
Abstract
This article examines the degree to which various demographic characteristics, personality traits, and environmental factors are associated with overall emotional well-being of 125 adolescent girls whose mothers were involved in welfare reform. Daughters participated in a 4-year, mixed method study and annually completed a structured interview protocol and a sub-group also completed a qualitative interview. The quantitative findings from the study suggest that daughters having an internal locus of control, experiencing fewer negative life events, and reporting stronger parental and teacher social support had enhanced emotional well-being over the 4-year study compared to daughters without these factors. The findings were further elaborated with examples from qualitative interviews conducted with the daughters. The findings were used to propose prevention activities using a tertiary mental health preventive intervention framework.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
When Congress passed the Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA, P.L. 104–193)1 in 1996, welfare in America was dramatically changed. Known as the Temporary Assistance for Needy Families Program (TANF), the goal of this legislation was to assist recipients in becoming economically self-sufficient. The legislation included mandated work requirements for welfare recipients and services such as child care, transportation, and vocational training to assist recipients in their transition to work.1
Much of the initial welfare reform research focused on maternal outcomes such as employment and earnings with little emphasis placed on children.2 Furthermore, most of the early research on children focused on younger children who were perceived as most vulnerable to the effect of mothers’ work requirements. Substantially less attention was placed on adolescents.3 A meta-analysis of 16 randomized control studies3 assessed the effects of various welfare reform programs on adolescents aged 12 to 18 raising cause for concern. In each study, a number of parents were assigned to programs that included a combination of three common welfare reform strategies: mandatory employment, earnings supplements, and limits on welfare receipt, whereas other parents were randomly assigned to control groups. Follow-up periods ranged from 24 to 60 months after random assignment. The outcome measures in most of the studies focused on school performance and school-related behaviors. Three ethnographies3 provided context for the quantitative findings. The results of their analysis indicate that parents of youths in the welfare reform programs reported poorer school performance, higher rates of grade retention, and greater use of special education services compared to parents in the control groups. Furthermore, they found that adolescents with siblings experienced even worse outcomes as they were also more likely to be suspended or expelled from school and to drop out. No single reform initiative could explain the programs’ adverse effects on the adolescents. The authors concluded that adolescents’ school performance was negatively affected by various welfare and work policies and that these effects were compounded by the inflexibility inherent in many of the jobs filled by low-income individuals that often increased the challenges associated with being a single parent. They recommend that TANF programs work more closely with parents who are transitioning into employment and that new programs be tested for low-income youths and their families.
Of further concern is the fact that findings from some studies suggest that these negative effects may be even more devastating to girls.4 Such findings have resulted in investigators stressing the need for early interventions to assist girls in “breaking the cycle”.5 For example, in the study of Furstenberg,6 it is noted that even though 80% of the daughters of welfare mothers do not become dependent themselves, they are more likely to receive welfare (approximately 20%) compared to daughters of nonwelfare mothers (about 3%). Other investigators,7 however, attribute this increased rate to the powerful effects of poverty and single parenthood.
Regardless of which side of this debate one assumes, one issue is clear. Poverty has a negative impact on adolescents, and early findings from studies on welfare reform suggest that these initiatives may be deleterious to adolescents. Growing up poor is significantly associated with, among other things, poorer health and mental health outcomes,8 – 10 an increased likelihood of teenage pregnancy11 and substance involvement.12
Adolescents living in poverty often encounter other risk factors that may predispose them to mental health problems as well as protective factors that may modify this predisposition. The constructs of risk and protective factors are related to resilience, a youth’s capacity to use internal and external resources to successfully master stage-specific developmental issues.13 Resilience is conceptualized as a process—a capacity that develops over time through transactions of the individual with their environment. A review of the literature on stress, coping, and resilience in children14 concluded that resilience is defined in three ways. First, resilience is equated with coping, defined as efforts to restore or maintain equilibrium in the presence of significant stress. Second, resilience is conceptualized as the ability to recover in the face of trauma. Third, resilience is defined as protective factors or mechanisms that mediate the relationship between risk and competence. Various authors have proposed that the construct of child resilience includes two essential factors: the presence of serious threats to adaptation or development, and the achievement of positive adaptation and good outcomes.15 – 17 The need to use a developmental perspective is a common theme in theoretical frameworks for child resilience. A developmental perspective takes into account the youth’s developmental level and functioning, the multiple levels of influence on a child’s developmental pathways, and the reciprocity between the risk and protective factors and the youth’s adjustment.
Previous studies have demonstrated that parents and peer groups are relatively more important than neighborhood influences on the behaviors of urban African-American adolescents18 and that maternal involvement, the support of extended family members, and socialization regarding future orientation are important predictors of adolescents’ future orientation.19 Both direct and indirect pathways for the role of parents’ values in shaping adolescents’ occupational aspirations have been found for African-American and white youths.20
In this article, a tertiary model of universal, selected, and indicated preventive mental health intervention strategies21 is proposed that is informed by the empirical findings regarding the factors that are associated with the emotional well-being of a sample of 125 adolescent girls growing up in families receiving welfare. Through this analysis, the relationship between the risk and protective factors in these daughters’ lives, how these factors impact their emotional well-being over the course of the study, and how to develop strategies to help mitigate these negative effects can be better understood. This study assists in determining what services and supports are helpful to teenage girls in making a successful and productive transition into adulthood. The study is unique in that it examined the emotional well-being of these adolescents as opposed to examining school performance and other indicators commonly addressed in studies about welfare reform.
Methods
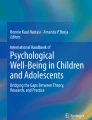
This mixed-method study consisted of two phases. Phase 1 involved structured interviews conducted with 125 mothers receiving TANF and their daughters using standardized measures (only data from the interviewed daughters are reported in this article). Phase 2 involved more intensive follow-up qualitative interviews conducted with a small sample of daughters who participated in phase 1. As shown in Figure 1 and based on a review of the literature on child resilience, the interview protocol included measures assessing risk and protective factors in the areas of personality traits (e.g., self-esteem, locus of control), family situation (e.g., parental relationships, family structure), and community environment (e.g., neighborhood violence, church, school, social supports).

Conceptual model.
Participants
In phase 1 during the first year of this study, a sample of 125 mothers in the Tampa Bay, Florida area, who were receiving TANF and their adolescent daughters aged 13–17, were identified from the 2000–2001 Florida Medicaid eligibility file using the family identifier and other matching variables (such as gender, address, and last name). The sample size of 125 pairs was originally selected to produce results within a ±8% margin of error with 95% confidence. Every year of this 4-year study, attempts were made to recontact and reinterview all 125 mothers and daughters.
In phase 2 of the first year of this study, a random sample of 20 girls was selected from among the phase 1 participants to complete a more comprehensive qualitative follow-up interview. Every year, attempts were made to conduct comprehensive qualitative interviews with these same 20 adolescents.
Participant selection and recruitment
Approximately 1,300 mothers receiving TANF with daughters thought to be between the ages of 13 and 17 were identified from the 2000–2001 Florida Medicaid eligibility file using a family identifier and other matching variables. Letters were mailed to 875 of these women, explaining the purpose of the study and that they might be contacted for possible participation in the study. To ensure diversity among study participants, the sample was stratified on race/ethnicity and urban/rural locations throughout the Tampa Bay, Florida region. Nearly 26% of the letters (n = 227) were returned due to incorrect addresses or because individuals had moved out of the state. Of the 648 women contacted, 340 (52%) had left the TANF rolls and 128 (20%) had daughters who were past their 18th birthday, therefore being ineligible to participate in the study. Approximately 8% of those contacted (n = 50) refused to enroll in the study, and 125 (19%) were enrolled in the study. The remaining 1% (n = 5) were never contacted as the desired sample size was reached.
Follow-up interview retention rates and attrition analysis
In longitudinal studies such as this, subject attrition presents significant methodological challenges. High follow-up retention rates are needed to ensure the validity of the study. Table 1 summarizes the phase-1 and phase-2 follow-up interview rates for the daughters.
Across the 4 years, phase-1 follow-up retention rates for daughters exceeded 88% in each year and averaged 91.2% over the 3-year follow-up period. Overall, completed phase-1 interviews were conducted with 81.6% across all 4 years. For the remaining 18.4%, completed phase-1 interviews were obtained for 10.4% of the daughters in 3 of the 4 years, 6.4% in 2 of the 4 years, and only two daughters (1.6%) were unable to be reinterviewed after the first year of the study. The follow-up rates for daughters participating in phase 2 were 90.0% or higher in each year, averaging 91.7% over the course of the study.
Table 2 compares the characteristics of daughters who were successfully interviewed during each year of the study with the characteristics of daughters who were interviewed on a less frequent basis. As shown in the table, no significant differences were found between daughters interviewed each year and those who were not regarding their age, race/ethnicity, whether they were attending school at the start of the study, or in their overall emotional well-being across the 4 years of the study (the dependent variable in this study).
Study design
The goal of phase 1 was to identify factors associated with these daughters’ emotional well-being using a highly structured interview process that incorporated a number of standardized measures. Interviews lasted between 1 and 1 1/2 hours. In phase 2, in-depth qualitative interviews were conducted with 20 daughters who participated in phase 1. These interviews were open-ended and explored in greater detail many of the same factors assessed in phase 1 regarding how these daughters were fairing.
Data collection instruments and methods
In phase 1 of this study, daughters completed annual structured interviews that contained previously developed and psychometrically tested measures assessing various domains associated with risk and protective factors. The protocol collected demographic data consistent with the minimum data standards established by the National Institute of Mental Health21 regarding client characteristics. In addition, these interviews collected information regarding the types of support that daughters perceived would be most beneficial in assisting them in successfully transitioning into adulthood independent of involvement with the welfare system.
Sixteen variables were used to predict daughters’ emotional well-being over this 4-year study. Predictors included several demographic variables and various risk and protective factors commonly cited in the literature22 presented in Figure 1. More specifically, the predictors included daughter demographic information (three variables: age, being black, being another minority race), relationship with father (one variable), school performance (one variable), perceived safety (one variable), quality of the neighborhood (one variable), religiousness (one variable), family functioning (one variable), locus of control (one variable), self-esteem (one variable), life events (one variable), and social support (four variables).
The dependent variable in the study (i.e., daughters’ emotional well-being) was assessed using a composite variable constructed from four measures assessing the daughters’ mental health status. Each of the variables used as predictor or to construct the composite dependent variable for this analysis is briefly described below.
Predictor variables
Self-reported daughter’s demographic information (i.e., age, race/ethnicity) was obtained during the first interview. Daughter’s self-reported responses to single items were used to assess their relationships with their fathers, school performance, perceived safety, and quality of their neighborhoods.
Religiousness/Spirituality was assessed using the religious intensity scale from the Brief Multidimensional Measure of Religiousness and Spirituality (BMMRS23). The two-item scale asks respondents to report the strength of the religiousness/spirituality using a 4-point scale ranging from “not at all” to “very”. The scale has good internal consistency reliability (0.71). For this analysis, the scale was recoded so that higher scores are indicative of greater religiousness.
Family functioning was assessed using the general functioning scale from the Family Assessment Device (FAD24). Scale scores were recoded so that higher scores indicated greater family functioning. The internal consistency of the general functioning scale is good, ranging between 0.83 and 0.86, and the scale also has adequate test–retest reliability at 0.71.25 – 27 The measure has low correlations with social desirability and moderate correlations with other self-report measures of family functioning, which provides evidence of concurrent validity of the scale.26 Discriminative validity was also demonstrated by clinical ratings, indicating that families rated by the clinicians as unhealthy also had significantly higher family mean scores, representing poorer functioning.26
The children’s version of the Nowicki–Strickland Locus of Control Scale (N–SLCS28) was used to assess the daughters’ locus of control. This popular measure has been used in over 1,000 studies and published in more than two dozen languages.29 The N–SLCS scale is a 40-item self-report measure in which respondents answer yes/no to each question. Higher scores on the N–SLCS reflect more external locus of control (lower scores reflect a more internal locus of control). The corrected split half reliability for grades 9–11 was 0.81, and the 6-week test–retest reliability was 0.71 for grade 10.28
Daughter’s self-esteem was assessed using the 10-item Rosenberg Self-Esteem Scale (RSES30). Respondents answer each question using a 4-point scale ranging from “strongly agree” to “strongly disagree”. Although originally developed as a Guttman scale, the RSES is now scored as a Likert scale. The RSES has good internal consistency reliability ranging from 0.74 to 0.8830 – 33 as well as good test–retest reliability ranging between 0.82 and 0.88.30 , 31 , 34
Significant life events that the daughters had experienced were assessed using the Children’s Life Events Inventory (CLEI35). The CLEI is a 40-item self-report measure of both positive and negative experiences. The scale was scored so that lower scores were reflective of having experienced fewer traumatic events. The authors conclude that the raters’ “estimates of the relative severity of the life event for children are very reliable” (for a review, see the work of Monaghan et al.35 (p. 66)
The four social support variables were derived from the Social Support Scale for Children (SSSC36). This 24-item self-report measure is designed to assess the degree to which the youths perceive support and regard from parents, teachers, close friends, and classmates. The internal consistency of the subscales is good, ranging from 0.72 to 0.88, and has adequate validity.36 , 37 Higher scores were indicative of greater levels of social support.
Dependent variable
Each year, three different indicators of daughters’ emotional well-being were obtained. These measures were used to construct a composite variable of daughters’ emotional well-being across the 4 years of the study. The measures used to develop the composite included the: (1) Center for Epidemiologic Studies Depression Scale (CES-D38) which was administered each year, (2) Pediatric Symptom Checklist (PSC39) which was administered in years 1–3 and was replaced by the Colorado Symptom Index (CSI40) in year 4 for age appropriateness reasons, and (3) a single self-report item of perceived mental health need. This composite was used as the dependent variable in a regression analysis to identify what factors were predictive of these youths’ overall emotional well-being.
In each year of the study, daughters completed the CES-D38 which is a 20-item self-report measure of depression. Daughters reported the frequency with which they experience various feelings or behaviors such as feeling “hopeful about the future” or having “crying spells” on a 4-point scale ranging from 0 = “rarely or none of the time” to 3 = “most or all of the time”. The internal consistency reliability of the CES-D is high, ranging between 0.85 and 0.90.38 , 41 The validity of the CES-D is supported given that its four factors, (1) depressed affect, (2) positive affect, (3) somatic complaints, and (4) interpersonal problems, have been replicated among various respondent populations.42 – 45
Daughters completed the PSC during years 1–3.39 The PSC is a 35-item, self-report, psychosocial screening measure. Daughters reported how often they exhibited specific behaviors such as “being irritable or angry” and “having trouble concentrating” on a 3-point scale ranging from 0 = “never” to 2 = “often”. Studies have documented high levels of agreement between parents’ and professionals’ PSC ratings46 – 48, good internal consistency (0.89) and test–retest reliability (0.86)39, and acceptable validity.49 Normative data suggest that PSC scores of 28 or above reflect a need for further psychosocial evaluation and that 10 to 13% of children in a general pediatric sample exceed this criterion.39 , 49 – 51 The measure has good sensitivity (87 to 95) and specificity (68 to 100).46 , 48
To ensure age appropriateness of the measures used in the study, the PSC was replaced with the CSI39 in year 4. The CSI is a 14-item, adult self-report measure of mental health symptoms. Respondents are asked to report the frequency with which they have experienced each symptom during the past month. Although the CSI has been used frequently in mental health services research, little is known about its psychometric properties.
In phase 2, the comprehensive interviews were open-ended and explored in more detail the impact of personal, familial, and environmental factors on these girls’ lives. The personal domain included their dreams and hopes for the future, sense of self-esteem, their perceptions about the roles they played in society, and relationships with family, peers, teachers, employers, and others. The family domain focused on family values and expectations, roles the adolescents played in their family, and family support. The environmental domain included their perceptions of home, community, and school environments; educational, recreational, and employment opportunities; and barriers to accessing these resources. Over time, some modifications were made to the interview protocol based on previous years’ findings. For example, a specific question was added regarding social support from teachers and other school personnel. To reflect the TANF changes that occurred during the study, a question was added regarding the requirement for premarital counseling. Given that over time many of the daughters were moving into the workforce, the employment section in the protocol was expanded.
Procedures
In phase 1 of the first year, letters were mailed to prospective participants, informing them about the study and indicating that field staff would contact them regarding their possible interest in the study. Individuals not wanting to be contacted were instructed to call a toll-free number provided in the letter to make known their wishes. Staff hired and trained specifically for this study began contacting eligible mothers and daughters in January 2002, explaining the purpose and scope of the study to them and inviting them. For those mothers and daughters agreeing to participate, both signed informed consent and provided permission to link their interview responses to existing administrative data. Each of the mothers and daughters who participated in the initial face-to-face interviews was paid $40.00 as compensation for her time. These same procedures were repeated in each of the three follow-up years of the study (i.e., 2003–2005).
Phase-2 participants also received $40.00 for completing this interview. Interviews were taped and transcribed to ensure the accuracy of the data. The same 20 daughters were asked to complete phase-2 follow-up interviews in each year of the study.
In each year, before initiating any project activities, all proposed study procedures were reviewed and approved by the University of South Florida’s Institutional Review Board to ensure that participants’ rights were protected. To protect the confidentiality of respondents’ information, different field staffs were used to interview the mothers and daughters. Both mothers and daughters were informed at the start of the interview that their responses would not be shared with each other; however, they were encouraged to talk with each other about their responses on their own. Additionally, different field staff were used to complete the quantitative and qualitative phases of the study. Different interviewers were used to conduct the Phase 1 quantitative interviews and the Phase 2 qualitative interviews. This was done to maximize the respective expertise of the different interviewers and help ensure that the interpretations of the qualitative interviews were not influenced or biased by respondents’ answers to the quantitative interviewers.
Data analysis
The phase-1 statistical analyses were largely descriptive in nature and intended to address the basic questions associated with the conceptual model. Comparative (i.e., inferential) analyses were performed to assess changes in daughters’ emotional status over time across the 4 years.
A forced entry regression analysis was performed to examine what factors were associated with daughters’ emotional well-being throughout the study. To develop the composite emotional well-being indicator that was used as the dependent variable in this analysis, in each year, daughters were classified as being above or below the criterion score on each of the four measures previously described and whether they reported a need for mental health services. The various measures provided three indicators of emotional well-being for each daughter in each year (12 indicators across the 4-year study). The composite indicator was adjusted for the number of interviews the daughters completed. The numbers of times daughters were below the criterion score or did not report needing mental health services were summed to produce an overall index of emotional well-being across the study period. This was used as the dependent variable in the regression analysis. A more detailed review of the study findings is summarized elsewhere.52
For the phase-2 qualitative analysis, the research team developed an initial coding scheme that reflected the three specific areas of the adolescents’ lives that were explored in the interviews: personal, family, and environment. A thematic analysis of the transcriptions was conducted for these key domains using the initial set of codes, and additional codes were added as new themes emerged from the data. During the year-1 data analysis, the two qualitative researchers both coded a number of interviews to establish interrater reliability. These two team members conducted all data collection and data analysis throughout the study. The findings from both phases of the study were triangulated at the end of each study year to provide a more comprehensive understanding of the risk and protective factors in these girls’ lives and of how these factors contributed to their overall emotional well-being.
Results
Characteristics of the daughters
Table 3 summarizes the background characteristics of the 125 daughters at the start of the study in 2002, including their race/ethnicity, age, educational status, marital status, and housing status.
At the start of the study, daughters’ ages ranged from 13 to 17 years old, averaging 15.5 (SD = 0.99). The daughters represented a culturally diverse sample as 34% were white, 41% were black/African-American, and 26% were Hispanic. None of the daughters were married at the start of the study, and all of them were living at home. At the time of the initial interview, 28% of the daughters had already dropped out of school.
Although not shown in the table, some important changes were observed over time in these daughters’ characteristics. While most of the daughters (89%) remained unmarried, 10% either married or began living as married during the course of the study. At the start of the study, slightly over a quarter of the daughters had dropped out of school and none had yet graduated. By year 4, 44% of the daughters had dropped out of school and 35% had graduated from high school or received their general education degree (GED). The remaining daughters were still attending school.
Changes in daughters emotional well-being during the study
here was a steady increase in the percentage of daughters who scored above the criterion on at least one of the three emotional well-being indictors in each year, indicating that they were experiencing some level of emotional distress. In year 1, 37.9% of the girls exceeded the criterion on at least one mental health indicator (see Table 4). The figure rose to 41.2% in year 2. By year 3, over half of the daughters (50.9%) scored above the criterion on at least one indicator, indicating some level of emotional distress. Finally, in year 4, 52.2% of the daughter exceeded the criterion on at least one indicator. Overall, two-thirds of the daughters (66.7%) exceeded the criterion on at least one mental health indicator at some point during the course of the 4-year study, indicating some level of emotional distress.
Despite this high rate of self-reported emotional distress among these daughters, not more than 5% of them reported receiving a mental health service during any year of the study. Collectively, only 11% of the adolescents reported using a mental health service at any point in time.
Prediction of daughters emotional well-being
A forced entry least-squares regression analysis was conducted using phase-1 data from year 1 to examine the extent to which preexisting risk and protective factors were associated with daughters’ emotional well-being throughout the study. The composite variable of daughters’ emotional well-being previously described was regressed on to a set of 16 variables considered to be important risk and protective factors associated with resilience. These predictors included daughter demographic information (three variables: age, being black, being another minority race), relationship with father (one variable), school performance (one variable), perceived safety (one variable), quality of the neighborhood (one variable), religiousness (one variable), family functioning (one variable), locus of control (one variable), self-esteem (one variable), life events (one variable), and social support (four variables).
The overall 16-variable model was statistically significant F(16,84) = 4.72, p < .001, and accounted for 37% of the variance in the composite emotional well-being variable. The results of this analysis are summarized in Table 5. Examination of the specific predictors indicates that four variables (i.e., locus of control, life events inventory score, parental social supports, and teacher social support) emerged as the variables more significantly associated with the daughters’ well-being. More specifically, having a more internal locus of control was associated with improved emotional well-being. Likewise, daughters who experienced fewer negative life events were also associated with better emotional well-being. Daughters reporting higher levels of parental social support also had better emotional well-being. Somewhat surprising, reports of less teacher social support were associated with better emotional well-being. This may be due to the fact that teachers assumed a supportive role primarily for those daughters who were struggling with their emotional well-being.
Parental social support was the best single predictor of daughters’ emotional well-being followed by teacher social support, locus of control, and life events (e.g., death of a parent, abuse). None of the remaining 12 predictors explained a significant amount of variance in daughters’ emotional well-being.
The following sections highlight the adolescents’ perspectives and voices on these four key risk and protective factors: parent support, locus of control, the absence of traumatic life events, and teacher support.
Daughters relationships with their parents
During the phase-2 interviews, daughters most often identified their mothers as their role models, highlighting how important this relationship was in their lives. Their response is consistent with the findings from the regression analysis in which parental social support was a significant predictor of the daughters’ emotional well-being. However, on an annual basis, a third to one-half of the daughters interviewed reported not being able to spend as much time with their mothers as they would like. The most frequent reasons daughters cited for this included the mothers and daughters’ work schedules, being busy with family matters, and just “getting older”. Despite the importance of these relationships, daughters were growing up and moving out and spending less time with their mothers.
All phase-2 daughters placed great value in their relationship with their mothers during years 1 and 2 of the study even when there were conflicts and disagreements. For them, their mothers were the most important persons in their lives, and they reported having close and nurturing relationships with their mothers. The mother of one of the daughters went away for approximately 6 months to receive substance abuse treatment, leaving the daughter under the grandmother’s custody. This daughter still felt very connected to her mother and reported that her mother was doing very well in her treatment.
Transition was a new theme when the daughters described their relationships with their mothers during the years 3 and 4 interviews. Most daughters remained very close to their mothers and described the many ways their mothers offered emotional support even when they were living apart: “encourages me”, “behind me 100%”, and “we talk everyday”. One daughter, who had run away from home and was estranged from her mother, noted that her pregnancy had resulted in an improved mother–daughter relationship. By the fourth year of the study, she proudly introduced her mother to the interviewer and described the many ways that her mother was supportive. However, some adolescents spoke of mothers giving mixed messages about leaving home and a perception that their mothers did not trust them. In addition, some daughters expressed more discrimination in what they confided in with their mother versus with their friends.
Locus of control
Most of the daughters in years 1 and 2 were aware of the amount of control they had over their lives and destinies. For example, they were cognizant of the fact that their educational success depends on whether they do what is required. Similarly, they knew that continuing their education would depend not only on their efforts but also on being able to access the financial resources necessary to pursue a college education.
The theme of importance of an internal locus of control was much stronger in years 3 and 4: “I’m not going to say it is easy because it’s not...you know how people put you down and say you can’t do this you can’t do that and you kind of proof to them that you can...it makes you feel awesome. Make you feel great.” As the adolescents approached changes in their lives, such as graduation or having a baby, reality presented itself in a manner that required some action. They were no longer thinking about the possibilities and wishing for things to be the way they dreamed them.
As the daughters turned 19 and 20, the presence or absence of financial and/or economic resources set the immediate course of events, “I need my diploma and my driver’s license and a car.” So for instance, the adolescent who graduated with fairly good grades but who is counting on a job and reliable transportation to be able to go to college is forced to look for ways to obtain these in order to work on her educational goals. The adolescents were not unrealistic in the previous years when they spoke about goals and aspirations, but they are now faced with the reality that they needed to “take control” because these things do not just fall into place. When asked whether things ever go wrong in her life, one adolescent said: “Yes, but you can’t let them get to you, you have things that really go wrong in your life but you just got to let it roll off and go on.” Another interviewee said: “I just need to focus on whatever I want. If I can focus on what I want, I can do it. Because there is nothing to stop me. I got this far, right, by focusing on what I wanted, so if I just focus, I get whatever.”
The role of life events
One of the life events that dramatically changed the trajectories of many girls was having a baby. Among the phase-2 girls, only a few reported in year 1 that they were involved in relationships or had previous relationships where they had engaged in sexual activity. By year 2, six of the daughters reported that they were involved in relationships. The one pregnant daughter had not planned this pregnancy and reported not wanting to have any more children. None of the other daughters were dating and reported not being interested in having children until they finished college and had a career.
At the time of the year-3 interviews, three of the daughters had a child that they were caring for, and another three were pregnant. For two of the three pregnant daughters, they were living with their boyfriend and felt that he and his family were supportive of the pregnancy. For the other daughter, the father had recently ended their relationship, and she expressed a sense of loss.
By the time of the year-4 interviews, 5 of the 18 daughters who were interviewed had a child, and 4 were living with the father of the child. One other adolescent was pregnant, and only three were not sexually active. None of the daughters was married although some who were living with a boyfriend or in a serious relationship believed that they would be married over the next few years. Pregnancy also altered friendships; one daughter who was pregnant mentioned that she “kept more to herself now”. The challenges related to having a baby and reaching one’s goals were especially dramatic for one adolescent whose baby had serious medical complications:
“Is my baby being sick, that is the only thing that you know. Because I think that if he would have been like an OK baby like wasn’t born with that, I would have probably been in school by now. You know, now I have to wait longer. I have to wait until he is at least a year old. In October, he’ll be a year, and then I have to wait until he is done with all those medical problems. That is all. Otherwise, I would’ve been in school and been got a job and been got a car and been out on my own place, but that is the only thing preventing me from doing all those kind of stuff.”
Sometimes, the adolescents expressed their views about traumatic life events when they were talking about their friends. One daughter described her reactions to a friend who was in a residential program for substance abuse users and was pregnant:
“Like she told me at work and I’m like why in the heck you didn’t tell me that, you know. But when she told me she was happy and I was like I’m so sorry. That is horrible, what are you going to do, are you going to get an abortion? But its just like what are you going to do, I mean her boyfriend is in the Keys and she is in this program like for another 2 months, she has no money, she owes everybody money. She wants to move to the Keys with her boyfriend and he doesn’t even have his own place he is staying with other people. And I’m like are you crazy? I mean, think about your kid if anything you know. She is just a little crazy, she is not thinking straight. And her boyfriend is pressuring her, so. She doesn’t know what she is going to do. Her mom is like don’t do it, but 1 day, she was over here and I hadn’t seen her or talked to her for a while and she was going to the program and she broke down and told me I don’t want to marry him, he’s pressuring me into marrying him and I don’t know how he is to live with, cause she just started going out with him.”
Teacher support
Relationships with teachers were significant for only a few of the phase-2 daughters in years 1 and 2 although most of them could identify a favorite teacher. Having a favorite teacher did not mean that they had a close relationship with him/her but rather a recognition of the commitment these teachers had to their students to help them learn and to help them do in their classes. One daughter said, “...my ROTC teacher at school, he is the person I look up the most because I see myself as him when I get to his age.” Another daughter described the ways a guidance counselor “gets you back on track if you fall off”. These positive effects of relationships are supported by recent research that identifies relationships as one of the five exemplary practices that help at-risk students to have positive secondary school experiences.53
These relationships, when they did exist, were affected by leaving school. By year 4, none of the phase-2 daughters were attending regular high school. Eight had graduated from high school, and six others were trying to get either their high-school diploma through online courses or a GED. One daughter who had quit school described her reasons: “That school weren’t right for me, I didn’t like it, it was like the teachers they don’t pay attention to you there, they don’t try to help you or nothing. So I’m gonna try to go to P-Tech.” This daughter, as well as several of the other interviewees, was not sure what grade she had completed (“about 11th”) and also did not know how long it would take for her to complete her GED. The daughters who quit school had many challenges with GED programs. They mentioned teachers who did not give them much direction, challenges with day care for their young children, and transportation barriers.
The effect of transitions on the daughters relationships
In addition to the relationships of the daughters with their parents and teachers, many adolescents mentioned the role of friendships with peers. Relationships with friends were reported as valuable during the early study years, and some daughters reported having long-lasting friendships that developed from the time they were in elementary and/or middle school. Throughout the study, some daughters made clear distinctions between friends, associates, and acquaintances. Friends were described as the people with whom they get together outside of the school context. Associates were described as school peers, and acquaintances as people with whom they may exchange a “hello” or have a brief conversation but would not go out with them. Close relatives such as cousins, older sisters, and aunts replaced the presence of friends for some daughters.
Transitions in years 3 and 4 affected the daughters’ relationships. Many girls had moved, either to live with a boyfriend or to get a place of their own, and had lost contact with friends. Others mentioned that graduating from high school resulted in losing contact with some friends and that some friends had moved or gone on to community colleges. One daughter noted that she was sad about graduating from high school because she had made many friends during her senior year. In summary, the girls experienced many changes in their significant relationships with mothers, teachers, and peers over the course of the study. It is possible that these relationship changes, although expectable during the transition from adolescence to adulthood, were more keenly felt due to life events such as dropping out of school, pregnancy, and loss of a boyfriend, and contributed to their relatively high levels of depression. In addition to the loss of and/or changes in key relationships, the daughters experienced many of the institutional challenges noted in the literature,54 which are related to the transition to young adulthood, including low utilization of mental health services, mistrust of educational institutions, and confusion regarding eligibility criteria for services such as GED programs.
Limitations
There are several limitations to this study that need to be acknowledged. First, although the sample was randomly selected from among all 2002 Medicaid eligible mother/daughter pairs in a five-county region in the Tampa Bay, Florida area, the representativeness of the sample to other areas of Florida or to other states remains unknown. This is important in this context given that all of the mothers and daughters in this study were served by the same regional service system. Another limitation relates to the fact that this is an observational study, and there is a lack of a comparison group against which the emotional well-being of these youths can be contrasted.
Discussion
These study findings can be used to inform a tertiary approach to mental health intervention.21 This model classifies interventions into universal, selected, and indicated preventive interventions. Universal preventive interventions are directed to a whole population group rather than to individuals who have been identified as high risk; in this case, adolescent girls whose mothers are enrolled in welfare reform. Individuals whose risk for developing mental health problems is significantly higher than average are the target for the second level of selected preventive interventions. This second level of intervention applies to those adolescent girls who have experienced a number of the risk factors identified in the study, such as lack of parental support, external locus of control, and teenage pregnancy. Indicated preventive interventions are reserved for those individuals with early signs of possible mental disorders, such as those girls identified as having emotional or behavioral problems by their mothers or teachers.
Clearly, society needs to invest in the future of adolescent girls whose mothers are enrolled in TANF so that these girls can do well in school, secure gainful employment, become caring parents, and participate as citizens in their communities. The gap between their emotional well-being and the use of mental health services suggests that the potential exists for substantial unmet mental health needs among these adolescents. However, the study data suggest that schools or any other one system, although an important part of the equation, cannot be the sole focus or solution for assisting these daughters in a healthy transition into adulthood. For example, at the start of the study, 28% of the daughters (ages 13–17) had already dropped out of school. Important variables identified in the study, such as teacher social support, did not exist for these daughters, indicating that other mechanisms are needed to assist them in their transitions. A multifaceted strategy carried out by all the systems with contact with these girls and their families is needed.
The beginning point for this strategy is to view a mother’s enrollment in TANF as an opportunity for tertiary prevention activities related to these at-risk adolescents. As part of the initial TANF application process, the intake worker would ask women whether they have daughters between the ages of 12 and 18. If the answer is yes, the role of the TANF program would be to monitor the daughters’ status each time that a mother comes into contact with the system. A brief series of standard questions about the status of key risk factors could be used to assist the mothers to identify any high-risk daughters. Other individuals who may serve as portals for identification of at-risk adolescents include teachers and public health practitioners.
Universal prevention activities could be suggested to mothers whose daughters do not appear to have multiple risk factors. Some of the phase-2 daughters, when asked what helped them to succeed, mentioned after-school and summer programs that offered recreational and educational experiences. These programs should use the framework of positive youth development, a process through which all adolescents attempt to meet their needs for safety, caring relationships, and community connections while building their academic, vocational, and social skills.55 This framework makes sense, given the study findings, because this approach taps into adolescents’ potential for positive development using the many personal, familial, and community protective factors identified in the literature.
Given the study findings, selected preventive intervention activities for daughters identified as having some risk factors should focus on a number of domains. First, as the adolescents told us in this study, educational support services are needed to keep the adolescents in school and prepare them for future academic pursuits or to enter the workforce. Study findings indicate that teachers assumed a supportive role primarily for those daughters who were struggling with their emotional well-being. Teachers and other school personnel need to identify and offer educational support and services to these at-risk youths. In addition to the lack of teacher support, many of the daughters had only a vague understanding of the academic requirements needed to graduate from high school, get into college and/or receive financial aid, and enter the profession to which they ascribed.
A second area is reproductive health education so that teenage pregnancies can be minimized. As noted earlier, over half of the daughters had been pregnant by the end of the study. Caring for a baby presented many challenges for these girls, both financially and emotionally. One possible resource is the programs for pregnant and parenting teens that are offered by middle and high schools. These programs offer concrete advice about parenting, provide child care on-site so that teens can stay in school, and offer emotional support. Finally, these youths need targeted efforts to foster and sustain significant adult relationships with individuals who can serve as role models and mentors, especially if their mothers are unable to fulfill this role. A recent synthesis of the role and outcomes of mentoring programs indicates that those who benefit the most are those who are the most at risk and that youths with mentors improve on a number of educational outcomes, including fewer unexcused absences, better school behaviors, and greater chances of attending college.56
For those girls needing employment, they need vocational assistance, including work skills development, job coaches, and employment opportunities. The importance of having a job was stressed by several of the girls in year 4, in relationship to having enough money to get a car, pay car insurance, attend community college, get an apartment, and/or care for their child. Several girls noted that minimum wage jobs were stressful: “Just working at Burger King, I know I am not going anywhere. Even as a manager there, I am not going to go anywhere, so I have thought about it too. Stressing out about working there is just too much; you work too much to get a little paycheck.” For this daughter, these conditions were strong motivators to finish high school.
Indicated prevention strategies are needed for TANF daughters whose mothers, teachers, or public health practitioners identify as experiencing challenges emotionally, behaviorally, and/or with substance use. For example, at TANF intake, the parents could be asked to complete a brief mental health screen about their daughter. Any number of short self-report measures could be used that are both in the public domain (i.e., they are available at no cost) and have been demonstrated to have good psychometric properties. A few of these measures include the CES-D,38 PSC,39 the CSI,40 and the Patient Health Questionnaire-9.57 For girls with identified mental health needs, timely referral and linkages are needed to appropriate behavioral health services and support.
Implications for Behavioral Health
Within this framework of planning and implementing a tertiary model of universal, selected, and indicated preventive interventions for this population, the local community mental health system has many roles to play. First, the behavioral health system needs to be an active player in a community cross-system infrastructure that coordinates services and supports for at-risk adolescents. This local coordinating body can be convened by any player, including a community mental health provider, the school district, or a group of concerned parents. Regardless of who organizes the effort, community mental health centers need to actively participate in local needs assessment activities, the identification of gaps in services and barriers to accessing services, and ongoing coordination of existing services and supports for at-risk youths.
Second, the behavioral health system should be engaged with the natural portals for mental health prevention and intervention, including the local TANF office, schools, and the public health system. Especially with poor young women, previous studies have indicated the importance of placing mental health identification and engagement services in settings where they are often seen.58 Community mental health centers need to be linked with these portals and perform a number of roles, including offering consultation to the intake staff and case managers, acting as a referral source, and providing further mental health and/or substance abuse assessment and evaluation for girls with identified needs. In addition, community mental health providers should agree to give priority to girls who are identified by the other systems as in need of further assessment. For example, if the number of referrals for behavioral health assessments increases at a portal, the community mental health system may offer to provide an on-site clinician a few days a week to assist with assessment and linkage activities. Finally, the behavioral health system should offer ongoing consultation and training for staff in the portal systems regarding the identification of at-risk youths, engagement of these youths in prevention and early intervention activities, and appropriate behavioral health referral sources and linkages.
Another implication from this study is that the behavioral health system needs to offer outreach, education, and engagement activities with at-risk adolescent girls and their mothers. Despite the disproportionate number of adolescents who reported some level of emotional problems, not more than 5% of the adolescents reported using a mental health service in any given year. The behavioral health system needs a media campaign to educate parents, teachers, and adolescents about the indicators of mental health and/or substance abuse problems and how to obtain help. Research has demonstrated that such efforts are effective in reducing the stigma tied to accessing behavioral health services.59 This recommendation is consistent with the President’s New Freedom Commission Report which states that “media-oriented and other types of mental health awareness campaigns can inform the public about where and how to obtain help”.60 (p. 23) Advanced multimedia strategies developed in the private sector have been adopted for and successfully used in the public health arena.61 For example, an evaluation of the mass media program VERB, launched in 2002 by the Centers for Disease Control and Prevention to increase the levels of physical activity among children, documented increased levels of awareness in the first year and higher levels of physical activity among some subgroups of children.62 As part of the Center for Mental Health Services “Caring for Every Child’s Mental Health Campaign”,63 to increase public awareness regarding the importance of ensuring the mental health of the nation’s youths, multiple media efforts have been made to engage local media, build rapport with reporters, create locally shaped messages, develop talking points, and conduct media follow-up. The basic messages are that youths’ mental health is important; many children experience real, painful, and severe problems, but that these problems if recognized can be successfully treated.
In summary, the behavioral health care system needs to be an active participant in a multisystem collaborative infrastructure that is accountable for planning, monitoring, media education, engagement, and offering services to at-risk adolescents in their community. Informed by a tertiary model of mental health prevention and intervention, this infrastructure can truly be the safety net that these girls need to become fully contributing adult members of their community.
References
Personal Responsibility and Work Opportunity Reconciliation Act of 1996, P.L. 104–193, 110 Stat. 2105.
Children Now. Content analysis on welfare reform reporting. Available at: http://www.childrennow.org/economics/welfref98/welfarereformshortdoc.html. Accessed June 17, 2003.
Gennetian LA, Duncan GJ, Knox VW, et al. How Welfare and Work Policies for Parents Affect Adolescents: A Synthesis of Research. New York: Manpower Development Research Corporation; 2002.
Taylor MH. The potential impact of gender roles socialization on welfare policy formation. Journal of Sociology and Social Welfare. 2000;27:135–152.
Brooks MG, Buckner JC. Work history and welfare: job histories, barriers to employment, and predictors of work among low-income single mothers. American Journal of Orthopsychiatry. 1996;66:526–537.
Furstenberg F. The next generation: the children of teenage mothers grow up. In: Rosenbaum M, Testa M, eds. Early Parenthood and Coming of Age in the 1990s. New Brunswick, NJ: Rutgers University Press; 1992:113–135.
Gottschalk P, McLanahan S, Sandefur G. The dynamics and intergenerational transmission of poverty and welfare participation. In: Danziger SH, Sandefour GD, Weinberg DH, eds. Confronting Poverty: Prescriptions for Change. Cambridge, MA: Harvard University Press; 1994:85–108.
Boothroyd RA, Olufokunbi D. Leaving the welfare rolls: the health and mental health status of current and former welfare recipients. Mental Health Service Research. 2001;3:119–128.
Boushey H, Gundersen B. When working just isn’t enough: measuring the hardships faced by families after moving from welfare to work. Available at: http://www.epinet.org/content.cfm/briefingpapers_hardships. Accessed April 5, 2002.
Lichter DT, Crowley MC. Poverty in American: beyond welfare reform. Population Bulletin. 2000;57:1–36.
Kirby D. No Easy Answers: Research Findings on Programs to Reduce Teen Pregnancy. Washington, DC: National Campaign to Prevent Teen Pregnancy, Task Force on Effective Programs and Research; 1997.
Fraser MW, ed. Risk and Resilience in Childhood: An Ecological Perspective. Washington, DC: NASW Press; 1997.
Egeland B, Carlson E, Sruofe LA. Resilience as process. Development and Psychopathology. 1993;5:517–528.
Smith C, Carlson BE. Stress, coping and resilience in children and youth. Social Service Review. 1997;71:231–256.
Masten AS, Morison P, Pellegrini D, et al. Competence under stress: risk and protective factors. In: Weintraub S, ed. Risk and Protective Factors in the Development of Psychopathology. Cambridge: Cambridge University Press; 1990:236–256.
Rutter M. Psychosocial resilience and protective mechanisms. In: Weintraub S, ed. Risk and Protective Factors in the Development of Psychopathology. Cambridge: Cambridge University Press; 1990:181–214.
Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work. Child Development. 2000;72:543–562.
Rankin BH, Quane JM. Social contexts and urban adolescent outcomes: The interrelated effects of neighborhoods, families, and peers on African-American youth. Social Problems. 2002;49:79–100.
McCabe KM, Barnett D. The relation between familial factors and the future orientation of urban, African American sixth graders. Journal of Child and Family Studies. 2000;9:491–508.
Jodl KM, Michael A, Oksana M, et al. Parents’ role in shaping early adolescents’ occupational aspirations. Child Development. 2001;72:1247–1265.
Mrazek PJ, Haggerty RH, eds. Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research/Committee on Prevention of Mental Disorders, Division of Biobehavioral Sciences and Mental Disorders, Institute of Medicine. Washington, D.C.: National Academy of Sciences; 1994.
Leginski WA, Croze C, Driggers J, et al. Data Standards for Mental Health Decision Support Systems. (ADM89-1589). Rockville, MD: National Institute of Mental Health; 1989.
Fetzer Institute, National Institute on Aging Working Group. Multidimensional measurement of religiousness, spirituality for use in health research. Kalamazoo, MI: Fetzer Institute; 2003 (1999).
Epstein NB, Baldwin LM, Bishop DS. The McMaster Family Assessment Device. Journal of Marital & Family Therapy. 1983;9:171–180.
Kabacoff RI, Miller IW, Bishop DS, et al. A psychometric study of the McMaster Family Assessment Device in psychiatric, medical and nonclinical samples. Journal of Family Psychology. 1990;3:431–439.
Miller IW, Epstein NB, Bishop DS, et al. The McMaster Family Assessment Device: reliability and validity. Journal of Marital and Family Therapy. 1985;1:345–356.
Byles J, Byrne C, Boyle MH, et al. Ontario Child Health Study: reliability and validity of the General Functioning Subscale of the McMaster Family Assessment Device. Family Process. 1988;27:97–104.
Norwicki S Jr, Strickland BR. Study presents reliability and validity evidence concerning measure of locus of control for children. Journal of Consulting and Clinical Psychology. 1973;40:148–154.
Smith VK. Analysis of Locus of Control and Educational Level Utilizing the Internal Control Index. Master’s Thesis, Marshall University; 2003.
Rosenberg M. Society and the Adolescent Self-Image. Princeton, New Jersey: Princeton University Press; 1965.
Blascovich J, Tomaka J. Measures of self-esteem. In: Robinson JP, Shaver PR, Wrightsman LS, eds. Measures of Personality and Social Psychological Attitudes. Third edition. Ann Arbor: Institute for Social Research; 1993:115–160.
McCarthy JD, Hoge DR. Analysis of age effects in longitudinal studies of adolescent self-esteem. Developmental Psychology. 1982;18:372–279.
Shahani C, Dipboye RL, Phillips AP. Global self-esteem as a correlate of work-related attitudes: a question of dimensionality. Journal of Personality Assessment. 1990;54:276–288.
Silbert E, Tippett JS. Self-esteem: clinical assessment and measurement validation. Psychological Reports. 1965;16:1017–1071.
Monaghan JJ, Robinson JO, Dodge JA. The children’s life events inventory. Journal of Psychosomatic Research. 1979;23:3–68.
Harter S. Manual for the Social Support Scale for Children. Denver, CO: University of Denver; 1985.
Varni JW, Katz ER. Stress, social support, and negative affectivity in children with newly diagnosed cancer: a prospective transactional analysis. Psychooncology. 1997;6:267–278.
Radloff LS. The CES-D Scale: a self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401.
Jellinek MS, Murphy JM, Burns BJ. Brief psychosocial screening in outpatient pediatric practice. The Journal of Pediatrics. 1986;109:371–378.
Shern DL, Wilson NZ, Coen AS, et al. Client outcomes II: longitudinal client data from the Colorado Treatment Outcome Study. The Milbank Quarterly. 1994;72:123–148.
Hann D, Winter K, Jacobsen P. Measurement of depressive symptoms in cancer patients. Evaluation of the Center for Epidemiological Studies Depression Scale (CES-D). Journal of Psychosomatic Research. 1999;46:437–443.
Hertzog C, Van Alstine J, Usala P, et al. Measurement properties of the Center for Epidemiological Studies Depression Scale (CES-D) in older populations. Psychological Assessment. 1990;2:64–72.
Knight RG, Williams S, McGee R, et al. Psychometric properties of the Center for Epidemiological Studies Depression Scale (CES-D) in a sample of women in middle life. Behavior Research and Therapy. 1997;35:373–380.
Nguyen HT, Kitner-Triolo M, Evans MK, et al. Factorial invariance of the CES-D in low socioeconomic status African Americans compared with a nationally representative sample. Psychiatry Research. 2004;126:177–187.
Weissman MM, Sholamskas D, Pottenger M, et al. Assessing depressive symptoms in five psychiatric populations: a validation study. American Journal of Epidemiology. 1977;106:203–214.
Jellinek M, Murphy JM, Robinson J, et al. The pediatric symptom checklist: screening school-aged children for psychosocial dysfunction. The Journal of Pediatrics. 1988;112:201–209.
Murphy JM, Jellinek MS, Milinsky S. The Pediatric Symptom Checklist: validation in real world middle school. Journal of Pediatric Psychology. 1989;14:629–639.
Murphy JM, Reede J, Jellinek MS, et al. Screening for psychosocial dysfunction in inner-city children: further validation of the Pediatric Symptom Checklist. Journal of the American Academy of Child Adolescent Psychiatry. 1992;31:1105–1111.
Jellinek MS, Murphy JM. The recognition of psychosocial disorders in pediatric office practice: the current status of the Pediatric Symptom Checklist. Journal of Developmental and Behavioral Pediatrics. 1990;11:273–278.
Jellinek MS, Murphy JM, Burns BJ. Brief psychosocial screening in outpatient pediatric practice. The Journal of Pediatrics. 1986;109:371–378.
Jellinek MS, Murphy JM, Little M, et al. Use of the Pediatric Symptom Checklist to screen for psychosocial problems in pediatric primary care. Archive of Adolescent Medicine. 1999;153:254–260.
Boothroyd RA, Gomez MI, Armstrong MI, et al. Young and poor: the well-being of adolescent girls living in families receiving temporary assistance for needy families program. Journal of Child and Family Studies. 2005;14:141–154.
Davis M. Addressing the needs of youth in transition to adulthood. Administration and Policy in Mental Health. 2003;30:495–509.
Wagner M, Davis M. How are we preparing students with emotional disturbances for the transition to young adulthood? Journal of Emotional and Behavioral Disorders. 2006;14:86–98.
Quinn J. Where need meets opportunity: youth development programs for early teens. The Future of Children. 1999;9:96–116.
Jekielek MA, Moore KA, Hair EC. Mentoring Programs and Youth Development: A Synthesis. Washington, DC: Child Trends; 2002.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: a new depression diagnostic and severity measure. Psychiatric Annals. 2002;32:509–515.
Miranda J, Green BL. The need for mental health services research focusing on poor young women. The Journal of Mental Health Policy and Economics. 1999;2:73–80.
Corrigan PW, Penn DL. Lessons from social psychology on discrediting psychiatric stigma. American Psychologist. 1999;54:765–776.
The President’s New Freedom Commission on Mental Health. Achieving the Promise: Transforming Mental Health Care in America. Rockville MD: DHHS Pub. No. SMA-03-3832; 2003.
Randolph W, Viswanath K. Lessons learned from public health mass media campaigns: marketing health in a crowded media world. Annual Review of Public Health. 2004;25:419–437.
Marian H, Potter LD, Wong FL, et al. Effects of a mass media campaign to increase physical activity among children: year-1 results of the VERB campaign. Pediatrics 2005;116:e277–e284. URL: http://www.pediatrics.org/cgi/doi/10.1542/peds.2005-0043.
Center for Mental Health Services. Caring for Every Child’s Mental Health Campaign. Available at: http://mentalhealth.samhsa.gov/child/. Accessed October 6, 2006.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Armstrong, M.I., Boothroyd, R.A. Predictors of Emotional Well-Being in At-Risk Adolescent Girls: Developing Preventive Intervention Strategies. J Behav Health Serv Res 35, 435–453 (2008). https://doi.org/10.1007/s11414-006-9048-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11414-006-9048-9