
Abstract
Objectives
Parents play an important role in supporting their child’s social, behavioral, and emotional development. In the past decade, research on parenting in general populations increasingly relied on Self-Determination Theory (SDT) to better understand the association between parenting behaviors and child behavioral outcomes. In populations of children with a developmental disability, however, very little research has examined parenting behaviors from an SDT perspective. This study examines associations between parenting dimensions (responsiveness, autonomy support, psychological control) and children’s psychosocial outcomes (behavioral problems and psychosocial strengths) in and across four specific groups.
Methods
Parents of children between 7 and 15 years old with autism spectrum disorder (n = 95), cerebral palsy (n = 121), Down syndrome (n = 73), and without any known disability (n = 120) rated their parenting and their child’s behaviors.
Results
Group comparisons indicated that mean levels of parenting did not vary widely across groups. By contrast, salient differences in behavioral presentations were observed, with parents of children with ASD reporting the most behavioral problems and the least psychosocial strengths. Multi-group structural equation models revealed similar, SDT-predicted relations between parenting dimensions and psychosocial development in each group. Three structural effects were found: whereas higher levels of psychologically controlling related to more externalizing problems, higher levels of responsive as well as autonomy-supportive parenting were associated with more psychosocial strengths.
Conclusion
These results confirm that need-supportive parenting is related to beneficial outcomes and that need-thwarting socialization is related to maladaptive development in and across youth growing up with and without special needs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In developmental psychology, a long and fruitful research tradition has addressed the role of parenting in supporting children’s social, emotional, and behavioral development (Collins et al. 2000). In the past two decades, this research tradition has witnessed a growing interest in applying Self-Determination Theory (SDT) to better understand the relation between parenting and child behavioral outcomes (Deci and Ryan 2000; Soenens et al. 2017). A central tenet in SDT is that each individual, from birth on, is equipped with three basic psychological needs that require fulfillment in order to incite personal growth and well-being. These three needs are considered to be innate and universal for all human beings and are identified as autonomy (feeling psychological freedom and authenticity), relatedness (feeling connected with and loved by others), and competence (feeling able to reach personal goals) (Deci and Ryan 2000; Ryan and Deci 2017). When these needs are satisfied, the development and personal growth of a person is stimulated, providing energy, vitality, feelings of wellness and higher levels of self-development. Conversely, when these needs are not adequately satisfied or even actively frustrated, a person’s psychological well-being and growth gets forestalled, which may result in more unfavorable outcomes (Deci and Ryan 2000; Vansteenkiste and Ryan 2013). According to SDT, the socialization environment is crucial to attaining either fulfillment or frustration of these three basic psychological needs. Socializing agents (e.g., caregivers, teachers) can be actively fostering, indifferent to, or antagonistic towards a person’s satisfaction of needs (Vansteenkiste and Ryan 2013).
In the past two decades, a substantial body of work in mainstream populations has convincingly demonstrated that this SDT framework helps to better understand how parenting is related to behavioral outcomes in children and adolescents, via the mediating role of need-satisfaction versus need-frustration (Soenens and Vansteenkiste 2010). Parenting strategies can be regarded as more or less adequate in supporting the child’s fundamental psychological needs. When a child experiences need-supportive parenting, this will promote the child’s adjustment, by strengthening the inner resources of the child and by nurturing feelings of well-being and psychological growth. Other parenting behaviors are more need-thwarting in nature and relate to more adjustment difficulties in the child, such as internalizing or externalizing problems (Joussemet et al. 2008; Soenens et al. 2017).
Research identifies at least two central dimensions of need-supportive parenting, that is, responsiveness and autonomy support (Ryan and Deci 2017; Mabbe et al. 2018). First, responsive parenting is characteristic of parents who are warm, sensitive, and affectionate towards the child and who are physically and mentally present (Davidov and Grusec 2006). In doing so, parents primarily support children’s need for relatedness. Many studies have shown that responsive parenting is related to children’s better psychosocial development (Prinzie et al. 2009; Stern et al. 2015). Second, parental support for autonomy involves being empathic towards the child’s frame of reference, attuning to the pace and rhythm of a child’s development, and encouraging a child’s initiative (Joussemet et al. 2008). This type of parenting nurtures all three basic psychological needs in children (Grolnick et al. 2018; Soenens et al. 2007; Vansteenkiste and Ryan 2013) and is related to various adaptive behavioral outcomes, such as better social functioning (Roth 2008) and better emotion regulation (Brenning et al. 2015).
In contrast to these dimensions of need-supportive parenting, psychologically controlling parenting is an intensively studied dimension of need-thwarting parenting (Soenens and Vansteenkiste 2010). Psychological control refers to an intrusive type of control, manifested in the use of manipulative tactics such as guilt induction, shaming, and love withdrawal and controlling language (Barber 1996). In SDT-based research, this type of autonomy-suppressing parenting dimension is often studied alongside the effect of autonomy-supporting parenting (e.g., Mabbe et al. 2018) as these two dimensions are only moderately and negatively correlated (Costa et al. 2016). In this regard, it has been shown that psychologically controlling parenting has a more actively undermining effect on children’s needs, resulting in feelings of need frustration, whereas the absence of autonomy support primarily results in feelings of low need satisfaction (Mabbe et al. 2018). To date, a large body of research, including cross-sectional, longitudinal, diary, and experimental designs, has convincingly demonstrated that psychological control strongly relates to both internalizing and externalizing problems in childhood and adolescence (Pinquart 2016, 2017).
While parenting-adjustment relations have been extensively studied in mainstream populations, there is a paucity of research evaluating these relations in youth with neurodevelopmental disabilities, including autism spectrum disorder (ASD), cerebral palsy (CP), and Down syndrome (DS). Therefore, an important lingering research question is to what extent these relations between need-supportive and need-frustrating parenting on the one hand and behavioral outcomes on the other generalize across youth growing up with and without disabilities. The past decades witnessed a growing interest in family dynamics in these groups, yet the majority of studies has focused on elevated levels of stress or mental health problems in parents of a child with disability (Hayes and Watson 2013; Yorke et al. 2018), and less on specific parenting behaviors. Nevertheless, a budding research discipline started to evaluate the role of parenting in behavioral development in children with disabilities (Dieleman et al. 2017; Maljaars et al. 2014; Phillips et al. 2017). This research, however, mostly focused on one single disability, with little input from similar research on another disability. To better understand whether relations are specific to one disability, or instead generalize across disabilities, a cross-disability perspective is warranted. Therefore, we adopt a focus comparing four groups: parents raising a child with autism spectrum disorder (ASD), cerebral palsy (CP), and Down syndrome (DS), and parents raising a child without any known disability (NO). These four groups entail a wide variation in disability characteristics, including children who experience differences at least in one of three domains of functioning: i.e., psychosocial, physical, and/or cognitive.
In the literatures on these disabilities, there is a substantial body of research evaluating internalizing and externalizing behaviors in youth with ASD, CP, and DS. Multiple studies demonstrated that children growing up with these developmental disabilities are at increased risk to develop behavioral, emotional, or psychiatric difficulties compared to their peers without a disability. The highest risks apply to youth with ASD (e.g., De Pauw et al. 2011; Maljaars et al. 2014), but research also indicates that youth with CP and DS are at increased risk to develop emotional and behavioral problems (e.g., Dieleman et al. 2018b; Vrijmoeth et al. 2012). At the same time, research in youth with ASD, CP, as well as DS highlighted large inter-individual variation in the manifestation of these behavioral difficulties (Dieleman et al. 2018b; Vrijmoeth et al. 2012; Yorke et al. 2018).
In recent years, there is a growing appeal to not only focus on problem behaviors in youth with disabilities, but also to examine psychosocial strengths. In samples of children with and without disabilities, some studies suggested that problem behaviors and psychosocial strengths are related, yet distinct constructs (Dieleman et al. 2018b). Psychosocial strengths, as defined by Epstein and Sharma (1998) and Epstein (2004), denote specific child behaviors and skills that create a sense of satisfaction, foster relationships, strengthen abilities to cope with adversity, and generally promote well-being and development. Two examples are the degree to which a child can express affection in close relationships or respond adaptively to distress in others by expressing concern or offering comfort. Recent studies suggested that the BERS-2 (Epstein 2004) is a promising instrument to assess psychosocial strengths in children with heterogeneous disabilities, including those with DS (e.g., Dieleman et al. 2018b; Sointu et al. 2012). Notably, this research on psychosocial strengths in children also highlighted important variation in the presentation of behavioral and emotional strengths among children with and without special needs (e.g., Dieleman et al. 2018b).
To date, still very little is known about factors involved in the heterogeneity of problems and strengths displayed by youth with disabilities. Quality of parenting may be one important factor that can clarify (at least partly) why some children develop more problems, whereas other children attain high levels of adaptive functioning (e.g., positive relations, vitality, well-being).
In this context, it remains a vital question to what extent the SDT framework on parenting-adjustment relationships can be applied to children with or without a disability. There are two main sets of arguments to assume that there will be fundamental similarities in these SDT-predicted relationships across parents raising a child without a disability and parents raising a child with ASD, CP, and DS. The first set of arguments is theoretical. SDT claims to be universally applicable, postulating that “all humans are active, growth-oriented organisms with innate psychological nutriments that are essential for ongoing psychological growth, integrity, and well-being” (Deci and Ryan 2000, p. 229). This universality claim implies that children with and without special needs have the same basic needs. In 1986, Deci and Chandler wrote a progressive essay on how SDT principles can help to foster motivation in youth with learning disabilities. In this review, they stated that self-determined functioning should be a goal of all education, including special education. In this context, they stated that “all children need to feel competent, to feel autonomous, and to feel loved” (Deci and Chandler 1986, p. 592). No study to date has addressed this universality claim in the context of parenting a child with special needs, but some indirect evidence stems from the few studies evaluating SDT premises in special educational settings. Deci et al. (1992) reported that when parents and teachers provided more autonomy support and involvement, youth with learning disabilities displayed more internal motivation, achievement, and adjustment at school. Shea et al. (2013) evaluated self-ratings of 26 adolescents with high-functioning ASD and found that perceived autonomy support by teachers was related to more intrinsic motives for doing schoolwork and academic self-regulation. A similar finding was reported by Katz and Cohen (2014) in a study on 88 students with intellectual disabilities, where student-perceived teacher autonomy correlated significantly with more autonomous motivation for school.
The second set of arguments stems from the limited empirical research evaluating associations between parenting and developmental outcomes in youth with ASD, CP, or DS, even though these studies used various parenting instruments and predominantly focused on associations with negative, but not positive child outcomes. In families of children with ASD (n = 48), Ventola et al. (2017) recently reported a moderate association between the use of parental psychological control and externalizing problems. Other studies (Boonen et al. 2014; Maljaars et al. 2014) found only weak correlations between parenting and problem behaviors in children with ASD, with some support indicating that demanding, negative controlling parenting is associated with more externalizing behavior. A few longitudinal studies also hint that negative controlling parenting relates to more externalizing problems later in development in youth with ASD (Dieleman et al. 2017; Greenberg et al. 2006). Notably, some studies evaluated the relationship between a more general composite score of positive parenting on the one hand and both problems and prosocial behaviors on the other but did not find significant effects (Boonen et al. 2014; Dieleman et al. 2017; Maljaars et al. 2014).
In the literature on children with CP, a few studies showed associations between need-supportive and need-thwarting parenting behaviors and children’s behavioral problems and well-being. One research group (Aran et al. 2007; Cohen et al. 2008) found that in a subset of 39 children with CP, autonomy-supportive and accepting parenting related to better mental health, higher self-esteem, and less social and emotional difficulties. In this small group of children, parenting was reported to have the only significant effect on psychosocial development, even exceeding any effect of physical disability. Another study showed that parental sensitivity, structuring, and non-intrusiveness were associated with fewer peer problems in 23 children with CP (Barfoot et al. 2017).
Research on relations between parenting and child behaviors among families of children with DS is even more limited. To the best of our knowledge, only one research project has evaluated parenting practices in the context of the child’s behavior in DS (Gilmore and Cuskelly 2012; Gilmore et al. 2016, 2009). This research longitudinally follows 25 mothers of a child with DS and 43 mothers of matched controls. Mothers whose young children with DS displayed many positive characteristics tended to be more autonomy-supportive, more consistent, and less detached in their parenting. By contrast, mothers whose child displayed many negative, socially undesirable behaviors were less likely to support the child’s autonomy and were more detached in their parenting as they avoided or withdrew more often from their child (Gilmore and Cuskelly 2012).
In sum, research has begun to demonstrate associations between important dimensions of parenting and the psychosocial adjustment of children with disabilities. Because the relationship between parenting and child adjustment is inherently reciprocal in nature (Collins et al. 2000; Pinquart 2017), these associations need to be interpreted bidirectionally: children’s problems are likely to elicit less need-supportive and more psychologically controlling parenting, with such parental behavior further reinforcing developmental difficulties in children. Importantly, while research has begun to examine the role of parenting in the context of specific disabilities, only few studies have formally examined similarities and differences in associations between parenting and child behavior across different developmental disabilities.
The present study complements the limited empirical research on the association between parenting and behaviors in youth with disabilities by addressing these relations across four diagnostic groups, including children with ASD, CP, DS, and children with no disability. To date, research has mostly focused on a single condition, with little input from similar research on another disability, precluding the evaluation of disability-specific or overarching relationships. Prior to examining associations between parenting and child outcomes across the four groups of children, for descriptive purposes, we will first explore mean-level group differences, applying a balanced perspective that focuses on both positive and negative dimensions of parenting (responsiveness, autonomy support, psychological control) as well as positive and negative behavioral outcomes (internalizing-externalizing problems and psychosocial strengths). To date, only few studies have examined mean-level differences in parental behaviors across disabilities. In one relevant study, Blacher et al. (2013) compared longitudinal observations of parenting behaviors across mothers of 12 young children with ASD, 9 with CP, and 10 with DS, to mothers of 115 preschoolers without any disability. This study reported that observed negative parenting behavior was higher in mothers of preschoolers with disabilities. Notably, they reported that observed positive parenting behaviors (including aspects of responsiveness and autonomy support) were highest in mothers raising a child with DS. Phillips et al. (2017) compared self-reports of parenting in 35 mothers of school-aged children with DS to 47 mothers of children without a disability. They found that mothers of children with DS used less verbal hostility (related to psychological control) and less reasoning/inductive parenting (related to autonomy support) than mothers of children without disability. The second and primary aim of this study is to address group differences in parenting-adjustment covariation, thereby examining the hypothesis that need-supportive socialization (i.e., responsive and autonomy-supportive parenting) will be associated with more positive outcomes (i.e., psychosocial strengths) and that need-thwarting socialization (i.e., psychological control) will be related to more behavioral difficulties (i.e., both externalizing and internalizing problems). Based on SDT’s universality claim and research in general populations, we hypothesize that these relations will generally be similar across all groups.
Method
Participants
Overall, 409 parents participated in this study: 95 parents had a child with ASD (Mage = 12.5 years), 121 parents had a child with CP (Mage = 10.9 years), 73 parents had a child with DS (Mage = 10.6 years), and 120 parents had a child without any known disability (Mage = 11.8 years). Across all groups, children were on average 11.5 years old (SD = 2.1, age range 7–15 years), and children from the ASD and NO group were on average slightly older than the children from the CP or DS group. All groups included more boys than girls, but this gender imbalance was less pronounced in the DS and NO group (53% and 54% boys) than in the CP and ASD group (66% and 77% boys). Mothers were the main informants in this study (overall, 94%). They were on average 42.5 years old (SD = 5.0 years), while fathers were on average 45.0 years (SD = 5.9 years). Mothers of the DS group were on average older than mothers of the ASD (p = 0.023), CP (p < 0.001), and the NO group (p < 0.001). The majority of participants (overall, 90.7%) have a Belgian nationality, 6.6% a European non-Belgian nationality, and 2.7% a non-European nationality. In line with the recruitment procedure, significantly more parents had a European non-Belgian (i.e., Dutch) nationality in the DS group compared to the other groups (χ2(6) = 73.66, p < 0.001). The majority of parents obtained a degree in higher education (overall, 61.9%), varying from 55.1% in the CP group to 69.7% in the DS group. No significant differences were found in parents’ educational level across groups (χ2(6) = 6.82, p = 0.338). Neither parents’ nationality nor their educational level was related to child or parental behavior (all p’s > 0.050).
In each disability group, there was large variability in severity of disability symptoms. In the ASD group, parents reported on the Social Responsiveness Scale (SRS; Constantino and Gruber 2005) to identify the presence and extent of social difficulties in their child. The reports showed an average total score of 98.42 (SD = 27.9, range 50–168), indicating that the large majority of the children experienced moderate (14.0%, range 60–75) or serious (76.7%, total score higher than 75) difficulties in social responsiveness. In the CP group, parents reported variable motor problems based on the Gross Motor Function Classification System-Family Report (GMFCS-FR; Palisano et al. 2008): 22.2% functioned at level I, 37.6% at level II, 17.9% at level III, 9.4% at level IV, and 12.8% at level V. In the DS group, 34.7% of parents reported that their child had a mild intellectual disability (ID), while 25.3% were labeled with a moderate ID, and 14.6% were reported to have a profound ID. For the remaining 25.4%, parents reported they did not know the ID classification of their child with DS. In the ASD group, 64.2% of the parents provided reports on the intellectual functioning of their child, of which 8.2% (n = 5) indicated that their child had an ID (IQ score lower than 70). Among parents of children with CP, 66.1% of the parents gave information about the intellectual functioning of their child, where a third (33.8%, n = 27) of the parents indicated that their child had an ID. Table 1 shows demographic characteristics of the overall sample by group status.
Procedure
This study uses data from an ongoing larger longitudinal project on psychosocial development in children with and without developmental disabilities in Flanders, Belgium. The ASD group was identified through the registries of four governmental centers providing support-at-home and counseling to families of a child with autism and by placing announcements on websites regarding ASD. Parents of children with CP were recruited through seven Flemish service centers for children with physical disabilities. The DS group included parents of a child with DS, who responded to announcements for this research distributed by the major Flemish family organizations for DS and by specified centers, schools, and support services. Additionally, invitations were also sent via a Facebook group of Belgian and Dutch parents of children with DS. The NO group included parents with a child without any known disability, who participated in the Flemish Study on Temperament and Personality across Childhood (FSTPC; De Pauw 2010), a longitudinal study periodically following the development of a cohort of children born in 2004–2005. This sample was used as a comparison group, even though the age range in this group was narrower than in the disability groups. The study received ethical approval from the Institutional Review Board of the host University and written informed consent was obtained from all participants.
Measures
Responsive Parenting
Parents rated their responsiveness towards their child using the corresponding scale from the Child Report of Parenting Behavior Inventory (CRPBI; Schaefer 1965). This scale consists of 7 items (e.g., “I give my son or daughter a lot of care and attention”) rated on a 5-point Likert scale, ranging from 1 (Completely not true) to 5 (Completely true). The CRPBI is a well-validated instrument in mainstream populations (e.g., Pinquart 2017) and also showed good reliability in youth with CP (Cohen et al. 2008). Cronbach α’s ranged from 0.63 (DS) to 0.80 (ASD).
Autonomy-Supportive Parenting
Parents were administered a reduced version of the well-validated Autonomy Support Scale of the Perceptions of Parents Scale (POPS; Grolnick et al. 1991). Two items of the original 7-item scale, which have to be reverse-scored according to the scoring instruction, were excluded as they tap into controlling parenting rather than into autonomy-supportive parenting (e.g., “I insist to do everything my way.”). This version includes 5 items (e.g., “I am usually willing to consider things from my child’s point of view”), which were scored on a 5-point Likert scale ranging from 1 (Completely not true) to 5 (Completely true). The POPS has been validated for use in parents of children with and without special needs (Dieleman et al. 2018a; Soenens et al. 2007). Cronbach α’s ranged from 0.60 (ASD) to 0.77 (NO).
Psychologically Controlling Parenting
Parents filled out the 8 items of the Psychological Control Scale (PCS; Barber 1996), which addresses several key aspects of psychologically controlling parenting, including guilt-induction (e.g., “I blame my child for other family members’ problems”), intrusiveness (e.g., “I try to change how my child feels or thinks about things”), and love withdrawal (e.g., “I am less friendly with my child when s/he does not see things my way”). Items are scored on a 5-point Likert scale, ranging from 1 (Completely not true) to 5 (Completely true). This instrument has been validated and frequently used in past research with and without children with disabilities (Dieleman et al. 2018a; Mabbe et al. 2016). Cronbach α’s ranged from 0.62 (DS) to 0.79 (CP).
Internalizing and Externalizing Problems
Emotional and behavioral problems were assessed with the Child Behavior Checklist (CBCL; Achenbach 2001). Using a 3-point Likert scale, parents indicated how often a child displayed specific behavior over the past 6 months, ranging from 0 (Never) to 2 (Often). The broadband scale internalizing problems comprised two scales: anxious/depressed (13 items; e.g., “cries a lot”) and withdrawn/depressed (8 items; e.g., “enjoys little”). We did not include somatic complaints, as we considered that, given to the specific nature of the disability groups, medical problems could falsely overestimate this internalizing score, especially within the CP and DS groups. The broadband scale externalizing problems included two scales: rule-breaking (17 items; e.g., “lies and cheats”) and aggressive behavior (18 items; e.g., “destroys things belonging to others”). The CBCL previously showed to be adequate for examining behavioral problems in youth with and without a disability (e.g., van Gameren-Oosterom et al. 2011; Holtmann et al. 2007). In this study, Cronbach α’s ranged from 0.80 (DS) to 0.89 (ASD) for internalizing and from 0.83 (NO) to 0.92 (ASD) for externalizing problems.
Child Psychosocial Strengths
Parents rated their child’s psychosocial strengths using the Behavioral and Emotional Rating Scale-2 (BERS-2; Epstein 2004), a strengths-based assessment scale specifically designed for addressing positive behavioral qualities of children in vulnerable situations. Each item is rated on a 5-point Likert scale, ranging from 1 (Completely not true) to 5 (Completely true). The overall strengths index comprises four subscales: Interpersonal Strengths (15 items; e.g., “admits mistakes”), Family Involvement (10 items; “trusts a significant person with his/her life”), Intrapersonal Strengths (11 items; “demonstrates a sense of humor”), and Affective Strengths (7 items; “expresses affection for others”). The BERS-2 was developed to be broadly applicable, and recently, scholars have successfully used this questionnaire in research on children with disabilities (e.g., Dieleman et al. 2018b; Sointu et al. 2012). Cronbach α’s ranged from 0.92 (ASD) to 0.96 (NO).
Data Analyses
Given the non-normal distribution of problem behaviors in each group, Kruskal-Wallis H tests were conducted to examine group differences in both parenting and psychosocial behavioral outcomes. The associations between parenting and behavioral problems/strengths were examined by bivariate correlation analyses within each group. Multi-group structural equation modeling (SEM) using Mplus 8 (Muthén and Muthén 1998–2012) was performed to evaluate the SDT-based premises that need-supportive parenting is associated with psychosocial strengths, whereas need-frustrating parenting is linked with behavioral difficulties in and across all groups. Missing values were missing completely at random, as the normed χ2/df (4489.10/3525) was 1.27 (i.e., smaller than the recommended cutoff of 2; Ullman 2001). Hence, model parameters were estimated using the full information maximum likelihood procedure (Schafer and Graham 2002). When conducting χ2-difference tests using the MLR estimator, χ2 was adjusted using the Satorra-Bentler scaling correction (Satorra and Bentler 1994). An item-to-construct balance method was used for constructing parcels with regard to the three parenting constructs. Within this method, an item with the highest item-scale correlation is paired with the item with the lowest item-scale correlation. Subsequently, the next highest and next lowest items were paired in a second parcel, and so on (Landis et al. 2000). This method was also used with regard to behavioral problems, since the model did not converge using the CBCL subscales as parcels and more than two indicators are recommended per construct (Little 2013). This item-to-construct balance method at the item-level resulted in three parcels for each parenting scale and in five parcels for internalizing and for externalizing problems. Two CBCL items (“sets fires,” “uses drugs for nonmedical purposes”) were excluded from the analyses, as no parent endorsed these items. As the conceptual construct of psychosocial strengths is multidimensional in nature, we used the internal-consistency approach (Kishton and Widaman 1994), using the four BERS subscales as indicators of the latent factor for psychosocial strengths (see Fig. 3).
Results
Group Differences in Parenting, Problem Behaviors, and Psychosocial Strengths
Kruskal-Wallis H tests were conducted to examine group differences in both parenting dimensions and psychosocial behavioral outcomes (Table 2). In all groups, we found relatively high and comparable levels of responsive and autonomy-supportive parenting as well as low levels of psychologically controlling parenting. These analyses revealed five significant, yet modest group differences (Fig. 1). Levels of responsive parenting were highest in parents of a child with CP, and significantly higher than reported in the NO (dCP-NO = 0.35) and ASD group (dCP-ASD = 0.39). As expected, levels of autonomy support were highest in parents of children in the NO-disability group, but they were only slightly higher than in parents raising a child with ASD or with CP. Only parents of a child with DS provided significantly less autonomy support than parents of a child without a disability (dNO-DS = 0.60). Levels of psychologically controlling were markedly lower than need-supportive parenting behaviors. Again, these levels were highest in parents of a child with NO disability, followed by parents raising a child with ASD, CP, and DS. Notably, differences were only statistically significant between parents of a child with NO disability and of a child with CP (dNO-CP = 0.29) and with DS (dNO-DS = 0.50).

Group differences in parenting behaviors. *p < 0.05. ASD, autism spectrum disorder; CP, cerebral palsy; DS, Down syndrome; NO, without any known disability
In contrast to the modest mean-level differences in parenting, analyses revealed striking group differences in psychosocial outcomes: five of six pairwise group comparisons were significant for children’s internalizing and externalizing problems, as well as for psychosocial strengths (Fig. 2). As anticipated, children with ASD showed the most challenging profile, with on average the highest levels of internalizing and externalizing problems and the lowest levels of strengths across the four groups. Effect sizes were large to very large in magnitude for internalizing (dASD-CP = 0.99, dASD-NO = 1.29, dASD-DS = 1.48), moderate to very large for externalizing problems (dASD-DS = 0.64, dASD-CP = 0.70, dASD-NO = 1.31), and very large for psychosocial strengths (dASD-NO = 1.92, dASD-CP = 1.30, dASD-DS = 1.20). Children in the NO-disability group showed, as expected, the least externalizing problems and the most psychosocial strengths. Interestingly, parents of children with DS reported the lowest internalizing problems, but this was not significantly lower than in the NO-disability group. Children with CP, however, showed a higher risk to develop internalizing problems than the NO (dCP-NO = 0.34) and DS group (dCP-DS = 0.53). Both children with DS (dDS-NO = 0.81) and with CP (dCP-NO = 0.65) had comparable yet elevated levels of externalizing problems. Children with DS and CP also had comparable levels of psychosocial strengths, which were only moderately lower than children with no disability (dDS-NO = − 0.51, dCP-NO = − 0.59).

Group differences in internalizing and externalizing problems and psychosocial strengths. *p < 0.05. ASD, autism spectrum disorder; CP, cerebral palsy; DS, Down syndrome, NO, without any known disability
Associations Between Parenting and Psychosocial Outcomes Across Groups
As Kruskal-Wallis H and chi-square tests identified group differences in child age (H(3) = 41.87, p < 0.001), child gender (χ2(3) = 16.44, p < 0.001), and age of the informant (H(3) = 26.02, p < 0.001), correlations were controlled for these demographic differences. Differences between groups were evaluated by pairwise comparisons of the magnitude of the correlations, after Fisher r-to-z-transformation. None of the 90 possible bivariate pairwise comparisons reached statistical significance (p < 0.001). This finding indicated a rather consistent pattern of covariation across the four groups (Table 3).
In each group, sizeable yet moderate correlations between responsive and autonomy-supportive parenting were found. Psychological control was negatively and moderately related to responsiveness in each group, but surprisingly not to autonomy support in the three disability groups. In the NO-disability group, there was a moderate negative correlation (r = − 0.30). As anticipated, sizeable positive correlations between the two problem scales and negative correlations between behavioral problems and psychosocial strengths were found in each group. Regarding parenting-adjustment covariation, evidence for differential relations was found in each group, yielding modest-to-moderate correlations. In all groups, psychologically controlling parenting was associated with more externalizing problems (rs ranging from 0.23 in children with ASD to 0.45 in children with DS). In children with CP and children with no disability, both responsiveness and autonomy support were related to more psychosocial strengths. In children with DS, a sizeable association (r = 0.40) between autonomy support and psychosocial strengths was replicated, but the correlation with responsiveness did not reach significance. In children with ASD, we found that responsiveness but not autonomy support was associated with more strengths. Notably, internalizing problems were not associated with any of the parenting dimensions, except for a modest relation in the ASD group, where more autonomy-supportive parenting was related to more internalizing problems (r = 0.25).
Structural Relations Between Parenting Behavior and Psychosocial Outcomes Across Groups
In a first step, we examined measurement equivalence of the scales across the four groups, creating two separate measurement models: one for the parenting variables and one for the behavioral variables. In the first measurement model on parenting, a fully unconstrained model where all factor loadings were allowed to vary between groups was compared to a constrained model where the factor loadings were fixed to be equal across the groups. Results showed that the constrained model fitted the data equally well as the unconstrained model (ΔSBS-χ2(18) = 20.09, p = 0.330), indicating factorial invariance (Meredith 1993) of the three parenting scales across groups. In the second measurement model on the behavioral variables, the fully unconstrained model fitted the data better than the model with constrained factor loadings (ΔSBS-χ2(33) = 89.24, p < 0.001). Further analyses determined which loadings differed across groups. Three factor loadings differed significantly between groups: internalizing problems on the third and fifth parcel, and externalizing problems on the second parcel. Hence, the final measurement model consisted of constrained factor loadings for the parenting variables and three freely estimated factor loadings for the behavior variables.
In a second step, the structural model was tested, comparing constrained models to unconstrained models for each behavioral variable separately, in order to not overload the model. These analyses indicated no significant differences in the behavioral variables. The partially constrained model with unconstrained correlations between the latent variables had a significantly better fit than the constrained model with constrained paths between the latent variables (ΔSBS-χ2(18) = 51.21, p < 0.001). Further analyses indicated that this difference was due to a significantly stronger correlation between internalizing and externalizing problems in the CP group compared to the other groups (ΔSBS-χ2(3) = 15.60, p < 0.001) and a significantly stronger correlation between externalizing behavior and strengths in the ASD group compared to the other groups (ΔSBS-χ2(3) = 17.578, p < 0.001). Additionally, interaction effects between the parenting domains were explored across and within the study groups, but no significant interactions were found.
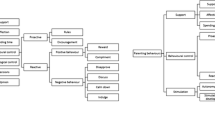
In a final step, we also controlled for the influence of the demographic variables child age, child gender, and informant age. Only child age had a significant effect on the behavioral variables. Overall, older children with CP and DS showed more strengths, and older children with CP and ASD scored lower on externalizing than younger children. Older children with CP also showed more internalizing problems. No age effect was found in the NO-disability group. Results from the final model, in which we controlled for these effects (χ2(1199) = 1863.14, p < 0.001; CFI = 0.852, SRMR = 0.108, TLI = 0.841, RMSEA = 0.077), are shown in Fig. 3. This final model (Fig. 3) identified three significant associations that held across all four groups. The first relationship indicated that, in all groups, higher levels of psychologically controlling parenting were positively related to externalizing problems. A relationship between parenting and internalizing problems did not emerge. The second and third significant relationship showed that higher levels of responsiveness as well as higher levels of autonomy support related to more strengths in all groups. Hence, this model supports the SDT-based premises in all groups. Only the anticipated relationship between need-thwarting parenting and internalizing problems was not corroborated.

Final structural model depicting the relation between parenting behavior and psychosocial functioning of the child. * = p < 0.050, ** = p < 0.010, *** = p < 0.001. Resp, responsive parenting; AutSup, autonomy-supportive parenting; PsyCon, psychologically controlling parenting. Unstandardized coefficients (standard error) are reported on the arrows that indicate direct effects between parenting behavior and psychosocial outcomes. The six latent variables and their indicators, displayed by three, four, or five parcels, are represented in respectively oval and square boxes. We estimated the correlations between the latent variables but these are not presented for reasons of parsimony
Discussion
Although associations between parenting and behavioral child outcomes have been extensively studied in mainstream populations, research on these relations in children with special needs, such as ASD, CP, and DS, is still in its infancy. The last decade has witnessed a growing interest in family dynamics in these groups, yet most studies have focused on the elevated levels of stress in parents of children with disabilities (e.g., Hayes and Watson 2013; Pinquart 2013; Yorke et al. 2018) and not on parenting behaviors (Dieleman et al. 2017; Maljaars et al. 2014; Phillips et al. 2017). Moreover, the limited, available empirical research has mostly focused on one specific disability, thereby limiting the possibilities to identify potential disability-specific parenting dynamics. Also, these few studies commonly relied on small to modest sample sizes (e.g., Blacher et al. 2013; Phillips et al. 2017; Ventola et al. 2017).
Exploring Differences Across Groups
The first aim of this study was to explore mean-level differences in parenting, behavioral problems, and psychosocial strengths across the four study groups. All included instruments were originally developed for mainstream populations of children and adolescents, but acceptable to excellent internal consistencies were found for all scales in this study, warranting their use in research with special needs populations.
Strikingly, levels of parenting behaviors did not vary widely between groups. In each group, parents reported high levels of responsiveness and autonomy support, and low levels of psychologically controlling parenting. Nevertheless, some small-to-modest group differences were found, yielding intriguing indications on disability-specific aspects of parenting. First, parents of children with CP reported significantly more responsiveness than parents of children with NO disability or children with ASD. Even though these effects were small, they mesh with observations that children with CP often develop intense and close relations with their parents, so that parents are strongly attuned to their child’s needs for both physical and emotional support (Whittingham et al. 2013). Parents of children with DS also reported high levels of responsive parenting, but these were not significantly different than in other groups. Hence, this study (based on self-report) does not confirm Blacher et al.’s (2013) suggestion (based on observations) that children with DS may evoke more positive parenting behaviors in parents than children with other disabilities, such as autism, given the presumed more positive personality characteristics (i.e., being cheerful and friendly) in DS.
Second, parents in the DS group reported significantly lower levels of autonomy support than parents in the NO group. This moderate effect is in line with suggestions emerging from earlier studies showing that parents of young children with DS tend to be more directive than parents whose children are developing without disabilities (de Falco et al. 2011; Glenn et al. 2001). However, this is not a consistent finding as some studies found no significant differences in directiveness and autonomy support (e.g., Gilmore et al. 2009). A more in-depth examination with qualitative interviews clarified that even though mothers of children with DS reported that they held strong aspirations for their child’s future autonomy and independence, they often felt that their capacity to promote autonomy was constrained by a range of child and family factors, such as concerns about the child’s safety, difficulties with communication, competing family responsibilities, sensory issues, or sibling influences (Gilmore et al. 2016). Future research should further replicate and evaluate these potential barriers for autonomy support towards children with DS, in comparison to other disability conditions. In this regard, this study found no differences in autonomy support between the CP, ASD, and NO group, even though parents might face diverse challenges in promoting autonomy of their child with or without a disability.
Third, parents in both the DS and the CP group reported lower levels of psychological control than parents in the NO group. Interestingly, the finding for DS corroborates a study by Phillips et al. (2017) who observed less verbal hostility in mother-child interactions in families with a child with DS compared to controls. These authors related this finding to the presumed more characteristically pleasant personalities of the child with DS, even hypothesizing that this unique phenotype in DS may lead to the use of less coercion in these families, compared to children with other disabilities. Again, this intriguing hypothesis warrants further inquiry, preferably by studies addressing both quantitative and qualitative differences in parenting and simultaneously evaluating these processes in and across multiple disabilities.
Although not a central aim of this study, our findings further confirmed that mean levels of both internalizing, externalizing and psychosocial strengths strongly varied across groups, a finding contrasting sharply with the minor mean-level differences in parenting. In line with previous research (De Pauw et al. 2011; Maljaars et al. 2014), children with ASD were rated with the most challenging behavioral profile, showing the most internalizing and externalizing problems and the least psychosocial strengths. These large behavioral differences partly reflect diagnostic features of ASD (e.g., lower interpersonal skills), yet also corroborate the finding that children with ASD are at increased risk to developing more anxious, withdrawn, depressive as well as more rule-breaking and aggressive behaviors. However, the large variances in these behavioral scales suggested that it would be unwarranted to create stereotypes of children with a disability based on these children’s mean-level profile. Instead, these large variances call for a consideration of the unique profile of behavioral difficulties and strengths of each individual with ASD.
Mean-level differences corroborate previous findings that children with CP show elevated levels of externalizing and to a lesser extent, internalizing problems compared to controls (Vrijmoeth et al. 2012). Our cross-disability comparison also revealed that children with DS were rated with the lowest levels of internalizing problems of all groups, which is also in line with prior findings (van Gameren-Oosterom et al. 2011). This lower score might reflect true differences, but an alternative explanation might be that children with DS have less abilities to express these symptoms, which makes it more difficult for parents to recognize these symptoms. Notably, the mean score on externalizing problems in children with DS was (just as in children with CP) more than twice as high than the mean score in the NO group. This finding confirms that also children with DS are at increased risk to develop behavioral difficulties (Dieleman et al. 2018b; van Gameren-Oosterom et al. 2011). Yet, also in these groups, there was large variation in parent’s reports of problems.
In addition to its focus on behavioral problems, this study addressed psychosocial strengths in and across the four groups. We found that in all four groups, parents reported relatively high levels of strengths in their children in spite of relatively large group differences. Children from the NO group scored only about 0.5 SD higher than children with DS and CP, but 1.5 SD higher than children with ASD. This research provides additional support that addressing a child’s strengths is important in both research and practice, as it might provide crucial keys to support children and their families. Focusing on a child’s strengths, as well as his/her behavioral difficulties, not only provides a more holistic view of the child but can also facilitate feelings of empowerment and positivity in support interventions (Dieleman et al. 2018b).
Testing an SDT-Based Model of Parenting-Adjustment Associations
The second, and most important, aim of this study was to address SDT-based premises on how the three parenting dimensions relate to problem behaviors and postulated strengths, in and across the four groups. Based upon SDT’s universality claim, we expected the emergence of two differential pathways in all four groups: a “bright” pathway indicating that need-supportive parenting is associated with more psychosocial strengths, versus a “dark” pathway showing that need-thwarting parenting is associated with more problem behaviors (Soenens et al. 2017; Vansteenkiste and Ryan 2013).
Overall, based upon both correlational analyses and multi-group SEM modeling, this study provides cross-disability support for these two differential paths. Pairwise comparisons of correlations across groups yielded no significant differences, providing first evidence for similarity in the pattern of parenting-adjustment associations across groups. Multi-group SEM analyses further supported measurement invariance for both parenting and behavioral variables. These multi-group SEM analyses revealed three significant paths, uncovering a “bright” and “dark” pathway. In all groups, both indicators of contextual need-support, responsiveness and autonomy support, related to more psychosocial strengths, whereas the indicator for need-thwarting parenting, psychological control, was associated with more externalizing problems in the child. In contrast to other studies (Barber and Harmon 2002; Pinquart 2016), this study did not find a significant association between parenting and internalizing problems, except for a small and counter-intuitive correlation in the ASD group, where more autonomy support related to more internalizing problems. Previous research on the association between parental control and child outcomes in children with developmental delays showed mixed findings (Green et al. 2014). These mixed findings may be partially accounted by the potential differences between types of parental control (Grolnick and Pomerantz 2009). On the one hand, constructive control, which is described as “structure” in the SDT literature, is related to the child’s current focus or goal (Soenens et al. 2017). This type of control is suggested to be beneficial, especially for children who need structure, prompting, and direction because of their disability. On the other hand, intrusive or interfering control, which is unrelated to the child’s goal, is suggested to be detrimental (Green et al. 2014). The counterintuitive correlation in the ASD group might be related to a disability-specific effect, where parenting behavior that might be considered developmentally appropriate for most children, might be experienced as less supportive for a child with ASD. For instance, autonomy-supportive parenting behavior that encourages initiative, by providing choice and stimulating dialogue, might be experienced as more stress-inducing for a child with ASD, who is likely to need more structure and direction. More research is needed to replicate and unravel the meaning of this possible relation in raising a child with ASD. Furthermore, associations between parenting and internalizing problems might be underestimated when relying only on parent reports, because internalizing problems sometimes remain unnoticed by parents (Kolko and Kazdin 1993; van de Looij-Jansen et al. 2011). Therefore, future research would do well to include also child reports of parenting and child behavior.
Overall, this study corroborates associations between need-supportive parenting and beneficial outcomes and associations of need-thwarting parenting with psychosocial problems in all children, regardless of the diagnostic group. Consequently, this study provides unique evidence for the universality claim of SDT in the context of parenting a child with special needs. As such, it complements the few conceptual and empirical SDT-based studies on the benefits of basic need satisfaction in special education settings (Deci et al. 1992; Deci and Chandler 1986; Katz and Cohen 2014; Shea et al. 2013). Importantly, the associations obtained in this study need to be interpreted from a transactional perspective on parenting. That is, need-supportive parenting is likely to not only foster children’s strengths but also to be affected by these strengths. It is easier for parents to be patient and attuned to the child’s needs when the child is socially competent and emotionally stable. Similarly, psychologically controlling parenting and externalizing problems are likely to mutually reinforce one another in a vicious negative cycle (Pinquart 2017). Moreover, this study adds cross-disability evidence for a “dark” pathway, revealing that guilt induction, shaming, and love withdrawal rather strongly relates to behavioral problems in all groups. Also, it sheds light on a “bright” pathway in and across children with and without ASD, CP, and DS, indicating that sensitive, warm parents who seek to attune their parenting to the developmental needs of their child, and actively searching for opportunities to promote autonomy, also recognize more strengths in their child.
These findings have both theoretical and practical relevance, as they identify SDT as a valuable theory to further examine motivational dynamics to promote well-being and quality of life of both children with special needs and their families. As SDT-based interventions in mainstream populations now suggest that encouraging parents to engage in need-supportive parenting is beneficial for both parents’ and children’s mental health (Allen et al. 2018; Joussemet et al. 2014), these interventions might be beneficial for families with children with a disability as well. Additionally, these findings underscore the importance for parents of children with special needs to be responsive and autonomy-supportive towards their child, even though they are frequently challenged to cope with difficult child behavior. In order to better understand these findings, future research could examine more in depth how parents’ expectations of their child and coping strategies relate to their parenting behavior (Heiman 2002).
Limitations and Future Directions
When interpreting the current results, some limitations need to be taken into account. First, the generalizability of findings is limited by the specific choice of parenting and behavior parent-report instruments and by relying on mothers as the primary source of information. Future research should replicate whether these relations also generalize across alternative measures of parenting, such as observations, and other indicators of behaviors and well-being. Also, future research could benefit from including multiple informants, especially fathers, as prior research especially highlighted the significant impact of paternal parenting on child development (Prinzie et al. 2009). Furthermore, the majority of participating parents had a Belgian nationality, were highly educated, and participated voluntarily, which might impact the generalizability of the findings as well. For instance, because financially well-resourced parents generally face fewer stressors, it might be easier for them to display stably high levels of warm parenting (Taraban and Shaw 2018). Future research hence should attempt to collect more diverse samples of parents.
Second, this study did not formally tap into the mediating mechanism of basic psychological need satisfaction/frustration in the relation between socialization contexts and behavioral outcomes. Future studies should actually assess such experiences of need satisfaction or need frustration in children with developmental disabilities. Recently, a self-report questionnaire operationalizing satisfaction and frustration with the three basic SDT needs has become available for adults with mild intellectual disability (Frielink et al. 2016), yet more work is needed to address need-satisfaction in younger age groups with disabilities.
Third, it could be interesting to further explore the impact of other factors that previously have been shown to regulate or moderate differences in how parenting behavior relates to psychosocial functioning, such as child temperament and personality (De Pauw et al. 2011; Mabbe et al. 2016), parental personality (Prinzie et al. 2009), parental psychological functioning, stress, and support (Taraban and Shaw 2018). Given the elevated levels of parental stress among parents of children with disabilities (e.g., Hayes and Watson 2013; Phillips et al. 2017; Pinquart 2013), parental stress might be a particularly important mediator in the relation between parenting and child behavior within these families (Dieleman et al. 2018a; Yorke et al. 2018). Furthermore, the role of intellectual disability could not be comprehensively addressed in this study, as we primarily relied upon parent reports and not all parents provided IQ information of their child. In future research, more objective assessments of intellectual functioning should be included.
Finally, the cross-sectional design of this study allows no causal interpretations of the relations between parenting and child behavior. Most likely, these relations are bidirectional in nature, with parenting not only affecting children’s development, but with children’s behavior also eliciting specific parental behaviors. Future research with prospective longitudinal designs should evaluate this fundamental issue of transactional developmental effects in and across children with and without disabilities. Previous research confirmed the bidirectional relationships between SDT-based parenting behavior and child behavior problems in youth with ASD (Dieleman et al. 2017), but no study to date explored these processes in families of children with CP and DS.
To conclude, this study showed that parenting is associated with behavioral outcomes in large samples of children with and without ASD, CP, and DS. Our analyses revealed only minor mean-level differences in parenting behaviors across the study groups, in spite of large differences in children’s behavioral presentations. In addition, our findings provide cross-disability support for the similarity of parenting-adjustment relations across children with and without ASD, CP, and DS. In all groups, two differential paths emerged: need-supportive parenting (responsiveness and autonomy support) was associated with more positive outcomes (psychosocial strengths) and need-thwarting parenting (psychological control) was related with more behavior difficulties (externalizing, but not internalizing problems). Overall, this study suggests that Self-Determination Theory may be a valuable framework to further study parenting dynamics in special needs families. Corroborating the beneficial links of need-supporting parenting and the detrimental association of need-thwarting parenting and psychosocial functioning, this study provides initial support to SDT’s universality claim that “all children need to feel loved, autonomous and competent” (Deci et al. 1992), including those growing up with special needs.
References
Achenbach, T. M. (2001). Manual for the child behavior checklist/6-18 and 2001 profile. Burlington: University of Vermont.
Allen, E. S., Grolnick, W. S., & Córdova, J. V. (2018). Evaluating a self-determination theory-based preventive parenting consultation: the parent check-in. Journal of Child and Family Studies, 28, 732–743.
Aran, A., Shalev, R. S., Biran, G., & Gross-Tsur, V. (2007). Parenting style impacts on quality of life in children with cerebral palsy. Journal of Pediatrics, 151, 56–60. https://doi.org/10.1016/j.jpeds.2007.02.011.
Barber, B. K. (1996). Parental psychological control: revisiting a neglected construct. Child Development, 67, 3296–3319. https://doi.org/10.1111/j.1467-8624.1996.tb01915.
Barber, B. K., & Harmon, E. L. (2002). Violating the self: parental psychological control of children and adolescents. In B. K. Barber (Ed.), Intrusive parenting: how psychological control affects children and adolescents (pp. 15–52). Washington, DC: American Psychological Association.
Barfoot, J., Meredith, P., Ziviani, J., & Whittingham, K. (2017). Parent-child interactions and children with cerebral palsy: an exploratory study investigating emotional availability, functional ability, and parent distress. Child: Care, Health and Development, 43, 812–822. https://doi.org/10.1111/cch.12493.
Blacher, J., Baker, B. L., & Kaladjian, A. (2013). Syndrome specificity and mother–child interactions: examining positive and negative parenting across contexts and time. Journal of Autism and Developmental Disorders, 43, 761–774. https://doi.org/10.1007/s10803-012-1605.
Boonen, H., Maljaars, J., Lambrechts, G., Zink, I., Van Leeuwen, K., & Noens, I. (2014). Behavior problems among school-aged children with autism spectrum disorder: associations with children’s communication difficulties and parenting behaviors. Research in Autism Spectrum Disorders, 8, 716–725. https://doi.org/10.1016/j.rasd.2014.03.008.
Brenning, K., Soenens, B., Van Petegem, S., & Vansteenkiste, M. (2015). Perceived maternal autonomy support and early adolescent emotion regulation: a longitudinal study. Social Development, 24, 561–578. https://doi.org/10.1111/sode.12107.
Cohen, E., Biran, G., Aran, A., & Gross-Tsur, V. (2008). Locus of control, perceived parenting style, and anxiety in children with cerebral palsy. Journal of Developmental and Physical Disabilities, 20, 415–423. https://doi.org/10.1007/s10882-008-9106-8.
Collins, W. A., Maccoby, E. E., Steinberg, L., Hetherington, E. M., & Bornstein, M. H. (2000). Contemporary research on parenting: the case for nature and nurture. American Psychologist, 55, 218. https://doi.org/10.1037/0003-066X.55.2.218.
Constantino, J., & Gruber, C. (2005). The social responsiveness scale manual. Los Angeles: Western Psychological Services.
Costa, S., Cuzzocrea, F., Gugliandolo, M. C., & Larcan, R. (2016). Associations between parental psychological control and autonomy support, and psychological outcomes in adolescents: the mediating role of need satisfaction and need frustration. Child Indicators Research, 9, 1059–1076. https://doi.org/10.1007/s12187-015-9353-z.
Davidov, M., & Grusec, J. E. (2006). Untangling the links of parental responsiveness to distress and warmth to child outcomes. Child Development, 77, 44–58. https://doi.org/10.1111/j.1467-8624.2006.00855.
de Falco, S., Venuti, P., Esposito, G., & Bornstein, M. H. (2011). Maternal and paternal pragmatic speech directed to young children with Down syndrome and typical development. Infant Behavior & Development, 34, 161–169. https://doi.org/10.1016/j.infbeh.2010.12.002.
De Pauw, S. S. W. (2010). The contribution of temperament and personality to problem behavior in children and adolescents. Doctoral dissertation, Ghent University, Ghent, Belgium.
De Pauw, S. S. W., Mervielde, I., Van Leeuwen, K. G., & De Clercq, B. J. (2011). How temperament and personality contribute to the maladjustment of children with autism. Journal of Autism and Developmental Disorders, 41, 196–212. https://doi.org/10.1007/s10803-010-1043-6.
Deci, E. L., & Chandler, C. L. (1986). The importance of motivation for the future of the LD field. Journal of Learning Disabilities, 19, 587–594.
Deci, E. L., & Ryan, R. M. (2000). The “what” and “why” of goal pursuits: human needs and the self-determination of behavior. Psychological Inquiry, 11, 227–268. https://doi.org/10.1207/S15327965PLI1104_01.
Deci, E. L., Hodges, R., Pierson, L., & Tomassone, J. (1992). Autonomy and competence as motivational factors in students with learning disabilities and emotional handicaps. Journal of Learning Disabilities, 25, 457–471.
Dieleman, L. M., De Pauw, S. S., Soenens, B., Beyers, W., & Prinzie, P. (2017). Examining bidirectional relationships between parenting and child maladjustment in youth with autism spectrum disorder: a 9-year longitudinal study. Development and Psychopathology, 29, 1199–1213. https://doi.org/10.1017/S0954579416001243.
Dieleman, L. M., De Pauw, S. S. W., Soenens, B., Mabbe, E., Campbell, R., & Prinzie, P. (2018a). Relations between problem behaviors, perceived symptom severity and parenting in adolescents and emerging adults with ASD: the mediating role of parental psychological need frustration. Research in Developmental Disabilities, 73, 21–30. https://doi.org/10.1016/j.ridd.2017.12.012.
Dieleman, L. M., De Pauw, S. S. W., Soenens, B., Van Hove, G., & Prinzie, P. (2018b). Behavioral problems and psychosocial strengths: unique factors contributing to the behavioral profile of youth with Down syndrome. American Journal on Intellectual and Developmental Disabilities, 123, 212–227. https://doi.org/10.1352/1944-7558-123.3.212.
Epstein, M. H. (2004). Behavioral and emotional rating scale-2nd edition. A strengths-based approach to assessment. Austin: PRO-ED.
Epstein, M. H., & Sharma, J. (1998). Behavioral and emotional rating scale: a strength-based approach to assessment. Austin: PRO-ED.
Frielink, N., Schuengel, C., & Embregts, P. J. C. M. (2016). Psychometric properties of the Basic Psychological Need Satisfaction and Frustration Scale – Intellectual Disability (BPNSFS-ID). European Journal of Psychological Assessment, 35(1), 37–45. https://doi.org/10.1027/1015-5759/a000366.
Gilmore, L., & Cuskelly, M. (2012). Parenting satisfaction and self-efficacy: a longitudinal study of mothers of children with Down syndrome. Journal of Family Studies, 18, 28–35. https://doi.org/10.5172/jfs.2012.18.1.28.
Gilmore, L., Cuskelly, M., Jobling, A., & Hayes, A. (2009). Maternal support for autonomy: relationships with persistence for children with down syndrome and typically developing children. Research in Developmental Disabilities, 30, 1023–1033. https://doi.org/10.1016/j.ridd.2009.02.005.
Gilmore, L., Ryan, B., Cuskelly, M., & Gavidia-Payne, S. (2016). Understanding maternal support for autonomy in young children with Down syndrome. Journal of Policy and Practice in Intellectual Disabilities, 13, 92–101. https://doi.org/10.1111/jppi.12163.
Glenn, S. M., Dayus, B., Cunningham, C., & Horgan, M. (2001). Mastery motivation in children with Down syndrome. Down Syndrome Research and Practice, 10, 53–60.
Green, S., Caplan, B., & Baker, B. (2014). Maternal supportive and interfering control as predictors of adaptive and social development in children with and without developmental delays. Journal of Intellectual Disability Research, 58, 691–703.
Greenberg, J. S., Seltzer, M. M., Hong, J., & Orsmond, G. I. (2006). Bidirectional effects of expressed emotion and behavior problems and symptoms in adolescents and adults with autism. American Journal on Mental Retardation, 111, 229–249.
Grolnick, W. S., & Pomerantz, E. M. (2009). Issues and challenges in studying parental control: toward a new conceptualization. Child Development Perspectives, 3, 165–170.
Grolnick, W. S., Ryan, R. M., & Deci, E. L. (1991). Inner resources for school-achievement: motivational mediators of children’s perceptions of their parents. Journal of Educational Psychology, 83, 508–517. https://doi.org/10.1037/0022-0663.83.4.508.
Grolnick, W. S., Levitt, M., & Caruso, A. (2018). Adolescent autonomy in context: facilitating parenting in different cultures, domains, and settings. In B. Soenens, M. Vansteenkiste, & S. Van Petegem (Eds.), Autonomy in adolescent development (pp. 110–134). Psychology Press.
Hayes, S. A., & Watson, S. L. (2013). The impact of parenting stress: a meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. Journal of Autism and Developmental Disorders, 43, 629–642. https://doi.org/10.1007/s10803-012-1604-y.
Heiman, T. (2002). Parents of children with disabilities: resilience, coping, and future expectations. Journal of Developmental and Physical Disabilities, 14, 159–171.
Holtmann, M., Bolte, S., & Poustka, F. (2007). Autism spectrum disorders: sex differences in autistic behaviour domains and coexisting psychopathology. Developmental Medicine and Child Neurology, 49, 361–366.
Joussemet, M., Landry, R., & Koestner, R. (2008). A self-determination theory perspective on parenting. Canadian Psychology-Psychologie Canadienne, 49, 194–200. https://doi.org/10.1037/a0012754.
Joussemet, M., Mageau, G. A., & Koestner, R. (2014). Promoting optimal parenting and children’s mental health: a preliminary evaluation of the how-to parenting program. Journal of Child and Family Studies, 23, 949–964. https://doi.org/10.1007/s10826-013-9751-0.
Katz, I., & Cohen, R. (2014). Assessing autonomous motivation in students with cognitive impairment. Journal of Intellectual and Developmental Disability, 39, 323–332. https://doi.org/10.3109/13668250.2014.934791.
Kishton, J. M., & Widaman, K. F. (1994). Unidimensional versus domain representative parceling of questionnaire items: an empirical example. Educational and Psychological Measurement, 54, 757–765.
Kolko, D. J., & Kazdin, A. E. (1993). Emotional/behavioral problems in clinic and nonclinic children: correspondence among child, parent and teacher reports. Journal of Child Psychology and Psychiatry, 34, 991–1006.
Landis, R. S., Beal, D. J., & Tesluk, P. E. (2000). A comparison of approaches to forming composite measures in structural equation models. Organizational Research Methods, 3, 186–207. https://doi.org/10.1177/109442810032003.
Little, T. D. (2013). Longitudinal structural equation modeling. New York: Guilford press.
Mabbe, E., Soenens, B., Vansteenkiste, M., & Van Leeuwen, K. (2016). Do personality traits moderate relations between psychologically controlling parenting and problem behavior in adolescents? Journal of Personality, 84, 381–392. https://doi.org/10.1111/jopy.12166.
Mabbe, E., Soenens, B., Vansteenkiste, M., van der Kaap-Deeder, J., & Mouratidis, A. (2018). Day-to-day variation in autonomy-supportive and psychologically controlling parenting: the role of parents’ daily experiences of need satisfaction and need frustration. Parenting, 18, 86–109. https://doi.org/10.1080/15295192.2018.1444131.
Maljaars, J., Boonen, H., Lambrechts, G., Van Leeuwen, K., & Noens, I. (2014). Maternal parenting behavior and child behavior problems in families of children and adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 44, 501–512. https://doi.org/10.1007/s10803-013-1894-8.
Meredith, W. (1993). Measurement invariance, factor analysis and factorial invariance. Psychometrika, 58, 525–543.
Muthén, L. K., & Muthén, B. O. (1998–2012). Mplus user’s guide, 7th edn. Los Angeles: Muthén & Muthén.
Palisano, R. J., Rosenbaum, P., Bartlett, D., & Livingston, M. H. (2008). Content validity of the expanded and revised gross motor function classification system. Developmental Medicine and Child Neurology, 50, 744–750. https://doi.org/10.1111/j.1469-8749.2008.03089.
Phillips, B. A., Conners, F., & Curtner-Smith, M. E. (2017). Parenting children with Down syndrome: an analysis of parenting styles, parenting dimensions, and parental stress. Research in Developmental Disabilities, 68, 9–19. https://doi.org/10.1016/j.ridd.2017.06.010.
Pinquart, M. (2013). Do the parent–child relationship and parenting behaviors differ between families with a child with and without chronic illness? A meta-analysis. Journal of Pediatric Psychology, 38, 708–721. https://doi.org/10.1093/jpepsy/jst020.
Pinquart, M. (2016). Associations of parenting dimensions and styles with internalizing symptoms in children and adolescents: a meta-analysis. Marriage and Family Review, 53, 613–640. https://doi.org/10.1080/01494929.2016.1247761.
Pinquart, M. (2017). Associations of parenting dimensions and styles with externalizing problems of children and adolescents: an updated meta-analysis. Developmental Psychology, 53, 873–932. https://doi.org/10.1037/dev0000295.
Prinzie, P., Stams, G. J. J., Deković, M., Reijntjes, A. H., & Belsky, J. (2009). The relations between parents’ Big Five personality factors and parenting: a meta-analytic review. Journal of Personality and Social Psychology, 97, 351. https://doi.org/10.1037/a0015823.
Roth, G. (2008). Perceived parental conditional regard and autonomy support as predictors of young adults’ self-versus other-oriented prosocial tendencies. Journal of Personality, 76, 513–533. https://doi.org/10.1111/j.1467-6494.2008.00494.
Ryan, R. M., & Deci, E. L. (2017). Self-Determination Theory: basic psychological needs in motivation, development and wellness. New York: Guilford Press.
Satorra, A., & Bentler, P. M. (1994). Corrections to test statistics and standard errors in covariance structure analysis. In A. von Eye & C. C. Clogg (Eds.), Latent variables analysis: applications for developmental research (pp. 399–419). Thousand Oaks: Sage.
Schaefer, E. S. (1965). Children’s reports of parental behavior: an inventory. Child Development, 36, 413–424.
Schafer, J. L., & Graham, J. W. (2002). Missing data: our view of the state of the art. Psychological Methods, 7, 147–177. https://doi.org/10.1037/1082-989X.7.2.147.
Shea, N. M., Millea, M. A., & Diehl, J. J. (2013). Perceived autonomy support in children with autism spectrum disorder. Autism-Open Acces, 3, 2. https://doi.org/10.4172/2165-7890.S3-001.
Soenens, B., & Vansteenkiste, M. (2010). A theoretical upgrade of the concept of parental psychological control: proposing new insights on the basis of self-determination theory. Developmental Review, 30, 74–99. https://doi.org/10.1016/j.dr.2009.11.001.
Soenens, B., Vansteenkiste, M., Lens, W., Luyckx, K., Goossens, L., Beyers, W., & Ryan, R. M. (2007). Conceptualizing parental autonomy support: adolescent perceptions of promotion of independence versus promotion of volitional functioning. Developmental Psychology, 43, 633–646. https://doi.org/10.1037/0012-1649.43.3.633.
Soenens, B., Deci, E. L., & Vansteenkiste, M. (2017). How parents contribute to children’s psychological health: the critical role of psychological need support. In M. L. Wehmeyer, T. D. Little, S. J. Lopez, K. A. Shogren, & R. Ryan (Eds.), Handbook on the Development of Self-Determination (pp. 171–187). New York: Springer.
Sointu, E. T., Savolainen, H., Lappalainen, K., & Epstein, M. H. (2012). Parent, teacher and student cross informant agreement of behavioral and emotional strengths: students with and without special education support. Journal of Child and Family Studies, 21, 682–690. https://doi.org/10.1007/s10826-011-9520-x.
Stern, J. A., Borelli, J. L., & Smiley, P. A. (2015). Assessing parental empathy: a role for empathy in child attachment. Attachment and Human Development, 17, 1–22. https://doi.org/10.1080/14616734.2014.969749.
Taraban, L., & Shaw, D. S. (2018). Parenting in context: revisiting Belsky’s classic process of parenting model in early childhood. Developmental Review, 48, 55–81. https://doi.org/10.1016/j.dr.2018.03.006.
Ullman, J. B. (2001). Structural equation modeling. In B. G. Tabachnick & L. S. Fidell (Eds.), Using multivariate statistics (4th ed., pp. 653–771). Boston: Allyn & Bacon.
van de Looij-Jansen, P. M., Jansen, W., de Wilde, E. J., Donker, M. C., & Verhulst, F. C. (2011). Discrepancies between parent-child reports of internalizing problems among preadolescent children: relationships with gender, ethnic background, and future internalizing problems. The Journal of Early Adolescence, 31, 443–462.
van Gameren-Oosterom, H. B., Fekkes, M., Buitendijk, S. E., Mohangoo, A. D., Bruil, J., & Van Wouwe, J. P. (2011). Development, problem behavior, and quality of life in a population based sample of eight-year-old children with Down syndrome. PloS one, 6, e21879. https://doi.org/10.1371/journal.pone.0021879.
Vansteenkiste, M., & Ryan, R. M. (2013). On psychological growth and vulnerability: basic psychological need satisfaction and need frustration as a unifying principle. Journal of Psychotherapy Integration, 23, 263–280.
Ventola, P., Lei, J., Paisley, C., Lebowitz, E., & Silverman, W. (2017). Parenting a child with ASD: comparison of parenting style between ASD, anxiety, and typical development. Journal of Autism and Developmental Disorders, 47, 2873–2884. https://doi.org/10.1007/s10803-017-3210-5.
Vrijmoeth, C., Monbaliu, E., Lagast, E., & Prinzie, P. (2012). Behavioral problems in children with motor and intellectual disabilities: prevalence and associations with maladaptive personality and marital relationship. Research in Developmental Disabilities, 33, 1027–1038. https://doi.org/10.1016/j.ridd.2012.01.010.
Whittingham, K., Wee, D., Sanders, M. R., & Boyd, R. (2013). Predictors of psychological adjustment, experienced parenting burden and chronic sorrow symptoms in parents of children with cerebral palsy. Child: Care, Health and Development, 39, 366–373. https://doi.org/10.1111/j.1365-2214.2012.01396.
Yorke, I., White, P., Weston, A., Rafla, M., Charman, T., & Simonoff, E. (2018). The association between emotional and behavioral problems in children with autism spectrum disorder and psychological distress in their parents: a systematic review and meta-analysis. Journal of Autism and Developmental Disorders, 48, 1–23. https://doi.org/10.1007/s10803-018-3656-0.
Author information
Authors and Affiliations
Contributions
LDC: collaborated with the data collection, executed the data analyses, and wrote the main part of the paper. JVdK: assisted with the data analyses and collaborated in the writing of the results. LD: collaborated with the data collection and editing of the final manuscript. BS: collaborated in the data analyses and editing of the final manuscript. PP: collaborated in the writing of the final manuscript. SDP: designed the study and collaborated thoroughly with the data analyses and writing of the paper.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no competing interest.
Ethics Approval
The study received ethical approval from the Institutional Review Board of the Faculty of Psychology and Educational Sciences, Ghent University, Belgium.
Informed Consent
A written informed consent was obtained from all participants.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
De Clercq, L., Van der Kaap-Deeder, J., Dieleman, L.M. et al. Parenting and Psychosocial Development in Youth with and without Autism Spectrum Disorder, Cerebral Palsy, and Down Syndrome: a Cross-Disability Comparison. Adv Neurodev Disord 3, 220–234 (2019). https://doi.org/10.1007/s41252-019-00112-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41252-019-00112-2