
Abstract
Purpose
To review the impact of tyrosine kinase inhibitors (TKIs) on fertility in men and women, embryo development, and early pregnancy, and discuss considerations for fertility preservation in patients taking TKIs.
Methods
A comprehensive literature search using the PubMed database was performed through February 2021 to evaluate the current literature on imatinib, nilotinib, dasatinib, and bosutinib as it relates to fertility and reproduction. Published case series were analyzed for pregnancy outcomes.
Results
TKIs adversely affect oocyte and sperm maturation, gonadal function, and overall fertility potential in a self-limited manner. There are insufficient studies regarding long-term consequences on fertility after discontinuation of TKIs. A total of 396 women and 236 men were on a first- or second-generation TKI at the time of conception. Of the women with detailed pregnancy and delivery outcomes (n = 361), 51% (186/361) resulted in a term birth of a normal infant, 4.3% (16/361) of pregnancies had a pregnancy complication, and 5% (20/361) of pregnancies resulted in the live birth of an infant with a congenital anomaly. About 22% of pregnant women (87/396) elected to undergo a termination of pregnancy, while 16% (63/396) of pregnancies ended in a spontaneous abortion. In contrast, of the 236 men, 87% conceived pregnancies which resulted in term deliveries of normal infants. Elective terminations, miscarriage rate, pregnancy complication rate, and incidence of a congenital malformation were all less than those seen in females (4%, 3%, 2%, and 2.5%, respectively).
Conclusion
Women should be advised to avoid conception while taking a TKI. Women on TKIs who are considering pregnancy should be encouraged to plan the pregnancy to minimize inadvertent first trimester exposure. In women who conceive while taking TKIs, the serious risk of relapse due to discontinuation of TKI should be balanced against the potential risks to the fetus. The risk of teratogenicity to a fathered pregnancy with TKI use is considerably lower. Fertility preservation for a woman taking a TKI can be considered to plan a pregnancy with a minimal TKI-free period. With careful monitoring, providers may consider a TKI washout period followed by controlled ovarian stimulation to cryopreserve oocytes or embryos, with a plan to resume TKIs until ready to conceive or to transfer an embryo to achieve pregnancy quickly. Fertility preservation is also indicated if a patient on TKI is requiring a gonadotoxic therapy or reproductive surgery impacting fertility.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Tyrosine kinase inhibitors (TKIs) are a class of small molecule targeted anticancer therapy that block cell surface tyrosine kinase receptor phosphorylation and thus inhibit cell signaling. Imatinib mesylate (marketed as Gleevec in the USA and Glivec in the rest of the world), a first-generation TKI, was the first TKI approved by the United States Food and Drug Administration as specific therapy for chronic myelogenous leukemia (CML) in 2001 [1]. CML is characterized by a balanced translocation, t(9;22)(q34;q11.2), involving the fusion of the Abelson gene (ABL1) from chromosome 9 and the breakpoint cluster region (BCR) gene on chromosome 22. This rearrangement, known as the Philadelphia chromosome, leads to the generation of the BCR-ABL1 oncogene that leads to production of the BCR-ABL oncoprotein. Imatinib is orally active, and acts as a highly selective inhibitor of the constitutively activated intracellular tyrosine kinase on the BCR-ABL oncoprotein by competitively binding to and inhibiting the interaction of the oncoprotein and adenosine triphosphate (ATP), thus blocking cellular proliferation. With the success seen in imatinib, three additional second-generation TKIs are now approved as first-line treatment of CML in the chronic phase: nilotinib, dasatinib, and bosutinib, all with varying affinities for the BCR-ABL oncoprotein.
Although designed to bind the BCR-ABL tyrosine kinase, first- and second-generation TKIs have demonstrated high affinity for binding to other tyrosine kinase receptors, including c-KIT and platelet-derived growth factor receptor-alpha (PDGFR-a). This has expanded the use of TKIs to treat gastrointestinal stromal tumors (GIST) and pediatric leukemias. GIST is a rare form of primary gastrointestinal neoplasms with characteristics of both mesenchymal and neural tumors [2]. These tumors were previously treated as leiomyosarcomas of the GI tract, until the discovery that the majority of these tumors carry a mutation in the c-KIT protooncogene, a transmembrane tyrosine kinase receptor, leading to a constitutively activated state, and subsequently tumor growth [3]. Similarly, bosutinib and dasatinib target a wide variety of tyrosine kinases. In addition to targeting the BCR-ABL tyrosine kinase, they are effective inhibitors of the Src-family kinases. The Src-family kinases include nine members (Src, Yes, Fyn, Fgr, Lck, Hck, Blk, Lyn, Frk) and are expressed on various different cell types and play key roles in signal transduction [4]. Src-family kinases have been found to be dysregulated in many solid organ malignancies [5]. As activation of BCR-ABL independent pathway including Src-family kinases can be associated with imatinib resistance, dasatinib is approved for treatment of imatinib-resistant CML or treatment of Philadelphia chromosome–positive acute lymphoblastic leukemia resistant to treatment with first-line therapies [6]. The advent of tyrosine TKIs drastically improved the progression-free survival of those patients with activating tumors in these transmembrane receptors, with 10-year survival rates above 80–90% [7]. With the advances in cancer diagnosis and treatments, the number of reproductive age cancer survivors has grown exponentially. For example, 30–40% of patients diagnosed with CML are considered to be of reproductive age [8,9,10]. Many of these young adults have achieved stable remission while taking oral TKIs and are now considering childbearing. In this review, we will summarize the current literature on the reproductive impact of TKIs on fertility in men and women, including the impact on early pregnancy, and we discuss approaches for fertility preservation in patients taking TKIs.
Methods
In this review, we performed a comprehensive literature search using the PubMed database (www.pubmed.org) to obtain any and all relevant articles published in the English language from PubMed’s inception through February 11, 2021. Search phrases included “imatinib and fertility,” “fertility preservation and imatinib,” “effects of imatinib on oocyte function,” “effects of imatinib on male fertility,” “effects of imatinib on a placenta,” “imatinib and pregnancy,” and “imatinib and in vitro fertilization.” These same search phrases were used with the substitution of nilotinib, dasatinib, and bosutinib, respectively. Included data needed to specify reproductive and/or pregnancy outcomes while on one of the four TKIs discussed. PubMed was last screened on February 11, 2021. Case reports or case series with fewer than 2 patients were largely excluded except in those presenting new information. Likewise, other review papers were excluded unless presenting new clinical or scientific information. Abstracts and otherwise unpublished data were not included. Once relevant articles were identified and carefully reviewed, references from these articles were also reviewed for additional sources. An Institutional Review Board approval was not required for this study as only published data with deidentified patient markers were used for this review.
Statistical analysis was performed with respect to pregnancy outcomes in males and females using a first- or second-generation TKI at the time of conception, as well as a sub-analysis of each individual TKI assessed in this review. We examined total number of pregnancies which resulted in a term pregnancy without complications, elective abortion, spontaneous abortion, and pregnancies resulting in a complication, with categorical data analyzed as percentages for pregnancies. We also assessed the total number of live births with congenital malformations. This parameter was not a proportion of the total number of pregnancies but rather total live births (data not shown) as our study included multifetal pregnancies.
Discussion
Effects of TKIs on ovarian function
As with numerous other chemotherapeutic agents, TKIs have been implicated in affecting future female reproductive potential. This impact on fertility is a result of blocking c-KIT and PDGFR-a, known target receptors of imatinib and other TKIs (Fig. 1). c-KIT is expressed on the surface of human ovaries and, when exposed to a TKI, results in decreased cell proliferation and increased apoptosis [11, 12]. PDGFR-a is also found on primordial follicles and is involved in follicular development. TKIs have been shown to disrupt the developmental process forming a primary follicle, thus decreasing the total follicle count by blocking the PDGFR-a receptor [11,12,13]. Similarly, strong evidence indicates the importance of the Src-family kinases in oocyte maturation and meiotic spindle function in the metaphase II oocyte [14, 15]. However, specific research linking inhibition of Src-family kinases by TKIs in germ cells and gonads is sparse.

Proposed impact of tyrosine kinase inhibitors on reproduction
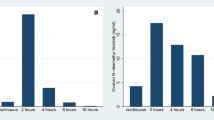
Zamah et al. demonstrated that ovarian function is compromised in the presence of imatinib, thereby affecting women who desire to undergo ovarian stimulation for fertility preservation [16]. When ovarian stimulation was attempted in a woman taking imatinib, estradiol concentrations were significantly decreased and a lower number of oocytes were retrieved compared to her own control cycle off the drug 2 months later, despite similar conditions of the stimulation, indicating imatinib can negatively affect steroidogenesis and oocyte retrieval [16]. They hypothesized that the granulosa cells may have undergone apoptosis leading to oocyte atresia and lower egg recovery; however, when they treated primary human granulosa cell cultures with varying concentrations of imatinib in an in vitro model, they did not see a significant difference in cell survival or the ability of granulosa cells to produce estradiol from testosterone when stimulated with gonadotropins. Based on these results, they postulated that imatinib may have an effect on either theca cells or granulosa cell proliferation during the follicular phase. This same effect has also been established in mouse models [17]. Additionally, Salem et al. demonstrated TKIs negatively impact ovarian reserve by reducing the proportion of primordial follicles [13]. Although this has not been corroborated in larger studies, women and couples attempting fertility preservation should be made aware of this negative effect on oocyte recruitment and recovery due to concomitant TKI use as this may serve as a poor prognostic factor.
As with imatinib, other second-generation TKIs have varying levels of activity against c-KIT and PDGFR, indicating TKIs can affect folliculogenesis. A study by Seval e. al. demonstrated a statistically significant decrease in the total follicle count in female mice treated with nilotinib [12]. In preclinical trials, bosutinib was shown to have a negative effect on fertility and reproduction; however, no studies have directly assessed its impact on ovaries or oocytes [18, 19]. There is a paucity of data on the effects of dasatinib on female fertility. In a preclinical study, Cortes et al. demonstrated dasatinib does not appear to affect female fertility across different levels of the drug tested in exposed rats, while exposure to dasatinib increased embryo-lethality [20].
There is insufficient evidence regarding the impact of long-term TKI use on fertility [16, 17]. Zamah et al. demonstrated that follicular fluid concentrations of imatinib are at a steady state with plasma levels, and there was no evidence of imatinib or its metabolite once the drug was cleared [16]. Although studies have shown TKIs affect folliculogenesis, there are numerous case reports of women conceiving while on a TKI, indicating at least some gonadal function is still preserved [21]. Thus far, there has only been one published report of primary ovarian insufficiency documented in a CML patient receiving a high dose of imatinib [22]. The potential long-term effects of TKIs remain unknown as only a limited number of patients have been followed for extended periods of time.
To our knowledge, there are only 3 case reports published involving patients with CML undergoing controlled ovarian stimulation (COS) to achieve pregnancy. Gazdaru et al. were the first to describe a successful COS followed by cryopreservation of 9 zygotes in a 26-year-old woman with CML after a 19-day washout period from nilotinib [21]. The patient had been on multiple TKIs (imatinib, dasatinib, and nilotinib) over the course of 9 years prior to the decision to proceed with stem cell transplantation due to relapse. The authors used a gonadotropin-releasing hormone antagonist stimulation protocol and retrieved 12 mature oocytes. Following intracytoplasmic sperm injection (ICSI), a total of 9 zygotes were cryopreserved. Furukawa et al. described the first successful frozen embryo transfer (FET) and full-term delivery in a 38-year-old woman with CML treated with imatinib for 8 years [23]. The patient had discontinued imatinib 6 months prior to initiating infertility treatment during which time she underwent treatment with interferon (IFN)-α and, after 3 unsuccessful cycles of intrauterine insemination (IUI), proceeded to in vitro fertilization (IVF). The authors used an agonist protocol, and after 3 cycles achieved 2 blastocyst-stage embryos, which were cryopreserved. As the patient had elevated levels of BCR-ABL during her infertility treatment, she was started on dasatinib. Once levels were undetectable again, the patient had a 3-month washout and underwent a successful transfer. The neonate was found to have a meningocele, which was repaired at birth. Although the patient had a TKI-free period of 6 months prior to attempting IVF and a 3-month washout prior to her embryo transfer, the authors postulated the meningocele was due to a folate deficiency from her underlying leukemia and not a TKI-induced effect, although folate levels were not assessed in the patient during pregnancy [23]. The study also did not indicate specifically if the patient was on a prenatal vitamin containing folic acid. The most recent case was reported by Rios et al. who described a successful fresh embryo transfer in a 23-year-old woman with CML [24]. After 6 years of imatinib therapy, the patient discontinued the medication to attempt natural conception for 4 months, followed by two unsuccessful IUIs. As the patient had lost her major molecular response at this point and was on IFN-α therapy, she underwent COS with an antagonist protocol, and following ICSI achieved 2 blastocyst-stage embryos which were cryopreserved. IFN-α therapy was discontinued during her stimulation cycle due to toxicity. The patient was started on nilotinib following her retrieval, and after 16 months of treatment discontinued for transfer. Seven days after discontinuing nilotinib, the patient underwent two consecutive FETs, which both failed. She underwent a second COS and achieved 5 blastocyst-stage embryos, 4 of which were cryopreserved and one transferred successfully. She went on to deliver a healthy full-term infant without needing further treatment of CML during her pregnancy [24]. These three case reports demonstrate that stopping a TKI for a short period of time is reasonable to preserve fertility, and more importantly, to minimize a TKI-free period, COS should be considered to achieve pregnancy quickly [23].
Effect of TKIs on male fertility
Most animal studies and case reports have shown that the overall effects of TKIs on male fertility are self-limited [8]. As with human ovaries, the proper development of testicles, hormone production, and subsequently spermatogenesis relies heavily on the functions of c-KIT and PDGFR-a, describing a pathway for the finding of decreased spermatogenesis, testicular weight, and testosterone concentrations described in male rodents exposed to imatinib [12, 16, 25, 26]. PDGFR is known to be expressed on Leydig cells of testis, and disruption of normal signaling by imatinib results in apoptosis and a decrease in the total number of these cells [25,26,27] (Fig. 1). Testicular development and alterations to the hypothalamus-pituitary-testes axis are disrupted in rats exposed to imatinib during the early postnatal period, and inhibition of Leydig cell maturation during development can lead to detrimental effects [9, 12, 25, 27, 28]. For humans, a similar effect has been demonstrated in case reports describing severe oligospermia in males treated with imatinib prior to puberty [29]. However, data regarding effects of imatinib on sperm have been conflicting. Early studies by Nurmio et al. revealed that, although the total number of spermatogonia was decreased, it did not affect sperm production [25]. In accordance with this, data from Heim et al. also showed that, despite overall survival of differentiating spermatogonia was decreased in the presence of imatinib, exposure to the medication did not disrupt the process of spermatogenesis, and therefore, future fertility was protected [27]. Chang et al. demonstrated imatinib crosses the blood-testis barrier, resulting in reduced semen parameters including decreased sperm counts [30]. Despite decreases in sperm counts, nearly 200 case reports of pregnancies with male partners on imatinib have been described.
Along with a decrease in the total number of Leydig cells, a study by Gambacorti-Passerini et al. revealed 92% of men on long-term imatinib had a reduction in their serum testosterone concentrations, with 73% of these also having low free testosterone [31]. As the target receptors of imatinib, c-KIT and PDGFR-a are expressed on Leydig cells and these receptors are responsible for a complex interplay ultimately stimulating testosterone production, which reveals a clear pathway for a decrease in testosterone levels under the influence of imatinib [26, 31]. Interestingly, 18% of men also developed gynecomastia, likely due to the reduction in testosterone and a buildup of the testosterone precursors progesterone and 17-hydroxyprogesterone in the steroidogenesis pathway [31]. Despite a decreased level of testosterone observed in mice exposed to imatinib, levels normalized following removal of the drug [26]. Interestingly, data regarding effects of imatinib on testosterone levels have been conflicting, with recent studies showing minimal decrease in total testosterone levels, with levels again normalizing after stopping imatinib; however, these studies were small [9, 28, 30, 32]. These recent data demonstrate TKIs may have less of an effect on male fertility when administered in adulthood, and exposure to a TKI prior to puberty could have more severe consequences [9].
Similar to imatinib, second-generation TKIs have activity against c-KIT and PDGFR, however, due to their different molecular weights demonstrating varying effects on male fertility. For example, nilotinib has a larger molecular weight compared to imatinib and does not readily cross the blood-testis barrier, therefore demonstrates minimal effects on male fertility [8, 33]. In mice exposed to nilotinib, Seval et al. demonstrated spermatogenesis is preserved [12]. Likewise, dasatinib also does not appear to affect male fertility; however, adverse side effects of its use in mice studies include decreased size and secretion of seminal vesicles, and an immature prostate [8, 33]. At this time, very little is known regarding the effects of bosutinib on male fertility; however, it, too, has a larger molecular weight similar to nilotinib and therefore less likely to cross the blood-testis barrier [33]. Murine studies revealed both dasatinib and bosutinib did not have a statistically significant impact on testosterone levels compared to controls [32].
Fertility preservation in males traditionally has not posed as much difficulty as seen in women. For male partners looking to conceive, cryopreservation of sperm should be considered prior to initiating TKI therapy. If the disease state is stable, providers may consider stopping chemotherapy for a 72-day washout period to allow for sperm maturation followed by either natural conception or sperm cryopreservation [9, 33].
Treatment duration of TKI therapy and impact on fertility
For most cancers, there are a finite number of treatment cycles with chemotherapeutic agents to achieve remission followed by discontinuation of the agent. CML and other leukemias are unique in that these cancers are not often fatal, with the advent of TKIs reducing annual mortality in CML from 10–20% to 1–2%. With such highly effective treatment, many patients can live decades with their disease. With the development of oral chemotherapeutic agents that prolong progression-free survival, the question then becomes when is the optimal time to temporarily stop all therapies to undergo IVF or carry a pregnancy?
The ultimate duration of TKI therapy is dependent on the cancer it is treating. For treatment of GI stromal tumors, standard of care for adjuvant therapy is 3 years with most experts advocating for cessation of therapy at this point, and only to restart treatment once recurrence has been documented [34, 35]. Presently, there have not been any studies that have followed patients to observe long-term effects or survival benefits of continuing imatinib beyond 5 years [34]. For CML, treatment is often lifelong; however, the multicenter STIM trial and other subsequent studies have demonstrated the feasibility of temporarily discontinuing once deep molecular remission has been achieved for 2 years [7, 28, 36,37,38]. Studies have shown there is progression of disease once a TKI is stopped, with most recurrences 6 to 24 months after discontinuing adjuvant therapy in GI stromal tumors, and 6 to 8 months in CML [2, 3, 34, 37]. Given that side effects of TKIs as a class are generally well tolerated, patients with good response could be on lifelong treatment [2, 37]. Approximately 50–60% of patients with CML who have discontinued therapy will relapse into another crisis 6 months following cessation of treatment [10]. Therefore, the risks and benefits of discontinuing treatment during pregnancy should be carefully discussed with a multidisciplinary approach. For couples trying to conceive, timing and cessation of TKI therapy for reproductive treatment, conception, and pregnancy require a coordinated effort between the patient’s oncologist and obstetrician/gynecologist. Fertility counseling in young adults may also be required if treatment of CML is complicated by gonadotoxic therapies such as regimens for bone marrow/stem cell transplantation [39].
Effects of imatinib and other TKIs on the placenta and early embryo
In pregnancy, the mature placenta acts as a barrier preventing drugs with large molecular weights from readily crossing and exposing the fetus to potentially harmful toxins. For the most part, TKIs have large molecular weights (~ 500 g/mole), therefore do not easily cross the placenta. A study by Abellar et al. examined 3rd trimester placentas in women exposed to imatinib during pregnancy for treatment of CML [40]. Although a small sample size (n = 4), the placentas only demonstrated nonspecific changes with weights all appropriate for gestational age. Similarly, other studies demonstrated umbilical cord blood and placental tissue had only a fraction of the concentration of imatinib as maternal serum concentrations [41, 42]. These histopathology results are in line with other studies which suggest imatinib does not readily cross a 3rd trimester placenta, and therefore may be considered safe to use following organogenesis [40,41,42]. Despite this, long-term exposure to imatinib in mice models, even after cessation of the drug, led to small placentas with abnormal vasculature [43]. Furthermore, long-term use of imatinib has been shown to affect the cellular differentiation of an embryo prior to implantation by decreasing the total number of cells in the blastocyst stage, thereby reducing the embryo’s overall developmental potential [13]. Early exposure prior to development of the blood-placenta barrier and the inhibition of c-KIT and PDGFR likely lead to abnormal placentation and angiogenesis, thus leading to the malformations seen with imatinib use [42, 43] (Fig. 1). Similar to imatinib, nilotinib does not readily cross the placenta, due to its molecular weight having the lowest placenta to maternal concentrations of all TKIs [42]. Bosutinib is also considered a larger molecule; however, no studies have directly evaluated placental transfer of the drug [8]. On the other hand, dasatinib is a considerably smaller molecule which has been shown to cross the placenta. Dasatinib inhibits the Src-family kinases which are needed for proper implantation and fetal maturation [44]. Cortes et al. demonstrated transplacental concentrations of dasatinib to be 75% of maternal serum concentrations; therefore, extreme caution should be employed in sexually active women on dasatinib [20].
Possible teratogenic effects of imatinib and other TKIs
CML represents 10% of all leukemias diagnosed during pregnancy [44]. Despite warnings against conceiving and/or continuing imatinib and other second-generation TKIs during pregnancy, there have been multiple case reports of both men and women conceiving while on imatinib without increased prevalence of spontaneous abortion and congenital anomalies in offspring compared to the general population [16, 45]. Spontaneous abortion is described as a nonviable, intrauterine pregnancy with an empty gestational sac or a gestational sac containing an embryo or fetus lacking fetal heart activity in early pregnancy (that is, up to 13 completed weeks of pregnancy) [46]. It is well documented that the incidence of spontaneous abortions, also known as early pregnancy loss, is frequent, occurring in approximately 10% of all clinically documented pregnancies in the general population[47,48,49]. Regarding congenital anomalies, major structural or genetic birth defects affect one in every 33 babies (about 3% of all babies) born in the USA each year [50]. There are over 300 published cases of women who conceived while on imatinib (Table 1). Of these studies, roughly 50–66% of pregnancies resulted in normal births [20, 51]. Still, there are several case reports describing teratogenic effects on infants conceived while a parent was on imatinib. Reported malformations include clinodactyly, cleft palate, hypospadias, and low-set ears, as well as severe deformities including cardiac malformations (such as dextrocardia, situs inversus, and overriding aorta), neurologic deformities (such as ventriculomegaly, hydrocephalus, and cerebellar hypoplasia), and kidney malformations including mal-positioned or even absent kidneys [45, 52]. The largest retrospective study by Pye et al. investigated pregnancy outcomes in 180 women (125 with known outcomes) exposed to imatinib during their pregnancy, with 26% of patients in the study continuing imatinib throughout the duration of their pregnancy [45]. In this study, a total of 9.6% of the pregnancies resulted in some form of fetal abnormality. Interestingly, they described a cluster of skeletal abnormalities (craniosynostosis, exencephaly, encephalocele, scoliosis, and hemivertebrae) in 4% of pregnancies, along with an omphalocele in 2.5% of these pregnancies, whereas the incidence in the general population of this same defect is 1:3000 to 1:4000, with roughly half of these resulting in stillbirths [45]. As this same cluster of malformations (skeletal, renal, and/or abdominal wall defects) were also seen in mice models with PDGFR-knockouts, they postulated such abnormalities were not by random chance but likely due to a TKI-induced syndromic effect.
In the included studies, we found 331 reported cases of women who either conceived while on imatinib or were exposed during early pregnancy (Table 1). Of those with known delivery outcomes (n = 296), 53% (158/296) of patients had term deliveries of normal infants, with 3.7% of deliveries resulting in a pregnancy complication (fetal growth restriction, premature delivery, and intrauterine fetal demise). Of all pregnancies, 20% (66/331) of women elected for a termination of pregnancy, and 16% (53/331) resulted in a spontaneous abortion. A total of 5.1% (17/331) of all pregnancies resulted in some form of a congenital malformation. The reported number of elective terminations in these women (20%) was much higher than the rate of elective terminations reported in the general US population (11.3 abortions per 1000 women aged 15–44 years) [53]. There is paucity of data regarding the gestational age and the indications for elective termination of pregnancy. Of the ten studies presenting data regarding elective terminations of pregnancy in women taking TKIs [9, 18, 20, 36, 44, 45, 54,55,56,57], only three studies indicate that the termination was performed in the first trimester [9, 55, 56] and two studies indicate that women underwent elective terminations in the first and second trimester [20, 36]. Few reported indications included fetal malformations on ultrasound [45, 54, 56] and early growth restriction [9]; however, most studies did not comment on the indication of the elective terminations [18, 36, 44, 55, 57].
In contrast, male partners on TKI therapy do not appear to have the same teratogenic effects on embryos seen in females taking TKIs during conception (Table 2). Most case reports of males conceiving while on TKIs have resulted in normal pregnancies. There are no case studies that have demonstrated an increased risk of spontaneous miscarriage or congenital malformations in males taking imatinib during conception [8, 33]. In the included studies, 186 men were on imatinib at the time of conception (Table 1). This resulted in 88% (164/186) term deliveries of normal infants, and 2.7% of pregnancies resulting in a spontaneous abortion. There were only 4 documented congenital malformations, including a mild intestinal malrotation, mild hydrocephalus, primary hydronephrosis, and a complex cardiac anomaly [55, 56, 61].
Pregnancy outcomes for men and women on dasatinib during conception are similar to published reports regarding imatinib (Table 3). A large case series by Cortes et al. evaluated 147 pregnancies conceived by men and women while on dasatinib that were submitted to a national database [20]. Of the 78 women who conceived while on dasatinib, pregnancy outcomes were reported for 59% (46 of 78 patients). Of these, 33% (15/46) resulted in full-term deliveries, while 4 women had pregnancy complications (one IUGR observed at term, one IUGR with preterm delivery at 28 weeks, and one placental abruption at 34 weeks of gestation). In this study, 39% (18/46) underwent elective termination of pregnancy and 17% (8/46) suffered spontaneous miscarriage. Despite the vast majority of women discontinuing treatment upon confirmation of pregnancy, fetal abnormalities were identified in seven infants, two after birth, and five after abortion (two spontaneous and three elective) which included hydrops fetalis, renal abnormalities, CNS/cranial abnormalities, and skeletal abnormalities similar to those seen with exposure to imatinib during the development stage [20]. Of the 69 pregnancies conceived by men on dasatinib, 43% (33/69) have reported outcomes, and of these, an overwhelming 91% resulted in full-term deliveries of normal neonates [20].
There is a paucity of data on the effects of nilotinib during conception and pregnancy (Table 4). Case reports and small case series published in literature of three women and three men who conceived while on nilotinib resulted in four normal pregnancies, one neonate born with an omphalocele, and one unidentified fetal abnormality [20, 33]. More recently, Dou et al. published a case series of 4 women who either conceived while on nilotinib and subsequently discontinued after confirmation of pregnancy or discontinued a few weeks prior to planned pregnancy [63]. Three resulted in normal full-term deliveries, with one pregnancy resulting in a spontaneous abortion. All of these women were able to achieve a complete molecular response after reinitiating therapy following delivery [63].
A recent study by Cortes et al. examined the safety profile of bosutinib as it relates to conception and pregnancy [18]. Sixteen pregnancies were identified in women who conceived while on bosutinib (Table 5). Of those with known outcomes (n = 10 pregnancies), 60% (6/10) resulted in live births, 30% (3/10) elective abortion, and 10% (1/10) spontaneous abortion. In this study, seventeen males also conceived while on bosutinib. Fourteen pregnancies had known outcomes, including 64% (9/14) full-term live births, 29% (4/14) elective abortion, and 7% (1/7) spontaneous abortion [18]. Although data in humans is limited, studies in rabbits demonstrated congenital fetal anomalies in pregnant rabbits exposed to bosutinib, leading to the manufacturer recommendation of avoiding pregnancy while on treatment [8, 18].
A total of 396 women were on a first- or second-generation TKI therapy at the time of conception or early pregnancy (Table 6). Of the cases with detailed pregnancy and delivery outcomes (n = 361), 51% (186/361) resulted in a term birth of a normal infant without complications, similar to previously reported rates [45]. Interestingly, in 22% of the total pregnancies (87/396), women elected to undergo a termination of pregnancy, while 16% (63/396) of pregnancies ended in a spontaneous abortion. This is slightly higher than the spontaneous abortion rate of 10% for women in the general population [45, 46], which could indicate the early teratogenicity of TKIs leading to a miscarriage. Overall, 4.3% (16/361) of pregnancies resulting in live birth had a pregnancy complication, and 5% of pregnancies resulted in the live birth of an infant with a congenital anomaly. In contrast, of the 236 men included in our study, 87% conceived pregnancies which resulted in term deliveries of normal infants. Elective terminations, miscarriage rate, pregnancy complication rate, and incidence of a congenital malformation were all less than those seen in females (4%, 3%, 2%, and 2.5%, respectively).
In women who are taking TKI, breastfeeding is not recommended. Chelysheva et al. measured concentrations of imatinib and nilotinib in human breast milk and found that the estimated maximal dose for both the drugs is less than the therapeutic doses [64]. However, the impact of low-dose chronic exposure of these TKIs on infants remains unknown.
Conclusion
The use of TKIs on a more global scale for treatment of CML has drastically improved survival rates of reproductive age adults. With this improvement in survivorship, there is a growing need to understand the effects of TKIs on fertility. While there is limited data on imatinib and other 2nd-generation TKIs’ short- and long-term effects on fertility, as a class they are considered a category D medication during pregnancy. Several studies have shown imatinib’s use has adverse effects on ovarian function, which is important to keep in mind when counseling women who otherwise may not have considered assisted reproductive technology to maintain future fertility [16].
Mouse and human studies looking at the reproductive effects of TKIs have shown adverse effects on ovarian stimulation and ongoing spermatogenesis; however, there are insufficient studies regarding long-term consequences from use of TKI on fertility potential [12, 16, 25, 27]. Though there is data that approximately 50–60% of women who conceived while taking a TKI during pregnancy have delivered normal fetuses [45], analysis of existing literature indicates a higher risk of spontaneous abortion, congenital malformation, and elective terminations in women who conceived while taking a TKI. Because of this, women should be advised to avoid conception while taking a TKI. Women on TKIs who are considering pregnancy should be encouraged to plan the pregnancy to minimize inadvertent first trimester exposure. In women who conceive while taking TKIs, the serious risk of relapse due to discontinuation of TKI should be balanced against the potential risks to the fetus. Providers should utilize individualized decision-making and may allow for observation of the pregnancy without treatment with TKIs with close monitoring and surveillance of the pregnancy with a maternal fetal medicine specialist or to restart the TKI or other forms of treatment if maternal health is at risk. Fertility preservation for a woman taking a TKI can be considered to plan a pregnancy to minimize the TKI-free period. With careful monitoring, providers may consider a TKI washout period (even though evidence is limited regarding the ideal washout period), followed by controlled ovarian stimulation to cryopreserve oocytes or embryos, with a plan to resume TKIs until ready to conceive or to transfer an embryo to achieve pregnancy quickly. Fertility preservation is also indicated if a patient on TKI is requiring a gonadotoxic therapy such as regimens for stem cell transplantation or reproductive surgery impacting fertility. Women should also be advised that they can resume therapy once they are delivered with favorable outcomes despite a break in treatment [35, 38]. The risk of teratogenicity to a fathered pregnancy with TKI use is considerably lower; however, they should be warned their fertility could be compromised during the duration of treatment. Further studies evaluating any long-term teratogenic effects of TKIs in humans beyond the developmental stage, such as epigenetic changes, should be considered.
There are several strengths to this study. To our knowledge, this is the largest review in the English language of pregnancies conceived (exclusive of case reports and non-indexed data) while on one of the four TKIs discussed in this review. By including pregnancy complications, such as preterm birth, and all malformations described in the literature, we have provided a thorough overview of the risks and benefits of conceiving while on a TKI. We believe our comprehensive review will give providers the necessary information to make informed decisions with their patients regarding effects of TKIs on fertility and pregnancy. However, our review also highlights the paucity of data available on second-generation TKIs despite these drugs being now considered first line in the treatment of CML. Additional studies on the effects of TKIs on fertility and reproduction, especially as it relates to the use of nilotinib, dasatinib, and bosutinib, are needed.
The results of the study are limited by reported pregnancies currently published in literature. Given the nature of this study, there is an inability to control for confounders which may affect reported pregnancy rates or comment on the true effect of TKIs on fertility, such as a preexisting infertility diagnosis. Furthermore, as there is currently no standardization for a TKI-free period prior to conception to minimize risks of teratogenicity, the true prevalence of fetal malformations could be higher and subjected to reporting bias. This study is only applicable to imatinib and the second-generation TKIs nilotinib, dasatinib, and bosutinib, and generalization to newer TKIs should be used with caution. Further studies are needed to elucidate the timing of cessation of a TKI prior to conception to reduce the risk of teratogenic effects. Long-term studies to determine whether there are epigenetic risks to babies born even after cessation of a TKI should be considered. Ultimately, patients on TKIs contemplating pregnancy or fertility preservation should be encouraged to collaborate with their reproductive endocrinologist, medical oncologist, and maternal fetal medicine specialist to individualize care in order to achieve the best maternal and neonatal outcomes.
References
Druker BJ, Talpaz M, Resta DJ, Peng B, Buchdunger E, Ford JM, et al. Efficacy and safety of a specific inhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. N Engl J Med. 2001;344(14):1031–7. https://doi.org/10.1056/nejm200104053441401.
Cioffi A, Maki RG. GI stromal tumors: 15 years of lessons from a rare cancer. J Clin Oncol. 2015;33(16):1849–54. https://doi.org/10.1200/jco.2014.59.7344.
von Mehren M, Joensuu H. Gastrointestinal stromal tumors. J Clin Oncol Off J Am Soc Clin Oncol. 2018;36(2):136–43. https://doi.org/10.1200/jco.2017.74.9705.
Parsons SJ, Parsons JT. Src family kinases, key regulators of signal transduction. Oncogene. 2004;23(48):7906–9. https://doi.org/10.1038/sj.onc.1208160.
Montero JC, Seoane S, Ocaña A, Pandiella A. Inhibition of SRC family kinases and receptor tyrosine kinases by dasatinib: possible combinations in solid tumors. Clin Cancer Res. 2011;17(17):5546–52. https://doi.org/10.1158/1078-0432.Ccr-10-2616.
DeAngelo DJ, Attar EC. Use of dasatinib and nilotinib in imatinib-resistant chronic myeloid leukemia: translating preclinical findings to clinical practice. Leuk Lymphoma. 2010;51(3):363–75. https://doi.org/10.3109/10428190903518295.
Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2020 update on diagnosis, therapy and monitoring. Am J Hematol. 2020;95(6):691–709. https://doi.org/10.1002/ajh.25792.
Abruzzese E, Trawinska MM, de Fabritiis P, Baccarani M. Management of pregnant chronic myeloid leukemia patients. Expert Rev Hematol. 2016;9(8):781–91. https://doi.org/10.1080/17474086.2016.1205479.
Zhou L, You JH, Wu W, Li JM, Shen ZX, Wang AH. Pregnancies in patients with chronic myeloid leukemia treated with tyrosine kinase inhibitor. Leuk Res. 2013;37(10):1216–21. https://doi.org/10.1016/j.leukres.2013.07.020.
Pallera A, Altman JK, Berman E, Abboud CN, Bhatnagar B, Curtin P, et al. NCCN guidelines insights: chronic myeloid leukemia, Version 1.2017. J Natl Compr Cancer Netw. 2016;14(12):1505–12. https://doi.org/10.6004/jnccn.2016.0162.
Chu S, Alexiadis M, Fuller PJ. Expression, mutational analysis and in vitro response of imatinib mesylate and nilotinib target genes in ovarian granulosa cell tumors. Gynecol Oncol. 2008;108(1):182–90. https://doi.org/10.1016/j.ygyno.2007.09.017.
Cengiz Seval G, Özkavukçu S, Seval M, Aylı M. Gonadotoxic effects of nilotinib in chronic myeloid leukemia treatment dose in a mouse model. Turk J Hematol. 2017;34(2):137–42. https://doi.org/10.4274/tjh.2016.0092.
Salem W, Ho JR, Woo I, Ingles SA, Chung K, Paulson RJ, et al. Long-term imatinib diminishes ovarian reserve and impacts embryo quality. J Assist Reprod Genet. 2020;37(6):1459–66. https://doi.org/10.1007/s10815-020-01778-7.
McGinnis LK, Albertini DF, Kinsey WH. Localized activation of Src-family protein kinases in the mouse egg. Dev Biol. 2007;306(1):241–54. https://doi.org/10.1016/j.ydbio.2007.03.024.
McGinnis LK, Kinsey WH, Albertini DF. Functions of Fyn kinase in the completion of meiosis in mouse oocytes. Dev Biol. 2009;327(2):280–7. https://doi.org/10.1016/j.ydbio.2008.11.038.
Zamah AM, Mauro MJ, Druker BJ, Oktay K, Egorin MJ, Cedars MI, et al. Will imatinib compromise reproductive capacity? Oncologist. 2011;16(10):1422–7. https://doi.org/10.1634/theoncologist.2011-0137.
Bernard V, Bouilly J, Kramer P, Carré N, Schlumberger M, Visser JA, et al. The tyrosine kinase inhibitor sunitinib affects ovulation but not ovarian reserve in mouse: a preclinical study. PLoS One. 2016;11(4):e0152872. https://doi.org/10.1371/journal.pone.0152872.
Cortes JE, Gambacorti-Passerini C, Deininger M, Abruzzese E, DeAnnuntis L, Brümmendorf TH. Pregnancy outcomes in patients treated with bosutinib. International journal of hematologic oncology 9 (2):Ijh26. 2020. https://doi.org/10.2217/ijh-2020-0004.
US FDA bosulif (bosutinib) prescribing information. 2017. https://www.accessdata.fda.gov/drugsatfdadocs/label/2017/203341s009lbl.pdf. Accessed 17 Feb 2021.
Cortes JE, Abruzzese E, Chelysheva E, Guha M, Wallis N, Apperley JF. The impact of dasatinib on pregnancy outcomes. Am J Hematol. 2015;90(12):1111–5. https://doi.org/10.1002/ajh.24186.
Gazdaru S, Perey L, Rosselet A, Mathevet P, Chalandon Y, Vulliemoz N. Successful ovarian stimulation for fertility preservation in a patient with chronic myeloid leukemia: switch from nilotinib to interferon-α. Oncologist. 2018;23(6):719–21. https://doi.org/10.1634/theoncologist.2017-0381.
Christopoulos C, Dimakopoulou V, Rotas E. Primary ovarian insufficiency associated with imatinib therapy. N Engl J Med. 2008;358(10):1079–80. https://doi.org/10.1056/NEJMc0707841.
Furukawa Y, Takahashi T, Suganuma R, Ohara M, Ota K, Kyozuka H, et al. Successful planned pregnancy through vitrified-warmed embryo transfer in a woman with chronic myeloid leukemia: case report and literature review. Mediterr J Hematol Infect Dis. 2020;12(1):e2020005. https://doi.org/10.4084/mjhid.2020.005.
Rios SJ, Martínez-Montesinos L, Aroca C, Teruel-Montoya R, Ferrer-Marín F. Successful ovarian stimulation and pregnancy in an infertile woman with chronic myeloid leukemia. J Assist Reprod Genet. 2020;37(10):2473–6. https://doi.org/10.1007/s10815-020-01907-2.
Nurmio M, Toppari J, Zaman F, Andersson AM, Paranko J, Söder O, et al. Inhibition of tyrosine kinases PDGFR and C-Kit by imatinib mesylate interferes with postnatal testicular development in the rat. Int J Androl. 2007;30(4):366–76; discussion 376. https://doi.org/10.1111/j.1365-2605.2007.00755.x.
Prasad AM, Ramnarayan K, Nalini K, Bairy KL. Effect of imatinib on the biochemical parameters of the reproductive function in male Swiss albino mice. Indian J Pharm. 2011;43(4):389–92. https://doi.org/10.4103/0253-7613.83107.
Heim C, Minniear K, Dann CT. Imatinib has deleterious effects on differentiating spermatogonia while sparing spermatogonial stem cell self renewal. Reprod Toxicol (Elmsford, NY). 2011;31(4):454–63. https://doi.org/10.1016/j.reprotox.2010.12.056.
Samis J, Lee P, Zimmerman D, Arceci RJ, Suttorp M, Hijiya N. Recognizing endocrinopathies associated with tyrosine kinase inhibitor therapy in children with chronic myelogenous leukemia. Pediatr Blood Cancer. 2016;63(8):1332–8. https://doi.org/10.1002/pbc.26028.
Mariani S, Basciani S, Fabbri A, Agati L, Ulisse S, Lubrano C, et al. Severe oligozoospermia in a young man with chronic myeloid leukemia on long-term treatment with imatinib started before puberty. Fertil Steril. 2011;95(3):1120.e1115–27. https://doi.org/10.1016/j.fertnstert.2010.08.060.
Chang X, Zhou L, Chen X, Xu B, Cheng Y, Sun S, et al. Impact of imatinib on the fertility of male patients with chronic myelogenous leukaemia in the chronic phase. Target Oncol. 2017;12(6):827–32. https://doi.org/10.1007/s11523-017-0521-6.
Gambacorti-Passerini C, Tornaghi L, Cavagnini F, Rossi P, Pecori-Giraldi F, Mariani L, et al. Gynaecomastia in men with chronic myeloid leukaemia after imatinib. Lancet. 2003;361(9373):1954–6. https://doi.org/10.1016/s0140-6736(03)13554-4.
Tauer JT, Ulmer A, Glauche I, Jung R, Suttorp M. Long-term imatinib treatment does not cause testicular toxicity in male adolescents with chronic myeloid leukemia and in a juvenile rat model. Klin Padiatr. 2014;226(3):169–74. https://doi.org/10.1055/s-0034-1372643.
Abruzzese E, Trawinska MM, Perrotti AP, De Fabritiis P. Tyrosine kinase inhibitors and pregnancy. Mediterr J Hematol Infect Dis. 2014;6(1):e2014028. https://doi.org/10.4084/mjhid.2014.028.
Benjamin RS, Casali PG. Adjuvant imatinib for GI stromal tumors: when and for how long? J Clin Oncol. 2016;34(3):215–8. https://doi.org/10.1200/jco.2015.64.0102.
Rousselot P, Huguet F, Rea D, Legros L, Cayuela JM, Maarek O, et al. Imatinib mesylate discontinuation in patients with chronic myelogenous leukemia in complete molecular remission for more than 2 years. Blood. 2007;109(1):58–60. https://doi.org/10.1182/blood-2006-03-011239.
Iqbal J, Ali Z, Khan AU, Aziz Z. Pregnancy outcomes in patients with chronic myeloid leukemia treated with imatinib mesylate: short report from a developing country. Leuk Lymphoma. 2014;55(9):2109–13. https://doi.org/10.3109/10428194.2013.866662.
Hochhaus A, Baccarani M, Silver RT, Schiffer C, Apperley JF, Cervantes F, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34(4):966–84. https://doi.org/10.1038/s41375-020-0776-2.
Mahon FX, Réa D, Guilhot J, Guilhot F, Huguet F, Nicolini F, et al. Discontinuation of imatinib in patients with chronic myeloid leukaemia who have maintained complete molecular remission for at least 2 years: the prospective, multicentre Stop Imatinib (STIM) trial. Lancet Oncol. 2010;11(11):1029–35. https://doi.org/10.1016/s1470-2045(10)70233-3.
Liu J, Malhotra R, Voltarelli J, Stracieri AB, Oliveira L, Simoes BP, et al. Ovarian recovery after stem cell transplantation. Bone Marrow Transplant. 2008;41(3):275–8. https://doi.org/10.1038/sj.bmt.1705893.
Abellar RG, Pepperell JR, Greco D, Gundogan F, Kostadinov S, Schwartz J, et al. Effects of chemotherapy during pregnancy on the placenta. Pediatr Dev Pathol. 2009;12(1):35–41. https://doi.org/10.2350/08-03-0435.1.
Russell MA, Carpenter MW, Akhtar MS, Lagattuta TF, Egorin MJ. Imatinib mesylate and metabolite concentrations in maternal blood, umbilical cord blood, placenta and breast milk. J Perinatol: official journal of the California Perinatal Association. 2007;27(4):241–3. https://doi.org/10.1038/sj.jp.7211665.
Chelysheva E, Turkina A, Polushkina E, Shmakov R, Zeifman A, Aleshin S, et al. Placental transfer of tyrosine kinase inhibitors used for chronic myeloid leukemia treatment. Leuk Lymphoma. 2018;59(3):733–8. https://doi.org/10.1080/10428194.2017.1347929.
Salem W, Li K, Krapp C, Ingles SA, Bartolomei MS, Chung K, et al. Imatinib treatments have long-term impact on placentation and embryo survival. Sci Rep. 2019;9(1):2535. https://doi.org/10.1038/s41598-019-39134-0.
Madabhavi I, Sarkar M, Modi M, Kadakol N. Pregnancy outcomes in chronic myeloid leukemia: a single center experience. J Glob Oncol. 2019;5:1–11. https://doi.org/10.1200/jgo.18.00211.
Pye SM, Cortes J, Ault P, Hatfield A, Kantarjian H, Pilot R, et al. The effects of imatinib on pregnancy outcome. Blood. 2008;111(12):5505–8. https://doi.org/10.1182/blood-2007-10-114900.
ACOG Practice Bulletin No. 200. Early Pregnancy Loss. Obstet Gynecol. 2018;132(5):e197–207. https://doi.org/10.1097/aog.0000000000002899.
Wang X, Chen C, Wang L, Chen D, Guang W, French J. Conception, early pregnancy loss, and time to clinical pregnancy: a population-based prospective study. Fertil Steril. 2003;79(3):577–84. https://doi.org/10.1016/s0015-0282(02)04694-0.
Wilcox AJ, Weinberg CR, O’Connor JF, Baird DD, Schlatterer JP, Canfield RE, et al. Incidence of early loss of pregnancy. N Engl J Med. 1988;319(4):189–94. https://doi.org/10.1056/nejm198807283190401.
Zinaman MJ, Clegg ED, Brown CC, O’Connor J, Selevan SG. Estimates of human fertility and pregnancy loss. Fertil Steril. 1996;65(3):503–9.
Centers for Disease Control and Prevention (CDC). Update on overall prevalence of major birth defects–Atlanta, Georgia, 1978–2005. MMWR Morb Mortal Wkly Rep. 2008;57(1):1–5.
Cole S, Kantarjian H, Ault P, Cortés JE. Successful completion of pregnancy in a patient with chronic myeloid leukemia without active intervention: a case report and review of the literature. Clin Lymphoma Myeloma. 2009;9(4):324–7. https://doi.org/10.3816/CLM.2009.n.064.
Jain N, Sharma D, Agrawal R, Jain A. A newborn with teratogenic effect of imatinib mesylate: a very rare case report. Med Princ Pract. 2015;24(3):291–3. https://doi.org/10.1159/000381806.
Kortsmit K, Jatlaoui TC, Mandel MG, Reeves JA, Oduyebo T, Petersen E, et al. Abortion Surveillance - United States, 2018. Morbidity and mortality weekly report. Surveill Summ (Washington, DC: 2002). 2020;69(7):1–29. https://doi.org/10.15585/mmwr.ss6907a1.
Hensley ML, Ford JM. Imatinib treatment: specific issues related to safety, fertility, and pregnancy. Semin Hematol. 2003;40(2 Suppl 2):21–5. https://doi.org/10.1053/shem.2003.50038.
Ault P, Kantarjian H, O’Brien S, Faderl S, Beran M, Rios MB, et al. Pregnancy among patients with chronic myeloid leukemia treated with imatinib. J Clin Oncol. 2006;24(7):1204–8. https://doi.org/10.1200/jco.2005.04.6557.
Mukhopadhyay A, Dasgupta S, Kanti Ray U, Gharami F, Bose CK, Mukhopadhyay S. Pregnancy outcome in chronic myeloid leukemia patients on imatinib therapy. Ir J Med Sci. 2015;184(1):183–8. https://doi.org/10.1007/s11845-014-1084-5.
Lasica M, Willcox A, Burbury K, Ross DM, Branford S, Butler J, et al. The effect of tyrosine kinase inhibitor interruption and interferon use on pregnancy outcomes and long-term disease control in chronic myeloid leukemia. Leuk Lymphoma. 2019;60(7):1796–802. https://doi.org/10.1080/10428194.2018.1551533.
Ramasamy K, Hayden J, Lim Z, Mufti GJ, Ho AY. Successful pregnancies involving men with chronic myeloid leukaemia on imatinib therapy. Br J Haematol. 2007;137(4):374–5. https://doi.org/10.1111/j.1365-2141.2007.06542.x.
Breccia M, Cannella L, Montefusco E, Frustaci A, Pacilli M, Alimena G. Male patients with chronic myeloid leukemia treated with imatinib involved in healthy pregnancies: report of five cases. Leuk Res. 2008;32(3):519–20. https://doi.org/10.1016/j.leukres.2007.07.022.
Alizadeh H, Jaafar H, Rajnics P, Khan MI, Kajtár B. Outcome of pregnancy in chronic myeloid leukaemia patients treated with tyrosine kinase inhibitors: short report from a single centre. Leuk Res. 2015;39(1):47–51. https://doi.org/10.1016/j.leukres.2014.10.002.
Carlier P, Markarian M, Bernard N, Lagarce L, Dautriche A, Béné J, et al. Pregnancy outcome among partners of male patients receiving imatinib, dasatinib or nilotinib in chronic myeloid leukemia: reports collected by the French network pharmacovigilance centers. Arch Gynecol Obstet. 2017;295(2):269–71. https://doi.org/10.1007/s00404-016-4262-z.
Moura AC, Delamain MT, Duarte GBO, Lorand-Metze I, Souza CA, Pagnano KBB. Management of chronic myeloid leukemia during pregnancy: a retrospective analysis at a single center. Hematol Transfus Cell Ther. 2019;41(2):125–8. https://doi.org/10.1016/j.htct.2018.10.001.
Dou X, Qin Y, Huang X, Jiang Q. Planned pregnancy in female patients with chronic myeloid leukemia receiving tyrosine kinase inhibitor Therapy. Oncologist. 2019;24(11):e1141–7. https://doi.org/10.1634/theoncologist.2019-0109.
Chelysheva E, Aleshin S, Polushkina E, Shmakov R, Shokhin I, Chilov G, et al. Breastfeeding in patients with chronic myeloid leukaemia: case series with measurements of drug concentrations in maternal milk and literature review. Mediterr J Hematol Infect Dis. 2018;10(1):e2018027. https://doi.org/10.4084/mjhid.2018.027.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rambhatla, A., Strug, M.R., De Paredes, J.G. et al. Fertility considerations in targeted biologic therapy with tyrosine kinase inhibitors: a review. J Assist Reprod Genet 38, 1897–1908 (2021). https://doi.org/10.1007/s10815-021-02181-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-021-02181-6