
Abstract
There has been ongoing concern about the negative impact of residential treatment on youth in care. Research examining the impact of negative peer influence in juvenile justice, education, and residential care settings is reviewed. A study was conducted to examine the impact of negative peer contagion on the level of problem behavior in a residential care program, and the extent to which caregiver experience and youth time-in-program mediated that relationship. The study used archival data for 1,438 first-time admissions to a large Midwestern out-of-home residential program for youth with emotional and behavioral problems. Hierarchical Linear Modeling was used to examine the relationship between daily reports of conduct and oppositional defiant disorder (CD/ODD) behaviors and the percentage of conduct disorder youth living in a home. Greater exposure to conduct disordered peers was not related to increased rates of CD/ODD behavior. CD/ODD behavior was directly related to direct care staff level of experience and youth time in program. Implications for residential care are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The goal of residential care programs is to provide effective treatment for troubled youth, minimizing those situations where these youth might run the risk of getting worse. At various times, concerns have been raised about the negative impact of residential treatment on youth in care (Friman et al. 1996; Roca et al. 2009). One area of concern that has had a recent resurgence is the potential for negative peer contagion (Dodge and Sherrill 2006; Lilienfeld 2007; Rhule 2005).
Concern about negative peer contagion for youth in group care settings has been long-standing and widely shared (Osgood and Briddell 2006). There is no question that negative peer influence is significantly associated with problem and antisocial behavior in youth (Dishion et al. 2006; Dodge et al. 2006). The bulk of research examining negative peer influence, however, has been conducted in naturally occurring peer groups (Gifford-Smith 2005), and may have limited relevance to group treatment settings (Handwerk et al. 2000; Weiss et al. 2005). Research examining the impact of negative peer influence has been conducted in three general settings: juvenile justice, education, and residential care. A brief overview of the research findings in each of these areas follows.
Juvenile Justice
Negative peer influence has received quite a bit of research attention in juvenile justice settings (Chapman et al. 2006; Myers and Farrell 2008), with detention programs demonstrating the greatest potential for a negative peer influence effect (Osgood and Briddell 2006). Researchers have found a significant relationship between the amount of time spent in juvenile justice detention or work programs with adolescent and adult criminality (Bayer et al. 2003; Florsheim et al. 2004), and the worsening of prior mental health and substance abuse problems (Harrington et al. 2005). An example of this is a study which found that juvenile justice youth sent to custodial care placements had higher recidivism rates, even after controlling for variables such as self-reported criminality, level of family supervision, and best-friend deviant peers (Gatti et al. 2009).
A key issue here may be the distinction between custodial and treatment settings (Arieli et al. 2001; Osgood and Briddell 2006). Custodial settings typically are unstructured environments where adult supervision is minimal and limited treatment may do little more than periodically bring delinquent youth together. Meta-analysis supports the distinction between custody and treatment, where penal theory/deterrence was the only intervention associated with an increase in recidivism, whereas well defined behavioral and cognitive-behavior treatment approaches were shown to have the greatest impact on reducing recidivism for juvenile justice populations (Lipsey 1992; Redondo et al. 1999). For these reasons it has been observed that correctional programs seem to maximize the conditions for negative peer contagion (Osgood and Briddell 2006).
Education
There have been many studies of group interventions in educational settings for aggressive and conduct disordered youth (e.g., Boxer et al. 2005; Fraser et al. 2005; Hughes et al. 2005; Stearns et al. 2008), and several studies have found worsening behavior (typically aggression) of youth placed in group interventions delivered in educational settings (Gottfredson and Soulé 2005; Lavallee et al. 2005; Warren et al. 2005).
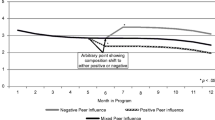
For instance, one study found that a once-a-week after school program to reduce aggression was associated with teachers reporting increased delinquency rates (Poulin et al. 2001). Other educational setting intervention research has shown that youth tend to be pulled toward the group’s average for aggression, making the most aggressive youth look less aggressive and the least aggressive youth look more aggressive (Boxer et al. 2005). While this dynamic may benefit the most aggressive youth in a group intervention, the potential for harm in these situations is for less aggressive youth to increase negative behavior to match the general group norm. Similarly, one meta-analysis showed that the treatment effects for education-based interventions with all deviant youth groups were significantly lower than the treatment effects for mixed groups or individual treatment (Ang and Hughes 2001). In contrast to this, however, another study found that adolescents in groups consisting entirely of conduct disordered youth engaged in higher levels of adaptive in-session behavior and later received lower scores on the parent and teacher ratings of externalizing behavior than youth in a group consisting of adolescents both with and without behavioral problems (Mager et al. 2005).
A potential problem for school-based group treatment programs, however, is that they can only monitor youth behavior during the brief times that youth are actually in the intervention, and cannot control the nature of the interaction between youth during non-session times (e.g., immediately before and after the session). The unintended harm sometimes associated with these programs may originate in having introduced troubled youth to one another and then allowing them too much unsupervised time. Indeed, in contrast to the research cited above, studies have found that strong classroom management and monitoring of youth interactions during free time can mediate negative peer influence in schools (Kellam et al. 1998; Raver et al. 2008; Raver et al. 2009; Webster-Stratton et al. 2008). Programs which fail to provide adequate monitoring of youth beyond the treatment setting also seem to potentially maximize the odds of deviant peers having a negative influence on each other.
Residential Care
While there is concern that residential care settings are iatrogenic, in part due to assumed negative peer contagion effects (Barth 2005; Dishion et al. 1999), there are few studies that have examined negative peer contagion in residential care settings (Connor et al. 2002; Huefner et al. 2009; Lee and Thompson 2009). Because there is little direct evidence of negative peer contagion in residential care settings, it has been argued that this generalization is perhaps premature (Handwerk et al. 2000).
One notable study that directly examined peer contagion in a residential care setting found that only a minority of youth (8%) demonstrated worsening behavior, and that the exposure to deviant peers did not have an impact on externalizing behavior trajectories for over 80% of youth (Lee and Thompson 2009). Other research found that youth placed in a treatment-focused residential care program, even the most severely disturbed, demonstrated significantly fewer externalizing problem behaviors and symptoms over time (Huefner et al. 2009). Similarly, in a study comparing residential care versus treatment foster care outcomes using propensity score matching, researchers found that residential care youth were more likely to be favorably discharged, to return home, and less likely to experience subsequent out-of-home placement than were the treatment foster care youth (Lee and Thompson 2008).
There are studies, however, on youth in residential settings that have found results consistent with a negative peer contagion effect. For instance, in one study researchers found that while youth tended to demonstrate improvement for most risk behaviors (e.g., suicide ideation, aggression toward people) and several symptoms (e.g., depression, reality assessment, sleep disturbance), two symptoms became reliably worse over time (i.e., anxiety and activity level; Lyons et al. 2001). No specific outcome hypotheses were stated for the study. Based on current negative peer contagion literature, however, the most likely expectation would be a worsening in oppositional defiance and conduct problems, not anxiety and hyperactivity. Less ambiguously, in another study of residential care, over two thirds of the youth got worse (clinical deterioration as measured by the Devereux Scales of Mental Disorders) from admit to discharge, where youth with histories of physical or sexual abuse and to have been younger in age at first placement outside their home were at even greater risk of clinical deterioration (Connor et al. 2002).
Overall, there is a fair amount of research examining the course of clinical change for youth receiving treatment in group settings. In spite of articles expressing concern about negative peer contagion in the group treatment settings (e.g., Dishion et al. 1999; Dodge et al. 2006), meta-analyses have shown that generally there is little evidence of this across studies (Knorth et al. 2008; Lipsey 2006; Weiss et al. 2005). Lacking definite evidence for negative peer contagion in group treatment settings, it still is imperative that agencies meet the challenge of providing youth optimal group interventions (Burleson et al. 2006).
Factors that have been found to mitigate the effect of negative peer contagion are negative peer density, youth time in program, and leader expertise. A brief rationale for each of these factors follows.
Negative Peer Density (NPD)
An underlying assumption in negative peer contagion is that if association with one negative peer is bad, association with a group of negative peers has to be worse. Some studies have found that the number of children in a treatment setting with histories of behavioral problems is directly related to disproportionately higher levels of problem behavior in the overall group (Boxer et al. 2005; Haynie 2002). This has led to the observation that, “peer groups that foster adverse effects are those populated by a preponderance of youth who are slightly more deviant than a particular youth in question” (Dodge and Sherrill 2006, p. 120). But this is not always the case, and one study specifically examining the impact of all conduct disordered (CD) versus mixed groups found that the all CD group did better both in terms of treatment group behavior and long term decrease in conduct problems (Mager et al. 2005). The present study will directly examine this by examining the relationship between the percentage of CD youth and the overall level of problem behavior in a residential treatment setting.
Youth Time in Program
Children in residential placements are typically referred to those programs due to their behavioral problems (Ryan and Testa 2005). Previous research in the setting used in this study has shown that youth problem behavior decreases as their time in the program increases (Handwerk et al. 2006; Huefner et al. 2010; Larzelere et al. 2004). Because youth show decreasing levels of problem behavior over time, average length of stay for youth in a home should be directly related to the average level of CD/ODD behavior. Specifically, homes with higher average lengths of stay should have lower averages of CD/ODD behavior. The statistical model will account for this tendency when examining the impact of the other variables on CD/ODD behavior.
Caregiver Experience
There is a well-established literature showing that negative peer contagion is associated with poor adult monitoring, both within family and treatment milieus (Ary et al. 1999; Chamberlain et al. 2008; Patterson et al. 1989; Ryan and Testa 2005; Svensson 2000). Mental health research has shown that negative peer contagion can be minimized, or even negated, by strong adult monitoring and involvement in youths’ lives (Ardelt and Day 2002; Gifford-Smith 2005; Pettit et al. 2001; Weaver and Prelow 2005). To state it simply, “deviant peer influence effects can be mitigated by leaders who have the expertise to know how to impose a high degree of structure and control and who administer the intervention with high fidelity” (Dodge and Sherrill 2006, p. 120). Lacking a direct measure of level of adult supervision for each youth, this study will use caregiver job tenure as the measure of experience in dealing with troubled youth.
The object of this study was to examine whether NPD, caregiver experience, and youth time-in-program impact behavioral problems in a residential care setting. We hypothesized that negative peer contagion will be reflected in higher levels of problem behavior in homes where there is a larger proportion of CD to non-CD youth for that week. Specifically, oppositional defiant and conduct disorder (CD/ODD) behavior should increase as the NPD increases. We further hypothesize that NPD will not have an impact on externalizing behavioral problems after controlling for caregiver experience and youth time-in-home.
Method
Participants
The study sample included data for all first-time admissions to a large Midwestern out-of-home family-style residential treatment facility for youth with emotional and behavioral problems between the calendar years of 2001 and 2004 (N = 1,438). Participants were 60% male, and 60% Caucasian, with ages ranging from 7 to 18 (M = 15, SD = 1.67). The percentage of youth identified by the Diagnostic Interview Schedule for Children (DISC; Shaffer et al. 2000) as qualifying for a CD diagnosis was 26.2% These youth were placed in one of 61 homes, with 6–8 youth per home. The average length of stay in the program for youth was 16.3 months, and they averaged 12.9 months in any given home.
Program/Intervention
The primary goal of the residential program is to provide a safe and therapeutic environment for at-risk youth (Daly and Dowd 1992). The youth typically come from unstable environments and face a wide array of problems such as prior abuse, behavioral disorders, and antisocial behavior (Handwerk et al. 2006; Huefner et al. 2007). The treatment model for the residential program is a modification of the Teaching Family Model, and is a family-style, community-based intervention that serves adolescent males and females (usually between the ages 12 and 18). Six to eight youth live in a home along with a specially trained married couple (Family-Teachers) and an Assistant Family-Teacher. Family-Teachers provide structured supervision for youth in daily living and treatment activities. The theoretical foundation for the program is cognitive-behavioral theory, and is characterized by five key elements: building and maintaining healthy relationships, developing interpersonal and life skills, moral and social development, family-style living, and self-government and self-determination (Davis and Daly 2003). This treatment approach has been found to be a successful approach to bringing positive behavioral change to youth both during and shortly after treatment (Larzelere et al. 2004), as well as in intermediate- and long-term follow-up studies (Huefner et al. 2007; Kingsley et al. 2008; Thompson et al. 2005).
Measures
Daily Incident Report (DIR)
Direct observations of conduct disorder behaviors were gathered from the Daily Incident Report (DIR). This report logs all significant events that occur at the residential facility each day for every youth (e.g., extreme noncompliance, aggressive behavior). Each recorded incident includes a descriptive narrative of the behavior or event and at least one categorizing code (some incidents may include more than one code). Each code has been operationalized via a brief description of the code along with a prototypical example (e.g., physical assault on staff: youth assaults a staff member. Injury may or may not have resulted, but aggressive physical contact occurred. Examples include biting, choking, kicking, punching, pushing). The potential range for daily incident data begins at 0 (no negative behavior occurred), with no real upper limit.
The reliability of the DIR has been established in several studies. First, Wright (2001) investigated how likely Family-Teachers were to report youths problem behaviors to clinical supervisors. Using a questionnaire distributed to 54 Family-Teachers containing 43 scenarios, reporting reliability for all events was 83.5%, indicating a moderate but acceptable level of agreement between Family-Teachers and clinical supervisors. Additionally, Larzelere (1996) conducted analyses of intercoder reliability of the narratives by administrative staff. Kappa coefficients ranged from .66 to .97 (M = .91) for codes entered for the same narratives by different coders. Therefore, at the level of coding the narrative descriptions, the DIR possesses good to excellent reliability. Taken together, both at the level of reporting and coding, the DIR appears to possess adequate reliability.
We used a weekly summed total of unique occurrences within each treatment home across 22 incident codes. Each code corresponded to a specific conduct disorder and oppositional defiant (CD/ODD) problem behavior (e.g., non-cooperative school behavior, property damage, running away, physical aggression). These weekly incident scores were aggregated by home to calculate the daily average number of problem behaviors during each week for each treatment home. A treatment home consisted of a Teaching Family couple within a specific house. If there was a change of Teaching Family couple within a given home, this was counted as a new treatment home. For the 4 year study period, the number of data points (i.e., weeks of data) for each home ranged from 2 to 192.
Negative Peer Density (NPD)
The measure of NPD was based on the DISC Conduct Disorder (CD) diagnosis at the time of admission to the program. The weekly proportion of youth in each home that had a CD diagnosis at the time of their admission was computed. NPD was the proportion of CD peers in the environment, which could change from week to week as youth departed the program, moved to different homes, or new youth entered the program.
Youth Length of Stay in Home
This measure was calculated as the treatment home average of the total number of weeks in the program for the youth in that particular home. Previous research has shown that youth demonstrate significant clinical improvement during their stay in the program (e.g., Handwerk et al. 2006; Huefner et al. 2009). While there is daily behavioral data, however, there was no independent measure of clinical change. As a means of assessing the impact of the presumed clinical improvement over time, youth time within a given home was used to determine the collective impact of youth program experience on levels of CD/ODD misbehavior in the home.
Family Teacher Level of Experience
This was a fixed score and was calculated as the average number of months a Teaching Family couple had worked in that position during the study period. For example, if a Teaching Family couple had 12 months of experience at the beginning of the study, and 24 months at the end, their experience score would be 18 months. Longer program tenure was taken to indicate greater familiarity with the treatment model and greater experience dealing with the problems associated with caring for youth with behavioral issues. This measure was included to determine the impact of experience in implementing the treatment model as well as dealing with conduct disordered youth. The average Family Teacher tenure in the program was 30.5 months, with a range of less than a week to 102.6 months.
Analysis
Negative peer contagion is a social phenomenon, that is, it posits that troubled individuals negatively impact the behavior of the group in which they interact. The focus of this study is not on individual behavior, but on the collective behavior of the youth within a home. The unit of analysis in this study is the weekly sum of CD/ODD behavior in a treatment home for a given Teaching-Family couple. Because of the nested structure of the data (weekly CD/ODD behavior nested within homes), Hierarchical Linear Modeling (HLM) was used to analyze the data. There were 129 home/Family Teacher combinations, with the total number of weeks for these combinations ranging from 2 to 192 during the 4 year period. All data were archival and the study was IRB approved following Federal guidelines.
Results
Descriptive Statistics
Daily Incident Report
The mean number of CD/ODD incidents per home per week ranged from zero to 7.75 (M = .39; SD = .60). The mode was 0 and median was .17, indicating that most homes had very few incidents during a typical week.
Analysis of Outcome
Level 1
The outcome variable was the daily average number of CD/ODD incidents in the home for a week. Given the nature of these incident data (i.e., counts) and its highly skewed distribution (mode = 0), we conducted a square-root transformation on the outcome variable. This transformation helps the data to be more normally distributed (Tabachnick and Fidell 1989) in order to meet the underlying assumption of the HLM analysis.
The Level 1 variable was NPD (i.e., the percentage of conduct disordered youth in the home for a given week). HLM revealed the intercept to be significant (β = .51, t (128) = 12.14, p < .001), whereas NPD (the slope) was not significant (β = −.0006, t (128) = −.53, p = .598). This indicated that in homes with no conduct disordered youth (at the intercept), the number of CD/ODD symptoms was significantly greater than zero. However, as NPD increased it did not account for any change in CD/ODD behavior. Indeed, the addition of NPD to the model only accounted for about 3.5% of the variance, with the trend being the opposite of what negative peer contagion would predict (i.e., as NPD increased CD/ODD behaviors decreased slightly).
Combined Model (Levels 1 and 2)
A key feature of HLM is that it allows the intercept and slope parameters from the Level 1 model (the within home data) to be used as dependent variables in the Level 2 (the between homes) model (Bray et al. 2001). This allows for the determination of the amount of variance accounted for by the between-subjects variables (i.e., differences between the homes). This “combined” model used the mean length of stay of the youth in each home and the mean length of employment for the home’s Family Teaching Couple as Level 2 variables. Both time on campus variables (youth’s length of stay in the home and Family Teacher level of experience) were significant at the intercept but not on the slope (see Table 1). This indicates that, at zero percent NPD (the intercept) youth’s length of stay in the home and Family Teacher level of experience were both significantly related to fewer incidents in the home. Indeed, the level 2 variables accounted for 9.2% of the variance on the intercept. However, as NPD increased, the number of CD/ODD incidents in the home did not change, regardless of youth’s length of stay in the home or Family Teacher level of experience. In other words there is no interaction between NPD and youth length of stay or Family Teacher level of experience, that is, the slopes for the level 2 variables were also flat.
Discussion
The goal of this study was to examine the relationship between NPD (i.e., negative peer density) and behavioral problems within a residential care setting. Within the residential treatment setting studied here, NPD was not significantly related to the number of CD/ODD behaviors manifest within a home. The results of this study are consistent with meta-analyses which found little support for a negative peer contagion effect for adolescent group treatments (Lipsey 2006; Weiss et al. 2005). In fact, the non-significant trend in our research was for higher NPD to be associated with slightly lower numbers of CD/ODD behavior. This is probably a spurious outcome, but it is similar to the results of at least one prior study (Mager et al. 2005).
CD/ODD problems in the homes were, however, significantly related directly to Youth Length of Stay in Home and Family Teacher Level of Experience. We had hypothesized that these two variables would moderate the impact of NPD on behavioral problems, but this was not the case. In respect to youth length of stay, as youth in the home collectively had spent more time in the treatment milieu, there were significantly fewer CD/ODD incidents. This was true for youth with a conduct disorder diagnosis at the time of admission, as well as those with other diagnoses.
We draw two conclusions from this result. First, the significantly lower levels of CD/ODD behavior in homes where the average length of stay was greater supports the effectiveness of the program in helping youth with their problem behaviors. Second, lower levels of problem behavior may lay a foundation for a home culture supportive of this improvement. The results of this study are consistent with research that found that 70% of antisocial youth’s outcome was predicted by changes in their peers’ behavior (Feldman 1992), and the view that here may be an advantage to mixing more program experienced youth with those new to a program (Boxer et al. 2005; Lipsey 2006).
We also found that as Family Teachers had more program experience there were fewer problem behaviors in their home. As a couple becomes seasoned they typically become better at program implementation (Duppong et al. 2008). This is the product of experience and ongoing training, and is verified through evaluation and a recertification process. The results of this study support the view that direct-care staff with longer tenures are more effective in helping behaviorally troubled youth control unwanted behaviors, and is consistent with research showing that adult oversight is a protective factor in correcting for negative peer influence (Dishion et al. 2004; Laird et al. 2010; Vieno et al. 2009).
There are, of course, several major limitations to this study. First, the data comes from a single treatment agency, which potentially limits the generalizability of the findings. We argue, however, that while these results might be a unique function of this specific environment, we feel that the results for any treatment-focused program with a high degree of monitoring of youth behavior would likely produce the same results. Second, there was no random assignment of youth to homes. Youth are specifically assigned to meet perceived treatment needs, family teacher strengths and experience, and overall difficulty of youth already in home. Perhaps these results were a function of the clinical sense of what will work for specific youth more than the variables accounted for in the analysis. Finally, there was no ongoing measure of clinical status, and youth length of stay within the program is admittedly a very crude measure of improvement that probably assumes too much. The analysis would have been much stronger if a clear measure of clinical improvement/status was available.
It is becoming increasingly clear that it is not simple exposure to negative peers that produces problem behavior; rather it is the nature of the time youth spend together that holds the potential disruptive behavior due to the effect of peer contagion (see Granic and Dishion 2003; Haynie and Osgood 2005). Settings that provide even non-troubled youth unstructured, unsupervised time hold the greatest potential for resulting misbehavior (Mahoney and Parente 2009; Maimon and Browning 2010). Clearly this is even more likely to be the case for troubled youth placed in group treatment settings with minimal focus on supervision or remediation of problems behaviors (Osgood and Briddell 2006).
Conversely, it has been argued that the close level of supervision in well managed group homes is actually a strength of these settings (Anglin 2001). The importance of adult monitoring in reducing deviant behavior in children has been noted by those most concerned about the impact of negative peer contagion (Dishion and McMahon 1998; Dishion et al. 2004). Group care that emphasizes close monitoring of behavior and utilizes an evidence based intervention (e.g., Teaching Family Home Model for behaviorally troubled youth; Dodge et al. 2006a) can produce substantial and sustained improvement in antisocial behavior (Handwerk et al. 2000). Researchers have suggested that specific traps to avoid include (1) providing weak or virtually no treatment, (2) situations where the intervention provides access to deviant peers who can then interact freely outside the treatment setting, and (3) where there is a lack of sufficient adult monitoring to mediate the influence of negative peers (Lipsey 2006; Weiss et al. 2005).
Among those concerned with negative peer contagion in aggregate care settings there is the recognition that “it is possible that group treatment per se is not iatrogenic and that novel ways of structuring this experience or delivering treatment in group settings can be found” (Dodge et al. 2006b, p. 13). We argue that residential care can be structured in a way that can maximize treatment benefits while avoiding the impact of negative peer contagion.
References
Ang, R., & Hughes, J. (2001). Differential benefits of skills training with antisocial youth based on group composition: A meta-analytic investigation. School Psychology Review, 31, 164–185.
Anglin, J. P. (2001, February). Presentation and dialogue on findings of a research study on staffed group homes for children and youth. Paper presented in the CWLC National Teleconference Series, Canada.
Ardelt, M., & Day, L. (2002). Parents, siblings, and peers: Close social relationships and adolescent deviance. Journal of Early Adolescence, 22, 310–349. doi:10.1177/02731602022003004.
Arieli, M., Beker, J., & Kashti, Y. (2001). Residential group care as a socializing environment: Toward a broader perspective. Child & Youth Care Forum, 30, 403–414. doi:10.1023/A:1015321302983.
Ary, D. V., Duncan, T. E., Duncan, S. C., & Hops, H. (1999). Adolescent problem behavior: The influence of parents and peers. Behaviour Research and Therapy, 37, 217–230. doi:10.1016/S0005-7967(98)00133-8.
Barth, R. P. (2005). Residential care: From here to eternity. International Journal of Social Welfare, 14, 158–162. doi:10.1111/j.1468-2397.2005.00355.x.
Bayer, P., Pintoff, R., & Pozen, D. E. (2003). Building criminal capital behind bars: Social learning in juvenile corrections. Center Discussion Paper No. 864. New Haven, CT: Economic Growth Center, Yale University.
Boxer, P., Guerra, N. G., Huesmann, L. R., & Morales, J. (2005). Proximal peer-level effects of a small-group selected prevention on aggression in elementary school children: An investigation of the peer contagion hypothesis. Journal of Abnormal Child Psychology, 33, 325–338. doi:10.1007/s10802-005-3568-2.
Bray, J. H., Adams, G. J., Getz, J. G., & Baer, P. E. (2001). Developmental, family, and ethnic in influences on adolescent alcohol usage: A growth curve approach. Journal of Family Psychology, 15, 301–314. doi:10.1037/0893-3200.15.2.301.
Burleson, J. A., Kaminer, Y., & Dennis, M. L. (2006). Absence of iatrogenic or contagion effects in adolescent group therapy: Findings from the Cannabis Youth Treatment (CYT) Study. The American Journal on Addictions, 15, 4–15. doi:10.1080/10550490601003656.
Chamberlain, P., Price, J., Leve, L. D., Landsverk, J. A., Reid, J. B., & Laurent, H. (2008). Prevention of behavior problems for children in foster care: Outcomes and mediation effects. Prevention Science, 9, 17–27. doi:10.1007/s11121-007-0080-7.
Chapman, J. F., Desai, R. A., & Falzer, P. R. (2006). Mental health service provision in juvenile justice facilities: Pre- and postrelease psychiatric care. Child and Adolescent Psychiatric Clinics of North America, 15, 445–458. doi:10.1016/j.chc.2005.11.002.
Connor, D. F., Miller, K. P., Cunningham, J. A., & Melloni, J. (2002). What does getting better mean? Child improvement and measure of outcome in residential treatment. American Journal of Orthopsychiatry, 72, 110–117. doi:10.1037/0002-9432.72.1.110.
Daly, D. L., & Dowd, T. P. (1992). Characteristics of effective, harm-free environments for children in out-of-home care. Child Welfare Journal, 71, 487–496.
Davis, J., & Daly, D. L. (2003). Girls and boys town long-term residential program: Training manual (4th ed.). Boys Town, NE: Father Flanagan’s Boys’ Home.
Dishion, T. J., Dodge, K. A., & Lansford, J. E. (2006). Findings and recommendations: A blueprint to minimize deviant peer influence in youth interventions and programs. In K. A. Dodge, T. J. Dishion, & J. E. Lansford (Eds.), Deviant peer influences in programs for youth: Problems and solutions (pp. 366–394). Guilford Press: New York.
Dishion, T. J., McCord, J., & Poulin, F. (1999). When interventions harm: Peer groups and problem behavior. American Psychologist, 54, 755–764. doi:10.1037/0003-066X.54.9.755.
Dishion, T. J., & McMahon, R. J. (1998). Parental monitoring and the prevention of child and adolescent problem behavior: A conceptual and empirical formulation. Clinical Child and Family Psychology Review, 1, 61–75. doi:10.1023/A:1021800432380.
Dishion, T. J., Nelson, S. E., & Bullock, B. M. (2004). Premature adolescent autonomy: Parent disengagement and deviant peer process in the amplification of problem behaviour. Journal of Adolescence, 27, 515–530. doi:10.1016/j.adolescence.2004.06.005.
Dodge, K. A., Dishion, T. J., & Lansford, J. E. (2006a). Deviant peer influences in intervention and public policy for youth. Social Policy Report, 20, 3–19.
Dodge, K. A., Lansford, J. E., & Dishion, T. J. (2006b). The problem of deviant peer influences in intervention programs. In K. A. Dodge, T. J. Dishion, & J. E. Lansford (Eds.), Deviant peer influences in programs for youth: Problems and solutions (pp. 3–13). Guilford Press: New York.
Dodge, K. A., & Sherrill, M. R. (2006). Deviant peer group effects in youth mental health interventions. In K. A. Dodge, T. J. Dishion, & J. E. Lansford (Eds.), Deviant peer influences in programs for youth: Problems and solutions (pp. 97–121). Guilford Press: New York.
Duppong Hurley, K., Shaw, T., Thompson, R., Griffith, A., Farmer, E. M., & Tierney, J. (2008). Assessing staff competence at implementing a multifaceted residential program for youth: Development and initial psychometrics of a staff observation form. Residential Treatment for Children & Youth, 23, 83–104.
Feldman, R. A. (1992). The St. Louis experiment: Effective treatment of antisocial youths in prosocial peer groups. In J. McCord & R. E. Tremblay (Eds.), Preventing antisocial behavior: Interventions from birth through adolescence (pp. 233–252). Guilford Press: New York.
Florsheim, P., Behling, S., South, M., Fowles, T. R., & DeWitt, J. (2004). Does the youth corrections system work? Tracking the effectiveness of intervention efforts with delinquent boys in state custody. Psychological Services, 1, 126–139. doi:10.1037/1541-1559.1.2.126.
Fraser, M. W., Galinsky, M. J., Smokowski, P. R., Day, S. H., Terzian, M. A., Rose, R. A., et al. (2005). Social information-processing skills training to promote social competence and prevent aggressive behavior in the third grades. Journal of Consulting and Clinical Psychology, 73, 1045–1055. doi:10.1037/0022-006X.73.6.1045.
Friman, P. C., Osgood, D. W., Smith, G. L., Shanahan, D., Thompson, R. W., Larzelere, R. E., et al. (1996). A longitudinal evaluation of prevalent negative beliefs about residential placement for troubled adolescents. Journal of Abnormal Child Psychology, 24, 299–324. doi:10.1007/BF01441633.
Gatti, U., Tremblay, R. E., & Vitaro, F. (2009). Iatrogenic effect of juvenile justice. Journal of Child Psychology and Psychiatry, 50, 991–998. doi:10.1111/j.1469-7610.2008.02057.x.
Gifford-Smith, Mary. (2005). Peer influence in children and adolescents: Crossing the bridge from developmental to intervention science. Journal of Abnormal Child Psychology, 33, 255–265. doi:10.1007/s10802-005-3563-7.
Gottfredson, D. C., & Soulé, D. A. (2005). The timing of property crime, violent crime, and substance use among juveniles. Journal of Research in Crime and Delinquency, 42, 110–120. doi:10.1177/0022427804266563.
Granic, I., & Dishion, T. J. (2003). Deviant talk in adolescent friendships: A step toward measuring a pathogenic attractor process. Social Development, 12, 314–334.
Handwerk, M. L., Clopton, K., Huefner, J. C., Smith, G. L., Hoff, K. E., & Lucas, C. P. (2006). Gender differences in adolescents in residential treatment. American Journal of Orthopsychiatry, 76, 312–324. doi:10.1037/0002-9432.76.3.312.
Handwerk, M. L., Field, C., & Friman, P. C. (2000). The iatrogenic effects of group intervention for antisocial youth: Premature extrapolations? Journal of Behavioral Education, 10, 223–238. doi:10.1023/A:1012299716053.
Harrington, R. C., Kroll, L., Rothwell, J., McCarthy, K., Bradley, D., & Bailey, S. (2005). Psychosocial needs of boys in secure care for serious or persistent offending. Journal of Child Psychology and Psychiatry, 46, 859–866. doi:10.1111/j.1469-7610.2004.00388.x.
Haynie, D. L. (2002). Friendship networks and delinquency: The relative nature of peer delinquency. Journal of Quantitative Criminology, 18, 99–134. doi:10.1023/A:1015227414929.
Haynie, D. L., & Osgood, D. W. (2005). Reconsidering peers and delinquency: How do peers matter? Social Forces, 84, 1109–1130.
Huefner, J. C., Handwerk, M. L., Ringle, J. L., & Field, C. E. (2009). Conduct disordered youth in group care: An examination of negative peer influence. Journal of Child and Family Studies, 18, 719–730. doi:10.1007/s10826-009-9278-6.
Huefner, J. C., James, S., Ringle, J., Thompson, R. W., & Daly, D. L. (2010). Patterns of movement for youth within an integrated continuum of residential services. Children and Youth Services Review, 32, 857–864. doi:10.1016/j.childyouth.2010.02.005.
Huefner, J. C., Ringle, J. L., Chmelka, M. B., & Ingram, S. D. (2007). Breaking the cycle of intergenerational abuse: The long-term impact of a residential care program. Child Abuse and Neglect, 31, 187–199. doi:10.1016/j.chiabu.2006.09.003.
Hughes, J. N., Cavell, T. A., Meehan, B. T., Zhang, D., & Collie, C. (2005). Adverse school context moderates the outcomes of selective interventions for aggressive children. Journal of Consulting and Clinical Psychology, 73, 731–736. doi:10.1037/0022-006X.73.4.731.
Kellam, S. G., Ling, X., Merisca, R., Brown, C. H., & Ialongo, N. (1998). The effect of the level of aggression in the first grade classroom on the course and malleability of aggressive behavior into middle school. Development and Psychopathology, 10, 165–185. doi:10.1037/0022-006X.73.4.731.
Kingsley, D. E., Ringle, J. L., Thompson, R. W., Chmelka, M. B., & Ingram, S. D. (2008). Cox Proportional Hazards Regression Analysis as a modeling technique for informing program improvement: Predicting recidivism in a Girls and Boys Town five-year follow-up study. The Journal of Behavior Analysis of Offender and Victim Treatment and Prevention, 1, 82–97.
Knorth, E. J., Harder, A. T., Zandberg, T., & Kendrick, A. J. (2008). Under one roof: A review and selective meta-analysis on the outcomes of residential child and youth care. Children and Youth Services Review, 30, 123–140.
Laird, R. D., Marrero, M. D., & Sentse, M. (2010). Revisiting parental monitoring: Evidence that parental solicitation can be effective when needed most. Journal of Youth and Adolescence, 39, 1431–1441. doi:10.1007/s10964-009-9453-5.
Larzelere, R. E. (1996). Inter-coder reliabilities and construct groupings for some important codes on the Daily Incident Report (NRI 001–96). Boys Town, NE: Father Flanagan’s Boys’ Home.
Larzelere, R. E., Daly, D. L., Davis, J. L., Chmelka, M. B., & Handwerk, M. L. (2004). Outcome evaluation of the Girls and Boys Town Family Home Program. Education & Treatment of Children, 27, 130–149.
Lavallee, K. L., Bierman, K. L., & Nix, R. L. (2005). The impact of first-grade “friendship group” experiences on child social outcomes in the Fast Track program. Journal of Abnormal Child Psychology, 33, 307–324. doi:10.1007/s10802-005-3567-3.
Lee, B. R., & Thompson, R. W. (2008). Comparing outcomes for youth in treatment foster care and family style group care. Children and Youth Services Review, 30, 746–757. doi:10.1016/j.childyouth.2007.12.002.
Lee, B. R., & Thompson, R. W. (2009). Examining externalizing behavior trajectories of youth in group homes: Is there evidence for peer contagion? Journal of Abnormal Child Psychology, 37, 31–44. doi:10.1007/s10802-008-9254-4.
Lilienfeld, S. O. (2007). Psychological treatments that cause harm. Perspectives on Psychological Science, 2, 53–70. doi:10.1111/j.1745-6916.2007.00029.x.
Lipsey, M. W. (1992). Juvenile delinquency treatment: A meta-analytic inquiry into the variability of effects. In T. D. Cook, H. Cooper, D. S. Cordray, H. Hartmann, L. V. Hedges, R. J. Light, T. A. Louis, & F. Mosteller (Eds.), Meta-analysis for explanation: A casebook (pp. 83–127). New York: Russel Sage Foundation.
Lipsey, M. W. (2006). The effects of community-based group treatment for delinquency: A meta-analytic search for cross-study generalizations. In K. A. Dodge, T. J. Dishion, & J. E. Lansford (Eds.), Deviant peer influences in programs for youth: Problems and solutions (pp. 162–184). New York: Guilford Press.
Lyons, J. S., Terry, P., Martinovich, Z., Peterson, J., & Bouska, B. (2001). Outcome trajectories for adolescents in residential treatment: A statewide evaluation. Journal of Child and Family Studies, 10, 333–345. doi:10.1023/A:1012576826136.
Mager, W., Milich, R., Harris, M. J., & Howard, A. (2005). Intervention groups for adolescents with conduct problems: Is aggregation harmful or helpful? Journal of Abnormal Child Psychology, 33, 349–362. doi:10.1007/s10802-005-3572-6.
Mahoney, J. L., & Parente, M. E. (2009). Should we care about adolescents who care for themselves? What we have learned and what we need to know about youth in self-care. American Journal of Community Psychology, 45, 285–293.
Maimon, D., & Browning, C. R. (2010). Unstructured socializing, collective efficacy, and violent behavior among urban youth. Criminology, 48, 443–474.
Myers, D. M., & Farrell, A. F. (2008). Reclaiming lost opportunities: Applying public health models in juvenile justice. Children and Youth Services Review, 30, 1159–1177. doi:10.1016/j.childyouth.2008.03.002.
Osgood, D. W., & Briddell, L. (2006). Peer effects in juvenile justice. In K. A. Dodge, T. J. Dishion, & J. E. Lansford (Eds.), Deviant peer influences in programs for youth: Problems and solutions (pp. 141–161). New York: Guilford Press.
Patterson, G. R., DeBaryshe, B. D., & Ramsey, E. (1989). A developmental perspective on antisocial behavior. American Psychologist, 44, 329–335. doi:10.1037/0003-066X.44.2.329.
Pettit, G. S., Laird, R. D., Dodge, K. A., Bates, J. E., & Criss, M. M. (2001). Antecedents and behavior-problem outcomes of parental monitoring and psychological control in early adolescence. Child Development, 72, 583–598. doi:10.1111/1467-8624.00298.
Poulin, F., Dishion, T. J., & Burraston, B. (2001). 3-Year iatrogenic effects associated with aggregating high-risk adolescents in cognitive-behavioral preventive interventions. Applied Developmental Science, 5, 214–224. doi:10.1207/S1532480XADS0504_03.
Raver, C. C., Jones, S. M., Li-Grining, C. P., Metzger, M., Champion, K. M., & Sardin, L. (2008). Improving preschool classroom processes: Preliminary findings from a randomized trial implemented in Head Start settings. Early Childhood Research Quarterly, 23, 10–26. doi:10.1016/j.ecresq.2007.09.001.
Raver, C. C., Jones, S. M., Li-Grining, C., Zhai, F., Metzger, M. W., & Solomon, B. (2009). Targeting children’s behavior problems in preschool classrooms: A cluster-randomized controlled trial. Journal of Consulting and Clinical Psychology, 77, 302–316. doi:10.1037/a0015302.
Redondo, S., Sanchez-Meca, J., & Garrido, V. (1999). The influence of treatment programmes on the recidivism of juvenile and adult offenders: An European meta-analytic review. Psychology, Crime & Law, 5, 251–278. doi:10.1080/10683169908401769.
Rhule, D. M. (2005). Take care to do no harm: Harmful interventions for youth problem behavior. Professional Psychology: Research and Practice, 36, 618–625. doi:10.1037/0735-7028.36.6.618.
Roca, J. S., Garcia, M. J., Biarnes, A. V., & Rodriquez, M. (2009). Analysis of factors involved in the social inclusion process of young people fostered in residential care institutions. Children and Youth Services Review, 31, 1251–1257. doi:10.1016/j.childyouth.2009.05.010.
Ryan, J. P., & Testa, M. F. (2005). Child maltreatment and juvenile delinquency: Investigating the role of placement and placement instability. Children and Youth Services Review, 27, 227–249. doi:10.1016/j.childyouth.2004.05.007.
Shaffer, D., Fisher, P., Lucas, C. P., Dulcan, M. K., & Schwab-Stone, M. E. (2000). NIMH Diagnostic Interview Schedule for Children Version IV (NIMH DISC-IV): Description, differences from previous versions, and reliability of some common diagnoses. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 28–38.
Stearns, E., Dodge, K. A., & Nicholson, M. (2008). Peer contextual influences on the growth of authority-acceptance problems in early elementary school. Merrill-Palmer Quarterly, 54, 208–231.
Svensson, R. (2000). Risk factors for different dimensions of adolescent drug use. Journal of Child & Adolescent Substance Abuse, 9, 67–90. doi:10.1300/J029v09n03_05.
Tabachnick, B. G. & Fidell, L. S. (1989). Using multivariate statistics (2nd ed.). New York: Harper Collins.
Thompson, R. W., Huefner, J. C., Ringle, J. L., & Daly, D. L. (2005). Adult outcomes of Girls and Boys Town youth: A follow-up report. In C. Newman, C. J. Liberton, K. Kutash, & R. M. Friedman (Eds.), 17th Annual conference proceedings—A system of care for children’s mental health: expanding the research base (pp. 529–534). Tampa, Florida: University of Florida Research and Training Center for Children’s Mental Health.
Vieno, A., Nation, M., Pastore, M., & Santinello, M. (2009). Parenting and antisocial behavior: A model of the relationship between adolescent self-disclosure, parental closeness, parental control, and adolescent antisocial behavior. Developmental Psychology, 45, 1509–1519. doi:10.1037/a0016929.
Warren, K., Schoppelrey, S., Moberg, D. P., & McDonald, M. (2005). A model of contagion through competition in the aggressive behaviors of elementary school students. Journal of Abnormal Child Psychology, 33, 283–292. doi:10.1007/s10802-005-3565-5.
Weaver, S. R., & Prelow, H. M. (2005). A mediated-moderation model of maternal parenting style, association with deviant peers, and problem behaviors in urban African American and European American adolescents. Journal of Child and Family Studies, 14, 343–356. doi:10.1007/s10826-005-6847-1.
Webster-Stratton, C., Reid, M. J., & Stoolmiller, M. (2008). Preventing conduct problems and improving school readiness: Evaluation of the Incredible Years teacher and child training programs in high-risk schools. Journal of Child Psychology and Psychiatry, 49, 471–488. doi:10.1111/j.1469-7610.2007.01861.x.
Weiss, B., Caron, A., Ball, S., Tapp, J., Johnson, M., & Weisz, J. R. (2005). Iatrogenic effects of group treatment for antisocial youths. Journal of Consulting and Clinical Psychology, 73, 1036–1044. doi:10.1037/0022-006X.73.6.1036.
Wright, D. J. (2001). The relationship of anxiety and externalizing disorders. Dissertation Abstracts International: Section B: The Sciences and Engineering, 62, 2084B.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Huefner, J.C., Ringle, J.L. Examination of Negative Peer Contagion in a Residential Care Setting. J Child Fam Stud 21, 807–815 (2012). https://doi.org/10.1007/s10826-011-9540-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-011-9540-6