006) No role for estrogen receptor 1 gene intron 1 Pvu II and exon 4 C325G polymorphisms in migraine susceptibility. BMC Med Genet 7:12
Curran JE, Lea RA, Rutherford S et al (2001) Association of estrogen receptor and glucocorticoid receptor gene polymorphisms with sporadic breast cancer. Int J Cancer 95:271–275
Sarkar G, Kapelner S, Grandy DK et al (1991) Direct sequencing of the dopamine D2 receptor (DRD2) in schizophrenic’s reveals three polymorphisms but no structural change in the receptor. Genomics 11:8–14
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associates, Hillsdale
Kimura K, Iguchi Y, Shibazaki K et al (2008) Hemorrhagic transformation of ischemic brain tissue after t-PA thrombolysis as detected by MRI may be asymptomatic, but impair neurological recovery. J Neurol Sci 272:136–142
Lee TC, Wang HP, Chiu HM et al (2010) Male gender and renal dysfunction are predictors of adverse outcome in nonpostoperative ischemic colitis patients. J Clin Gastroenterol 44:e96–e100
Ishii M, Sakairi Y, Hara H et al. (2011) Negative predictors of clinical response to triptans in patients with migraine. Neurol Sci. doi:10.1007/s10072-011-0716-z
Mattsson P, Ekselius L (2002) Migraine, major depression, panic disorder, and personality traits in women aged 40–74 years: a population-based study. Cephalalgia 22:543–551
Mongini F, Fassino S, Rota E et al (2005) The temperament and character inventory in women with migraine. J Headache Pain 6:247–249
Mikolajczyk E, Zietek J, Samochowiec A et al (2008) Personality dimensions measured using the temperament and character inventory (TCI) and NEO-FFI on a Polish sample. Int J Methods Psychiatr Res 17:210–219
Ozelius L, Hsu YP, Bruns G et al (1988) Human monoamine oxidase gene (MAOA): chromosome position (Xp21–p11) and DNA polymorphism. Genomics 3:53–58
Hinds HL, Hendriks RW, Craig IW et al (1992) Characterization of a highly polymorphic region near the first exon of the human MAOA gene containing a GT dinucleotide and a novel VNTR motif. Genomics 13:896–897
Fan M, Liu B, Jiang T et al (2010) Meta-analysis of the association between the monoamine oxidase-A gene and mood disorders. Psychiatr Genet 20:1–7
Taylor LM Jr, DeFrang RD, Harris EJ Jr et al (1991) The association of elevated plasma homocyst(e)ine with progression of symptomatic peripheral arterial disease. J Vasc Surg 13:128–136
Prasad K (1999) Homocysteine, a risk factor for cardiovascular disease. Int J Angiol 8:76–86
Blount BC, Mack MM, Wehr CM et al (1997) Folate deficiency causes uracil misincorporation into human DNA and chromosome breakage: implications for cancer and neuronal damage. Proc Natl Acad Sci USA 94:3290–3295
Duthie SJ, Narayanan S, Brand GM et al (2002) Impact of folate deficiency on DNA stability. J Nutr 132(suppl):2444S–2449S
de Bree A, Verschuren WM, Bjorke-Monsen AL et al (2003) Effect of the methylenetetrahydrofolate reductase 677C– > T mutation on the relations among folate intake and plasma folate and homocysteine concentrations in a general population sample. Am J Clin Nutr 77:687–693
Moschiano F, D’Amico D, Usai S et al (2008) Homocysteine plasma levels in patients with migraine with aura. Neurol Sci 29(suppl 1):S173–S175
Rubino E, Ferrero M, Rainero I et al (2009) Association of the C677T polymorphism in the MTHFR gene with migraine: a meta-analysis. Cephalalgia 29:818–825
Todt U, Freudenberg J, Goebel I et al (2006) MTHFR C677T polymorphism and migraine with aura. Ann Neurol 60:621–622
Kaunisto MA, Kallela M, Hamalainen E et al (2006) Testing of variants of the MTHFR and ESR1 genes in 1,798 Finnish individuals fails to confirm the association with migraine with aura. Cephalalgia 26:1462–1472
Oterino A, Toriello M, Valle N et al (2010) The relationship between homocysteine and genes of folate-related enzymes in migraine patients. Headache 50:99–168
Gilbody S, Lewis S, Lightfoot T (2007) Methylenetetrahydrofolate reductase (MTHFR) genetic polymorphisms and psychiatric disorders: a HuGE review. Am J Epidemiol 165:1–13
Miller AL (2008) The methylation, neurotransmitter, and antioxidant connections between folate and depression. Altern Med Rev 13:216–226
Koslow SH, Butler IJ (1977) Biogenic amine synthesis defect in dihydropteridine reductase deficiency. Science 198:522–523
Miwa S, Watanabe Y, Hayashi O (1985) 6R-L-erythro-5, 6, 7, 8-tetrahydrobiopterin as a regulator of dopamine and serotonin biosynthesis in the rat brain. Arch Biochem Biophys 239:234–241
Trabace S, Brioli G, Lulli P et al (2002) Tumor necrosis fator gene polymorphism in migraine. Headache 42:341–345
Ghosh J, Joshi G, Pradhan S et al (2010) Investigation of TNFA 308G > A and TNFB 252G > A polymorphisms in genetic susceptibility to migraine. J Neurol 257:898–904
Abraham LJ, French MA, Dawkins RL (1993) Polymorphic MHC ancestral haplotypes affect the activity of tumour necrosis factor-alpha. Clin Exp Immunol 92:14–18
Grimble RF, Howell WM, O’Reilly G et al (2002) The ability of fish oil to suppress tumor necrosis factor α production by peripheral blood mononuclear cells in healthy men is associated with polymorphisms in genes that influence tumor necrosis factor α production. Am J Clin Nutr 76:454–459
Messer G, Spengler U, Jung MC et al (1991) Polymorphic structure of the tumor necrosis factor (TNF) locus: an NcoI polymorphism in the first intron of the human TNF-β gene correlates with a variant amino acid in position 26 and a reduced level of TNF-β production. J Exp Med 173:209–219
Perini F, D’Andrea G, Galloni E et al (2005) Plasma cytokine levels in migraineurs and controls. Headache 45:926–931
Ophoff RA, Terwindt GM, Vergouwe MN et al (1996) Familial hemiplegic migraine and episodic ataxia type-2 are caused by mutations in the Ca2+ channel gene CACNL1A4. Cell 87:543–552
De Fusco M, Marconi R, Silvestri L et al (2003) Haploinsufficiency of ATP1A2 encoding the Na+/K+ pump α2 subunit associated with familial hemiplegic migraine type 2. Nat Genet 33:192–196
Acknowledgments
This study was supported in part by a grant of Private University High Technology Research Center Project matching fund subsidy from Ministry of Education, Culture, Sport, Science, and Technology, Japan (MEXT).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ishii, M., Shimizu, S., Sakairi, Y. et al. MAOA, MTHFR, and TNF-β genes polymorphisms and personality traits in the pathogenesis of migraine. Mol Cell Biochem 363, 357–366 (2012). https://doi.org/10.1007/s11010-011-1188-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11010-011-1188-4