
Abstract
Background
Cardiac-specific markers of myocardial injury, such as troponin I (TnI), are often elevated following procedures that stimulate the myocardium. This study aimed to determine the effect of synchronized direct current (DC) cardioversion of atrial arrhythmias on myocardial injury 6-h post-procedure, as measured by cardiac TnI in patients with and without cardiomyopathy.
Methods
Seventy-three individuals (59 M:14 F) participated in this study. Inclusion criteria were subjects 18 and older undergoing DC cardioversion for an atrial arrhythmia, including elective and non-elective admissions. Exclusion criteria included MI or CABG within the past month, cardioversion for a ventricular arrhythmia, or recent shock by implantable internal cardioverter defibrillator. Patients underwent standard DC cardioversion procedure with blood work (TnI and CRP) prior to and 6-h post-cardioversion. Primary outcome was change in TnI. Secondary outcomes included changes in CRP, correlation of TnI with cumulative energy and LVM, and a sub-group analysis in patients with cardiomyopathy.
Results
There was no significant change in TnI following cardioversion (20.4 ± 7.9 vs. 17.5 ± 6.5 ng/L, F(1,72) = 2.651, p = 0.108). When stratified by cardiomyopathy status, there was a statistically significant reduction in TnI following cardioversion in the non-cardiomyopathy group (6.7 ± 3.7 ng/L vs. 6.2 ± 3.2 ng/L, F(1,58) = 6.481, p = 0.014) and a clinically significant reduction in the cardiomyopathy group (74.4 ± 136.7 ng/L vs. 54.6 ± 104.3 ng/L, F(1,13) = 3.676, p = 0.07). There was no significant relationship between change in TnI and cumulative energy or LVM (r = 0.137, p = 0.306 and r = 0.125, p = 0.412 respectively).
Conclusions
Synchronized DC cardioversion of an atrial arrhythmia did not cause myocardial injury 6-h post-cardioversion. Sub-group analysis suggests that cardioversion of patients with cardiomyopathy may result in normalization of TnI levels.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
It is widely accepted that the cardiac-specific enzymes troponin T and I are highly specific markers of myocardial injury. These enzymes have been shown to be elevated during acute coronary syndromes such as myocardial infarction, acute heart failure, pulmonary embolism, infectious conditions of the heart including myocarditis and pericarditis, sepsis, and with cardiomyopathies [1,2,3,4]. There is also evidence to suggest that atrial arrhythmias can cause myocardial injury as indicated by elevations in both C-reactive protein (CRP) and cardiac troponin T [5, 6].
Of the various types of atrial arrhythmias, atrial fibrillation is the most common and recent evidence suggests an increasing prevalence and incidence of atrial fibrillation worldwide [7, 8]. Advances in electrophysiological procedures have resulted in external synchronized electrical direct current (DC) cardioversion becoming the gold standard treatment for atrial arrhythmias [9]. While other procedures that stimulate the myocardium, such as percutaneous coronary intervention, coronary artery bypass grafting, and pulmonary vein embolization, have been shown to create an inflammatory response, as represented by an increase in circulatory inflammatory and serum cardiac markers [10, 11]; there is limited data on the acute incidence of myocardial injury following the external DC cardioversion.
Previous studies in animals have suggested that electrical cardioversion can cause myocardial injury [12]. However, these studies did not look directly at biochemical markers of myocardial injury. Additionally, it is unknown whether the energy levels used for cardioversion in animal models correspond to those used in humans. In humans, several clinical studies have attempted to characterize the changes in cardiac troponin I (TnI) following cardioversion; however, the results are conflicting [13,14,15,16]. Additionally, some of the data from these studies were collected following the use of a monophasic defibrillator, which has also been shown to cause greater myocardial injury when compared with the current gold standard biphasic defibrillators [13, 17]. A recent study investigating the effects of DC cardioversion on myocardial injury as measured by cardiac troponin T showed no significant changes following cardioversion [18]; however, these results have not been repeated using TnI.
In addition to atrial arrhythmias, there is evidence to suggest that patients with cardiomyopathy have elevated cardiac troponins [19]. The pathophysiology of this troponin release has been described as myocardial necrosis and myocardial apoptosis leading to ventricular remodeling and further impairment of systolic and diastolic function [20]. Patients with cardiomyopathy and an atrial or ventricular arrhythmia have been shown to have higher baseline levels of plasma cardiac troponins than those without an arrhythmia [21, 22]. Clinically it has been observed that patients presenting with atrial arrhythmias and underlying cardiomyopathy have elevated levels of cardiac troponin; however, the effect of cardioversion and subsequent return to sinus rhythm on myocardial leak of troponin has yet to be investigated in this cohort.
The objectives of this study were therefore to determine if synchronized DC cardioversion of atrial arrhythmias causes myocardial injury 6 h post-cardioversion by measuring cardiac TnI. Additionally, we aim to determine if there is a relationship between the change in cardiac TnI and cumulative energy given during cardioversion or left ventricular mass (as measured by echocardiography). Secondary objectives include a sub-group analysis of patients with cardiomyopathy to determine if any relationship exists between DC cardioversion and TnI levels.
2 Methods
2.1 Study design
This study was a prospective, observational study that assessed biochemical and structural parameters of cardiac function in patients undergoing synchronized DC cardioversion for atrial arrhythmias. Participants underwent a procedure during a single visit to the Department of Cardiology at Cork University Hospital in Cork, Ireland. During this visit, blood sampling was obtained prior to and 6 h following the patients’ DC cardioversion.
2.2 Participants
Individuals undergoing synchronized DC cardioversion for atrial arrhythmias at Cork University Hospital in Cork, Ireland, were approached for participation in this study. A total of 73 individuals (59 men, 14 women) agreed to participate in the study. Inclusion criteria included all subjects greater than 18 years of age who were undergoing synchronized DC cardioversion for an atrial arrhythmia. This included both elective and non-elective admissions and included patients with atrial fibrillation, atrial flutter, and focal atrial tachycardia. Exclusion criteria included a myocardial infarction within the past month, coronary artery bypass grafting within the past month, cardioversion for a ventricular arrhythmia, and any recent shocks by an implantable internal cardioverter defibrillator. All procedures conformed to the Declaration of Helsinki and were approved by the Clinical Research Ethics Committee at University College Cork. Written and informed consent was obtained from all participants.
2.3 Biochemistry and cardiac markers
Baseline blood tests, which included a basic electrolyte panel, C-reactive protein, and cardiac TnI, were recorded in all participants. Blood samples were collected by a registered nurse or advanced nurse practitioner into lithium heparin blood bottles. Blood samples were transported to the Cork University Hospital biochemistry laboratory within 15 min of being drawn, and analysis of blood samples were completed immediately upon receipt. Six hours following DC cardioversion, repeat blood samples for C-reactive protein and cardiac TnI quantification were collected via direct venous puncture. The measurement of pre-cardioversion and 6 h post was determined by the Third Universal Definition of Myocardial Infarction guidelines on “Biomarker Detection of Myocardial Injury with Necrosis” [23].
2.4 Synchronized DC cardioversion
All patients underwent synchronized DC cardioversion of their arrhythmias according to standard protocol. In brief, pre-procedural electrocardiogram was obtained for confirmation of the presenting arrhythmia and participants received general anesthesia. The Philips HeartStart biphasic Defibrillator XL (Phillips, Amsterdam, Netherlands) was used for the procedure with pad placed in the anterior-posterior position. Adhesive gel pads were used for all procedures. Once sedated, a shock of 150 J was delivered to the patient. If this was sufficient energy to cardiovert to sinus rhythm, the procedure was complete. If the patient remained in arrhythmia, a subsequent shock of 200 J was delivered up to two more times. Following the third overall attempt, pads were changed and a fourth and final attempt was made with an energy of 200 J. The exact energy of the shock delivered and measured impedance was recorded from the rhythm strip of the defibrillator. A successful cardioversion was defined as at least three consecutive beats of sinus rhythm on the rhythm strip following cardioversion.
2.5 Echocardiography
Two-dimensional transthoracic echocardiography was performed in the left lateral decubitus position by a trained echocardiographer (GE Vivid E9 Imaging System, GE Medical, Horton, Norway) using a M4S Matrix Sector Array Probe (2–5 MHz). Standard views (parasternal long axis and apical two, four, and five chambers) were collected and analyzed according to the recommendations of the American Society for Echocardiography [24, 25] using a dedicated software program (GE EchoPAC v201, GE, Horton, Norway); LV mass was subsequently calculated using the Devereux formula: LV Mass = 0.8[1.04[([LVEDD + IVSd + PWd]3 − LVEDD3)]} + 0.6 [26].
2.6 Statistics
Preliminary analysis of the data showed potential response differences in patients with cardiomyopathy and as such data were stratified accordingly for additional analysis. Statistical analyses were performed using Statistical Package for Social Sciences software v25 (IBM Corporation, Armonk, NY, USA) and GraphPad Prism (GraphPad Software Inc., La Jolla, CA, USA). Data was assessed using repeated measures ANOVA and Pearson’s correlation coefficients as a full dataset and stratified by cardiomyopathy status. Data are reported as mean ± standard deviation with a significance level of a = 0.05.
3 Results
Of the 103 patients approached to participate in the study, 73 patients were recruited (25 did not wish to participate, 6 did not meet exclusion criteria), 14 of which were known to have a diagnosed cardiomyopathy. Baseline clinical parameters are shown in Table 1. Of the participants with cardiomyopathy, two had hypertrophic, three dilated, four ischemic, and five tachycardia induced.
Of the 73 patients that underwent synchronized DC cardioversion for an atrial arrhythmia, 100% achieved sinus rhythm. Fifty-five (75%) achieved sinus rhythm with a single shock and 7 (9.5%) cases received three or more shocks. The cumulative energy delivered is displayed in Table 1.
All laboratory samples taken were analyzed by the biochemistry laboratory, with no reports of any samples being hemolyzed. The upper reference limit of cardiac TnI was > 34 ng/L with the minimum reporting value of 5 ng/L. The cardiac TnI and C-reactive protein before and after cardioversion in both cohorts are shown in Table 2 with the differences displayed in Fig. 1. Repeated measures ANOVA showed a significant decrease in cardiac TnI following cardioversion in patients without cardiomyopathy (6.7 ± 3.7 ng/L vs. 6.2 ± 3.2 ng/L, F(1,58) = 6.481, p = 0.014). A non-significant reduction in TnI was seen in the cardiomyopathy group (74.4 ± 136.7 ng/L vs. 54.6 ± 104.3 ng/L, F(1,13) = 3.676, p = 0.07). There was also a significant reduction in C-reactive protein in all participants (5.0 ± 0.83 U/L vs. 4.7 ± 0.77 U/L, F(1,72) = 4.313, p = 0.04) and the cardiomyopathy sub-analysis (2.8 ± 2.4 U/L vs. 2.6 ± 2.4 U/L, F(1,13) = 7.602, p = 0.017) following cardioversion (Fig. 1).

Differences in troponin I (a) and C-reactive protein (b) before and after cardioversion when stratified by presence of cardiomyopathy
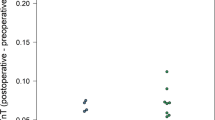
When the change in cardiac TnI from pre- to post-cardioversion is plotted against cumulative energy delivered during cardioversion (Fig. 2a) and LV mass (Fig. 2b), there was no significant relationship amongst the small changes observed (r = 0.137, p = 0.306 and r = 0.125, p = 0.412 respectively). However, in the cardiomyopathy group (Fig. 2, gray), there are a few select cases that showed significant reductions in cardiac TnI.

Changes in troponin I from pre- to post-cardioversion as plotted against cumulative energy in Joules (a) and left ventricular mass (b)
4 Discussion
The results of this study indicated that external DC cardioversion did not result in myocardial injury, as measured by cardiac TnI. When stratifying by patients with cardiomyopathy, there was a statistically significant reduction in cardiac TnI following cardioversion in the non-cardiomyopathy sub-group; however, this was likely not a clinically relevant change as values were below the threshold of clinical significance. Analyzing changes in CRP showed statistically significant reduction in both the whole group analysis and the cardiomyopathy group following cardioversion.
4.1 Cardiac biomarkers
When evaluating the changes in cardiac TnI, we need to consider the clinical relevance of the changes following cardioversion in addition to the statistical significance of the changes. The assay used in this study had an upper limit of normal of 34 ng/L. Although the non-cardiomyopathy group showed a statistically significant reduction in TnI (Table 2), the difference of less than 1 ng/L is not clinically significant. The range of TnI (5–26 ng/L) also revealed that no patients had clinically significant troponin elevations. In the cardiomyopathy group, the reduction in TnI following cardioversion had greater clinical significance. The average pre-cardioversion troponin was above the upper limit of normal, suggesting possible baseline myocardial injury. This is largely in agreement with the literature, which states that individuals with cardiomyopathy often have elevated troponin at baseline [20, 27]. Even though these values are not statistically significant, the clinical relevance is hypothesis generating for the role of cardioversions for myocardium protection in patients suffering from atrial arrhythmias. To our knowledge, there is no prior evidence to suggest that cardioversion can result in an improvement in myocardial injury in patients with cardiomyopathy and an atrial arrhythmia.
Regarding the changes in CRP, the observed reductions, although statistically significant, do not likely carry clinical significance. Elevations in CRP have been shown to increase with myocardial injury to predict severity of myocardial injury [28]. However, the specific test used in our study to assess CRP suggests that an elevation above 10 mg/L indicates mild inflammation. The average CRP values detected in the whole population and cardiomyopathy group (Table 2) are below 10 mg/L, and therefore, the detected differences are not likely clinical important at the population level.
4.2 Cumulative energy and LV mass
When comparing changes in cardiac TnI to cumulative energy delivered during cardioversion and left ventricular mass, no relationships were observed. This suggests that increased energy delivered during cardioversion does not injure the myocardium in a dose-dependent manner. Since we have shown that increased cumulative energy does not likely cause myocardial injury, the usage of higher energy shocks should be considered for emergent cardioversions in order to increase the likelihood of successful cardioversion [29].
4.3 Clinical relevance
This study has allowed several hypotheses to be drawn when considering its clinical relevance. The lack of TnI elevation confirms the results from Lobo et al. (2018) who reported no evidence of myocardial injury following DC cardioversion by measuring changes in cardiac troponin T. This implies that an elevated troponin following cardioversion should not be considered a benign finding but may suggest a more serious myocardial pathology that requires further investigation. The release of troponin during arrhythmias may be due to excessive myocardial stretching and alteration in the structure of integrins, thus allowing for release of cytosolic troponin into the plasma [30]. In patients with cardiomyopathy, the addition of an atrial arrhythmia may lead to additive myocardial injury and thus result in increased myocardial leak of cardiac troponin. Cardioversion of patients with cardiomyopathy who present to with significant myocardial injury, as measured by elevated TnI, may thus have a greater overall benefit from return to sinus rhythm by reducing mechanical stress and myocardial stretching.
4.4 Strengths and limitations
This study has several notable strengths but is also not without limitations. Firstly, we observed clinically significant reductions in cardiac TnI following cardioversion in patients with cardiomyopathy though our sample size may be underpowered to detect statistically significant differences. Additionally, our study was conducted at a single center and is thus subject to possible population bias and limitations to generalizability of the results. Lastly, the Third Universal Definition guidelines on “Biomarker Detection of Myocardial Injury” suggest that cardiac troponin peaks approximately 12 h following an MI [25], which may limit the internal validity of this study as we used a time point of 6 h post-procedure to collect hematologic samples.
Future studies should focus on recruiting more individuals with cardiomyopathies and atrial arrhythmias to determine if cardioversion can result in a significant clinical improvement in myocardial injury in these patients. Additionally, further time points post-cardioversion should be considered to determine if reductions in TnI continue to occur after the 6-h time point, potentially showing further benefits of a return to sinus rhythm in the cardiomyopathy cohort.
5 Conclusion
Synchronized DC cardioversion of an atrial arrhythmia did not cause myocardial injury 6-h post-cardioversion, as measured by the highly sensitive cardiac TnI. Sub-group analysis stratified by the presence of cardiomyopathy suggests that cardioversion of patients with cardiomyopathy may result in normalization of TnI and thus an improvement in myocardial strain or injury. These data imply that elevations in troponin post-cardioversion should be taken as a serious complication and investigated further. Finally, it may be of benefit for patients with cardiomyopathy and atrial arrhythmias to have cardioversion more urgently as it may help to improve myocardial injury and offer long-term cardioprotection.
Data availability
The data can be made available by request from the corresponding author.
References
Dhoot GK, Gell PG, Perry SV. The localization of the different forms of troponin I in skeletal and cardiac muscle cells. Exp Cell Res. 1978;117(2):357–70.
Dhoot GK, Perry SV. Distribution of polymorphic forms of troponin components and tropomyosin in skeletal muscle. Nature. 1979;278(5706):714–8.
Knayzer B, Abramov D, Natalia B, Tovbin D, Ganiel A, Katz A. Atrial fibrillation and plasma troponin I elevation after cardiac surgery: relation to inflammation-associated parameters. J Card Surg. 2007;22(2):117–23. https://doi.org/10.1111/j.1540-8191.2006.00366.x.
Oltrona L, Ottani F, Galvani M, Italian Working Group on Atherosclerosis T, Vascular B, the Associazione Nazionale Medici Cardiologi O. Clinical significance of a single measurement of troponin-I and C-reactive protein at admission in 1773 consecutive patients with acute coronary syndromes. Am Heart J. 2004;148(3):405–15. https://doi.org/10.1016/j.ahj.2004.03.023.
Iakobishvili Z, Weissler A, Buturlin K, Goldenberg G, Strassberg B, Tur R, et al. High sensitivity cardiac troponin T levels after elective cardioversion for atrial fibrillation/flutter. The Israel Medical Association journal : IMAJ. 2015;17(10):607–11.
Chung MK, Martin DO, Sprecher D, Wazni O, Kanderian A, Carnes CA, et al. C-reactive protein elevation in patients with atrial arrhythmias: inflammatory mechanisms and persistence of atrial fibrillation. Circulation. 2001;104(24):2886–91. https://doi.org/10.1161/hc4901.101760.
Lip GYH, Brechin CM, Lane DA. The global burden of atrial fibrillation and stroke: a systematic review of the epidemiology of atrial fibrillation in regions outside North America and Europe. Chest. 2012;142(6):1489–98. https://doi.org/10.1378/chest.11-2888.
Chugh SS, Havmoeller R, Narayanan K, Singh D, Rienstra M, Benjamin EJ, et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014;129(8):837–47. https://doi.org/10.1161/CIRCULATIONAHA.113.005119.
Hernandez-Madrid A, Svendsen JH, Lip GY, Van Gelder IC, Dobreanu D, Blomstrom-Lundqvist C, et al. Cardioversion for atrial fibrillation in current European practice: results of the European Heart Rhythm Association survey. Europace: European pacing, arrhythmias, and cardiac electrophysiology: journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2013;15(6):915–8. https://doi.org/10.1093/europace/eut143.
Januzzi JL Jr. Troponin testing after cardiac surgery. HSR Proc Intensive Care Cardiovasc Anesth. 2009;1(3):22–32.
Okmen E, Cam N, Sanli A, Unal S, Tartan Z, Vural M. Cardiac troponin I increase after successful percutaneous coronary angioplasty: predictors and long-term prognostic value. Angiology. 2006;57(2):161–9. https://doi.org/10.1177/000331970605700205.
Guensch DP, Yu J, Nadeshalingam G, Fischer K, Shearer J, Friedrich MG. Evidence for acute myocardial and skeletal muscle injury after serial transthoracic shocks in healthy swine. PLoS One. 2016;11(9):e0162245. https://doi.org/10.1371/journal.pone.0162245.
Kosior DA, Opolski G, Tadeusiak W, Chwyczko T, Wozakowska-Kaplon B, Stawicki S, et al. Serum troponin I and myoglobin after monophasic versus biphasic transthoracic shocks for cardioversion of persistent atrial fibrillation. Pacing Clin Electrophysiol. 2005;28(Suppl 1):S128–32. https://doi.org/10.1111/j.1540-8159.2005.00038.x.
Piechota W, Gielerak G, Ryczek R, Kazmierczak A, Bejm J, Piechota W. Cardiac troponin I after external electrical cardioversion for atrial fibrillation as a marker of myocardial injury--a preliminary report. Kardiol Pol. 2007;65(6):664–9 discussion 70-1.
Cemin R, Rauhe W, Marini M, Pescoller F, Pitscheider W. Serum troponin I level after external electrical direct current synchronized cardioversion in patients with normal or reduced ejection fraction: no evidence of myocytes injury. Clin Cardiol. 2005;28(10):467–70.
Santos ES, Pereira MP, Minuzzo L, Moreira DA, Ramos R, Avezum A et al. [Electrical cardioversion and myocardial injury: evaluation by new cardiac injury markers]. Arquivos brasileiros de cardiologia. 2006;86(3):191–7. doi:/S0066-782x2006000300006.
Faddy SC, Powell J, Craig JC. Biphasic and monophasic shocks for transthoracic defibrillation: a meta analysis of randomised controlled trials. Resuscitation. 2003;58(1):9–16. https://doi.org/10.1016/s0300-9572(03)00077-7.
Lobo R, Jaffe AS, Cahill C, Blake O, Abbas S, Meany TB, et al. Significance of high-sensitivity troponin T after elective external direct current cardioversion for atrial fibrillation or atrial flutter. Am J Cardiol. 2018;121(2):188–92. https://doi.org/10.1016/j.amjcard.2017.10.009.
Missov E, Calzolari C, Pau B. Circulating cardiac troponin I in severe congestive heart failure. Circulation. 1997;96(9):2953–8. https://doi.org/10.1161/01.cir.96.9.2953.
Giannoni A, Pastormerlo LE, Barison A. Troponin in non-ischaemic dilated cardiomyopathy. European Cardiology Review. 2011;7(3).
Zhou Y, Yu M, Yuan J, Liu S, Hu F, Yang Z, et al. Cardiac troponin I is associated with non-sustained ventricular tachycardia in patients with hypertrophic obstructive cardiomyopathy. Heart Vessel. 2020;35(6):876–85. https://doi.org/10.1007/s00380-019-01549-0.
Jesel L, Berthon C, Messas N, Lim HS, Girardey M, Marzak H, et al. Atrial arrhythmias in Takotsubo cardiomyopathy: incidence, predictive factors, and prognosis. Europace. 2019;21(2):298–305. https://doi.org/10.1093/europace/euy147.
Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, et al. Third universal definition of myocardial infarction. J Am Coll Cardiol. 2012;60(16):1581–98. https://doi.org/10.1016/j.jacc.2012.08.001.
Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2005;18(12):1440–63. https://doi.org/10.1016/j.echo.2005.10.005.
Voigt JU, Pedrizzetti G, Lysyansky P, Marwick TH, Houle H, Baumann R, et al. Definitions for a common standard for 2D speckle tracking echocardiography: consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. J Am Soc Echocardiogr. 2015;28(2):183–93. https://doi.org/10.1016/j.echo.2014.11.003.
Jafary FH. Devereux formula for left ventricular mass--be careful to use the right units of measurement. J Am Soc Echocardiogr. 2007;20(6):783. https://doi.org/10.1016/j.echo.2007.02.034.
Sato Y, Taniguchi R, Nagai K, Makiyama T, Okada H, Yamada T, et al. Measurements of cardiac troponin T in patients with hypertrophic cardiomyopathy. Heart. 2003;89(6):659–60. https://doi.org/10.1136/heart.89.6.659.
Dedobbeleer C, Melot C, Renard M. C-reactive protein increase in acute myocardial infarction. Acta Cardiol. 2004;59(3):291–6. https://doi.org/10.2143/AC.59.3.2005184.
Berg RA, Hemphill R, Abella BS, Aufderheide TP, Cave DM, Hazinski MF, et al. Part 5: adult basic life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S685–705. https://doi.org/10.1161/CIRCULATIONAHA.110.970939.
Costabel JP, Burgos LM, Trivi M. The significance of troponin elevation in atrial fibrillation. J Atr Fibrillation. 2017;9(6):1530. https://doi.org/10.4022/jafib.1530.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethics approval
Ethical approval for this study was obtained from the University College Cork Clinical Research Ethics Committee.
Consent to participate
All patients signed an informed consent document that included their consent to participate and consent for the study results to be published in a medical journal.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sless, R.T., Allen, G., Hayward, N.E. et al. Characterization of troponin I levels post synchronized direct current cardioversion of atrial arrhythmias in patients with and without cardiomyopathy. J Interv Card Electrophysiol 60, 329–335 (2021). https://doi.org/10.1007/s10840-020-00814-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-020-00814-x