
Abstract
Objectives
This study examined associations between child disability and parent-reported overparenting, autonomy granting, and affect management among a purposeful sample of parents whose children attended a camp serving early adolescents with disabilities or a camp serving early adolescents without disabilities.
Methods
868 parents completed a post-camp online questionnaire designed to measure overparenting, autonomy granting, and affect management. The measure’s factor structure and model fit were examined through Confirmatory Factor Analysis (CFA) and the relations between variables were tested using a Structural Equation Model (SEM).
Results
Parents of children attending the camp serving early adolescents with disabilities reported higher levels of overparenting as compared to parents of early adolescents without a disability. Further, overparenting had a positive effect on affect management, but not on autonomy granting. Finally, disability status did not have a statistically significant negative effect on affect management or autonomy granting.
Conclusions
Overparenting appears at higher rates among parents of early adolescents with disabilities, which may reflect overparenting as normative for parents with children with disabilities. Such overparenting behaviors may support children with disabilities to perform more consistently when compared to their peers.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Overparenting represents a group of well-intended parental behaviors taken to an excessive degree (Gagnon and Garst 2019; Segrin et al. 2012) and correspondingly reflects the extreme “tail” of the parenting behavior spectrum. When at “normative” levels, these parental behaviors are developmentally appropriate. That is, when parents are properly involved in their child’s life, help their child navigate common challenges, and provide appropriate boundaries for their child, their children generally have greater rates of wellbeing, academic success, and lower rates of maladaptive behaviors (Darling et al. 2006). Conversely, when parents do not involve themselves in their child’s life, this absence of parental involvement, support, and encouragement can result in greater rates of child substance abuse and lower levels of child well-being (Patock-Peckham and Morgan-Lopez 2006; Wisherth et al. 2016). Reflecting the opposite end of the parenting spectrum, when a parent engages in excessive guidance, support, and problem solving (i.e., overparenting behaviors), these excessive behaviors may also result in negative developmental consequences for the child (Leung and Shek 2018; Segrin et al. 2015). Thus, parenting can be viewed as an inverted u-shaped curve where an optimal amount of parental involvement is associated with positive outcomes, whereas too little or too much support is generally associated with poorer outcomes for the child (Liss and Schiffrin 2014). Given individual differences in children’s needs and abilities, a challenge among parenting researchers is determining when parenting behaviors are considered “normative” and developmentally-appropriate versus excessive and intrusive (Clarke et al. 2013). For example, while some research suggests that children with a disability or special medical need may receive excessive amounts of protection from their parents (Holmbeck et al. 2002), other studies suggest such children may not experience such excessive parenting behaviors (Tillery et al. 2014).
Although the motivation underlying overparenting may be to facilitate the best possible short- and long-term outcomes for one’s child (Rousseau and Scharf 2018; Segrin et al. 2013), overparenting behaviors have been linked to a range of negative consequences. An emerging body of evidence suggests that children whose parents engage in overparenting demonstrate poorer academic outcomes, lower levels of self-esteem, poorer relationships with peers, higher rates of anxiety and depression, and higher levels of substance use compared to children whose parents do not exhibit overparenting behaviors (LeMoyne and Buchanan 2011; Schiffrin et al. 2014; Wong et al. 2018). Because most overparenting studies have focused on college-aged students (e.g., Burke et al. 2018; Cui, Allen et al. 2019; Leung and Shek 2018; Segrin et al. 2012), it is unclear when overparenting behaviors may emerge and begin to positively or negatively impact children. Studying overparenting in other developmental periods is important given that the manifestation of overparenting, and corresponding developmental consequences, are likely to transpire before emerging adulthood (Cui, Darling et al. 2019; LeMoyne and Buchanan 2011). Although few in number, some studies have documented associations between overparenting and negative outcomes in children in elementary school (Hong et al. 2015) and early adolescence (Gagnon 2019). This work suggests the link between overparenting and negative developmental outcomes may reflect expected advancement of independence, confidence, and social skills—important developmental goals during adolescence (Butner et al. 2009)—that may be stifled by overparenting (Hong et al. 2015). Considering that overparenting may become increasingly likely as children get older (Segrin and Flora 2019), adolescence may be a particularly salient period to study overparenting as that is the time when adolescents are negotiating attachment with and independence from their parents (McElhaney et al. 2009). Another limitation of previous overparenting research is that few studies have considered the extent to which overparenting may manifest differently depending on the characteristics of the child (Dempsey and Keen 2008; Kouros et al. 2017; Raya et al. 2013), as behaviors that may seem “overparent-like” and excessive within one population (i.e., children with disabilities) may actually be normative and developmentally-appropriate in another (i.e., children without disabilities) (Garst and Gagnon 2015; Shucksmith et al. 1995; Tung and Lee 2018).
Approximately 20% of youth in the United States have a chronic health condition (Centers for Disease Control and Prevention 2018) requiring greater parent involvement and support (Harris et al. 2001). The unique characteristics associated with these children’s physical, motor, cognitive, and/or developmental disabilities as well as special medical needs (e.g., diabetes or heart conditions) may influence the expression of overparenting. For instance, having a child with a disability may require additional parental involvement, support, and warmth to ensure the child has access to necessary services to achieve similar outcomes and developmental milestones as their peers without disabilities in both academic and out-of-school time (OST) contexts (Burrell and Borrego 2012; Dempsey and Keen 2008).
While overparenting has not been explicitly researched within parents of children with disabilities, there is evidence to support differences in parenting behaviors closely related to overparenting. For example, parents of children with disabilities tend to be more involved in both their child’s academic and OST experiences (Floyd and Gallagher 1997; Wagner et al. 2005). Having a child with a disability is also associated with differential levels of parental control, parental overprotection, encouragement, warmth, affect management, and intrusiveness (Clarke et al. 2013; Gau et al. 2008; Harris et al. 2001; Holmbeck et al. 2002; Phillips et al. 2017). In a longitudinal examination of the relations between child disability and parental warmth (e.g., encouraging and supporting the child), Eshbaugh et al. (2011) indicated parents of children with disabilities were less likely to demonstrate encouraging and supportive behaviors to their child, behaviors analogous to the affect management construct in overparenting research (e.g., I say or do things to cheer my child up) (Segrin et al. 2012). Similarly, Su et al. (2017) indicated mothers of children with an intellectual disability reported lower rates of autonomy support than mothers of children without an intellectual disability. The research both within and outside of the sphere of overparenting (i.e., research exploring parental behavior, style, and child disability), suggests parents of children with disabilities may express greater rates of overparenting-centric behaviors than parents whose children do not have disabilities. This difference, however, has not been explicitly tested. Exploration of parenting practices in children with disabilities also suggests excessive rates of parental involvement and affect management are associated with erosion of a child’s self-efficacy and disability management (Clarke et al. 2013; Reaven 2011; Yotyodying and Wild 2016). A review conducted by Harris et al. (2001) supports how these well-intentioned but excessive parent behaviors may harm a child. Specifically, these overparenting behaviors do not foster children’s autonomy in their own self-care; this suppression of autonomy, in turn, can lead to consequences when the child is outside of the parent’s care. A robust literature (see Vasquez et al. 2016) and theory (e.g., self-determination theory; Deci and Ryan 2008) supports the importance of autonomy-supportive environments for children’s development and psychological well-being.
To better understand overparenting within the contexts of families inclusive of a child with a disability, this study compared overparenting across parents of children with and without disabilities. Given the dearth of research on overparenting among children with disabilities, the study first established the construct validity of a measure of overparenting for use within this population. We tested the effect of overparenting on two commonly associated parenting behaviors, affect management and autonomy granting. These parenting behaviors were selected because their associations with overparenting behavior have been established in previous studies of emerging adult children (i.e., adult children averaging ~20 years of age) without disabilities (Segrin et al. 2012; Padilla-Walker and Nelson 2012). We hypothesized overparenting would have a positive effect on affect management (H1A) and a negative effect on autonomy granting behaviors (H1B). Our primary study intent was to test the extent to which parenting behavior differed based on child disability status. Based upon the extant literature, we hypothesized that parents of children with a disability would report higher levels of overparenting (H2A) and affect management (H2B), and lower levels of autonomy granting (H2C) as compared to parents of children without a disability.
Method
Participants
Data were collected from 868 parents of youth attending a one-week residential camp hosted by organization A (Summer 2017; serving children with disabilities, n = 471) and organization B (Summer 2016; serving children without disabilities n = 397). Parental respondents were primarily mothers (83%); well educated, with 67.3% of the sample reporting an associate degree or greater; and relatively affluent with 75% of the sample reporting annual household income (USD) greater than $50,000 per year (M = $100,343; SD = $64,494). Parental respondents primarily identified as White (84.8%), with smaller groups identifying as Hispanic or Latino origin (6.8%), African-American (4.1%), multiple race (2.1%), Asian origin (1.5%), and Native American (0.7%). The children in this study, about whom parents were reporting, were primarily female (57.1%) and on average were 11.64 years old (SD = 2.22 years). Youth also were primarily identified as White (79.1%), Hispanic or Latino origin (8%), multiple race (6.6%), African-American (4.7%), Asian Origin (1.3%), and Native American (0.4%). For demographic breakouts between organization A and organization B of these descriptive variables see Table 1.
Procedures
A purposeful sample of parents was identified based on criteria that included having a child with or without a diagnosed disability who was engaging in a camp experience and whose data were readily available for collection (Yin 2016). The organizations were selected for the current study due to their longstanding history of program evaluation and strong rapport with parents, fostering higher response rates to online parent survey research. Organization A serves primarily children with physical and/or neurological disabilities (e.g., Type 1 Diabetes, asthma, hearing impaired/deaf, vision impaired/blind, epilepsy) and a smaller group of children with cognitive disabilities (e.g., Fragile X syndrome, Down syndrome). Organization A provides week-long residential programs to children residing in one state within the southwest United States, providing a full-scholarship for their attendance.
All camp sessions at both organizations were intentionally designed to enhance independence, relatedness, and confidence through the provision of organized activities such as horseback riding, ropes course navigation, backcountry camping, and adaptive sports. Beyond these basic psychological needs, at Organization A, each weekly camp session also targeted the improvement of disability self-management alongside camp activities (e.g., diabetes insulin management, independent movement for children in wheelchairs). At Organization A, each weekly camp session serves a specific group of children by disability group (e.g., week one: hearing impaired/deaf, week seven: Type 1 Diabetes). Children with cognitive disabilities such as Down Syndrome are served in a single week. Organization A does not typically serve children with behavioral, emotional, or personality disorders (e.g., Attention Deficit Hyperactivity Disorder, ADHD; Autism Spectrum Disorder, ASD; Oppositional Defiant Disorder, ODD), but may unintentionally serve them when a targeted disability is also present (e.g., a child with Type 1 Diabetes and ADHD).
Organization B serves primarily children without disabilities; however, no criteria exclude children with disabilities from participating. Specifically, programs at Organization B are not deliberately designed to facilitate/enhance disability self-care, but those camp administrators responsible for program design and implementation provide reasonable accommodations when possible for children with disabilities. Children attending Organization B primarily reside in one state within the southeast United States and pay for their one-week residential experience (versus the full-scholarship provided at Organization A). Similar to Organization A, weekly camp sessions were intentionally designed to enhance independence, relatedness, and confidence, through the provision of organized activities such as shooting sports, robotics, outdoor camping skills, environmental and marine sciences, and rock climbing. At both Organization A and B, programs are generally coeducational (i.e., mixed sex) with children residing in single sex dormitory style cabins while attending the 5–7 day (4–6 night) sessions. Importantly, aside from the focus on disability self-care at Organization A, both organizations camps follow a similar curriculum and structure. Furthermore, both organizations adhered to programmatic, health, safety, and risk management standards of the camp industry’s governing body (American Camp Association 2019).
Parents were recruited for the study through an email containing a web-based Qualtrics questionnaire, sent one week after the completion of their child’s camp experience. Parents who did not complete the questionnaire after the first email were sent a reminder 14 days after the completion of their child’s camp experience. To incentivize parental participation in the study, respondents were offered entry to win one of six $100 gift cards. Additionally, to further enhance response rates, the email was sent by the lead administrator of each organization, with whom parents had already been corresponding regarding the logistics and potential benefits of their child’s camp experience. The combination of these strategies resulted in an overall response rate of 41.09% (Overall: 868/2112 potential respondents; organization A: 471/1061 potential respondents = 44.39%; organization B: 397/1051 potential respondents = 37.77%). The study was approved by the corresponding author’s institutional review board, and parents provided informed consent to participate in the study.
Measures
As part of a larger research program examining parental perceptions of their child’s OST experiences like summer camp, parents reported basic demographic information about themselves and their child attending the camp, and completed measures relating to their parental behaviors. Prior to responding to the measures described below, parents were primed with the prompt: Many factors influence whether or not parents will allow their child(ren) to participate in activities like camp and we are interested in learning more about your perspectives as a parent. The following questions will help us understand factors that influence the types of opportunities you support for your child. There are no right or wrong answers- we just want to learn more about your perspectives.
Child disability status
To conduct between-group analyses, data were dummy coded, where 0 indicated a child with a disability and 1 indicated a child without a disability (Fig. 1).

Structural model demonstrating child disability status as a predictor of overparenting. Covariances, error terms, items, and FIML constant excluded for parsimony of presentation; #Overparenting is a 2nd order factor, reflecting excessive control, excessive support, and excessive problem solving. *p ≤ 0.05
Overparenting
Overparenting was assessed with an adapted version of the overparenting subscale of the Parental Anxiety associated with Outdoor Experiences and Overparenting measure (PAOEO) developed by Gagnon and Garst (2019). In their study and the present one, overparenting was represented as a second-order factor (i.e., common cause) reflecting three first-order factors: (1) excessive control (e.g., I tell my child that he/she needs my support to succeed in life), (2) excessive support (e.g., When my child is engaged in an important task or project, I do some of it for them) and (3) excessive problem solving (e.g., If something doesn’t work out for my child, I do what I can to fix it). Response options on the 9-item 3-factor measure were rated on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree), where higher scores signify increasingly excessive levels of control, support, and problem solving and correspondingly greater rates of overparenting. Due to established evidence of nonsignificant differences between paternal and maternal reports of overparenting in prior studies utilizing the selected scales, these reports were not differentiated in the present study (Burke et al. 2018; Gagnon and Garst 2019). Gagnon and Garst (2019) reported high internal consistency of the overparenting scale in their study (α = 0.95) (see Table 2).
Affect management
In the current study, affect management was based on Segrin et al.’s (2012) scale development work. Their overparenting measure included an advice/affect management scale in which items related to advice management assessed the extent to which parents provided suggestions and ideas on how to manage life events (e.g., “I share ideas with my child about to handle the various situations that s/he encounters” and “I make suggestions to my child to help him/her get things accomplished”), and items related to affect management assessed the extent to which the parent engages in supportive, warm, and caring behaviors when the child is feeling or acting anxious or depressed (e.g., “I say or do things to cheer my child up”). Given potential issues with floor and ceiling effects identified in studies utilizing these scales (e.g., Burke et al. 2018), the response options were expanded from a 5-point to a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree). In the current study, the three items related to affect management were selected to create a latent affect management variable, which demonstrated acceptable levels of internal consistency (see Table 2).
Autonomy granting
Autonomy granting was assessed using an adapted version of the autonomy granting subscale of Kunz and Grych (2013). In this scale, parents rated their level of agreement on 3 items (e.g., I encourage my child to express their individual views and opinions). The rating scale was modified in the current study from a 5-point to a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree) with higher scores reflecting greater levels of autonomy granting parental behaviors. Kunz and Grych reported acceptable levels of internal consistency of their measure for fathers (α = 0.88) and mothers (α = 0.84). In the current study the three items were selected to create a latent autonomy granting variable, and internal consistency was also acceptable (see Table 2).
Data Analyses
Prior to planned analyses, the data were screened for normality, outliers, and missingness. First, the data distributions were examined for multivariate kurtosis in EQS 6.3 software, which indicated the data were non-normal (Yuan, Lambert, & Fouldi’s coefficient ≥ 10.00; = 26.74) (Bentler 2006; Byrne 2006). Similar kurtotic distributions have been demonstrated in prior investigations utilizing the selected scales. However, as the planned analyses assumed multivariate normality, a robust estimation technique was utilized to mitigate potential problems (i.e., Satorra–Bentler chi-square (S/Bχ²); Bentler 2006). The data were then screened for outliers excessively harming multivariate normality, which indicated 20 respondents were significantly contributing to nonnormality within the data set; as such these cases were removed from any further analyses, leading to a pre-hypothesis testing sample size of 869.
The data were then screened to determine if missingness was completely at random (MCAR) utilizing Little’s (1988) test of MCAR. The significant results of this analysis indicated a potential systematic cause of missingness, χ²(535) = 683.479, p ≤ 0.001. As such, data were inspected for evidence of a systematic cause of missingness. This inspection indicated no item (i.e., question) had greater than 5% of missing values (range = 0–3.34%), 95.16% of the sample had no missing values, and the ratio of incomplete data cells to complete data cells was less than 1% (173/13,020 = 0.013%). Thus, given the low rate of missing data across these dimensions and the lack of demographic differentiation between respondents with and without missing data, a full information maximum likelihood (FIML) approach was utilized to simulate missing values in proceeding analyses (Enders 2010).
Model fit for both the Confirmatory Factor Analysis (CFA) and Structural Equation Model (SEM) was examined through several robust criteria (Bentler 2006). Specifically, the Comparative Fit Indices (CFI) and the Non-Normed Fit Indices (N-NFI) were utilized to compare the sample covariance matrix with the independence (null) model, where values ≥ 0.90 generally indicate better model fit. To assess model fit in comparison with the covariance matrix, the Root Mean Squared Error of Approximation (RMSEA) was examined with values ≤ 0.08 typically representing better fit (Marsh et al. 2004). Within the CFA, convergent validity was assessed through a combination of factor loadings (λ ≥ 0.500), Cronbach’s alpha levels (α ≥ 0.600), and Average Variance Extracted (AVE ≥ 0.500) scores. Additionally, within the CFA, discriminant validity was assessed to determine whether the identified factors measured discrete constructs, where low between-factor correlations (i.e., r≤ 0.700) suggests discrimination across factors in combination with √AVE values, where √AVE levels should be greater than between factor correlations to ensure the factor is accounting for more unique variance than error (Byrne 2006; Kline 2016). Upon establishment of acceptable measurement properties, the study aims were tested through a SEM, shown in Fig. 1. In this model, the 2nd order overparenting factor was regressed onto affect management and autonomy granting parenting factors (aim 1) and secondly, affect management, autonomy granting, and the 2nd order overparenting factor were regressed onto child disability status to test for group differences in parenting behavior (aim 2).
Confirmatory Factor Analyses
The results from testing the measurement model (e.g., CFA) prior to testing the study hypotheses indicated one-item from the first-order excessive control factor (i.e., I make important decisions for my child) was significantly harming global model fit: [S/Bχ²(96) = 835.968, p ≤ 0.001, N-NFI = 0.836, CFI = 0.869, RMSEA = 0.093 (90%, CI 0.087–0.099)]. Inspection of the poor performing item’s factor loading (λ = 0.391), the item’s associations within the CFA covariance matrices, and LaGrange Multiplier (LM) test, results indicated respecification of the item to another factor would not result in meaningful improvement in model fit (Bentler 2006; Brown 2015). The LM test results also indicated items within the first-order overparenting factors were sharing a high-level of error variance. As the items illustrated acceptable factor loadings (λ = 0.540–0.871), the items and corresponding factors were retained and their errors covaried for the SEM (indicated by a # in Table 2). After the removal of the poor performing item, the CFA was repeated, which demonstrated acceptable model fit [S/Bχ²(82) = 351.997, p ≤ 0.001, N-NFI = 0.933, CFI = 0.947, RMSEA = 0.060 (90%, CI 0.054–0.067)]. As illustrated in Table 2, the scale exhibited evidence of convergent validity with all structural factor Cronbach alphas greater than 0.600 (α = 0.805–0.842), all structural factor loadings above 0.500 (λ = 0.521–0.990), and all structural factor AVE levels above 0.500 (AVE = 0.592–0.701). Further, as illustrated in Table 3, the scale exhibited discriminant validity with all between factor correlations lower than 0.700 (r = −0.075–0.342) and all √AVE values greater than corresponding between factor correlations (Kline 2016).
Results
As with the CFA model fit indices, the SEM exhibited fit approaching acceptability: [S/Bχ²(93) = 538.392, p < 0.001, N-NFI = 0.894, CFI = 0.918, RMSEA = 0.073 (90%, CI 0.067–0.079)]. Specifically, the N-NFI and RMSEA levels were close to being unacceptable (Byrne 2006). However, inspection of the LaGrange Multiplier (LM) test results and covariance matrices did not indicate any modifications would result in meaningful improvement to the model, without engaging in atheoretical “mindless modelling” and prescribing to “golden rules” (see also Kline 2016; Marsh et al. 2004). As such, the SEM was unmodified, and the study hypotheses were tested. Reinspection of the data as part of the SEM process indicated one additional case was contributing to multivariate kurtosis and was correspondingly removed from the data set, leading to the final study sample size of 868.
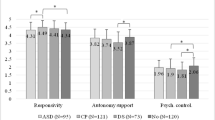
In partial support of hypotheses for the first research aim, overparenting had a positive direct effect on affect management (H1A; β = 0.385, SE = 0.032, p< 0.001), but did not have an effect on autonomy granting (H1B; β = −0.032, SE = 0.023, p = 0.844). Consistent with the hypothesis for the primary aim, parents of children with disabilities reported significantly higher levels of overparenting (H2A; β = −0.248, SE = 0.077, p < 0.001). However, counter to hypotheses, levels of affect management (H2B; β = −0.065, SE = 0.052, p = 0.060) and autonomy granting (H2C; β = 0.014, SE = 0.048, p = 0.693) did not differ between parents of children with and without disabilities.
After testing of the study hypotheses, an exploratory post-hoc analysis was conducted to determine if the associations between overparenting, affect management, and autonomy granting differed between parents of children with or without disabilities. Specifically, the samples were separated into their two respective data sets and the correlations between the three latent variables were explored. As illustrated in Table 4, parents of children without disabilities reported significant associations between overparenting and affect management (r = 0.375, p < 0.001), affect management and autonomy support (r= 0.230, p < 0.001), and a significant negative association between autonomy support and overparenting (r= −0.166, p = 0.004). Similarly, parents of children with disabilities reported significant associations between overparenting and affect management (r = 0.266, p < 0.001) as well as affect management and autonomy support (r = 0.420, p < 0.001). However, parents of children with disabilities did not report a significant association between overparenting and autonomy support (r = 0.002, p = 0.968), whereas parents in the sample of children without disabilities did report such a significant association.
Discussion
The purpose of this study was to compare overparenting across parents of children with and without disabilities. In doing so, associations between child disability and parent-reported overparenting and two established correlates of overparenting—affect management and autonomy granting—were examined. As hypothesized, overparenting had a positive direct effect on affect management, such that higher levels of overparenting indicated higher levels of parental support for their child’s affect (i.e., cheering up their child, providing words of encouragement to their child). This finding is consistent with Segrin et al. (2012), who also found that affect management was positively related to overparenting in a sample of emerging adults. Counter to the hypothesized relation, overparenting did not directly predict autonomy granting behaviors in the full sample. In the exploratory post-hoc analyses, however, we did find a small, negative correlation between overparenting and autonomy granting behavior, but only among parents with a child without a disability. There have been mixed findings in the literature on the association between overparenting and autonomy granting behavior, with some studies finding an inverse relation (Cui, Allen et al. 2019; Padilla-Walker and Nelson 2012), some studies finding a positive relation (Schiffrin et al. 2014), and some finding no relation (Kouros et al. 2017; Reed et al. 2016). These differences may be explained by a measurement effect based on differences in how overparenting was conceptualized and measured in these studies and the present study (i.e., the difference between a perception of overparenting and the display of an overparenting behavior). Additionally, the findings underscore that the association between overparenting and autonomy granting behavior may depend on characteristics of the child (Kouros et al. 2017).
As hypothesized, parents of children with a disability reported significantly higher levels of overparenting than parents of children without a disability. The findings contribute to the literature on overparenting by examining this parenting construct in early adolescence and by demonstrating that this dimension of parenting significantly differs based on children’s needs and abilities. One interpretation of the findings is that overparenting may be normative for parents with children with disabilities, and therefore occurs at higher levels as compared to parents of children without disabilities. This is consistent with similar investigations of parental control, overprotection, and intrusiveness in this parent population (Clarke et al. 2013; Gau et al. 2008; Holmbeck et al. 2002; Su et al. 2017). If overparenting is indeed normative among parents whose children have disabilities, then it may not be associated with the same negative consequences (e.g., anxiety and depression) identified in prior research (LeMoyne and Buchanan 2011; Schiffrin et al. 2014; Wong et al. 2018). Future research should examine if and how overparenting may impact developmental outcomes of children with disabilities. Furthermore, given that parents of children with disabilities engage in more overparenting behavior, future research should also examine how overparenting may impact parents’ well-being. This is especially relevant given parents of children with disabilities typically report higher rates of stress compared to parents of children without a disability (Floyd and Gallagher 1997; Rao and Beidel 2009). Parental well-being may be further impaired if parents believe their child needs more support (i.e., time and energy) than an over-extended and stressed overparent feels they can provide (Fingerman et al. 2012).
Counter to the study hypotheses, group differences in levels of affect management and autonomy granting behaviors were not indicated due to child disability. These results suggest that parents were just as likely to demonstrate affect management and autonomy-granting behaviors regardless of their child’s disability status. Although prior research has found that parents of children with disabilities engage in more affect management compared to parents of children without disabilities (Blacher et al. 2013), our study finding is consistent with Gau et al. (2008) who found no significant association between having a child with a disability and greater provision of affect management. With regard to autonomy supportive behavior, previous studies have reported that parents of children with a disability were significantly less likely to engage in autonomy supportive behavior (e.g., Gau et al. 2008; Phillips et al. 2017; Su et al. 2017). The lack of significant differences in these parenting dimensions in the present study between parents of children with and without a disability may reflect a sampling effect, such that parents of children with a disability in the current study were already comfortable sending their child to camp, thus provisioning some autonomy and affect management to their child.
Limitations
The limitations of the current study also provide direction for future research. First, this study incorporated a cross-sectional design common to overparenting studies (Kouros et al. 2017; Luebbe et al. 2018), which limits the conclusions that can be drawn as well as the ability to make causal statements. Further, parents completed self-report measures and, therefore, we cannot rule out the possibility that some findings may be due to mono-method reporter bias. Second, the sample was predominantly White and mostly consisted of mothers. Although these demographics are consistent with participants involved in other overparenting studies (Gagnon and Garst 2019; Segrin et al. 2012, 2015), this study provides a glimpse into overparenting among a relatively narrow range of parents of children with disabilities. Other parent samples, including fathers, those with lower rates of education, and those across a broader income range, may respond differently than the parents examined in this study. Future research in this area should also consider using ethnically and racially diverse samples. Third, data regarding disability status were not collected from Organization B (serving children without disabilities), and it is possible children with disabilities may have attended camp at Organization B. Given Organization B was not tailored for children with disabilities, it is likely that children attending this camp had higher levels of functioning, which may also have impacted the lack of a difference between camps serving and not serving children with disabilities. Fourth, parents were categorized into two groups (having a child with or without a disability) and it is possible there may be differences across disability subcategories (e.g., Down syndrome versus Type 1 Diabetes). Prior research, however, has not found meaningful differences in reports of parental behaviors based on type of child disability (Dyches et al. 2012). Fifth, the organizations examined in this study differed in that Organization A youth attended camp for free and Organization B youth attended camp for a fee. Because household income can differ between families with and without a family member with a disability (Kraus et al. 2018), and that living with or caring for a family member with a disability produces additional costs to families (Mitra et al. 2017; Stabile and Allin 2012), there may have been important differences between parents served by Organization A and parents served by Organization B. Sixth, although the overparenting measure used in this study performed relatively well, there has been differentiation in the construction of overparenting at a conceptual and theoretical level (e.g., Gagnon and Garst 2019; Leung and Shek 2018; Luebbe et al. 2018; Padilla-Walker and Nelson 2012; Schiffrin et al. 2014; Segrin et al. 2012). Research towards unifying concepts (e.g., overparenting dimensions that may include excessive support, control, protection, problem-solving, and limitations on autonomy granting) may be beneficial to ensure congruence within and across the developing areas of study and to guide the measurement of overparenting among targeted parent populations such as parents of children with disabilities.
Further, in the present study, there were only two groups represented (i.e., parents of children with disabilities and parent of children without disabilities). As disability and corresponding levels of necessary parental support tend to occur on a spectrum, it is likely that overparenting may manifest differently dependent on the child’s level of functioning. Specifically, research within the context of recreation therapy has indicated families tend to involve, advocate, and parent differently dependent on a child’s level of necessary language, adaptive living, physical/psychological, and intellectual support (Dodd et al. 2009; Dyches et al. 2004). Moreover, the age of child’s disability diagnosis as well as the levels of family and community level resources avaliable may promote or inhibit the manifestation of the excessive behaviors demonstrated by parents engaging in overparenting, offering another avenue of research. Put differently, exploration of the micro (e.g., individual child level of functioning, child-age at diagnosis) and macro-level (e.g., special education resources, level of adaptive programming) may provide a more holistic perspective on how and for whom overparenting behaviors occur and the potential benefits and consequences of these behaviors.
This study provides evidence that overparenting is more common among parents of children with disabilities when compared to a population of parents of children without disabilities. Although there may be many complementary explanations for why overparenting is higher among parents of children with disabilities, these explanations may boil down to a relatively simple rationale—these parents want their child to have the same opportunities as children without disabilities to grow into a successful and contributing member of society (Heiman 2002). However, due to challenges at the individual as well as system level, these parents must advocate for their child to a greater (and potentially “excessive”) degree to ensure their child has the same opportunities as their child’s peers without disabilities (Gau et al. 2008). As such, these overparents may provide the proper balance needed to counteract some of the deleterious effects associated with childhood disability. The effect of overparenting behavior in this younger population of children with disabilities, however, is unknown and remains a compelling future research direction. It is possible that overparenting may be protective in this context, allowing children with disabilities to perform at a level more consistent with their peers and resist maladaptive behaviors, despite the daily challenges and hardships associated with the disability the youth may face (Clarke et al. 2013; Earle and LaBrie 2016). Moreover, overparenting may also positively impact families. For example, in their study of the influence of repeated participation within medical specialty camps, Gagnon et al. (2019) suggested a potential avenue of research is examining how medical specialty camp participation may reduce later medical costs associated with a child’s camp participation, which could confer significant benefits to families with regard to expenses associated with a child’s disability. These and other potentially positive child and family-level outcomes of overparenting are ripe for further exploration.
It is also possible, however, that overparenting confers the same risks as has been documented in children without disabilities (LeMoyne and Buchanan 2011; Schiffrin et al. 2014; Wong et al. 2018), by interfering with a child’s ability to attain developmental goals of autonomy and competence, and negatively affecting their self-esteem. Moreover, even if overparenting does confer some advantages to children with disabilities, it is possible that overparenting may ultimately adversely affect children with disabilities indirectly by contributing to lower psychological well-being (e.g., stress and anxiety) among their parents over time. For example, Rizzo et al. (2012) reported that intensive parenting among mothers of preschoolers (without disabilities) was associated with greater maternal stress and depressive symptoms. In other research, Clark et al. (2013) and Gagnon and Garst (2019) found positive associations between excessive forms of parenting (e.g., overprotection, overparenting) and parent anxiety. Thus, future exploration of overparenting among children with disabilities should examine the potential negative outcomes of escalating levels of overparenting behavior for parents. Research exploring the differential effects of overparenting across children with disabilities should also consider how overparenting may impact service delivery within the context of human service programs (Garst and Gagnon 2015; Locke et al. 2012). For example, Garst and Gagnon (2015) proposed that overparenting may be a source of strain on staff and administrative resources devoted to OST programs and services. Thus, closer investigation of possible indirect and inadvertent outcomes of overparenting is warranted. Similar challenges have been noted in studies examining overparenting within college and university settings (Earle and LaBrie 2016).
Future overparenting research should also examine if and how specific parent (e.g., age, gender, education, income) and family characteristics (e.g., family structure including married, divorced, or separated parents) may influence how much parents engage in overparenting as well as how overparenting impacts child outcomes, as research into these associations has produced mixed results. For example, some studies have found that mothers engage in more overparenting than fathers (Fingerman et al. 2012; Rousseau and Scharf 2015; Van Ingen et al. 2015), yet other research has failed to find such an association between gender and overparenting (Gagnon and Garst 2019). Another avenue for future research is to examine the extent to which overparenting among parents of children with disabilities is dependent on parental and family characteristics. As parents are delaying childbirth until later in life (Mathews and Hamilton 2016), it is possible the widening gap between child age and parent age could influence rates of overparenting behaviors. Specifically, the provision of greater parental resources to their children through more protective, effortful, and indulgent parenting may be linked to overparenting behaviors, and these resources may reflect overparents’ greater socioeconomic status (Gagnon 2019). Further, as the body of parenting research is grounded in traditional family structures (e.g., biological father, biological mother, and children), so is the body of overparenting research. It is likely other family structures (e.g., single parent, step parent, same sex parents, grandparents, cohabiting) and demographic characteristics (e.g., ethnic group, socioeconomic status) may have differing influences on the manifestation of overparenting (Leung and Shek 2018; Segrin et al. 2012; Willoughby et al. 2015). As illustrated by the study findings, understanding of the impact and prevalence of overparenting among children with and without disabilities is only beginning to be understood. Indeed, the present study findings seem to illustrate more questions and gaps in our understanding of the potential effects of overparenting on diverse populations and contexts.
References
American Camp Association. (2019). Accreditation Process Guide. Monterey, CA: American Camp Association/Healthy Learning.
Bentler, P. M. (2006). EQS 6 Structural Equations Program Manual. Encino, CA: Multivariate Software, Inc.
Blacher, J., Baker, B. L., & Kaladjian, A. (2013). Syndrome specificity and mother–child interactions: examining positive and negative parenting across contexts and time. Journal of Autism and Developmental Disorders, 43(4), 761–774. https://doi.org/10.1007/s10803-012-1605-x.
Brown, T. A. (2015). Confirmatory factor analysis for applied research. 2nd ed. New York, NY: Guilford Press.
Burke, T. J., Segrin, C., & Farris, K. L. (2018). Young adult and parent perceptions of facilitation: associations with overparenting, family functioning, and student adjustment. Journal of Family Communication, 18(3), 233–247. https://doi.org/10.1080/15267431.2018.1467913.
Burrell, T. L., & Borrego, J. (2012). Parents’ involvement in ASD treatment: what is their role? Cognitive and Behavioral Practice, 19, 423–432. https://doi.org/10.1016/j.cbpra.2011.04.003.
Butner, J., Berg, C., Osborn, Butler, J., Godri, C., Fortenberry, K., Barach, I., Le, H., & Wiebe, D. (2009). Parent–adolescent discrepancies in adolescents’ competence and the balance of adolescent autonomy and adolescent and parent well-being in the context of Type 1 diabetes. Developmental Psychology, 45(3), 835–849. https://doi.org/10.1037/a0015363.
Byrne, B. M. (2006). Structural equation modeling with EQS: basic concepts, applications and programming. 2nd ed New York, NY: Routledge.
Centers for Disease Control and Prevention. (2018). Children and youth with special healthcare needs in emergencies. https://www.cdc.gov/childrenindisasters/children-with-special-healthcare-needs.html.
Clarke, K., Cooper, P., & Creswell, C. (2013). The parental overprotection scale: associations with child and parental anxiety. Journal of Affective Disorders, 151, 618–624. https://doi.org/10.1016/j.jad.2013.07.007.
Cui, M., Darling, C. A., Coccia, C., Fincham, F. D., & May, R. W. (2019). Indulgent parenting, helicopter parenting, and well-being of parents and emerging adults. Journal of Child and Family Studies, 28(3), 860–871. https://doi.org/10.1007/s10826-018-01314-3.
Cui, M., Allen, J., Fincham, F. D., May, R. W., & Love, H. (2019). Helicopter parenting, self-regulatory processes, and alcohol use among female college students. Journal of Adult Development, 26(2), 97–104. https://doi.org/10.1007/s10804-018-9301-5
Darling, N., Cumsille, P., Caldwell, L. L., & Dowdy, B. (2006). Predictors of adolescents’ disclosure to parents and perceived parental knowledge: Between- and within-person differences. Journal of Youth and Adolescence, 35(4), 667–678. https://doi.org/10.1007/s10964-006-9058-1.
Deci, E. L., & Ryan, R. M. (2008). Facilitating optimal motivation and psychological well-being across life’s domains. Canadian Psychology, 49, 14–23. https://doi.org/10.1037/0708-5591.49.1.14.
Dempsey, I., & Keen, D. (2008). A review of processes and outcomes in family-centered services for children with a disability. Topics in Early Childhood Special Education, 28(1), 42–52. https://doi.org/10.1177/0271121408316699.
Dodd, D. C. H., Zabriskie, R. B., Widmer, M. A., & Egget, D. (2009). Contributions of family leisure to family functioning among families that include children with developmental disabilities. Journal of Leisure Research, 41(2), 261–286. https://doi.org/10.1080/00222216.2009.11950169.
Dyches, T., Cichella, E., Olsen, S. F., & Mandleco, B. (2004). Snapshots of life: perspectives of school-aged individuals with developmental disabilities. Research and Practice for Persons with Sever Disabilities, 29(3), 172–182. https://doi.org/10.2511/rpsd.29.3.172.
Dyches, T., Smith, T. B., Korth, B. B., Olsen-Roper, S., & Mandleco, B. (2012). Positive parenting of children with developmental disabilities: a meta-analysis. Research in Developmental Disabilities, 33, 2213–2220. https://doi.org/10.1016/j.ridd.2012.06.015.
Earle, A. M., & LaBrie, J. W. (2016). The upside of helicopter parenting: engaging parents to reduce first-year student drinking. Journal of Student Affairs Research and Practice, 53(3), 319–330. https://doi.org/10.1080/19496591.2016.1165108.
Enders, C. K. (2010). Applied missing data analysis. New York, NY: The Guilford Press.
Eshbaugh, E. M., Peterson, C. A., Wall, S., Carta, J. J., Luze, G., Swanson, M., & Jeon, H.-J. (2011). Low-income parents’ warmth and parent–child activities for children with disabilities, suspected delays and biological risk. Infant and Child Development, 20, 509–524. https://doi.org/10.1002/icd.717.
Fingerman, K. L., Cheng, Y.-P., Wesselmann, E. D., Zarit, S., Furstenberg, F., & Birditt, K. S. (2012). Helicopter parents and landing pad kids: Intense parental support of grown children. Journal of Marriage and Family, 74, 880–896. https://doi.org/10.1111/j.1741-3737.2012.00987.x.
Floyd, F. J., & Gallagher, E. M. (1997). Parental stress, care demands, and use of support services for school-age children with disabilities and behavior problems. Family Relations, 46(4), 359–371.
Gagnon, R. J. (2019). Examining overparenting, socioeconomic status, and parental out-of-school time experience: Does socioeconomic status and out-of-school-time experience matter? Children and Youth Services Review. https://doi.org/10.1016/j.childyouth.2019.04.003.
Gagnon, R. J., & Garst, B. (2019). Exploring overparenting in summer camp: adapting, developing, and implementing a measure. Annals of Leisure Research, 22(2), 161–182. https://doi.org/10.1080/11745398.2018.1452619.
Gagnon, R. J., Garst, B. A., & Townsend, J. (2019). Tough decisions in medical specialty camps: examining the relationship between camp dosage, outcomes, and camper attendance. Social Science and Medicine, 221, 49–57. https://doi.org/10.1016/j.socscimed.2018.12.014.
Garst, B., & Gagnon, R. J. (2015). Exploring overparenting within the context of youth development programs. Journal of Youth Development, 10(1), 6–18. https://doi.org/10.5195/jyd.2015.416.
Gau, S. S., Chiou, Y., Soong, W., & Lee, M. (2008). Parental characteristics, parenting style, and behavioral problems among Chinese children with Down Syndrome, their siblings and controls in Taiwan. Journal of the Formosan Medical Association, 107(9), 693–703. https://doi.org/10.1016/S0929-6646(08)60114-X.
Harris, M. A., Mertlich, D., & Rothweiler, J. (2001). Parenting children with diabetes. Diabetes Spectrum, 14(4), 182–184. https://doi.org/10.2337/diaspect.14.4.182.
Heiman, T. (2002). Parents of children with disabilities: resilience, coping, and future expectations. Journal of Developmental and Physical Disabilities, 14(2), 159–171. https://doi.org/10.1023/A:1015219514621.
Holmbeck, G. N., Johnson, S. Z., Wills, K. E., McKernon, W., Rose, B., Erklin, S., & Kemper, T. (2002). Observed and perceived parental overprotection in relation to psychosocial adjustment in preadolescents with a physical disability: the mediational role of behavioral autonomy. Journal of Consulting and Clinical Psychology, 70(1), 96–110. https://doi.org/10.1037/0022-006X.70.1.96.
Hong, J. C., Hwang, M. Y., Kuo, Y. C., & Hsu, W. Y. (2015). Parental monitoring and helicopter parenting relevant to vocational student’s procrastination and self-regulated learning. Learning and Individual Differences, 42, 139–146. https://doi.org/10.1016/j.lindif.2015.08.003.
Kline, R. B. (2016). Principles and practice of structural equation modeling. 4th ed. New York, NY: Guilford Press.
Kouros, C. D., Pruitt, M. M., Ekas, N. V., Kiriaki, R., & Sunderland, M. (2017). Helicopter parenting, autonomy support, and college students’ mental health and well-being: the moderating role of sex and ethnicity. Journal of Child and Family Studies, 26, 939–949. https://doi.org/10.1007/s10826-016-0614-3.
Kraus, L, Lauer, E, Coleman, R., & Houtenville, A. 2018). 2017 Disability Statistics Annual Report. Durham, NH: University of New Hampshire. https://disabilitycompendium.org/sites/default/files/user-uploads/2017_AnnualReport_2017_FINAL.pdf.
Kunz, J. H., & Grych, J. H. (2013). Parental psychological control and autonomy granting: distinctions and associations with child and family functioning. Parenting, 13(2), 77–94. https://doi.org/10.1080/15295192.2012.709147.
LeMoyne, T., & Buchanan, T. (2011). Does “hovering” matter? Helicopter parenting and its effect on well-being. Sociological Spectrum, 31(4), 399–418. https://doi.org/10.1080/02732173.2011.574038.
Leung, J. T. Y., & Shek, D. T. L. (2018). Validation of the perceived Chinese overparenting scale in emerging adults in Hong Kong. Journal of Child and Family Studies, 27, 103–117. https://doi.org/10.1007/s10826-017-0880-8.
Little, R. J. A. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83(404), 1198–1202. https://doi.org/10.2307/2290157.
Liss, M., & Schiffrin, H. H. (2014). Balancing the big stuff: finding happiness in work, family, and life. Lanham, MD: Rowman & Littlefield.
Locke, J. Y., Campbell, M. A., & Kavanagh, D. (2012). Can a parent do too much for their child? An examination by parenting professionals of the concept of overparenting. Australian Journal of Guidance and Counselling, 22(2), 249–265. https://doi.org/10.1017/jgc.2012.29.
Luebbe, A. M., Mancini, K. J., Kiel, E. J., Spangler, B. R., Semlak, J. L., & Fussner, L. M. (2018). Dimensionality of helicopter parenting and relations to emotional, decision-making, and academic functioning in emerging adults. Assessment, 25(7), 841–857. https://doi.org/10.1177/1073191116665907.
Marsh, H. W., Hau, K.-T., & Wen, Z. (2004). In search of golden rules: comment on hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler’s (1999) findings. Structural Equation Modeling, 11(3), 320–341. https://doi.org/10.1207/s15328007sem1103_2.
Mathews, T. J., & Hamilton, B. E. (2016). Mean age of mothers is on the rise: United States, 2000–2014. National Center for Health Statistics Data Brief, 232, 1–8. https://www.ncbi.nlm.nih.gov/pubmed/26828319.
McElhaney, K. B., Allen, J. P., Stephenson, J. C., & Hare, A. L. (2009). Attachment and autonomy during adolescence. In R. M. Lerner & L. Steinberg (Eds), Handbook of adolescent psychology: individual bases of adolescent development (pp. 358–403). Hoboken, NJ, US: John Wiley & Sons Inc.
Mitra, S., Palmer, M., Kim, H., Mont, D., & Groce, N. (2017). Extra costs of living with a disability: a review and agenda for research. Disability and Health Journal, 10(4), 475–484. https://doi.org/10.1016/j.dhjo.2017.04.007.
Padilla-Walker, L. M., & Nelson, L. J. (2012). Black hawk down: establishing helicopter parenting as a distinct construct from other forms of parental control during emerging adulthood. Journal of Adolescence, 35, 1177–1190. https://doi.org/10.1016/j.adolescence.2012.03.007.
Patock-Peckham, J. A., & Morgan-Lopez, A. A. (2006). College drinking behaviors: mediational links between parenting styles, impulse control, and alcohol-related outcomes. Psychology of Addictive Behaviors, 20(2), 117–125. https://doi.org/10.1037/0893-164X.20.2.117.
Phillips, B. A., Conners, F., & Curtner-Smith, M. E. (2017). Parenting children with down syndrome: an analysis of parenting styles, parenting dimensions, and parental stress. Research in Developmental Disabilities, 68, 9–19. https://doi.org/10.1016/j.ridd.2017.06.010.
Rao, P. A., & Beidel, D. C. (2009). The impact of children with high-functioning autism on parental stress, sibling adjustment, and family functioning. Behavior Modification, 33(4), 437–451. https://doi.org/10.1177/0145445509336427.
Raya, A. F., Ruiz-Olivares, Pino, J., & Herruzo, J. (2013). Parenting style and parenting practices in disabled children and its relationship with academic competence and behavior problems. Procedia: Social and Behavioral Sciences, 89, 702–709.
Reed, K., Duncan, J. M., Lucier-Greer, M., Fixelle, C., & Ferraro, A. J. (2016). Helicopter parenting and emerging adult self-efficacy: implications for mental and physical health. Journal of Child and Family Studies, 25, 3136–3149. https://doi.org/10.1007/s10826-016-0466-x.
Reaven, J. (2011). The treatment of anxiety symptoms in youth with high-functioning autism spectrum disorders: developmental considerations for parents. Brain Research, 1380, 255–263. https://doi.org/10.1016/j.brainres.2010.09.075.
Rizzo, K. M., Schiffrin, H. H., & Liss, M. (2012). Insight into the parenthood paradox: mental health outcomes of intensive mothering. Journal of Child and Family Studies, 22, 614–620. https://doi.org/10.1007/s10826-012-9615-z.
Rousseau, S., & Scharf, M. (2015). I will guide you: the indirect link between overparenting and young adults’ adjustment. Psychiatry Research, 228, 826–834. https://doi.org/10.1016/j.psychres.2015.05.016.
Rousseau, S., & Scharf, M. (2018). Why people helicopter parent? An actor–partner interdependence study of maternal and paternal prevention/promotion focus and interpersonal/ self-regret. Journal of Social and Personal Relationships, 35(7), 919–935. https://doi.org/10.1177/0265407517700514.
Schiffrin, H. H., Liss, M., Miles-McLean, H., Gear, K. A., Erchull, M. J., & Tashner, T. (2014). Helping or hovering? The effects of helicopter parenting on college students’ well-being. Journal of Child and Family Studies, 23, 548–557. https://doi.org/10.1007/s10826-013-9716-3.
Segrin, C., & Flora, J. (2019). Fostering social and emotional intelligence: What are the best current strategies in parenting? Social and Personality Psychology Compass, e12439. https://doi.org/10.1111/spc3.12439.
Segrin, C., Givertz, M., Swaitkowski, P., & Montgomery, N. (2015). Overparenting is associated with child problems and a critical family environment. Journal of Child and Family Studies, 24, 470–479. https://doi.org/10.1007/s10826-013-9858-3.
Segrin, C., Woszidlo, A., Givertz, M., Bauer, A., & Taylor-Murphy, M. (2012). The association between overparenting, parent‐child communication, and entitlement and adaptive traits in adult children. Family Relations, 61(2), 237–252. https://doi.org/10.1111/j.1741-3729.2011.00689.x.
Segrin, C., Woszidlo, A., Givertz, M., & Montgomery, N. (2013). Parent and child traits associated with overparenting. Journal of Social and Clinical Psychology, 32(6), 569–595. https://doi.org/10.1521/jscp.2013.32.6.569.
Shucksmith, J., Hendry, L. B., & Glendinning, A. (1995). Models of parenting: implications for adolescent well-being within different types of family contexts. Journal of Adolescence, 18(3), 253–270. https://doi.org/10.1006/jado.1995.1018.
Stabile, M., & Allin, S. (2012). The economic costs of childhood disability. The Future of Children, 65–96. https://doi.org/10.1353/foc.2012.0008.
Su, H., Cuskelly, M., Gilmore, L., & Sullivan, K. (2017). Authoritative parenting of Chinese mothers of children with and without intellectual disability. Journal of Child and Family Studies, 26, 1173–1183. https://doi.org/10.1007/s10826-016-0628-x.
Tillery, R., Long, A., & Phipps, S. (2014). Child perceptions of parental care and overprotection in children with cancer and healthy children. Journal of Clinical Psychology in Medical Settings, 21(2), 165–172. https://doi.org/10.1007/s10880-014-9392-5.
Tung, I., & Lee, S. S. (2018). Context-specific associations between harsh parenting and peer rejection on child conduct problems at home and school. Journal of Clinical Child & Adolescent Psychology, 47(4), 642–654. https://doi.org/10.1080/15374416.2015.1102071.
Van Ingen, D. J., Freiheit, S. R., Steinfeldt, J. A., Moore, L. L., Wimer, D. J., Knutt, A. D., Scapinello, S., & Roberts, A. (2015). Helicopter parenting: the effect of an overbearing caregiving style on peer attachment and self- efficacy. Journal of College Counseling, 18, 7–20. https://doi.org/10.1002/j.2161-1882.2015.00065.x.
Vasquez, A. C., Patall, E. A., Fong, C. J., Corrigan, A. S., & Pine, L. (2016). Parent autonomy support, academic achievement, and psychosocial functioning: a meta-analysis of research. Educational Psychology Review, 28, 605–644. https://doi.org/10.1007/s10648-015-9329-z.
Wagner, M., Kutash, K., Duchnowski, A. J., Epstein, M. H., & Sumi, W. C. (2005). The children and youth we serve: a national picture of the characteristics of students with emotional disturbances receiving special education. Journal of Emotional and Behavioral Disorders, 13(2), 79–96. https://doi.org/10.1177/10634266050130020201.
Willoughby, B. J., Hersh, J. N., Padilla-Walker, L. M., & Nelson, L. J. (2015). “Back off”! Helicopter parenting and a retreat from marriage among emerging adults. Journal of Family Issues, 36(5), 669–692. https://doi.org/10.1177/0192513X13495854.
Wisherth, G. A., Mulvaney, M. K., Brackett, M. A., & Perkins, D. (2016). The adverse influence of permissive parenting on personal growth and the mediating role of emotional intelligence. The Journal of Genetic Psychology, 177(5), 185–189. https://doi.org/10.1080/00221325.2016.1224223.
Wong, R., Ho, F., Wong, W., Tung, K., Chow, C., Rao, N., Chan, K., & Ip, P. (2018). Parental involvement in primary school education: its relationship with children’s academic performance and psychosocial competence through engaging children with school. Journal of Child and Family Studies, 27, 1544–1555. https://doi.org/10.1007/s10826-017-1011-2.
Yotyodying, S., & Wild, E. (2016). Predictors of the quantity and different qualities of home-based parental involvement: evidence from parents of children with learning disabilities. Learning and Individual Differences, 49, 74–84. https://doi.org/10.1016/j.lindif.2016.05.003.
Yin, R. K. (2016). Qualitative research from start to finish. 2nd ed. New York, NY: The Guilford Press.
Author Contributions
R.J.G.: designed and executed the study, conducted the data analyses, and wrote the paper. B.A.G.: collaborated with the design and writing of the study. C.D.K., H.S., and M.C.: collaborated in the writing and editing of the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
This research was supported in part by Texas Lions Camp. The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of Texas Lions Camp. Texas Lions Camp had no involvement in the study design, analysis of data, or the development of this manuscript.
Ethical Approval
This research was approved by the Institutional Review Board (IRB) at Clemson University where it was conducted, which has Federal-wide Assurance from the Office of Human Research Protection (OHRP). Thus, all procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study. No identifying information was obtained during data collection.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gagnon, R.J., Garst, B.A., Kouros, C.D. et al. When Overparenting is Normal Parenting: Examining Child Disability and Overparenting in Early Adolescence. J Child Fam Stud 29, 413–425 (2020). https://doi.org/10.1007/s10826-019-01623-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-019-01623-1