
Abstract
Objectives
Racial and ethnic groups in the US exhibit major differences in low birthweight (LBW) rates. While previous studies have shown that community level social indicators associated with LBW vary by race and ethnicity, it is not known whether these differences exist among racial or ethnic groups who live in the same neighborhood or community. To address this question, we examined the association of community level features with LBW among African American, White and Hispanic women who live in similar geographic areas.
Methods
The analysis is based on geocoded birth certificates for all singleton live births in the year 2000 to women residing in 805 California ZIP codes. Community level social and demographic data were obtained from U.S. Census data files for the year 2000 and surrogate indices of population level alcohol and drug abuse and dependence were derived from hospital discharge data (HDD). Tobit and bootstrap analyses were used to test associations with birth outcomes, maternal characteristics, and community level social and demographic features within and across the three groups of women living in similar geographic areas.
Results
The results demonstrate major racial and ethnic differences in community level correlates of LBW. Rates of LBW among African Americans were lower if they lived in areas that were more densely populated, had greater income disparities, were more racially segregated, and had low rates of alcohol abuse or dependence. These associations were different or absent for Hispanic and White women.
Conclusions for Practice
The results suggest that despite living in the same areas, major differences in neighborhood features and social processes are linked to birth outcomes of African American women compared to Hispanic and White women. Further research, especially using multilevel approaches, is needed to precisely identify these differences to help reduce racial and ethnic disparities in LBW.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Significance
What is already known on this subject
Previous studies show that community correlates of LBW such as poverty and employment status differ among women in different ethnic or racial groups. However it is not known whether these factors affect LBW differently in racial and ethnic groups who live in the same geographic areas.
What this study adds
Tobit and bootstrap analyses indicated that very different community level correlates are related to LBW rates between racial and ethnic groups living in the same zip code areas in California. This is particularly true for African American women who showed considerably more differences in model coefficients when compared to both White and Hispanic women.
Background
Serious persistent racial and ethnic disparities in rates of low birthweight (LBW) exist in the US. In 2009, LBW rates were 13.6 % for African Americans, 7.2 % for Whites and 6.9 % for Hispanics [1]. LBW infants account for 69 % of all infant deaths [2] and are at increased risk of infant mortality, prolonged neonatal hospitalization, respiratory disease and poor neurodevelopmental outcomes [3]. Studies exploring determinants of disparities in LBW have mainly focused on individual factors such as maternal health and pregnancy status, and health behaviors [4–6]. Although individual-level risk factors are important correlates of LBW, they account for only a small fraction of the variance in LBW rates among African American and White women [5].
Recent studies have expanded explanations for disparities in LBW to include contextual and structural factors like neighborhood poverty, racial segregation, income disparities, social support and crime [7–9]. This research suggests that community correlates of LBW differ by race/ethnicity [11–13]. For instance, Pearl et al. [10] showed that neighborhood unemployment levels were positively related to LBW rates for Asian and African Americans, had little relationship for Whites, and were negatively related to LBW rates for foreign-born Hispanics.
While evidence from these studies suggests that community level correlates of LBW may differ between racial/ethnic groups, most existing data do not actually confirm these relationships for several reasons. First, the neighborhood environments of different racial and ethnic groups are sometimes so different that comparisons of community level structural factors and racial/ethnic background on differences in health outcomes are not meaningful. Second, the social meaning of community level characteristics like residential segregation can differ for racial and ethnic groups [13–15]. Third, statistical assessments of the correlates of health outcomes can be misleading. These kinds of analyses are prone to Type I errors due to large numbers of comparisons between ethnic groups (e.g., comparing effects between 3 groups across 10 covariates leads to 30 possible tests). In addition, claims about structural differences between groups are often based upon tests of significance of the relationship between LBW and social characteristics within particular groups when these tests should, instead, compare magnitudes of coefficient relationships between groups using structural tests. Thus, the fact that longer gestation periods are significantly related to lower risks for LBW in two groups does not ensure that these risks are the same between groups; in fact, they may be very different.
In this paper, we examine the relationship between community level characteristics and LBW among African American, White and Hispanic women residing in similar geographic areas in California to assess whether mothers of diverse ethnic groups are affected by similar environmental conditions in different ways. We draw on a sample of ZIP codes in California which allows comparisons of statistical relationships between neighborhood conditions and LBW rates across ethnic and racial groups, minimizes Type I errors through their control in testing procedures, and provides explicit structural tests of covariate effects between groups. In addition, we include novel community level indicators such as availability of retail stores and of alcohol stores, alcohol dependence and drug abuse that may affect rates of LBW [14, 16–21].
Methods
Electronic maps of California [22–24] were used to identify 1637 contiguous ZIP code polygon areas of the state with non-zero populations. ZIP code areas were the only coordinating area unit between the several data sources examined in these analyses. To ensure representation of the three ethnic groups in each area we selected 866 ZIP codes that had at least 200 residents. An additional 61 ZIP codes (7.0 %) were removed as outliers or due to incomplete data. This procedure yielded 805 areas of the state for analysis in which African, Hispanic and White American mothers jointly lived and worked.
Data Elements
The primary outcome was the number of singleton LBW births (weight < 2500 g) per 1000 singleton live births among African, Hispanic and White American mothers within each ZIP code of the state for the year 2000. Data on birthweight, gestational age and maternal characteristics were obtained from Public Use Birth Records provided by the California Department of Health Services and geolocated to ZIP code area.
Community level variables included in the analyses measuring socio-economic status, social stability, immigrant status, retail density and alcohol and drug dependency are described in Table 1. These measures were obtained from the Census 2000 Summary File 1, SF1, Census of Population and Housing [25] and Census CD 2000 Long Form Summary File 3, SF3 [24]. SF1 data were geocoded to internal points for each block; SF3 data were geocoded to internal points for each block group. Census blocks and block groups were spatially assigned to ZIP codes by matching internal block centroids. Using this procedure, 96.0 % of Census blocks and 93.8 % of Census block groups fell within the ZIP code polygons defined for the study. These blocks and block groups covered more than 98.3 % of the state’s population and were proper area subsets of the defined ZIP code areas (i.e., wholly contained within single ZIP code areas).
Definitions of race or ethnic group memberships were consistent across all data sources. African American and White American groups were defined exclusively, but Hispanic Americans were defined inclusively, including both African American and White American populations.
Statistical Approach
Descriptive statistics were calculated for all variables and measures included in the study. In addition, three parallel statistical analyses of ZIP code level on LBW rates among African American, Hispanic and White mothers were conducted using TOBIT censored linear regression models [26]. Each analysis provided a separate assessment of the significance of community level covariates related to LBW among mothers in each group. Rates of LBW were treated as zero censored (no negative values could be observed) and this information was used to statistically correct effects estimates for any excess of zeros naturally observed with respect to model covariates. The TOBIT regressions also provided a means of addressing small area effects through the use of appropriate sampling weights and a statistical control for heteroskedasticity related to differences in sizes of birth cohorts between ZIP codes (i.e., errors in estimate inversely proportional to numbers of births). Finally, since a few of the zip codes had small numbers of live births (e.g., 17 or 2.11 % with fewer than 50), we performed sensitivity analyses using areas with more than 50, 100, and 200 live births. With some reduction in power due to the loss of sample units, overall effects of the analyses remained the same as reported here.
Statistical tests of structural differences in correlates of LBW rates across racial or ethnic groups were computed using constraint tests that assessed the equivalence of results between groups [26]. Nonparametric bootstrap estimates [27] were then used to assess the statistical magnitudes of differences in coefficient estimates between groups. One thousand bootstrap samples of ZIP code areas were drawn with replacement, TOBIT models for each sample and racial or ethnic group were estimated, and differences between effects estimates computed. Effects sizes were calculated as the average difference in coefficient estimates across bootstraps divided by their standard deviation, with p values referred to a Gaussian normal distribution. In each case, positive values indicate greater impacts in the first relative to the second group and negative values indicate greater impacts in the second relative to the first group. In all cases effect size estimates correct for effects related to all other covariates in the analysis models. The distributions of differences between coefficient estimates were used to estimate the extent to which specific coefficients differed between groups. The statistical effects observed within group-specific models (e.g., an insignificant effect relating poverty to LBW in one racial or ethnic group vs. a significant effect relating poverty to LBW rates in another) may or may not correspond to significant differences in coefficient estimates between models.
Results
Table 2 presents unweighted descriptive statistics for the measures in the study showing large variations in measures across ZIP codes for all race/ethnic groups. Population densities ranged widely across ZIP codes, from a minimum of 0.13 persons per roadway mile (among African Americans) to a maximum of 1884.59 per roadway mile (among Hispanics). Percent of households in poverty ranged from 0.00 % for all three groups to a high of 82 % among African Americans. Median household incomes were greatest among Whites, but with some areas having populations with median incomes well in excess of $100,000 for all race/ethnic groups. High school graduation rates similarly overlapped across racial/ethnic groups. Rates of hospital discharges of patients with drug dependence or alcohol abuse were highest among African Americans, followed by Whites and were lowest among Hispanics.
Showing similar range and variation across ZIP codes, the measure of persons who changed households in the past 5 years ranged by a factor of about 3, the percent of vacant housing ranged by a factor of about 52, and percent foreign born residents by a factor of about 29. The index of concentrated extremes ranged from a minimum of −76.93 (concentrated poverty) to +82.70 (concentrated wealth). The measure of segregation was greatest on average among African Americans, but varied substantially across ZIP codes for all racial/ethnic groups. In addition, densities of retail stores and all alcohol outlets as well as proportions of on-premise alcohol outlets and bars also exhibited large ranges across ZIP codes.
Finally, white mothers were somewhat older than African American and Hispanic mothers, tended to have somewhat longer gestation periods, and had a lower proportion of Caesarian births than African American mothers.
Table 3 shows the beta coefficients, z-scores and p values (p < 0.05 one-tailed test) for the associations between the covariates and LBW rates from the censored regression models for each of the three groups. The upper portion of the table presents effects related to birth characteristics and other variables that were measured specific to each group (e.g., poverty rates among African Americans). The middle portion of the table presents effects related to variables commonly measured across groups (e.g., vacant housing). The lower portion of the table provides statistical information relevant to each model. Focusing on this aspect of the table first, the estimated standard deviations of errors from the censored regression models show that LBW rates varied most among African Americans and was 4–6 times greater than variation among Whites or Hispanics. As expected, heteroskedasticity was negatively related to the size of each birth cohort. Each model accounted for a significant portion of the variance in birth rates across ZIP codes (likelihood ratio χ2 tests), performing least well with respect to Hispanic LBW births (pseudo-R2 values, [28]).
Only two community level variables were significant and consistently related to LBW rates across two groups. Living in areas with greater vacant housing was related to greater rates of LBW for African American and Hispanic mothers and living in areas with higher densities of retail stores was related to greater LBW rates among White and African American mothers. Overall, correlates of LBW rates differed substantially for women from different racial/ethnic backgrounds.
Structural Disparities
If common biological, behavioral and social mechanisms were responsible for the statistical patterns observed in this study, then the signs and effect sizes observed in Table 3 should be similar across racial or ethnic groups. The effects reported in Table 3 may be interpreted to provide a rough guide to differences between groups but test the wrong counterfactual. Each effect may or may not be statistically different from zero within groups irrespective of differences in effect size between groups. Thus, the proper null hypothesis for testing structural disparities between racial/ethnic groups is that effects are of the same magnitude and sign between groups and that the differences in effect sizes are zero. Since constraint tests, indicated very substantive differences in coefficient vectors between groups (the smallest constraint test was between Hispanic and African American models, G2 = 775.38, p < 0.001), further exploration of the sources of these differences was done using nonparametric bootstrap methods.
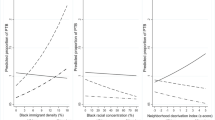
Figure 1 shows the results of the bootstrap analyses. Each of the three separate bar plots show, from left to right, African American minus Hispanic estimates, Hispanic minus White estimates, and African American minus White estimates. Significant differences were found in the community correlates of White, African American and Hispanic LBW rates. The first bar chart shows that African American and Hispanic LBW rates significantly (p < 0.005) differed in effects related to gestational age, population density, proportion of foreign born, income extremes, and segregation; each of these characteristics was associated with lower rates of LBW among African Americans. Greater alcohol abuse and dependence in a community was related to greater rates of LBW among African American versus Hispanic mothers (p < 0.050).

Standardized differences in coefficient estimates between groups. Black p < 0.005, Grey p < 0.050, White ns
The second bar chart shows that Hispanic and White LBW rates differed (p < 0.005) significantly with respect to the impacts of poverty and vacant housing. In addition, greater maternal age and gestational age were positively related to LBW among White versus Hispanic mothers (p < 0.050).
The third bar chart shows that African American and White LBW rates significantly (p < 0.005) differed with respect to the impacts of gestational age, population density, alcohol dependence, income extremes and segregation. Living in communities with greater amounts of vacant housing and smaller proportions of foreign-born populations were related to greater rates of LBW among African American versus White mothers (p < 0.050).
Comparing the results obtained within race/ethnic groups reported in Table 2 with those observed between race/ethnic groups in Fig. 1, we get a more complete picture of the heterogeneity of community level effects across groups of women. For example, both income extremes and residential segregation are related to lower rates of LBW rates among African American mothers when compared to White mothers (Fig. 1), but these effects are negligible among Hispanic and White women (Table 2). Similarly, measures of social disorganization, such as vacant housing, are related to greater levels of LBW rates among African American and Hispanic mothers (Fig. 1) and negligibly so among White mothers (Table 2), with greatest relative effects among Hispanics (Fig. 1). Greater levels of poverty are related to greater rates of LBW among White mothers (Table 1) with greatest differential impacts on LBW rates between Hispanic and White mothers (Fig. 1).
Supplementary analyses compared the same models for foreign versus US born women within each racial or ethnic group and found no statistically significant differences (data not shown). Sensitivity analyses further examined whether the relationships between community-level factors and LBW rates changed when adding preterm births (less than 37 weeks gestation) as a covariate in the models. As expected, preterm births were a significant correlate of low birth weight births in each group but did not substantively alter either the significance or effect size of the community-level variables within or between groups.
Discussion
Our study demonstrates that markedly different community level correlates (e.g., population density, economic disparity, poverty, residential segregation, population density, vacant housing and alcohol dependence) are related to LBW rates in racial/ethnic groups living in the same ZIP code areas in California.
African American women in particular showed considerably more differences when compared to both White and Hispanic women. Notably rates of LBW were lower in high density communities where African Americans lived compared with similar communities where Hispanc and White mothers resided, a finding that has not been reported in previous studies in the US. The strong association of high population density (urban areas) with decreasing risk of LBW for African American women might be explained by better access to health care and to material resources which may result in lower stress levels than among women living in more remote areas [29, 30]. In addition behavioral risks for LBW such as smoking have been shown to be lower for women living in metropolitan versus rural areas in some countries [29].
Living in communities with greater income extremes is related to lower rates of LBW among African American mothers but not among Whites and Hispanics. The finding for African Americans is consistent with literature suggesting that families living in mixed economic areas benefit both from exposure to affluent residents, and from the presence of services and institutions aimed at assisting lower-income residents [31], but contradict neighborhood, state or national analyses showing that rates of low birth weight are generally higher in areas with high levels of income inequality (see [32–35]). These inconsistent results may be due to the size and composition of the units of analysis involved, residual confounding from unmeasured variables or to differences in populations sampled.
Although residential segregation has been shown to be positively related to low birth weight after controlling for poverty in metropolitan areas across the US [36] and in New York City [37], our findings show that African American, but not White or Hispanic women living in segregated areas have significantly lower rates of LBW infants. This finding parallels growing evidence of the benefits of high levels of racial group density on health conditions for African Americans [9, 38] and with research showing that racial segregation was not associated with LBW for Hispanic women [13]. In addition, other research has shown that living in immigrant enclaves is associated with lower rates of LBW among Mexican born women [39].
In our study, community level poverty was a negligible correlate for LBW rates among minority women, but a significant one for rates among White women. The findings for Hispanic women are consistent with the results of other research showing that poverty is weakly or not associated with increased rates of LBW, especially for foreign-born women [29, 40, 41].
The finding that birth weights of White mothers in our study were more affected by poverty than those for African American women contradicts previous studies, which generally indicate a reversal of these associations [10, 12, 30, 42]. These divergent findings could stem from differences in analytic units (e.g., census tracts vs. ZIP codes) used, ethnic/racial composition of areas studied and analysis strategies employed or from unmeasured residual confounding. An important feature of this study was identifying common areas of the state across which racial/ethnic group-specific rates of LBW could be compared and where substantial populations of all three racial and ethnic groups reside. This approach may illuminate different relationships to community level socio-economic status than when racial groups are compared across vastly different, and potentially more economically polarized environments. In addition, the use of structural comparison models enable us to make more rigorous comparisons about socio-economic differences between groups than other approaches that rely on examining differences in effect sizes of variables within specific ethnic or racial groups.
Minority women, especially Hispanics differed from White women in exhibiting strong positive, relationships between community levels of vacant housing and high rates of LBW. The findings for minority women are similar to previous studies showing the negative impact of neighborhood disorganization on stress levels and health status [43, 44]. However, relative to whites, African American birth weights have been shown to improve by living in neighborhoods with higher numbers of foreign-born residents which could be attributed to the low crime rates, high levels of collective efficacy and social connectedness; and access to businesses and services described for these areas in some studies [36, 45].
Rates of alcohol abuse/dependence were associated with low birth weight only among African American mothers in contrast to other women, especially Whites. Although prior studies have shown adverse effects of maternal drug and alcohol use on birth weight [16, 46], no other studies to our knowledge have described the negative impact of community level alcohol abuse on low birth weight. High rates of community level alcohol abuse/dependence could be linked with LBW by indicating that African American women residing in these areas are more likely to be problem or excessive drinkers; or that these neighborhoods are characterized by high rates of public drinking and drunkenness associated with blight, neighborhood deterioration and low levels of social integration and support—factors which are known to constitute sources of chronic stress [47, 48].
Limitations
Our study has three substantial limitations. First, the models do not include a full range of variables that determine birth outcomes, therefore there is considerable unmeasured residual confounding, especially at the individual-level. Second, the observed ecological correlations may arise from population-level social processes which result in specific disadvantages to racial or ethnic groups (e.g., violent crime rates). Third, the spatial units may be too aggregate to ensure common exposures between racial or ethnic groups to population risks. Small cities and communities of less than 100,000 persons are often represented by a single ZIP code and among larger cities in the state, ZIP code areas only crudely represent neighborhood environments. Smaller geographic units would be preferable, but using current data sources, plausible strategies to disaggregate ZIP code level measures to smaller units introduce other sources of measurement bias. For example, one plausible strategy would be to use smaller geographic units and impute values to those units using geographic overlays and map algebras. However, the degree to which aggregation or disaggregation biases might arise in such imputations (e.g., from ZIP codes to Census tracts) is unknown and would induce unknown biases into the results of this study.
Despite these limitations, the study exhibits several important strengths. First, the study examined the impact of a wide array of important community level factors on LBW rates. Second, the ZIP code areas included in the analysis were unique in that they generally included enough births by mothers from each ethnic or racial group to enable direct comparisons of correlates of birth outcomes between groups while errors in estimation due to small area effects and heteroskedasticity were statistically controlled and the potentially biasing impacts of areas with small populations and few births were minimized. Thus, the sample and methods provide a reasonable approach to comparing associations between groups using community level data and minimize Type I errors and provide explicit structural tests of covariate effects between groups. In addition, the results increase understanding of the way in which community level factors impact adverse birth outcomes in three different racial or ethnic groups. For example, the results suggest that very different community-level variables are linked to birth outcomes of African American women compared to Hispanic and White women when they live in roughly contiguous areas. Further research, especially using multilevel approaches using more current data, is needed to precisely identify these differences to help close the gap in health disparities in rates of LBW and to examine the relationship between community-level variables and other birth outcomes such as preterm delivery.
References
U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau. (2011). Child Health USA 2011. Rockville, MD: U.S. Department of Health and Human Services.
Mathews, T. J., & MacDorman, M. F. (2006). Infant mortality statistics from the 2003 period linked birth/infant death data set. National Vital Statistics Reports, 54(16), 1–29.
Reyes, L., & Manalich, R. (2005). Long-term consequences of low birth weight. Kidney International. Supplement, 97, S107–S111.
Goldenberg, R. L., Cliver, S. P., Mulvihill, F. X., Hickey, C. A., Hoffman, H. J., Klerman, L. V., et al. (1996). Medical, psychosocial, and behavioral risk factors do not explain the increased risk for low birth weight among black women. American Journal of Obstetrics and Gynecology, 175(5), 1317–1324.
Lu, M. C., & Halfon, N. (2003). Racial and ethnic disparities in birth outcomes: A life-course perspective. Maternal and Child Health Journal, 7(1), 13–30.
Giscombe, C. L., & Lobel, M. (2005). Explaining disproportionately high rates of adverse birth outcomes among African Americans: The impact of stress, racism, and related factors in pregnancy. Psychological Bulletin, 131(5), 662–683.
Diez Roux AV. (2001). Investigating neighborhood and area effects on health. American Journal of Public Health, 91(11), 1783–1789.
Sellstrom, E., & Bremberg, S. (2006). The significance of neighbourhood context to child and adolescent health and well-being: A systematic refiew of multilevel studies. Scandinavian Journal of Public Health, 34, 544–554.
Pickett, K. E., Collins, J. W., Masi, C. M., & Wilkinson, R. G. (2005). The effects of racial density and income incongruity on pregnancy outcomes. Social Science and Medicine, 60(10), 2229–2238.
Pearl, M., Braveman, P., & Abrams, B. (2001). The relationship of neighborhood socioeconomic characteristics to birthweight among 5 ethnic groups in California. American Journal of Public Health, 91(11), 1808–1814.
Messer, L. C., Kaufman, J. S., Dole, N., Savitz, D. A., & Laraia, B. A. (2006). Neighborhood crime, deprivation, and preterm birth. Annals of Epidemiology, 16(6), 455–462.
Buka, S. L., Brennan, R. T., Rich-Edwards, J. W., Raudenbush, S. W., & Earls, F. (2003). Neighborhood support and the birth weight of urban infants. American Journal of Epidemiology, 157(1), 1–8.
Walton, E. (2009). Residential segregation and birth weight among racial and ethnic minorities in the United States. Journal of Health and Social Behavior, 50(4), 427–442.
White, K., & Borrell, L. N. (2011). Racial/ethnic residential segregation: Framing the context of health risk and health disparities. Health Place, 17(2), 438–448.
Kramer, M. R., & Hogue, C. R. (2009). Is segregation bad for your health? Epidemiologic Review, 31, 178–194.
Visscher, W. A., Feder, M., Burns, A. M., Brady, T. M., & Bray, R. M. (2003). The impact of smoking and other substance use by urban women on the birthweight of their infants. Substance Use and Misuse, 38(8), 1063–1093.
Zambrana, R. E., Dunkel-Schetter, C., Collins, N. L., & Scrimshaw, S. C. (1999). Mediators of ethnic-associated differences in infant birth weight. Journal of Urban Health, 76(1), 102–116.
Noble, A., Vega, W. A., Kolody, B., Porter, P., Hwang, J., Merk, G. A., & Bole, A. (1997). Prenatal substance abuse in California: Findings from the perinatal substance exposure study. Journal of Psychoactive Drugs, 29(1), 43–53.
Scribner, R. A., Cohen, D. A., & Fisher, W. (2000). Evidence of a structural effect for alcohol outlet density: A multilevel analysis. Alcoholism, Clinical and Experimental Research, 24(2), 188–195.
Scribner, R. A., MacKinnon, D. P., & Dwyer, J. H. (1995). The risk of assaultive violence and alcohol availability in Los Angeles County. American Journal of Public Health, 85(3), 335–340.
Scribner, R. A., Cohen, D. A., & Farley, T. A. (1998). A geographic relation between alcohol availibility and gonorrhea rates. Sexually Transmitted Diseases, 25(10), 544–548.
Environmental Systems Research Institute. (2000). ESRI data and maps. Redlands, CA: Environmental Systems Research Institute.
Environmental Systems Research Institute. (2002). ESRI data and maps. Redlands, CA: Environmental Systems Research Institute.
GeoLytics I. (2002). CensusCD 2000 long form summary file 3, SF3. East Brunswick, NJ: GeoLytics, Inc.
U.S. Census Bureau, Census 2000 Summary File 1: Census of Population and Housing. DVD issued September 2001 (V1-D00-S1AS-08-US1), U.S. Department of Commerce Economics and Statistics Administration, Washington, DC, 2001.
Greene, W. H. (1993). Econometric analysis. New York: MacMillan.
Efron, B., & Tibshirani, R. J. (1993). An introduction to the bootstrap. New York: Chapman & Hall.
Maddala, G. S. (1983). Limited-dependent and qualitative variables in econometrics. New York: Cambridge University Press.
Auger, N., Autheri, M., Martinez, J., & Daniel, M. (2009). The association between rural-urban continuum, maternal education and adverse birth outcomes in Québec, Canada. The Journal of Rural Health, 25(4), 342–351.
Burns, L., Black, E., Powers, J. R., Loxton, D., Elliott, E., Shakeshaft, A., & Dunlop, A. (2011). Geographic and maternal characteristics associated with alcohol use in pregnancy. Alcoholism, Clinical and Experimental Research, 35(7), 1230–1237.
Carpiano, R. M., Lloyd, J. E., & Hertzman, C. (2009). Concentrated affluence, concentrated disadvantage, and children’s readiness for school: A population-based, multi-level investigation. Social Science and Medicine, 69(3), 420–432.
Kaplan, G. A., Pamuk, E. R., Lynch, J. W., & Cohen, R. D. (1996). Inequality in income and mortality in the United States: Analysis of mortality and potential pathways. British Medical Journal, 312(7037), 999.
Lynch, J., Smith, G. D., Hillemeier, M., Shaw, M., Raghunathan, T., & Kaplan, G. (2001). Income inequality, the psychosocial environment, and health: Comparisons of wealthy nations. Lancet, 358(9277), 194–200.
Muntaner, C., Lynch, J. W., Hillemeier, M., Lee, J. H., David, R., Benach, J., & Borrell, C. (2002). Economic inequality, working-class power, social capital, and cause-specific mortality in wealthy countries. International Journal of Health Services, 32(4), 629–656.
Nkansah-Amankra, S., Dhawain, A., Hussey, J. R., & Luchok, K. J. (2010). Maternal social support and neighborhood income inequality as predictors of low birth weight and preterm birth outcome disparities: Analysis of south Carolina pregnancy risk assessment and monitoring system survey, 2000–2003. Maternal and Child Health Journal, 14(5), 774–785.
Polednak, A. P. (1996). Trends in US urban black infant mortality, by degree of residential segregation. American Journal of Public Health, 86(5), 723–726.
Grady, S. C. (2006). Racial disparities in low birthweight and the contribution of residential segregation: A multilevel analysis. Social Science and Medicine, 63(12), 3013–3029.
Vinikoor, L. C., Kaufman, J. S., MacLehose, R. F., & Laraia, B. A. (2008). Effects of racial density and income incongruity on pregnancy outcomes in less segregated communities. Social Science and Medicine, 66, 255–259.
Osypuk, T., Schmidt, N. M., Baates, L. M., Tchetgen, E. J., Earls, F. J., & Glymor, M. M. (2010). Another Mexican birthweight paradox? The role of residential enclaves and neighborhood poverty in the birthweight of Mexican origin infants. Social Science and Medicine, 70(4), 550–560.
Pearl, M., Braveman, P., & Abrams, B. (2001). The relationship of neighborhood socioeconomic characteristics to birthweight among 5 ethnic groups in California. American Journal of Public Health, 91(11), 1808–1814.
Collins, J. W, Jr, & Shay, D. K. (1994). Prevalence of low birth weight among Hispanic infants with United States-born and foreign-born mothers: The effect of urban poverty. American Journal of Epidemiology, 139(2), 184–192.
Rauh, V. A., Andrews, H. F., & Garfinkel, R. S. (2001). The contribution of maternal age to racial disparities in birthweight: A multilevel perspective. American Journal of Public Health, 91(11), 1815–1824.
Ouyang, R. (2009). There goes the neighborhood: The relationship between the built environment and birth weight in central Durham, NC. Durham, NC: Duke University.
Schulz, A. J., Zenk, S. N., Israel, B. A., Mentz, G., Stokes, C., & Galea, S. (2008). Do neighborhood economic characteristics, racial composition, and residential stability predict perceptions of stress associated with the physical and social environment? Findings from a multilevel analysis in Detroit. Journal of Urban Health, 85(5), 642–661.
Wilson, W. J. (1996). When work disappears: The world of the new urban poor. New York: Random House.
Zambrana, R. E., Dunkel-Schetter, C., Collins, N. L., & Scrimshaw, S. C. (1999). Mediators of ethnic-associated differences in infant birth weight. Journal of Urban Health, 76(1), 102–116.
Cutrona, C. E., Wallace, G., & Wesner, K. A. (2006). Neighborhood characteristics and depression. Current Directions in Psychological Science, 15(4), 188–192.
Steptoe, A., & Feldman, P. J. (2001). Neighborhood problems as sources of chronic stress: Development of a measure of neighborhood problems, and associations with socioeconomic status and health. Annals of Behavioral Medicine, 23(3), 177–185.
Acknowledgments
Research for and preparation of this manuscript were supported by a UC Berkeley Research Futures Grant Program Award and National Institute on Alcohol Abuse and Alcoholism Center Grant No. P60-AA06282 and research Grant R37-AA12927. Thanks to Evan Sicuranza, Angela Ni, Sami Newlan, and Zayn Karssli for bibliographic and manuscript preparation support.
Conflict of interest
The authors declare they have no competing of interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Herd, D., Gruenewald, P., Remer, L. et al. Community Level Correlates of Low Birthweight Among African American, Hispanic and White Women in California. Matern Child Health J 19, 2251–2260 (2015). https://doi.org/10.1007/s10995-015-1744-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-015-1744-8