
Abstract
Recently, mass casualty incidents (MCIs) have been occurring frequently and have gained international attention. There is an urgent need for scientifically proven and effective emergency responses to MCIs, particularly as the severity of incidents is continuously increasing. The emergency response to MCIs is a multi-dimensional and multi-participant dynamic process that changes in real-time. The evacuation decisions that assign casualties to different hospitals in a region are very important and impact both the results of emergency treatment and the efficiency of medical resource utilization. Previously, decisions related to casualty evacuation were made by an incident commander with emergency experience and in accordance with macro emergency guidelines. There are few decision-supporting tools available to reduce the difficulty and psychological pressure associated with the evacuation decisions an incident commander must make. In this study, we have designed a mobile-based system to collect medical and temporal data produced during an emergency response to an MCI. Using this information, our system’s decision-making model can provide personal evacuation suggestions that improve the overall outcome of an emergency response. The effectiveness of our system in reducing overall mortality has been validated by an agent-based simulation model established to simulate an emergency response to an MCI.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Recently, mass casualty incidents (MCIs) have been occurring more frequently and have drawn increased international attention. The terrorist attacks of September 11, 2001 made the public realize the seriousness of MCIs [1]. In addition, the terrorist train bombings in Madrid on March 11, 2004 [2], the terrorist bombings in London on July 7, 2005 [3], the 2013 Boston marathon bombings [4] and the suicide bomber attack in downtown Tel Aviv on April 17, 2006 [5] have enhanced public awareness of the dangers of MCIs. The above MCIs are different from the MCIs caused by natural disasters. MCIs caused by natural disasters, such as floods, hurricanes, earthquakes and tsunamis, will result in serious damage to the local infrastructure, especially the communication and network infrastructures that may remain intact after MCIs that occur in urban areas, such as traffic accidents. With the recent worldwide increase in urbanization, emergency medical resources in urban areas have become strained [6, 7], making emergency medical responses more difficult when responding to terrorist attacks or natural disasters that cause MCIs in urban areas. There is an urgent need for scientifically proven and effective emergency responses to MCIs as the severity of such incidents continues to increase.
The emergency response to MCIs is a multi-dimensional and multi-participant dynamic process that must change in real-time. There are many sub-processes that need to be considered during an emergency response to MCIs, including casualty injury assessment and triage at the scene, medical resource allocation among different emergency sites, casualty evacuation strategies and strategies for admission to medical institutions [8]. MCIs can occur anywhere, and the causes of such incidents vary and include both natural disasters and man-made damage. The number of casualties suffered in an incident cannot be determined at the beginning of the event, and there is a large gap in casualty numbers among different incidents. The distribution of emergency medical resources, such as medical staff, medical equipment and evacuation vehicles is not balanced. The challenges faced during an emergency response to MCIs are far different from the response under normal circumstances and will vary based on specific circumstances. Large-scale public health emergencies can result in an overwhelming demand for healthcare resources [9]. There may be many critical casualties needing emergency treatment within a short time after an MCI. The injury types can vary, and thus it may be difficult for a single medical institution to handle all the casualties; the shortage of emergency medical resources can also become very significant. The above features suggest that post-MCI emergency response strategies should be efficiency-based rather than patient-focused to save as many lives as possible despite the shortage of emergency resources.
The current study of the emergency response to MCIs is focused on optimizing the use of existing medical resources and includes the following aspects. First, there is research focused on selecting indicators for casualty injury assessment at the scene of the incident and establishing a triage scoring system. The main aim of this research is to classify casualties according to the extent of injuries and to assign the appropriate level of medical resources based on those classifications; the goal of such research is the optimal utilization of existing medical resources. There are a number of scoring systems used to assess the extent of a casualty injury. The injury severity score (ISS) focuses on assessing casualties with combined injuries [10]. The revised trauma score (RTS) evaluates injuries based on systolic blood pressure (SBP), respiration rate and the Glasgow coma scale (GCS) [11]. The trauma and injury severity score (TRISS) determines the probability of survival based on ISS, RTS and patient age [12]. There are some triage schemas that give brief guidelines to emergency providers for rapidly processing as many casualties as possible and discriminating injury severity through color tags. These triage schemas include simple triage and rapid treatment (START), sort-assess-lifesaving interventions-treatment/transport (SALT), Careflight and others [13–17]. These schemas propose that casualties be sorted into four categories: immediate, delayed, expectant and ambulatory. Immediate patients are those deemed to be critically injured and requiring immediate intervention. Delayed patients are those injured “but not expected to die within the first hour if care is delayed.” Expectant patients are those who are presumed deceased or who have catastrophic injuries, with survival not expected. The START strategy treats immediate patients first, delayed patients second, and then others as possible. In practice, providers typically try to treat the patients in the worst condition first within each category. The Sacco Triage Method (STM) provides a mathematical model of resource-constrained triage, with an objective to maximize expected survival given constraints on timing and resource availability. Compared with START, STM has a better expected survival rate for casualties under simulated conditions [18]. There are special triage schemas for special casualties. Pediatric triage tape is an easy to use, major incident primary triage tool based on a modification of the triage sieve [19]. The jump START pediatric MCI triage tool is the world’s first objective tool developed specifically for the triage of children in multi-casualty/disaster settings [20, 21]. There are some shortcomings in the current triage scoring systems. Most triage schemas are based on simulations or exercise validation and have not been validated using evidence-based research in practical applications [22]. No triage schema can cover the numerous casualty types that may be faced in an MCI, which can reduce the adaptability and flexibility required for various MCIs. In practical applications, emergency providers differ widely in psychological quality, maturity and experience, which impacts triage decisions and affects the entire emergency response outcome after an MCI [14–16, 18, 23, 24].
Second, medical resources are limited during an emergency response to an MCI. Medical resources include medical staff, medical equipment, evacuation vehicles and the capacity of a medical institution to accept casualties. Although emergency physicians are often on the front lines of a disaster situation, too often they have not considered how they should modify their decision-making or use of resources to allow the “greatest good for the greatest number” [25]. Hence, studying the effectiveness of the emergency response strategy for MCIs is important. At present, many different types of research adopt mathematical models and computer simulations to verify and validate specific emergency response strategies. F. Fiedrich et al. [26] reported a dynamic optimization model that used a detailed description of operational areas and available resources to calculate resource performance and efficiency for different tasks related to an emergency response. John L. Hick et al. [25] categorized space, staff, supplies and specialization as four aspects to measure the emergency response ability of medical institutions. These resources are independent of each other and need to be allocated effectively during the emergency response. The allocation of scarce medical resources requires a trade-off between efficiency and ethics. Hui Cao et al. [27] used a discrete event simulation to evaluate four scarce resource-rationing principles, including first come first served, random, most serious first and least serious first. Although the least serious first principle exhibits the highest efficiency, it is not ethically flawless. Considering the tradeoff between the lifesaving efficiency and ethical issues, random selection is a relatively fair and efficient principle for allocating scarce medical resources in a natural disaster response. Current studies on resource allocation during an emergency response focus on evaluating macro decision principles using simulation methods. As a result, there is no evidence-based tool with the ability to adjust its resource allocation configuration according to the emergency response conditions.
Third, as information and communication technology has developed, new approaches have been created to address the emergency response to an MCI. The electronic triage tag was invented and is used as an information carrier for casualties. With the help of radio frequency identification (RFID) technology, the casualty’s medical data, which is recorded on the electronic triage tag, can be accessed throughout the entire emergency response process, improving the timeliness and reliability of information transmission [28–33]. Using mobile health and sensor technology, some wearable equipment can automatically obtain patient vital signs and transfer them to a networked mobile or computer application [29, 34, 35]. There are also systems that can link the MCI scene to medical institutions and share casualty information with all emergency organizations, which improves the quantity of emergency medical services [36–39]. Using computer modeling and simulation technology, researchers can simulate emergency response and evaluate special strategies for resource allocation or casualty treatment [40–48]. The emergency response to an MCI is a dynamic process during which information is continually produced and constantly aggregated. Collecting and analyzing the emergency information produced by all stakeholders involved in an MCI has high value. Taking advantage of emergency information, an emergency response process can be developed and implemented in an orderly manner, even in a chaotic MCI environment, which can maximize treatment efficiency and save more lives.
Considering the characteristics of the emergency response to MCIs, we have designed a mobile-based system that can support emergency providers in making evacuation decisions. The emergency staff and incident commander can interact with the system through a mobile application. The casualty’s entire medical data obtained during the emergency response can be integrated through standard data exchange interface health level 7 (HL7). The decision-making model is based on the casualty’s medical information and temporal data. Personalized evacuation suggestions offered by the decision-making model can maximize emergency resource utilization and minimize the casualty mortality rate. We also designed an agent-based simulation model to validate our system.
System architecture and methods
System architecture
By collecting and aggregating emergency information during MCIs, our system extends the management of temporal casualty data. The decision-making model in our system combines emergency medical data and temporal data to offer personalized evacuation suggestions that dynamically adjust evacuation strategies based on the efficiency of emergency resources utilization. Emergency providers and incident commanders can interact with our system through a mobile application to manage casualty information and gain decision support.
In our previous study, we examined the system components of our mobile system, which includes “first-responder mobile devices”, “triage and transportation supporting devices” and “the emergency data transfer bus” [49]. With regard to this issue and based on our previous study, we added two new modules (a temporal data management module and an evacuation decision-making module) to improve the mobile system’s performance in an emergency response to an MCI. Using a mobile application, emergency providers have the ability to record a casualty’s vital signs at the scene of the incident, assess injury extent, evacuate the casualty to a medical institution and manage the casualty’s temporal data during the entire emergency response process. The casualty’s medical information is transmitted to the emergency center server by HL7 message. If the casualty has been evacuated to a medical institution, the emergency staff of the medical institution can access emergency information collected at the scene or on the way to the hospital through the HL7 interface. Then, medical and temporal data produced at the evacuation hospital will be transmitted to the emergency center server. As shown in Fig. 1, the emergency center server consists of four parts: the HL7 adapter, the temporal data server, the emergency clinical data server and the decision-making model. The HL7 adapter can acquire and analyze HL7 messages and store casualty data in an emergency database according to data organization rules. The temporal data server is used to store and manage the casualty’s temporal data produced during the entire emergency response, and these temporal data can be used to monitor the distribution of casualties and emergency medical resources. The emergency clinical data server is used to store and manage all the clinical information for the casualties; this clinical information includes vital sign data, treatment data, injury data, evacuation data and hospital admittance data. Section “System database model” details the database models of the clinical and temporal databases. The decision-making model is the core module of our system. The decision-making model combines casualty survival prediction and emergency process analysis by extracting data from both the emergency clinical and the temporal databases. Section “Decision-making model” shows a novel data-driven casualty evacuation decision support model that offers personalized evacuation suggestions based on effective regional emergency resource utilization.

System architecture
System database model
Our system not only has the ability to manage emergency medical data gathered by emergency providers but can also record the casualty’s temporal changes during the emergency response to an MCI. The data management of our system needs to meet the demands of a decision-making model that queries and analyzes data efficiently and in real-time. To meet the above requirements, we designed our system database model as shown in Fig. 2. The database model is divided into three parts using three distinguishing colors. Blue identifies the data model used to store and manage a casualty’s temporal information. The temporal data model tracks a casualty’s position throughout the emergency response to an MCI. Yellow identifies emergency resources such as evacuation vehicles, evacuation medical institutions and medical care sites. The care sites are divided by type into incident sites, emergency departments (EDs), intensive care units (ICUs) and general wards (GWs); with the help of the data model named environment, the system has the capacity to store information regarding the environment of the incident site, which includes environmental characteristics, such as open fire or nuclear disclosure. The information regarding the environment will help the emergency providers to perform the corresponding disposal. The database records the emergency response capacity of each care site. In this study, the emergency response capacity of a care site is measured by the number of casualties who can be taken to the care site. There are many factors that affect the actual emergency response ability, including the number of available medical staff, the amount of emergency equipment, the number of available beds and the amounts of pharmaceuticals and consumables. A shortage of any these factors may have an effect on a casualty’s emergency treatment. Hence, we determine the number of casualties who can be taken to a care site as the capacity of that care site to directly connect the emergency resource to the emergency treatment outcome. For example, an ICU is an important site for the continuous monitoring of critical patients. The core resource in ICUs is the ICU beds that are required to continuously care for the patients and provide life support. In the ICU ward, the medical staff members are arranged according to beds. Therefore, we take the available bed number in the ICU as the measurement of its capacity. In the case of transportation, there has recently been an increase in the types of vehicles that can be used to evacuate casualties to medical institutions from incident sites [38, 50, 51]. Our system includes an interface to manage and coordinate various types of evacuation vehicles. The interface makes our system more flexible and allows it to adapt to the multi-level resource allocation required in a metropolis. Green indicates the part of the data model responsible for storing and managing casualty medical information. This part focuses on recording the injury and vital signs of casualties at the scene of the incident. We designed this vital sign data model based on the conception of entity-attribute-value to allow the flexibility to expand vital sign types. There is some medical information produced at medical institutions that is temporarily not included in our data model. These data belong to the inner business processes of medical institutions and have a low effect on the emergency response to an MCI. If needed, these data can be extracted from the clinical data center using the HL7 interface. Our data model is chiefly concerned with the final destination and outcomes and is focused on providing accurate and reliable data.

System database model
Decision-making model
To dynamically assign casualties to the appropriate medical institutions, we propose a decision model based on survival prediction and emergency process data. For every casualty, this model can provide a special evacuation suggestion that can be used by emergency providers. The proposed model meets the emergency resource needs of the casualty and balances the emergency response capacity among different medical institutions, improving the overall survival probability. At the scene of the incident, an incident commander receives the suggestion provided by the decision-making model using a mobile application. The process of the decision-making model is shown in Fig. 3. The variables used in decision-making model are as follows:

Process of the decision-making model
-
i symbol: a casualty who is about to be evacuated to a medical institution
-
j symbol: a medical institution
-
S(i,t) symbol: the survival prediction function for casualty i. The variable t represents the time interval.
-
ESP(i,j) symbol: expected survival probability for casualty i if i has been evacuated to medical institution j.
-
D(i) symbol: expected department to which casualty i should be admitted.
-
WT(i,j,D(i)) symbol: casualty i’s expected wait time for D(i) of medical institution j.
-
RESP(i,j) symbol: revised expected survival probability for casualty i, including wait time.
When the incident commander considers where to evacuate a casualty, the suggestion is given by following the automatic operation steps provided by the decision-making model. First, our system calculates the casualty’s survival probability based on his/her injury information. Our previous study has developed a method for predicting survival probability over time based on initial injury information. Second, our system calculates the expected survival probability for casualty i if i has been evacuated to medical institution j:
where T j represents the time needed to evacuate the casualty to medical institution j.
Third, our system chooses one department D(i) from ED, ICU or GW to which casualty i should be admitted based on his/her ESP(i,j). Then, the expected wait time WT(i,j,D(i)) is calculated using the following equation, where M represents the number of casualties who have been treated in D(i) of institution j:
The decision-making model is an optimization problem that is used to identify the maximum of the following function:
The institution j, which makes the RESP(i,j) obtain the maximum, is the chosen medical institution and will be the evacuation target of casualty i.
System validation
In order to valid our system, especially the decision making model, we design an agent-based simulation model to simulate the emergency response to an MCI. There have been many approaches used to simulate emergency responses to MCIs, including analytical models and simulation models. The analytical models rely on a mathematical model to determine the optimal solution for the emergency response to an MCI, including the minimum response time and maximum coverage. In contrast to the analytical model, a simulation model is used to model each entity in an MCI to describe the entity’s properties and expected behavior during events. Simulation models can provide an entity’s final outcome by analyzing a special behavior pattern based on its relationship with other entities and between the entity and relevant circumstances. There are two approaches adopted in simulation research: one is discrete event simulation, and the other is agent-based simulation. The agent-based simulation model (ABM) contains a collection of autonomous agents that can perceive the environment, exchange information, make operational decisions and act based on these decisions [52]. For our system to be validated, the casualty’s flow through emergency response must be simulated, and the system must adjust the process based on the determinations of our decision-making model. The simulation model can aggregate and analyze interactions among different entities and interactions between the entity and its circumstances. Based on the requirements discussed above, we chose an agent-based simulation model to validate our system.
Agents in the simulation model represent actual entities involved in emergency response to a MCI. The casualty agents are pseudo-agents that cannot move by themselves. They can be loaded and moved by ambulance or by medical staff in medical institutions. The first responder agents represent and behave as the emergency medical staff at the scene of an incident. Once the first responders arrive at the scene of an incident, they immediately begin to triage casualties and label those casualties with a colored tag. The incident commander agent has the ability to obtain information from other agents, such as the ambulance agent, casualty agent and hospital agent. The incident commander assigns casualties to medical institutions. The ambulance agents represent evacuation vehicles. They can load, transport and unload casualty agents and can evacuate casualties from the incident site to medical institutions. The target of the ambulance agent corresponds to the orders of the incident commander agent. The hospital agents represent medical institutions and include EDs, ICUs and GWs.
We adopted a casualty’s respiratory rate, pulse rate and best motor response (RPM) as representative of a casualty’s injury severity [53]. A RPM score is an integer value between 0 and 12, with smaller values corresponding to a more severe injury and lower survival probability. Each casualty was randomly assigned a RPM score at the beginning of the simulation. When the casualty is triaged by the first responder, he or she is then triaged into one of four categories based on the initial RPM score. The casualties with RPM scores of 1–4 are triaged as “Red”, RPM scores of 5–8 are triaged as “Yellow”, RPM scores of 9–12 are triaged as “Green” and RPM scores of 0 are triaged as “Black”. After the ambulance agents arrive at the scene of the incident, they begin to load casualties based on the setting rules and the incident commander’s orders. The ambulance agents act according to the following rules: only load casualties who have been triaged, use the worst-first pick up strategy, the number of passengers is limited by the capacity of the ambulance, one red casualty can be carried per vehicle and no waiting at the incident. When a casualty is evacuated to a medial institution, the first information that must be determined is whether the casualty can be treated at the hospital. If there aren’t enough medical resources to support a critical casualty’s medical treatment, there will be an ambulance diversion, and the ambulance will take the casualty to another hospital. Once casualties have arrived at a medical institution, they are admitted first to the ED, where the emergency staff assigns casualties to the appropriate medical treatment department (ICU, GW or ED). Casualties with RPM scores of 1–4 are sent to the ICU, those with RPM scores of 5–9 are sent to the GW, and those with RPM scores of 10–12 remain in the ED. All changes to a casualty’s injury during the emergency response are represented in the casualty’s RPM score. The casualty’s RPM score will decrease in the manner of Sacco’s Delphi estimates of casualty deterioration during the period before the casualty receives treatment [18]. The deterioration of RPM reflects the fact that without timely care or treatment, the health condition of a casualty could deteriorate continuously. In our simulation, the deterioration stops when the casualty enters a special department and receives medical treatment.
As shown in Fig. 4, one casualty is first triaged by the first responder agent and is given a triage tag that indicates the extent of his/her injury. Then, the incident commander agent gives an order to the ambulance agent to load the casualty and deliver him/her to a particular medical institution. When the casualty arrives at the hospital, he/she will first enter the ED room. After a second injury assessment, the casualty enters the ICU, GW or remains in the ED based on his/her assessment. Then, the medical staff in each department treats the casualty until he/she is ready for discharge. In this situation, there are three waiting queues that the causality must go through in order to receive treatment, which is due to the limited capacities of the different departments.

The process flow of casualty agents in the agent-based simulation model
Results
The Recursive Porous Agent Simulation Toolkit (Repast) was used as our simulation platform [54]. Repast has an abstract feature set and three concrete implementations. There are six models in the Repast feature set. These modules are the Engine, the Logging Module, the Interactive Run Module, the Batch Run Module, the Adaptive Behavior Module and the Domains Module. Repast has good platform compatibility and is easy to scale. Additionally, the simulation model can be combined with real geographic data using Repast.
The performance of our system is measured by mortality related to the emergency response to an MCI. We not only measure the overall mortality during the emergency response but also analyze the distribution of the locations of death, such as death on the way to a medical institution, death in the hospital and death at the scene of the incident. These measures are used to show the differences among different evacuation decision patterns. These decision patterns are shown in Table 1. There are two groups of patterns classified based on how casualties are selected when more than one casualty is present in a triage category. Pattern_1 to Pattern_4 are group one and rely on the random selection of a casualty when there is more than one casualty in each triage category; Pattern_5 to Pattern_8 comprise group two and consider the survival prediction provided using our decision model when each triage category has more than one casualty.
We assume that an MCI has occurred in an urban area. The number of casualties suffered in this MCI is 150. There are three medical institutions that can be used as evacuation targets. The initial emergency response capacity of the ED, ICU and GW in each hospital is 5. The simulation model runs 100 replications for each pattern.
We ran the simulation model through 100 replications of each evacuation decision pattern. The average mortality rate of these 100 replications was considered the pattern’s mortality rate. This approach avoids the randomness of a single experiment and reflects the impact of different patterns on the overall outcome of an emergency response to an MCI.
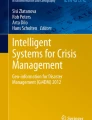
Figure 5 shows the morality rates associated with the evacuation decision patterns. This figure shows the following phenomena.

Mortality rate of the evacuation decision patterns
First, in each pattern group, the pattern that randomly chose hospitals had a relatively low overall mortality rate, which is an interesting phenomenon, suggesting that randomly choosing evacuation targets may evenly balance the load among the hospitals, which avoids long waiting times and situations in which there are no beds for patients who have been transported to the hospital. This randomization achieves a fairly good result. Second, in each pattern group, the pattern that considered the emergency capacity of medical institutions when choosing an evacuation target had the highest mortality rate. This outcome occurs because emergency capacity considered by the incident commander when he/she makes the evacuation decision is an instantaneous result that is different when the evacuated casualty has actually arrived at the hospital. In these decision-making patterns, the incident commander assigns many casualties to hospitals with the highest emergency capacity, but the emergency resources may have become overwhelmed by the time these casualties have arrived. As a result, the casualties were bound to either wait at the hospital for emergency treatment or be diverted to another facility, which results in a higher mortality rate. Third, in each pattern group, the pattern using the evacuation suggestion provided by our system’s decision model achieved the lowest mortality rate. This phenomenon shows the benefit of our decision-making model. Our system provides personalized evacuation suggestions to each casualty, which fulfills the specific requirements needed in that situation. The decision model also balances casualty admission pressure at each hospital in a manner similar to the random pattern. As a result, our model achieves the lowest simulated mortality rate. Fourth, when comparing groups, the group 2 patterns resulted in lower mortality rates than that in group 1 because group 2 considered the differences among casualty injuries in each triage category. This differentiation allows the incident commander to make an easy decision about how to preferentially evacuate casualties and contributes to a lower overall mortality.
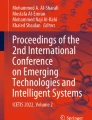
We analyzed the distribution of the location of death in detail. The location of death includes death on the way to medical institutions, death in hospitals and death at the scene of the incident. We compared a new performance measure named “the emergency effect rate” among different patterns. The emergency effect rate is the proportion of fatalities of treated casualties in terms of overall fatalities. The effects of different evacuation decision patterns on the MCI emergency response are clear. A lower emergency effect rate suggests more effective casualty assignment during the emergency response to an MCI. Figure 6 shows the emergency rate of the different patterns and reveals the following phenomena. First, the emergency effect rates of pattern_2 and pattern_6 were the worst. We presume that an inappropriate evacuation decision pattern not only failed to improve the emergency response outcome but also reduced the efficiency compared with a random pattern. Second, pattern_3 and pattern_7 performed better than pattern_2 and pattern_6, which indicates that considering emergency treatment waiting time at medical institutions, is more useful than considering the emergency capacity of those medical institutions when choosing an evacuation target. Third, pattern_8 shows the best performance with respect to the emergency effect rate. Most deaths occurred at the scene of incident as a result of a lack of emergency medical service. Minimal fatalities occurred during the casualty treatment process as patients were triaged by the first responders and either died or were discharged from the hospitals. Pattern_8 uses a different method for identifying the casualty’s injury, classifying casualties into four categories and distinguishing them with colored tags. Using our system, pattern_8 provides survival prediction to the incident commander based on injury information. This approach also reduces the difficulty and mental pressure placed on the incident commander by avoiding a comparison of casualties in same triage category. Pattern_8 utilizes the evacuation suggestion provided by our decision-making model, which uses a casualty’s expected survival probability as the evacuation target indicator. This approach mixes the casualty’s personal emergency requirements with the overall emergency resources available during an MCI emergency response. For example, when the emergency resources of hospital A are constrained, the waiting time for treatment in hospital A is prolonged and a casualty’s expected survival probability decreases. Once a casualty’s expected survival probability at hospital B is higher than at hospital A, the decision-making model will suggest that the incident commander evacuate the casualty to hospital B. Using this dynamic, real-time, personal decision-making model, pattern_8 achieves the best performance in the emergency effect rate.

Emergency effect rate of different patterns
Discussion
Making appropriate casualty evacuation decisions are of fundamental importance during the emergency response to a MCI. The evacuation decision refers to the strategy followed to transfer casualties to hospitals from the incident site. The casualty’s priority, the evacuation vehicle and the hospital’s emergency capacity are involved in making evacuation decisions. First, with respect to the casualty’s priority in the evacuation queue, assessing the casualty’s injury and providing an appropriate triage label are important. Once the casualty has been triaged, the emergency participants can treat the casualty according to his/her triage label, which also distinguishes the required level of emergency treatment. Casualties with the same triage tag will receive the same level of medical treatment. This approach provides high maneuverability and can simplify emergency operations at the scene of incidents, reducing the decision-making burden placed on emergency providers. Currently, most triage schemas used after MCIs follow the above principle. Triage schemas including START, STM, SALT and jumpSTART give evacuation priority to casualties based on triage decisions. However, when one triage category has many casualties, the incident commander must make a difficult decision about which casualties should be evacuated first. Hui Cao et al. [27] found that evacuating the least serious casualty first contributed to better overall emergency response outcomes, which is against the traditional triage principle of evacuating the worst casualty first. Second, the evacuation decision is associated with the emergency resource configuration in a MCI. There is some research using mathematical models to improve emergency resource configurations [26, 55, 56]. This research seems to have overlooked one important fact—that optimal emergency resource configuration is not the target. If the emergency resource does not provide the emergency treatment needed by casualties, an optimal configuration is useless. Because knowing the time, site and scale of an MCI in advance is difficult, the above research lacks actual operational and practical experience. Another idea to address emergency resource configuration utilizes evacuation decisions to assign casualties to different hospitals. An excellent evacuation decision can maximize the use of the emergency medical resources of each hospital in a region. There are many factors that must be considered, including the distance between the incident and the target hospital, the emergency capacity of the target hospital and the target hospital’s ability to address specific casualties. A study by Sharon Einav et al. [57] indicated that the nearest hospital plays an important role in MCIs, but a study by Yu Wang et al. [46] disputed those results. The simulation result of Yu Wang et al. [46] suggests that evacuating casualties to the nearest hospital may not be good for survival and instead increases overall mortality. Last but not least, as previously mentioned, the evacuation decision involves multi-dimensional, multi-domain and multi-participant coordination. We need not only a macro principle to fulfill the emergency response goal after a MCI but also operational approaches to implement this macro principle. We were unable to identify a similar method employed in the research area of the medical system, but some issues in the research area of operations research demonstrate various macro-principles in the emergency response to a MCI using a simulation method [44, 46, 47, 58]. Compared with the above study, our mobile system and evacuation decision model provide a more practical and individualized approach to the emergency response to a MCI. From the perspective of overall mortality, our mobile system is as good as the best result achieved in the above operation research.
In this study, we have designed a mobile-based system to collect medical and temporal data produced during an emergency response to an MCI. Using this information, our system’s decision-making model can provide personal evacuation suggestions that improve the overall outcomes of an emergency response. The effectiveness of our system in reducing overall mortality has been validated by an agent-based simulation model simulating an emergency response to an MCI. The aim of our system is to provide a solution to the problems associated with the rapid assessment of injuries at the scene of the incident by choosing evacuation targets based on individual injuries and dynamically allocating emergency resources within the region. The approach used to assess the casualty injuries at the scene of incidents has changed. Previously, emergency providers at the incident scene needed a variety of medical equipment devices to obtain vital signs and assess the casualty’s injury. With the development of sensor technology, there are now many wearable devices that integrate various vital sign acquisition sensors. These wearable devices facilitate more rapid vital sign collection and increase the efficiency of casualty injury assessment. These wearable devices produce a large amount of data that needs to be leveraged. In our previous study, we proposed a survival prediction model based on casualty injury data that include vital signs obtained by wearable devices. Survival prediction provides emergency providers with more detail about the deterioration of a casualty’s injury. In this study, the evacuation decision-making model is based on a combination of a casualty survival prediction model and available temporal data. Our system mainly fulfills the emergency treatment requirements for each casualty. Additionally, our system considers the emergency response capacity of different hospitals when providing an evacuation suggestion for each casualty. Our system controls the number of casualties assigned to each hospital from the incident source. By integrating the above decision-making approaches, the performance of our system in the simulation was the best. The overall mortality and emergency effect rates using our system were lower than the other simulated approaches.
We take advantage of the benefits of a mobile system to support evacuation decision making. By providing a personal evacuation suggestion for each casualty using a mobile terminator, our system greatly reduces the work load and psychological pressure faced by emergency providers at the incident scene. Our system interacts with all emergency response participants using a mobile application. Using our system, emergency response participants with different emergency training levels follow consistent evacuation principles when making evacuation decisions, which ensure that each casualty has the same opportunity to receive emergency treatment regardless of who is making the evacuation decision. With the help of wearable sensors, our mobile system has the capacity to monitor the casualty’s vital signs in real-time and provide a solid basis for decision making.
However, some challenges and limitations in the implementation of our mobile system were encountered. First, the predefined emergency response protocol (PERP) is an important prerequisite for the implementation of our system. The PERP will establish criteria for all of the emergency medical institutions within the area. The key to the PERP is to normalize the transmission of emergency information that is related to the information level and the information publicity of medical institutions. If a medical institution does not meet the criteria, the institution might not be included in the PERP until the level of its medical information improves. Second, in our mobile system, part of the patient’s medical record is required to train survival prediction models, and this requirement involves issues regarding patient privacy and data security. To protect a patient’s privacy, we must seek the patient’s informed consent or use an anonymizing method to mask personal data. Third, the implementation of our mobile system also involves medical staff training and exercising. In the traditional emergency response process, emergency providers do not need to operate the mobile application. Therefore, these providers might feel uncomfortable when they first receive/send emergency information through our mobile system. Various studies indicate that the system may not perform well if the users are unfamiliar with the system. Therefore, as the emergency provider becomes more and more familiar with our mobile system, our system will become more suitable for an emergency response to a MCI. Our system can be a practical and flexible method for determining the emergency response to an MCI.
Conclusions
In this study, we have designed a mobile-based system to collect medical and temporal casualty data produced during an emergency response to an MCI. Using this information, our system’s decision-making model can provide personal evacuation suggestions that improve the overall outcome of an emergency response. The effectiveness of our system in reducing overall mortality has been validated by an agent-based simulation model of the emergency response to an MCI.
References
Yurt, R. W., Bessey, P. Q., Alden, N. E., Meisels, D., Delaney, J. J., Rabbitts, A., and Greene, W. T., Burn-injured patients in a disaster: September 11th revisited. J. Burn Care Res. 27(5):635–641, 2006. doi:10.1097/01.bcr.0000236836.46410.f2.
Turegano-Fuentes, F., Perez-Diaz, D., Sanz-Sanchez, M., and Alonso, J. O., Overall asessment of the response to terrorist bombings in trains, Madrid, 11 March 2004. Eur. J. Trauma Emerg. Surg. 34(5):433–441, 2008. doi:10.1007/s00068-008-8805-2.
Aylwin, C. J., Konig, T. C., Brennan, N. W., Shirley, P. J., Davies, G., Walsh, M. S., and Brohi, K., Reduction in critical mortality in urban mass casualty incidents: analysis of triage, surge, and resource use after the London bombings on July 7, 2005. Lancet 368(9554):2219–2225, 2006. doi:10.1016/s0140-6736(06)69896-6.
D’Andrea, S. M., Goralnick, E., and Kayden, S. R., 2013 Boston marathon bombings: Overview of an emergency department response to a Mass Casualty Incident. Dis. Med. Public Health Prep 7(2):118–121, 2013. doi:10.1017/dmp.2013.53.
Raiter, Y., Farfel, A., Lehavi, O., Goren, O. B., Shamiss, A., Priel, Z., Koren, I., Davidson, B., Schwartz, D., Goldberg, A., and Bar-Dayan, Y., Mass casualty incident management, triage, injury distribution of casualties and rate of arrival of casualties at the hospitals: lessons from a suicide bomber attack in downtown Tel Aviv. Emerg. Med. J. 25(4):225–229, 2008. doi:10.1136/emj.2007.052399.
Derlet, R. W., and Richards, J. R., Overcrowding in the nation’s emergency departments: Complex causes and disturbing effects. Ann. Emerg. Med. 35(1):63–68, 2000. doi:10.1016/S0196-0644(00)70105-3.
Kadri, F., Harrou, F., Chaabane, S., and Tahon, C., Time series modelling and forecasting of emergency department overcrowding. J. Med. Syst. 38(9):1–20, 2014. doi:10.1007/s10916-014-0107-0.
Hirshberg, A., Holcomb, J. B., and Mattox, K. L., Hospital trauma care in multiple-casualty incidents: A critical view. Ann. Emerg. Med. 37(6):647–652, 2001. doi:10.1067/mem.2001.115650.
Arora, H., Raghu, T. S., and Vinze, A., Resource allocation for demand surge mitigation during disaster response. Decis. Support. Syst. 50(1):304–315, 2010. doi:10.1016/j.dss.2010.08.032.
Baker, S. P., O’Neill, B., Haddon, W., Jr., and Long, W. B., The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 14(3):187–196, 1974.
Moore, L., Lavoie, A., LeSage, N., Abdous, B., Bergeron, E., Liberman, M., and Emond, M., Statistical validation of the Revised Trauma Score. J Trauma Inj. Infect. Crit. Care 60(2):305–311, 2006. doi:10.1097/01.ta.0000200840.89685.b0.
Demetriades, D., Chan, L. S., Velmahos, G., Berne, T. V., Cornwell, E. E., Belzberg, H., Asensio, J. A., Murray, J., Berne, J., and Shoemaker, W., TRISS methodology in trauma: the need for alternatives. Br. J. Surg. 85(3):379–384, 1998. doi:10.1046/j.1365-2168.1998.00610.x.
Ryan, J. M., and Doll, D., In: Velmahos, G. C. C., Degiannis, E., and Doll, D. (Eds.), Mass casualties and triage. Springer, Berlin Heidelberg, pp. 151–159, 2012. doi:10.1007/978-3-642-20453-1_21.
Garner, A., Lee, A., Harrison, K., and Schultz, C. H., Comparative analysis of multiple-casualty incident triage algorithms. Ann. Emerg. Med. 38(5):541–548, 2001. doi:10.1067/mem.2001.119053.
Cross, K. P., and Cicero, M. X., Head-to-head comparison of disaster triage methods in pediatric, adult, and geriatric patients. Ann. Emerg. Med. 61(6):668–676.e667, 2013. doi:10.1016/j.annemergmed.2012.12.023.
Jenkins, J. L., McCarthy, M. L., Sauer, L. M., Green, G. B., Stuart, S., Thomas, T. L., and Hsu, E. B., Mass-casualty triage: time for an evidence-based approach. Prehospital Disaster Med. 23(1):3–8, 2008.
Lerner, E. B., Schwartz, R. B., Coule, P. L., and Pirrallo, R. G., Use of SALT triage in a simulated mass-casualty incident. Prehospital Emerg. Care 14(1):21–25, 2010. doi:10.3109/10903120903349812.
Sacco, W. J., Navin, D. M., Fiedler, K. E., Waddell, R. K., II, Long, W. B., and Buckman, R. F., Precise formulation and evidence-based application of resource-constrained triage. Acad. Emerg. Med. 12(8):759–770, 2005. doi:10.1197/j.aem.2005.04.003.
Wallis, L. A., and Carley, S., Validation of the paediatric triage tape. Emerg. Med. J. 23(1):47–50, 2006. doi:10.1136/emj.2005.024893.
Wallis, L. A., and Carley, S., Comparison of paediatric major incident primary triage tools. Emerg. Med. J. 23(6):475–478, 2006. doi:10.1136/emj.2005.032672.
Cicero, M. X., Riera, A., Northrup, V., Auerbach, M., Pearson, K., and Baum, C. R., Design, validity, and reliability of a pediatric resident JumpSTART disaster triage scoring instrument. Acad Pediatr 13(1):48–54, 2013. doi:10.1016/j.acap.2012.09.002.
Timbie, J. W., Ringel, J. S., Fox, D. S., Pillemer, F., Waxman, D. A., Moore, M., Hansen, C. K., Knebel, A. R., Ricciardi, R., and Kellermann, A. L., Systematic review of strategies to manage and allocate scarce resources during mass casualty events. Ann. Emerg. Med. 61(6):677–689.e101, 2013. doi:10.1016/j.annemergmed.2013.02.005.
Kahn, C. A., Schultz, C. H., Miller, K. T., and Anderson, C. L., Does START triage work? An outcomes assessment after a disaster. Ann. Emerg. Med. 54(3):424–430, 2009. doi:10.1016/j.annemergmed.2008.12.035.
Hong, R., Sierzenski, P. R., O’Connor, R. E., Bollinger, M., and Durie, C. C., Does the simple triage and rapid treatment method appropriately triage patients based on trauma injury severity score? Ann. Emerg. Med. 50(3, Supplement):S13, 2007. doi:10.1016/j.annemergmed.2007.06.069.
Hick, J. L., Hanfling, D., and Cantrill, S. V., Allocating scarce resources in disasters: Emergency department principles. Ann. Emerg. Med. 59(3):177–187, 2012. doi:10.1016/j.annemergmed.2011.06.012.
Fiedrich, F., Gehbauer, F., and Rickers, U., Optimized resource allocation for emergency response after earthquake disasters. Saf. Sci. 35(1–3):41–57, 2000. doi:10.1016/S0925-7535(00)00021-7.
Cao, H., and Huang, S., Principles of scarce medical resource allocation in natural disaster relief: A simulation approach. Med. Decis. Mak. 32(3):470–476, 2012. doi:10.1177/0272989x12437247.
Gao, T., and White, D., A next generation electronic triage to aid mass casualty emergency medical response. Conference Proceedings: Annual International Conference of the IEEE Engineering in Medicine and Biology Society IEEE Engineering in Medicine and Biology Society Conference Suppl 6501–6504, 2006. doi:10.1109/iembs.2006.260881.
Gao, T., Massey, T., Selavo, L., Crawford, D., Chen, B. R., Lorincz, K., Shnayder, V., Hauenstein, L., Dabiri, F., Jeng, J., Chanmugam, A., White, D., Sarrafzadeh, M., and Welsh, M., The advanced health and disaster aid network: A light-weight wireless medical system for triage. IEEE Trans. Biomed. Circ. Syst. 1(3):203–216, 2007. doi:10.1109/tbcas.2007.910901.
Morris, T. J., Pajak, J., Havlik, F., Kenyon, J., and Calcagni, D., Battlefield Medical Information System-Tactical (BMIST): the application of mobile computing technologies to support health surveillance in the Department of Defense. Telemed. J. E-Health Off. J. Am. Telemed Assoc 12(4):409–416, 2006. doi:10.1089/tmj.2006.12.409.
Fry, E. A., Lenert, L. A., MASCAL: RFID tracking of patients, staff and equipment to enhance hospital response to mass casualty events. AMIA Annual Symposium proceedings / AMIA Symposium AMIA Symposium 261–265, 2005.
Jokela, J., Simons, T., Kuronen, P., Tammela, J., Jalasvirta, P., Nurmi, J., Harkke, V., and Castren, M., Implementing RFID technology in a novel triage system during a simulated mass casualty situation. Int. J. Electron. Healthc. 4(1):105–118, 2008.
Ingrassia, P. L., Carenzo, L., Barra, F. L., Colombo, D., Ragazzoni, L., Tengattini, M., Prato, F., Geddo, A., and Della Corte, F., Data collection in a live mass casualty incident simulation: automated RFID technology versus manually recorded system. Eur. J. Emerg. Med. 19(1):35–39, 2012. doi:10.1097/MEJ.0b013e328347a2c7.
Lenert, L. A., Kirsh, D., Griswold, W. G., Buono, C., Lyon, J., Rao, R., and Chan, T. C., Design and evaluation of a wireless electronic health records system for field care in mass casualty settings. J. Am. Med. Inform. Assoc. 18(6):842–852, 2011. doi:10.1136/amiajnl-2011-000229.
Tollefsen, W. W., Gaynor, M., Pepe, M., Myung, D., Welsh, M., and Moulton, S., iRevive: a pre-hospital database system for emergency medical services. Int. J. Healthc. Technol. Manag. 6(4):454–469, 2005.
Poulymenopoulou, M., Malamateniou, F., and Vassilacopoulos, G., Emergency healthcare process automation using mobile computing and cloud services. J. Med. Syst. 36(5):3233–3241, 2012. doi:10.1007/s10916-011-9814-y.
Amailef, K., and Lu, J., Mobile-based emergency response system using ontology-supported information extraction. In: Lu, J., Jain, L., and Zhang, G. (Eds.), Handbook on decision making, vol. 33. Intelligent Systems Reference Library, Springer Berlin Heidelberg, pp. 429–449, 2012. doi:10.1007/978-3-642-25755-1_21.
Anantharaman, V., and Swee Han, L., Hospital and emergency ambulance link: Using IT to enhance emergency pre-hospital care. Int. J. Med. Inform. 61(2–3):147–161, 2001. doi:10.1016/S1386-5056(01)00137-X.
Mears, G. D., Pratt, D., Glickman, S. W., Brice, J. H., Glickman, L. T., Cabañas, J. G., and Cairns, C. B., The North Carolina EMS data system: A comprehensive integrated emergency medical services quality improvement program. Prehospital Emerg. Care 14(1):85–94, 2010. doi:10.3109/10903120903349846.
Amram, O., Schuurman, N., Hedley, N., and Hameed, S. M., A web-based model to support patient-to-hospital allocation in mass casualty incidents. J. Trauma Acute Care Surg. 72(5):1323–1328, 2012. doi:10.1097/TA.0b013e318246e879.
Kondaveti, R., and Ganz, A., Decision support system for resource allocation in disaster management. In: Engineering in Medicine and Biology Society, 2009. EMBC 2009. Annual International Conference of the IEEE, 3–6 Sept. 2009. pp 3425–3428. doi:10.1109/IEMBS.2009.5332498.
Reddy, M. C., Paul, S. A., Abraham, J., McNeese, M., DeFlitch, C., and Yen, J., Challenges to effective crisis management: Using information and communication technologies to coordinate emergency medical services and emergency department teams. Int. J. Med. Inform. 78(4):259–269, 2009. doi:10.1016/j.ijmedinf.2008.08.003.
Scheulen, J. J., Thanner, M. H., Hsu, E. B., Latimer, C. K., Brown, J., and Kelen, G. D., Electronic Mass Casualty Assessment and Planning Scenarios (EMCAPS): Development and application of computer modeling to selected national planning scenarios for high-consequence events. Ann. Emerg. Med. 53(2):226–232.e222, 2009. doi:10.1016/j.annemergmed.2008.09.014.
Hupert, N., Mushlin, A. I., and Callahan, M. A., Modeling the public health response to bioterrorism: Using discrete event simulation to design antibiotic distribution centers. Med. Decis. Mak. 22(5 suppl):S17–S25, 2002. doi:10.1177/027298902237709.
Su, S., and Shih, C.-L., Resource reallocation in an emergency medical service system using computer simulation. Am. J. Emerg. Med. 20(7):627–634, 2002. doi:10.1053/ajem.2002.35453.
Wang, Y., Luangkesorn, K. L., and Shuman, L., Modeling emergency medical response to a mass casualty incident using agent based simulation. Socio Econ. Plan. Sci. 46(4):281–290, 2012. doi:10.1016/j.seps.2012.07.002.
Cohen, I., Mandelbaum, A., and Zychlinski, N., Minimizing mortality in a mass casualty event: Fluid networks in support of modeling and staffing. IIE Transs Null Null, 2013. doi:10.1080/0740817X.2013.855846.
Rauner, M., Schaffhauser-Linzatti, M., and Niessner, H., Resource planning for ambulance services in mass casualty incidents: A DES-based policy model. Health Care Manag. Sci. 15(3):254–269, 2012. doi:10.1007/s10729-012-9198-7.
Tian, Y., Zhou, T.-S., Wang, Y., Zhang, M., and Li, J.-S., Design and development of a mobile-based system for supporting emergency triage decision making. J. Med. Syst. 38(6):1–10, 2014. doi:10.1007/s10916-014-0065-6.
Kearns, R. D., Hubble, M. W., Holmes, J. H., and Cairns, B. A., Disaster planning: Transportation resources and considerations for managing a burn disaster. J. Burn Care Res. 35(1):E21–E32, 2014. doi:10.1097/BCR.0b013e3182853cf7.
Taylor, C. B., Curtis, K., Jan, S., and Newcombe, M., Helicopter emergency medical services (HEMS) over-triage and the financial implications for major trauma centres in NSW, Australia. BMC Emerg. Med. 13:11, 2013. doi:10.1186/1471-227x-13-11.
Bonabeau, E., Agent-based modeling: Methods and techniques for simulating human systems. Proc. Natl. Acad. Sci. 99(suppl 3):7280–7287, 2002. doi:10.1073/pnas.082080899.
Sacco, W. J., Navin, D. M., Waddell, R. K. I., Fiedler, K. E., Long, W. B., and Buckman, R. F. J., A new resource-constrained triage method applied to victims of penetrating injury. J. Trauma Acute Care Surg. 63(2):316–325, 2007. doi:10.1097/TA.0b013e31806bf212.
North, M. J., Collier, N. T., and Vos, J. R., Experiences creating three implementations of the repast agent modeling toolkit. ACM Trans. Model. Comput. Simul. 16(1):1–25, 2006. doi:10.1145/1122012.1122013.
Wilson, D. T., Hawe, G. I., Coates, G., and Crouch, R. S., A multi-objective combinatorial model of casualty processing in major incident response. Eur. J. Oper. Res. 230(3):643–655, 2013. doi:10.1016/j.ejor.2013.04.040.
Messelis, T., and De Causmaecker, P., An automatic algorithm selection approach for the multi-mode resource-constrained project scheduling problem. Eur. J. Oper. Res. 233(3):511–528, 2014. doi:10.1016/j.ejor.2013.08.021.
Einav, S., Feigenberg, Z., Weissman, C., Zaichik, D., Caspi, G., Kotler, D., and Freund, H. R., Evacuation priorities in mass casualty terror-related events: Implications for contingency planning. Ann. Surg. 239(3):304–310, 2004. doi:10.1097/01.sla.0000114013.19114.57.
Martínez-Pérez, B., de la Torre-Díez, I., López-Coronado, M., Sainz-de-Abajo, B., Robles, M., and García-Gómez, J., Mobile clinical decision support systems and applications: A literature and commercial review. J. Med. Syst. 38(1):1–10, 2014. doi:10.1007/s10916-013-0004-y.
Acknowledgments
This work was supported by the National Natural Science Foundation (Grant No. 61173127), National High-tech R&D Program (No. 2013AA041201) and Zhejiang University Top Disciplinary Partnership Program.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Mobile Systems
Rights and permissions
About this article

Cite this article
Tian, Y., Zhou, TS., Yao, Q. et al. Use of an Agent-Based Simulation Model to Evaluate a Mobile-Based System for Supporting Emergency Evacuation Decision Making. J Med Syst 38, 149 (2014). https://doi.org/10.1007/s10916-014-0149-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10916-014-0149-3