
Abstract
Objectives We partnered with a Massachusetts family workgroup to analyze state level data that would be most useful to consumers and advocates in Massachusetts. Methods Massachusetts’ and US data from the 2001 National Survey of Children with Special Health Care Needs (NSCSHCN) were analyzed. We examined types of need and prevalence of unmet need for all CSHCN and for more severely affected CSHCN. We also correlated unmet need to child and family characteristics using multivariate logistic regression. Results In Massachusetts, 17% of CSHCN and 37% of children more severely affected did not receive needed care. CSHCN who were uninsured anytime during the previous year were nearly 5 times more likely to experience an unmet need (OR = 4.95, CI: 1.69–14.51). Children with more functional limitations (OR = 3.15; CI: 1.59–6.24) and unstable health care needs (OR = 3.26; CI: 1.33–8.00) were also more likely to experience an unmet need. Receiving coordinated care in a medical home (OR = 0.46; CI: 0.23–0.90) was associated with reduced reports of unmet need. Conclusions With input from families of CSHCN, researchers can direct their analyses to answering the questions and concerns most meaningful to families. We estimate that 1 in 6 CSHCN in Massachusetts did not receive needed care, with more than 1 in 3 CSHCN with a more severe condition experiencing an unmet need. Enabling factors were predictors of unmet need suggesting solutions such as expanding insurance coverage and improving services systems for CSHCN.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The National Survey of Children with Special Health Care Needs [1] (NSCSHCN) provides a unique opportunity to examine issues related to children with special health care needs (CSHCN) and their families on both a state and national level. With accessible state level data, we sought to use a form of Participatory Action Research (PAR) in order to provide research most relevant to Massachusetts’ families. PAR is a research approach whereby researchers and families collaborate in all phases of research, which can result in increased relevance of research, increased research utilization, and mutual learning opportunities [2].
We sought direction from the Family Participation Workgroup of the Massachusetts Consortium for Children with Special Health Care Needs (FPWG) [3] to determine the most appropriate topic of research and to guide the research in a direction that would be most relevant to families. Most members are parents of CSHCN and have personal experience with challenges and deficiencies in the health care and related systems. For example, at one meeting with the FPWG, families discussed issues including a lack of a coordinated source of information, limited mental heath coverage, lack of insurance coverage for Autism and syndromes, and a limited state capacity for certain specialists. These personal experiences prompted the group’s particular interest in better understanding unmet needs among CSHCN and children with more severe conditions.
Sponsored by the US Maternal and Child Health Bureau (MCHB), the NSCSHCN was designed to produce reliable state and national level estimates of the prevalence and characteristics of CSHCN [1]. The survey is part of a monitoring strategy designed to measure progress towards MCHB’s national agenda [4] and the Healthy People 2010 [5] national goal to increase the proportion of states that have systems of care for CSHCN that are family-centered, community-based, coordinated and culturally competent [5]. MCHB developed six core outcomes for measuring progress in implementing these community-based systems of services:
-
1.
Families of CSHCN will partner in decision-making and will be satisfied with the services they receive.
-
2.
CSHCN will receive coordinated ongoing comprehensive care within a medical home.
-
3.
Families of CSHCN will have adequate private and/or public insurance to pay for the services they need.
-
4.
Children will be screened early and continuously for special health care needs.
-
5.
Community-based service systems will be organized so families can use them easily.
-
6.
Youth with special health care needs will receive the services necessary to make transitions to adult life, including adult health care, work, and independence [4, 6].
These outcomes are operationalized and measured in the NSCSHCN and are being used as performance measures in federal and state Title V Maternal and Child Health programs. Title V provides block grants to states that match funds in order to improve the health of all mothers and children, with 30% of federal block grant funds dedicated to CSHCN [7].
The NSCSHCN identifies children with special health care needs using a broad definition released by MCHB in 1998 [8]. CSHCN are those children who require services beyond that required by children generally because of a chronic physical, developmental, behavioral or emotional condition. Using this definition, approximately 13% of children in the United States and 15% of children in Massachusetts have a special health care need (SHCN) [9]. Studies have shown that CSHCN use more health care services than children without special needs [10–13]. Further, families experience a variety of consequences of caring for a child with a SHCN including those which can contribute to an increased need for services such as lost employment [14–17] and increased financial burden [16].
National studies have shown that CSHCN have higher rates of unmet need for medical services, compared to children without a SHCN [13, 18, 19]. The NSCSHCN shows that for the US, more than 1 in 6 (17.7%) CSHCN had an unmet health care need (any of 14 health care services) [20]. Specific services with reported rates of unmet need include specialty care (7.3%) [21], dental care (10.4%) [22], therapy services (11.1%), communication aids (24.7%) and mobility aids (9.0%) [23]. A study using data from the National Health Interview Survey reported rates of unmet need for health care services (medical care, dental care, prescriptions, eyeglasses and mental health care) among CSHCN at 12%, with rates of unmet need for specific services ranging from 1.2% for mental health care to 8.1% for dental care [24].
Consistently, lack of insurance has been associated with unmet need for all children [25] as well as for CSHCN. Studies using the NSCSHCN have reported strong associations between unmet need and lack of health insurance, with odds ratios ranging from 1.61 for unmet dental care need [22] to 7.51 for unmet routine care [21]. Newacheck et al. [24] found that uninsured CSHCN were 4 times more likely to have an unmet need than insured children. Insurance, however, does not guarantee access to care; between 10% and 16% of insured CSHCN experience an unmet need [20, 24]. Underinsurance is a likely contributor; underinsured CSHCN were more than twice as likely to experience an unmet need than children adequately insured [26]. Other factors associated with unmet need among CSHCN include poverty, adolescent age group, and more severe limitations [20–23, 27, 28].
As guided by the FPWG, we examined unmet health care and family service needs for all CSHCN and for those children with more severe conditions. We also sought to determine how Massachusetts is doing in meeting families’ needs. To do this, we examined unmet need as it relates to MCHB’s core outcomes of progress [4] towards the Healthy People 2010 [5] national goal to increase the proportion of states that have systems of care for CSHCN.
Methods
Family Participation
The Massachusetts Consortium for Children with Special Health Care Needs (http://www.neserve.org/maconsortium/index.html) is a working group dedicated to improving systems of care for CSHCN and their families in the state. Its members include parents and health care providers as well as representatives from state agencies, parent organizations, health plans, universities, research programs, and advocacy and support organizations. The Consortium’s Family Participation Work Group (FPWG) promotes and supports the role that families play in improving systems of care by strengthening partnerships between family members and policymakers at all levels of public and private sector organizations. This project explicitly involved and relied on family members from the FPWG in all stages of research.
Specifically, several meetings between the research staff and the FPWG determined the topic of study, directed the analyses, interpreted the findings and developed the final products. For example, when presented with preliminary results on unmet need for all CSHCN, the parents in the group were surprised at what they viewed as low levels of unmet need for care in Massachusetts, in light of their own family experiences. This surprise led to a discussion about condition severity and the impact of severity on levels of unmet need. As a result, the workgroup and the research team worked on identifying the appropriate parameters for selecting children with more severe special health care needs. As such, we re-analyzed the data to look only at the more severely affected children, with several discussions centered on how to define this population.
Sample
Massachusetts’ data from the 2001 NSCSHCN were analyzed, with US data analyzed for comparison. CSHCN were identified using the CSHCN Screener [29], which identifies CSHCN as those with prescription medication dependency, elevated health care or educational service use, or a functional limitation due to a health condition that has lasted or is expected to last at least 12 months. The Massachusetts sample included 744 CSHCN; the national sample included 38,886 CSHCN.
For the subanalysis, children with a more severe condition were selected if screened positive for 2 or more CSHCN Screener items and either of the following: a condition affects ability ‘a great deal’; or a parent rank of severity 8+ (on scale of 0–10). The subsample of children with more severe conditions included 94 children in Massachusetts and 5,203 children in the US.
Measures
Dependent Variable
The survey asked parents about the perceived need for care (including 14 health care and 4 family support services) for their child and if that care was received. For each, a two-part question was asked: whether the child needed that care in the year prior to the survey, and of those who answered “Yes,” whether that child received the needed care. A composite variable was developed from those 18 service needs (see Table 4 for the specific services). This dichotomous variable indicated whether the child needed but did not receive one or more types of health care or family services or whether all needs were met.
Because professional care coordination is also included in the independent variable for MCHB core outcome #2 (see below), we performed a sensitivity analysis with the Massachusetts imputed data using a dependent variable both with and without professional care coordination. Since only minor differences were seen (noted below) we ultimately decided to include professional care coordination in the dependent variable because of the importance of the need for CSHCN and the relevance to the FPWG.
Independent Variables
We used the Behavioral Model of Health Services Use as a conceptual model to help guide our analysis [30]. This model suggests that a person’s use of health care services is a function of the person’s predisposing, enabling, and need factors. Predisposing factors include sociodemographic characteristics, enabling factors include resources that facilitate or inhibit use, and need factors include the individual’s illness or perceived need for services.
Predisposing factors: We examined age in years, race (White or other), Hispanic ethnicity, and the mother’s education level (less than high school degree, high school degree, some post high school, 4-year college degree or more).
Enabling factors: We included family poverty level (<100%, 100–199%, 200–299%, 300–399%, 400%+) and child’s insurance type (uninsured anytime during the past year, public, both public and private, private insurance at time of survey). Public insurance included Medicaid, SCHIP, military insurance, Title V or other public insurance. Of particular interest were MCHB’s six core outcomes that have been operationalized in the NSCSHCN [31] by developing composite variables comprised of various elements of each measure. We examined whether the family met 4 of the 6 MCHB core outcomes: (#1) Families of CSHCN will partner in decision-making and will be satisfied with the services they receive; (#2) CSHCN will receive coordinated ongoing comprehensive care within a medical home; (#3) Families of CSHCN will have adequate private and/or public insurance to pay for the services they need; and (#5) Community-based service systems will be organized so families can use them easily.
Need factors: We examined three measures of need: amount of time condition affects child’s ability (never, sometimes, usually or always), stability of child’s health care needs (needs usually stable, needs change once in awhile, needs change all the time) and severity of condition (using the definition described above for the subsample analysis; this factor was not included in the multivariate analysis on the subsample of CSHCN with a more severe condition).
Data Analysis
We examined types of need and prevalence of unmet need for all CSHCN and for children with more severe conditions. We compared all CSHCN in Massachusetts to all CSHCN in the US and compared all CSHCN to children more severely affected (in both Massachusetts and US) and determined significant differences by comparing 95% confidence intervals (overlapping confidence intervals are not significant) [32]. Next, we correlated any unmet need to the independent variables described above. We constructed multivariate logistic regression models to examine the relations between each of the independent variables and the outcome (any unmet need) controlling for the other variables using an alpha level of 0.05. All independent variables theoretically related to unmet need were included in the multivariate analysis. Most analyses use the Massachusetts data, with US data included for comparison. However, due to the small Massachusetts sample size for CSHCN with more severe conditions, only US data were examined for the multivariate logistic regressions.
Model fitting methods were chosen to reflect the complex survey design used in NSCSHCN as well as the sample weights provided by the survey designers to account for the unequal selection probabilities. For this reason, we used SUDAAN [33] to analyze the national data, and for the state-level analyses, we used SAS/STAT software [34] and SUDAAN [33]. Because the methodologies used above do not account for item nonresponse (partial missingness per respondent, e.g., respondent answered ‘do not know’ or ‘refused’ to demographic or need questions), we carried out a multiple imputation inference. We multiply imputed the data ten times [35, 36] and each imputed data was analyzed in the same fashion as if it were complete. In the final stage, we combined 10 sets of regression coefficients and standard errors [37].
Results
Sample Characteristics
Table 1 lists the sample characteristics for both the Massachusetts and US samples. Compared with all CSHCN in the US, CSHCN in Massachusetts were significantly less likely to be non-white (15.5% vs. 24.9%), near poor (15.0% vs. 22.0%) and uninsured (6.9% vs. 11.6%). Massachusetts also had a higher percentage of CSHCN who receive care in a medical home (61.0% vs. 52.6%) compared to all CSHCN in the US. Most notably, compared to all US CSHCN, US children with more severe conditions were significantly more likely to be male (66.4% vs. 59.8%), non-white (31.8% vs. 24.9%), poor (23.8% vs. 15.0%), near poor (29.5% vs. 22.0%) and on public insurance (33.1% vs. 19.2%). Additionally, these children were found to be significantly less likely to have met all 4 of the MCHB outcomes studied. US parents whose children were more severely affected were significantly less likely to report that they partner in their child’s health care decision-making (40.0% vs. 57.5%), that their child has coordinated care in a medical home (37.9% vs. 52.6%), that their child has adequate health insurance (50.0% vs. 59.6%) or that their community-based services are organized for easy use (61.2% vs.74.3%). Though similar differences were also seen between all CSHCN and children with more severe conditions in the Massachusetts data, they were not statistically significant.
Types of Need
Table 2 lists the types of needs reported. Most CSHCN in Massachusetts (98.0%) and the US (98.7%) reported at least one need for health care or family support services. Prescription medications, routine preventive care, and dental care were the top three health care needs reported for all CSHCN in Massachusetts (87.5, 87.3, and 85.5%, respectively) as well as the US (87.9, 74.4, and 78.2%, respectively). Mental health care for family members and professional care coordination were the top family support needs reported in both Massachusetts (16.7%, 11.0%, respectively) and the US (13.2%, 11.8%, respectively). Though about the same percentage of CSHCN with more severe conditions needed any services, the types of need differed from all CSHCN. For example, compared to all CSHCN, Massachusetts’ children with more severe conditions required significantly more specialty care (75.6% vs. 55.5%), mental health care (53.8% vs. 33.3%), special therapy (53.7% vs. 26.6%), home health care (17.7% vs. 4.3%), communication aids (10.8% vs. 2.5%), professional care coordination (25.6% vs. 11.1%) and respite care (18.0% vs. 6.5%). Similar relationships are found for US children.
Prevalence of Unmet Need
Among CSHCN in Massachusetts who reported a need for services, 16.9% (an estimated 35,140) did not receive needed care; 13.2% (an estimated 27,434) did not receive needed health care services and 21.2% (an estimated 13,541) did not receive needed family support services (Table 3). Results were similar in the US sample (20.9, 18.4, and 22.9%, respectively). Significantly more children with severe conditions experienced an unmet need compared to all CSHCN. In Massachusetts, more than a third (37.3% or an estimated 11,304) of children more severely affected who had a need for care experienced an unmet need in the year prior to the survey. Nationally, 40.8% (or an estimated 522,252) of children with more severe conditions who reported a need for services had at least one of those needs unmet.
Among all Massachusetts’ CSHCN and Massachusetts’ children with more severe conditions, genetic counseling (27.0% and 50.8%), respite care (25.4% and 49.6%), mental health care for family members (13.9% and 18.9%) and communication aids/devices (12.9% and 21.0%) were among the five most common unmet needs (Table 4). For children in Massachusetts with more severe conditions mobility aids/devices (26.5%) replaced substance abuse treatment (23.0%) in the top five unmet needs for all CSHCN. In the US, the most common unmet need was for communication aids with nearly a quarter (24.7%) of CSHCN and 38.3% of more severely affected children reporting they did not receive needed aids. Also in the US, more severely affected children reported significantly more unmet need for prescription medication (3.7% vs. 1.7%), routine care (5.5% vs. 3.2%), dental care (16.4% vs. 10.4%), specialty care (11.8% vs. 7.3%), special therapy (11.1% vs. 16.5%), mental health care for the child (23.8% vs. 18.1%) and family (28.5% vs. 20.9%), and respite care (35.2% vs. 24.3%) than all CSHCN.
Factors Associated with Any Unmet Need
Table 5 shows the odds ratios from multivariate logistic regression analysis that assesses the independent effects of predisposing, enabling and need characteristics on the likelihood of experiencing any unmet need for all CSHCN in Massachusetts and US and for CSHCN with a more severe condition in US. In Massachusetts, older children were more likely to report an unmet need (OR = 1.07; CI: 1.00–1.15). Insurance status was also strongly correlated with experiencing any unmet need: CSHCN who were uninsured anytime during the previous year were nearly 5 times more likely to experience an unmet need (OR = 4.95, CI: 1.69–14.51) than children privately insured. Receiving coordinated care in a medical home (OR = 0.46; CI: 0.23–0.90) was associated with reduced reports of unmet need. Need factors associated with unmet need include having a condition that usually or always affects the child’s ability compared to never (OR = 3.15; CI: 1.59–6.24) and having needs that change all the time compared to needs that are usually stable (OR = 3.26; CI: 1.33–8.00). In the sensitivity analysis with professional care coordination excluded from the dependent variable (results not shown), family poverty level became significant (OR = 0.72, CI: 0.54–0.95).
In addition to the same associations in the Massachusetts data, factors associated with reduced unmet need in the US data include male gender (OR = 0.90; CI: 0.81–0.99), and higher family poverty status (OR = 0.87; CI: 0.83–0.90). Moreover, all four MCHB outcomes studied were associated with reduced reports of unmet need in the US sample of all CSHCN. Protection from having an unmet need was found among families who partner in their child’s health care decision-making (OR = 0.61; CI: 0.53–0.71), and who have community-based services that are organized for easy use (OR = 0.78; CI: 0.68–0.89), as well as among children who receive ongoing coordinated care in a medical home (OR = 0.55; CI: 0.49–0.62), and have adequate health insurance (OR = 0.50; CI: 0.45–0.57). Factors associated with unmet need among children with more severe conditions were similar to the total US sample, with the exception of gender and family poverty, which were not significant.
Discussion
Members of the FPWG found the percentages of CSHCN experiencing an unmet need in Massachusetts (17%) to be much lower than they expected. In particular, the group was concerned about the overall low percentages with respect to frequency of need for support services. This raised a number of questions about the survey design. For example, do families really know what care coordination or respite care is? Because of these concerns, the group requested further analysis that examined children with more severe conditions. Although the percentage reporting unmet need increased among this subgroup of children (37%), the FPWG still felt that the survey underestimated unmet need in Massachusetts.
Nevertheless, we estimate that approximately 1 in 6 CSHCN in Massachusetts who needed care did not receive that care. As with studies on national-level data, lack of insurance [21, 22, 24] and underinsurance [26] were strongly associated with unmet need. It has been estimated that over half (59%) the uninsured children in Massachusetts are eligible for Medicaid or SCHIP but not enrolled [38]. Studies have shown that barriers to enrollment include lack of knowledge (of program and/or eligibility), the complex enrollment process, and language barriers [39–41]. Streamlining the enrolling process, and increasing outreach and education may help improve access to care. Improving the public insurance systems for CSHCN may also improve access to care. For example, Davidoff et al. [42], showed that expansions in SCHIP led to increases in insured CSHCN as well as decreases in unmet need.
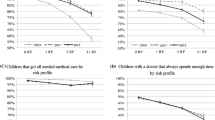
Additionally our findings show that the MCHB indicators of good systems of care, as measured in the Title V performance measures, are associated with less unmet need in Massachusetts (medical home) and the US (all 4 indicators studied). Our data suggests that, in Massachusetts, CSHCN who receive coordinated care within a medical home experience less unmet need than CSHCN who do not receive care in a medical home. Though not significant in the Massachusetts analysis (possibly due to small sample size), the US data showed all 4 of the MCHB indicators (partner in decision-making, medical home, adequate insurance, organized community services) to be protective factors against unmet need. These findings suggest that good systems of care may reduce unmet need, particularly among CSHCN with more severe conditions who were more likely to be poor and less likely to meet any of the 4 MCHB outcomes.
Although Massachusetts generally ranks higher on the performance measures than most other states, room for improvement exists. For example, Massachusetts appears strong in certain components of the medical home, including children having a usual source of care (91%) and a personal doctor or nurse (95%), however, considerably weaker in other components of the medical home including receiving family centered care (70%) and coordinated care (49%) [43]. During focus groups conducted by the Massachusetts Department of Public Health (MDPH) for the 2005 MCH Needs Assessment, families noted issues with obtaining adequate health insurance including restrictive definitions of “medically necessary,” limits to mental health coverage and fee increases to the Medicaid program [43]. Today, Massachusetts’s efforts to improve these systems of care include continued collaboration between MDPH and families of CSHCN (through organizations such as the Massachusetts Consortium for CSHCN and The Federation for Children with Special Needs) and several state programs (Table 6).
Further, these results raise significant concerns regarding the state budget crisis, which began in 2001 (just after the administration of the NSCSHCN) and its effects on access to care for CSHCN in Massachusetts. Historically, Massachusetts held a longstanding reputation for its commitment and successes in public health [44], including expansions in Massachusetts’ Medicaid Program (MassHealth) beginning in 1997, targeting children with disabilities [45]. However, with an approximate 30% cut in funding in MDPH programs between 2001 and 2004, many of the public health programs that contributed to that reputation have been reduced [44]. In terms of specific programs for CSHCN, Medicaid was left largely intact, however, premium increases for MassHealth Standard and CommonHealth (a Medicaid buy-in program for children with disabilities whose families are over-income limits for Medicaid or S-CHIP), enrollment caps to the Children’s Medical Security Plan (for any children not eligible for MassHealth), and cuts to provider payment reducing the number of providers who accept MassHealth will likely affect access to care for CSHCN [45, 46].
The NSCSHCN was repeated in 2005–2006, with plans to repeat the survey every 3–5 years [1]. This provides an opportunity to examine unmet need among CSHCN over time and possibly note any effects of the state budget crisis. Further, future releases of the survey may note any effects of the new Massachusetts health care reform bill signed in April 2006. The bill, which includes an increase in Medicaid eligibility for children up to 300% of the federal poverty level, has already begun implementation [47].
This study has some limitations. Unmet need was determined from parent report of perceived need and receipt of care. This is subject to both recognition and recall error [25]. Another limitation of this study is that the use of state-level data generates small sample sizes, which may reduce the power of the statistical methods. This was apparent in the multivariate analysis where the confidence intervals of some of the odds ratios were large and statistically insignificant, although significant in the US analysis (e.g., MCHB indicators). Further, small sample size prevents the analysis of subpopulations as seen here in the analysis of CSHCN with more severe conditions in Massachusetts.
Bridging the gap between families and research has allowed parents and consumers to directly inform the project in order to ensure that analyses will be relevant and practical to those who will be using the results. The FPWG conducts projects focused on the specific goals for system improvement and the results of this data analysis are being used by the workgroup to bolster current projects. This project was also a precursor to the Family-Professional Partners Institute, a new initiative by the Massachusetts Consortium for CSHCN, in which families work with organizations to develop roles for consumers that help shape programs, influence policy and impact the care that children and families receive. Further, this project has been indicative of the importance of family participation and paved the way for other partnerships for both the FPWG and this research team.
References
van Dyck, P. C., McPherson, M., Strickland, B. B., Nesseler, K., Blumberg, S. J., Cynamon, M. L., et al. (2002). The national survey of children with special health care needs. Ambulatory Pediatrics, 2(1), 29–37.
Turnbull, A. P., Friesen, B. J., & Ramirez, C. (1998). Participatory action research as a model for conducting family research. Journal of The Association for Persons with Severe Handicaps, 23(3), 178–188.
Massachusetts Consortium for Children with Special Health Care Needs. Accessed: January 12, 2004. http://www.neserve.org/maconsortium/index.html
U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau. (1989). Achieving and Measuring Success: A National Agenda for Children with Special Health Care Needs. Accessed: 3/17/04. http://mchb.hrsa.gov/programs/specialneeds/measuresuccess.htm
U.S. Department of Health, Human Services (2000). Healthy people2010: Understanding and improving health (2nd ed.). Washington: U.S. Government Printing Office.
U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. Progress Toward Implementing Community-Based Systems of Services for CSHCN: Summary Tables from the National Survey of Children with Special Health Care Needs, 2001. April 28, 2003. Accessed: March 17, 2004. http://www.cdc.gov/nchs/data/slaits/CSHCN%20Progress%20Tables1.pdf
Health Resources and Services Administration, Maternal and Child Health Bureau. (2005). Title V Information System. Accessed: May 1, 2007. https://www.perfdata.hrsa.gov/mchb/mchreports/Search/search.asp
McPherson, M., Arango, P., Fox, H., Lauver, C., McManus, M., & Newacheck, P. W., et al. (1998). A new definition of children with special health care needs.[comment]. Pediatrics, 102(1 Pt 1), 137–140.
U.S. Department of Health, Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau. (2004). The national survey of children with special health care needs chartbook 2001. Rockville: U.S. Department of Health and Human Services.
Szilagyi, P. G., Shenkman, E., Brach, C., LaClair, B. J., Swigonski, N., & Dick, A., et al. (2003). Children with special health care needs enrolled in the state children’s health insurance program (SCHIP): Patient characteristics and health care needs. Pediatrics, 112(6), e508–e520.
Newacheck, P. W., & Kim, S. E. (2005). A national profile of health care utilization and expenditures for children with special health care needs. Archives of Pediatrics & Adolescent Medicine, 159(1), 10–17.
Chevarley, F. M. (2006). Utilization and expenditures for children with special health care needs. Research findings No. 24. Rockville: Agency for Healthcare Research and Quality.
Newacheck, P. W., Strickland, B., Shonkoff, J. P., Perrin, J. M., McPherson, M., & McManus, M., et al. (1998). An epidemiologic profile of children with special health care needs. Pediatrics, 102(1 Pt 1), 117–123.
Kuhlthau, K. A., & Perrin, J. M. (2001). Child health status and parental employment. Archives of Pediatrics and Adolescent Medicine, 155, 1346–1350.
Thyen, U., Kuhlthau, K. A., & Perrin, J. M. (1999). The effect of child health status on maternal employment. Pediatrics, 103, 1235–1242.
Kuhlthau, K. A., Hill, K. S., Yucel, R., & Perrin, J. M. (2005). Financial burden for families of children with special health care needs. Maternal and Child Health Journal, 9, 207–218.
Hirst, M. (1985). Young adults with disabilities: Health, employment and financial costs for family. Child Care Health and Development, 11, 291–307.
Silver, E. J., & Stein, R. E. (2001). Access to care, unmet health needs, and poverty status among children with and without chronic conditions. Ambulatory Pediatrics, 1(6), 314–320.
Chevarley, F. M. (2005). Access to needed medical care among children under 18 years of age with special health care needs, 2002. Rockville: Agency for Healthcare Research and Quality.
van Dyck, P. C., Kogan, M. D., McPherson, M. G., Weissman, G. R., & Newacheck, P. W. (2004). Prevalence and characteristics of children with special health care needs. Archives of Pediatrics & Adolescent Medicine, 158(9), 884–890.
Mayer, M. L., Cockrell Skinner, A., & Slifkin, R. T. (2004). Unmet need for routine and specialty care: Data from the national survey of children with special health care needs. Pediatrics, 113(2), e109–e115.
Lewis, C., Robertson, A. S., & Phelps, S. (2005). Unmet dental care needs among children with special health care needs: implications for the medical home. Pediatrics, 116(3), e426–e431.
Dusing, S. C., Skinner, A. C., & Mayer, M. L. (2004). Unmet need for therapy services, assistive devices, and related services: data from the national survey of children with special health care needs. Ambulatory Pediatrics, 4(5), 448–454.
Newacheck, P. W., McManus, M., Fox, H. B., Hung, Y. Y., & Halfon, N. (2000). Access to health care for children with special health care needs. Pediatrics, 105(4 Pt 1), 760–766.
Newacheck, P. W., Hughes, D. C., Hung, Y. Y., Wong, S., & Stoddard, J. J. (2000). The unmet health needs of America’s children. Pediatrics, 105(4 Pt 2), 989–997.
Kogan, M. D., Newacheck, P. W., Honberg, L., & Strickland, B. (2005). Association between underinsurance and access to care among children with special health care needs in the United States. Pediatrics, 116(5), 1162–1169.
Huang, Z. J., Kogan, M. D., Yu, S. M., & Strickland, B. (2005). Delayed or forgone care among children with special health care needs: An analysis of the 2001 National Survey of Children with Special Health Care Needs. Ambulatory Pediatrics, 5(1), 60–67.
Newacheck, P. W., Hung, Y. Y., & Wright, K. K. (2002). Racial and ethnic disparities in access to care for children with special health care needs. Ambulatory Pediatrics, 2(4), 247–254.
Bethell, C. D., Read, D., Stein, R. E., Blumberg, S. J., Wells, N., & Newacheck, P. W. (2002). Identifying children with special health care needs: development and evaluation of a short screening instrument. Ambulatory Pediatrics, 2(1), 38–48.
Anderson, R. M. (1995). Revisiting the behavioral model and access to medical care: Does it matter? Journal of Health and Social Behavior, 36(1), 1–10.
Department of Health, Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. Progress Toward Implementing Community-Based Systems of Services for CSHCN: Summary Tables from the National Survey of Children with Special Health Care Needs, 2001. April 28, 2003. Accessed: March 17, 2004. http://www.cdc.gov/nchs/data/slaits/CSHCN%20Progress%20Tables1.pdf
Smith, R. W. (1997). Visual Hypothesis Testing with Confidence Intervals. In: Proceedings of the Twenty-Second Annual SAS® Users Group International Conference; March 16–19, San Diego, CA: SAS Institute Inc., Cary, NC; p. 1252–1257. http://www2.sas.com/proceedings/sugi22/STATS/PAPER270.PDF
Research Triangle Institute. (2005). SUDAAN software for the statistical analysis of correlated data 9.0.1. Research Triangle Park, NC.
SAS Institute, Inc. SAS/STAT 9.1.3. Cary, NC. 2002–2003.
Schafer, J. L. (1997). Analysis of incomplete multivariate data. London: Chapman & Hall.
Yucel, R. M., & Schafer, J. L. (2002). Computational strategies for multivariate linear mixed-effects models with missing values. Journal of Computational and Graphical Statistics, 11(2), 437–457.
Rubin, D. B. (1996). Multiple imputation after 18+ years. Journal of the American Statistical Association, 91, 473–489.
National Association of Children’s Hospitals, American Academy of Pediatrics. (2005). Massachusetts Medicaid Facts. Accessed: May 9, 2007. http://www.aap.org/advocacy/washing/elections/mfs_ma.pdf
Feinberg, E., Swartz, K., Zaslavsky, A. M., Gardner, J., & Walker, D. K. (2002). Language proficiency and the enrollment of medicaid-eligible children in publicly funded health insurance programs. Maternal & Child Health Journal, 6(1), 5–18.
Kenney, G., & Haley, J. (2007). Why Aren’t More Uninsured Children Enrolled in Medicaid or SCHIP? 2001. The Urban Institute. Accessed: May 10, 2007. http://www.urban.org/UploadedPDF/310217_ANF_B35.pdf
Perry, M., Kannel, S., Valdez, R. B., & Chang C. (2000). Medicaid and Children Overcoming Barriers to Enrollment Findings from a National Survey. The Kaiser Commission on Medicaid and the Uninsured. Accessed: May 10, 2007. http://www.kff.org/medicaid/loader.cfm?url=/commonspot/security/getfile.cfm&PageID=13449
Davidoff, A., Kenney, G., & Dubay, L. (2005). Effects of the state children’s health insurance program expansions on children with chronic health conditions. Pediatrics, 116(1), e34–e42.
Health Resources and Services Administration, Maternal and Child Health Bureau. (2005). Title V Information System, State Needs Assessments, Massachusetts MCH Needs Assessment 2005. Accessed: May 7, 2007. https://perfdata.hrsa.gov/MCHB/MCHReports/documents/NeedsAssessments/2006/MA-NeedsAssessment.pdf
Kurland, J., & Walker, D. W. (2004). Funding Cuts to Public Health in Massachusetts: Losses over Gains. Massachusetts Health Policy Forum. Accessed: May 1, 2007. http://masshealthpolicyforum.brandeis.edu/publications/pdfs/21-Jul04/IB%20FundCutsLossesGains%2021.pdf
Na’im, A., & Wagman, N. (2005). Kids, Cuts, and Consequences: How Cuts to Effective Programs Hurt Our Children. The Massachusetts Budget and Policy Center. Accessed: May 1, 2006. http://www.massbudget.org/KidsCutsandConsequences.pdf
Bovbjerg, R. R. (2005). State Case Study: Medicaid and the 2003–2005 Budget Crisis-A Look At How Massachusetts Responded. Kaiser Commission on Medicaid and the Uninsured. Accessed: May 9, 2007. http://www.kff.org/medicaid/upload/State-Case-Study-Medicaid-and-the-2003-05-Budget-Crisis-A-Look-At-How-Massachusetts-Responded-Report.pdf
Community Catalyst. (2006). Massachusetts Health Reform: What it does, How it was done, The Challenges Ahead. Boston, MA: Community Catalyst, Inc. April 21, 2006. Accessed June 12, 2006. http://www.communitycatalyst.org/resource.php?base_id=1023
Acknowledgments
Massachusetts Consortium for Children with Special Health Care Needs Family Participation Workgroup for their enthusiasm and contributions to this project and Nancy Wilber, EdD, Massachusetts Department of Public Health for information regarding the service systems in Massachusetts for children with special health care needs. Source of Support: The Deborah Munroe Noonan Memorial Fund.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hill, K.S., Freeman, L.C., Yucel, R.M. et al. Unmet Need among Children with Special Health Care Needs in Massachusetts. Matern Child Health J 12, 650–661 (2008). https://doi.org/10.1007/s10995-007-0283-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-007-0283-3