
Abstract
Purpose
Patients with primary immunodeficiency diseases (PIDD) may present with recurrent infections affecting different organs, organ-specific inflammation/autoimmunity, and also increased cancer risk, particularly hematopoietic malignancies. The diversity of PIDD and the wide age range over which these clinical occurrences become apparent often make the identification of patients difficult for physicians other than immunologists. The aim of this report is to develop a tool for educative programs targeted to specialists and applied by clinical immunologists.
Methods
Considering the data from national surveys and clinical reports of experiences with specific PIDD patients, an evidence-based list of symptoms, signs, and corresponding laboratory tests were elaborated to help physicians other than immunologists look for PIDD.
Results
Tables including main clinical manifestations, restricted immunological evaluation, and possible related diagnosis were organized for general practitioners and 5 specialties. Tables include information on specific warning signs of PIDD for pulmonologists, gastroenterologists, dermatologists, hematologists, and infectious disease specialists.
Conclusions
This report provides clinical immunologists with an instrument they can use to introduce specialists in other areas of medicine to the warning signs of PIDD and increase early diagnosis. Educational programs should be developed attending the needs of each specialty.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Primary immunodeficiency diseases (PIDD) are a heterogeneous group of more than 150 disorders that result from many different congenital, or even acquired, genetic defects affecting the innate and adaptive immune systems [1, 2]. Despite major advances over the last 20 years in the clinical and molecular characterization of PIDD, many patients remain undiagnosed or have a substantially delayed diagnosis with adverse results on morbidity and mortality.
The diagnosis of PIDD is most often suggested by recurrent or unusual infections and inflammatory or autoimmune conditions. Several lists of warning signs for children or adults are based on these main clinical presentations and, in some cases, family history [3–6]. Arkwright and Gennery concluded that the 10 warning signs promoted by the Jeffrey Modell Foundation have a sensitivity of 56 % and a specificity of 16 % [7]. Subbarayan et al. evaluated 563 children and concluded that the strongest identifier of PIDD is family history. Of secondary relevance were the use of intravenous antibiotics for sepsis, and failure to thrive in children with T lymphocyte primary immunodeficiency disease [8]. Mehra et al. observed that 20 % of hospitalized patients with suspected immune defects would not be included for immunologic investigation according to the 10 warning signs [9].
All currently available lists of warning signs are based on family history and descriptions of infections suggestive of an immunodeficiency. These are general signs that should be known by all physicians. However, there are many specific warning signs that certain specialists need to be aware of. Because of the diversity of immune defects, their respective clinical presentations, and the difficulties in reaching many non-immunology subspecialists with these general warning signs, many signs that should raise suspicion of PIDD are missed by physicians and a large proportion of patients are not properly diagnosed [10–12].
Here, we provide lists of specific warning signs in tables that can be used to familiarize subspecialists with signs and symptoms of PIDD that they are likely to see in patients referred to their practices. The tables will provide quick summaries of the many warning signs and diagnoses encountered by different specialists, with suggestions for appropriate screenings, immunological evaluations, and proper referrals to clinical immunologists.
Methods
The information offered in this article is based on a review of the pertinent literature and the clinical experience of all authors. Tables I and II list the tests that are recommended for screening of the main immunologic functions, along with histories and infections that all physicians and health care workers need to recognize as warning signs of a possible immunodeficiency. Subsequent tables list special clinical presentations that should alert specific groups of specialists. When presenting information about PIDD from this article, it is important to always include Tables I and II, and the pertinent tables prepared for various specialties.
General Screening and Evaluation
Table I lists the tests that should be performed according to the main clinical presentations specified in the subsequent tables. In some situations the relevant evaluation is not part of generally available screening tests, and it is preferable to refer the patient directly to an immunologist so that routine and specialized tests can be performed simultaneously. The tables for specialists will provide data for further laboratory investigation.
Recurrent, Severe, or Unusual Infections
Our recommendations are similar to those in published lists of warning signs that consider the frequency of various types of infections. However, it is also important to consider the infection type, the circumstances under which infections occur, and which organs and tissues they affect. In our experience, this is a more effective way to identify PIDD than emphasizing exact numbers of different infections or special definitions of severity. When severity is considered, it is important to consider the pathogenicity of an infectious agent; infections with any pathogen of low pathogenicity, such as atypical mycobacteria or toxoplasma, are suggestive of an immune defect even if the infection is not severe. Epidemiological data about infectious agents should be considered as well. For example, paracoccidioidomycosis should be more commonly identified in tropical countries than in European or North American countries (Table II). A general condition that should make any infection suspicious is the concomitant presence of noninfectious complications commonly associated with PIDD, including severe allergy, autoimmunity, unregulated inflammation, or malignancies.
A positive family history definitely suggests a PIDD. However, it is also important to consider certain negative family histories—for example, a family in which only one of 4 siblings has recurrent infections. The fact that the other 3 siblings and parents are healthy rules out environmental factors as the factors predisposing an individual to recurrent infections; it also highlights the immunopathogenic effects of genetic alterations that may have occurred in a single family member.
Recurrent infections are often attributed to the presence of non-immune abnormalities, such as Down syndrome, muscular dystrophy, or various congenital heart defects. Such patients may also have an immunodeficiency, and appropriate recognition and treatment may significantly improve their quality of life.
Infectious Diseases
Many PIDDs have unique susceptibilities to some pathogens and/or sites of infections that are listed in Table III. Antibody-mediated immunity needs to be evaluated in all severe or unusual infections, in addition to other possible concurring immunological defects. A practical point is to screen for combined immunodeficiencies.
Infectious disease is the hallmark of PIDD, and infectious disease specialists are the physicians most likely to encounter patients with PIDD in their daily practice. The burden of infectious disease is immense even in children with healthy immune systems. Recurrent otitis media is considered to be more than 4 episodes of acute otitis media during the past 12 months with complete resolution of the disease between episodes [13–15].
Any patient with severe or recurrent infections or infection by opportunistic or uncommon microorganisms must be investigated for PIDD after discarding the possibility of infection with human immunodeficiency virus (HIV).
Pyogenic encapsulated bacteria (Streptococcus pneumoniae, Haemophilus influenzae) are frequently associated with infections in patients with antibody or complement deficiencies. Patients with complement deficiencies may also present with meningitis and sepsis associated with pathogens such as Neisseria [16].
Agammaglobulinemic patients and, to a lesser extent, patients with common variable immunodeficiency (CVID) have an increased risk of developing bloodstream bacterial infections [17]. A study of 201 patients with X-linked agammaglobulinemia (XLA) indicated that 11 % had at least one episode of meningitis or encephalitis, 10 % had at least one episode of sepsis, and 8 % had at least one episode of septic arthritis [18]. Patients with XLA or CVID are at an increased risk for severe and often fatal infections with enteroviruses, including echoviruses, polioviruses, and coxsackie viruses [17]. The central nervous system is nearly always involved in these infections, and evidence of systemic involvement of muscle, liver, and/or joints is present in about 40 % of patients. These infections are associated with high mortality and morbidity [19].
Other organisms, including Staphylococcus aureus, Pseudomonas spp, Mycoplasma spp, Enterobacteriaceae, Campylobacter spp, Giardia, and enteroviruses, may be isolated from patients with specific types of PIDD [17]. Infections caused by Serratia marcessens, Nocardia spp, Chrombacterium violaceum, Granulobacter bethesdensis, Burholderia cepacia, and gladioli are strongly suggestive of chronic granulomatous disease (CGD). Evaluation of 259 patients with the X-linked recessive form of CGD indicated that 21 % had a history of either bacteremia or fungemia [20].
Infections caused by mycobacteria, Salmonella, Leishmania, and Cryptococcus suggest defects in the interferon-γ/interleukin-12 axis included in innate immunity (Table III) [21]. As previously mentioned, the incidence of certain infectious agents must be considered according to their endemicity in particular geographical regions. Side effects of Bacillus Calmette-Guérin (BCG) occur in more than 50 % of the severe combined immunodeficiency (SCID) patients in Brazil and more than 17 % of CGD patients in Latin America; this is a relevant warning sign for PIDD [22]. Adverse reactions to other live attenuated viral vaccines such as poliovirus and rotavirus should be carefully observed as well [23]. Several developing countries maintain campaigns with Sabin immunization with the possibility to cause vaccine-derived disease [24].
Although the respiratory and gastrointestinal tracts are the most common systems for presenting illness, the authors observed lymphadenopathy as the most common manifestation in the group of combined T and B cell immunodeficiencies, and superficial abscesses and lymphadenopathy in the group of congenital defects of phagocyte number and/or function [22, 25, 26] (Table III).
Otorhinolaryngology and Pulmonology
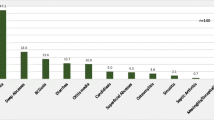
High percentages of pediatric and adult patients with PIDD have upper and/or lower respiratory tract bacterial infections; thus, they may be referred to otorhinolaryngologists or pulmonologists. Rezaei reported on 930 patients with PIDD, 353 cases of which were identified in the last 5 years. The most common presenting feature of PIDD was pneumonia, which was seen in 20.1 % of patients, followed by diarrhea (13.7 %), sinusitis (10.3 %), and otitis media (9.6 %) [27]. It is important to rule out the existence of cofactors that might be associated with upper respiratory infections (e.g., smoking, day care attendance, gastroesophageal reflux, allergy) before performing extensive immunological evaluation. The most common of these infections are recurrent otitis media, chronic sinusitis, and pneumonia. Recurrent sinus infections have been reported as a presenting occurrence in 19 % to 98 % of patients with PIDD (wide range reflects the variety of PIDD) [28, 29]. An assessment of 103 pediatric and adult patients with a history of recurrent or chronic ear, nose, or throat infections indicated that 16.5 % had defects in antibody-mediated immunity: CVID (n = 2), IgA deficiency (n = 4), IgG subclass deficiency (n = 3), and specific antibody deficiency against polysaccharide antigens (n = 8) [30]. Warning signs for patients with recurrent otitis include progressive infections leading to mastoiditis; associated abscesses or systemic infections; lack of responsiveness to adequate antibiotic treatment; or occurrence of unusual, severe, or frequently relapsing infections in other sites [31] (Table II).
Pneumonia is a common infectious manifestation of PIDD; one study of patients with CVID indicated that at least two-thirds had one or more pneumonia diagnoses prior to diagnosis of PIDD [32]. According to some registries [33, 34], approximately 50 % of patients with humoral immunodeficiency suffered from upper respiratory tract infections, and 40 % of XLA and CVID patients suffered from recurring pneumonia [27, 35]. Pathogens frequently associated with pneumonia in patients with antibody deficiencies include S pneumoniae, H influenzae type b, Haemophilus parainfluenzae, Mycoplasma spp, Pseudomonas spp, and Staphylococcus spp [17]. Patients with cellular deficiencies such as CD40 Ligand (CD40L) deficiency present with pneumonia that is a result of opportunistic pathogens such as Pneumocystis, fungal, or viral infections [36] (Table IV).
Several observational studies have indicated that complications and sequelae of infectious diseases such as bronchiectasis (76 %), recurrent chest infections (21 %), and granulomatous lung disease (5 %) should also raise suspicion of PIDD [37]. A systematic review of the literature conducted by Wood et al. included results from 7 surveys showing that respiratory/chest infections were presenting symptoms for 37 % to 90 % of patients with PIDD [29]. Touw et al. reviewed 26 studies that included 587 patients with CVID and found that up to 73 % developed chronic structural pulmonary complications—most often bronchiectasis and bronchial wall thickening [38]. In another study, pulmonary imaging by chest computed tomography in 30 patients with PIDD revealed abnormalities in 53 %; among these were bronchiectasis (75 %), peribronchial thickening (19 %), air trapping (31 %), lung volume reduction (25 %), atelectasis (12 %), follicular bronchiolitis (12 %), ground-glass abnormality (12 %), and parenchyma nodules (6 %). In this study, pulmonary function testing also indicated abnormalities in 18 patients; these included an obstructive (38.8 %), restrictive (44.4 %), or mixed (16.7 %) pattern of lung function abnormalities [39].
Results from other studies have indicated that Staphylococcus-associated pneumonia and bronchial aspergillosis [40] are seen in CGD; lung abscesses represent usual characteristics in hyper IgE syndrome (HIES); and interstitial pneumonia may be observed in patients with SCID [41] (Table IV).
Gastroenterology
Frequent gastrointestinal manifestations are malabsorption, diarrhea, hepatomegaly, and inflammatory bowel disease (IBD) and all of these are commonly associated with increased morbidity [42–44]. In a systematic review, Wood et al. indicated that GI infections were a presenting symptom in 6 % to 19 % of patients with PIDD [29]. Severe diarrhea can start early in life in patients with SCID or immunodysregulation, polyendocrinopathy, and enteropathy, X-linked (IPEX); both of these PIDD are considered pediatric emergencies [45–47]. Rezei et al., in their study of 930 patients with PIDD, indicated that infectious diarrhea occurred in 40.4 % of patients [27]. Recurrent or chronic giardiasis is suggestive of an underlying antibody deficiency [17]. Other pathogens in patients with infectious colitis include rotavirus, Campylobacter, enteroviruses, Cryptosporidium parvum, Salmonella spp, and Clostridium difficile [18]. Liver abscesses caused mainly by S aureus may also be seen in patients with CGD and HIES (Table V).
Results from a study focusing mainly on pediatric patients with PIDD indicated clinical evidence of liver disease, including hepatomegaly, in 35.5 %; 8 patients (13 %) had clinical and/or laboratory evidence of chronic liver disease. Hepatobiliary infection, sclerosing cholangitis, nodular regenerative hyperplasia, and portal hypertension are frequent conditions in CD40L deficiency [48, 49].
Rheumatology
The risk for autoimmune diseases is elevated in patients with PIDD and is sometimes the only clinical manifestation of their causative condition. Results from a larger study of 248 patients with CVID indicated that 69 (27.8 %) had autoimmune disease. The most common conditions were thrombocytopenia in 18 patients, hemolytic anemia in 12, rheumatoid arthritis in 5, and juvenile rheumatoid arthritis in 4 [50, 51]. Results from another study of 189 patients with systemic lupus erythematosus (SLE) indicated that 6 % had IgA deficiency [52].
Other PIDD are the result of genetic defects that lead to immune dysregulation associated with autoimmune occurrences. Patients with autoimmune lymphoproliferative syndrome (ALPS) develop generalized lymphadenopathy, hepatosplenomegaly, hypergammaglobulinemia, B cell lymphocytosis, and autoimmune manifestations that commonly include hemolytic anemia, glomerulonephritis, and idiopathic thrombocytopenic purpura [53]. Autoimmune polyendocrinopathy, candidiasis, and ectodermal dystrophy (APECED) are also associated with symptoms of autoimmune disease [54]. Patients with IPEX have mutations in the FOXP3 gene in regulatory T cells, which leads to severe autoimmunity with a high mortality rate [55]. First components of complement deficiency have also been shown to be associated with conditions such as SLE and are likely to prompt referral to a rheumatologist [56]. An important “red flag” for SLE and complement defects is negative serology to double-stranded DNA [57].
Bone and joint abnormalities can occur in patients with PIDD. The most common of these is arthritis, which may be associated with antibody deficiencies, and, less often, with CGD and Wiskott-Aldrich syndrome (WAS) [58, 59]. Importantly, infections with Ureaplasma urealyticum, and Mycoplasma ssp may lead to erosive arthritis in patients with severe antibody deficiencies. These infections most often result in large-joint monoarthritis involving the knee, shoulder, elbow, or hip joints, and less often in symmetrical polyarthritis [17].
Patients with certain PIDD, such as autoinflammatory syndromes, will present with generalized serositis that might be confused with infectious arthritis. This is often accompanied by a myriad of symptoms, including elevation of acute phase reactants, rash, deafness, joint deformity, and multifocal osteomyelitis [60].
Dermatology
Patients with PIDD may have skin conditions including fungal, bacterial, or viral infections; eczematous dermatitis; erythroderma; skin symptoms of autoimmune diseases such as SLE or scleroderma; vasculitis; granuloma formation; and/or problems characteristic of specific immunodeficiency syndromes (e.g., telangiectasia, gray hair, and depigmentation) [61]. An immunological assessment of 382,383 pediatric patients admitted to an outpatient dermatology group indicated that 130 had PIDD. Of these, 69 % had skin infections, 29 % had eczema-dermatitis, and 44 % had other associated cutaneous conditions. In 79 % of this cohort, cutaneous abnormalities preceded and were the basis for the clinical immunologic diagnosis [62], demonstrating the relevance and high frequency of dermatologic manifestations in PIDD patients.
Results from a cross-sectional study of 210 pediatric patients with PIDD (68 with antibody deficiencies, 22 with T cell and combined deficiencies, 57 with phagocytic defects, and 63 with other PIDD) indicated that 67 of the patients (31.9 %) had cutaneous abnormalities preceding the diagnosis of PIDD. Overall, 99 patients had infections and 27 had eczematous dermatitis [63].
Candida infections that may be among the first signs of PIDD include mucocutaneous candidiasis, Candida paronychia, granuloma formation, and erythroderma [64]. Patients with phagocytic, cellular, combined, and other PIDD exhibit immune deficits that confer increased susceptibility to fungal infections. Infections associated with Candida, Aspergillus, Cryptococcus, Histoplasma, Paecilomyces, Scedosporium, Trichosporon, Penicillium, and other fungal organisms have been observed in patients with CGD, SCID, HIES, defects in the interferon-γ/interleukin-12 axis, DiGeorge syndrome/22q deletion syndrome, CD40L deficiency, WAS, and CVID [64]. Patients with Chediak-Higashi or Griscelli syndromes present partial albinism and gray hair; dermatologists are frequently the first consulted specialists [65]. Prompt diagnosis is established by demonstration of giant intracellular granules in eosinophils, basophils, and monocytes, and are pathognomonic of this disease [66].
Eczema and high serum IgE levels in the first months of life frequently lead to referral to allergists due to suspicion of cow milk protein allergy. However, these occurrences are also present in patients with hypomorphic SCID, IPEX, WAS, DOCK8, and HIES [67]; it has been shown that differential diagnosis is crucial for prognosis [68]. Zhang et al. described DOCK8 mutations in patients with a variant of combined immunodeficiency characterized by unusual susceptibility to cutaneous viral infections and cancers. In addition, DOCK8 deficiency was found in a subgroup of patients who were previously thought to have autosomal recessive HIES with severe allergic manifestations [69]. These syndromes exemplify the need for improved knowledge of PIDD for dermatologists (Table VI). In addition, angioedema without urticaria is often referred to both allergists and dermatologists. Family histories are helpful for such cases, and C4 levels could be a useful screening test [70].
Hematology/Oncology
Autoimmune hemolytic anemia, thrombocytopenia, and/or neutropenia are also seen in patients with selective IgA deficiency, CVID, and class switch recombination (CSR) defects [50, 71]. In some patients, hematologic abnormalities reflect the underlying pathology responsible for the immunodeficiency. Wiskott-Aldrich syndrome is associated with defects in both B-lymphocyte and T-lymphocyte function, and these patients also have intrinsic platelet abnormalities and significant thrombocytopenia with small platelets [71]. In addition to congenital neutropenia, neutropenia is also associated with XLA, CD40L deficiency, CVID, SCID, and Shwachman-Diamond syndrome [72, 73]. Hemophagocytic lymphohistiocytosis (HLH) is characterized by multisystem inflammation, a reactive process resulting from hyperactivation of macrophages, histiocytes and CD8+ T cells, and abnormalities in the function of natural killer cells (NK cells). The most frequent clinical and laboratorial findings include fever, splenomegaly, cytopenias, hypertriglyceridemia, and elevated ferritin [74]. Both Chediak-Higashi and Griscelli syndromes present as hemophagocytic, with an accelerated phase affecting all patients by late childhood. This accelerated phase is characterized by the infiltration of nonmalignant lymphoid and histiocytoid cells into the viscera, usually induced by Epstein-Barr virus. Clinical findings include hepatosplenomegaly, lymphadenopathy, and pancytopenia [75]. Impaired humoral and cellular immune responses, including disturbances in B, T, NK, and dendritic cells, along with chronic inflammatory autoimmune diseases, recurrent bacterial infections, and persistent antigenic stimulation, are speculated to favor carcinogenesis in CVID patients. Lymphoma and gastric cancer are the most frequent neoplasms related to this immunologic defect [76, 77]. The risk of cancer in PIDD patients mainly takes the form of T cell malignancies (70-fold and 250-fold increased risks of leukemia and lymphoma, respectively), and B cell malignancies are high when compared with the general population [78]. The Spanish registry identified that 1.3 % of the 1,069 patients developed cancer; however, the survey was developed within reference hospitals [34].
Non-Hodgkin lymphoma and Hodgkin lymphoma are 2 of the most common PIDD-associated malignancies [79]. A recent large-scale assessment of 1,132 patients in the PIDD registry of the Australasian Society of Clinical Immunology and Allergy indicated that this group had a 1.6-fold excess relative risk of cancer [80]. The relative risk was significantly increased for non-Hodgkin lymphoma, leukemia, and stomach cancer (Table VII).
Conclusions
During recent years, new PIDD have been identified, including some with susceptibility to specific infectious agents and some diagnosed only in adulthood. Training specialists to recognize PIDD is important in order to identify the diverse PIDD phenotypes. The majority of patients initially present to hospital doctors; therefore, a focus on hospital specialists has been suggested.
Clinical immunologists have an important educational role. Introducing other specialists and health care workers to the relevant warning signs will facilitate the early diagnosis of PIDD in patients, leading to better treatments with less sequelae, or possible cures.
In this review we have addressed the presentations of PIDD that are seen by different medical subspecialists. These warning signs are further influenced by the socioeconomic, climate-related, and living conditions found in different regions of the world. A review of warning signs that are specific to different areas of the world should eventually be undertaken by a worldwide PIDD community of which LASID plays an important part.
Abbreviations
- ALPS:
-
Autoimmune lymphoproliferative syndrome
- ANA:
-
Antinuclear antibodies
- AP50:
-
Alternative pathway of complement system
- APECED:
-
Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy
- C1INH:
-
C1 esterase inhibitor
- CBC:
-
Complete blood count
- CD40L:
-
CD40 ligand (L) deficiency
- CGD:
-
Chronic granulomatous disease
- CSR:
-
Class switch recombination
- CVID:
-
Common variable immunodeficiency
- DHR:
-
Dihydrorhodamine
- EBNA:
-
Epstein-Barr nuclear antigen
- FHL:
-
Familial hemophagocytic lymphohistiocytosis
- HAE:
-
Hereditary angioedema
- HIES:
-
Hyper-IgE syndrome
- HLH:
-
Hemophagocytic lymphohistiocytosis
- IPEX:
-
Immunodysregulation, polyendocrinopathy and enteropathy, X-linked
- OPV:
-
Oral poliovirus vaccine
- RCP:
-
Reactive C protein
- SCID:
-
Severe combined immunodeficiency
- SLE:
-
Systemic lupus erythematosus
- TSH:
-
Thyroid-stimulating hormone
- WAS:
-
Wiskott-Aldrich syndrome
- WHIM:
-
Warts, hypogammaglobulinemia, infections, and myelokathexis syndrome
- XLA:
-
X-linked agammaglobulinemia
- XLP:
-
X-linked lymphoproliferative syndrome
References
Arason GJ, Jorgensen GH, Ludviksson BR. Primary immunodeficiency and autoimmunity: lessons from human diseases. Scand J Immunol. 2010;71:317–28.
Al-Herz W, Bousfiha A, Casanova JL, Chapel H, Conley ME, Cunningham-Rundles C, et al. Primary immunodeficiency diseases: an update on the classification from the International Union of Immunological Societies Expert Committee for Primary Immunodeficiency. Front Immunol. 2011;2:54.
Jeffrey Modell Foundation. 10 Warning Signs [2013-01-30]. Available from: http://www.info4pi.org/aboutPI/index.cfm?section=aboutPI&content=warningsigns. Accessed 22 May 2013.
European Society for Immunodeficiencies. 10 Warning Signs of PID-General [2013-01-30]. Available from: http://www.esid.org/clinical-10-warning-signs-of-pid-general-339-0. Accessed 22 May 2013.
US Immunodeficiency Network. Disease Registry [1992]. Available from: http://www.usidnet.org/pub/Disease-Registry. Accessed 22 May 2013.
Immune Deficiency Foundation. About Primary Immunodeficiency Diseases. Available from: http://primaryimmune.org/about-primary-immunodeficiency-diseases. Accessed 22 May 2013.
Arkwright PD, Gennery AR. Ten warning signs of primary immunodeficiency: a new paradigm is needed for the 21st century. Ann NY Acad Sci. 2011;1238:7–14.
Subbarayan A, Colarusso G, Hughes SM, Gennery AR, Slatter M, Cant AJ, et al. Clinical features that identify children with primary immunodeficiency diseases. Pediatrics. 2011;27:810–6.
Mehra A, Sidi P, Doucette J, Rouvelas H, Cunningham-Rundles C. Subspecialty evaluation of chronically ill hospitalized patients with suspected immune defects. Ann Allergy Asthma Immunol. 2007;99:14.
Shearer WT, Cunningham-Rundles C, Ochs HD. Primary immunodeficiency: looking backwards, looking forwards. J Allergy Clin Immunol. 2004;113(4):607–9.
Buckley RH. Primary immunodeficiency or not? Making the correct diagnosis. J Allergy Clin Immunol. 2006;117(4):756–8.
Ballow M, Notarangelo L, Grimbacher B, Cunningham Rundles C, Stein M, Helbert M, et al. Immunodeficiencies. Clin Exp Immunol. 2009;158:14–22.
Pichichero ME, Casey JR. Otitis media. Expert Opin Pharmacother. 2002;3:1073–90.
Benninger MS, Ferguson BJ, Hadley JA, Hamilos DL, Jacobs M, Kennedy DW, et al. Adult chronic rhinosinusitis: definitions, diagnosis, epidemiology, and pathophysiology. Otolaryngol Head Neck Surg. 2003;129(3 Suppl):S1–32.
von Linstow ML, Holst KK, Larsen K, Koch A, Andersen PK, Høgh B. Acute respiratory symptoms and general illness during the first year of life: a population-based birth cohort study. Pediatr Pulmonol. 2008;43(6):584–93.
Grimnes G, Beckman H, Lappegård KT, Mollnes TE, Skogen V. Recurrent meningococcal sepsis in a presumptive immunocompetent host shown to be complement C5 deficient—a case report. APMIS. 2011;119:479–84.
Fried AJ, Bonilla FA. Pathogenesis, diagnosis, and management of primary antibody deficiencies and infections. Clin Microbiol Rev. 2009;22:396–414.
Winkelstein JA, Marino MC, Lederman HM, Jones SM, Sullivan K, Burks AW, et al. X-linked agammaglobulinemia: report on a United States registry of 201 patients. Medicine (Baltimore). 2006;85:193–202.
Halliday E, Winkelstein J, Webster AD. Enteroviral infections in primary immunodeficiency (PID): a survey of morbidity and mortality. J Infect. 2003;46:1–8.
Winkelstein JA, Marino MC, Johnston Jr RB, Boyle J, Curnutte J, Gallin JI, et al. Chronic granulomatous disease. Report on a national registry of 368 patients. Medicine (Baltimore). 2000;79:155–69.
de Beaucoudrey L, Samarina A, Bustamante J, Cobat A, Boisson-Dupuis S, Feinberg J, et al. Revisiting human IL-12Rβ1 deficiency: a survey of 141 patients from 30 countries. Medicine (Baltimore). 2010;89:381–402.
Mazzucchelli JL, Buzolin M, Vilela MS, Moraes LL, Porto Neto AC, Monteiro FP, et al. Severe combined immunodeficiency in Brazil: a multi-center analysis of demographics; clinical features regarding BCG infection and outcome in 33 patients. J Clin Immunol. 2011;31 Suppl 1:S1–71.
Patel MM, Lopez-Collada R, Bulhões MM, De Oliveira LH, Marquez AB, Fannery B, et al. Intussusception risk and benefits of rotavirus vaccination in Mexico and Brazil. N Engl J Med. 2011;364:2283–92.
Gumede N, Muthambi V, Schoub BD. Immunodeficiency-associated vaccine-derived poliovirus type 3 in infant, South Africa, 2011. Emerg Infect Dis. 2012;18(6):992–4.
Condino-Neto A, Oleastro M. Phenotype and genotype spectrum of chronic granulomatous disease in Latin American patients: results from the LASID Registry. J Clin Immunol. 2012;32 Suppl 1:S188.
Woellner C, Gertz EM, Schäffer AA, Lagos M, Perro M, Glocker EO, et al. Mutations in STAT3 and diagnostic guidelines for hyper-IgE syndrome. J Allergy Clin Immunol. 2010;125(2):424–32.
Rezaei N, Aghamohammadi A, Moin M, Pourpak Z, Movahedi M, Gharagozlou M, et al. Frequency and clinical manifestations of patients with primary immunodeficiency disorders in Iran: update from the Iranian Primary Immunodeficiency Registry. J Clin Immunol. 2006;26:519–32.
Richtsmeier WJ. Top 10 reasons for endoscopic maxillary sinus surgery failure. Laryngoscope. 2001;111:1952–6.
Wood P, Stanworth S, Burton J, Jones A, Peckham DG, Green T, et al. Recognition, clinical diagnosis and management of patients with primary antibody deficiencies: a systematic review. Clin Exp Immunol. 2007;149:410–23.
Aghamohammadi A, Moin M, Karimi A, Naraghi M, Zandieh F, Isaeian A, et al. Immunologic evaluation of patients with recurrent ear, nose, and throat infections. Am J Otolaryngol. 2008;29:385–92.
Urschel S. Otitis media in children with congenital immunodeficiencies. Curr Allergy Asthma Rep. 2010;10:425–33.
Cunningham-Rundles C, Bodian C. Common variable immunodeficiency: clinical and immunological features of 248 patients. Clin Immunol. 1999;92:34–48.
Ryser O, Morell A, Hitzig WH. Primary immunodeficiencies in Switzerland: first report of the national registry in adults and children. J Clin Immunol. 1988;8:479–85.
Matamoros Florí N, Mila Llambi J, Español Boren T, Raga Borja S, Fontan CG. Primary immunodeficiency syndrome in Spain: first report of the National Registry in Children and Adults. J Clin Immunol. 1997;17:333–9.
Aghamohammadi A, Moein M, Farhoudi A, Pourpak Z, Rezaei N, Abolmaali K, et al. Primary immunodeficiency in Iran: first report of the National Registry of PID in Children and Adults. J Clin Immunol. 2002;22:375–80.
Winkelstein JA, Marino MC, Ochs H, Fuleihan R, Scholl PR, Geha R, et al. The X-linked hyper-IgM syndrome: clinical and immunologic features of 79 patients. Medicine (Baltimore). 2003;82:373–84.
Thickett KM, Kumararatne DS, Banerjee AK, Dudley R, Stableforth DE. Common variable immune deficiency: respiratory manifestations, pulmonary function and high-resolution CT scan findings. QJM. 2002;95:655–62.
Touw CM, van de Ven AA, de Jong PA, Terheggen-Lagro S, Beek E, Sanders EA, et al. Detection of pulmonary complications in common variable immunodeficiency. Pediatr Allergy Immunol. 2010;21:793–805.
Costa-Carvalho BT, Wandalsen GF, Pulici G, Aranda CS, Solé D. Pulmonary complications in patients with antibody deficiency. Allergol Immunopathol (Madr). 2011;39:128–32.
Jones LB, McGrogan P, Flood TJ, Gennery AR, Morton L, Thrasher A, et al. Special article: chronic granulomatous disease in the United Kingdom and Ireland: a comprehensive national patient-based registry. Clin Exp Immunol. 2008;152:211–8.
Woodsford MA, Spencer DA, Cant AJ. Immune deficiency and the lung. Paediat Child Health. 2011;21:213–8.
Agarwal S, Mayer L. Gastrointestinal manifestations in primary immune disorders. Inflamm Bowel Dis. 2010;16:703–11.
Al-Muhsen SZ. Gastrointestinal and hepatic manifestations of primary immune deficiency diseases. Saudi J Gastroenterol. 2010;16:66–74.
Guerrerio AL, Frischmeyer-Guerrerio PA, Lederman HM, Oliva-Hemker M. Recognizing gastrointestinal and hepatic manifestations of primary immunodeficiency diseases. J Pediatr Gastroenterol Nutr. 2010;51:548–55.
Carneiro-Sampaio M, Jacob CM, Leone CR. A proposal of warning signs for primary immunodeficiencies in the first year of life. Pediatr Allergy Immunol. 2011;22:345–6.
Harbuz R, Lespinasse J, Boulet S, Francannet C, Creveaux I, Benkhelifa M, et al. Identification of new FOXP3 mutations and prenatal diagnosis of IPEX syndrome. Prenat Diagn. 2010;30:1072–8.
Ozdemir O. Severe combined immune deficiency in an adenosine deaminase deficient patient. Allergy Asthma Proc. 2006;27:172–4.
Malamut G, Ziol M, Suarez F, Beaugrand M, Viallard JF, Lascaux AS, et al. Nodular regenerative hyperplasia: the main liver disease in patients with primary hypogammaglobulinemia and hepatic abnormalities. J Hepatol. 2008;48(1):74–82.
Motamed F, Aghamohammadi A, Soltani M, Mansouri M, Rezaei N, Teimourian S, et al. Evaluation of liver diseases in Iranian patients with primary antibody deficiencies. Ann Hepatol. 2009;8:196–202.
Cunningham-Rundles C. Hematologic complications of primary immune deficiencies. Blood Rev. 2002;16:61–4.
Michel M, Chanet V, Galicier L, Ruivard M, Levy Y, Hermine O, et al. Autoimmune thrombocytopenic purpura and common variable immunodeficiency: analysis of 21 cases and review of the literature. Medicine (Baltimore). 2004;83:254–63.
Mantovani AP, Monclaro MP, Skare TL. Prevalence of IgA deficiency in adult systemic lupus erythematosus and the study of the association with its clinical and autoantibody profiles. Rev Bras Reumatol. 2010;50:273–82.
Desai NK, Morkhandikar S, Bajpai S, Pazare AR. Autoimmune lymphoproliferative disorder in an adult patient. J Postgrad Med. 2011;57:131–3.
Lankisch TO, Jaeckel E, Strassburg CP. The autoimmune polyendocrinopathycandidiasis-ectodermal dystrophy or autoimmune polyglandular syndrome type 1. Semin Liver Dis. 2009;29:307–14.
Michels AW, Gottlieb PA. Autoimmune polyglandular syndromes. Nat Rev Endocrinol. 2010;6:270–7.
Jesus AA, Liphaus BL, Silva CA, Bando SY, Andrade LE, Coutinho A, et al. Complement and antibody primary immunodeficiency in juvenile systemic lupus erythematosus patients. Lupus. 2011;20:1275–84.
American College of Rheumatology Ad Hoc Committee on Immunologic Testing Guidelines. Guidelines for immunologic laboratory testing in the rheumatic diseases: an introduction. Arthritis Rheum. 2002;47(4):429–33.
Machado P, Santos A, Faria E, Silva J, Malcata A, Chieira C. Arthritis and X linked agammaglobulinemia. Acta Reumatol Port. 2008;33:464–7.
Sordet C, Cantagrel A, Schaeverbeke T, Sibilia J. Bone and joint disease associated with primary immune deficiencies. Joint Bone Spine. 2005;72:503–14.
Goldbach-Mansky R, Kastner DL. Autoinflammation: the prominent role of IL-1 in monogenic autoinflammatory diseases and implications for common illnesses. J Allergy Clin Immunol. 2009;124:1141–9.
Sillevis Smitt JH, Wulffraat NM, Kuijpers TW. The skin in primary immunodeficiency disorders. Eur J Dermatol. 2005;15:425–32.
Berron-Ruiz A, Berron-Perez R, Ruiz-Maldonado R. Cutaneous markers of primary immunodeficiency diseases in children. Pediatr Dermatol. 2000;17:91–6.
Moin A, Farhoudi A, Moin M, Pourpak Z, Bazargan N. Cutaneous manifestations of primary immunodeficiency diseases in children. Iran J Allergy Asthma Immunol. 2006;5:121–6.
Antachopoulos C, Walsh TJ, Roilides E. Fungal infections in primary immunodeficiencies. Eur J Pediatr. 2007;166:1099–117.
Valente NYS, Machado MCMR, Boggio P, Alves ACF, Bergonse FN, Casella E, et al. Polarized light microscopy of hair shafts aids in the differential diagnosis of Chédiak-Higashi and Griscelli-Prunieras syndromes. Clinics. 2006;61:327–32.
Huizing M, Helip-Wooley A, Westbroek W, Gunay-Aygun M, Gahl WA. Disorders of lysosome-related organelle biogenesis: clinical and molecular genetics. Annu Rev Genomics Hum Genet. 2008;9:359–86.
Ozcan E, Notarangelo LD, Geha RS. Primary immune deficiencies with aberrant IgE production. J Allergy Clin Immunol. 2008;122:1054–62.
Bezrodnik L, Raccio AC, Canil LM, Rey MA, Carabajal PC, Fossati CA, et al. Hypogammaglobulinaemia secondary to cow-milk allergy in children under 2 years of age. Immunology. 2007;122:140–6.
Zhang Q, Davis JC, Ian MPH, Lamborn T, Freeman AF, Jing H, et al. Combined immunodeficiency associated with DOCK8 mutations. N Engl J Med. 2009;361:2046–55.
Bowen T, Cicardi M, Farkas H, Bork K, Longhurst HJ, Zuraw B, et al. 2010 International consensus algorithm for the diagnosis, therapy and management of hereditary angioedema. Allergy Asthma Clin Immunol. 2010;6:24.
Immune Deficiencies Foundation of New Zealand. The clinical presentation of the primary immunodeficiency diseases a primer for physicians. In: Immune Deficiencies Foundation of New Zealand;1993. Available from: http://www.idfnz.org.nz/pub/cms/resources__medical/files/GPPRIM1.pdf. Accessed 28 May 2013.
Cabral-Marques O, Schimke LF, Pereira PV, Falcai A, de Oliveira JB, Hackett MJ, et al. Expanding the clinical and genetic spectrum of human CD40L deficiency: the occurrence of paracoccidioidomycosis and other unusual infections in Brazilian patients. J Clin Immunol. 2012;32:212–20.
Rezaei N, Farhoudi A, Pourpak Z, Aghamohammadi A, Moin M, Movahedi M, et al. Neutropenia in Iranian patients with primary immunodeficiency disorders. Haematologica. 2005;90:554–6.
Filipovich AH. Hemophagocytic lymphohistiocytosis and related disorders. Curr Opin Allergy Clin Immunol. 2006;6:410–5.
Abrams M, Paller A. Genetic immunodeficiency diseases. Adv Dermatol. 2007;23:197–229.
Rezaei N, Hedayat M, Aghamohammadi A, Nichols KE. Primary immunodeficiency diseases associated with increased susceptibility to viral infections and malignancies. J Allergy Clin Immunol. 2011;127:1329–41.
Chua I, Quinti I, Grimbacher B. Lymphoma in common variable immunodeficiency: interplay between immune dysregulation, infection and genetics. Curr Opin Hematol. 2008;15:368–74.
Regueiro JR, Porras O, Lavin M. Ataxia-telangiectasia. A primary immunodeficiency revisited. Immunol Allergy Clin North Am. 2000;20:177–206.
Shapiro RS. Malignancies in the setting of primary immunodeficiency: implications for hematologists/oncologists. Am J Hematol. 2011;86:48–55.
Vajdic CM, Mao L, van Leeuwen MT, Kirkpatrick P, Grulich AE, Riminton S. Are antibody deficiency disorders associated with a narrower range of cancers than other forms of immunodeficiency? Blood. 2010;116:1228–34.
Acknowledgments
The authors would like to acknowledge the Jeffrey Modell Foundation for their support of educational programs in Latin America. We also acknowledge the editorial assistance of BSG Communications, which is supported by Baxter.
Support
This work was supported by the Latin American Society of Primary Immunodeficiencies through an unrestricted educational grant from Baxter Bioscience.
Conflicts of interest and funding sources
Dr. Grumach is on the advisory board of Baxter, Shire, and Dyax Pharmaceuticals, has consulted for and received grants, payments, and travel support from Shire, and has received travel expenses from CSL Behring. Dr. Franco is a board member and consultant for and has received payments and travel support from Baxter. Dr. Condino-Neto has received research grants from Fundacao de Amparo a Pesquisa do Estado de São Paulo, Conselho Nacional de Desenvolvimento Científico e Tecnológico, Brazil, and Baxter Bioscience Research Grants. The other authors had nothing to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
Beatriz Tavares Costa-Carvalho and Anete Sevciovic Grumach contributed equally
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Costa-Carvalho, B.T., Grumach, A.S., Franco, J.L. et al. Attending to Warning Signs of Primary Immunodeficiency Diseases Across the Range of Clinical Practice. J Clin Immunol 34, 10–22 (2014). https://doi.org/10.1007/s10875-013-9954-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-013-9954-6