
Abstract
The adverse consequences of postpartum depression on the health of the mother and her child are well documented. However, there is little information on postpartum depression among mothers with disabilities. This study examines the patterns of depression and depressive symptoms before, during and after pregnancy and the association between depression before and during pregnancy and postpartum depression symptomatology (PPD) among women with and without disabilities. Data from the 2009–2011 Rhode Island Pregnancy Risk Assessment Monitoring System (PRAMS) were analyzed in 2013. Almost 30 % (28.9 %; 95 % CI 22.8–35.8) of mothers with disabilities reported often or always feeling down, depressed or sad after childbirth compared to 10 % of those without disabilities (95 % CI 8.9–11.3). Compared to other women in the study, women with disabilities had a greater likelihood for PPD symptoms (RR 1.6, 95 % CI 1.1–2.2) after accounting for sociodemographics, maternal characteristics related to PPD, and depression before and during pregnancy. Adjusting for other covariates, self-reported prenatal diagnosis of depression was not associated with symptoms of PPD and depression during pregnancy was marginally associated with PPD symptomatology for women with disabilities. Women with disabilities are at a greater risk of experiencing symptoms of postpartum depression than other women. Screening for PPD among new mothers with disabilities and timely referral of those with PPD diagnosis are vital to the health of mothers with disabilities and their children.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Increasing numbers of women with disabilities are choosing to become pregnant and bear children [1, 2]. A recent analysis of National Health Interview Survey data found that 2 % of US women with chronic physical disabilities between 18 and 49 years of age are currently pregnant [3]. Although more women with disabilities are having children, there is little systematic information on the experience of women with disabilities before, during and after childbirth [1, 4]. Nonetheless, anecdotal evidence and several studies suggest that women with disabilities have higher risks for various complications during pregnancy and are more likely to have adverse pregnancy outcomes [5–7]. However, little information is available about the likelihood of one particularly serious outcome—postpartum depression—among women with disabilities who give birth.
The association between disability and depression is well documented. Persons with disabilities are more likely than those without disabilities to report depression and depressive symptoms [8–12]. Approximately 37 % of people with disabilities reported lifetime depression compared to 11 % of those without disabilities [13]. Compared to women in the general population, women with disabilities are at a greater risk for depression [14]. Among women with disabilities, 42 % reported ever having been depressed compared to 14 % of those without disabilities [13]. However, an important question is whether experiencing depression at other times in life is associated with higher rates of postpartum depression among women with disabilities.
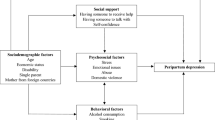
Postpartum depression (PPD) is a serious mental health condition affecting approximately 12–20 % of US mothers [15]. PPD can have severe consequences, affecting the health and well-being of the mother and her child [16]. It can impair maternal–infant bonding, leading to attachment insecurity and developmental delays in children [17–22]. Studies have also shown that children affected by mothers who experience PPD are more likely to develop behavioral problems over time [19]. Women who experience PPD are also more likely to experience future episodes of depression [18]. Risk factors for PPD include personal or family history of depression, history of maltreatment, childhood sexual and physical abuse, very young maternal age (adolescence), low income, limited social supports, poor relationship with partner, urban residence, history of preterm births, and maternal and partner substance abuse [23–28]. Women from racial and ethnic minority groups and immigrant women are also at higher risk for postpartum depression [29]. Despite the extensive research on PPD, the effects of disability on PPD incidence have received little study.
The purpose of this study is to explore patterns of depression among women with and without disabilities who have given birth. In addition to examining depression before and during pregnancy, we focus specifically on PPD symptomatology and ask how depression before and during pregnancy affect the likelihood of PPD symptomatology for women with and without disabilities. We use a unique population-based data set that contains considerable information on the attributes and pregnancy experiences of women in Rhode Island who recently gave birth, the Pregnancy Risk Assessment Monitoring System (PRAMS) survey [30, 31]. We address the following research questions:
-
1.
What are the patterns of depression and depressive symptoms of women with and without disabilities before, during, and after pregnancy?
-
2.
What factors are associated with PPD symptomatology for women with and without disabilities?
-
3.
How do patterns of depression/depressive symptoms and postpartum depressive symptomatology associations differ for women with versus without disabilities?
This study is the first of which we are aware to examine the incidence of PPD among women with disabilities. Furthermore, it is the first to look at how depression-related experiences at other time points are associated with PPD for women with disabilities.
Methods
Data Source
We studied data from the 2009 to 2011 Rhode Island Pregnancy Risk Assessment Monitoring System (PRAMS). The PRAMS is a population-based surveillance system that collects state-specific data on maternal attitudes and experiences before, during, and shortly after pregnancy. Survey participants were sampled from a frame of eligible birth certificates that included all live-born infants born to RI-resident women [30, 31]. Selected women are first contacted by mail and those not responding to repeated mailings are contacted and interviewed by telephone. The survey is conducted in English and Spanish.
The RI PRAMS data include information collected from the birth certificate and the maternal survey. The birth certificate serves as the source for demographic and clinical information about the mother and her infant; the RI PRAMS questionnaire serves as the principal source for maternal behavioral information for the time before, during and after her most recent pregnancy.
Rhode Island implemented PRAMS in 2002 and is one of 40 states that conduct the survey. Each month about 165 RI women who recently gave birth are randomly chosen to receive the survey. The RI PRAMS surveys all mothers who deliver a low-birth weight infant and over-samples births occurring in the cities of Central Falls, Newport, Pawtucket, Providence, West Warwick and Woonsocket. About 2,000 or more than 15 % of recent mothers are selected to participate in the PRAMS each year in RI.
Rhode Island is one of only two states that include a disability screener in their PRAMS surveys. For this study we included data from the RI PRAMS because it includes a disability screener and also detailed questions on depression before, during and after pregnancy. We combined 3 years of data from the RI-PRAMS (2009–2011) in order to get an effective sample size of recent mothers with disabilities.
From 2009 to 2011, 5,582 Rhode Island women were sampled and the weighted response rates were 71.4 % in 2009, 68.0 % in 2010 and 69.2 % in 2011. Details about the purpose, sampling methods, and data collection of the PRAMS methodology are available elsewhere [13, 31]. Our analysis has been approved by University of Massachusetts Medical School Institutional Review Board.
Disability and Depression Measures
We used responses to the following RI PRAMS question to determine disability status: “Are you limited in any way in any activities because of physical, mental, or emotional problems?” The RI PRAMS included several questions on depression before, during and after pregnancy. Women were asked whether they were diagnosed with depression before and during their most recent pregnancy. Respondents were asked whether they had visited a health care provider during the 12 months before their pregnancy for depression or anxiety.
Those who responded to having been diagnosed with depression during their pregnancy were asked whether they had taken prescription medication and they had gone for counseling during their last pregnancy. They were also asked whether their doctor had spoken to them about “babyblues” or “postpartum depression” during their last pregnancy.
Respondents were asked how often they felt down, depressed, or sad since their baby was born. Those responding “often” or “always” were included in the group of women experiencing symptoms of PPD. The RI PRAMS included two other questions on the emotional state of women after delivery. They were asked how often they felt hopeless since their baby was born and how often they felt slowed down since the birth of their baby.
Other Predictor Variables
We included a number of other indicators previously found to be associated with PPD in earlier studies [32–34]. These indicators included previous live births or parity, smoking in the last trimester of pregnancy, physical abuse during pregnancy, stressful life events, medical complications during pregnancy, breastfeeding, pregnancy intention and discussion about mental health with a provider. To capture maternal stress, the PRAMS includes a list of 13 stressful life events such as moving, loss of job by mother or partner, divorce, and homelessness. If mothers responded yes to any of these events, they were included as having a stressful life event in our analysis. Women who reported experiencing medical problems such as kidney infections, high blood pressure, severe dehydration and nausea were included in the analysis as having a medical complication during pregnancy. We also included being diagnosed with depression before and during pregnancy in our analyses.
Other covariates included maternal age (<20, 20–29, 30–39, 40+ years), education (<high school, high school, >high school), race/Hispanic ethnicity (White non-Hispanic, Black non-Hispanic, Hispanic, Asian non-Hispanic, other non-Hispanic), marital status, private or public health insurance, and household poverty status measured as a ratio of family income to poverty threshold (≤100 %, >100 %).
The birth certificate provided data on maternal age, education, race/Hispanic ethnicity, and marital status; data for the other measures were obtained from the RI PRAMS questionnaire.
Statistical Analysis
We conducted bivariate analyses to examine the distribution of selected socio-demographic characteristics, depressive symptomatology, and other health indicators by mothers’ disability status (Tables 1, 2). The 95 % confidence intervals (CI) around the population estimates were calculated by using the point estimates and their standard errors.
Using stepwise multiple logistic regression we examined the association of disability status with symptoms of postpartum depression (Table 3). First, we included the association between disability status and PPD symptoms (step 1), after which we adjusted for socio-demographic characteristics (step 2), maternal characteristics found to be correlated with PPD in prior studies (step 3) and finally maternal depression before and during pregnancy as well as provider interactions related to their mental health.
Due to the small sample size of women with disabilities, we did not have power in the study to test for interactions. As a result, we ran two separate logistic regression models for women with disabilities and for women without disabilities to examine the association between depression before and during pregnancy and PPD symptomatology (Table 4). In the first model (n = 287) we examined how depression/depressive symptoms before and during pregnancy are associated with PPD symptomatology among women with disabilities. Similarly in the second model (n = 3,440) we examined the association between depression and depressive symptoms before and during pregnancy and PPD symptoms among women without disabilities. In order to construct more parsimonious models, we included only those variables that were significant in the stepwise multiple logistic regression models.
To account for complex survey design of RI PRAMS surveys, SUDAAN 11.0.0 was used to conduct the analyses for this study. The RI PRAMS study has been approved by the Rhode Island Department of Public Health Research and Data Access Review Institutional Review Board.
Results
Study Population
Among women who gave birth in Rhode Island, 6.8 % (95 % CI 5.8–7.8) reported a disability. There were significant differences in maternal characteristics and health indicators by disability status (Table 1). Recent mothers with disabilities were more likely to be younger, unmarried, have less formal education, be on public insurance, and have a household poverty status equal to or <100 % of the federal poverty level (FPL) than those without disabilities. They were also more likely to smoke in the last 3 months of their pregnancy, report physical abuse during pregnancy, and experience maternal stressors and medical complications during pregnancy.
Disability and Depression Symptomatology Before, During and After Pregnancy
Disability-related differences were found in the mental health of the mothers before, during and after pregnancy (see Table 2). Almost 40 % of mothers with disabilities (39.2 %; 95 % CI 32.3–46.5) reported being diagnosed with depression before their pregnancy compared to 16.3 % of non-disabled mothers (95 % CI 14.9–17.8). One in four mothers with disabilities (25.2 %; 95 % CI 19.5–31.9) reported being diagnosed with depression during their pregnancy compared to 7.6 % of other mothers (95 % CI 6.6–8.7). Compared to those without disabilities, mothers with disabilities were more likely to talk to their health care provider during their pregnancy about “what to do” if they felt depressed during their pregnancy or during postpartum.
Almost 30 % (28.9 %; 95 % CI 22.8–35.8) of mothers with disabilities reported often or always feeling down, depressed or sad after childbirth compared to 10 % of those without disabilities (95 % CI 8.9–11.3). Similar differences by disability status were found to the questions on feeling “slowed down” and feeling “hopeless” since the baby was born (see Table 2).
Disability and Postpartum Depression Symptomatology
In the unadjusted model, women with disabilities were 2.2 times more likely to report PPD symptoms (95 % CI 1.7–2.9) compared to women without disabilities (Table 3). The addition of sociodemographic characteristics (step 2) slightly weakened the association between a mother’s disability status and having PPD symptoms (RR 2.0; 95 % CI 1.5–2.6). While the addition of other maternal characteristics that have been found to be associated with PPD in the literature further weakened the association between disability and symptoms of PPD, women with disabilities were 1.8 times more likely to experience symptoms of PPD (95 % CI 1.3–2.4) compared to women without disabilities. In the final step of the model we accounted for depression before and during pregnancy and discussion about mood with a health care professional during pregnancy (step 4). In contrast to women not reporting a disability, women with disabilities had greater likelihood for PPD symptoms after accounting for sociodemographics, other maternal characteristics related to PPD, prior to and during pregnancy diagnosis of depression and visiting a provider for depression or anxiety.
Association Between Depression Before and During Pregnancy and Postpartum Depression Symptomatology
In this next step we examined the association between depression before and during pregnancy with PPD symptoms among women with and without disabilities (Table 4). Adjusting for other covariates, self-reported prenatal diagnosis of depression was not associated with PPD symptomatology for women with disabilities. However, depression during pregnancy for women with disabilities was marginally associated with PPD symptoms (p < 0.10; RR 1.7; 95 % CI 1.0–2.9). In contrast, women without disabilities who had a prenatal diagnosis of depression or had reported depression during their pregnancy were more likely to report symptoms of PPD.
Among other risk factors associated with PPD symptomatology among women with disabilities, we found that those who experienced medical problems during pregnancy or who had reported being physically abused by a current or former partner during their pregnancy were more likely to report symptoms of PPD. There were no significant associations between other demographic characteristics and PPD symptoms for women with disabilities. In contrast, other risk factors associated with PPD among women without self-reported disabilities included Hispanic ethnicity, maternal stressors, medical complications during pregnancy, and unintended pregnancy.
Discussion
This study demonstrates that women with disabilities are at a greater risk of experiencing symptoms of postpartum depression than women without disabilities. Adjusting for demographic characteristics, and other maternal characteristics associated with PPD symptoms, women with disabilities were significantly more likely to report symptoms of PPD. Interestingly, even after controlling for depression diagnosis before and during pregnancy, women who self-reported having a disability were still substantially more likely to report PPD symptoms.
We also examined the association between depression before and during pregnancy with PPD symptoms. Interestingly, for women with disabilities there was no association between depression diagnosis prior to pregnancy and symptoms of PPD. However, diagnosis of depression during pregnancy was marginally associated with PPD symptoms for women with disabilities. Potentially with a larger sample size of women with disabilities this association could achieve significance. This raises the question whether circumstances that occur during pregnancy may contribute both to depression during pregnancy and ultimately to postpartum depression for these women. For example, medical problems and physical abuse during pregnancy, both predictors of PPD symptomatology among women with disabilities in this study, may also contribute to depression during pregnancy.
Another possible explanation is that factors not measured in this study including stigma, lack of access to health care and services, lack of social and familial support, and unmet need for informal and formal care for women with disabilities during pregnancy and at postpartum could also contribute to postpartum depression for women with disabilities. Findings from other studies suggest that women with disabilities are less likely to have access to prenatal care and poorer access to adequate medical care altogether. In addition, women with disabilities may encounter negative attitudes from health care providers [35–39] and from their partner, family members and friends [1, 40, 41]. Further studies are needed to examine the association between informal and formal support during pregnancy and during postpartum, attitudes towards pregnancy in women with disabilities by health care providers and others, and other factors not measured in the PRAMS survey and depression during and after pregnancy among women with disabilities.
This is the first study to our knowledge, to examine postpartum depression among women with disabilities using a population-based dataset. Ross and Dennis [42] in their systematic review of PPD among women with chronic illness and disabilities including women with rheumatoid arthritis, multiple sclerosis, lupus, fibromyalgia, cancer, cerebral palsy, autoimmune disease and other chronic diseases and disabilities concluded that there was a concerning lack of research on postpartum mental health among women with disabilities. Only four studies on postpartum mental health were identified in their systematic review, including studies on women with HIV [43, 44], chronic health conditions [45], and rheumatoid arthritis and ankylosing spondylitis [46]. However none of these studies were based on representative or population-based samples of women with disabilities or long-term chronic health problems and furthermore, no studies on PPD were identified among women with multiple sclerosis, fibromyalgia, heart disease, asthma, and other chronic conditions and disabilities.
The detrimental effects of PPD on the health of mothers, their relationships with their partners, and their ability to bond with their infants as well as long-term health and wellbeing of their infants are well established [16–21, 47]. These adverse consequences of PPD observed among women and their infants in the general population could potentially be worse among mothers with disabilities given the structural and attitudinal barriers faced by women with disabilities during their pregnancy. The small but growing literature on pregnancy and disability suggests that women with disabilities have difficulty accessing maternity services, are at an increased risk of pregnancy-related complications and are at a higher risk for adverse obstetric outcomes [48–52]. Therefore, the impact of PPD and PPD symptoms among women with disabilities and their infants may likely be worse than the impact on the general obstetric population.
This study has several limitations. Given limitations of the PRAMS methodology, our research excluded pregnancies that resulted in stillbirths or live births of multiples of four or more infants. The RI-PRAMS data do not allow for determination of type of disability or severity of disability, both of which may have an impact on the experience of PPD symptoms. For example, women who identify as having a disability may be disabled by a serious or persistent mental illness which could confound the analysis. Interestingly, however, the results of this study did not detect a relationship between depression before pregnancy (which likely includes women disabled due to serious mental illness) and symptoms of PPD among women with disabilities. The data from the PRAMS survey are subject to self-report and recall biases. In addition, there may be limitations to the validity of birth certificate data included in the RI-PRAMS. Previous studies examining the validity of birth certificate data have had mixed results [53–55]. The rates of PPD symptoms reported in this study represent self-reported postpartum depressive symptomatology and may not reflect a clinical diagnosis of postpartum depression diagnosis or actual rates of PPD among women with and without disabilities. Finally, conclusions about causality cannot be drawn as the PRAMS utilizes a cross-sectional survey design.
Despite these limitations, the results of the present study suggest that women with disabilities are at a heightened risk for depression before, during and after pregnancy. Given the findings from this study, a more in-depth examination of PPD and postpartum depressive symptoms among women with disabilities and follow-up longitudinal studies are needed to understand the causal pathways and consequences of PPD symptomatology among women with disabilities. Fundamental to additional surveillance of PPD and disability are the inclusion of questions that identify disability in surveys that collect data on maternal health including the PRAMS. As of 2013, only two of the forty states with PRAMS surveys included disability identifiers. Given the dearth of information on the maternal health of women with disabilities, it is imperative that all states include disability identifiers in their PRAMS. Finally, screening for PPD symptomatology among recent mothers with disabilities by health care providers and timely referral of those with PPD diagnosis are critical to improving the health of both mothers with disabilities and their children.
References
Signore, C., Spong, C. Y., Krotoski, D., Shinowara, N. L., & Blackwell, S. C. (2011). Pregnancy in women with physical disabilities. Obstetrics and Gynecology, 117(4), 935.
Smeltzer, S. C. (2007). Pregnancy in women with physical disabilities. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 36(1), 88–96.
Iezzoni, L. I., Yu, J., Wint, A. J., Smeltzer, S. C., & Ecker, J. L. (2013). Prevalence of current pregnancy among US women with and without chronic physical disabilities. Medical Care, 51(6), 555–562.
Walsh-Gallagher, D., Sinclair, M., & Mc Conkey, R. (2012). The ambiguity of disabled women’s experiences of pregnancy, childbirth and motherhood: A phenomenological understanding. Midwifery., 28(2), 156–162.
Chakravarty, E. F., Nelson, L., & Krishnan, E. (2006). Obstetric hospitalizations in the United States for women with systemic lupus erythematosus and rheumatoid arthritis. Arthritis and Rheumatism, 54(3), 899–907.
Rogers, J., & Matsumura, M. (2005). The disabled woman’s guide to pregnancy and birth. New York City: Demos Medical Publishing.
Kelly, V. M., Nelson, L. M., & Chakravarty, E. F. (2009). Obstetric outcomes in women with multiple sclerosis and epilepsy. Neurology., 73(22), 1831–1836.
Bruce, M. L., Seeman, T. E., Merrill, S. S., & Blazer, D. G. (1994). The impact of depressive symptomatology on physical disability: MacArthur studies of successful aging. American Journal of Public Health, 84(11), 1796–1799.
Turner, R. J., & Noh, S. (1988). Physical disability and depression: A longitudinal analysis. Journal of Health and Social Behavior, 29(1), 23–37.
MacDonald, M. R., Nielson, W. R., & Cameron, M. G. (1987). Depression and activity patterns of spinal cord injured persons living in the community. Archives of Physical Medicine and Rehabilitation, 68(6), 339–343.
Fullerton, D. T., Harvey, R. F., Klein, M. H., & Howell, T. (1981). Psychiatric disorders in patients with spinal cord injuries. Archives of General Psychiatry, 38(12), 1369–1371.
Vahle, V. J., Andresen, E. M., & Hagglund, K. J. (2000). Depression measures in outcomes research. Archives of Physical Medicine and Rehabilitation, 81(12 Suppl 2), S53–S62.
Disability and Health Data System (DHDS). (2013). http://dhds.cdc.gov.
Chevarley, F. M., Thierry, J. M., Gill, C. J., Ryerson, A. B., & Nosek, M. A. (2006). Health, preventive health care, and health care access among women with disabilities in the 1994–1995 national health interview survey, supplement on disability. Womens Health Issues, 16(6), 297–312.
Centers for Disease Control and Prevention. (2008). Morbidity and mortality weekly report (MMWR). Prevalence of self-reported postpartum depressive symptoms—17 states, 2004–2005. CDC 57(14).
Goodman, J. H. (2004). Postpartum depression beyond the early postpartum period. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 33(4), 410–420.
Vigod, S. N., Villegas, L., Dennis, C. L., & Ross, L. E. (2010). Prevalence and risk factors for postpartum depression among women with preterm and low-birth-weight infants: A systematic review. BJOG, 117(5), 540–550.
Beck, C. T. (1998). The effects of postpartum depression on child development: A meta-analysis. Archives of Psychiatric Nursing, 12(1), 12–20.
Luoma, I., Tamminen, T., Kaukonen, P., Laippala, P., Puura, K., Salmelin, R., et al. (2001). Longitudinal study of maternal depressive symptoms and child well-being. Journal of the American Academy of Child and Adolescent Psychiatry, 40(12), 1367–1374.
Nelson, D. R., Hammen, C., Brennan, P. A., & Ullman, J. B. (2003). The impact of maternal depression on adolescent adjustment: The role of expressed emotion. Journal of Consulting and Clinical Psychology, 71(5), 935–944.
Martins, C., & Gaffan, E. A. (2000). Effects of early maternal depression on patterns of infant-mother attachment: A meta-analytic investigation. Journal of Child Psychology and Psychiatry, 41(6), 737–746.
Weinberg, M. K., & Tronick, E. Z. (1998). The impact of maternal psychiatric illness on infant development. Journal of Clinical Psychiatry, 59(Suppl 2), 53–61.
Marcus, S. M., & Heringhausen, J. E. (2009). Depression in childbearing women: When depression complicates pregnancy. Primary Care, 36(1), 151–165.
O’hara, M. W., & Swain, A. M. (1996). Rates and risk of postpartum depression: A meta-analysis. Int Rev Psychiatry, 8(1), 37–54.
Altshuler, L. L., Cohen, L. S., Moline, M. L., Kahn, D. A., Carpenter, D., Docherty, J. P., et al. (2001). Treatment of depression in women: A summary of the expert consensus guidelines. J Psychiatr Pract., 7(3), 185–208.
Dennis, C. L., & Vigod, S. (2013). The relationship between postpartum depression, domestic violence, childhood violence, and substance use: Epidemiologic study of a large community sample. Violence Against Women., 19(4), 503–517.
Dennis, C.-E., Janssen, P. A., & Singer, J. (2004). Identifying women at-risk for postpartum depression in the immediate postpartum period. Acta Psychiatrica Scand., 110(5), 338–346.
Robertson, E., Grace, S., Wallington, T., & Stewart, D. E. (2004). Antenatal risk factors for postpartum depression: A synthesis of recent literature. General Hospital Psychiatry, 26(4), 289–295.
Clare, C. A., & Yeh, J. (2012). Postpartum depression in special populations: A review. Obstetrical & Gynecological Survey, 67(5), 313–323.
Rhode Island Department of Public Health. (2009–2011). Pregnancy risk assessment monitoring system (PRAMS).
Pregnancy Risk Assessment Monitoring System (PRAMS). http://www.health.ri.gov/programs/pregnancyriskassessmentmonitoring/.
Leigh, B., & Milgrom, J. (2008). Risk factors for antenatal depression, postnatal depression and parenting stress. BMC Psychiatry. doi:10.1186/1471-244X-8-24.
Liu, C. H., & Tronick, E. (2012). Rates and predictors of postpartum depression by race and ethnicity: Results from the 2004 to 2007 New York City PRAMS survey (Pregnancy Risk Assessment Monitoring System). Maternal and Child Health Journal, 17(9), 1599–1610.
Robertson, E., Grace, S., Wallington, T., & Stewart, D. E. (2004). Antenatal risk factors for postpartum depression: A synthesis of recent literature. General Hospital Psychiatry, 26(4), 289–295.
Prilleltensky, O. (2003). A ramp to motherhood: The experiences of mothers with physical disabilities. Sex Disab., 21(1), 21–47.
Nosek, M. A., Young, M. E., Rintala, D. H., Howland, C. A., Foley, C. C., & Bennett, J. L. (1995). Barriers to reproductive health maintenance among women with physical disabilities. Journal of Women’s Health., 4(5), 505–518.
Office of the Surgeon General (US), Office on Disability (US). (2005). The Surgeon General’s call to action to improve the health and wellness of persons with disabilities. Rockville, MD: US Department of Health and Human Services.
Breslin, M. L., & Yee, S. (2009). The current state of health care for people with disabilities. Washington, DC: National Council on Disability.
Mason, M. G., & Long-Bellil, L. (2012). Taking care: Lessons from mothers with disabilities. Lanham, Maryland: University Press of America.
Smeltzer, S. C. (2002). Reproductive decision making in women with multiple sclerosis. Journal of Neuroscience Nursing, 34(3), 145.
Llewellyn, G., & McConnell, D. (2002). Mothers with learning difficulties and their support networks. Journal of Intellectual Disability Research, 46(Pt 1), 17–34.
Ross, L. E., & Dennis, C. L. (2009). The prevalence of postpartum depression among women with substance use, an abuse history, or chronic illness: A systematic review. J Womens Health (Larchmt)., 18(4), 475–486.
Larrabee, K. D., Monga, M., Eriksen, N., & Helfgott, A. (1996). Quality of life assessment in pregnant women with the human immunodeficiency virus. Obstetrics and Gynecology, 88(6), 1016–1020.
Ethier, K. A., Ickovics, J. R., Fernandez, M. I., Wilson, T. E., Royce, R. A., Koenig, L. J., et al. (2002). The perinatal guidelines evaluation project HIV and pregnancy study: Overview and cohort description. Public Health Reports, 117(2), 137–147.
Chaaya, M., Campbell, O. M., El Kak, F., Shaar, D., Harb, H., & Kaddour, A. (2002). Postpartum depression: Prevalence and determinants in Lebanon. Arch Womens Ment Health., 5(2), 65–72.
Forger, F., Ostensen, M., Schumacher, A., & Villiger, P. M. (2005). Impact of pregnancy on health related quality of life evaluated prospectively in pregnant women with rheumatic diseases by the SF-36 health survey. Annals of the Rheumatic Diseases, 64(10), 1494–1499.
Weinberg, M. K., & Tronick, E. Z. (1998). The impact of maternal psychiatric illness on infant development. Journal of Clinical Psychiatry, 59(Suppl 2), 53–61.
Thomas, C., & Curtis, P. (1997). Having a baby: Some disabled women’s reproductive experiences. Midwifery., 13(4), 202–209.
Mitra, M., Lu, E., & Diop, H. (2012). Smoking among pregnant women with disabilities. Womens Health Issues., 22(2), e233–e239.
Mitra, M., Manning, S. E., & Lu, E. (2012). Physical abuse around the time of pregnancy among women with disabilities. Maternal and Child Health Journal, 16(4), 802–806.
Lipson, J. G., & Rogers, J. G. (2000). Pregnancy, birth, and disability: Women’s health care experiences. Health Care for Women International, 21(1), 11–26.
Blackford, K. A., Richardson, H., & Grieve, S. (2000). Prenatal education for mothers with disabilities. Journal of Advanced Nursing, 32(4), 898–904.
Andrade, S. E., Scott, P. E., Davis, R. L., Li, D. K., Getahun, D., Cheetham, T. C., et al. (2013). Validity of health plan and birth certificate data for pregnancy research. Pharmacoepidemiology and Drug Safety, 22(1), 7–15.
Kane, D. J., & Sappenfield, W. M. (2014). Ascertainment of medicaid payment for delivery on the Iowa birth certificate: Is accuracy sufficient for timely policy and program relevant analysis? Maternal and Child Health Journal, 18(4), 970–977.
Mason, L. R., Nam, Y., & Kim, Y. (2014). Validity of infant race/ethnicity from birth certificates in the context of U.S. demographic change. Health Services Research, 49(1), 249–267.
Acknowledgments
This research is funded by a Grant from the National Institutes of Health, Eunice Kennedy Shriver National Institute of Child Health & Human Development. Grant Number: 1R01HD074581.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mitra, M., Iezzoni, L.I., Zhang, J. et al. Prevalence and Risk Factors for Postpartum Depression Symptoms Among Women with Disabilities. Matern Child Health J 19, 362–372 (2015). https://doi.org/10.1007/s10995-014-1518-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-014-1518-8