
Abstract
Purpose The objective of this study was to identify organizational factors that are predictive of return-to-work (RTW) among workers with musculoskeletal (MSD) and common mental disorders (CMD), and to subsequently catalogue and characterize the questionnaires (tools) used to measure them. Methods A systematic search on PubMed, Web of Science and PsycINFO library databases and grey literature was conducted. First, a list of organizational factors predictive of RTW for the two populations considered was built. Second, the questionnaires used to measure these factors were retrieved. Third, we looked in the scientific literature for studies on the psychometric properties and practical relevance of these questionnaires. Results Among the factors retained, perceived social support from supervisor and co-workers, work accommodations, and job strain were identified as common RTW factors. Other risk/protective factors, and associated tools, specifically targeting either people with MSD or CMD were also analysed. Conclusions Researchers and practitioners are often uncertain of which tools to use to measure organizational factors which can facilitate or hinder RTW. This study provides an evaluation of the tools measuring predictive organizational RTW factors in people with MSD and CMD. The identified tools can be used in everyday practice and/or research.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Musculoskeletal (MSD; e.g., low back pain) and common mental disorders (CMD; e.g., depression) represent prominent causes of sickness absence and work disability worldwide [1]. Alongside with the health of workers being compromised, MSD and CMD create a substantial burden on the public health and insurance systems, on the businesses economy, and more generally to society [2, 3]. Consequently, it is important to identify which factors may facilitate the return-to-work (RTW) of people suffering from MSD and/or CMD. There is solid recognition in the literature that successful RTW of people with MSD and CMD depends on individual and organizational factors—some of them acting as facilitators, and others as obstacles to RTW [4, 5]. Yet, among studies, mixed results are found on which factors contribute to RTW and how. Another challenge for researchers and practitioners is the way these factors can be measured, because different tools exist [6].
This paper stems from a broader research project that aimed at identifying individual, organizational, and health-related factors predictive of RTW in people with MSD and CMD. The specific aims of this paper are (1) to report the results concerning RTW predictive organizational factors, and (2) to consider and evaluate the corresponding evaluation tools. Because we were specifically interested in identifying predictive RTW factors, we decided not to include in our review cross-sectional studies, and to only focus on prospective cohort studies.
Methods
Literature Review
Data Source
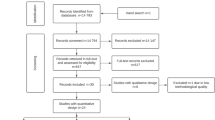
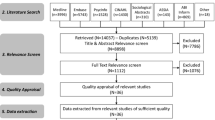
For the purpose of this paper, we conducted a search for full text, peer-reviewed, scientific publications on the topic of organizational determinants of RTW among people with MSD and CMD available in the PubMed, PsycINFO, and Web of Science databases. Contextually, we also performed a complementary search on non-indexed literature (Google Scholar). Additional articles were extracted from bibliographic references mentioned in the relevant articles. Searches were run in 2016 and then at the end of 2017. In our study we considered two primary indicators of success in returning to work: (1) the probability of being back at work at the time of study follow-up (i.e. single event); or (2) the time to return to the workplace, meaning the duration of work absence since the first work absence day due to MSD or CMD. Studies considering RTW as a single event and studies considering sustainable RTW were included in the review. Four groups of keywords served to identify articles for review: (1) disability condition (e.g., absence, sick-listed); (2) outcome of interest (e.g., return-to-work); (3) organizational factors (e.g., social support, job strain); (4) study type (e.g., longitudinal). A copy of the search strategy is available upon request. For the larger research project including individual, organizational, and health factors, the search strategy generated 2263 unique references, after deletion of duplicates (Fig. 1). The present paper focuses on the 55 final hits concerning organizational determinants of RTW in people with MSD and CMD. The articles were organized into a table to read and extract the data (Fig. 1; Table 1).

Results of the systematic search strategy
Article Selection (Eligibility)
Studies were included if (1) they were prospective cohort studies published in the last 20 years (January 1998–January 2018); (2) study subjects had a MSD or CMD or, for mixed population studies, at least two thirds (67%) of the study sample was composed of people suffering from MSD and/or CMD; (3) study subjects were workers on sick leave at the moment of data collection (i.e. baseline), or if that was not the case, the condition of those not on sick leave or not employed was controlled for in the analyses; (4) the studies analysed return-to-work as an outcome; (5) organizational factors were measured as predictors of the outcome in multivariate analyses controlling for at least age, sex/gender, and formal education; (6) studies were written in English or French. Literature reviews, case studies and cross-sectional investigations were excluded from our analysis. Studies conducted on sick-listed workers with unspecified work disability were also disqualified from our analysis.
Several steps eliminated articles that did not correspond to our criteria (Fig. 1). A first inspection of article titles discarded irrelevant articles. Then, a more accurate selection was performed by reading the abstracts. This was performed by three trained reviewers, PhD or Master students. Two additional independent reviewers (the two first authors) double checked approximately 30% of all the references. In case of discrepancy, agreement was reached through discussion based on the information available in the title and abstract. A second selection was performed by one researcher (the first author) reading the full version of papers. If the inclusion of an article was uncertain, another researcher (the second author) read the full article to reach a joint decision. When disagreement occurred after readings, a third researcher (last author) was consulted to reach full agreement.
Data Extraction
For each study selected, we gathered information about the organizational factors considered. We listed the population in which they were tested (i.e. MSD, CMD, or mixed), the univariate and multivariate effects tested, and the type of outcomes. From this information we classified the organizational factors as having a “limited”, “moderate”, “strong”, “inconsistent”, or “insufficient” level of evidence of their ability to predict RTW in the two populations considered separately. The level of evidence was attributed by counting the number of multivariate effects tested that were statistically significant (p < 0.05) with a positive relationship with the outcome, statistically significant with a negative relationship with the outcome, and not statistically significant. The detailed evidence-synthesis rules are documented in Fig. 2. More specifically, adapting the level of evidence reported in a paper of Gragnano and colleagues [4] the following categories of predictors were considered: (1) limited, when one effect (positive or negative) is found, or the ratio among significant and non-significant evidences is between 60 and 64.9%; (2) moderate, when two effects are found, or the ratio is between 65 and 79.9%; (3) strong, when three or more effects are found, or the ratio is between 80 and 100%; (4) inconsistent, when the studies do not meet the criteria for any level of evidence and there is no consistent agreement in reported outcomes; and (5) insufficient, when information is not inconsistent but does not meet the criteria for limited evidence (Fig. 2). To avoid misunderstandings, it is important to clarify that the effect size of the studies was not considered. The labels “limited”, “moderate” and “strong” are to be considered merely as indications of the quantity of the effects on RTW (number of statistically significant and not statistically significant effects) and their direction (negative or positive) in the literature, rather than expressing the degree to which a given factor influences the RTW process.

Adapted from [4]
Rules applied to synthesize the evidence within a review or an “additional papers” group.
Inventory of Tools
The inventory of tools was made for each organizational factor predictive of RTW with at least a limited level of evidence. We recorded the measurement tools used in all the studies that reported a statistically significant effect for the factor under consideration. We considered either questionnaires referenced in the bibliography or questionnaires devised specifically for the needs of the study. For each study retained contributing to the at least limited level of evidentiary, the measurement tool for evaluating the predictive factor was recorded. For each measurement tool, we searched for the first article that ever validated it by checking the reference list in the article or performing a search in the same databased used for the main literature review (i.e. PubMed, PsycINFO, and Web of Science).
Critical Analyses of the Questionnaires
To provide an objective evaluation of tools, we recorded the psychometric properties of the questionnaires retained and the qualities that a practitioner would look for in standard practice. Psychometric characteristics considered were as follows (for a similar procedure, see [7]): (1) predictive validity; (2) face validity; (3) construct validity; (4) internal consistency; (5) convergent validity; (6) test–retest reliability. More specifically, the predictive validity of the tools stemmed from the results of the first aim of the study, i.e. to identify predictive RTW organizational factors. A qualitative evaluation of the items used to measure a specific factor/concept was performed to estimate the face validity of the tool. Construct validity was evaluated positively if a factor analysis of the structure of the measure does exist. Internal consistency was evaluated positively with ratings for Cronbach’s alpha between 0.70 and 0.95. Convergent validity was evaluated by significant and positive correlations with theoretically similar concepts. Test–retest reliability was rated positively when repeated testing of the same condition had yielded to comparable results (correlation coefficients higher than 0.60).
Other more practical criteria (practical relevance) were also considered in our study, such as (1) time to complete, (2) administrative burden, (3) the cost/need for training to administer it and interpret the scores, and (4) availability of an English or French version of the instrument. More specifically, timing for completion of the measure was rated as favourable for questionnaires having less than 8 items to complete or taking ≤ 5 min. Administrative burden was assessed as favourable/easy when the questionnaire final score was calculated simply by adding up the items and unfavourable/difficult when a more complex formula was needed, or when reversed items were present. The availability of free English or French version of tools not requiring specific training for administration was evaluated positively (for a similar procedure see, [6, 8]).
Three reviewers (first, third, and forth authors) independently evaluated each measure using the above criteria. Findings were then compared, and any discrepancies resolved through discussion. Finally, a global evaluation of tools was characterized as “excellent”, “good” or “questionable” by crossing the psychometric score with the practical one as showed in Fig. 3.

Evaluation of measurement tools strategy
Results
For the purpose of this study, only organizational predictive factors of RTW reaching the minimum level of evidence (i.e. limited) for at least one of the two populations considered, and related measurement tools, are reported and discussed. Table 1 presents the information obtained from the 55 included studies. In total, 8 organizational factors contributing to RTW among people with MSD and/or CMD were identified, namely: (1) social support from supervisor and co-workers; (2) workplace accommodations; (3) job strain; (4) organizational injustice; (5) effort-reward imbalance at work; (6) job demands; (7) quality of leadership; and (8) job control. Table 2 reports the psychometric and practical characteristics of the measurement tools used in each predictive study retained from the literature review. In total, 19 measures were critically evaluated.
Social Support from Supervisor and Co-workers
As shown in Table 1, moderate level of evidence was found for people with MSD and limited evidence for people with CMD for social support provided by the supervisor and co-workers. All evidences for both populations [9,10,11,12,13,14,15,16,17,18,19] are in the same direction, indicating that higher social support from supervisor and co-workers is a protective factor, i.e. it reduces the time needed to RTW after sick leave regardless of the type of work disability considered (mental or musculoskeletal). Social support from co-workers only and social support from supervisor only did not reach the sufficient level of evidence required by our criteria to be considered a predictive factor for both populations considered. From the predictive studies accounting for social support from supervisor and co-workers factor found in our literature review, four different tools emerged, namely: (1) the Job Content Questionnaire—social support scale [20], used in seven studies that included both populations [9, 12,13,14, 17,18,19]; (2) the modified work APGAR—social support at work scale [21], used in one study for MSD population [10]; (3) the Obstacles to Return-to-Work Questionnaire [15], used in one study for MSD population [15]; and (4) the Copenhagen Psychosocial Questionnaire—social support scale [22], used in one study in a CMD sample [16]. Following the evaluation strategy described in Fig. 3, all the identified tools for social support in the workplace were classified as being excellent in reason of their psychometric and practical features considered together (Table 2). A separate analyses of psychometric criteria and practical relevance indicates the Job Content Questionnaire—social support scale [20] and the Copenhagen Psychosocial Questionnaire—social support scale [22] as two tools with excellent scores on both the criteria considered (i.e. psychometric and practical).
Workplace Accommodations
Work accommodations are modifications or adjustments to the workplace procedures that allow a worker with special needs to perform the task required. It emerged in our literature review as a factor positively related to a quicker return-to-work among people with MSD and CMD with a limited level of evidence [23,24,25,26]. Each predictive study used a different tool to measure work accommodations (Table 2). All tools presented excellent practical relevance criteria (i.e. all practical criteria met), yet none of them met sufficient psychometric criteria (i.e. only predictive validity and face validity criteria met). For this reason, all tools were evaluated as questionable. One tool [26] is currently available in Swedish language solely, and thus it was not possible to evaluate it in the present study.
Job Strain
Job strain, defined as the combination of high demands and low levels of job control, emerged as a predictive factor of longer RTW with a strong level of evidence for MSD [11, 12, 18, 23] and a moderate level of evidence for CMD [11, 12]. The tool of choice for all studies was the Job Content Questionnaire (i.e., subscales: decision authority, skill discretion, and psychological job demands) [20], which showed excellent proprieties on psychometric and practical characteristics (Table 2).
Organizational Injustice
One study [27] was identified in finding the feeling of organizational injustice as significant predictor of RTW for the MSD population. The evaluation tool used in the study is the Return-to-Work Obstacles and Self-Efficacy Scale—organizational injustice dimension [27], used for both MSD and CMD population, but showing predictive evidence for the MSD population only (limited evidence). The tools showed excellent psychometric and practical characteristics.
Effort-Reward Imbalance
Effort-reward imbalance emerged as a risk factor with limited level of evidence in one study conducted among people with MSD [10]. This study used two items retrieved from the Effort Reward Imbalance questionnaire conceptualized by Siegrist and colleagues in 2004 [28]. Because the tool was not administered in its full validated version (i.e. only two items were used), the measure method used in the predictive study was evaluated as being questionable, because no complete judgment could be done on psychometric proprieties (i.e. only face validity and predictive validity could be evaluated).
Job Demands
Job demands emerged as a risk factor for RTW in MSD population with a limited level of evidence [15, 27, 29]. Insufficient evidence was obtained for the CMD population. Three tools were used in the predictive studies, two of which with excellent psychometric and practical characteristics, i.e. the Obstacles to RTW Questionnaire—Physical Workload and Harmfulness scale [15] and the Return-to-Work Obstacles and Self-Efficacy Scale—Job demands subscale [27]. The Questionnaire on the Experience and Evaluation of Work—Pace and amount of work subscale [30] used in one study [29] was judged as having good qualities (i.e. four on six criteria met as for psychometric evaluation, and three on four criteria met for practical relevance).
Quality of Leadership
Using the quality of leadership dimension of the Copenhagen Psychosocial Questionnaire [22], one study [31] identified the quality of leadership as predictor of RTW among people with CMD (limited evidence, Table 1). The tool showed excellent characteristics both on psychometric criteria (i.e. six on six) and practical relevance (i.e. four on four) (Table 2).
Job Control
Job control is defined as the ability of a person to influence what happens in the work environment. It emerged as a risk factor associated to RTW in the CMD population with a limited level of evidence [11, 12, 16, 19, 32], while insufficient evidences were found for the MSD population. Three different tools were used in the predictive studies, namely (1) the Job Content Questionnaire—Decision Authority and Skills Discretion subscales [20], evaluated with excellent qualities (i.e. six on six criteria met on psychometric characteristics), (2) the Copenhagen Psychosocial Questionnaire—Influence at work and Possibilities for development subscales [22], judged as having excellent psychometric (i.e. six on six criteria met on psychometric characteristics) and practical characteristics (i.e. three on four criteria met on practical relevance), and (3) the Questionnaire on the Experience and Evaluation of Work—Variety in your work and Independence in your work subscales [30], which was evaluated as excellent (i.e. four on six criteria met on psychometric characteristics and three on four criteria met on practical relevance).
Discussion
Summary of Main Results
In this systematic search and review, eight categories of organizational factors predicting RTW or long sickness absence in people with MSD and CMD were identified: social support from supervisor and co-workers, workplace accommodations, job strain, organizational injustice, effort-reward imbalance at work, job demands, quality of leadership of the supervisor and job control. For each of these factors, the measurement tools used to demonstrate the predictive validity were catalogued. Nineteen measurement tools were identified, ten of which showing good predictive validity for RTW in MSD populations, seven in CMD ones, and two in both populations. Among all identified tools, sixteen had been already validated and used in other studies, whereas three had no reference in the literature and were specifically designed for the purpose of the study in which they were used (i.e., self-constructed measurements). A wide range of psychometric and practical characteristics of the different measures was identified in this study concluding with most of the tools showing both excellent psychometric and practical characteristics.
Social support from supervisor and co-workers was found to be a significant predictor of RTW among people with MSD. Supervisors are usually directly involved in daily management of work disability in organizations, because of their role that makes them close and aware of most of the social dynamics happening in the workplace [33]. Supervisors are also the stakeholders employees refer to in order to change their work situation or to negotiate work accommodations [34]. It thus appears to play a particularly important role in facilitating RTW [35,36,37]. Co-workers can play a central role in shaping the work experience, and can potentially influence the management of work disability within organizations by keeping interactions and contacts with an injured colleague [38,39,40]. The literature also stresses out that having good relationships with co-workers can lead to a higher motivation to RTW after an injury [41]. In the literature concerning specifically the CMD population, it is mentioned that workplace social support reduces the risk for depressive symptoms [42, 43]. Supportive behavior from supervisor and co-workers makes also the RTW process somehow easier [44,45,46]. Concerning the tools used to measure social support from supervisor and co-workers, the Copenhagen Psychological Questionnaire [22] and the Job Content Questionnaire [20], specifically in their respective social support scales, were found to be the most commonly used by authors in our review, and showed predictive validity in both populations. These tools are characterized by both good psychometric and practical features, and within the years they have been validated in different versions and adapted to a variety of cultural contexts and languages.
Results of our study are in line with the literature posing that people who has been in sick leave need some sort of work accommodation (such as time off for clinical appointments) to facilitate their return to work (e.g., [47, 48]). Providing work accommodation is a common and recommended practice to facilitate the RTW and stay at work of the disabled employee (e.g., [49, 50]). What seems less clear in the literature is how to account and measure for work accommodations. In our appraisal of measurement tools, none emerged as having both good or excellent psychometric and practical characteristics. This calls for the development of new tools with more satisfying features, or for new investigations using existing validated tools (e.g., WANSS [51]) in RTW studies. As highlighted in the results of a recent scoping review [34], measuring adequately requested and feasible work accommodations will be useful for all RTW stakeholders since they need to coordinate their efforts during the RTW process, and make the most relevant choice all together.
Unsurprisingly, results from our systematic search and review showed perceived stress at work as an important factor of delayed RTW in both MSD and CMD populations. In general, it is well established in the literature that employees in high-strain jobs have lower RTW rates compared to employees in low-strain jobs [52]. Job strain is a well-known concept that refers to high demands and low control at work, which is, usually, measured using a combination of dimensions delivered from the Job Content Questionnaire [20]. The questionnaire showed both excellent psychometric and practical characteristics in our review. Remaining out of work in the case of excessive demanding and stressful jobs can be considered as a coping strategy to avoid or reduce the source of stress generated by the working conditions [53].
Organizational injustice refers to the employee’s belief that there has been an unfair treatment in the workplace, in terms of outcomes, procedures or interpersonal relations [54]. Some studies have shown that organizational injustice is associated with decreased risk of sickness absence [55,56,57,58,59]. However, inconsistent results and large between-study differences persist in the literature [60]. In the present review focusing on the RTW process (not on the risk of sickness absence), only one study investigated organizational injustice as predictor of RTW. In the study of Corbière and colleagues [27], the feeling of organizational injustice was found to delay RTW among the population with MSD, but not with CMD. Regarding the latter, it seems important to mention how the relationship between mental health and perceptions of organizational injustice remains an open debate in the literature, with some authors suggesting that health difficulties may affect perceptions of the work environment [61]. The tool used in the predictive study identified in our review is the dimension “feeling of organizational injustice” of the Return-to-Work Obstacles and Self-Efficacy Scale [27], which had both excellent psychometric and practical characteristics.
One study investigating the imbalance between effort and reward found it to be linked to RTW in a sample of workers with MSD [10], while one study conducted among a CMD sample showed insignificant results with this respect [62]. The tool most commonly used to measure effort-reward imbalance is the ERI questionnaire [63] which has been vastly used in the literature.
Job demands, meaning work pressure and workload experienced at work, emerged as risk factor of delayed RTW for people with MSD. This result is in line with the work of White and collaborators [64] which synthesised 27 systematic reviews concluding with job demands identified as a risk factor for disability and work absence. Under certain circumstances, job demands can motivate people at work and can be associated with feelings of learning and personal growth at work [52]. However, in the context of a physical disorder such as MSD, and in the specific RTW situation, job demands can be perceived more as an additional physical burden to the physical impairment causing disability [e.g., 63]. Moreover, it has been suggested that high job demands may induce a fear of relapse or worsening the health condition, reducing indirectly the employee’s wish to return to work quickly [65]. Other studies linked job demands to fear-avoidance behaviour in the MSD population, suggesting this as an explanation for the delay in RTW [66]. According to the quality appraisal, it appears that measurement tools of job demands do not need further developments.
Good leadership quality from the supervisor was shown to be linked to well-being and to decreased sickness absence in several studies [67, 68]. It appears to be central in the RTW process as well, as it facilitates a structured environment, which is a crucial feature for people with mental health issues. A leader who structures the work environment helps vulnerable employees to remain at work [69]. It is worth mentioning the partial conceptual overlapping between leadership quality and supervisor support since a good leader has to perform some form of employees support. In the present literature review, quality of leadership was found to be a predictor of quick RTW in people with CMD, while no studies were found investigating this concept among MSD populations. The associated measurement tools, a dimension of the Copenhagen Psychosocial Questionnaire [22] dealing with the nearest leaders’ ability to solve conflicts, plan work, prioritize well-being and ensure development opportunities, showed both excellent psychometric and practical characteristics.
Finally, job control emerged as a risk factor for delayed RTW in people with CMD. This finding further confirms results of other studies suggesting low job control influencing disability and absenteeism [64, 65, 70]. For people with CMD it seems important to count on a certain degree of control over their job. The worker could thus have a certain amount of flexibility and adjustment possibilities at work that might help in the regulation of their job tasks based on how they feel (i.e., their health conditions). This could indirectly increase the possibility of returning to work [71]. The measurement tools of job control that were identified and appraised here are excellent in terms of measurement properties, both on psychometric criteria and practical relevance.
Strengths and Limitations
This paper focused only on longitudinal associations between organizational factors and RTW outcomes. This is of relevance, as interventions on organizational factors can be planned to facilitate RTW. All independent variables of the studies selected were measured at baseline, with participants being sick-listed at that time. This paper also provides an evaluation of the tools used in the predictive studies, granting researchers and practitioners with information and suggestions on the use of a number of tools that showed predictive validity in people with MSD and CMD. Future researchers could eventually use the tools retained in this review to establish international comparisons.
The present study is subject to several limitations. Notably, a quality evaluation of studies (i.e., meta-analysis) included in the literature review was not conducted. The level of evidence is limited to the quantity of studies found with respect to our selection criteria, and to the arbitrary ratio coefficient chosen a priori. It is plausible that with an evaluation of the quality of studies, and with slightly different ratio coefficients, the level of evidence for some factors would have been different. However, one must remind that only prospective cohort studies were included, reinforcing our conclusions. The study was further limited by the choice of English or French languages: we may have missed important and meaningful studies presented in other languages. In relation to the evaluation of measurements and tools, we decided to limit it to the first validation study conducted (i.e., the original article) in order to fairly balance each tool evaluation. Many tools reported in this paper have updated versions that researchers and practitioners should prefer to use in future researches and in their day-to-day practice. Another potential limit is the fact that all the identified organizational factors in this review are studied by self-administered questionnaires. Moreover, we limited our search in classical/conventional databases, while it would have been interesting to also perform a search in databases specialized in tools and measurement instruments (e.g., Health and Psychosocial Instruments database—EBSCO, Registry of Scales and Measures).
Conclusions
Promoting RTW after the onset of a physical or mental disability has become a priority in all industrialized countries. Despite the important role played in the RTW process, organizational factors are usually less studied compared to other psychosocial characteristics. Our study provided a review of the modifiable organizational factors and associated measurements tools that showed predictive validity among people with MSD and CMD. The protective and risk working conditions that contribute to a quick or delayed RTW, and on which interventions can be programmed on, as well as the tools having high psychometric and practical characteristics to measure them were identified, reported, and discussed in this study. Notwithstanding the advantage to use standardized tools in international studies, we believe that information provided in this paper will be useful and highly valuable not only for health professionals working on work disability, but also for policymakers who are involved in the development of RTW policies.
References
Global Burden Disease. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017 - The Lancet [Internet]. 2017 [cité 5 févr 2019].
Dewa CS, Loong D, Bonato S. Work outcomes of sickness absence related to mental disorders: a systematic literature review. BMJ Open. 2014;4:e005533.
Sultan-Taïeb H, Parent-Lamarche A, Gaillard A, Stock S, Nicolakakis N, Hong QN, et al. Economic evaluations of ergonomic interventions preventing work-related musculoskeletal disorders: a systematic review of organizational-level interventions. BMC Public Health. 2017;17:935.
Gragnano A, Negrini A, Miglioretti M, Corbière M. Common psychosocial factors predicting return to work after common mental disorders, cardiovascular diseases, and cancers: a review of reviews supporting a cross-disease approach. J Occup Rehabil. 2018;28(2):215–231.
Dionne CE, Bourbonnais R, Fremont P, Rossignol M, Stock SR, Laperriere E. Obstacles to and facilitators of return to work after work-disabling back pain: the workers’ perspective. J Occup Rehabil. 2013;23(2):280–289.
Gray H, Adefolarin AT, Howe TE. A systematic review of instruments for the assessment of work-related psychosocial factors (Blue Flags) in individuals with non-specific low back pain. Manual Theraphy. 2011;16:531–543.
Corbière M, Fraccaroli F. La conception, la validation, la traduction et l’adaptation transculturelle d’outils de mesure: exemples dans le domaine de la santé mentale (Conception, validation and transcultural adaptation of tools: examples in the filed of mental health). In: Corbière M, Larivière N, editors, Méthodes qualitatives, quantitatives et mixtes dans la recherche en sciences humaines, sociales et de la santé. Québec: Presses de l’Université du Québec; 2014. p. 577–620.
Lecomte T, Corbière M, Briand C. Psychosocial functioning assessment. In: Mueser KT, Jeste DV, editors. Clinical handbook of schizophrenia. Guilford: Press NY; 2008. p. 135–144.
Baltov P, Cote J, Truchon M, Feldman DE. Psychosocial and socio-demographic factors associated with outcomes for patients undergoing rehabilitation for chronic whiplash associated disorders: a pilot study. Disabil Rehabil. 2008;30(25):1947–1955.
Dionne CE, Bourbonnais R, Fremont P, Rossignol M, Stock SR, Nouwen A, et al. Determinants of « return to work in good health » among workers with back pain who consult in primary care settings: a 2-year prospective study. Eur Spine J. 2007;16(5):641–655.
Haveraaen LA, Skarpaas LS, Aas RW. Job demands and decision control predicted return to work: the rapid-RTW cohort study. BMC Public Health. 2017;17(1):154.
Haveraaen LA, Skarpaas LS, Berg JE, Aas RW. Do psychological job demands, decision control and social support predictreturn to work three months after a return-to-work (RTW) programme? The rapid-RTW cohort study. Work. 2016;53(1):61–71.
Heymans M, de Vet H, Knol D, Bongers P, Koes B, van Mechelen W. Workers’ beliefs and expectations affect return to work over 12 months. J Occup Rehabil. 2006;16(4):685–695.
Lindell O, Johansson S-E, Strender L-E. Predictors of stable return-to-work in non-acute, non-specific spinal pain: low total prior sick-listing, high self prediction and young age. A two-year prospective cohort study. BMC Family Pract. 2010;11:79–89.
Marhold C, Linton SJ, Melin L. Identification of obstacles for chronic pain patients to return to work: evaluation of a questionnaire. J Occup Rehabil. 2002;12(2):65–75.
Netterstrom B, Eller NH, Borritz M. Prognostic factors of returning to work after sick leave due to work-related common mental disorders: a one- and three-year follow-up study. BioMed Res Intl. 2015;2015:596572.
Opsahl J, Eriksen HR, Tveito TH. Do expectancies of return to work and Job satisfaction predict actual return to work in workers with long lasting LBP? BMC Musculoskelet Disord. 2016;17(1):481.
Soucy I, Truchon M, Côté D. Work-related factors contributing to chronic disability in low back pain. Work. 2006;26(3):313–326.
Vemer P, Bouwmans CA, Zijlstra-Vlasveld MC, van der Feltz-Cornelis CM, Hakkaart-van Roijen L. Let’s get back to work: survival analysis on the return-to-work after depression. Neuropsychiatr Dis Treat. 2013;9:1637–1645.
Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick B. The Job Content Questionnaire (JCQ): an instrument for internationally comparative assessments of psychosocial job characteristics. J Occup Health Psychol. 1998;3(4):322–355.
Bigos SJ, Battié MC, Spengler DM, Fisher LD, Fordyce WE, Hansson TH, et al. A prospective study of work perceptions and psychosocial factors affecting the report of back injury. Spine. 1991;16(1):1–6.
Kristensen TS, Borritz M, Villadsen E, Christensen KB. The Copenhagen Burnout Inventory: a new tool for the assessment of burnout. Work Stress. 2005;19:192–207.
Anema J, Schellart A, Cassidy J, Loisel P, Veerman T, van der Beek A. Can cross country differences in return-to-work after chronic occupational back pain be explained? An exploratory analysis on disability policies in a six country cohort study. J Occup Rehabil. 2009;19(4):419–426.
Franche R, Severin C, Hogg-Johnson S, Côté P, Vidmar M, Lee H. The impact of early workplace-based return-to-work strategies on work absence duration: a 6-month longitudinal study following an occupational musculoskeletal injury. J Occup Environ Med. 2007;49(9):960–974.
Hogg-Johnson S, Cole D. Early prognostic factors for duration on temporary total benefits in the first year among workers with compensated occupational soft tissue injuries. Occup Environ Med. 2003;60(4):244–253.
Ekberg K, Wåhlin C, Persson J, Bernfort L, Öberg B. Early and late return to work after sick leave: predictors in a cohort of sick-listed individuals with common mental disorders. J Occup Rehabil. 2015;25(3):627–637.
Corbière M, Negrini A, Durand M-J, St-Arnaud L, Briand C, Fassier J-B, et al. Development of the Return-to-Work Obstacles and Self-Efficacy Scale (ROSES) and validation with workers suffering from a common mental disorder or musculoskeletal disorder. J Occup Rehabil. 2017;27(3):342.
Siegrist J, Starke D, Chandola T, Godin I, Marmot M, Niedhammer I, et al. The measurement of effort-reward imbalance at work: European comparisons. Soc Sci Med. 2004;58(8):1483–1499.
van der Weide W, Verbeek J, Sallé H, van Dijk F. Prognostic factors for chronic disability from acute low-back pain in occupational health care. Scand J Work Environ Health. 1999;25(1):50–56.
van Veldhoven M, Meijman T. Het meten van psychosociale arbeidsbelasting meteen vragenlijst. De Vragenlijst Beleving en Beoordeling van de Arbeid (VBBA) [Measuring psychosocial workload by means of a questionnaire. Questionnaire on the experience and evaluation of work]. Amsterdam: NIA; 1994.
Munir F, Burr H, Hansen JV, Rugulies R, Nielsen K. Do positive psychosocial work factors protect against 2-year incidence of long-term sickness absence among employees with and those without depressive symptoms? A prospective study. J Psychosom Res. 2011;70(1):3–9.
Norder G, Roelen C, van der Klink J, Bültmann U, Sluiter J, Nieuwenhuijsen K. External validation and update of a prediction rule for the duration of sickness absence due to common mental disorders. J Occup Rehabil. 2017;27:202–209.
Lemieux P, Durand MJ, Hong QN. Supervisors’ perception of the factors influencing the return to work of workers with common mental disorders. J Occup Rehabil. 2011;21(3):293–303.
Corbière M, Mazaniello-Chézol M, Bastien M-F, Wathieu E, Bouchard R, Panaccio A, Guay S, Lecomte T. Stakeholders’ role and actions in the return-to-work process of employees on sick-leave due to common mental disorders: a scoping review. J Occup Rehabil. 2019. https://doi.org/10.1007/s10926-019-09861-2.
Corbière M, Bergeron G, Negrini A, Coutu M-F, Samson E, Sauvé G, Lecomte T. Employee perceptions about factors influencing their return to work after a sick-leave due to depression. J Rehabil. 2018;84(3):3–13.
Durand M-J, Corbière M, Coutu M-F, Reinharz D, Albert V. A review of best work-absence management and return-to-work practices for workers with musculoskeletal or common mental disorders. Work. 2014;48(4):579–589.
Jetha A, LaMontagne AD, Lilley R, Hogg-Johnson S, Sim M, Smith P. Workplace social system and sustained return-to-work: a study of supervisor and co-worker supportiveness and injury reaction. J Occup Rehabil. 2018;28(3):486–494.
Chiaburu DS, Harrison DA. Do peers make the place? Conceptual synthesis and meta-analysis of coworker effects on perceptions, attitudes, OCBs, and performance. J Appl Psychol. 2008;93(5):1082–1103.
Dunstan DA, MacEachen E. Bearing the brunt: co-workers’ experiences of work reintegration processes. J Occup Rehabil. 2013;23(1):44–54.
Kosny A, Lifshen M, Pugliese D, Majesky G, Kramer D, Steenstra I, et al. Buddies in bad times? The role of co-workers after a work-related injury. J Occup Rehabil. 2013;23(3):438–449.
Main CJ, Burton AK. Economic and occupational influences on pain and disability. In: Main CJ, Spanswick CC, éditeurs. Pain management: an interdisciplinary approach [Internet]. Churchill Livingstone Publishers; 1999 [cité 5 févr 2019]. p. 63–88. Disponible sur: http://eprints.hud.ac.uk/id/eprint/7528/.
Netterstrøm B, Conrad N, Bech P, Fink P, Olsen O, Rugulies R, et al. The relation between work-related psychosocial factors and the development of depression. Epidemiol Rev. 2008;30(1):118–132.
Rugulies R, Bültmann U, Aust B, Burr H. Psychosocial work environment and incidence of severe depressive symptoms: prospective findings from a 5-year follow-up of the Danish Work Environment Cohort Study. Am J Epidemiol. 2006;163(10):877–887.
De Raeve L, Jansen NW, van den Brandt PA, Vasse RM, Kant Ij. Risk factors for interpersonal conflicts at work. Scand J Work Environ Health. 2008;34(2):96–106.
Janssen N, van den Heuvel WPM, Beurskens AJH, Nijhuis FJN, Schröer CAP, van Eijk JTM. The Demand-Control-Support model as a predictor of return to work. Int J Rehabil Res. 2003;26:1–9.
Nieuwenhuijsen K, Verbeek J, de Boer AGEM, Blonk R, van Dijk FJH. Supervisory behaviour as a predictor of return to work in employees absent from work due to mental health problems. Occup Environ Med. 2004;61(10):817–823.
Williams-Whitt K, Bültmann U, Amick B, Munir F, Tveito T, Anema J. Hopkinton Conference Working Group on Workplace. Disability Prevention Workplace interventions to prevent disability from both the scientific and practice perspectives: a comparison of scientific literature, grey literature and stakeholder observations. J Occup Rehabil. 2016;26(4):417–433.
Bastien M, Corbière M. Return-to-work following depression: what work accommodations do employers and human resources directors put in place? J Occup Rehabil. 2019;29(2):423–432.
Joyce S, Modini M, Christensen H, Mykletun A, Bryant R, Mitchell P, et al. Workplace interventions for common mental disorders: a systematic meta-review. Psychol Med. 2016;46(4):683–697.
Dewa CS, Trojanowski L, Joosen MC, Bonato S. Employer best practice guidelines for the return to work of workers on mental disorder-related disability leave: a systematic review. Can J Psychiatry. 2016;61(3):176–185.
Corbière M, Villotti P, Lecomte T, Bond GR, Lesage A, Goldner EM. Work accommodations and natural supports for maintaining employment. Psychiatric Rehabil J. 2014;37:90–98.
Karasek R, Theorell T. Healthy work: stress, productivity, and the reconstruction of working life. New York: Basic Books; 1990.
Kristensen T. Sickness absence and work strain among Danish slaughterhouse workers: an analysis of absence from work regarded as coping behaviour. Soc Sci Med. 1991;32(1):15–27.
Cropanzano R, Greenberg J. Progress in organizational justice: tunneling through the maze. In: Intl Rev Ind Org Psychol. New York: Wiley; 1997. p. 317–372.
Elovainio M, Kivimäki M, Steen N, Vahtera J. Job decision latitude, organizational justice and health: Multilevel covariance structure analysis. Soc Sci Med. 2004;58:1659–1669.
Head J, Kivimäki M, Siegrist J, Ferrie JE, Vahtera J, Shipley MJ, et al. Effort-reward imbalance and relational injustice at work predict sickness absence: the Whitehall II study. J Psychosom Res. 2007;63(4):433–440.
Hjarsbech PU, Christensen KB, Bjorner JB, Madsen IE, Thorsen SV, Carneiro IG, et al. A multi-wave study of organizational justice at work and long-term sickness absence among employees with depressive symptoms. Scand J Work Environ Health. 2014;40(2):176–185.
Kivimäki M, Elovainio M, Vahtera J, Ferrie JE. Organisational justice and health of employees: prospective cohort study. Occup Environ Med. 2003;60:27–33.
Ybema JF, van den Bos K. Effects of organizational justice on depressive symptoms and sickness absence: a longitudinal perspective. Soc Sci Med. 2010;70:1609–1617.
Robbins J, Ford M, Tetrick LE. Perceived unfairness and employee health: a meta-analytic integration. J Appl Psychol. 2012;97:235–272.
Kawachi I. Injustice at work and health: causation or correlation? Occup Environ Med. 2006;63(9):578–579.
Norlund S, Reuterwall C, Hoog J, Nordin M, Edlund C, Slunga Birgander L. Work related factors and sick leave after rehabilitation in burnout patients: experiences from the REST-project. J Occup Rehabil. 2011;21(1):23–30.
Siegrist J, Starke D, Chandola T, Godin I, Marmot M, Niedhammer I, et al. The measurement of effort-reward imbalance at work: European comparisons. Soc Sci Med. 2004;58(8):1483–1499.
White M, Wagner S, Schultz IZ, Murray E, Bradley SM, Hsu V, et al. Modifiable workplace risk factors contributing to workplace absence across health conditions: a stakeholder-centered best-evidence synthesis of systematic reviews. Work. 2013;45(4):1–12.
Janssen N, van den Heuvel W, Beurskens A, Nijhuis F, Schröer C, van Eik J. The demand-control-support model as a predictor of return to work. Int J Rehabil Res. 2003;26(1):1–9.
Soderberg M, Rosengren A, Gustavsson S, Schioler L, Harenstam A, Toren K. Psychosocial job conditions, fear avoidance beliefs and expected return to work following acute coronary syndrome: a cross-sectional study of fear-avoidance as a potential mediator. BMC Public Health. 2015;15:1263.
Lund T, Labriola M, Christensen KB, Bültmann U, Villadsen E, Burr H. Psychosocial work environment exposures as risk factors for long-term sickness absence among Danish employees: results from DWECS/DREAM. J Occup Environ Med. 2005;47(11):1141–1147.
Vahtera J, Kivimäki M, Pentti J, Theorell T. Effect of change in the psychosocial work environment on sickness absence: a seven year follow up of initially healthy employees. J Epidemiol Commun Health. 2000;54(7):484–493.
Nyberg A, Westerlund H, Magnusson Hanson LL, Theorell T. Managerial leadership is associated with self-reported sickness absence and sickness presenteeism among Swedish men and women. Scand J Public Health. 2008;36(8):803–811.
Krause N, Frank J, Dasinger L, Sullivan T, Sinclair S. Determinants of duration of disability and return-to-work after work-related injury and illness: challenges for future research. Am J Ind Med. 2001;40:464–484.
Johansson G, Lundberg O, Lundberg I. Return to work and adjustment latitude among employees on long-term sickness absence. J Occup Rehabil. 2006;16(2):185–195.
Huijs J, Koppes L, Taris T, Blonk R. Differences in predictors of return to work among long-term sick-listed employees with different self-reported reasons for sick leave. J Occup Rehabil. 2012;22:301–311.
Brendbekken R, Vaktskjold A, Harris A, Tangen T. Predictors of return-to-work in patients with chronic musculoskeletal pain: a randomized clinical trial. J Rehabil Med. 2018;50(2):193–199.
Schultz I, Crook J, Meloche G, Berkowitz J, Milner R, Zuberbier O, et al. Psychosocial factors predictive of occupational low back disability: towards development of a return-to-work model. Pain. 2004;107:77–85.
Vendrig A, Schaafsma F. Reliability and validity of the work and well-being inventory (WBI) for employees. J Occup Rehabil. 2018;28(2):377–390.
Bontoux L, Roquelaure Y, Billabert C, Dubus V, Sancho P, Colin D, et al. Prospective study of the outcome at one year of patients with chronic low back pain in a program of intensive functional restoration and ergonomic intervention. Factors predicting their return to work. Ann Readapt Med Phys. 2004;47(8):563–572.
van Duijn M, Lotters M, Burdof A. Influence of modified work on return to work for employees on sick leave due to musculoskeletal complaints. J Rehabil Med. 2005;37(3):172–179.
Stapelfeldt C, Christiansen D, Jensen O, Nielsen C, Petersen K, Jensen C. Subgroup analyses on return to work in sick-listed employees with low back pain in a randomised trial comparing brief and multidisciplinary intervention. BMC Musculoskelet Disord. 2011;12:112.
Nieuwenhuijsen K, Verbeek J, de Boer A, Blonk R, van Dijk F. Predicting the duration of sickness absence for patients with common mental disorders in occupational health care. Scand J Work Environ Health. 2006;32(1):67–74.
Munir F, Burr H, Hansen J, Rugulies R, Nielsen K. Do positive psychosocial work factors protect against 2-year incidence of long-term sickness absence among employees with and those without depressive symptoms? A prospective study. J Psychosom Res. 2011;70(1):3–9.
Katz J, Amick B, Keller R, Fossel A, Ossman J, Soucie V, et al. Determinants of work absence following surgery for carpal tunnel syndrome. Am J Ind Med. 2005;47(2):120–130.
Schultz I, Crook J, Berkowitz J, Meloche G, Milner R, Zuberbier O, et al. Biopsychosocial multivariate predictive model of occupational low back disability. Spine. 2002;27(23):2720–2725.
van der Giezen A, Bouter L, Nijhuis F. Prediction of return-to-work of low back pain patients sicklisted for 3–4 months. Pain. 2000;87(3):285–294.
Lammerts L, Schaafsma F, Eikelenboom M, Vermeulen S, van Mechelen W, Anema J, et al. Longitudinal associations between biopsychosocial factors and sustainable return to work of sick-listed workers with a depressive or anxiety disorder. J Occup Rehabil. 2016;26(1):70–79.
Moorman R. Relationship between organizational justice and organizational citizenship behaviors: do fairness perceptions influence employee citizenship? J Appl Psychol. 1991;76(6):845–855.
Acknowledgements
We acknowledge the valuable contributions of Maryse Gagnon (IRSST), Jean-Philippe Lachance (IUSMM), Julie Chabot, Annabelle Beauvais-St-Pierre, Scarlett Olivares-Fontaine and Marie-Andrée Richard to this study.
Funding
This study was supported by a grant from the Institut de recherche Robert-Sauvé en santé et sécurité du travail (Grant Number: 2014-0010).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Villotti, P., Gragnano, A., Larivière, C. et al. Tools Appraisal of Organizational Factors Associated with Return-to-Work in Workers on Sick Leave Due to Musculoskeletal and Common Mental Disorders: A Systematic Search and Review. J Occup Rehabil 31, 7–25 (2021). https://doi.org/10.1007/s10926-020-09902-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-020-09902-1