
Abstract
Theistic and spiritually based beliefs and behaviors have been demonstrated to consistently predict physical and mental health, although the psychological processes underlying these relationships are unclear. This study investigated associative relationships and pathways of mediation between religious functioning, locus of control (LOC) and health. The sample consisted of 122 Christians (79 women, 43 men) who were predominately Catholic, ranging in age from 18 to 80 (M = 45.47, SD = 15.0). Participants were recruited from churches in the Western suburbs of Melbourne, Australia, and completed a questionnaire package measuring (1) psychological and physical health, (2) the religious variables of awareness of God, instability and impression management, and (3) God, internal and external LOC domains. Results indicated that awareness of God and internal LOC were associated with better health, whereas external LOC and instability were associated with poorer health. God LOC and impression management were not significantly associated with health. Sobel tests were used to analyse mediation hypotheses. Internal LOC was found to mediate the relationship between awareness of God and better psychological health, and external LOC was found to mediate the relationship between instability and poorer psychological health. These findings are of considerable clinical significance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Prominent author and psychiatrist Scott Peck wrote, “Psychiatry is, I believe, currently in a predicament. I call it a predicament because its traditional neglect of the issue of spirituality has lead to … inadequate research and theory” (Peck 1993, p. 278). This observation underscores the contention that without a psychological understanding of spirituality and religion, modern psychology is inhibiting its potential to understand human thoughts, beliefs and actions (Peck). Yet it has only been somewhat recently that psychologists and academics have engaged this topic extensively, either theoretically or empirically. Indeed, study of the influence of religious faith on both psychological and physical health has escalated in recent years, accompanied by increasingly sophisticated empirical methodology. Early studies in this field were limited by small samples and simple statistical analysis, such as associations between church attendance and mortality rates (e.g., Dwyer et al. 1990; Levin and Vanderpool 1989; Meyers et al. 1992). However, consistent findings have provided an impetus for further exploration of the relationships between elements of religiosity and health. In particular, individual psychological factors potentially related to religious or spiritual functioning are increasingly becoming a focus for scrutiny as possible mediators between religiosity and health. It is towards this purpose that the psychological construct of locus of control is examined in this study.
Defining ‘religion’ and ‘spirituality’ is fraught with difficulty and varies substantially between academic disciplines. At a psychological level of analysis, both terms may be taken in some sense to refer to a set of beliefs, attitudes and/or behaviors, which reflect an understanding or acknowledgement of something numinous (i.e., deity, life force, etc.), which is beyond and/or greater than the individual, and which potentially influences or is able to be influenced by the individual. In this context, using a Christian sample, we will refer to such beliefs, attitudes and behaviors as aspects of ‘religious functioning’ and undertake to operationalise this form of psychological functioning with respect to specific psychometric instruments.
Locus of Control and Health
An extensive amount of research has investigated locus of control (LOC) of reinforcement as a predictor of health. LOC can be defined as a general belief about whether rewards are the result of one’s own actions, or a product of an external entity/force. Specifically, the literature suggests that an internal LOC is a belief that reinforcements are contingent upon personal effort; and higher endorsements of this belief are generally linked with improved physical and psychological health (Armstrong and Boothroyd 2008; Pannells and Claxton 2008). An external LOC is an expectation that reinforcements/rewards are the result of external forces such as luck, fate or the actions of powerful others. Research has consistently linked external LOC with psychological distress and dysfunctional behavior, as well as poorer mental and physical health (Lauer et al. 2008). Indeed, high levels of external LOC are frequently implicated in depression and anxiety disorders (Kennedy et al. 1998; Presson and Bensassi 1996).
Internal and external LOC were originally formulated by Rotter (1966) to represent the end points of a unidimensional continuum. However, there is evidence to suggest an internal–external dichotomy, respectively, linked to better or poorer health, may be an over-simplification in some contexts (e.g., O’Hea et al. 2009). Subsequent developments of the LOC construct have often incorporated multiple external dimensions (for example Levenson’s (1981) scale distinguishes between ‘chance’ and ‘powerful other’ dimensions of externality), and many have also included a God LOC subscale (e.g., Wallston et al. 1999). Indeed, effect sizes in a large number of studies attest to the health benefits of endorsing a God LOC. These findings underscore the importance and relevance of general LOC to overall health, and suggest a potential pathway for the association between religious functioning and health.
Religious Functioning and Health
Perhaps as a consequence of the ambiguity which surrounds the multidisciplinary definition of religion, there are currently over 100 measures exploring aspects of religious and spiritual life (see Hill and Hood 1999). For our study, we have sought a Christian sample and in order to provide a clear operationalisation of religious functioning, we have adopted the Spiritual Assessment Inventory developed by Hall and Edwards (2002); however, only three of the variables comprising this scale were utilised: awareness of God, impression management and instability.
Awareness of God is a construct that captures how strongly a person feels the presence of a God in daily life (Hall and Edwards 1996). Unlike miraculous religious experiences (such as out-of-body experiences), it measures the intensity of one’s faith in a theistic context. Individuals with high levels of awareness of God believe their relationship with God will protect and guide them (Hall and Edwards) and thus can be expected to be more optimistic and confident. The attributes that make up an awareness of God (i.e., belief in divine guidance, a sense of God’s presence and assistance from divine sources) have been linked with improved psychological health (Benson and Spilka 1973; Hood 1992; Koenig et al. 1998; Pargament 1997).
Impression management assesses the degree to which a person practises (or has an inclination to practise) meritorious spiritual behavior, such as praying. Constructs of this nature have also shown an affinity with improved health (Benson and Spilka 1973; Ellison et al. 2001; Koenig 1998; Lawler-Row and Elliott 2009). Originally, the impression management subscale was designed to identify respondents who exaggerated their religious beliefs, possibly in an attempt to give socially desirable answers. However, the creators of the spiritual assessment inventory also suggest that the subscale could be used to measure the frequency and intensity of behaviors and attitudes that pertain to a religious context (T. W. Hall, personal communication, May 5, 2009). There are multiple explanations for why religious practices are associated with improved health, most suggesting that religious acts have qualities that serve as a buffer against stress or anxiety (Seybold and Hill 2001). There are, however, also a few studies that link religious practice with poorer health outcomes (Larson et al. 1992; Seybold and Hill 2001; Thune-Boyle et al. 2006).
Indeed, the final religious variable to be examined here is instability, which reflects anxiety that stems from religious beliefs. This specific form of anxiety could be described as a fear of abandonment or punishment from God, and has been linked with unhealthy psychological issues such as intense feelings of guilt and shame, as well as an external LOC (Benson and Spilka 1973; Meadow and Kahoe 1984; Ziebertz et al. 2001). This form of religious functioning, however, does not feature in the literature nearly as frequently as the more positive attributes of religiosity; thus, this variable in particular has been neglected by researchers.
Mediation Analysis: The Link Between Religious Functioning, LOC and Health
Several studies have sought to determine potential mediational relationships between religiosity, health and LOC. Wigert (2001) hypothesised that the relationship between LOC and health was mediated by religious commitment, however, no mediating effect was found. Wigert’s attempt to find an indirect effect possibly failed for two reasons. First, Wigert used a model of religious functioning that has been heavily criticised and deemed invalid by multiple studies (Brewczynski and MacDonald 2006; Kirkpatrick and Hood 1990; Pargament 1992). Second, LOC was treated as a moderating rather than mediating factor. However, the second study seeking mediation was more successful. Fiori et al. (2006) revealed that an external LOC mediated the effect between religiosity and improved psychological health. However, as stated by Fiori et al., the unexpected link between higher external LOC and improved psychological health may have been due to issues regarding measurement. For instance, external LOC and psychological health were measured with just three questions each, while internal LOC was measured with just two questions. Furthermore, religious functioning was not divided into its various elements; thus, there was no way of determining which element of religious functioning was moderating the relationship. Most details regarding the psychometric properties of the scales used were absent in the article; therefore, no clinical implications could be drawn from the study.
Rationale and Aims of the Study
Potential mediatory relationships between LOC, health and religious functioning remain, therefore, unclear and largely unexplored. Furthermore, research investigating religious functioning in problem solving and its relation to general health reveals both a positive and negative potential. It might well be argued that specific elements of religious functioning, such as instability, will be associated with an external LOC and that more positive elements of religious functioning, such as awareness of God, will be associated with an internal LOC. This study aimed to explore these relationships.
It was hypothesised, in the first instance, that higher scores on variables of internal LOC, God LOC, awareness of God and impression management would correlate with better psychological and physical health scores. Furthermore, it was predicted that higher scores on variables of external LOC and instability would be associated with poorer psychological and physical health. Third, it was hypothesised that an awareness of God would predict improved health and that this would be mediated by internal LOC. Finally, it was hypothesised that instability would predict poorer health and that this would be mediated by external LOC.
Method
Participants
The sample comprised 122 Christians (76% Catholic, 10% Anglican, 14% other denominations). Of these participants, 65% were women, 35% men; ages ranged from 18 to 80 (M = 45.47, SD = 15.0). Ethnic backgrounds were divided into five categories: 40% were Caucasian, 12% were south-east Asian (i.e., Malaysian, Filipino, Indonesian, etc.), 10% were southern European (i.e., Italian, Maltase, Greek, etc.), 7% were south Asian (i.e., Indian, Pakistani or Sri Lankan) and 31% were either mixed, or gave no response. Respondents were also asked to indicate their marital status: 69% were married, 20% were single, 8% were in a relationship, 1% in a de facto relationship and 2% were divorced. Additionally, participants had an average of 14.75 years of schooling and/or tertiary education (SD = 3.6 years). Most of the participants were residents of the Western suburbs of Melbourne, Australia, and none were paid or reimbursed in any manner for their involvement.
Materials
All participants completed a battery of questionnaires relating to the following variables. Health was measured using the psychological and physical health subscales of the World Health Organisation’s WHOQoL BREF (Skevington et al. 2004). The WHOQoL BREF contains 26 questions divided into four categories: psychological, physical, social and environmental. The WHOQoL BREF defines psychological health essentially as the absence of symptoms pertaining to depression, anxiety and general psychopathology. Physical health is conceptualised as an ability to meet the physical requirements of one’s lifestyle. The WHOQoL BREF is ideal for research due to its clarity, brevity and cross-cultural applicability. Internal consistency has been verified with Cronbach’s α > .80, as well as acceptable discriminant and construct validity (Skevington et al.).
Locus of control was assessed with the Belief in Personal Control Scale (Berrenberg 1987). This test was selected for the present study because it distinguishes internal, external and God LOC dimensions. Internal consistency is strong with Cronbach’s α > .85 across the three factors, and construct validity has been established with high correlations with several theoretically related measures (Berrenberg).
Religious functioning was assessed using Hall and Edwards’ (2002) Spiritual Assessment Inventory (SAI). The SAI differs from other religious scales in that it measures both positive and negative elements of religious functioning (cf. WHOQoL SRPB Group 2002). Exploratory and confirmatory factor analysis in addition to correlations with other well-established religious scales provides empirical support for the validity of the SAI (Hall and Edwards). Internal consistency has also been confirmed with Cronbach’s α > .77. Only the subscales of awareness, instability and impression management were utilised to assess religious functioning. The subscales of realistic acceptance, disappointment and grandiosity were excluded from this study.
Procedure
After obtaining approval from the RMIT Human Research Ethics Committee, a large representation of Christian parishes in the Western suburbs of Melbourne was approached for permission to publicly appeal for volunteers during Sunday services. Before any public appeals, however, written consent was gained from the parish’s priest/minister. Following approval from several parishes, participants were asked just prior to the conclusion of Sunday mass/service if they would like to take part in the study. All participants were issued a plain language statement that clearly outlined relevant information, such as participants’ rights and the purpose of the study. Additionally, since no identifying information was collected, all participants were informed that their responses would be anonymous.
The majority of participants took the questionnaire home and sent it back to the researcher using a provided reply-paid envelope. A few, however, did complete the questionnaire immediately after the mass/service and handed it directly to the researcher. Approximately 400 questionnaires were handed out over a 6-week period, and 122 were completed and returned. The questionnaire took approximately 15 minutes to complete and contained 190 questions. While not all the questions from various instruments were used in the current analysis, non-relevant questions were kept to preserve the reliability and validity of the individual scales within the questionnaire. Statistical analysis was conducted using the Statistical Package for the Social Sciences (SPSS), version 17. In addition to the standard features of SPSS, a software add-on was used to test for pathways of mediation. The software add-on was written by Kristopher Preacher and Andrew Hayes; all technical details regarding the software can be found in the corresponding article (see Preacher and Hayes 2004).
Results
Preliminary analysis of the data used the total sample to obtain descriptive statistics (Table 1) and to create a correlational matrix (Table 2). Significant Pearson’s correlations (i.e., relationships where P < .05) were identified. Importantly, higher levels of instability were strongly correlated with both poorer psychological and physical health. Conversely, higher levels of an awareness of God were found to have a moderately positive relationship with improved psychological but not physical health. Furthermore, impression management and God LOC were not significantly correlated with either health variable. A significant positive correlation was found between an awareness of God and internal LOC; God LOC also positively correlated with internal LOC; additionally, instability positively correlated with external LOC. Given the multiple significant relationships between variables, mediation analysis was undertaken.
Prior to conducting the mediation analysis, the data were examined to ensure that the assumptions underlying the mediation analysis were not violated. First, an examination of the correlational matrix confirmed the absence of excessively high correlations among predictors (i.e., relationships exceeding ±.80) and therefore supported the independence of predicting variables (Field 2003). Additionally, residual scatterplots, Cook’s distance and Mahalanobis values were utilised to test for outliers; results revealed that one case needed to be removed (Pallant 2009). Finally, assumptions regarding normality, homoscedasticity and independence of residuals were confirmed using scatterplots (Pallant).
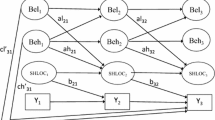
The first mediation model predicted that internal LOC would mediate the relationship between an awareness of God and psychological health; Sobel’s equation revealed a significant mediating effect, z = 2.30, P = .02. Preacher and Hayes’ (2004) procedure was used to reveal that 3.46% of the variance in psychological health could be explained by this indirect effect (see Fig. 1). The second mediation model predicted that external LOC would mediate the relationship between instability and psychological health; Sobel’s equation for mediation revealed a significant effect, z = −2.64, P = .01. Thus, Preacher and Hayes’ procedure followed and revealed that 9.35% of the variance in psychological health was explained by this mediating effect (see Fig. 2).

The first model of mediation. A theory-driven model in which internal LOC mediated the relationship between awareness of God and psychological health

The second model of mediation. A theory-driven model in which external LOC mediated the relationship between instability and psychological health
Discussion
This study sought to evaluate relationships between religious functioning, locus of control, and physical and mental health. Results largely confirmed all four hypotheses insofar as significant associations between elements of religious functioning, LOC and indices of health were found. Additionally, hypotheses predicting that LOC would mediate observed relationships between religious functioning and health were also substantively supported.
Religious Functioning, LOC and Associations With Health
In accord with the first hypothesis and previous literature (Armstrong and Boothroyd 2008; Pannells and Claxton 2008), internal LOC positively correlated with better psychological and physical health, although awareness of God correlated positively only with psychological health. Possible directional relationships between these variables will be discussed during examination of the third hypothesis. The results also revealed that God LOC and impression management did not significantly predict health (psychological or physical) and thus failed to support the first hypothesis and previous research (Benson and Spilka 1973; Ellison et al. 2001; Goggin et al. 2007; Jenkins and Pargament 1988; Koenig 1998; Krause 2005; Lawler-Row and Elliott 2009; Wallston et al. 1999). It is not entirely clear why God LOC did not yield significant associations with health scores. Considering that God LOC did produce a non-significant positive relationship with psychological health, it might well be argued that this study lacked sufficient statistical power to reveal a significant relationship with psychological health. In other words, factors such as the size of the sample may have contributed to a type-II error. Interestingly, God LOC (which might theoretically be construed as a form of external, ‘powerful others’, LOC) was positively correlated with internal LOC. Given also that God LOC and awareness of God were strongly correlated (r = .70), it may be that the construct of God LOC requires further clarification both theoretically and empirically. Similarly, impression management did not significantly correlate with either psychological or physical health. A possible explanation for this outcome is that the subscale has not been used previously as a measure of religious activities and involvement. Thus, the subscale may be more useful as a gauge of test-taker attitude.
The second hypothesis was supported by the finding that health scores were strongly (and negatively) associated with both SAI instability and external LOC and therefore corroborates established links in the literature (Benson and Spilka 1973; Kennedy et al. 1998; Lauer et al. 2008; Meadow and Kahoe 1984; Presson and Bensassi 1996; Ziebertz et al. 2001). Possible directional relationships between these variables will be discussed at length during the examination of the fourth hypothesis.
In summary, results relevant to the first two hypotheses revealed both positive and negative health associations with different elements of religious functioning. These differential findings are theoretically meaningful and warrant further elaboration in subsequent discourse and research regarding both detrimental and/or beneficial aspects of the relationship between religiosity and health.
Models of Mediation
Internal LOC was found to mediate the relationship between SAI awareness of God and psychological health, supporting the third hypothesis. While previous research has observed consistent associative relationships between religious functioning, LOC and health (Meadow and Kahoe 1984), the present study is the first to reveal an internal LOC mediatory effect. Similar associations with religious functioning and health have also been found with the variable of coping method. For example, Pargament (1997) observed that positive mental health was best associated with individuals who not only utilised a self-directed approach to problem solving but also felt that God was assisting. Indeed, the link between awareness of God and internal LOC becomes more apparent with an examination of the SAI. For example, one of the items measuring awareness of God is, “When I consult God about decisions in my life, I am aware of his directions and help”. Theoretically, individuals who score highly on such items use their religious beliefs to strengthen their internal LOC, since God is less ‘external reinforcement contingency’ in this context and more ‘mentor and advisor’ (in line with the ‘collaborative style’ of religious coping suggested by Pargament et al. 1988; see also Francis 2009). With respect to Hall and Edwards’ (2002) SAI utilised for the current study, individuals with high levels of awareness of God believe their relationship with God will protect and guide them and thus can be expected to be more optimistic and confident. It follows that such individuals would be more likely to endorse an internal LOC. Therefore, on the basis of the mediation model supported here, it is postulated that an awareness of God fosters an internal LOC, and an internal LOC in turn leads to improved health.
Finally, support was also found for the fourth hypothesis (second model of mediation) when results indicated that external LOC mediated the relationship between SAI instability and psychological health. As described, the Hall and Edwards dimension of instability reflects anxiety that develops from religious beliefs. This specific form of anxiety could be described as a fear of abandonment or punishment from God and has been linked with unhealthy psychological issues such as intense feelings of guilt and shame. In this conceptualisation, instability is characterised by a strong belief that some events and circumstances are controlled by God and thus also a belief of reduced personal control over the environment or future. Further, people with high levels of SAI instability fear punishment from God and therefore suffer feelings of insecurity. Such patterns mirror personality studies that link neuroticism with external LOC (e.g., Brosschot et al. 1994); indeed, an opportunity for future research would be to include personality in the assessment of religious functioning to distinguish the unique effects of various individual factors. Thus, the results for the second mediation model suggest that SAI instability may foster an external LOC, and external LOC in turn leads to less positive psychological health. In summary, the current findings support well-established connections between internal and external locus of control and better and poorer health, respectively. Furthermore, it has been determined that, consistent with past research, there is potential for both positive and negative effects of religious functioning on physical and mental health. This study contributes to the understanding that at least some of these positive and negative effects of religious functioning on health are in fact mediated by internal and external LOC, respectively.
General Limitations
In this study, it was found that internal LOC was associated with health benefits, while external LOC was associated with poorer health outcomes. God LOC showed non-significant relationships with health but was positively correlated with internal LOC. On the face of it, this might seem at odds given that God is typically conceived of as a ‘powerful other’. The construct of God LOC therefore requires further clarification both theoretically and empirically. While the classification of religious coping styles propounded by Pargament et al. (1988) provides important insights (see also Francis 2009), a clearer and more specific operationalisation of God LOC is required in the literature. This should also consider the potential adaptiveness of an external LOC in some situations, in the same way that Pargament et al. (1988) ‘surrendering style’ is posited to provide relief, comfort and security in highly stressful situations.
Future studies would benefit from the use of multiple and diverse religious groupings, as well as an atheistic control group to more accurately determine the health benefits or costs of religious functioning. Here, we have focussed on a single faith group in order to clearly elaborate the proposed relationships between variables. We are therefore unable to generalise our findings freely to other faith groups or spiritual orientations. Indeed, it is unclear as to whether the sample from this study is representative of Christians more generally as well. Considering that the sample was predominately Catholic and from one geographical area, it is not possible to say (at least presently) whether the results apply broadly.
Implications, Future Research and Conclusions
Notwithstanding these limitations, there are several implications that can be drawn from the results. Previous literature hailing the salutary effects of religious functioning has frequently assumed the benefits stemmed from the ‘positive experience’ (Seybold and Hill 2001). For instance, religious functioning provides health benefits through accrued social support, intellectual stimulation, emotional soundboarding, and so forth. While possibly true, the bases for these types of explanations are generally speculative and/or anecdotal, and lack empirical rigour. Additionally, such speculation fails to explain cases that associate religious functioning with poorer health.
This study sheds light on this apparent paradox by revealing differential health effects of both positive and negative components of religious functioning, and also highlights the potential LOC pathways for explaining at least part of this effect. While analysis of the data revealed that the first (SAI awareness of God) and second (SAI instability) models of mediation explained only 3.46 and 9.35% of variance in psychological health, respectively, these are not dissimilar to the magnitude of variance accounted for by religious variables in previous studies. For instance, a meta-analysis of 34 studies by Hackney and Sanders (2003) revealed religious functioning was associated with improved psychological health with an average effect size of .12 (95% confidence intervals .11, .13).
The findings from this study highlight a potential strategy for therapists. Symptoms of poor mental health may have roots embedded within a spirito-religious belief system. Thus, therapists may need to address less favourable elements of religious functioning and consider, particularly, how beliefs influence a client’s LOC paradigm. Moreover, the results from this study support claims that religious functioning can ameliorate symptoms of poor mental health or even help avoid mental illness altogether (Koenig 2008). Therefore, it follows that religious educators and spiritual counselors should emphasise the positive and empowering elements of religious functioning. However, findings from the present study do require replication, and future studies should consider simultaneously the influence of other psychological factors such as personality, as well as more broadly addressing aspects of physical health as well.
The psychology of religion and spirituality presents a plethora of opportunities for future research, with potential to contribute importantly to our understandings of both mental health and psychopathology. Given that more than three-quarters of the world’s population can be described as either spiritual or religious, the findings from this field of research are potentially of great significance and broadly relevant and applicable.
References
Armstrong, M., & Boothroyd, R. (2008). Predictors of emotional well-being in at-risk adolescent girls: Developing preventive intervention strategies. The Journal of Behavioral Health Services and Research, 35(4), 435–453.
Benson, P., & Spilka, B. (1973). God image as a function of self-esteem and locus of control. Journal for the Scientific Study of Religion, 12, 297–310.
Berrenberg, J. L. (1987). The belief in personal control scale: A measure of God-mediated and exaggerated control. Journal of Personality Assessment, 51(2), 194–206.
Brewczynski, J., & MacDonald, D. (2006). Confirmatory factor analysis of the Allport and Ross religious orientation scale with a Polish sample. International Journal for the Psychology of Religion, 16, 63–76.
Brosschot, J. F., Gebhardt, W. A., & Godaert, G. L. (1994). Internal, powerful others and chance locus of control: Relationships with personality, coping, stress and health. Personality and Individual Differences, 16(6), 839–852.
Dwyer, J. W., Clarke, L. L., & Miller, M. K. (1990). The effect of religious concentration and affiliation on county cancer mortality rates. Journal of Health and Social Behaviour, 31, 185–202.
Ellison, C., Boardman, J. D., Williams, D. R., & Jackson, J. S. (2001). Religious involvement, stress and mental health: Findings from the 1995 Detroit area study. Social Forces, 80, 215–235.
Field, A. (2003). Discovering statistics using SPSS for windows. London: Sage Publications.
Fiori, K. L., Brown, E. E., Cortina, K. S., & Antonucci, T. C. (2006). Locus of control as a mediator of the relationship between religiosity and life satisfaction: Age, race and gender differences. Mental Health Religion and Culture, 9(3), 239–263.
Francis, A. J. P. (2009). Locus of control. In D. A. Leeming, K. Madden, & S. Marlan (Eds.), Encyclopedia of psychology and religion. New York: Springer.
Goggin, K., Murray, T. S., Malcarne, V. L., Brown, S. A., & Wallston, K. A. (2007). Do religious and control cognitions predict risky behavior? I. Development and validation of the Alcohol-related God Locus of Control Scale for Adolescents (AGLOC-A). Cognitive Therapy and Research, 31(1), 111–122.
Hackney, C. H., & Sanders, G. S. (2003). Religiosity and mental health: A meta-analysis of recent studies. Journal for the Scientific Study of Religion, 42, 43–55.
Hall, T. W., & Edwards, K. J. (1996). The initial development and factor analysis of the spiritual assessment inventory. Journal of Psychology and Theology, 24(3), 233–246.
Hall, T. W., & Edwards, K. J. (2002). The spiritual assessment inventory: A theistic model and measure for assessing spiritual development. Journal for the Scientific Study of Religion, 41(2), 341–357.
Hill, P. C., & Hood, R. W. (Eds.). (1999). Measures of religiosity. Birminghamd, AL: Religious Education Press.
Hood, R. W. (1992). Sin and guilt in faith traditions: Issues for self-esteem. In J. F. Schumaker (Ed.), Religion and mental health (pp. 110–121). New York: Oxford University Press.
Jenkins, R. A., & Pargament, K. I. (1988). Cognitive appraisals in cancer patients. Social Science and Medicine, 26, 625–633.
Kennedy, B. L., Lynch, G. V., & Schwab, J. J. (1998). Assessment of locus of control in patients with anxiety and depressive disorders. Journal of Clinical Psychology, 54(4), 509–515.
Kirkpatrick, L. A., & Hood, R. W. (1990). Intrinsic-extrinsic religious orientation: The boon or bane of contemporary psychology of religion? Journal for the Scientific Study of Religion, 29, 442–462.
Koenig, H. G. (Ed.). (1998). Handbook of religion and mental health. San Diego, CA: Academic Press.
Koenig, H. G. (2008). Medicine religion and health: Where science and spirituality meet. West Conshohocken, PA: Templeton Foundation Press.
Koenig, H. G., Pargament, K. I., & Nielsen, J. (1998). Religious coping and health status in medically ill hospitalized older adults. Journal of Nervous and Mental Disease, 189, 513–521.
Krause, N. (2005). God-mediated control and psychological well-being in late life. Research on Aging, 27(2), 136–164.
Larson, D. B., Sherrill, K. A., Lyons, J. S., Craigie, F. C., Thielman, S. B., Greenwold, M. A., et al. (1992). Associations between dimensions of religious commitment and mental health reported in the American Journal of Psychiatry and Archives of General Psychiatry: 1978–1989. American Journal of Psychiatry, 149, 557–559.
Lauer, S., Man, A., Marquez, S., & Ades, J. (2008). External locus of control, problem-focused coping and attempted suicide. North American Journal of Psychology, 10(3), 625–633.
Lawler-Row, K. A., & Elliott, J. (2009). The role of religious activity and spirituality in the health and well-being of older adults. Journal of Health Psychology, 14, 43–52.
Levenson, H. (1981). Differentiating among internality, powerful others, and chance. In H. M. Lefcourt (Ed.), Research with the locus of control construct (pp. 15–63). New York: Academic Press.
Levin, J. S., & Vanderpool, H. Y. (1989). Is religion therapeutically significant for hypertension? Social Science and Medicine, 29, 69–78.
Meadow, M. J., & Kahoe, R. D. (1984). Psychology of religion: Religion in individual lives. New York: Harper and Row.
Meyers, M. S., Altmaier, E. M., & Burns, C. P. (1992). Religious orientation and coping with cancer. Journal of Religion and Health, 31, 273–279.
O’Hea, E. L., Moon, S., Grothe, K. B., Boudreaux, E., Bodenlos, J. S., Wallston, K., et al. (2009). The interaction of locus of control, self-efficacy, and outcome expectancy in relation to HbA1c in medically underserved individuals with type 2 diabetes. Journal of Behavioral Medicine, 32(1), 106–117.
Pallant, J. (2009). SPSS survival manual (3rd ed.). Crows Nest, Australia: Allen and Unwin.
Pannells, T. C., & Claxton, A. F. (2008). Happiness, creative ideation, and locus of control. Creativity Research Journal, 20(1), 67–71.
Pargament, K. I. (1992). Of means and ends: Religion and the search for significance. The International Journal for the Psychology of Religion, 2, 201–229.
Pargament, K. I. (1997). The psychology of religion and coping. New York: Guilford Press.
Pargament, K. I., Kennell, J., Hathaway, W., Grevengoed, N., Newman, J., & Jones, W. (1988). Religion and the problem-solving process: Three styles of coping. Journal for the Scientific Study of Religion, 27, 90–104.
Peck, M. S. (1993). Further along the road less travelled. London: Simon and Schuster.
Preacher, K. J., & Hayes, A. F. (2004). SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behaviour Research Methods, instruments and computers, 36(4), 717–731.
Presson, P. K., & Bensassi, V. A. (1996). Locus of control orientation and depressive symptomatology: A meta-analysis. Journal of Social Behavior and Personality, 11, 201–212.
Rotter, J. B. (1966). Generalized expectancies for internal versus external control of reinforcement. Psychological Monographs, 80(609).
Seybold, K. S., & Hill, P. C. (2001). The role of religion and spirituality in mental and physical health. Current Directions in Psychological Science, 10, 21–24.
Skevington, S. M., Lotfy, M., & O’Connell, K. A. (2004). The World Health Organsiation’s WHOQoL BREF quality of life assessment: Psychometric properties and results of the international field trial. Quality of Life Research, 13, 299–310.
Thune-Boyle, I. C., Stygall, J. A., Keshtgar, M. R., & Newman, S. P. (2006). Do religious/spiritual coping strategies affect illness adjustment in patients with cancer? A systematic review of the literature. Social Science and Medicine, 63, 151–164.
Wallston, K., Malcarne, V. L., Flores, L., Hansdottir, I., Smith, C. A., Stein, M. J., et al. (1999). Does God determine your health? The God locus of health control scale. Cognitive Therapy and Research, 23(2), 131–142.
WHOQOL SRPB Group. (2002). WHOQOL spirituality, religiousness and personal BelieF. Geneva, Switzerland.
Wigert, L. R. (2001). An investigation of the relationships among personality traits, locus of control, religious orientation and life satisfaction: A path analytical study. Retrieved from ProQuest Digital Dissertations (ATT 3028663).
Ziebertz, H. G., Schweitzer, F., Haring, H., & Browning, D. (2001). The human image of God. Leiden, The Netherlands: Brill.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ryan, M.E., Francis, A.J.P. Locus of Control Beliefs Mediate the Relationship Between Religious Functioning and Psychological Health. J Relig Health 51, 774–785 (2012). https://doi.org/10.1007/s10943-010-9386-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-010-9386-z