
Abstract
Posttraumatic Stress Disorder (PTSD) is common among primary care patients and is associated with significant functional impairment, physical health concerns, and mental health comorbidities. Significant barriers to receiving adequate treatment often exist for primary care patients with PTSD. Mental health professionals operating as part of the primary care team have the potential to provide effective brief intervention services. While good PTSD screening and assessment measures are available for the primary care setting, there are currently no empirically supported primary care-based brief interventions for PTSD. This article reviews early research on the development and testing of primary care-based PTSD treatments and also reviews other brief PTSD interventions (i.e., telehealth and early intervention) that could be adapted to the primary care setting. Cognitive and behavioral therapies currently have the strongest evidence base for establishing an empirically supported brief intervention for PTSD in primary care. Recommendations are made for future research and clinical practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
PTSD in Primary Care is Common and Associated with Poorer Functioning
Posttraumatic Stress Disorder (PTSD) is a common psychiatric condition among primary care patients. Research conducted in civilian and Department of Veterans Affairs (VA) primary care clinics has found that 11–12% of patients have PTSD (Magruder et al., 2005; Stein, McQuaid, Pedrilli, Lenox, & McCahill, 2000), compared to an 8% prevalence found in research conducted with the general population (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995), suggesting that individuals with PTSD may be more likely to engage in primary care services than individuals without PTSD. Among special populations, such as veterans of the Iraq and Afghanistan Wars, as many as 58% of primary care patients may have PTSD (Seal et al., 2010).
PTSD symptoms are associated with significant functional impairment, higher rates of medical utilization, more intense physical symptoms, and poorer health functioning (Gillock, Zayfert, Hegel, & Ferguson, 2005; Stein et al., 2000). Increased negative health perceptions and a higher likelihood of suicide are also found among older adults with PTSD in both VA and civilian primary care settings (Rauch, Morales, Zubritsky, Knott, & Oslin, 2006). Among primary care patients, PTSD is often comorbid with other psychiatric disorders, especially depression and alcohol use disorders (Hankin, Spiro, Miller, & Kazis, 1999; Stein et al., 2000). In primary care, depression-PTSD comorbidity is associated with lower social support, greater health care utilization and more severe depressive symptoms, compared to patients with depression only (Campbell et al., 2007). Research with civilians with substance use disorders demonstrates that individuals with chronic PTSD symptoms have poorer substance use treatment outcomes then those with PTSD that remits over the course of treatment (Read, Brown, & Kahler, 2004). Also, PTSD in the primary care setting has been found to be a persistent illness: even those patients who “recover” often still suffer from functional impairment related to subthreshold PTSD symptoms (Zlotnick et al., 2004). In fact, subthreshold PTSD, defined as reporting a traumatic stressor, at least one re-experiencing symptom and either three avoidance or two arousal symptoms from the DSM-IV diagnostic criteria (Grubaugh et al., 2005), is very common in primary care. As many as 25% of civilian primary care patients may meet criteria for PTSD and it is associated with multiple impairments, including more bodily pain and poorer physical functioning (Gillock et al., 2005).
Barriers Associated with PTSD Treatment
Individuals with PTSD often have problems seeking and accessing appropriate mental health services. For instance, in a sample of civilian women who experienced sexual assault, physical symptoms and psychological distress were related to seeking more medical treatment, but not more mental health treatment (Kimerling & Calhoun, 1994). Active duty military personnel who screened positive for PTSD were twice as likely to report perceived barriers to seeking treatment compared to those who did not screen positive, with only 23–40% seeking PTSD treatment (Hoge et al., 2004). The most common barriers concerned the stigma of receiving mental health treatment (e.g., “I would be seen as weak” and “it would harm my career”). Practical barriers were also frequently reported, such as difficulty getting time off from work. PTSD avoidance symptoms can play a large role in treatment avoidance (Sayer et al., 2009). Veterans with PTSD often refuse treatment due to negative perceptions about service accessibility, delivery and efficacy (Desai, Stefanovics, & Rosenheck, 2005).
A large study of Iraq and Afghanistan veterans found that those who received PTSD diagnoses in primary care were significantly less likely to receive adequate PTSD treatment compared to patients receiving PTSD diagnoses in a specialty mental health setting (Spoont, Murdoch, Hodges, & Nugent, 2010). The authors speculate that this gap in treatment services may be because patients have trouble following through on referrals made to services outside of the primary care clinic. Primary care clinics not located within larger health care systems may have trouble finding appropriate mental health professionals to which to refer patients with PTSD. There is a shortage of licensed mental health professionals in general, and a significant lack of professionals specifically trained to provide evidence-based PTSD treatment (Frueh, Cusack, Grubaugh, Sauvageot, & Wells, 2006). Individuals with PTSD may perceive fewer barriers for seeking treatment in primary care than in traditional mental health settings. This is evidenced by research findings that individuals with PTSD tend to be more likely to present to primary care settings than to mental health care settings (Stein et al., 2000; Zlotnick et al., 2004). This may be due to patients feeling more comfortable in the primary setting or because they are presenting with physical complaints. Regardless, primary care may offer a unique opportunity to increase access to PTSD treatment.
The Need for Primary-Care Based PTSD Treatments
In recent years several factors have contributed to there being a greater need for PTSD treatments to be provided in primary care. Patients with PTSD are more likely to report PTSD symptoms and related functional problems to primary care providers than mental health providers (Butterfield & Becker, 2002). In healthcare systems where regular PTSD screening has been implemented, (e.g., VA), the disorder is being detected more often (Kimerling et al., 2006). This has led to more referrals to mental health providers for treatment. With increasing frequency, both civilian and military healthcare systems have integrated mental health professionals into the primary care setting (Robinson & Strosahl, 2009; VHA, 2008). However, there are no evidence based-treatment guidelines on how integrated primary care mental health providers should treat PTSD. This makes treating PTSD in primary care difficult and leaves many providers guessing on how to most appropriately address PTSD symptoms. Research is needed to develop and test evidence based interventions for PTSD appropriate for the primary care setting.
Benefits of Mental Health Services Provided Within Primary Care
The rationale for providing behavioral health treatment in primary care is well established: (1) Primary care patients with mental health problems often do not receive adequate mental health treatment, are more likely to be see their primary care provider than a mental health provider, and often have comorbid medical concerns; (2) evidence-based interventions have been successfully developed for depression, generalized anxiety, and alcohol misuse (see Butler et al., 2008 for review); and (3) primary care-based treatment has the potential to increase treatment access by reducing the stigma associated with specialty mental health treatment, and increasing the convenience of receiving treatment by allowing patients to receive comprehensive healthcare in one setting.
Primary Care-Mental Health Integration (PC-MHI) offers several benefits for engaging patients in treatment and enabling the health care environment run more smoothly. The primary care provider is often able to introduce the patient to the mental health provider in-person, increasing the likelihood of patient engagement (Blount, 2003). In fact, referrals by a medical provider and familiarity with a mental health provider are the strongest predictors of whether a patient will engage in mental health treatment (Ledoux, Barnett, Garcini, & Baker, 2009). PC-MHI also enables a stepped-care approach where patients with symptoms of mild to moderate severity can be treated within primary care and PC-MHI providers can facilitate the transfer of more severe patients to specialty mental health to ensure that patients are not lost in the system. Stepped-care frees up specialty care to focus on patients most in need of specialized services. PC-MHI providers can also offer education and consultations to primary care providers about how to encourage ambivalent patients to accept referrals and to manage patients with mental health problems most effectively. However, primary care providers have many competing demands within the brief time they spend with each patient, including the patient’s presenting health concerns, routine medical tests, health behaviors (e.g., exercise), and addictions (including nicotine). To date, primary care guidelines have not prioritized PTSD assessment and treatment and this will require education and support from administration and mental health professionals (Prins, Cimpean, & Schnurr, 2009).
Screening and Assessment for PTSD in Primary Care
Primary care offers an excellent opportunity to administer brief screening measures for PTSD. Screening is a vital first step to determine if more extensive PTSD assessment is required. General principles for effective screening for trauma symptoms include that it be done with every patient routinely and that follow-up be conducted in a private setting (Resnick, Acierno, Holmes, Dammeyer, & Kilpatrick, 2000). Considerable research efforts have been made to validate and implement PTSD screening instruments in VA primary care clinics. Kimerling et al. (2006) found a 7-item PTSD screen to have good test–retest reliability and good sensitivity and specificity when compared to the gold standard of PTSD assessments, the Clinician-Administered PTSD Scale (CAPS). Prins et al. (2003) validated the 4-item Primary Care PTSD Screen (PC-PTSD) among a sample of male and female VA primary care patients and found that a cut-off score of 3 offered good sensitivity and specificity compared to the CAPS. The PC-PTSD is now required to be administered to every VA primary care patient nationwide on an annual basis. VA/Department of Defense (DOD) Clinical Practice Guidelines (2004) state that patients who screen positive on the PC-PTSD need to be further evaluated either by their primary care provider or by a mental health provider. Further evaluation should include an assessment of all DSM-IV PTSD symptoms, which can be accomplished by the PTSD Checklist (PCL), a 17-item scale that has also been validated with veteran primary care patients (Yeager, Magruder, Knapp, Nicholas, & Frueh, 2007). When using the PCL in primary care, lower cut-offs scores are recommended. Brewin (2005) recommends cut-offs between 30 and 44 for civilian primary care patents, while the typical cut-off for psychiatric patients is 50. In addition, the VA/DOD guidelines recommend that characteristics of the trauma exposure, dangerousness to self and others, physical and mental health functioning, and comorbid psychiatric problems should be assessed.
Unfortunately, less progress has been made in screening for PTSD in the civilian sector. Nonetheless, regular screening is desperately needed. Liebschutz et al. (2007) found that that only 11% of civilian primary care patients with PTSD had the diagnosis listed in their medical charts. Brief screening instruments like the PC-PTSD need to be validated in civilian primary care clinics and regular screening for PTSD needs to be prioritized in order to reduce the burden placed on healthcare systems by patients with undetected conditions. The VA/DOD guidelines described above could serve as a guide for assessing PTSD in civilian primary care settings.
Important Considerations When Developing a Primary Care-Based PTSD Treatment
The civilian, VA and military guidelines for treating PTSD in specialty mental health settings should be taken into account when considering how to develop brief interventions for primary care. VA/DOD Clinical Practice Guidelines (2004) recommend several specific psychopharmacology (i.e., selective serotonin re-Uptake inhibitors) and psychotherapy (Cognitive Therapy, Exposure Therapy, Stress Inoculation Training, and Eye Movement Desensitization and Reprocessing) first-line treatments. The more recent Institute of Medicine guidelines (2008) conclude that the current evidence for efficacy for patients with PTSD is inadequate for all classes of medications and only found support for the efficacy of exposure therapies for treating PTSD. It was noted that exposure therapies contain components of other cognitive-behavioral approaches and therefore their conclusions should not be interpreted too narrowly. In consideration of both sets of guidelines, it appears that cognitive-behavioral exposure therapies currently have the best evidence base and offer considerable promise for developing PTSD intervention for the primary care setting. However, since this field of inquiry is still in its infancy it is important to continue to investigate the efficacy of other psychotherapies and pharmacological interventions for PTSD.
When considering how to develop interventions to treat PTSD within primary care, it is important to reflect on previous work that describes what type of mental health interventions work best within this unique setting. Decades of research and clinical practice have found that briefer interventions are better accepted by patients and providers in the fast-paced setting of primary care (e.g., Gunn & Blount, 2009; McDaniel & LeRoux, 2007). The Primary Care Behavioral Health Model developed by Robinson and Strosahl (2009) emphasizes providing immediate access to behavioral health services by placing a behavioral health provider in the exam room area of primary care to function as a core member of the primary care team. This model has significantly influenced the Primary Care-Mental Health Integration (PC-MHI) models utilized by Kaiser Permanente, VA, Air Force, and other large health care systems. PC-MHI often includes two components: care management and co-located collaborative care. Care management utilizes a nurse care manager who tracks and reinforces patient’s adherence to medical and mental health treatment plans. Co-located collaborative care utilizes an integrated mental health provider to provide a broad spectrum of behavioral health services, work collaboratively with other members of the medical team, and take a population-based approach focused on time-limited, problem-focused, and solution-oriented interventions (Beehler, Finnell, Foltz, & Edwards, 2010).
Interventions for Treating PTSD in Primary Care
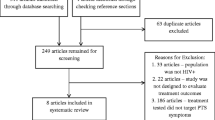
The remainder of this article reviews two types of PTSD treatments: those that have been tested within primary care (n = 4, Table 1) and those from other settings (e.g., telehealth, medical trauma units) with the potential to inform brief primary care-based treatments for PTSD (n = 9). Tables 1 and 2 summarize important aspects of each treatment including setting, diagnostic focuses in addition to PTSD, treatment length, whether the treatment is in a standardized format (e.g., manualized), the type of research evidence available, PTSD outcome measure(s) used, and intervention effect sizes for PTSD. Table 3 summaries the specific types of therapeutic interventions (e.g., relaxation, written exposure) utilized in each PTSD treatment reviewed. Symptom assessment was delivered in each treatment package and therefore is not included in Table 3. The text below describes the treatments in more detail and discusses implications for developing an empirically supported primary care-based PTSD intervention.
Effect sizes not reported by authors were calculated (Cohen’s d = (M 1 − M 2/(SD 1 + SD 2/2) for all but one study, which did not provide enough information for a calculation. For quasi-experimental studies with no comparison group, effect sizes are a measure of the magnitude of change in PTSD symptoms from pre- to post-intervention. For randomized controlled trials, effect sizes are a measure of the magnitude of the difference between the intervention and comparison group at 6 month follow-up, unless otherwise noted in Tables 1 and 2. Effect sizes were interpreted according to whether the intervention had a minimal, moderate, or strong “practically significant” effect (Ferguson, 2009).
Care Management
Two care management models for depression have been modified to incorporate the treatment of PTSD in military personnel and veterans. The Army has developed Re-Engineering Systems of Primary Care for PTSD and Depression in the Military (RESPECT-Mil) in which a primary care provider assesses for PTSD using the PCL and depression using the Patient Health Questionnaire-Depression Module (PHQ-9). Patients who score positive are provided education on current symptoms, and offered medication management or a referral for counseling. Nurse care managers call the patient to reassess symptoms and encourage treatment adherence. A psychiatrist serves as a behavioral health specialist and provides consultations to the primary care provider and the care manager. Engel et al. (2008) reported that the majority of 69 patients receiving RESPECT-Mil experienced clinically meaningful reductions in PTSD and/or depressive symptoms over 6 weeks of treatment. Specifically, 14 out of the 21 participants who received a follow-up PCL 6–10 weeks after beginning RESPECT-Mil reported at least a 5 point decrease. Mean and standard deviations were not reported. The VA is now conducting two randomized clinical trials to evaluate two care management treatments for primary care patients with PTSD. RESPECT-P is based on the RESPECT-Mil model for treating PTSD in primary care. The second VA model being tested, Translating Initiatives for Depression into Effective Solutions-PTSD (TIDES/PTSD) is based on the empirically supported TIDES model of care management for depression (Hedrick et al., 2003). TIDES/PTSD provides nurse care manager telephone support for medication management, psychosocial support and a workbook for patient self-management of PTSD symptoms. Results from the RESPECT-P and TIDES/PTSD clinical trials are not yet available. While the RESPECT-Mil, RESPECT-P, and TIDES/PTSD are major initial steps in bringing PTSD treatment into the primary setting, limitations include the need to refer outside of primary care for counseling/therapy, and that the interventions consist mostly of medication management. As discussed earlier, CBT and exposure therapies currently have the strongest evidence base for PTSD.
Interventions for PTSD Led by Mental Health Professionals
Research is beginning to emerge that describes the development and testing of primary care-based treatments for PTSD delivered by mental health professionals. The literature varies in that some interventions have tested “treatment as usual” approaches, and others have developed manualized treatments and conducted randomized controlled trials. These treatments generally fit the criteria for co-located collaborative care described above.
Corso et al. (2009) published an informative article about the PC-MHI treatment approach offered to primary care patients with PTSD in Air Force family medicine clinics. Treatment involves several empirically supported components delivered within five or fewer 30 min sessions. Treatment as usual (TAU) includes relaxation training and behavioral activation, including pleasant events scheduling and enhanced problem solving. Some patients also complete writing assignments for homework. Writing can be combat-focused, a form of imaginal exposure, or impact-focused (i.e., centered on the impact and meaning of a traumatic combat experience), a form of cognitive restructuring. A pilot study non-randomly assigned 19 participants with PTSD to one of three groups: TAU, TAU plus combat-focused writing, or TAU plus impact-focused writing. Significant decreases in pre–post PCL scores were only found for the impact-focused writers (M = 11, SD = 8, 95% CI = 5–17, t = 4.3, p = .003, d = 1.4). This study is an excellent example of how mental health professionals developed a treatment approach within their normal practice and have now begun to empirically investigate its effectiveness. Advantages of this treatment approach include its brevity and use of evidence-based strategies. The fact that it was implemented by regular PC-MHI staff increases its feasibility in primary care. A treatment manual, however, needs to be developed to adequately investigate efficacy within a clinical trial.
Coordinated Anxiety Learning and Management (CALM) is an intervention for primary care patients with PTSD or three other anxiety disorders, that offers assessment, psychoeducation, and the option of computer-assisted CBT, medication management, or both provided by an Anxiety Clinical Specialist (usually a nurse or social worker) working in conjunction with the primary care provider (Craske et al., 2009). CALM computer-assisted CBT consists of approximately eight 60 min sessions where the Anxiety Clinical Specialist leads the patient through an interactive computer program that teaches self-monitoring, relaxation, cognitive restructuring, and exposure to feared stimuli. An analysis of 261 participants who received at least one session of CALM CBT found that patients self-reported significant improvements in anxiety and depression on post-session rating scales, regardless of the type of anxiety disorder they were diagnosed with or whether they were using psychiatric medication (Craske et al., 2009). Also, participant understanding of the CBT module significantly predicted final session anxiety rating scores. A clinical trial (n = 1004) that took place in 17 civilian primary care clinics found that compared to usual care, CALM participants reported significant improvements in anxiety symptoms as measured by the Brief Symptom Inventory-12 at 6, 12 and 18 months (Roy-Burne et al., 2010). For participants with PTSD (n = 181) the largest effect was found at 6 months (mean difference −5 points; 95% CI = −8 to −2 points; p < .001, d = −.469) (Roy-Byrne et al., 2010). Major strengths of this intervention include the use of empirically supported anxiety management strategies, computer-assisted delivery that allows non-expert clinicians to provide high fidelity treatment, and the program’s ability to treat any 1 of 4 anxiety disorders with disorder-specific content. A limitation is that the session length and duration of treatment is more typical of a specialty care setting and may not be feasible in primary care. Also, since a PTSD symptoms measure was not used, how the intervention affected specific PTSD symptoms is unknown.
Cognitive Behavioral Therapy-Primary Care (CBT-PC) is a manualized treatment program adapted from the full length Cognitive Restructuring for PTSD program (Hamblen, Mueser, Rosenberg, & Rosenberg, 2005). Six, 1 h sessions focus on psychoeducation, identifying and replacing distorted thinking, practicing newly learned skills for homework, and relapse prevention. A pilot study (N = 10) was conducted with CBT-PC delivered by specially trained primary care providers to civilian primary care patients. A significant improvement in PTSD was found from baseline (mean PCL score = 56, SD = 13) to 3 month follow-up (mean PCL score = 28, SD = 9) (Prins et al., 2009). CBT-PC utilizes CBT techniques with significant empirical support and its manualized format makes future research and clinical demonstration projects highly feasible. Further information is needed on the feasibility of training primary care providers to deliver CBT and delivering 1 h sessions in primary care.
Brief PTSD Interventions that Could Be Adapted for the Primary Care Setting
Telehealth Interventions
Telehealth interventions, including internet-based treatments, are being developed to treat PTSD. These interventions are unique in that they are not housed in specialty or primary care, but are virtual and therefore more easily applied to diverse settings. Previous research (e.g., CALM) has shown that technology can be effectively used to treat PTSD in primary care. Also telehealth has the potential to be efficient, low-cost, and stigma reducing. Patients can be trained within primary care to utilize a telehealth intervention and then assigned to engage in the intervention at home. Research supports that rural and urban dwelling individuals with PTSD are receptive to receiving telemental health care (Grubaugh, Cain, Elhai, Patrick, & Frueh, 2008). Individuals with PTSD are especially likely to choose to live in remote areas to reduce over stimulation, hyperarousal and interpersonal conflict (Morland, Freuh, Pierce, & Miyahira, 2003) and thus are potentially good candidates for virtual treatments. Telehealth treatments are also a good fit for military personnel who report high levels of experience with the internet and often prefer to receive mental health treatment via technology-based approaches (Wilson, Onorati, Mishkind, Reger, & Gahm, 2008).
Delivery of Self Training and Education for Stressful Situations (DE-STRESS) is a therapist assisted, self-management CBT intervention for PTSD delivered via the internet (Litz, Engel, Bryant, & Papa, 2007). It was designed for military personnel and seeks to teach patients strategies to help them cope and manage their reactions to situations that trigger recall of traumatic experiences. Patients are enrolled in DE-STRESS for 8 weeks and are encouraged to log-on daily to complete symptom self-monitoring, didactics on stress management, graduated self-guided in vivo exposure to triggers of distress, eight trauma-focused narratives, and relapse prevention. After an initial in-person session, therapists communicate with patients by phone and email as needed. A randomized controlled trial compared 8 weeks of DE-STRESS to supportive internet-based counseling (i.e., self-monitoring, writing about non-traumatic stress, and supportive counselor input). DE-STRESS participants reported greater mean PTSD symptom decreases over 6 months as measured by the PTSD Symptom Scale (PSS) (baseline mean = 27, SD = 9, follow-up mean = 9, SD = 8) compared to supportive therapy participants (baseline mean = 29, SD = 10, follow-up mean = 18, SD = 10) (t(2,16) = 2.02, p = .06). DE-STRESS appears to have successfully combined several evidence-based CBT strategies within one internet-based treatment package. It allows patients to receive an intensive daily therapeutic experience with minimal therapist input.
Interapy is an internet-based written emotional disclosure protocol for traumatized civilians (Lange et al., 2003). This CBT intervention focuses on habituation to a traumatic experience through imaginal exposure and cognitive reappraisal of automatic thoughts and misattributions. Patients engage in Interapy via email correspondence with a therapist. In the first 2 weeks, four essays focused on habituation to the targeted traumatic experience are written, followed by 2 weeks of writing four cognitive reappraisal essays (i.e., challenging dysfunctional automatic thoughts, reinterpreting misattributions, and creating a new symbolic meaning for the trauma), and 1 week of writing two essays in the form of letters “taking leave of the past.” Therapists give email feedback after each essay. Several trials of Interapy have been conducted with Dutch and German participants with various traumatic experiences (e.g., Knaevelsrud & Maercker, 2010). Results from the largest trial are reported here (Lange et al., 2003). A RCT comparing Interapy (n = 69) to a wait-list control group (n = 32) found significant decreases in PTSD symptoms, as measured by the Impact of Event Scale (IES), from pre–post treatment (9 point decrease for intrusions, 8 point decrease for avoidance) and gains were maintained at 6 week follow-up. Results also revealed that participant gender, age, or level of internet expertise were not associated with treatment outcomes. Interapy is a simple and novel way to engage patients with evidence-based CBT to reduce trauma symptoms.
PTSD Online is a 10 week, therapist-assisted internet treatment program for civilians with PTSD focused on CBT and exposure strategies (Klein et al., 2010). Participants are asked to read one module per week, complete homework and communicate with the therapist via email. There is no face-to-face contact between study staff/therapists and participants. Twenty-two participants reported a small, but significant decrease in PCL scores from pre-intervention (mean = 54, SD = 14) to 3 month follow-up (mean = 45, SD = 14) (F(2,40) = 7.38, p = .002). Average therapist time spent emailing participants was approximately 3 h per participant, a substantial decrease from the amount of time face-to-face CBT typically takes (twelve 50 min sessions). Despite minimal therapist contact, participants reported a strong therapeutic alliance and high module content understanding.
Hirai and Clum (2005) created the 8 week internet-based Self-Help for Trauma Consequences (SHTC) program for civilians with subthreshold PTSD. The program includes relaxation training, cognitive restructuring, and written exposure. Participants wrote in present tense about the details and their emotional response to one traumatic event. No feedback was given to the participants about their writing. Participants (N = 27) were randomized to SHTC or a wait-list control group. SHTC participants reported non-statistically significant decreases on PTSD symptoms on the IES, but did report significant decreases in the frequency of intrusions (SHTC mean = −6, SD = 3, wait-list mean = −3, SD = 3, F(1,24) = 14.68, p < .01) and avoidance (SHTC mean = −3, SD = 3, wait-list mean = −1, SD = 3, F(91.24) = 5.21, p < .05) at post-treatment. SHTC is unique in two ways. It is the only PTSD treatment reviewed here that does not include therapeutic interactions from a mental health profession. This makes it truly a “self-help” treatment, a modality that is largely unexplored in PTSD intervention research. Also, individuals with subthreshold PTSD symptoms participated in SHTC. As discussed earlier, subthreshold PTSD symptoms are common and often very impairing for primary care patients.
Each of the telehealth interventions discussed thus far enable more intensive PTSD treatment to be provided with minimal in-clinic patient time and provider time. This makes these interventions applicable to the primary care setting. However, decreased patient-provider contact may need to be compensated for with careful selection of patients and close monitoring of symptoms over the course of treatment to minimize any patient safety risks.
Early Intervention Research
Researchers investigating early intervention and secondary prevention for PTSD and Acute Stress Disorder (ASD) have developed brief treatments that could be adapted to the primary care setting. These interventions tend to rely heavily on exposure to trauma-related stimuli and some also incorporate other cognitive-behavioral anxiety management strategies. Cigrang, Peterson, and Schobitz (2005) published a series of three case studies of active duty military personnel with combat-related PTSD symptoms who were treated with four sessions of exposure therapy while serving in Iraq. Based on Prolonged Exposure (PE) guidelines, psychologists delivered imaginal exposure and encouraged patients to engage in self-exposure to any stimuli they were avoiding outside of session. On average, the participants showed a 56% decrease in PTSD symptoms and each no longer met criteria for PTSD on the PCL post-treatment. Similar treatments have been delivered to civilian populations. Bryant, Sackville, Dang, Moulds, and Guthrie (1999) ran a randomized clinical trial (n = 45) where civilian participants received either five sessions of PE, PE plus CBT anxiety management strategies (e.g., cognitive restructuring), or supportive psychotherapy. Posttreatment and 6 month follow-up CAPS PTSD scores showed that both exposure-based treatments were superior to supportive psychotherapy and no significant differences were found between PE alone and PE plus anxiety management (mean total CAPS scores at 6 month follow-up for supportive therapy = 56, SD = 9, PE alone = 25, SD = 13, PE + anxiety management = 30, SD = 14), indicating that cognitive restructuring may add no benefit to brief exposure treatments. One other unique application of brief ASD intervention bears mentioning. Hickling, Blanchard, and Kuhn (2005) provided two sessions of treatment focusing on imaginal exposure and cognitive therapy techniques with a check-in phone call in between the two sessions to three civilian patients with ASD or PTSD related to a motor vehicle accident. All three participants demonstrated significant improvement in PTSD symptoms 6 months post-treatment, averaging a 25 point decrease on their PCL scores. These early intervention studies demonstrate that both civilians and military personnel can benefit from very brief CBT treatment and the use of phone check-in sessions may be a time and cost-efficient way to provide additional treatment. However, further research is needed to investigate whether these treatments are effective for chronic PTSD, as seen in primary care.
Another setting where brief PTSD treatments have been investigated is inpatient medical units for physically injured trauma survivors. Zatzick et al. (2004) investigated the efficacy of a collaborative stepped-care intervention that consisted of immediate case management and motivational interviewing targeting alcohol use, and evidence-based psychopharmacology and/or CBT if PTSD symptoms persisted for 3 months post-trauma. Civilian patients (N = 120) were randomized to receive this intervention or usual post-trauma medical care. Twelve patients met diagnostic criteria for PTSD at 3 months: 5 patients opted to receive 5–12 sessions of CBT (i.e., psychoeducation, muscle relaxation, cognitive restructuring and graded exposure) and 10 patients opted for medication (i.e., SSRIs). From baseline to 12 month follow-up, intervention participants experienced a 24% decrease in alcohol use (95% CI = −20 to −29%) as measured by the Composite International Diagnostic Interview (CIDI) and no change in PTSD symptoms (95% CI = −4 to 4%) as measured by the PCL, while usual care participants had a 13% increase in alcohol use (95% CI = 8–18%) and a 6% increase in PTSD symptoms (95% CI = 3–9%). The intervention appears to have successfully prevented the exacerbation of PTSD while effectively treating alcohol misuse. However, PTSD and alcohol use are known to fluctuate together (Read et al., 2004) and it is possible that an effective alcohol treatment could decrease PTSD symptoms. Regardless, PTSD and alcohol use commonly occur in the primary care setting (Hankin et al., 1999) and developing brief combined treatments is an important area of investigation.
Another early intervention for physically injured trauma survivors with PTSD symptoms is behavioral activation (BA). BA is a common component of CBT and is an evidence-based stand alone treatment for depression (Martell, Addis, & Jacobson, 2001). BA is theorized to be effective for PTSD because increased guided activities may break patterns of avoidance that maintain PTSD. Increasing activities consistent with short and long term goals is the central component of BA. Wagner, Zatzick, Ghesquiere, and Jurkovich (2007) piloted BA for physically injured civilian trauma survivors (N = 8) with PTSD 1 month post-injury. Participants were assigned to 4–6 sessions of 60–90 min in length or usual medical care. BA participants reported a mean decrease of 15 PCL points from pre- to post-treatment compared to usual care participants who reported a mean increase of 2 PCL points. BA has also been piloted with veterans (n = 11) with PTSD with similar results (Jakupcak et al., 2006). Focusing on just one CBT component, like BA, may be an effective strategy for developing a very brief treatment suitable for primary care.
Recommendations for Future Research and Clinical Practice
In this paper, several PTSD treatments were reviewed in order to inform future treatment development and clinical practice focused on reducing PTSD symptoms in the primary care setting. This review is able to answer several important and highly relevant questions. Mental health clinicians typically provide treatment in 12 or more sessions. This has led to considerable skepticism as to whether brief treatments really work for a disorder as complicated and impairing as PTSD. Research evidence is now accumulating that informs us that brief PTSD treatment is effective for many patients. Moderate effect sizes were found for most of the brief treatments reviewed. This is important because brief interventions place a smaller burden on the health care system and some patients are not ready or willing to engage in longer treatments in specialty care settings. Another area of skepticism and debate is whether exposure therapy for PTSD can be safely and effectively administered in non-traditional ways, such as in brief interventions and using telehealth approaches. This review has demonstrated that imaginal (i.e., written and verbal) and in vivo exposure therapies can be safely and effectively delivered in non-traditional ways. The majority of treatments reviewed utilized exposure strategies, with those using in vivo exposure having particularly large effect sizes. However, this is not to say that it is necessary to use exposure therapy to treat patients with PTSD. Several treatment packages demonstrate that PTSD symptoms can be reduced using other CBT strategies or medications (e.g., Engel et al., 2008; Prins et al., 2009; Wagner et al., 2007). Therefore, an argument can be made that further treatment development and testing is warranted for brief PTSD interventions that both utilize and do not utilize exposure therapies.
Psychological treatment can be viewed on a continuum of provider and patient contact ranging from self-guided interventions assigned by a medical provider with no involvement of a mental health professional, to traditional specialty care settings where patients meet with providers for 60–90 min sessions on a frequent and ongoing basis. This review found that initial evidence exists for PTSD treatments in the middle of this continuum, i.e., brief in-person and telehealth treatments guided by a therapist. Most of these treatments emphasize the delivery of cognitive and/or behavioral interventions. Given this, behavioral health providers in primary care should consider brief cognitive or behavioral intervention as a first-line treatment. Incorporating telehealth, especially the use of the internet, into therapist-led treatments also seems warranted given patients’ interest in using the internet, the potential for time and cost savings, and the initial promising research results.
In a primary care setting, the interaction time between patient and provider must be brief. Therefore, which cognitive or behavioral strategies to incorporate into a treatment package must be chosen carefully. As can be seen in Table 3, there are several common elements of the reviewed PTSD treatments. While ongoing assessment and psycho-education seem vital to include in any treatment package, relaxation strategies, cognitive restructuring, and some type of exposure appear to also be important ingredients. Dismantling studies exploring which aspects of CBT are most effective in brief treatments are needed. The study by Bryant et al. (1999) demonstrating that adding anxiety management strategies to imaginal exposure did not produce additional symptom relief, is an example of the type of research that can guide the selection of the most relevant CBT components. Focusing on one specific strategy such as BA (Wagner et al., 2007) or written imaginal exposure (Lange et al., 2003) may also continue to prove to be an effective approach. One behavioral intervention that is used within the primary care setting for a variety of behavioral disorders, but has not yet been tested with primary care patients with PTSD is Acceptance and Commitment Therapy (ACT) (Robinson, Gregg, Dahl, & Lundgren, 2004). ACT conceptualizes that dysfunction from PTSD arises from attempts to avoid or eliminate emotions, thoughts or memories related to trauma (Walser & Westrup, 2007). ACT may be more acceptable to some patients who do not initially feel ready for exposure work. Exposure follows interventions focused on clarifying personal values and gaining distance from painful emotions and takes the form of increased willingness to experience painful emotions and acceptance of past traumatic events.
Self-help research is another area that has been neglected in regards to PTSD treatment development. Self-help treatments commonly teach evidence-based CBT strategies and are assigned and monitored by regular primary care staff. There is often no involvement of mental health professionals. Currently no primary care-based self-help treatments for PTSD exist. This is an important venue for investigation for several reasons. Brief primary care-based self-help treatments for anxiety and depression have been successfully developed and implemented. A recent meta-analysis of guided self-help psychotherapy for depression and anxiety examined 21 studies and concluded that self-help treatments were at least as effective as face-to-face treatments (Cuijpers, Donker, van Straten, Li, & Andersson, 2010). As detailed earlier, a telehealth self-help intervention for PTSD (SHTC) has also found initial positive results. Self-help treatment would be useful in primary care settings where provider and patient time and resources are scarce.
Half of the primary care-based treatments and two out of nine of the treatments reviewed in Table 2 have been conducted with military personnel or veterans. The question remains as to whether PTSD treatments focused specifically on combat trauma can be generalized to individuals who have experienced other traumatic events, such as interpersonal violence and natural disasters. However, we do know that full length empirically supported PTSD treatments, such as PE and Cognitive Processing Therapy are effective in reducing PTSD symptoms in individuals who have experienced combat and non-combat traumas (Institute of Medicine, 2008). Also, the PTSD treatments reviewed here share many common elements regardless of the traumatic events that triggered PTSD (Table 3). Therefore, a treatment developed for veterans could likely be successfully modified to treat civilian trauma survivors.
In individuals with PTSD, the issue of medical and psychiatric comorbidities must be taken into account when developing treatments. Careful monitoring of physical health, depression, and substance use throughout the course of treatment is necessary to assess the impact the intervention has on comorbidities. Once an empirically supported brief PTSD intervention is developed, the next step would be to develop brief treatments that focus on simultaneously treating common comorbidities. In relation to comorbidities, there are many specific problems that individuals with PTSD often struggle with such as, impaired sleep, anger, and relationship problems. These areas are also important specific targets for primary care-based treatment. Often addressing these concerns first may prepare patients to engage in PTSD-focused treatment whether it is in primary or specialty care.
One overarching recommendation is that a variety of treatments need to be developed in order to match treatments to patients’ needs and preferences. Some patients will prefer self-guided and internet-based treatment, while others will want face-to-face contact with a therapist. Individuals with PTSD may feel ready for intensive verbal imaginal exposure work, while others may prefer to use cognitive restructuring or behavioral activation. Still others may be open to alternative exposure strategies, such as those implemented in ACT. With the large amount of research that needs to be accomplished it is vital that full-time researchers, as well as, scientist–practitioners get involved in treatment development and testing. Many primary care psychologists have developed interventions to treat PTSD. Describing these “treatment as usual” approaches well and gathering pre- and post-treatment symptom data (similar to Corso et al., 2009) is an excellent step to establishing empirically supported primary care-based PTSD treatments.
As can be seen in Tables 1 and 2, a variety of PTSD symptom measures are commonly used in intervention research. While clinical interviews, such as the CAPS and PSS offer the richest and most valid data, these can be impractical in real world research settings. Self-report measures that have been validated with primary care samples, such as the PCL, offer sound alternatives to clinical interviews. Researchers should avoid using measures that are not specific to PTSD symptoms (e.g., BSI) and those that do not measure all PTSD symptoms (e.g., IES). For the many interventions that found positive results with case studies and pilot studies, larger multisite randomized controlled trials are now needed to establish a strong evidence base. Many of the telehealth interventions still need to be tested with primary care patients and early interventions need to be investigated with primary care patients with chronic PTSD. Overall, results from this review are very promising. With increased research attention to establishing empirically supported primary care-based PTSD treatments, we could be helping significantly more primary care patients with PTSD within the next decade.
References
References marked with an asterisk are reviewed in Tables 1, 2, and 3.
Beehler, G. P., Finnell, D. S., Foltz, K., & Edwards, D. (2010). Patient exit interviews for assessing fidelity to the VA VISN 2 Integrated Primary Care Model: Results from a pilot feasibility study. Journal of Interprofessional Care, 24, 323–326.
Blount, A. (2003). Integrated primary care: Organizing the evidence. Families, Systems, and Health, 21, 121–133.
Brewin, C. R. (2005). Systematic review of screening instruments for adults at risk of PTSD. Journal of Traumatic Stress, 18, 53–62.
*Bryant, R. A., Sackville, T., Dang, S. T., Moulds, M. L., & Guthrie, R. M. (1999). Treating acute stress disorder: An evaluation of cognitive behavior therapy and supportive counseling techniques. American Journal of Psychiatry, 156, 1780–1786.
Butler, M., Kane, R. L., McAlpine, D., Kathol, R. G., Fu, S. S., Hadorn, H., et al. (2008). Integration of mental health/substance abuse and primary care. Rockville, MD: Agency of Healthcare Research and Quality.
Butterfield, M. I., & Becker, M. E. (2002). Posttraumatic stress disorder in women: Assessment and treatment in primary care. Primary Care: Clinics in Office Practice, 29, 151–170.
Campbell, D., Felker, B., Liu, C.-F., Yano, E., Kirchner, J., Chan, D., et al. (2007). Prevalence of depression–PTSD comorbidity: Implications for clinical practice guidelines and primary care-based interventions. Journal of General Internal Medicine, 22, 711–718.
*Cigrang, J. A., Peterson, A. L., & Schobitz, R. P. (2005). Three American troops in Iraq: Evaluation of a brief exposure therapy treatment for the secondary prevention of combat-related PTSD. Pragmatic Case Studies in Psychotherapy, 1, 1–25.
*Corso, K. A., Bryan, C. J., Morrow, C. E., Appolonio, K. K., Dodendorf, D. M., & Baker, M. T. (2009). Managing posttraumatic stress disorder symptoms in active-duty military personnel in primary care settings. Journal of Mental Health Counseling, 31, 119–136.
Craske, M. G., Roy-Burne, P. P., Stein, M. B., Sullivan, G., Sherbourne, C., & Bystritsky, A. (2009). Treatment of anxiety disorders: Efficacy to effectiveness to implementation. Behavior Research and Therapy, 47, 931–937.
Cuijpers, P., Donker, T., van Straten, A., Li, J., & Andersson, G. (2010). Is guided self-help as effective as face to face psychotherapy for depression and anxiety disorders? A systematic review and meta-analysis of comparative outcome studies. Psychological Medicine, 40, 1943–1957.
Desai, R. A., Stefanovics, E. A., & Rosenheck, R. A. (2005). The role of psychiatric diagnosis in satisfaction with primary care: Data from the Department of Veterans Affairs. Medical Care, 43, 1208–1216.
*Engel, C. C., Oxman, T., Yamamoto, C., Gould, D., Barry, S., Stewart, P., et al. (2008). RESPECT-Mil: Feasibility of a systems-level collaborative care approach to depression and post-traumatic stress disorder in military primary care. Military Medicine, 173, 935–940.
Ferguson, C. J. (2009). An effect size primer: A guide for clinicians and researchers. Professional Psychology: Research and Practice, 40, 532–538.
Frueh, B. C., Cusack, K. J., Grubaugh, A. L., Sauvageot, J. A., & Wells, C. (2006). Clinicians’ perspectives on cognitive-behavioral treatment for PTSD among persons with severe mental illness. Psychiatric Services, 57, 1027–1031.
Gillock, K. L., Zayfert, C., Hegel, M. T., & Ferguson, R. J. (2005). Posttraumatic stress disorder in primary care: Prevalence and relationships with physical symptoms and medical utilization. General Hospital Psychiatry, 27, 392–399.
Grubaugh, A. L., Cain, G., Elhai, J. D., Patrick, S. L., & Frueh, B. C. (2008). Attitudes toward medical and mental health care delivered via telehealth applications among rural and urban primary care patients. Journal of Nervous and Mental Disease, 196, 166–170.
Grubaugh, A. L., Magruder, K. M., Waldrop, A. E., Elhai, J. D., Knapp, R. G., & Frueh, B. C. (2005). Subthreshold PTSD in primary care: Prevalence, psychiatric disorders, healthcare use, and functional status. Journal of Nervous and Mental Disease, 193, 658–664.
Gunn, W. B., Jr., & Blount, A. (2009). Primary care mental health: A new frontier for psychology. Journal of Clinical Psychology, 65, 235–252.
Hamblen, J. L., Mueser, K. T., Rosenberg, S. D., & Rosenberg, H. J. (2005). Brief cognitive behavioral treatment for PTSD: Treatment manual and handouts. Lebanon, NH: Dartmouth Trauma Interventions Research Center.
Hankin, C. S., Spiro, A., I. I. I., Miller, D. R., & Kazis, L. (1999). Mental disorders and mental health treatment among U.S. Department of Veterans Affairs outpatients: The veterans health study. American Journal of Psychiatry, 156, 1924–1930.
Hedrick, S. C., Chaney, E. F., Felker, B., Liu, C.-F., Hasenberg, N., Heagerty, P., et al. (2003). Effectiveness of collaborative care depression treatment in Veterans’ Affairs primary care. Journal of General Internal Medicine, 18, 9–16.
*Hickling, E. J., Blanchard, E. B., & Kuhn, E. (2005). Brief, early treatment for ASD/PTSD following motor vehicle accidents. Cognitive and Behavioral Practice, 12, 461–467.
*Hirai, M., & Clum, G. A. (2005). An internet-based self change program for traumatic event related fear, distress, and maladaptive coping. Journal of Traumatic Stress, 18, 631–636.
Hoge, C. W., Castro, C. A., Messer, S. C., McGurk, D., Cotting, D. I., & Koffman, R. L. (2004). Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. New England Journal of Medicine, 351, 13–22.
Institute of Medicine of the National Academies. (2008). Treatment of posttraumatic stress disorder: An assessment of the evidence. Washington, DC: The National Academies Press.
Jakupcak, M., Roberts, L. J., Martell, C., Mulick, P., Michael, S., Reed, R., et al. (2006). A pilot study of behavioral activation for veterans with posttraumatic stress disorder. Journal of Traumatic Stress, 19, 387–391.
Kessler, R. C., Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. B. (1995). Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry, 52, 1048–1060.
Kimerling, R., & Calhoun, K. S. (1994). Somatic symptoms, social support, and treatment seeking among sexual assault victims. Journal of Consulting and Clinical Psychology, 62, 333–340.
Kimerling, R., Ouimette, P., Prins, A., Nisco, P., Lawler, C., Cronkite, R., et al. (2006). Brief report: Utility of a short screening scale for DSM-IV PTSD in primary care. Journal of General Internal Medicine, 21, 65–67.
*Klein, B., Mitchell, J., Abbott, J., Shandley, K., Austin, D., & Gilson, K., (2010). A therapist-assisted cognitive behavior therapy internet intervention for PTSD: Pre-, post-, and 3-month follow-up results from an open trial. Journal of Anxiety Disorders, 24, 635–644.
Knaevelsrud, C., & Maercker, A. (2010). Long-term effects of an internet-based treatment for posttraumatic stress. Cognitive Behavior Therapy, 39, 72–77.
*Lange, A., Rietdijk, D., Hudcovicova, M., van de Ven, J.-P, Schrieken, B., & Emmelkamp, M. G. (2003). Interapy: A controlled randomized trial of the standardized treatment of posttramatic stress through the internet. Journal of Consulting and Clinical Psychology, 71, 901–909.
Ledoux, T., Barnett, M. D., Garcini, L. M., & Baker, J. (2009). Predictors of recent mental health service use in a medical population: Implications for integrated care. Journal of Clinical Psychology in Medical Settings, 16, 304–310.
Liebschutz, J., Saitz, R., Brower, V., Keane, T. M., Lloyd-Travaglini, C., Averbuch, T., et al. (2007). PTSD in urban primary care: High prevalence and low physician recognition. Journal of General Internal Medicine, 22, 719–726.
*Litz, B. T., Engel, C. C., Bryant, R. A., & Papa, A. (2007). A randomized, controlled proof-of-concept trial of an Internet-based, therapist-assisted self-management treatment for posttraumatic stress disorder. American Journal of Psychiatry, 164, 1676–1683.
Magruder, K. M., Frueh, B. C., Knapp, R. G., Davis, L., Hamner, M. B., Martin, R. H., et al. (2005). Prevalence of posttraumatic stress disorder in Veterans Affairs primary care clinics. General Hospital Psychiatry, 27, 167–179.
Martell, C. R., Addis, M. E., & Jacobson, N. S. (2001). Depression in context: Strategies for guided action. New York, NY: W W Norton & Co.
McDaniel, S. H., & LeRoux, P. (2007). An overview of primary care family psychology. Journal of Clinical Psychology in Medical Settings, 14, 23–32.
Morland, L. A., Freuh, C., Pierce, K., & Miyahira, S. (2003). PTSD and telemental health: Updates and future directions. National Center for PTSD Clinical Quarterly, 12, 1–5.
*Prins, A., Cimpean, D., & Schnurr, P. P. (2009). Treatment in primary care settings. In K. T. Mueser, S. D. Rosenberg, & H. J. Rosenberg (Eds.), Treatment of posttraumatic stress disorder in special populations: A cognitive restructuring program (pp. 301–314). Washington, DC: American Psychological Association.
Prins, A., Ouimette, P., Kimerling, R., Cameron, R. P., Hugelshofer, D. S., Shaw-Hegwer, J., et al. (2003). The Primary Care PTSD Screen (PC-PTSD): Development and operating characteristics. Primary Care Psychiatry, 9, 9–14.
Rauch, S. A., Morales, K. H., Zubritsky, C., Knott, K., & Oslin, D. (2006). Posttraumatic stress, depression, and health among older adults in primary care. American Journal of Geriatric Psychiatry, 14, 316–324.
Read, J. P., Brown, P. J., & Kahler, C. W. (2004). Substance use and posttraumatic stress disorders: Symptom interplay and effects on outcome. Addictive Behaviors, 29, 1665–1672.
Resnick, H., Acierno, R., Holmes, M., Dammeyer, M., & Kilpatrick, D. (2000). Emergency evaluation and intervention with female victims of rape and other violence. Journal of Clinical Psychology, 56, 1317–1333.
Robinson, P. J., Gregg, J., Dahl, J., & Lundgren, T. (2004). ACT in medical settings. In S. C. Hayes & K. Strosahl (Eds.), A practical guide to acceptance and commitment therapy (pp. 295–314). New York, NY: Springer.
Robinson, P. J., & Strosahl, K. D. (2009). Behavioral health consultation and primary care: Lessons learned. Journal of Clinical Psychology in Medical Settings, 16, 58–71.
*Roy-Burne, P., Craske, M. G., Sullivan, G., Rose, R. D., Edlund, M. J., Lang, A. J., et al. (2010). Delivery of Evidence-based treatment for multiple anxiety disorder in primary care. A randomized controlled trial. JAMA, 303, 1921–1928.
Sayer, N. A., Friedemann-Sanchez, G., Spoont, M., Murdoch, M., Parker, L. E., Chiros, C., et al. (2009). A qualitative study of determinants of PTSD treatment initiation in veterans. Psychiatry: Interpersonal and Biological Processes, 72, 238–255.
Seal, K. H., Maguen, S., Cohen, B., Gima, K. S., Metzler, T. J., Ren, L., et al. (2010). VA mental health services utilization in Iraq and Afghanistan veterans in the first year of receiving new mental health diagnoses. Journal of Traumatic Stress, 23, 5–16.
Spoont, M., Murdoch, M., Hodges, J., & Nugent, S. (2010). Treatment receipt by veterans after a PTSD diagnosis in PTSD, mental health, or general medical clinics. Psychiatric Services, 61, 58–63.
Stein, M. B., McQuaid, J. R., Pedrelli, P., Lenox, R., & McCahill, M. E. (2000). Posttraumatic stress disorder in the primary care medical setting. General Hospital Psychiatry, 22, 261–269.
Veterans Affairs/Department of Defense (VA/DoD). (2004). Acute stress disorder (ASD) and post-traumatic stress disorder (PTSD) in primary care. In VA/DoD clinical practice guideline for the management of post-traumatic stress (Module B). Retrieved from http://www.healthquality.va.gov/ptsd/ptsd_full.pdf.
Veterans Health Administration (VHA). (2008). VHA handbook 1160.01: Uniform mental health services in VA medical centers and clinics. Retrieved from http://www1.va.gov/vhapublications/ViewPublication.asp?pub_ID=1762.
*Wagner, A. W., Zatzick, D. F., Ghesquiere, A., & Jurkovich, G. J. (2007). Behavioral activation as an early intervention for posttraumatic stress disorder and depression among physically injured trauma survivors. Cognitive and Behavioral Practice, 14, 341–349.
Walser, R. D., & Westrup, D. (2007). Acceptance and commitment therapy for the treatment of post-traumatic stress disorder and trauma-related problems: A practitioner’s guide to using mindfulness and acceptance strategies. Oakland, CA: New Harbinger Publications.
Wilson, J. A. B., Onorati, K., Mishkind, M., Reger, M. A., & Gahm, G. A. (2008). Soldier attitudes about technology-based approaches to mental health care. Cyberpsychology and Behavior, 11, 767–769.
Yeager, D. E., Magruder, K. M., Knapp, R. G., Nicholas, J. S., & Frueh, B. C. (2007). Performance characteristics of the Posttraumatic Stress Disorder Checklist and SPAN in Veterans Affairs primary care settings. General Hospital Psychiatry, 29, 294–301.
*Zatzick, D., Roy-Byrne, P., Russo, J., Rivara, F., Droesch, R., Wagner, A., et al. (2004). A randomized effectiveness trial of stepped collaborative care for acutely injured trauma survivors. Archives of General Psychiatry, 61, 498–506.
Zlotnick, C., Rodriguez, B. F., Weisberg, R. B., Bruce, S. E., Spencer, M. A., Culpepper, L., et al. (2004). Chronicity in posttraumatic stress disorder and predictors of the course of posttraumatic stress disorder among primary care patients. Journal of Nervous and Mental Disease, 192, 153–159.
Acknowledgments
The author would like to thank Larry Lantinga, Ph.D. for his feedback and editorial expertise on this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Possemato, K. The Current State of Intervention Research for Posttraumatic Stress Disorder Within the Primary Care Setting. J Clin Psychol Med Settings 18, 268–280 (2011). https://doi.org/10.1007/s10880-011-9237-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10880-011-9237-4