
Abstract
The urgency to develop a vaccine against the 2019 coronavirus (COVID-19) has waxed stronger in speed, scale, and scope. However, wisdom dictates that we take a vantage position and start to examine the demographic predictors of COVID-19 vaccine hesitancy. The objective of this study was to examine the role of health locus of control (HLOC) in the relationship between religiosity and COVID-19 vaccination intention. In a cross-sectional survey (N = 501), we found a significantly negative association between religiosity and COVID-19 vaccination intention. This relationship was partially mediated by external HLOC. Collaborative efforts with religious institutions may influence COVID-19 vaccine uptake.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The novel 2019 coronavirus (COVID-19) has expanded to over 170 countries (WHO 2020). As of April 13, 2020, there has been a report of 1,773,084 cases and 111,652 deaths globally, with the USA leading in the number of cases (CDC 2020). The devastating impacts of this pandemic on lives, healthcare systems, social wellbeing, and the economy have led to the introduction of several mitigating measures such as regional lockdown, hygiene promotion, social distancing, travel restrictions, and vaccine development research (Wilder-Smith and Freedman 2020). Although containment measures and prevalence estimations are necessary to mitigate the impact of the virus and calibrate epidemiological responses, wisdom dictates that we take a vantage position, and start to examine the predictors of the COVID-19 vaccine hesitancy. This approach will stir up proactive measures and mobilize collaborative action among key stakeholders.
Researchers across various settings (academia, biotech, pharmaceuticals, and military) fervently work toward developing a vaccine against COVID-19. As the death toll rises, these efforts are likely to increase in intensity and speed (Lurie et al. 2020). More than $1 billion has been committed to its actualization, and at least two companies have already launched clinical trials (Amanat and Krammer 2020). While the progress and dedication pose promise for swiftly developing a vaccine, the news of vaccination against COVID-19 has already received mixed reactions from the general public. Recent findings suggest that vaccine misinformation has been communicated through conspiracy stories and myths (Singh et al. 2020). For instance, a famous COVID-19 vaccine conspiracy story that has been actively propagated through social media is about the 5G network (Lee 2020). This widely spread story speculates that the COVID-19 vaccine is an attempt by some powerful US corporations to insert a nanotechnology microchip that will allow humans to be controlled. This myth has been further adapted by some religious leaders to represent the end time sign of the mark of the anti-Christ (Pulpit and Pen 2020; Robins and Baxter 2020). Also, in the Muslim community, the COVID-19 vaccine has been portrayed as a “Western plot” to sterilize Muslim women (Ali 2020). It is therefore important to proactively investigate the likely predictors of COVID-19 hesitancy among religious groups and start to mobilize key actors within existing religious, scientific, and political structures toward a common goal of vaccination.
Religious Coping During Stressful Events
During stressful life events, adversities, and uncertainties, religion offers a source of relief as a means for coping with uncertainty (Koenig et al. 1997). Religious coping involves relying on one’s faith, not just for refuge and comfort, but also for possible explanations. Empirical evidence suggests that during tragic events, much emphasis is placed on prayer, scripture readings, and closeness to God as the way out of the crisis (Pargament 2001; Tix and Frazier 1998). For instance, in March 2020, an analysis of Google searches showed that for each 80,000 reported COVID-19 case, the Google search for “prayer” doubled (Bentzen 2020).
While religion assists in coping with life stressors, studies have also demonstrated religiosity to be strongly and positively correlated with trust in informal sources of information such as religious organization’s website, spiritual leaders, and family/friends (Cacciatore et al. 2018; Scheitle et al. 2018). However, the content of these informal sources may be contradictory to scientific evidence. In the USA, the tensions between science and religion are evident. Scientifically, individuals with high levels of religiosity are more likely to hold negative views toward scientific innovations and nanotechnology (Cacciatore et al. 2018; McPhetres and Zuckerman 2018; Scheufele et al. 2009). Therefore, while religion offers a source of comfort, higher levels of engagement in religious practices may unintentionally spread misinformation, yielding unsafe practices. During the era of COVID-19, misinformation regarding the disease and religious activities (e.g., “it is safe to gather for religious ceremonies because God will protect us”) may uniquely position highly religious individuals to engage in behaviors which risk greater community spread and death (Pereira 2020). Taken together, it is imperative to examine the role that religiosity plays during the COVID-19 pandemic such that information regarding COVID-19 vaccines (once available) is received positively by all communities, including those high in religiosity.
Religiosity and COVID-19 Vaccination
Previous studies have shown that religiosity is a strong predictor of anti-vaccine beliefs. For example, in a study among American Muslim physicians, respondents who sought bioethical guidance from Islamic juridical authorities had lower odds of recommending porcine-based flu vaccination to their patients (Mahdi et al. 2016). Also, Utah, where Mormon religion is dominant, and 74% of the residents rated themselves as being “highly religious” is ranked 46th in the nation as up to date with Human papillomavirus vaccination (Walker et al. 2017; Wormald 2015). A common determinant of vaccine acceptance among religious people is health locus of control-HLOC (Amit Aharon et al. 2018; Sinding Bentzen 2019; Wilson et al. 2016). HLOC is the extent of perception that each person has about the important factors that govern their health or illness (Wallston et al. 1978). Two domains of locus of health control (LOC) have been identified as internal and external LOC (Wallston 2005). Individuals who believe that they can positively influence their health outcomes (internal LOC) may actively seek preventive services such as vaccination. However, external LOC is the belief that a person’s health depends on external factors such as God, chance, or Powerful others. In a recent path analysis model among Jewish and Muslim parents, external HLOC was shown to be positively associated with low childhood vaccine uptake through parents’ attitudes (Amit Aharon et al. 2018). Nevertheless, weighing the virulent nature of COVID-19 against the existing evidence that religious individuals may offer explanations to a crisis by referencing it as “an Act of God of which humans have no control over” (Sinding Bentzen 2019), it is uncertain how HLOC will mediate the relationship between religiosity and COVID-19 vaccination intention.
Current Study
This current study seeks to take an anticipatory perspective in the ongoing efforts toward the management of COVID-19 by (i) examining the relationship between religiosity and intention to receive the COVID-19 vaccine if/when there is one, and (ii) assessing the mediating role of health locus of control in the relationship between religiosity and COVID-19 vaccination intention. We hope to provide highly informative empirical evidence that will stir up conversations, proactive preparation, and mobilization among religious leaders, clinicians, healthcare workers, and communication experts toward the likelihood of COVID-19 vaccine hesitancy.
Methods
To satisfy our study objectives, we deployed a survey tool with validated screening techniques for a rapid assessment of the relationship between religiosity and COVID-19 vaccination intention. This study was approved by the Institution Review Board of the University of Illinois at Chicago. All participants signed the online informed consent form before proceeding with the survey.
Study Sample
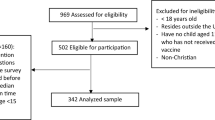
We recruited study participants via Prolific, an online crowdsourcing platform for researchers (Peer et al. 2017). Prolific has been shown to have a reputable and reliable track record of diverse participant pool and high data quality. Compared to other online recruitment platforms, participants from Prolific scored higher on attention-checks, engaged in lesser dishonest behavior, and reproduced existing results (Palan and Schitter 2018; Peer et al. 2017). We had 2 eligibility criteria for participation (i) residence in the USA and (ii) being 18 years or older. Cross-sectional data were collected from 502 participants on March 22, 2020, through the Qualtrics online survey link. Each participant received an incentive of $0.55 after survey completion.
Measures
Assessment of Religiosity
Religiosity was measured using the Duke University Religion Index (DUREL), which has been used in over 100 studies (Koenig and Büssing 2010). This 5-item scale captures three major domains of religiosity—the organizational, non-organizational, and intrinsic religiosity. This measure has demonstrated a high 2-week test–retest reliability of 0.91, reliable internal consistency (α = 0.78–0.91), and a convergent validity with other established measures of religiosity (r’s = 0.71–0.86). An example of an item on the scale is “My religious beliefs are what really lie behind my whole approach to life.” Response options ranged from definitely yes [1] to definitely not [5]. A reverse coding was performed such that higher values represented higher religiosity.
Assessment of Religious Affiliation
Religious affiliation was measured with a single item asking participants, “What is your religious affiliation?” Possible response categories were Catholic, Protestant, Adventist, Mormon, Islam, Buddhism, Hinduism, Agnostic, Atheist, and others (Dollinger 2001).
Assessment of Trust in Informal Sources of Information
Three items were used to assess trust in informal sources of information (Liao et al. 2011). The items were (i) Social media reports can be trusted, (ii) The best source of information about coronavirus is to watch and listen to what others say, and (iii) I tend to believe what my friends, colleagues, or neighbors say about coronavirus. Responses were reversely coded such that they ranged from strongly disagree [1] to strongly agree [5].
Assessment of Perceived Effectiveness of Religious Practices
The perceived effectiveness of prayer and scripture reading in protecting against COVID-19 were each assessed with a single item. Participants were asked, “What are your beliefs about the effectiveness or ineffectiveness of the following in preventing coronavirus?” (i) Prayer, and (ii) Scripture reading. Responses ranged from completely effective [1] to completely ineffective [5].
Assessment of Health Locus of Control
The measure of HLOC was based on the Multidimensional Health Locus of Control (MHLC) scale (α = 0.70; Wallston et al. 1978). Specifically, we measured the external LOC by adopting the following (i) No matter what I do, if I am going to get sick, I will get sick (ii) God controls whether one falls sick or not (iii) If it is meant to be, I will stay healthy. Responses were assessed on a 5-point Likert scale strongly agree [1] to strongly disagree [5]. Responses were reversely coded and averaged to range from 1 to 5 with low numbers indicating low external HLOC.
Assessment of Personal Believes Against Vaccination in General
Participants were asked if they had personal beliefs against vaccination in general. Response categories were Yes and No.
Assessment of COVID-19 Vaccination Intention
COVID-19 vaccination intention was assessed with a single item that asked participants, “If there is a preventive vaccine against COVID-19, how likely are you receive the vaccine?” Responses were assessed on a 5-point Likert scale ranging from extremely unlikely [1] to extremely likely [5].
Demographics
Since COVID-19 vaccination intention and religiosity are likely to be influenced by key demographics (e.g., age, household income), we collected key demographic variables for statistical control (Amit Aharon et al. 2018; Pashak et al. 2020). More specifically, participants reported on the following important demographic characteristics: age (continuous variable), sex (female, male) race (White, African American, Asian, Hispanic, American Indian, Middle East and North Africa (MENA) and others), and marital status. For marital status, categories included married, divorced, separated, widowed, and single/never married. Socioeconomic status (SES) factors included household income (< $20,000, $20,000 to < $35,000, $35,000 to < $50,000, $50,000 to < $75,000, and $75,000 or more); employment status, and education (less than high school, high school graduate, some college, college graduate or more).
Data Analysis
Participants’ characteristics were analyzed using descriptive statistics such as frequencies (and their proportions) and means (and their standard deviations). The one-way analysis of variance (ANOVA) was performed to investigate the mean differences in religiosity and COVID-19 vaccination intention by participants’ characteristics. Pearson correlations were calculated to test bivariate associations between the continuous variables. To further investigate the relationship between religiosity and COVID-19 vaccination intention, multivariable analysis was conducted. Model 1 tested the unadjusted relationships, Model 2 controlled for sociodemographic factors, and Model 3 added the SES variables. Statistical tests were 2-sided, and a P < .05 was considered statistically significant. Effect sizes and their confidence intervals, as suggested by Cumming (2014), were reported to interpret findings (Cumming 2014). Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Mediation Analysis
Mediation analysis with 1000 bootstrap resamples was conducted to test the possible mediating role of external HLOC in the relationship between religiosity and COVID-19 vaccination intention. Regression models were fitted in four steps according to the procedures outlined by Sobel to assess the mediating role of external HLOC (Sobel 1982). The purpose of steps 1–3 was to examine the zero-order relationships among the variables. However, as recommended by Hayes, religiosity was not required to demonstrate a significant overall zero-order association with the COVID-19 vaccination intention (Hayes 2009) in testing for mediation. This contemporary approach was chosen because of the possibility of the direct and indirect (meditational) paths operating in opposite directions, which can result in a nonsignificant total exposure-outcome association (Erdem et al. 2016).
Sensitivity Analysis
We conducted a sensitivity analysis to further test the robustness of our model under varying methodological conditions. One of the three items that assessed external HLOC was found to overlap with our measure of religiosity (DUREL) conceptually; hence, we conducted our analysis with the three items and with 2 of the three items to probe its impact on the effect size estimates. Sensitivity analysis was not used to choose an alternate conclusion to our study. Instead, our conclusions were based on the primary analysis, and the sensitivity analysis finding was presented to demonstrate the consistency of the primary findings (Thabane et al. 2013).
Results
After excluding one participant who failed the attention check (Table 1), the remaining participants (N = 501) reported a mean age of 32.44 ± 11.94 years, being females (55.29%), White (67.86%), single/never married (68.46%), college graduate or more (53.71%), and employed (54.89%). Participants reported a household income of over $75,000 (35.67%), personal belief against vaccines in general (3.79%), and religious affiliation as protestant (20.16%) and Agnostic (21.96%).
We recorded means (Table 2) of religiosity (2.09 ± 1.17), external HLOC (3.73 ± 0.97) and COVID-19 vaccination intention (4.24 ± 1.04), trust in informal sources of information (2.57 ± 0.76), effectiveness of prayer in protecting against COVID-19 was 1.98 ± 1.36. Mean vaccination intention by participants’ characteristics (Table 1) showed that participants who were Black/African American (3.53 ± 1.43), unemployed/retired/disabled/others (4.10 ± 1.15), with personal belief against vaccines in general (2.63 ± 1.57) had lower COVID-19 vaccination intention. Pearson’s correlation analysis (Table 2) showed that religiosity was positively correlated with external HLOC (r = 0.47; P < 0.001) and negatively correlated with COVID-19 vaccination intention (r = − 0.17; P < 0.001).
In Model 1 (Table 3), we found a significantly negative association between COVID-19 vaccination intention and (i) religiosity (β = − 0.15; 95% Confidence Interval (CI) = − 0.23 to − 0.08; P < 0.0001) and (ii) external HLOC (β = − 0.24; 95% CI = − 0.33 to − 0.15; P < 0.0001). These relationships remained significant in Model 2 for religiosity (β = − 0.13; 95% CI = − 0.21 to − 0.05; P = 0.0009) and external HLOC (β = − 0.20; 95% CI = − 0.30 to − 0.11; P < 0.0001). In Model 3 COVID-19 vaccination intention was also significantly and negatively associated with religiosity (β = − 0.14; 95% CI = − 0.22 to − 0.06; P = 0.0003) and external HLOC (β = − 0.20; 95% CI = − 0.29 to − 0.10; P < 0.0001).
Standardized mediation tests showed that external HLOC mediated 40.97% of the relationship between religiosity and COVID-19 vaccination intention (Fig. 1) with an indirect effect of β = − 0.06; 95% CI = − 0.11 to − 0.02; P = 0.006. After conducting a sensitivity analysis (Fig. 2), external HLOC mediated 22.04% of the relationship with an indirect effect of β = − 0.03 (− 0.06 to − 0.01; P = 0.02).

Mediation analysis: external health locus of control mediated 40.97% of the effect of religiosity on intention to vaccinate against COVID-19 with 1000 bootstrap resamples β = − 0.06, SE = 0.02. Bias-corrected 95% Confidence interval (− 0.11 to − 0.02)

Mediation test from the sensitivity analysis: external health locus of control mediated 22.04% of the effect of religiosity on intention to vaccinate against COVID-19 with 1000 bootstrap resamples β = − 0.03, SE = 0.01. Bias-corrected 95% Confidence interval (− 0.06 to − 0.01)
Discussion
In this analysis, religiosity was significantly and negatively associated with intention to vaccinate against COVID-19. Our findings suggest that external HLOC can serve as a pathway through which this association exists. Notably, the non-significance of the indirect effect in our primary analysis and its significance in the sensitivity analysis suggests that there is a conceptual overlap between the measures of religiosity and the external locus of control. Hence, this association should be interpreted with caution when both measures are used. However, the outcome of the sensitivity analysis (where the methodological, conceptual overlap is corrected) further lends credence to the possibility of a partial mediation of external locus of control in the relationship between religiosity and COVID-19 vaccine intention (Sjölander and Zetterqvist 2017). The results of this study confirm the principles of religious coping, which associates responses to stressful life events with external HLOC such that the crisis may be viewed as an Act of God that cannot be changed or prevented (Sinding Bentzen 2019). Furthermore, the novel coronavirus disease has been marked with rapid consumption of health information from informal sources (e.g., social media, religious website, family, friends and colleagues), which are prone to the dissemination of unclear, false or misleading health information and myths or conspiracy theories (Cuan-Baltazar et al. 2020; Kouzy et al. 2020). Hence, a possible explanation for our findings may be that highly religious individuals trust informal information sources (as evident in our result) whose contents may be dominated by anti-COVID-19 vaccination messages.
We, therefore, offer the following recommendations: first, religious leaders should consider educating their members on the need to take responsibility for their health. One way of doing this is to find scriptural contents that emphasize that individuals have a role to play regarding their lives and health outcomes (Harris et al. 1999; Holt et al. 2009; Le et al. 2018). Drawing on such scriptural themes can provide a faith-based justification for strengthening the internal health locus of control rather than leave health outcomes to chance because, if people consider themselves to be responsible for their health outcome, they are more likely to take up preventive measures such as vaccine uptake (Wallston 2005).
Second, since previous studies have established that religious leaders have a strong influence on their followers (Cacciatore et al. 2018; McPhetres and Zuckerman 2018; Scheufele et al. 2009), we strongly propose that as scientists scramble for the development of a COVID-19 vaccine, they also establish a strong partnership with religious institutions through their leaders. This working relationship should be rooted in the transparency of the ongoing vaccine development processes. If religious leaders are familiar with and have strong confidence in the vaccine development processes, they may use informal informational platforms to communicate scientifically valid messages regarding COVID-19 vaccine.
Finally, it is important to note that our study included adults, and if parents have a negative disposition toward the COVID-19 vaccine, they may also prevent their children from taking the vaccine (Amit Aharon et al. 2018). This premise has an implication for policymakers who may further examine the likelihood of vaccine uptake among various demographic groups and offer policy recommendations for COVID-19 vaccine acceptance. For example, in our study, African American participants reported a significantly low COVID-19 vaccination intention. Hence, in the stimulation of public response toward COVID-19 vaccine uptake, there is a need for multi-stakeholder collaboration that will cut across religious groups, community organizations, healthcare practitioners, media organizations, and policymakers. This collaborative effort may ensure that people receive the right information that will strengthen their health locus of control and allow them to take responsibility regarding their protection.
Limitations
Our study is not without its limitations. First, our sample consists mostly of young, educated adults and is therefore not generalizable across the USA; hence, it should be interpreted with caution. Second, the use of a cross-sectional study design makes it challenging to establish causality and requires a careful interpretation of our results. The novelty of the COVID-19 pandemic offers limited opportunity for comparing data at multiple data points. However, as more evidence emerges, further studies should longitudinally examine the pathways through which religiosity influences the likelihood of COVID-19 vaccine uptake.
Conclusion
In this study of 501 participants, external health locus of control mediated the relationship between religiosity and COVID-19 vaccination intention. As scientists scramble for the development of a COVID-19 vaccine, it is important also to establish a strong partnership with religious institutions that may be very instrumental in positively shaping the narrative around health locus of control and vaccine uptake among their members.
References
Ali, I. (2020). The COVID-19 Pandemic: Making Sense of Rumor and Fear: Op-Ed. Medical Anthropology, 39, 1–4.
Amanat, F., & Krammer, F. (2020). SARS-CoV-2 vaccines: status report. Immunity, 52, 583–589.
Amit Aharon, A., Nehama, H., Rishpon, S., & Baron-Epel, O. (2018). A path analysis model suggesting the association between health locus of control and compliance with childhood vaccinations. Human Vaccines & Immunotherapeutics, 14(7), 1618–1625.
Bentzen, J. S. (2020). In Crisis, We Pray: Religiosity and the COVID-19 Pandemic (CEPR Discussion Papers No. 14824). C.E.P.R. Discussion Papers. https://EconPapers.repec.org/RePEc:cpr:ceprdp:14824.
Cacciatore, M. A., Browning, N., Scheufele, D. A., Brossard, D., Xenos, M. A., & Corley, E. A. (2018). Opposing ends of the spectrum: Exploring trust in scientific and religious authorities. Public Understanding of Science, 27(1), 11–28.
CDC. (2020). Coronavirus Disease 2019 (COVID-19) in the U.S. Centers for Disease Control and Prevention. Retrieved from 17 March 2020. https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html.
Cuan-Baltazar, J. Y., Muñoz-Perez, M. J., Robledo-Vega, C., Pérez-Zepeda, M. F., & Soto-Vega, E. (2020). Misinformation of COVID-19 on the internet: Infodemiology study. JMIR Public Health and Surveillance, 6(2), e18444. https://doi.org/10.2196/18444.
Cumming, G. (2014). The new statistics. Psychological Science, 25(1), 7–29. https://doi.org/10.1177/0956797613504966.
Dollinger, S. J. (2001). Religious identity: An autophotographic study. The International Journal for the Psychology of Religion, 11(2), 71–92.
Erdem, G., DuBois, D. L., Larose, S., De Wit, D., & Lipman, E. L. (2016). Mentoring relationships, positive development, youth emotional and behavioral problems: Investigation of a mediational model: Mentoring and positive youth development. Journal of Community Psychology, 44(4), 464–483. https://doi.org/10.1002/jcop.21782.
Harris, A. H. S., Thoresen, C. E., Mccullough, M. E., & Larson, D. B. (1999). Spiritually and religiously oriented health interventions. Journal of Health Psychology, 4(3), 413–433. https://doi.org/10.1177/135910539900400309.
Hayes, A. F. (2009). Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Communication Monographs, 76(4), 408–420.
Holt, C. L., Wynn, T. A., Litaker, M. S., Southward, P., Jeames, S. E., & Schulz, E. K. (2009). A comparison of a spiritually based and non-spiritually based educational intervention for informed decision making for prostate cancer screening among church-attending African–American men. Urologic Nursing, 29(4), 249.
Koenig, H. G., & Büssing, A. (2010). The Duke University Religion Index (DUREL): A five-item measure for use in epidemological studies. Religions, 1(1), 78–85. https://doi.org/10.3390/rel1010078.
Koenig, H. G., Hays, J. C., George, L. K., Blazer, D. G., Larson, D. B., & Landerman, L. R. (1997). Modeling the cross-sectional relationships between religion, physical health, social support, and depressive symptoms. The American Journal of Geriatric Psychiatry, 5(2), 131–144.
Kouzy, R., Abi Jaoude, J., Kraitem, A., El Alam, M. B., Karam, B., Adib, E., et al. (2020). Coronavirus goes viral: Quantifying the COVID-19 misinformation epidemic on Twitter. Cureus, 12(3), e7255. https://doi.org/10.7759/cureus.7255.
Le, D., Aldoory, L., Garza, M. A., Fryer, C. S., Sawyer, R., & Holt, C. L. (2018). A spiritually-based text messaging program to increase cervical cancer awareness among African American women: Design and development of the CervixCheck Pilot Study. JMIR Formative Research, 2(1), e5. https://doi.org/10.2196/formative.8112.
Lee, B. Y. (2020). 5G Networks And COVID-19 Coronavirus: Here Are The Latest Conspiracy Theories. Forbes. Retrieved from 14 April 2020 https://www.forbes.com/sites/brucelee/2020/04/09/5g-networks-and-covid-19-coronavirus-here-are-the-latest-conspiracy-theories/.
Liao, Q., Cowling, B. J., Lam, W. W. T., & Fielding, R. (2011). The influence of social-cognitive factors on personal hygiene practices to protect against influenzas: Using modelling to compare Avian A/H5N1 and 2009 Pandemic A/H1N1 influenzas in Hong Kong. International Journal of Behavioral Medicine, 18(2), 93–104. https://doi.org/10.1007/s12529-010-9123-8.
Lurie, N., Saville, M., Hatchett, R., & Halton, J. (2020). Developing COVID-19 vaccines at pandemic speed. New England Journal of Medicine, 382(21), 1969–1973.
Mahdi, S., Ghannam, O., Watson, S., & Padela, A. I. (2016). Predictors of physician recommendation for ethically controversial medical procedures: findings from an exploratory national survey of American Muslim physicians. Journal of Religion and Health, 55(2), 403–421.
McPhetres, J., & Zuckerman, M. (2018). Religiosity predicts negative attitudes towards science and lower levels of science literacy. PLoS ONE, 13(11), e0207125.
Palan, S., & Schitter, C. (2018). Prolific. ac—A subject pool for online experiments. Journal of Behavioral and Experimental Finance, 17, 22–27.
Pargament, K. I. (2001). The psychology of religion and coping: Theory, research, practice. New York: Guilford Press.
Pashak, T. J., Justice, M. D., Burns, B. R., Lahar, K. I., Handal, P. J., & Creech, C. (2020). Separation of Church and Trait: Trait death anxiety is universal, distressing, and unbuffered by worldview in emerging adults. Journal of Religion and Health, 59(2), 725–742. https://doi.org/10.1007/s10943-018-0623-1.
Peer, E., Brandimarte, L., Samat, S., & Acquisti, A. (2017). Beyond the Turk: Alternative platforms for crowdsourcing behavioral research. Journal of Experimental Social Psychology, 70, 153–163. https://doi.org/10.1016/j.jesp.2017.01.006.
Pereira, I. (2020). Ongoing religious services spark debate over faith versus safety. ABC News. Retrieved from 16 April 2020. https://abcnews.go.com/Health/ongoing-religious-services-spark-debate-faith-verses-safety/story?id=69943088.
Pulpit and Pen. (2020). Charismatic prophet says coronavirus vaccine will be mark of the beast. Pulpit and Pen. Retrieved from 14 April 2020. https://pulpitandpen.org/2020/03/14/charismatic-prophet-says-coronavirus-vaccine-will-be-mark-of-the-beast/.
Robins, D., & Baxter, I. (2020). Is Bill Gates preparing to administer the mark of the beast? Endtime Ministries | End of the Age | Irvin Baxter and Dave Robbins. Retrieved from 14 April 2020. https://www.endtime.com/podcast/is-bill-gates-preparing-to-administer-the-mark-of-the-beast/.
Scheitle, C. P., Johnson, D. R., & Ecklund, E. H. (2018). Scientists and religious leaders compete for cultural authority of science. Public Understanding of Science, 27(1), 59–75.
Scheufele, D. A., Corley, E. A., Shih, T., Dalrymple, K. E., & Ho, S. S. (2009). Religious beliefs and public attitudes toward nanotechnology in Europe and the United States. Nature Nanotechnology, 4(2), 91–94. https://doi.org/10.1038/nnano.2008.361.
Sinding Bentzen, J. (2019). Acts of God? Religiosity and natural disasters across subnational world districts. The Economic Journal, 129(622), 2295–2321.
Singh, L., Bansal, S., Bode, L., Budak, C., Chi, G., Kawintiranon, K., et al. (2020). A first look at COVID-19 information and misinformation sharing on Twitter. arXiv preprint arXiv:2003.13907.
Sjölander, A., & Zetterqvist, J. (2017). Confounders, mediators, or colliders. Epidemiology, 28(4), 540–547.
Sobel, M. E. (1982). Asymptotic confidence intervals for indirect effects in structural equation models. Sociological Methodology, 13, 290–312.
Thabane, L., Mbuagbaw, L., Zhang, S., Samaan, Z., Marcucci, M., Ye, C., et al. (2013). A tutorial on sensitivity analyses in clinical trials: the what, why, when and how. BMC Medical Research Methodology, 13(1), 92. https://doi.org/10.1186/1471-2288-13-92.
Tix, A. P., & Frazier, P. A. (1998). The use of religious coping during stressful life events: main effects, moderation, and mediation. Journal of Consulting and Clinical Psychology, 66(2), 411.
Walker, T. Y., Elam-Evans, L. D., Singleton, J. A., Yankey, D., Markowitz, L. E., Fredua, B., et al. (2017). National, regional, state, and selected local area vaccination coverage among adolescents aged 13–17 years—United States, 2016. MMWR. Morbidity and Mortality Weekly Report, 66(33), 874–882. https://doi.org/10.15585/mmwr.mm6633a2.
Wallston, K. A. (2005). The validity of the multidimensional health locus of control scales. Journal of Health Psychology, 10(5), 623–631. https://doi.org/10.1177/1359105305055304.
Wallston, K. A., Strudler Wallston, B., & DeVellis, R. (1978). Development of the multidimensional health locus of control (MHLC) scales. Health Education Monographs, 6(1), 160–170.
WHO. (2020). Coronavirus disease 2019 (COVID-19) Situation Report 84 (No. 84). https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200413-sitrep-84-covid-19.pdf?sfvrsn=44f511ab_2.
Wilder-Smith, A., & Freedman, D. O. (2020). Isolation, quarantine, social distancing and community containment: pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. Journal of Travel Medicine. https://doi.org/10.1093/jtm/taaa020.
Wilson, A. R., Hashibe, M., Bodson, J., Gren, L. H., Taylor, B. A., Greenwood, J., et al. (2016). Factors related to HPV vaccine uptake and 3-dose completion among women in a low vaccination region of the USA: An observational study. BMC Women’s Health, 16(1), 41.
Wormald, B. (2015). Religious landscape study. Pew Research Center’s Religion & Public Life Project, 11.
Acknowledgements
We are grateful to Professor David DuBois for his advice on this paper.
Funding
None.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Ayokunle Olagoke and Ashley Hughes. The first draft of the manuscript was written by Ayokunle Olagoke and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
No conflict of interest pertinent to this research existed for the investigators.
Human Participants and/or Animals Rights
This article does not contain any studies with animals performed by any of the authors. Ethical approval was obtained from the Institution review board of the University of Illinois at Chicago. The procedures used in this study, involving human participants, adhered to the tenets of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
Standard procedures for obtaining consent and maintaining the confidentiality and anonymity of participants were instituted. Informed consent was obtained from all individual participants included in the study.
Ethics Approval
Approval was obtained from the ethics committee of the University of Illinois at Chicago. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent to Publish
The participants consented to the dissemination of the study findings through scholarly publications.
Financial or Non-financial Interests
No such interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Ayokunle Olagoke (MPH) founded Health Disseminate, a non-governmental organization on knowledge translation of public health research. She is a doctoral candidate at the Department of Community Health Sciences, School of Public Health, University of Illinois, Chicago. She is the founder and Minister in Charge of Friends Bible Study, an online non-denominational group with over 5000 total attendance since 2019 (https://sites.google.com/site/icallufriendz/home?authuser=0). She has worked as a Media Consultant to the Johns Hopkins public health initiative in Africa, funded by Bill and Melinda Gates Foundation. Her current project is the development of a Scripture-embedded message to improve human papillomavirus vaccination among religious parents.
Rights and permissions
About this article

Cite this article
Olagoke, A.A., Olagoke, O.O. & Hughes, A.M. Intention to Vaccinate Against the Novel 2019 Coronavirus Disease: The Role of Health Locus of Control and Religiosity. J Relig Health 60, 65–80 (2021). https://doi.org/10.1007/s10943-020-01090-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-020-01090-9