
Abstract
Choosing the most suitable treatment for the scoliosis relies heavily on accurate and reproducible spinal curvature measurement from radiographs. Our objective is to reduce the variability in spinal curvature measurement by reducing the user intervention and bias. In order to determine the reliability of the spinal curvature measurement as it is in the clinical measurement of scoliosis a methodological survey has been carried out that concludes with inter and intra observer error variation. The proposed method list out horizontal inclination of all the vertebrae’s in terms of slopes using active contour models and morphological operators. This facilitates the radiologist to decide end vertebrae and hence inter/intra observer variation is completely eliminated. Tables 1 and 2 shows the observer error variation between manual and proposed methods in terms of mean and standard deviation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
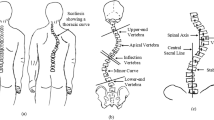
Scoliosis is defined as a substantial lateral curvature of the vertebral column. It involves lateral deviation of the spine in the frontal plane often accompanied by the rotation of individual vertebrae as shown in Fig. 1 [1]. Radiological imaging has traditionally been used in the identification, classification and monitoring the Scoliosis. Early detection and bracing treatment of juvenile and adolescent Scoliosis has decreased the need for surgery.

Normal and scoliotic spine
The management of the deformities usually involves observation, bracing and surgery. The severity of the condition has traditionally been measured by radiography. Assessment of the severity of the Scoliosis involves measuring the largest curvature of the spine known as the Cobb angle. This is measured on the back to front radiograph by selecting the most tilted vertebra at the top and bottom of the spine. This radiographic technique is standardized by the Scoliosis Research Society [12]. The Cobb–Lippman technique measures the curve severity by measuring the angle between the upper and lower endplates of the upper-end and lower-end vertebrae as shown in Fig. 2. The Cobb method is preferred because of its easier reproducibility, easier application and management of larger angles for more severe spinal curvature. Since the Cobb angle has been standardized a number of studies tested its reproducibility and reliability in measurement of Scoliosis.

Cobb angle calculation
This radiographic technique consists of identifying the end vertebrae of the curve (Fig. 2). The end vertebrae are defined as the inferior and superior-most segments that are inclined towards the concavity of the curvature being measured. A line is then drawn along the superior/inferior surface of the vertebra body of each of these two vertebrae. A perpendicular line is dropped from each of these lines. The angle formed by the two perpendicular lines is considered to be Cobb’s angle and represents the measurement of the curve [12]. Asymmetries in the contour lines indicate spinal deformity. Therefore the use of an accurate and reliable measuring method is important for a clear evaluation of the complex scoliotic curve. The reliability of radiographic measurement is crucial to treatment of idiopathic Scoliosis. Digital radiographs analysis will become more common as the technology becomes increasingly popular and affordable. Contrast, brightness and modification can be manipulated with digital techniques. However reliability of the technology for measuring the Cobb angle needs to be evaluated. Selecting the end vertebra significantly affects intra and inter-observer error. Use of different protractor, markers and pencil of varying width, poor quality radiographs are also intrinsic causes of error. In order to improve the reliability and accuracy of the Cobb angle measurement many computer algorithms were developed.
The proposed work in this paper uses advanced image processing techniques to automate quantification of spinal curvature. The motivation for the proposed work is discussed in section “Literature review” through the literature review. Followed by proposed work in section “Automated quantification of the spinal curvature” does automatic segmentation of all the vertebras within the radiographs and helps in deciding the true identification of superior and inferior vertebrae. Tilting of all these vertebras are calculated using morphological operators and Hough transform. In sections “Results” and “Discussion” the results and discussion of the proposed work. The paper concludes by eliminating the intrinsic source of error to minimize the measurement of discrepancies during quantification of scoliotic curvature.
Literature review
The human capability of quantitative evaluation of spinal curvature is limited due to non-symmetric search pattern. In addition to that technical limitation such as presence of noise, distinctive characteristic of imaging technique and variable positioning of the patient during image acquisition makes curvature measurement imprecise.
The Ferguson and the Cobb methods are the two commonly utilized techniques for measuring Scoliosis. In 1979 Barry F Jefferies [3] reported that a change in curvature of 5 degree may be due to variations in measurement rather than true improvement or worsening of the curve. They started a mathematical model and computer analysis for diagnosis of Scoliosis. The above said methods are based on drawing the lines parallel to superior endplate and inferior endplate. A second set of lines are drawn perpendicular to these end plates to determine the scoliotic angle, all these drawing needs human intervention, resulting in inter and intra observer variation.
In 1992 Arthur et al. [4] studied the difference between the scoliotic angle measured on posterior–anterior and anterior–posterior radiographs. Their study concludes that posterior-anterior has more variation error compared to anterior–posterior error.
In 1994 J E H Prujis et al. [5] tried to determine a reliable system for Cobb angle measurement for Scoliosis. Their study ends with a standard deviation about 3.2 degrees for the Cobb angle measurement, it should be taken into account when marking the decision in Scoliosis management.
K M Diab proposed a new method of measurement for scoliotic curve [6]. They reported that the level of significance of inter and intra observer difference between new, Cobb and Ferguson methods was significantly higher in curve with Cobb method. In the new method, the end vertebra and apical vertebra and four corners of each vertebra were identified using manual decision and the midpoint of each line was determined with a ruler.
In 2002 John Chung started analysis [7] of scoliotic deformity by means of computer assisted digital analysis. This study was to determine the reliability of computer assisted measuring system. All the computer assisted methods are bounded with human intervention, either in deciding the end plate vertebra or drawing the lines along those end plates.
Andrew V Linial et al. [8] proposed a direct method and apparatus for detection of Scoliosis. This innovative idea needs computer mouse to obtain continuous measurement of the human spine, hence ends with inter and intra variation.
In 2002 Ian et al. [20] tried to identify the sources of variability in scoliosis classification using rule based automated algorithm. For their rule based algorithm classification requires four different parameters from the standing posterior anterior radiographs. These four parameters are identifying apex level, end vertebra and Cobb angle. To obtain the quantitative measurement used in classification, unambiguously the coordinates of the bony landmarks identified visually in patients posterior-anterior radiographs. These leads to identification error as defined by Capassx [19].
Shannon et al. proposed a reliable Cobb angle measurement using active shape models in 2008 for idiopathic scoliosis [14]. They need a training set of radiographs representative of curves seen in scoliosis was used to train the software to recognize the vertebrae’s and active shape models cannot significantly deviate from variations and thus can only generate shapes similar to the training set. During the training set the boundary of the object is identified by manually digitizing n land marks points around the perimeter of the object in a image.
In 2007 Michael done the reliability assessment on the Cobb angle with manual versus digital measurement. They used ICC for the reliability assessment. They concluded that until a proper 3D measurement system, reliability cannot be assured. Digital radiography does not improve the measurement accuracy. For Cobb angle measurement, definition of the end vertebra introduces the main source of error [15].
In 2009 Hitesh Modi et al. [16] studied the reliability of Cobb angle between Juvenile and adolescent idiopathic scoliosis. In their study two observers independently measures the Cobb angle using computer based digital radiograms. Both the observer given pre-defined level of upper and lower end plates. Because of the pre-decision of the upper and lower end vertebraes, there was no significant difference in the Cobb angle measurement.
For the pediatric orthopedic [17], Eiten done the reliability analysis for the Cobb angle measurement using novel PACS computer software program. Their reliability relies on precise definition of bony landmarks for measurement angles, indexes and length of joints, limbs and spine. They concluded that most of the difference between specialist and non specialist were insignificant. The correlation between the results according to the number of bony landmarks that needed to be identified was also insignificant.
Finally technical report on Reliable Assessment of Cobb angle [18] using manual and digital methods says that Cobb angle in the frontal plane is an important parameter in the assessment of scoliosis, obtained from the radiographs. Technical advances allows increased use of digitized x- rays images in clinical practice. The computer assisted method is clinically advantageous and appropriate to assess the scoliotic curvature, but the end vertebra selection are the unsolved problem in this area.
In the above literature review on quantitative evaluation of spinal curvature is intended to avoid the human intervention in turn to remove inter and intra observer variation. The result of this study highlights the fact that even experienced spine specialist have significant difficulty in reliable and reproducible measurement of spinal curvature.
Automated quantification of the spinal curvature
The task is to provide a more reliable ways of performing scoliosis evaluation with more accurate and less time consuming and prone to fewer human error. The required manual point placement for quantification of spinal curvature on vertebral morphometry is time consuming and imprecise. It is difficult to place the marks exactly on the vertebral corners and furthermore, repeatability cannot be assured. Automatic determination of the detailed vertebral shape could enable more powerful quantitative tool for diagnosis of scoliosis through Cobb angle calculation. Goal is to prevent by early treatment of the deformity and cardiopulmonary complication secondary to scoliosis.
Traditional plane radiography currently and probably will remain the basic examination for the spinal deformities, because it provides on both the displacement and the deformation of the vertebral column. To use Cobb method, the end vertebral bodies must be determined. From the literature review, the decision of the end vertebrae itself is the main source of inter and intra observer error. The end vertebral bodies are those which have greatest tilt relative to horizontal baseline through the apex of the curve. These intervention causes the inter and intra observer error while deciding the most tilted end vertebral bodies. The automatic decision of the end vertebral bodies needs complete morphometry of all the vertebrae within the anterior-posterior view of the scoliotic radiographs. The proposed method shown in Fig. 3 relies on minimizing the user interaction in decision of the end plates and lines along the surface of superior/inferior end plates.

Automatic quantification of spinal curvature
Most segmentation relies on the edge information, objects with strong and continuous edges are relatively easier to segment. Because of low radiation, radiographs are noisy in nature. Inefficient imaging technique and interference from the other part makes the segmentation difficult. The major problem associated with edge based image segmentation algorithms are strongly dependent on target initialization and necessity for manual redesign of segmentation criteria whenever new segmentation problem encountered. It is difficult to fulfill the real data application especially in medical images where shape variation is a natural property. Its required to isolate the spine in order to remove undesired information, such as, the ribs, the head and legs. The process of segmenting the vertebral contour and its inclination are addressed in the next section through active contour models, morphological operators and Hough transform.
Anisotropic filtering
The anisotropic filter is based on the numerical solution of a partial differential equation describing the process of nonlinear anisotropic diffusion [9]
where f(x,y,t) represents the image function. The diffusion coefficient, g, is a decreasing function of the image gradient norm, \(\left\| \nabla f\right\|\). The diffusion process is inhibited around the edges where the image gradient is high. Different function can be used giving perceptually similar results such as:
The parameter K controls the rate at which the diffusion coefficient decreases as the norm of the image gradient increases. The value of K is set in relation to the gradient strength of edges of the vertebrae in the region of interest that are to be preserved during the diffusion [9].
Active contour models
For the segmentation of the vertebrae, Zhe Lin et al. [13] used template matching wherein the template comprised the whole vertebral body, which will suffer from when occlusion occurs. Computerized techniques have also been applied to vertebra extraction and will improve the landmark location. Performance of traditional approaches to edge based a medical image segmentation criterion that reflects higher level of knowledge about the segmented object that is through active contour models. In recent years researchers have published results using various forms of deformable template approach to segment the vertebrae. Without exception, these methods rely on user interaction for initialization. Snakes or active contours are extensively used in computer vision and image processing application [10].
A snake [10] is a deformable curve x(s) = [x(s), y(s)], s ∈ [0, 1], which gradually moves from its initial state under the influence of forces, and is expected to terminate on the object boundary at equilibrium. The curve evolution can be given by minimizing the snake total energy E:
where α and β are weighting parameters that control the snake’s tension and rigidity respectively, and x s (S) and x ss (S) denote the first and second derivatives of x(S) with respect to S. The external energy function E ext is derived from the image to take on its smaller values at boundaries. Minimizing the energy functional of Eq. 3 gives rise to the Euler equation
This can be viewed as a force balance equation: F int + F ext = 0, where the internal force, F int = αx ss (S) − βx ssss (S), discourages the snake stretching and bending and the external force, \(F_{\rm ext}=- \nabla E_{\rm ext}\), attracts the snake toward the image edges. Accordingly, the snake deformation can be described as the following evolution equation
The equilibrium solution of Eq. 5 represents the final snake curve under the influence of the internal and external forces which are counter balanced with each other.
Traditionally, the external force is formed by the gradient of the image or image edge map, which cannot pull the curve toward the desired boundary if the snake’s initial position is far away from the object boundary. To overcome this limit, the gradient vector flow (GVF) snake model [11] replaces the traditional external force with the GVF force v(x,y), which is defined as the equilibrium solution of the following vector diffusion equation:
where \(\nabla ^2\) is the Laplacian operator, \(\nabla\) is the gradient operator, f is the magnitude edge map of an image, and μ is a regulation parameter. The GVF force is nearly equal to the gradient of the edge map when it is large, but is slowly varying in homogeneous regions. Therefore, the GVF force has larger capture range and under its influence the snake can move into boundary concavities. Because of the nature of GVF, less sensitive to initialization, instead of manual initialization around the object of interest, it works with automatic initialization around the object of interest.
Morphological operation and Hough transform
GVF snakes results with complete vertebral boundary for the entire selected vertebra within the cropped region. Automatic decision of the end vertebra is based on the horizontal tilt information for the segmented vertebra. To retain the horizontal boundary information, we applied morphological operator with the proper structuring element as shown in Fig. 6. Hough transform will calculate the slope for these lines. This will be the direct information for the radiologist to deicide about the required vertebrae. Proposed method decides the end vertebras based on the objective criteria of measurement, so it eliminates inter and intra observer error.
Results
Reliability and reproducibility of the spinal curvature measurements is done through image processing techniques. In this work 250 radiographs are categorized into various groups based on the Cobb angle ([G1( < 100), G2(100 − 200), G3(200 − 300), G4(300 − 400), G5(400 − 500), G6( > 500)]) (Fig. 4).

Different groups of scoliotic radiograph [G1(<100), G2(100−200), G3(200−300), G4(300−400), G5(400−500), G6(>500)]
As read from the literature, it’s difficult to trace the vertebral boundary in presence of rib cage, pelvic and head part. We have chosen the region of interest, where exactly we can quantify the spinal curvature for diagnosing the scoliosis. Usually vertebrae have pixel with highest intensity in their neighborhood, although this brightness varies a lot among them. Therefore it needs a local threshold. That’s why anisotropic filtering is used to highlight the edges. Figure 5 shows the enhanced image after applying the anisotropic filtering. Anisotropic filtering is based on the numerical solution of partial differential equation describing the non linear isotropic diffusion. The diffusion process is inhibited around the edges where the image gradient is high.

Different groups of Enhanced Scoliotic radiograph [G1(<100), G2(100−200), G3(200−300), G4(300−400), G5(400−500), G6(>500)]
The enhanced images are given as input for the active contour algorithms. Parametric models need the initialization closer to the expected boundary. Snake algorithm takes the initialization as reference boundary, based on the presence of gradient value it converges to the expected boundary. But every time it’s difficult to work with manual initialization closer to the boundary in the noisy radiographs. To make the algorithm less sensitive to initialization, gradient vector filed snake is applied for better matching as explained in proposed section. To avoid the human intervention in the initialization step, it starts with an automated generation of template around/inside the expected boundary. Gradient vector flow snake works on the better matching based on the rotational and irrotational vector field for convergence. Figure 6 shows the GVF snake output based on the automatic initialization. Morphological operators are applied on the segmented output for the best fit slope decision of the superior and inferior end vertebrae for the quantification of Cobb angle. The results of the morphological operator is shown in Fig. 7. Hough transform is applied to get objective measurement parameter as slopes for the automatic decision of the end vertebraes.

Output of gradient vector field active contour segmentation

Output of morphological operator
Discussion
Quantitative measurement of spinal deformity is the preliminary step in order to plan a therapeutic regimen. On theoretical ground, the causes of errors in spinal curvature measurement are grouped as follows.
-
Errors in taking the radiographs
-
Errors intrinsic to the measurement method
-
Errors due to the anatomical deformity of the vertebra.
-
Observer error in measurement
The possible error introduced by the measurement is classified as identification error and technical error. Identification errors are due to the identification of superior, inferior and apical vertebrae. Technical errors are due to the drawing the lines tangent to the vertebral bodies, as it is not possible to draw the lines exactly tangent to the vertebral surfaces.
To reduce variability of Cobb angle measurement for Scoliosis assessment, a computerized method was developed. This method automatically measured the Cobb angle on spinal posterior-anterior radiographs after the brightness and the contrast of the image were adjusted, and the top and bottom of the vertebrae were selected. Here the selection of the vertebrae required for spinal curvature is once again by the manual decision.
To identify the extremes of the curve, it is necessary to evaluate the inclination of the vertebral bodies. The limiting vertebrae are the most oblique one while the apical vertebra is the most rotated and wedge done. To measure the Cobb angle, the end-vertebrae that tilt most severely toward the concavity of the spinal curve are identified. The Cobb angle can be manually measured by calculating the angle between the lines respectively drawn along the upper endplate of the superior end-vertebra and the lower endplate of the inferior end-vertebra, as shown in Fig. 2.
However, the manual measurement of Cobb angle depends on experience and judgment. Errors are due to selecting different end vertebrae and estimating different slopes of the vertebrae. The intra observer error variations, on the different groups of Cobb angle are noted in the Table 1. In addition, the manual measurement is tedious and time-consuming. This proposed work is a new approach which extracted the vertebral boundary using image processing technique for the decision of the end plates. After the decision of the end-vertebrae the Cobb angle is calculated.
Intra observer error in quantification of spinal curvature
The overall goal of this study was to reduce measurement error of the Cobb angle by reducing the judgment required in measuring the severity of idiopathic Scoliosis. In Table 1 we have noted down the mean and standard deviation in intra observer error variation for manual and automatic at three different intervals.
Proposed method eliminates the observer error through the true identification of the required end vertebras. Table 1 gives the observer error variation between manual and proposed method. We can conclude that observer error is more in case of manual method. Manual method causes error in different stages, while deciding the end vertebra, land marking on the noisy radiographs and finally while drawing the lines, hence it will have cumulative effect. With respect to the proposed system, decision of the end vertebra is automatic. It needs minimum human intervention while creating the initial contour that is part of preprocessing. Retaining the horizontal lines and slope estimation are completely automatic.
In Table 2, we can observe the inter observer error variation under different groups of Cobb angle. This table describes about the inter observer error variation between five different people for manual, and automated.
Conclusion
Reliability of Cobb angle measurement plays significant role in the treatment of scoliosis. Identifying the end vertebral plates is the main source of error and most of the computer assisted method works on the preselected end vertebras. The proposed work automates the identification of end vertebras using image processing techniques. Hence inter and intra observer errors during Cobb angle quantification is completely eliminated.
References
Cobb, J., Outline for the study of scoliosis. Ar. Acad. Orthop. Surg. Instr. Course Lect. 5:261–175, 1948.
Nash, C., and Moe, J., A study of vertebral rotation. J. Bone Jt. Surg. Am. 51:223–229, 1969.
Jeffries, B. F., et al., Computerized measurement and analysis of scoliosis. Pediatr. Radiol. 134:381–385, 1980.
Arthur, A., et al., A clinical study of the differences between the scoliotic angles measured on poster anterior and antero posterior radiographs. J. Bone Jt. Surg. 64(A):489–493, 1982.
Pruijis, J. E. H., et al., Variation in Cobb angle measurements in scoliosis. Skelet. Radiol. 23:517–520, 1994.
Diab, K. M., et al., Accuracy and applicability of measurement of the scoliotic angle at the frontal plane by Cobb’s method, by Ferguson’s method and by a new method. Eur. Spine J. 4:291–295, 1995.
Cheung, J., et al., The reliability of quantitative analysis on digital image of the scoliotic spine. Eur. Spine 11:535–542, 2002.
Linial, A. V., and Aktinson, R. W., Methods and apparatus for detection and measurement of scoliosis of the spine, USPatent-US2006/0015042 A1, 2006.
Perona, P., and Malik, J., Scale-space and edge detection using anisotropic diffusion. IEEE Trans. Pattern Anal. Mach. Intell. 12(7), 1990.
Kass, M., et al., Snakes: active contour models. Int. J. Comput. Vis. 9:321–331, 1988.
Xu, C., and Prince, J. L., Snakes, shapes, and gradient vector flow. IEEE Trans. Image Process. 7(3):359–369, 1998.
Vrtovec, T., et al., A review of methods for quantitative evaluation of spinal curvature. Eur. Spine. J., 2009.
Lin, Z., Davis, L. S., Doermann, D., and DeMenthon, D., Hierarchical part-template matching for human detection and segmentation. 978-1-4244-1631-8/07/25.00, IEEE, 2007.
Allen, S., Parent, E., Khorasani, M., Hill, D. L., Lou, E., and Raso, J. V., Validity and reliability of active shape models for the estimation of Cobb angle in patients with adolescent idiopathic scoliosis. J. Digit. Imaging 21(2):208–218, 2008.
Gstoettner, M., Sekyra, K., Walochnik, N., Winter, P., Wachter, R., and Bach, C. M., Inter and intra-observer reliability assessment of the Cobb angle: manual versus digital measurement tools. Eur. Spine J. 16:1587–1592, 2007.
Modi, H. N., Chen, T., Suh, S. W., Mehta, S., Srinivasalu, S., Yang, J.-H., and Song, H.-R., Observer reliability between juvenile and adolescent idiopathic scoliosis in measurement of stable Cobb’s angle. Eur. Spine J. 18:52–58, 2009.
Segev, E., Hemo, Y., Wientroub, S., Ovadia, D., Fishkin, M., Steinberg, D. M., and Hayek, S., Intra and interob server reliability analysis of digital radiographic measurements for pediatric orthopedic parameters using a novel PACS integrated computer software program. J. Child Orthop. 4:331–341, 2010.
Tanure, M. C., Pinheiro, A. P., and Oliveira, A. S., Technical report reliability assessment of Cobb angle measurements using manual and digital. Spine J. 10:769–774, 2010.
Capasso, G., et al., The validity and reliability of measurement of spinal deformity. Acta orthopedia Belgica 58(2):126–135, 1992.
Ian, A. F., et al., Identifying sources of variability in scoliosis classification using a rule-based automated algorithm. SPINE 27(24):2801–2805.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
H, A., Prabhu, G.K. Automatic Quantification of Spinal Curvature in Scoliotic Radiograph using Image Processing. J Med Syst 36, 1943–1951 (2012). https://doi.org/10.1007/s10916-011-9654-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10916-011-9654-9