
Abstract
This article describes the stepwise development of the website ‘E-info geneca’. The website provides counselees in breast cancer genetic counseling with computer-tailored information and a question prompt prior to their first consultation. Counselees generally do not know what to expect from genetic counseling and they tend to have a passive role, receiving large amounts of relatively standard information. Using the “intervention mapping approach,” we developed E-info geneca aiming to enhance counselees’ realistic expectations and participation during genetic counseling. The information on this website is tailored to counselees’ individual situation (e.g., the counselee’s age and cancer history). The website covers the topics of the genetic counseling process, breast cancer risk, meaning of being a carrier of a cancer gene mutation, emotional consequences and hereditary breast cancer. Finally, a question prompt encourages counselees to prepare questions for their genetic counseling visit.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cancer genetic counseling primarily aims to increase counselees’ realistic risk perceptions and adherence to cancer screening recommendations (Biesecker 2001). Most of the consultations center around hereditary breast cancer (Pieterse et al. 2005a). Counselees who are the first in their family to request counseling, typically are poorly prepared, unsure about what to expect from genetic counseling and expect to be offered a DNA-test independent of their disease status and risk profile (Hallowell et al. 1997; Metcalfe et al. 2007; Pieterse et al. 2005a). In addition, the content of the initial cancer genetic counseling visit appears relatively standard with large amounts of information being conveyed to counselees (Pieterse et al. 2005c). Also, counselors appear to direct the communication more than counselees and they initiate most of the discussion topics. Moreover, counselees do not appear to communicate in a manner that reflects their pre-visit needs. Provision of information prior to genetic counseling might prevent unnecessary anxiety and worry about the process of genetic counseling and allows individuals to prepare themselves regarding the wider implications for themselves and their families (Metcalfe et al. 2007). Consequently, counselees may be helped to participate more actively by receiving more information about the counseling process prior to their first visit, and by being advised to prepare questions for their visit (Pieterse et al. 2005c).
In order to avoid supplying counselees with large amounts of general information, pre-visit information may need to be tailored to each counselee’s situation and needs. Pre-visit information should be adapted to the individual risk profile, because information provided in genetic counseling differs for counselees with high versus low risk of being a carrier of a BRCA mutation. Moreover, as information needs differ among counselees (Pieterse et al. 2005a), focusing on providing information specific to each counselee’s needs might enhance its perceived relevance and limit the amount of redundant content. Tailored information, which is intended to reach one specific person and is therefore based on individual characteristics related to the outcome of interest (Kreuter et al. 1999), is realized via an assessment of individual characteristics, a message source file that provides the messages, and a computer program that connects the individual assessment with the relevant messages (De Nooijer et al. 2002; Dijkstra and de Vries 1999). These programs consist mainly of logical (‘if-then’) statements (Kreuter et al. 2000) used to determine message selection. Pre-counseling information could thus be tailored by adapting the information to counselees’ individual characteristics (Dijkstra 2008; Hawkins et al. 2008).
Few studies have been published on computer-tailored information provision in genetic counseling (Albada et al. 2007) or patient care (Bental et al. 1999; Beranova and Sykes 2007; Lewis 1999; Revere and Dunbar 2001). However, in primary and secondary prevention substantial research has been done assessing tailored information interventions. Reviews of tailored interventions for smoking cessation and dietary behavior show that computer-tailored information is more likely to be read and remembered compared to non-tailored, generic materials (Brug et al. 1999; Kroeze et al. 2006; Strecher 1999; Walters et al. 2006). Computer-tailored information also is found to have a greater impact on people’s intentions and behavior than generic information (Kroeze et al. 2006; Strecher 1999; Walters et al. 2006). Additionally, the option for counselees to pose questions in advance to be dealt with during the consultation can easily be integrated into an informative intervention. Such a question prompt sheet consists of space for counselee’s questions and has proved to be feasible and effective for enhancing patient participation during consultations (Brown et al. 2001). Thus computer-tailored interventions show promise as one way to facilitate communication between health professionals and patients.
The present paper describes the program development of an internet intervention, called “E-info geneca.” The intervention provides tailored pre-visit information and a question prompt for counselees in breast cancer genetic counseling who are the first in their family to request counseling. Intervention studies often focus on the effects of an intervention without specifying the precise characteristics of the intervention and the postulated processes involved in producing the effects (Bartholomew et al. 2006). Also, the way in which theory guided the development of tailored interventions is frequently implicit (Albada et al. 2007). Consequently, it is difficult to faithfully replicate effective interventions and challenging to identify techniques contributing to effectiveness across interventions (Abraham and Michie 2008). Inspired and guided by the “intervention mapping approach” (Bartholomew et al. 2006), a comprehensive framework for intervention development in which all steps in the development process need to be explicated, we systematically developed our intervention. This paper describes this process.
Method
We used the intervention mapping approach to develop a tailored intervention for breast cancer genetic counseling. Intervention mapping is a framework for systematic health promotion program planning, implementation and evaluation, that incorporates theory and empirical evidence to identify determinants of behavior, develop intervention objectives, and select methods and strategies for an intervention (Bartholomew et al. 2006; Perez-Rodrigo et al. 2005; Van Oostrom et al. 2007). Table 1 outlines the intervention mapping steps. In this iterative process, which spanned 13 months, many steps overlapped, which is encouraged in the intervention mapping approach. In the first intervention mapping step, we extracted counselees’ needs within cancer genetic counseling from a previous study by our research group (Pieterse et al. 2005a). Second, based on these needs, we explicated the objectives for the intervention. Third, based on literature we selected theory-based methods and practical strategies to achieve the stated objectives. To elucidate, theory-based methods are general techniques or processes, derived from empirical evidence that describe the association between an intervention and modification of determinants, whereas practical strategies are techniques for the application of these theory-based methods. Fourth, the intervention development phase integrated substeps for designing tailored information: preparation, tailoring and integration (Dijkstra and De Vries 1999), and presentation and readability, web design and testing. Finally, in the fifth and sixth intervention mapping steps we anticipated implementing and evaluating the intervention in a Dutch clinical genetic centre. These six intervention mapping steps are described in detail in the next section.
Development Process
Needs Assessment (Step 1)
In a previous study a needs assessment was conducted among counselees who were the first in their family seeking cancer genetic counseling (n = 128, 63% breast cancer counselees) (Pieterse et al. 2005a, c). This assessment showed that many counselees fostered unrealistic expectations regarding the process of counseling, especially about the indication for DNA-testing (Pieterse et al. 2005a). Counselees had a variety of specific information needs (e.g., about cancer risks, benefits and limitations of testing) (Pieterse et al. 2005a). After the first consultation, about one-fifth had unfulfilled needs regarding emotional matters and explanations about their own cancer risk. Accurate knowledge and personal control had increased and anxiety and risk perceptions had decreased (Pieterse et al. 2005b). However, marked overestimation of cancer risks persisted. Furthermore, a better fulfillment of needs was related to higher perceived personal control and lower anxiety scores.
Analysis of the communication in the initial visits showed that the content of these visits was relatively standard; counselors did not adapt to counselees’ pre-visit informational needs (Pieterse et al. 2005c). Overall, counselees had a stronger psychosocial focus than counselors. Counselors initiated discussion of most of the topics during the visit. Counselors provided more psychosocial information to counselees who had a higher need for emotional support, but they did not enquire more about their concerns. The counselors also did not adapt the counseling according to patients’ expectations or anxiety (Lobb et al. 2002). Counselees asked few questions in the initial visit and did not often verbalize their needs (Pieterse et al. 2005c). Consequently, counselors experienced difficulties in attuning to counselees’ agendas (Smets et al. 2007). Whereas most patients prefer to be informed and only a portion want to participate in decision making (Butow and Lobb 2004), younger, higher educated women without a severe condition generally prefer an active role within consultations (Benbassat et al. 1998).
In conclusion, the results of these studies suggest that counselees have unrealistic a priori expectations and unfulfilled needs after the counseling. They seem to be insufficiently acquainted with genetic counseling to prepare themselves and to take a more active role (Pieterse et al. 2005c). To improve the outcome of breast cancer genetic counseling, counselees should be prepared and encouraged to formulate questions.
Define Specific Intervention Objectives (Step 2)
According to our needs assessment, as described above, the outcomes of cancer genetic counseling, greater perceived control and less anxiety, will improve through a better fulfillment of counselees’ needs during the first genetic counseling visit. Barriers for fulfillment of counselees’ needs include counselees’ unrealistic expectations and their lack of participation such that they do not ask for the information they need.
Program Objective
The overall aim of the intervention is to increase counselees’ realistic expectations of breast cancer genetic counseling as well as their participation within the consultation. These effects should subsequently fulfill the indirect goals: more realistic perception of breast cancer risk, increased perceived control, a decrease in cancer worry and anxiety and, finally, an increase in adherence to screening advice.
Target Group and Stakeholders
The target group for the intervention consists of counselees in breast cancer genetic counseling. The counselors of the Department of Medical Genetics of the University Medical Centre Utrecht are the main stakeholders. As recommended (CHIQ 1999), we included representatives from both of these groups on our expert panel. This panel consisted of eight actively participating representatives: three former counselees in breast cancer genetic counseling (of which two are members of the Dutch Breast Cancer (Patient) Association), two clinical geneticists, a genetic nurse, a psychologist and an interdisciplinary social scientist. This panel met three times and conducted one feedback round via email. The draft of E-info geneca was circulated within the expert group and alterations were suggested. The draft was then modified by the first author before being re-circulated. The web texts were discussed with counselors during departmental meetings. The department of Medical Genetics approved the final website.
Performance Objectives
In order to determine the effect goals or performance objectives that eventually lead to the program objectives, the factors influencing counselees’ expectations and participation should be considered. An intervention should focus on the most important and changeable factors (Koelen and Van den Ban 2002). Results of a study on communication training for counselors indicate little effect on counselee participation (Pieterse et al. 2006). Therefore, this project aims at the counselee (individual) and at the interaction between counselee and counselor (interpersonal level). Table 2 lists these performance objectives and determinants of counselee behavior.
To achieve the first goal (i.e., realistic counselee expectations) the most important determinant is knowledge, more specifically, knowledge of the process of genetic counseling, outcomes of counseling, and hereditary breast cancer. The topics on which a need for information exist are based on the earlier conducted counselees’ needs analysis Quote geneca (Pieterse et al. 2005a). A factor analysis of the results of this instrument yielded five main information needs: process of genetic counseling, determination and consequences of being a carrier of a mutation in a cancer gene, breast cancer risk, and emotional consequences. Each of these topics was specified by items on the Quote geneca. The expert panel formulated additional items; for instance, the counselee experts emphasized the need for information about societal consequences, such as insurance (see Table 3).
The second goal (i.e. increased counselee participation) can be achieved by intervening on an external determinant, namely giving a question prompt as a cue (Van der Meulen et al. 2008). Additionally, prompting of question asking by the counselor during the consultation can encourage the counselee to ask questions (Butow 2004). Also, the counselee attitude towards question asking is a relevant determinant. This attitude could be changed by providing information about the benefits of question asking for fulfillment of counselee needs and recall. The expert panel formulated information items for this topic “In consultation” (see Table 3). A determinant that influences participation in decision making is the counselee’s attitude towards this process. Therefore, the topic “In consultation” includes information about the importance of participation in decision making.
Select Suitable Theory-Based Methods and Practical Strategies (Step 3)
Methods to Enhance Realistic Expectations
In the Netherlands, counselees in genetic counseling usually receive only a brief leaflet prior to counseling, providing information about the possible reasons for referral, organization of the clinic, and what to expect of the visit in general terms. Providing more pre-visit information could increase realistic expectations (Metcalfe et al. 2007). Several studies have shown that providing more extensive pre-counseling information can increase knowledge on breast cancer and heredity (Green et al. 2004; Green et al. 2005; Skinner et al. 2002). Moreover, use of a pre-counseling CD-ROM changed the focus of the communication within the consultation from basic education toward personal risk and decision making (Green et al. 2005).
The effect of this pre-visit information can be optimized by tailoring. Tailoring information to the individual is likely to increase perceived personal relevance (Brug et al. 1996), enhance perceived interest (Brug et al. 1996; Skinner et al. 1994, 2002), and improve recall (Brug et al. 1996; Campbell et al. 1994). Theoretical background for tailoring by adaptation of information is provided by the Elaboration Likelihood Model (ELM; Petty and Cacioppo 1986), which describes how a message can change attitudes. According to this model, attitudes can be adopted by two routes: centrally, by thoughtful consideration and evaluation of the given information or peripherally, by simply using heuristics or peripheral cues such as attractiveness, expert source or number of arguments. These centrally established attitudes are more enduring, more stable against contra argumentation, and they are better predictors of behavior. Therefore, health education should aim at central elaboration of information. The extent to which people are inclined to elaborate centrally is determined by their ability and motivation. A person’s ability is determined by factors such as message comprehensibility, time pressure or distraction. This motivation is mainly influenced by two factors: personal involvement with the attitude object and a more dispositional need for cognition (Drossaert et al. 1996; Petty and Cacioppo 1986). The ELM states that making the message more personally relevant by tailoring, stimulates motivation for thoughtful consideration, which leads to more stable attitudes (Bartholomew et al. 2006) and is supported by EEG research showing that tailored information increases attention rates (Ruiter et al. 2006).
Methods to Enhance Participation
Counselees can be stimulated to pose questions by use of a question prompt sheet (QPS). A recent review (Dimoska et al. 2008) shows that the use of a QPS in cancer consultations increased the amount of patient questions in a majority of studies. Moreover, a QPS empowered patients to ask questions about specific subjects, shifting the focus of the consultation. Another review additionally establishes limited evidence for a positive effect of a QPS on cancer patients’ recall of medical information provided that this sheet is actively endorsed by the physician (Van der Meulen et al. 2008). Generally, patients consider a QPS to be useful. However, effects on anxiety (an indirect goal in our program) were mixed (Dimoska et al. 2008; Van der Meulen et al. 2008). Overall, a QPS seems to be a useful tool to enhance patient participation and a feasible addition to the oncology consultation. Since up to half of the cancer genetic counselees in our clinic is affected by cancer (Pieterse 2005b) with many similar issues involved, the QPS is a promising tool in cancer genetic counseling. In a typical QPS, patients are confronted with a list of frequently asked questions and an option to formulate their own questions. However, to further individualize the counseling, we believe that no frequently asked questions should be supplied. The prompt in our intervention therefore consists of a request to counselees to formulate their own questions before the first genetic counseling visit.
During cancer genetic counseling visits several decisions have to be made (e.g., concerning involvement of affected relatives to ask for their medical data or their acceptance of a DNA-test, the decision to undergo genetic testing, to inform family members about test results, to start periodic surveillance or to opt for prophylactic surgery). Cancer patients who achieve their preferred role are most satisfied with their consultation, whereas patients who are less active than desired are least satisfied (Gattellari et al. 2001). Studies in oncology show that the use of a QPS without physician endorsement reduces the percentage of patients whose preferred involvement in decision making was achieved (Butow et al. 2004). Therefore counselors need to be prepared for how to use a QPS in order to adjust their counseling style to counselees’ increased participation and decision making involvement.
Counselee participation is considered to increase fulfillment of their needs. Results from previous research indicate that counselees have unfulfilled needs regarding emotional matters and personal risk estimation (Pieterse et al. 2005b). Other studies show that counselors provide detailed information on various topics related to cancer, but they neither consistently elicit emotional concerns (Butow and Lobb 2004) nor adapt their counseling to patients’ expectations or anxiety (Lobb et al. 2002). Thus, counselee question asking is needed to tailor the consultation to individual needs.
And finally, based on the ELM, we expect that an increase in counselee participation enhances central information processing and thus stable attitudes. The most effortful form of information processing occurs when attitude change results from the self-generation of arguments, instead of passive exposure (Petty and Cacioppo 1986). When an attitude is formed via direct personal experience it is automatically based on self-generated information. Counselee participation within the consultation implies increased counselee speech time, question asking and information giving. Consequently, there will likely be more self-generation of arguments. Therefore, we expect more accurate knowledge and risk perception as a result of E-info geneca. Furthermore, we expect a decrease in cancer worry and anxiety, and an increase in perceived control.
Strategy
The information and question prompt needs to be provided before the first consultation. To make the intervention most self paced and private, the intervention should be delivered at counselees’ homes. The most practical way to provide counselees with computer-tailored information with a question prompt is through the internet, because the tailored information does not need to be printed and the question prompt can easily be saved for the counselor. In 2007, 83% of Dutch inhabitants had internet access at home (Statistics Netherlands 2007). There are, however, huge differences in internet access and computer abilities (Huysmans et al. 2004; Korvorst and Linden 2008). In comparison to the general adult population, elderly, lower educated people and people without study or paid work are less likely to have internet access, they make less use of the internet, and they have poorer computer abilities. Since Dutch breast cancer genetic counseling counselees are generally young and higher educated (Van Asperen et al. 2002), we considered it feasible to opt for an internet-based intervention.
Intervention Development (Step 4)
We gathered patient and counselee information texts on the topics listed in Table 3. The texts are drawn from available brochures, standard counselee letters and web texts (Dutch Cancer Society 2005; University Medical Centre Utrecht 2002) for which we gained permission to use. When necessary, these texts were adjusted to the local breast cancer genetic counseling setting.
Preparation of Tailoring
In the first substep of the intervention development we developed a list of potentially relevant tailoring variables. This list is based on a review of tailored information about cancer risk and screening (Albada et al. 2007) in which we disentangled the tailoring variables of the studied interventions. Most evidence supporting effects of tailored health information is based on studies evaluating behavioral construct tailoring, which relies on variables specified in leading theories of health behavior change (Kreuter and Haughton 2006). The review established limited evidence for tailoring cancer risk information on these behavioral constructs and/or on risk factors (Albada et al. 2007). Next to behavioral constructs, demographic and medical variables and variables related to information processing were detected as possibly relevant variables for adapting information to the individual. One article retrieved in the review evaluated tailored education material for breast cancer genetic counseling. This information was tailored on sociodemographic characteristics, risk factors and information preferences and was effective in increasing knowledge about breast cancer and heredity and in enhancing accuracy of perceived risk of being a mutation carrier (Skinner et al. 2002). The tailoring variables for which indications of evidence were found include, behavioral variables, risk factors, medical history and information needs. These variables were proposed to the expert panel to apply in E-info geneca.
Deciding on Tailoring Variables
In the second substep of the intervention development the expert panel decided on relevant tailoring variables and appropriate adaptation of messages to each tailoring variable. Information in E-info geneca was adapted to the variables stated in Table 4. This substep resulted in a tailoring matrix for each intervention subject, presenting the number of tailored texts per subject (see Table 5 for an example). The information content was adapted to the value of the tailoring variables in the pre-visit individual assessment. The information on the website is tailored to counselees’ individual situation (e.g., counselee’s age, cancer history and probability of being a mutation carrier). For example, affected high risk counselees received information about the procedure of a DNA-test, stating that a DNA-test could be conducted on their DNA. Unaffected high risk counselees were told that a DNA-test could be performed on DNA of an affected family member. Additionally, information was adapted to the preferred extensiveness of information, defining whether the counselee receives extensive or concise information. This tailoring variable was based on the finding of Cassileth et al. (1980) that patients differ in their preferred amounts of information, and it is similar to the tailoring on information preference used by Skinner et al. (2002). The concise versions of the texts were created by omission of elaborations, elucidations and details. For example, the concise version of the text about privacy explained that the counselee’s information is documented in a medical file and that the counselee can request a copy. The extensive version of the text additionally specified the law in which these rights are stated. Consequently, the concise versions of the texts are shorter than the extensive versions, due to a lower average number of sentences and a somewhat lower average number of words per sentence.
Presentation and Readability
In the third substep of the intervention development the information was edited in accordance with guidelines for web information (CHIQ 1997). E-info geneca has a clear and simple text structure, which comprises representative headings and positioning of the main message at the beginning of the text and in every first paragraph sentence (Heij and Visser 2006). Because information materials for breast cancer patients are often too difficult for patients to understand (Beaver and Luker 1997), we have put specific effort in reaching an acceptable reading ease. The text was adjusted to the readability level of 4th grade high school, similar to reading ease (R.E.) score 60–70 on the Flesh scale. Text on this level is easy to understand without being irritating. It consists of short sentences (on average 10 words) and common, everyday words (Plain English Campaign 2001a). We used the Flesh readability formula adjusted for the Dutch language by Douma, which produced an R.E.-score of 58.4. E-info geneca has on average 10.7 words per sentence and 5.5 signs per word. Only 5% of the sentences are passively phrased. We eliminated wordiness and figurative talk.
The text was adjusted for the web by creating subheadings, short paragraphs and enumerations using bullets. Additionally, tooltips provided explanation for jargon. We added information on purpose, contact and ownership of the site, which can be contacted from every page (Plain English Campaign 2001b). The website contains pictures of the hospital department entrance, a consultation room, chromosomes and a rotating DNA helix. Additionally, one web page presents the names and photographs of the counselors.
All risks communicated within E-info geneca combined visual, numerical and verbal representations, because people appear to prefer a combination of approaches and they better understand risks when a combination is used (Lipkus and Hollands 1999; Paling 2003). This combination of risk representations is similar to that in a leaflet about risk of hereditary predisposition for breast cancer which increased correct risk perception and knowledge in unaffected counselees for breast cancer genetic counseling (Lobb et al. 2006). Diagrams for prevalence and heredity of breast and ovarian cancer were used similar to those in a decision aid that was effective in increasing counselees’ knowledge levels (Wakefield et al. 2008, 2007).
Finally, the texts of E-info geneca were checked with the EQIP (Ensuring Quality Information for Patients) instrument for assessing quality of written patient information (Moult et al. 2004). This instrument consists of quality items concerning clarity, readability, completeness of information. The E-info geneca texts scored satisfactorily on all applicable items.
Integration
In the fourth substep of intervention development we integrated all of the separately written messages in one coherent website. Possible subsequent texts should fit. Using fake-records (data from non-existing individuals) we tested the output of the system. Lastly, the question prompt was added, which can be accessed upon closing E-info geneca.
Web Design
The fifth substep in the intervention development consisted of web design. We used a web page layout and navigation similar to that of the University Medical Centre Utrecht, to enhance the design’s perceived credibility.
E-info geneca has a menu bar containing links to the homepage and the 5 main topics: hereditary breast cancer, genetic counseling, being a carrier, breast cancer risk, and emotional consequences. The order in which these topics are presented varies randomly across counselees. Additionally there is a main topic “In consultation,” that offers advice on how best to communicate with the genetic counselor. For example, it states the advice to express concerns, to notify the counselor when one does not understand the information given and to bring a spouse or family member to the consultation. Each of the main topics leads to several web pages (see Table 3 for this layered structure). For example, when clicking on the main topic “Hereditary breast cancer” in the menu, one accesses a web page about the prevalence of hereditary breast cancer in the Netherlands. In the left menu of this web page there are two links “How does cancer inherit in a family?” and “What are genes?” each leading to a webpage about that subject. The website consists of 19 web pages.
Counselees’ page views will be logged. Log files will contain the sequence of the web pages requested by each counselee and the date, time and duration of these requests. The questions posed on the question prompt will be saved in a questionnaire program. Respondents can visit E-info geneca only once, unless they receive a reminder including their personal link, which is sent in case of an incomplete evaluation form about E-info geneca.
Test Phase
In the sixth substep of the intervention development, E-info geneca was tested by counselees in breast cancer genetic counseling to ensure accessibility and understandability. These counselees were representative of the study population, in terms of being the first in their family to request genetic counseling. However, they were consulted after their final consultation instead of before their first consultation, because we wanted the opinion of experienced counselees. During their final consultation at the department of Medical Genetics of the University Medical Centre Utrecht the counselor approached them to evaluate E-info geneca. Consequently, they could not use the question prompt. We asked them to complete the pre-tailoring questionnaire, access E-info geneca through the link provided and complete the evaluation form. When this evaluation form was incomplete we sent an email reminder.
Thirteen respondents participated in this test phase. Their mean age was 43 years (SD = 11, Range, 22–61). Five were affected with breast cancer and one was affected with ovarian cancer. Nine respondents had one or more children. Eight respondents were referred by their GP; the other five were referred by a hospital physician. Six respondents indicated that the initiative for genetic counseling was both their own and their physician’s together. Three respondents indicated it was solely their own initiative. Two respondents said it was their family’s initiative, and another two indicated that it was their physician’s initiative. Seven respondents had searched the internet for other websites on cancer and heredity.
After completing the pre-tailoring questionnaire all 13 respondents visited E-info geneca. Eight visited only the homepage. The remaining five respondents viewed on average 10.2 web pages. Thus, when E-info geneca was visited beyond the homepage, more than half of all 19 web pages were viewed.
Seven respondents completed the evaluation form. Most of these respondents evaluated the website as clear and well arranged (6), easy to use and to search (7). Two respondents thought the website responded slowly. All respondents found the information useful, easy to understand, helpful for themselves and for family and friends, reliable, of present interest and of personal relevance. All but one of the respondents considered the information reassuring. One respondent considered the information disturbing, and two considered it confusing. Two respondents thought they were provided with too much information; however, both indicated a preference for extensive information in the pre-tailoring questionnaire. None of the respondents had missed particular information on the website. All respondents thought that future counselees would better know what to expect from genetic counseling after visiting E-info geneca.
To clarify respondents’ reasons for only visiting the homepage, we conducted three additional telephone interviews. Counselees appeared to have missed the menu, had not read the instructions on the homepage, or had left the homepage unintentionally.
Alterations After the Test Phase
Following up on the results of the test phase, we made the menu more attractive and improved the readability of the website instructions at the homepage. Also, we deleted the link to the evaluation form from the homepage. This link remained on all other pages and was enlarged to a button. Also, we added a possibility to return to E-info geneca after pushing this button. Furthermore, we improved the web design, the jargon explanations, and we made small alterations in the texts for clarification.
Implementation and Evaluation Plan (Step 5 and 6)
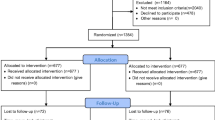
E-info geneca will be evaluated in a Randomized Controlled Trial (RCT) registered in the Dutch Trial Register (ISRCTN82643064). Two-hundred consecutive breast cancer counselees at the Department of Medical Genetics of the University Medical Centre Utrecht will receive a personal login by mail and email before their first genetic counseling consultation. After completing the individual assessment, half of them will receive a link to the website E-info geneca, which is constructed using the tailoring variables from the assessment. After closing the website these counselees will complete the QPS and evaluate the intervention by logging on to an evaluation form. The counselor will receive the posed questions at least one-half of an hour before the start of the consultation. Consultations will be videotaped, and both the counselee and the counselor will be asked to complete a questionnaire after each consultation. The effects of E-info geneca on expectations of genetic counseling, counselee participation, fulfillment of information needs and on post-counseling cancer worry, anxiety, risk perception, perceived control and adherence to screening advice will be studied.
Discussion
E-info geneca is intended to be complementary to genetic counseling sessions and cannot substitute for genetic counseling consultations. E-info geneca is developed for breast cancer specifically, but can be adapted to other types of hereditary cancer. With access to E-info geneca prior to the counseling we aim to make the first consultation more interactive. The intervention therefore could make the content of the consultation more focused on the situation of the individual counselee. Counselors may notice that counselees are better informed about genetic counseling and pose more questions through their preparation with E-info geneca. This will require a more flexible counseling style and will limit the need for provision of relatively standard information.
The objectives of the website E-info geneca are also relevant in other countries that offer breast cancer genetic counseling (e.g., USA, UK, Australia). The problem of poorly prepared counselees that expect to be offered a DNA-test independent of their risk profile has also been reported for the UK (Hallowell et al. 1997; Metcalfe et al. 2007). For the Australian situation it was reported that counselors did not adapt their counseling according to counselees’ expectations or anxiety (Lobb et al. 2002), resulting in relatively standard consultations in which counselors provided detailed information, but inconsistently elicited emotional concerns or facilitated communication (Butow and Lobb 2004). Similarly, Ellington et al. (2005) described the initial counseling sessions in a USA setting as predominantly educational in nature with minimal dialogue devoted to psychosocial issues. The rationale of E-info geneca could therefore also be applied in other countries. Although E-info geneca is written in Dutch, the website content would be similar for other countries. Therefore, the process of the website development could be replicated to produce an equivalent in English, addressing specifics in the genetic counseling process of a given country.
This program development study has some limitations. First, the test sample reflected the RCT study population, except for the fact that test respondents already had had their first consultation at the Department of Medical Genetics. Since E-info geneca is developed to provide counselees with pre-visit information about breast cancer genetic counseling, this information may seem inappropriately timed. This test design was chosen because we wanted the opinion of experienced counselees on whether they considered this information useful and correct.
Second, whereas we strived for readability at fourth grade level, E-info geneca actually appeared a bit more difficult to read. Due to certain long words which we frequently needed to use, such as genetic counseling and mammography, it was difficult to obtain the desired reading ease. However, based on the test outcomes, we expect that the information is understandable through the provided jargon explanations.
Third, in the test phase we were surprised by the number of respondents who visited only the homepage. The lack of clarity in the website navigation causing this respondent behavior could have been tackled with usability testing. Therefore, we recommend conducting usability tests in an early phase of future website development.
Conclusion
An intervention development process was prompted by the finding that counselees foster unrealistic expectations of breast cancer genetic counseling. Within intervention development a systematic procedure is necessary to include theory and experts’ advice as well as practical experiences with intervention modes. The intervention mapping approach structured these tasks and supported description of each step in the development process. The development process resulted in the website E-info geneca that provides computer-tailored information about breast cancer genetic counseling.
All information in E-info geneca is designed to be appropriate for the individual counselee. Based on the Elaboration Likelihood Model, which proposes that information perceived as personally relevant stimulates greater cognitive activity, we expect an increase in realistic expectations of genetic counseling after counselees consult E-info geneca. As an effect of the question prompt we expect an increase in counselee participation within the genetic counseling consultation. The effects of E-info geneca on counselees’ expectations, participation, and fulfillment of their information needs and its effects on their post-counseling cancer worry, anxiety, risk perception, perceived control and screening adherence are currently being assessed in an RCT.
References
Albada, A., Van Dulmen, S., Ausems, M. G. E. M., & Bensing, J. M. (2007, October). Tailored interventions in cancer risk communication. Abstract Book International Conference on Communication in Healthcare. Charleston, SC. USA.
Abraham, C., & Michie, S. (2008). A taxonomy of behavior change techniques used in interventions. Health Psychology, 27, 379–387. doi:https://doi.org/10.1037/0278-6133.27.3.379.
Bartholomew, L. K., Parcel, G. S., Kok, G., & Gottlieb, N. H. (2006). Planning health promotion programs, an intervention mapping approach. San Francisco: Wiley.
Beaver, K., & Luker, K. (1997). Readability of patient information booklets for women with breast cancer. Patient Education and Counseling, 31, 95–102. doi:https://doi.org/10.1016/S0738-3991(96)00988-3.
Benbassat, J., Pilpel, D., & Tidhar, M. (1998). Patients’ preferences for participation in clinical decision making: a review of published surveys. Behavioral Medicine, 24, 81–88.
Bental, S. B., Cawsey, A., & Jones, R. (1999). Patient information systems that tailor to the individual. Patient Education and Counseling, 36, 171–180. doi:https://doi.org/10.1016/S0738-3991(98)00133-5.
Beranova, E., & Sykes, C. (2007). A systematic review of computer-based softwares for educating patients with coronary heart disease. Patient Education and Counseling, 66, 21–28. doi:https://doi.org/10.1016/j.pec.2006.09.006.
Biesecker, B. B. (2001). Goals of genetic counseling. Clinical Genetics, 60, 323–330. doi:https://doi.org/10.1034/j.1399-0004.2001.600501.x.
Brown, R. F., Butow, P. N., Dunn, S. M., & Tattersall, M. H. N. (2001). Promoting patient participation and shortening cancer consultations: a randomised trial. British Journal of Cancer, 85, 1273–1279. doi:https://doi.org/10.1054/bjoc.2001.2073.
Brug, J., Steenhuis, I., Van Assema, P., & De Vries, H. (1996). The impact of a computer-tailored nutrition intervention. Preventive Medicine, 25, 236–242. doi:https://doi.org/10.1006/pmed.1996.0052.
Brug, J., Campbell, M., & Van Assema, P. (1999). The application and impact of computer-generated personalized nutrition education: a review of the literature. Patient Education and Counseling, 36, 145–156. doi:https://doi.org/10.1016/S0738-3991(98)00131-1.
Butow, P., & Lobb, E. (2004). Analyzing the process and content of genetic counseling in familial breast cancer consultations. Journal of Genetic Counseling, 13, 403–424. doi:https://doi.org/10.1023/B:JOGC.0000044201.73103.4f.
Butow, P., Devine, R., Boyer, M., Pendlebury, S., Jackson, M., & Tattersall, M. H. (2004). Cancer consultation preparation package: changing patients but not physicians is not enough. Journal of Clinical Oncology, 22, 4401–4409. doi:https://doi.org/10.1200/JCO.2004.66.155.
Campbell, M. K., DeVellis, B. M., Strecher, V. J., Ammerman, A. S., DeVellis, R. F., & Sandler, R. S. (1994). Improving dietary behavior: the effectiveness of tailored messages in primary care settings. American Journal of Public Health, 84, 783–787. doi:https://doi.org/10.2105/AJPH.84.5.783.
Cassileth, B. R., Zupkis, R. V., Sutton-Smith, K., & March, V. (1980). Information and participation preferences among cancer patients. Annals of Internal Medicine, 92, 832–836.
CHIQ. (1997). Readability and quality tools. https://doi.org/www.hfht.org/chiq/publications. Centre for Health Information Quality.
CHIQ. (1999). Involving consumers in the development and evaluation of health information. https://doi.org/www.hfht.org/chiq/publications. Centre for Health Information Quality.
De Nooijer, J., Lechner, L., & De Vries, H. (2002). Tailored versus general information on early detection of cancer: A comparison of the reactions of Dutch adults and the impact on attitudes and behaviours. Health Education Research, 17, 239–252. doi:https://doi.org/10.1093/her/17.2.239.
Dijkstra, A. (2008). The psychology of tailoring. Ingredients in computer-tailored persuasion. Social and personality psychology compass, 2, 765–784.
Dijkstra, A., & De Vries, H. (1999). The development of computer-generated tailored interventions. Patient Education and Counseling, 36, 193–203. doi:https://doi.org/10.1016/S0738-3991(98)00135-9.
Dimoska, A., Tattersall, M. H. N., Butow, P. N., Shepherd, H., & Kinnersley, P. (2008). Can a “Prompt List” empower cancer patients to ask relevant questions? Cancer, 113, 225–237. doi:https://doi.org/10.1002/cncr.23543.
Drossaert, C. H., Boer, H., & Seydel, E. R. (1996). Health education to improve repeat participation in the Dutch breast cancer screening programme: Evaluation of a leaflet tailored to previous participants. Patient Education and Counseling, 28, 121–131. doi:https://doi.org/10.1016/0738-3991(96)00889-0.
Dutch Cancer Society. (2005). Erfelijke borst- en eierstokkanker (Hereditary breast and ovarian cancer). Amsterdam: Dutch Cancer Society.
Ellington, L., Roter, D., Dudley, W. N., Baty, B. J., Upchurch, R., Larson, S., et al. (2005). Communication analysis of BRCA1 genetic counseling. Journal of Genetic Counseling, 14, 377–386. doi:https://doi.org/10.1007/s10897-005-3660-3.
Gattellari, M., Butow, P. N., & Tattersall, M. H. (2001). Sharing decisions in cancer care. Social Science & Medicine, 52, 1865–1878. doi:https://doi.org/10.1016/S0277-9536(00)00303-8.
Green, M. J., Peterson, S. K., Baker, M. W., Harper, G. R., Friedman, L. C., Rubinstein, W. S., et al. (2004). Effect of a computer-based decision aid on knowledge, perceptions, and intentions about genetic testing for breast cancer susceptibility: a randomized controlled trial. Journal of the American Medical Association, 292, 442–452. doi:https://doi.org/10.1001/jama.292.4.442.
Green, M. J., Peterson, S. K., Baker, M. W., Friedman, L. C., Harper, G. R., Rubinstein, W. S., et al. (2005). Use of an educational computer program before genetic counseling for breast cancer susceptibility: effects on duration and content of counseling sessions. Genetics in Medicine, 7, 221–229. doi:https://doi.org/10.1097/01.GIM.0000159905.13125.86.
Hallowell, N., Murton, F., Statham, H., Green, J. M., & Richards, M. P. M. (1997). Women's need for information before attending genetic counselling for familial breast or ovarian cancer: a questionnaire, interview, and observational study. BMJ (Clinical Research Ed.), 314, 281–283.
Hawkins, R. P., Kreuter, M., Resnicow, K., Fishbein, M., & Dijkstra, A. (2008). Understanding tailoring in communication about health. Health Education Research, 23, 454–466. doi:https://doi.org/10.1093/her/cyn004.
Heij, K., & Visser, W. (2006). Schrijven in eenvoudig Nederlands (Writing in plain Dutch). Den Haag: Sdu uitgevers.
Huysmans, F., De Haan, J., & Van den Broek, A. (2004). Achter de schermen, Een kwart eeuw lezen, luisteren, kijken en internetten (Half a century of reading, listening, watching and using the internet). Den Haag: Sociaal en Cultureel Planbureau.
Koelen, M. A., & Van den Ban, A. W. (2002). Health education and health promotion. Wageningen: Wageningen Academic Publishers.
Korvorst, M., & Linden, G. (2008). Vaardigheid Nederlandse internetter middelmatig (Dutch internet users have medium internet abilities). CBS StatLine.
Kreuter, M. W., & Haughton, L. T. (2006). Integrating culture into health information for African American Women. The American Behavioral Scientist, 49, 794–811. doi:https://doi.org/10.1177/0002764205283801.
Kreuter, M. W., Strecher, V. J., & Glassman, B. (1999). One size does not fit all: the case for tailoring print materials. Annals of Behavioral Medicine, 21, 276–283. doi:https://doi.org/10.1007/BF02895958.
Kreuter, M., Farrel, D. W., & Olevitch, L. (2000). Tailoring health messages, customizing communication with computer technology. NY: Lawrence Erlbaum Associates.
Kroeze, W., Werkman, A., & Brug, J. (2006). A systematic review of randomized trials on the effectiveness of computer-tailored education on physical activity and dietary behaviors. Annals of Behavioral Medicine, 31, 205–223. doi:https://doi.org/10.1207/s15324796abm3103_2.
Lewis, D. (1999). Computer-based approaches to patient education: a review of the literature. Journal of the American Medical Informatics Association, 6, 272–282.
Lipkus, I. M., & Hollands, J. G. (1999). The visual communication of risk. Journal of the National Cancer Institute. Monographs, 149–163.
Lobb, E. A., Butow, P. N., Meiser, B., Barratt, A., Gaff, C., Young, M. A., et al. (2002). Tailoring communication in consultations with women from high risk breast cancer families. British Journal of Cancer, 87, 502–508. doi:https://doi.org/10.1038/sj.bjc.6600484.
Lobb, E. A., Butow, P. N., Moore, A., Barratt, A., Tucker, K., Gaff, C., et al. (2006). Development of a communication aid to facilitate risk communication in consultations with unaffected women from high risk breast cancer families: a pilot study. Journal of Genetic Counseling, 15, 393–405. doi:https://doi.org/10.1007/s10897-006-9023-x.
Metcalfe, A., Werrett, J., Burgess, L., & Clifford, C. (2007). Psychosocial impact of the lack of information given at referral about familial risk for cancer. Psycho-Oncology, 16, 458–465. doi:https://doi.org/10.1002/pon.1081.
Moult, B., Franck, L. S., & Brady, H. (2004). Ensuring quality information for patients: development and preliminary validation of a new instrument to improve the quality of written health care information. Health Expectations, 7, 165–175. doi:https://doi.org/10.1111/j.1369-7625.2004.00273.x.
Paling, J. (2003). Strategies to help patients understand risks. BMJ (Clinical Research Ed.), 327, 745–748. doi:https://doi.org/10.1136/bmj.327.7417.745.
Perez-Rodrigo, C., Wind, M., Hildonen, C., Bjelland, M., Aranceta, J., Klepp, K. I., et al. (2005). The pro children intervention: applying the intervention mapping protocol to develop a school-based fruit and vegetable promotion programme. Annals of Nutrition & Metabolism, 49, 267–277. doi:https://doi.org/10.1159/000087249.
Petty, R., & Cacioppo, J. (1986). The elaboration likelihood model of persuasion. Advances in Experimental Social Psychology, 19, 123–205. doi:https://doi.org/10.1016/S0065-2601(08)60214-2.
Pieterse, A., Van Dulmen, S., Ausems, M., Schoemaker, A., Beemer, F., & Bensing, J. (2005a). QUOTE-geneca: development of a counselee-centered instrument to measure needs and preferences in genetic counseling for hereditary cancer. Psycho-Oncology, 14, 361–375. doi:https://doi.org/10.1002/pon.853.
Pieterse, A. H., Ausems, M. G. E. M., Van Dulmen, A. M., Beemer, F. A., & Bensing, J. M. (2005b). Initial cancer genetic counseling consultation: change in counselees’ cognitions and anxiety, and association with addressing their needs and preferences. American Journal of Medical Genetics, 137, 27–35.
Pieterse, A. H., Van Dulmen, A. M., Ausems, M. G. E. M., Beemer, F. A., & Bensing, J. M. (2005c). Communication in cancer genetic counselling: does it reflect counselees’ pre-visit needs and preferences? British Journal of Cancer, 92, 1671–1678. doi:https://doi.org/10.1038/sj.bjc.6602570.
Pieterse, A. H., Van Dulmen, A. M., Beemer, F. A., Ausems, M. G. E. M., & Bensing, J. (2006). Tailoring communication in cancer genetic counseling through individual video-supported feedback: a controlled pretest-posttest design. Patient Education and Counseling, 60, 326–335. doi:https://doi.org/10.1016/j.pec.2005.06.009.
Plain English Campaign. (2001a). How to write medical information in plain English. https://doi.org/www.plainenglish.co.uk/medicalguide.pdf.
Plain English Campaign. (2001b). Plain English tips for clear websites. https://doi.org/www.plainenglish.co.uk/files/websitesguide.pdf.
Revere, D., & Dunbar, P. J. (2001). Review of computer-generated outpatient health behavior interventions: clinical encounters “in absentia”. Journal of the American Medical Informatics Association, 8, 62–79.
Ruiter, R. A., Kessels, L. T., Jansma, B. M., & Brug, J. (2006). Increased attention for computer-tailored health communications: an event-related potential study. Health Psychology, 25, 300–306. doi:https://doi.org/10.1037/0278-6133.25.3.300.
Skinner, C. S., Strecher, V. J., & Hospers, H. (1994). Physicians’ recommendations for mammography: do tailored messages make a difference? American Journal of Public Health, 84, 43–49. doi:https://doi.org/10.2105/AJPH.84.1.43.
Skinner, C. S., Schildkraut, J. M., Berry, D., Calingaert, B., Marcom, P. K., Sugarman, J., et al. (2002). Pre-counseling education materials for BRCA testing: does tailoring make a difference? Genetic Testing, 6, 93–105. doi:https://doi.org/10.1089/10906570260199348.
Smets, E., Van Zwieten, M., & Michie, S. (2007). Comparing genetic counseling with non-genetic health care interactions: two of a kind? Patient Education and Counseling, 68, 225–234. doi:https://doi.org/10.1016/j.pec.2007.05.015.
Statistics Netherlands. (2007). Telefoneren via internet neemt snel toe. Voorburg/Heerlen: Statistics Netherlands.
Strecher, V. J. (1999). Computer-tailored smoking cessation materials: a review and discussion. Patient Education and Counseling, 36, 107–117. doi:https://doi.org/10.1016/S0738-3991(98)00128-1.
University Medical Centre Utrecht. (2002). Erfelijkheidsonderzoek de procedure (Genetic counseling the procedure). Utrecht: Department of Medical Genetics, University Medical Centre Utrecht.
Van Asperen, C., Van Dijk, S., Zoeteweij, M. W., Timmermans, D. R., De Bock, G. H., Meijers-Heijboer, E. J., et al. (2002). What do women really want to know? Motives for attending familial breast cancer clinics. Journal of Medical Genetics, 39, 410–414. doi:https://doi.org/10.1136/jmg.39.6.410.
Van der Meulen, N., Jansen, J., Van Dulmen, S., Bensing, J., & Van Weert, J. (2008). Interventions to improve recall of medical information in cancer patients: a systematic review of the literature. Psycho-Oncology, 17, 857–868. doi:https://doi.org/10.1002/pon.1290.
Van Oostrom, S. H., Anema, J. R., Terluin, B., Venema, A., De Vet, H. C., & Van Mechelen, W. (2007). Development of a workplace intervention for sick-listed employees with stress-related mental disorders: Intervention Mapping as a useful tool. BMC Health Services Research, 7, 127. doi:https://doi.org/10.1186/1472-6963-7-127.
Wakefield, C. E., Meiser, B., Homewood, J., Peate, M., Kirk, J., Warner, B., et al. (2007). Development and pilot testing of two decision AIDS for individuals considering genetic testing for cancer risk. Journal of Genetic Counseling, 16, 325–339. doi:https://doi.org/10.1007/s10897-006-9068-x.
Wakefield, C. E., Meiser, B., Homewood, J., Peate, M., Taylor, A., Lobb, E. A., et al. (2008). A randomized controlled trial of a decision aid for women considering genetic testing for breast and ovarian cancer risk. Breast Cancer Research and Treatment, 107, 289–301. doi:https://doi.org/10.1007/s10549-007-9539-2.
Walters, S. T., Wright, J. A., & Shegog, R. (2006A). Review of computer and Internet-based interventions for smoking behavior. Addictive Behaviors, 31, 264–277. doi:https://doi.org/10.1016/j.addbeh.2005.05.002.
Acknowledgment
We want to thank the programmers, Paul van der Heijden and Marcus Winckers, who developed the website. Also, we thank the members of the expert panel: Ms. C.J.M. van der Sijs-Bos (clinical geneticist), Ms. A.E. Schoemaker (genetic counselor), Ms. L. van Rossum (counselee-expert Dutch Breast Cancer Association), Ms. L. Vermaas (webmaster and counselee-expert Dutch Breast Cancer Association), Ms. E.M. Maas (counselee-expert). Finally, we would like to thank the respondents who participated in the test phase. This study was funded by a grant from the Dutch Cancer Society (Nivel 2006-3469).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Albada, A., van Dulmen, S., Otten, R. et al. Development of E-Info Geneca: A Website Providing Computer-Tailored Information and Question Prompt Prior to Breast Cancer Genetic Counseling. J Genet Counsel 18, 326–338 (2009). https://doi.org/10.1007/s10897-009-9221-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10897-009-9221-4