
Abstract
Latinos in the US are disproportionately affected by HIV and are at risk for late presentation to care. Between June 2011 and January 2012, we conducted a cross-sectional survey of 209 Baltimore Latinos at community-based venues to evaluate the feasibility of using information communication technology-based interventions to improve access to HIV testing and education within the Spanish-speaking community in Baltimore. Participants had a median age of 33 years interquartile range (IQR) (IQR 28–42), 51.7 % were male, and 95.7 % were foreign-born. Approximately two-thirds (63.2 %) had been in the US less than 10 years and 70.1 % had been previously tested for HIV. Cell phone (92.3 %) and text messaging (74.2 %) was used more than Internet (52.2 %) or e-mail (42.8 %) (p < 0.01). In multivariate analysis, older age and lower education were associated with less utilization of Internet, e-mail and text messaging, but not cell phones. Interest was high for receiving health education (73.1 %), HIV education (70.2 %), and test results (68.8 %) via text messaging. Innovative cell phone-based communication interventions have the potential to link Latino migrants to HIV prevention, testing and treatment services.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Latinos are the largest and fastest growing ethnic minority in the United States, with a total population of 50.5 million in 2010 [1]. During the last decade, the Latino population of Baltimore City increased by 135 %, primarily due to recent migration of individuals born in Central America and Mexico [2, 3]. As in other rapid-growth regions, such as the southeastern US, Latinos living in Baltimore are more likely to be young, male, foreign-born and in the US for less than 15 years, compared to those from states with well-established Latino communities such as New York, Florida, and California [4]. Demographic changes have resulted in high demand for culturally competent services, which may not be readily available in rapid growth states. Lack of services sensitive to the needs of migrants can exacerbate disparities in quality and access to health care.
Latinos living in the US are disproportionately affected by HIV, and have an estimated lifetime risk (ELR) of infection 3.2 times higher than for Whites [5]. From 1997 to 2006, rates of AIDS cases in Baltimore City decreased 40 % among non-Hispanic Blacks and 23 % among non-Hispanic Whites, but nearly doubled among Latinos (from 40.8 to 80.0 cases/100,000 people), and mortality due to AIDS among Latinos was twice that of non-Latino Whites [6]. Furthermore, Latinos are often diagnosed in the later stages of disease [7–11]. Late diagnosis is associated with high mortality, and unrecognized infection increases HIV transmission in the community [12].
Foreign-born Latinos are at particularly high risk for late presentation, with a shorter interval from HIV diagnosis to AIDS when compared with US-born Latinos [9]. CDC data shows that Latinos born in Mexico or Central America are more than twice as likely to be diagnosed late with HIV than Latinos born in the US [11]. Non-English speaking Latinos in Los Angeles county are almost three times more likely to present late to care than English-speaking Latinos [13]. In North Carolina, a state that has experienced a rapid increase in the Latino foreign-born population, Latinos present to HIV care with a lower CD4 count than African Americans (186 vs. 302 cells/mm3) and account for a majority of serious opportunistic infections in the clinic, including tuberculosis and histoplasmosis which are likely acquired in their country of origin [10, 14]. Therefore, immigrants have a particular need for targeted interventions to provide earlier access to HIV testing.
Foreign-born Latinos are also vulnerable to factors that have been shown to impact access to HIV services, such as self-awareness of risk, immigration status, cultural background, isolation, and disruptions of social and family relationships [15–17]. Stigma is also a major barrier to accessing HIV services among foreign-born Latinos [18, 19]. In 2008, the Baltimore City Health Department (BCHD) established a Latino Outreach Program to provide culturally-sensitive, Spanish-language HIV education, testing, and linkage to care services for Latino migrants. Program evaluation has shown over 95 % of clients served by the Latino Outreach program are foreign-born Latinos and that HIV testing rates in this population have increased from 37 to 62 % in the 2 years since the program was established [20, 21]. While traditional community-based outreach has improved access to testing for Latinos in Baltimore, novel approaches should be evaluated to complement these services and further improve HIV testing rates.
Over the past decade, information and communication technology (ICT), such as text messaging and Internet, have been utilized to improve health care and education in various settings. For example, interventions using cell phones and text messaging have been used to increase HIV testing rates [22], enhance medication adherence among HIV-positive individuals [23–28] and access of minority youth to information about HIV/AIDS and referral to STD care [29, 30]. Text-messaging interventions have also been used to reduce high-risk sexual behaviors and methamphetamine use among men who have sex with men (MSM) [31] and instant messaging has been used to counsel MSM about HIV in real-time. [32] When patients have been surveyed on their attitudes toward use of cell phones, text messaging and Internet for HIV interventions, their response has been positive [33]. Cell phone-based interventions may therefore be an effective means to disseminate health information to Latinos. While there are disparities in technology use between native and foreign-born Latinos, the digital divide is smaller for cellular phones, with 72 % of foreign-born compared to 80 % of native-born Latinos utilizing a cell phone [34]. According to the Pew Internet and American Life project, African Americans and Latinos are more likely than Whites to use cell phones and mobile devices to access the Internet, use instant messaging, visit social networking sites, look up health information, and track or manage their health [35].
We conducted a cross-sectional survey study of Latinos living in Baltimore to evaluate the feasibility of using communication technology-based interventions to improve access to HIV testing and education within the Spanish-speaking community in Baltimore. We evaluated the relationship between age, gender, and education and ICT use. We also assessed migrant-associated factors, such as country of origin and time in the US, because differences in socioeconomic and educational attainment between migrants from different countries could impact utilization of ICT [34, 36]. Identifying factors associated with communication technology use and acceptability is important to understand who may be reached by using technology-based interventions and what population may be missed due to the lack of technology use, particularly among individuals who have never been tested for HIV.
Methods
This was a cross-sectional survey of 209 Baltimore Latinos conducted between June 2011 and January 2012.
Study Setting and Participants
The survey was conducted in selected street and community-based venues in Baltimore City. Several methods were used to identify venues frequented by Latinos living in Baltimore. We interviewed 10 key informants, including outreach workers from the BCHD Latino outreach program, bar owners, bar clients, staff at community based organizations, and social workers familiar with the Latino community in Baltimore. Interview guides were developed in collaboration with the BCHD Latino Outreach program and included questions about barriers to HIV testing among Latinos, appropriate incentives for participation, identification of local events for Latinos, and places with high Latino presence. Once a list of venues was generated, we observed locations at various time intervals to to evaluate whether the target population could be assessed in sufficient numbers at each site. Eligibility for participation included self-identification as Latino, age ≥18 years old, ability to communicate in Spanish or English, and ability to give oral consent.
The institutional review board of the Johns Hopkins University School of Medicine approved this study.
Measures
We developed a 21-item survey querying: (1) demographics including age, gender, race, sex, education, years in the US, primary language and country of origin, (2) frequency of technology use, including cellular phone, text messaging, email and Internet, and (3) interest in receiving health information, HIV education and HIV testing results by each of the three modalities.
Technology use was assessed using the following questions: (1) Do you use a cell phone? (2) If so, how often do you use it? (3) Is your cell phone a smartphone? (4) Do you use short message service (SMS)/text messaging with your cell phone? (5) If so, how often do you use it? (6) Do you use the Internet? (6) If so, how often do you use it? (7) Do you use e-mail? (8) If so, how often to you use it? Frequency of use was assessed as “daily,” “weekly,” “less than once per week,” or “never.”
Interest in receiving health information by each of the different technologies was assessed using the following questions: (1) Would you be interested in receiving health information by (text message/SMS, Internet or e-mail)? (2) Would you be interested in receiving education about HIV by (text message/SMS, Internet or e-mail)? (3) Would you be interested in receiving HIV test results by (text message/SMS, Internet or e-mail)? The items selected for inclusion in the questionnaire were chosen based on review of the literature, and consultation with focus groups and key informants.
Data Collection
We used a stratified sampling scheme based on gender and venue to reach a representative population. Data from previous surveys were reviewed to assess the representation of specific subgroups (by gender, age, and country of origin) in the local Latino population [37–39]. Formative research including focus groups and key informant interviews was used to determine venues and times frequented by Latinos in the Baltimore community. Once sampling venues were defined through our formative research, we used a random number generator to select venues and times for sampling on specific dates to reach a representative sample of Latinos in Baltimore. Stratified sampling was not performed in health fair settings due to lack of feasibility. Because certain venues were gender-biased (e.g. male predominance in locations where day laborers congregate and in bars), we monitored data for gender balance and if either gender was grossly overrepresented, a sampling venue frequented by the opposite gender was chosen. During each sampling period, interviewers selected every third unit (i.e. family, single person, couple) who walked by to screen for eligibility and recruit to participate in the survey. Oral informed consent was obtained and participants received a $5 gift card for their participation. Consent and surveys were administered in Spanish or English, depending on each participant’s preference. The maximum number of participants for each venue was capped at twenty people with an aim to survey five people per 2-h sampling period. Each survey took approximately 15 min to complete (range 10–30 min). Individuals who refused participation were asked their age and a tally was maintained recording age, gender, and survey site for individuals who did not participate.
Data Analysis
Study data was collected and managed using REDCap electronic data capture tools hosted at Johns Hopkins University School of Medicine [40]. Survey responses were reviewed to examine the frequency of distributions and identify outliers, non-normality, and other data irregularities. Descriptive characteristics (mean, median, range and SD) were used to summarize responses. We compared participant characteristics and technology use between individuals previously tested for HIV versus those never tested using Pearson’s Chi square test for categorical variables and Wilcoxon-Mann–Whitney test for continuous variables. We used multivariable logistic regression to identify factors associated with previous HIV test, communication technology use, and interest in receiving health information via text messaging. Statistical analysis was performed using Stata version 10.0 for windows (Stata-Corp, College Station, Texas, USA).
Results
Baseline Characteristics
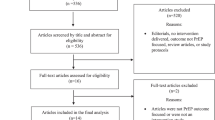
Over an 8 month period, we offered participation to 674 eligible individuals and interviewed 209 (response rate 31 %). There was no difference by age or gender between responders and non-responders. The majority (54.1 %) of surveys were done on the street, 27.8 % at health fairs, and 18.2 % at community-based organizations (Table 1). The median age of study participants was 33 years (IQR 28–42), 51.7 % were male, and the majority were foreign-born (95.7 %) and spoke Spanish (98.6 %) as their primary language. Educational level was relatively low, with 32.1 % of the sample completing less than 6th grade and only 23.9 % completing more than 12th grade. Countries of birth included Mexico (31.3 %), El Salvador (22.6 %), Honduras (14.9 %), Guatemala (13 %), US (4.3 %), and others (13.9 %). Approximately two-thirds (63.2 %) of participants had been in the US less than 10 years (median time in the US = 7 years, IQR 4–12).
ICT Use and Previous HIV Testing
The majority of our sample reported using cell phones (92.3 %) and text messaging (74.2 %). Internet use and e-mail were less common (52.2 and 42.8 %, respectively). The majority (91.5 %) of respondents had exclusive ownership of their cell phone, and 59.6 % owned a smartphone. Cell phone turnover was variable, with approximately half (53.1 %) of the cell phone numbers in use for less than 2 years. In univariate analysis, individuals who did not use Internet, e-mail or text messaging were less likely to have been tested previously for HIV. Women were twice as likely as men to have been previously tested for HIV and Guatemalans were the least likely to have had an HIV test in the past. Overall, the majority (70.1 %) had been previously tested for HIV. In multivariate analysis adjusting for demographic characteristics (gender, age, country of origin, and educational status), women were twice as likely to have been tested for HIV than men. Older individuals and those from Guatemala were less likely to report a previous HIV test.
Factors Associated with ICT Utilization and Acceptability for Dissemination of Health Information
In order to identify which Latino subgroups may not be reached effectively through communication technology interventions, we evaluated factors associated with its use. In multivariate analysis, older age and lower education were associated with less Internet, e-mail and text messaging utilization, but there was no association with cell phone use (Table 2). The only characteristic associated with cell phone use was gender, with less utilization among men.
We assessed three categories of acceptability for receiving health information of increasing sensitivity including health education, HIV education, and HIV test results by text messaging (Table 3). Acceptability was high for health education (73.1 %), HIV education (70.2 %), and even HIV test results (68.8 %). The common factor associated with interest in receiving health and HIV information or HIV test results via text messaging was exclusive cell phone ownership. Age and gender did not significantly impact the interest in receiving information via text message. Interest in receiving HIV education and test results was also associated with higher education. Compared to individuals who reported a previous HIV test, respondents who had never been tested for HIV were less interested in receiving general health education, but equally interested in receiving HIV information by text messaging. Respondents from El Salvador and Guatemala were less interested in receiving HIV test results by text messaging than individuals from Mexico.
Discussion
The rapid growth of Latino migrant populations in some regions of the US has increased the need for culturally-sensitive health interventions. Foreign-born Latinos are at high risk for late HIV diagnosis and worse HIV outcomes [9–11, 13]. Therefore, evaluating interest in new HIV interventions and promoting active community engagement is crucial to successfully reach vulnerable populations. In our study, respondents were as interested in receiving HIV education and HIV test results by text messaging as in receiving general health information. High interest in receiving HIV information via text messaging is consistent with findings from diverse resource-limited settings [24, 41].
Patient-centered issues such as privacy and literacy are important to consider prior to implementing ICT-based HIV interventions. The importance of privacy is evident in our study results, where exclusive cell phone ownership was strongly associated with interest in receiving health information via text messaging. Educational attainment was not associated with cell phone use, but did influence internet and e-mail utilization. Even though national data shows that foreign-born Latinos have lower ICT utilization than US-born Latinos [34], we did not find differences in ICT utilization by country of origin in our sample of primarily Spanish-speaking foreign-born Latinos. Country of origin was only associated with previous HIV testing (lower rates among Guatemalans) and lower interest in receiving HIV test results by text among individuals from Guatemala and El Salvador.
One factor that may explain the interest for text-based interventions is a relative shortage of culturally-appropriate health and HIV-related services for Latinos. US Latinos consider HIV/AIDS the second most concerning health issue in the US and are more likely than whites to be personally concerned about contracting HIV [42]. Baltimore Latinos also face significant structural barriers to accessing healthcare and are therefore more likely to seek care from public and community health initiatives. Approximately three-quarters of Baltimore Latinos do not have health insurance [43] compared to one-third of US Latinos, and 15 % of the general US population [44]. Cultural factors may also contribute to the interest in receiving HIV education by text messaging. For example, receptivity to provider initiated health information may be influenced by the cultural belief in medical authority [45].
An important consideration in developing technology-based interventions is ensuring that the technology is accessible to the target population. The lack of association between cell phone utilization and previous HIV testing is encouraging and suggests that text messaging can be used to reach individuals who have not been previously tested. We found that male gender was associated with lower cell phone utilization and a lower likelihood of previous HIV testing. Higher testing rates among women are consistent with both national [46] and local data [21], and may be partly related to testing during prenatal care. Even though cell phone utilization was more common among women than males, 82 % of males surveyed owned a personal cell phone, suggesting that cell phone ownership would not be a major barrier to receiving text messages with health information. It is also important to note that certain forms of ICT such as Internet use and text messaging appear to be less accessible to individuals of lower educational level, who may be the most vulnerable to inequities in health care access. Less education is associated with less HIV testing among Latinos in Baltimore City [20, 21] and nationwide [15], suggesting that less educated Baltimore City Latinos are the most vulnerable to being missed by developing an ICT intervention for HIV prevention. While cell phone use was common (85 %) among Latinos with less than 6th grade education, only 60 % were interested in receiving HIV education by text message. The lower utilization of text-based messaging among low education Latinos may be due to literacy levels, which was not measured in this study. However, an urban probability sampling study of foreign born Latinos living in Baltimore conducted in the same geographical location, showed >90 % basic Spanish literacy rates despite low educational attainment [38]. Our findings suggest that text messaging can be used to supplement, but not replace, other outreach activities.
Several limitations of this study should be considered. The cross-sectional design limits the ability to make causal associations. To minimize sampling bias, we used a stratified sampling scheme at venues identified during formative research. Only 31 % of individuals approached agreed to participate in the survey, but there was no difference in gender or age distribution among responders and non-responders. We did not collect data assessing the cause for non-participation, but potential factors could include lack of familiarity with research studies, mistrust of scientific investigations, time-constraints, or concerns regarding confidentiality [47, 48]. We attempted to enhance participant trust by ensuring that all study interviewers/recruiters were members of the community fluent in Spanish. It is also possible that hidden populations at particularly high risk for HIV, such as men who have sex with men or intravenous drug users, may not be represented in this sample. We found that low educational attainment was associated with less Internet, e-mail and text messaging utilization, but we did not enquire about literacy level, which would have provided an additional dimension to understanding the feasibility of text-based interventions. In addition, our ability to distinguish differences between US-born and foreign-born Latinos was limited because of the low numbers of US-born Latinos in our sample. While the study was conducted in a predominantly foreign-born Latino community in Baltimore City and results may not be generalizable to other Latino populations in the US, our findings may be particularly relevant to outreach programs in areas experiencing a similar rapid growth of foreign-born Latinos from Central America and Mexico. Finally, we developed the questionnaire used to collect data because there was no previously validated measure to assess ICT use among Latinos. Evidence of the survey’s content validity was conferred through review in focus groups and by key informant feedback.
Past accomplishments in HIV prevention through ICT in other populations have the potential to be used in Baltimore with culturally appropriate adaptations. San Francisco’s Department of Public Health developed a text message STI/HIV information and referral service and successfully reached low income adolescents in a relevant format [30]. A South African text message randomized controlled trial to encourage the uptake of HIV counseling and testing was able to determine the content, frequency and cost that led to motivating patients to get tested [22]. Previous work in Baltimore City showed that gaps in basic HIV knowledge, such as modes of HIV transmission and knowing that a person with HIV can look healthy, correlated with previous HIV testing patterns. Simple text messages reinforcing these concepts and directing people to free testing sites could be one way to use ICT to enhance HIV awareness and promote testing among Latinos.
In summary, the use of ICT, particularly cell phones, has the potential to expand the reach of traditional HIV outreach activities for foreign-born Latinos in Baltimore [21]. Novel initiatives should actively engage the community to develop focused and catchy messages that empower Baltimore Latinos to get involved in HIV prevention and care. Evaluation of the efficacy of such interventions on HIV awareness and health seeking behavior will be essential to ultimately achieve improvements in timely testing for HIV among Latinos.
New Contribution to the Literature
The expansion of culturally-sensitive outreach programs for Latinos living in Baltimore has improved HIV testing rates in this population over the past few years. However, late presentation to HIV care is still common among Latinos and novel interventions to improve HIV education and access to testing are needed. Previous studies have shown high cell phone use among native and foreign-born Latinos living in the US [34] but to our knowledge, this is the first study evaluating the interest in using ICT to disseminate HIV information among a primarily foreign-born Latino population. We found that cell phone use is common among Latinos living in Baltimore, and interest in receiving health and HIV information by text messaging is high, even among individuals who have never been previously tested for HIV. These findings suggest that ICT interventions could be used to bolster traditional outreach efforts.
References
Ennis S, Rios-Vargas M, Albert N. The Hispanic population: 2010. In: 2010 census briefs. U.S. Census Bureau; 2011. Available at http://www.census.gov/prod/cen2010/briefs/c2010br-04.pdf. Accessed 19 February 2013.
Maryland State Data Center. Census 2010 Demographic Profiles. Available at http://census.maryland.gov/census2010/databyrace.shtml. Accessed 19 February 2013.
Brodie M. National survey of Latinos: Summary of findings. Washington, DC: Pew Hispanic Center/Kaiser Family Foundation; 2002.
Kochhar R, Suro R, Tafoya S. The New Latino South: The context and consequences of rapid population growth. Washington, DC: Edited by Center PH; 2005.
Adih WK, Hu X, Campsmith ML, Espinoza L, Hall HI. Estimated lifetime risk for diagnosis of HIV infection among Hispanic/Latinos—37 States and Puerto Rico, 2007. Morb Mortal Wkly Rep. 2010;59(40):1297–301.
Office of Epidemiology and Planning BCHD. Baltimore City Health Department Status Report 2008. Maryland: Baltimore City; 2008.
Adih WK, Hu X, Campsmith ML, Espinoza L, Hall HI. Estimated lifetime risk for diagnosis of HIV infection among Hispanic/Latinos—37 States and Puerto Rico, 2007. MMWR. 2010;59(40):1297–301.
DC C. Late versus early testing of HIV—16 sites, United States, 2000–2003. MMWR. 2003;52:581–6.
Chen NE, Gallant JE, Page KR. A systematic review of HIV/AIDS survival and delayed diagnosis among HISPANICs in the United States. J Immigr Minor Health. 2012;14(1):65–81.
Dennis AM, Napravnik S, Sena AC, Eron JJ. Late entry to HIV care among Latinos compared with non-Latinos in a southeastern US cohort. Clin Infect Dis. 2011;53(5):480–7.
Espinoza L, Hall HI, Selik RM, Hu X. Characteristics of HIV infection among Hispanics, United States 2003–2006. J Acquir Immune Defic Syndr. 2008;49(1):94–101.
Girardi E, Sabin CA, Monforte AD. Late diagnosis of HIV infection: epidemiological features, consequences and strategies to encourage earlier testing. JAIDS. 2007;46:S3–8.
Wohl AR, Tejero J, Frye DM. Factors associated with late HIV testing for Latinos diagnosed with AIDS in Los Angeles. AIDS Care. 2009;21(9):1203–10.
del Rio C. Latinos and HIV care in the southeastern United States: new challenges complicating longstanding problems. Clin Infect Dis. 2011;53(5):488–9.
London AS, Driscoll AK. Correlates of HIV/AIDS knowledge among U.S.-born and foreign-born Hispanics in the United States. J Immigr Health. 1999;1(4):195–205.
Organista KC, Carrillo H, Ayala G. HIV prevention with Mexican migrants: review, critique, and recommendations. JAIDS. 2004;37:S227–39.
Shedlin MG, Decena CU, Oliver-Velez D. Initial acculturation and HIV risk among new Hispanic immigrants. J Natl Med Assoc. 2005;97(7 Suppl):32S–7S.
Dang B, Giordano T, Kim J. Sociocultural and structural barriers to care among undocumented Latino immigrants with HIV infection. J Immigr Minor Health. 2012;14(1):124–31.
Pollini RA, Blanco E, Crump C, Zúñiga ML. A community-based study of barriers to HIV care initiation. AIDS Patient Care STDs. 2011;25(10):601–9.
Chen N, Erbelding E, Yeh HC, Page K. Predictors of HIV testing among Latinos in Baltimore City. J Immigr Minor Health. 2010;12(6):867–74.
Chen NE, Meyer JP, Bollinger RC, Page KR. HIV testing behaviors among Latinos in Baltimore City. J Immigr Minor Health. 2012;14(4):540–51.
de Tolly K, Skinner D, Nembaware V, Benjamin P. Investigation into the use of short message services to expand uptake of human immunodeficiency virus testing, and whether content and dosage have impact. Telemed J E Health. 2012;18(1):18–23.
Hardy H, Kumar V, Doros G, Farmer E, Drainoni ML, Rybin D, Myung D, Jackson J, Backman E, Stanic A, et al. Randomized controlled trial of a personalized cellular phone reminder system to enhance adherence to antiretroviral therapy. AIDS Patient Care STDS. 2011;25(3):153–61.
Harris LT, Lehavot K, Huh D, Yard S, Andrasik MP, Dunbar PJ, Simoni JM. Two-way text messaging for health behavior change among human immunodeficiency virus-positive individuals. Telemed J E Health. 2010;16(10):1024–9.
Kalichman SC, Kalichman MO, Cherry C, Swetzes C, Amaral CM, White D, Jones M, Grebler T, Eaton L. Brief behavioral self-regulation counseling for HIV treatment adherence delivered by cell phone: an initial test of concept trial. AIDS Patient Care STDS. 2011;25(5):303–10.
Lester RT, Ritvo P, Mills EJ, Kariri A, Karanja S, Chung MH, Jack W, Habyarimana J, Sadatsafavi M, Najafzadeh M, et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial. Lancet. 2010;376(9755):1838–45.
Mbuagbaw L, Thabane L, Ongolo-Zogo P, Lester RT, Mills E, Volmink J, Yondo D, Essi MJ, Bonono-Momnougui RC, Mba R, et al. The Cameroon mobile phone SMS (CAMPS) trial: a protocol for a randomized controlled trial of mobile phone text messaging versus usual care for improving adherence to highly active anti-retroviral therapy. Trials. 2011;12:5.
Shet A, Arumugam K, Rodrigues R, Rajagopalan N, Shubha K, Raj T, D’Souza G, De Costa A. Designing a mobile phone-based intervention to promote adherence to antiretroviral therapy in South India. AIDS Behav. 2010;14(3):716–20.
Innovation profile. Texting service enhances minority youth access to HIV/AIDS information and testing. In: AHRQ health care innovations exchange. Rockville, MD: Agency for Healthcare Research and Quality Health Care Innovations Exchange. 2011. Available at http://www.innovations.ahrq.gov/content.aspx?id=3152. Accessed 19 February 2013.
Levine D, McCright J, Dobkin L, Woodruff AJ, Klausner JD. SEXINFO: a sexual health text messaging service for San Francisco youth. Am J Public Health. 2008;98(3):393–5.
Reback CJ, Ling D, Shoptaw S, Rohde J. Developing a Text messaging risk reduction intervention for methamphetamine-using MSM: research note. Open AIDS J. 2010;4:116–22.
Moskowitz DA, Melton D, Owczarzak J. PowerON: the use of instant message counseling and the Internet to facilitate HIV/STD education and prevention. Patient Educ Couns. 2009;77(1):20–6.
Curioso WH, Kurth AE. Access, use and perceptions regarding Internet, cell phones and PDAs as a means for health promotion for people living with HIV in Peru. BMC Med Inform Decis Mak. 2007;7:24.
Livingston G. The Latino digital divide: the native born versus the foreign born. Pew Hispanic Research Center. Available at http://www.pewhispanic.org/2010/07/28/the-latino-digital-divide-the-native-born-versus-the-foreign-born/. 2010.
Zickuhr K, Smith A. Pew Internet and American life project. Digital Differences. April 13, 2012. Found at http://pewinternet.org/~/media/Files/Reports/2012/PIP_Digital_differences_041312.pdf. Accessed 12–2012. 2012.
Motel S, Patten E. The 10 largest Hispanic origin groups: characteristics, rankings, top counties. Available at http://www.pewhispanic.org/2012/06/27/the-10-largest-hispanic-origin-groups-characteristics-rankings-top-counties/#i-overview. Pew Hispanic Center. 2012.
U.S. Census Bureau. Data for Baltimore City and U.S.: 2007 population estimates program. Data for Latinos: 2007. American Community Survey.
Fonseca-Becker F, Perez-Patron MJ, Munoz B, O’Leary M, Rosario E, West SK. Health competence as predictor of access to care among Latinos in Baltimore. J Immigr Minor Health. 2010;12(3):354–60.
Rawlings-Blake S, Barbot O. The health of Latinos in Baltimore City. Office of Epidemiology and Planning at the Baltimore City Health Department. 2011. Available at http://baltimorehealth.org/press/2011_10_20_Health_of_Latinos_Report_ENG.pdf. Accessed 11–2012. 2011.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81.
Mitchell KJ, Bull S, Kiwanuka J, Ybarra ML. Cell phone usage among adolescents in Uganda: acceptability for relaying health information. Health Educ Res. 2011;26(5):770–81.
HIV/AIDS Policy Fact Sheet. Latinos and HIV/AIDS. Washington, DC: Kaiser Family Foundation; 2006.
Martinez IL, Carter-Pokras O. Assessing health concerns and barriers in a heterogeneous Latino community. J Health Care Poor Underserved. 2006;17(4):899–909.
DeNavas-Walt C, Proctor BD, Smith JC. Income, poverty, and health insurance coverage in the United States: 2008. In: Bureau USC, editor. Current population reports, P60-236. Washington, DC: Bureau USC; 2009.
Wallace L, DeVoe J, Rogers E, Malagon-Rogers M, Fryer G. The medical dialogue: disentangling differences between Hispanic and non-Hispanic Whites. J Gen Intern Med. 2007;22(11):1538–43.
Duran D, Usman HR, Beltrami J, Alvarez M, Valleroy L, Lyles C. HIV counseling and testing among Hispanic adolescents and adults in the United States, Puerto Rico, and the U.S. Virgin Islands, 2005. Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. Centers for Disease Control; 2008.
Mann A, Hoke MM, Williams JC. Lessons learned: research with rural Mexican-American women. Nurs Outlook. 2005;53(3):141–6.
Yancey AK, Ortega AN, Kumanyika SK. Effective recruitment and retention of minority research participants. Annu Rev Public Health. 2006;27:1–28.
Author information
Authors and Affiliations
Corresponding author
Additional information
Lorena Leite and Megan Buresh contributed equally to this manuscript.
Rights and permissions
About this article
Cite this article
Leite, L., Buresh, M., Rios, N. et al. Cell Phone Utilization Among Foreign-Born Latinos: A Promising Tool for Dissemination of Health and HIV Information. J Immigrant Minority Health 16, 661–669 (2014). https://doi.org/10.1007/s10903-013-9792-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10903-013-9792-x