
Abstract
Purpose
To analyze the fertilization, embryo development, and clinical outcome of immature oocytes obtained from natural cycle IVF in women with regular cycles.
Methods
Natural cycle IVF was performed in 28 patients who had normal ovaries, > 6 antral follicle counts and were less than 40 years old (n = 28 cycles). An hCG trigger of 10,000 IU was administered 36 h before oocyte collection when the diameter of the dominant follicle (DF) was over 12 mm. Oocytes were retrieved from DF as well as from the cohort of smaller follicles. Embryological aspects of the mature and immature oocytes retrieved from these cycles as well as the implantation and clinical pregnancy rates depending on the origin of the embryos transferred were evaluated.
Result(s)
Overall clinical pregnancy and implantation rates were 20.8 % and 6.7 %, respectively. There were no differences in in vitro maturation (IVM), fertilization and embryo development between immature oocytes retrieved with and without in vivo matured oocytes. However, the clinical and implantation rates in cycles with embryos produced from in vivo matured oocytes transferred were better than the cycles where only IVM embryos were transferred (30.8 %, 9.1 % vs. 9.1 %, 3.2 %).
Conclusion(s)
Although our results show that immature oocytes from natural cycle IVF can fertilize normally and can be used to increase the number of embryos available for transfer, the embryos derived from the immature oocytes in natural cycles IVF have a poorer reproductive potential.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The first successful childbirth resulting from IVF was produced with a natural cycle of IVF [1]. Pregnancy rates in natural cycle IVF have been reported variously between 0 and 30 % after embryo transfer [2, 3]. This is most likely because the natural cycle depends solely upon the development of a dominant follicle (DF). As a result, ovarian stimulation was developed to generate more follicles and therefore more oocytes, replacing the natural cycle IVF [4, 5]. This increases the probability of a successful pregnancy. However, IVF as practiced today is complex, time-consuming and expensive. It generates much stress and side effects such as ovarian hyperstimulation. Thus, there has been a resurgence of interest in natural cycle IVF treatment in recent years including a modified form such as controlled natural cycle IVF, minimal stimulation IVF and in vitro maturation (IVM) [6]. Nevertheless, the disadvantage of fewer available oocytes and therefore fewer embryos remains. This result in relatively low pregnancy rates and high cancellation rates associated with these IVF cycles.
Recently, the concept of “natural cycle IVF combined with IVM (IVF/M)” has been proposed, which suggests that natural cycle IVF might be combined with immature oocyte retrieval and IVM [7–11]. In addition to the embryo produced by the mature oocyte from the DF, embryos produced by the IVM oocytes will also be available, therefore possibly increasing the chances of pregnancy in a natural cycle. Administrating hCG when the DF reaches 14 mm diameter [8] or more recently 12–14 mm [9–11] to obtain mature oocytes and viable sibling immature oocytes has been recommended. However, evidence is lacking on whether the immature oocytes retrieved after the follicle gains dominance (> 12 mm) in a natural cycle actually contribute to the pregnancy rate. Therefore, in this study, we assessed the embryological differences of immature oocytes retrieved in the course of natural cycle IVF as well as the mature oocytes. Outcomes were fertilization result, embryo quality, implantation rates, clinical pregnancy rate and live birth in embryos derived from mature and immature oocytes within the same natural cycle.
Materials and methods
Medical records of all women who underwent natural cycle IVF retrieved with immature oocytes from 2004 to 2008 at McGill University Health Centre, Montreal were evaluated. The retrospective study was approved by the Research and Ethics Board of the McGill University Health Centre.
Patients
A total of 28 patients (n = 28 cycles) who underwent natural cycle IVF were included in this analysis. Inclusion criteria were patients who had normal ovaries with regular cycles, > 6 antral follicle in both ovaries and less than 40 years old.
Monitoring
The treatment cycle was initiated on the basis of an ultrasound scan on day 3–5. Transvaginal ultrasound scans were repeated on day 7–9 and repeated at 1–3-day intervals until the leading follicle reached over 12 mm in diameter and the endometrial thickness was ≥ 6 mm. At this point 10,000 IU hCG was administered [9, 10].
Oocyte collection
The Oocyte retrieval was performed 36 h after hCG priming. Transvaginal ultrasound–guided collection of oocytes was performed using a 19-gauge aspiration needle (K-OPS-7035-RWH-ET, Cook, Australia) with a reduced aspiration pressure of 7.5 kPa. The aspirates were collected in tubes with prewarmed heparinized saline. The oocyte collection started with the DF and the needle was flushed completely with saline, and oocyte maturity was assessed. Subsequent collection of oocytes was performed according to accessibility of the smaller follicles following which the maturity level of the oocyte was determined. To avoid the possibility of missing oocytes with a small amount of cumulus cells, the remaining follicular aspirates were filtered using 70-μm mesh in hole size (Falcon, Becton Dickinson & Company, NJ, USA). They were washed with oocyte wash medium (Cooper Surgical, CT, USA) that contained HEPES buffer supplemented with recombinant human serum albumin and the oocytes were isolated under a stereomicroscope.
In vitro maturation
The nuclear maturity of the collected oocytes was assessed under the dissecting microscope with high magnification (x80) using the spreading method [12]. If no germinal vesicle (GV) was observed in the oocyte cytoplasm, the cumulus masses were removed with hyaluronidase and mechanical pipetting was carried out after the oocyte retrieval was completed. Reassessment of oocyte maturity was then performed. Oocytes that were mature on the oocyte retrieval day (Day 0: 0–6 h) were inseminated on the same day, while the immature oocytes (GV- or Germinal vesicle breakdown (GVBD)-stage) were cultured in IVM medium (Cooper Surgical, CT, USA) supplemented with 75 mIU/ml FSH and LH. Following culture on day 1 (24–30 h), the oocytes were denuded of cumulus cells with hyaluronidase and mechanical pipetting.
IVF, in vitro development and embryo transfer
Matured oocytes were inseminated by intracytoplasmic sperm injection (ICSI) using the partner’s spermatozoa. ICSI was performed at least 1 h after observing first polar body (PB) extrusion as suggested by Hyun et al. [13]. Fertilization was assessed 16–18 h after insemination for the appearance of two distinct pronuclei and two polar bodies. The zygotes were cultured in COOK cleavage medium (Cook company, Australia). Embryonic development was assessed on day 2 (41–43 h) and on day 3 (65–67 h) after insemination according to the regularity of blastomeres, the percentage and pattern of anucleate fragments, and all dysmorphic characteristics of the embryos. For this study, we defined embryos as good quality, if they had a 4-cell embryo on day 2 and a 7- or 8-cell embryo on day 3, contained <20 % anucleate fragments and exhibited no apparent morphological abnormalities. Embryos showing blastomere multi-nucleation, poor cell adhesion, uneven cell division and cytoplasmic abnormalities were defined as low quality. Embryos were transferred on day 2 or day 3 after ICSI, depending on the number and quality of the embryos, under ultrasound guidance using a Wallace catheter (SIMS Protex Ltd., Hyth, Kent, United Kingdom).
Endometrium preparation
For endometrial preparation, patients received estradiol valerate (Estrace; Roberts Pharmaceutical, Mississauga, Canada), starting on the day of oocyte retrieval. If the endometrial thickness was 6–8 mm, 8–10 mg dose was given, and if it was ≥ 8 mm, a 6 mg dose was administered, all in divided doses. Luteal support was provided by administering 50 mg of progesterone daily intra-muscularly starting on the day of ICSI and continued, along with estradiol valerate, until 12 weeks of gestation, if the pregnancy test was positive.
Data analysis
The IVM and embryo developmental potential of sibling immature oocytes were analyzed between cycles with and without in vivo matured oocytes. Clinical outcome of the natural IVF cycles was analyzed in two groups according to the origin of transferred embryos as follows; Group 1: cycles that only had IVM embryos transferred as a result of collecting only immature oocytes, failure of oocyte collection from the DF or failed fertilization of the in vivo matured oocytes, and Group 2: cycles that had transferred embryos derived from oocytes matured in vivo and in vitro.
Statistical analysis
Statistical analyses were performed using the χ 2, Fisher’s exact, McNemar’s or t-test as appropriate. All P-values quoted are two-sided, and values < 0.05 indicate statistical significance. Analyses were performed using the SPSS statistical package (SPSS, Inc., Chicago).
Results
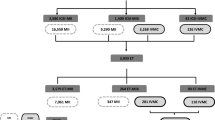
Characteristic of natural IVF cycles in this study is shown in Table 1. Table 2 summarizes the overall embryological and clinical aspects of this study. Out of 28 cycles, 3 cycles (DF: 13.5, 15 and 16 mm at hCG) did not undergo oocyte retrieval because of premature ovulation. One cycle did not undergo embryo transfer (ET) because of lack of maturation (DF = 16 mm at hCG). Sixteen out 28 cycles had in vivo matured oocytes. However, three cycles had no embryos generated from the in vivo matured oocytes because of failed fertilization and so they only had IVM embryos transferred. Overall clinical pregnancy and implantation rates after ET were 20.8 % (5/24) and 6.7 % (5/75), respectively. Table 3 summarizes the embryological aspects of in vivo matured oocytes and in vitro matured oocytes in the cycles. In the cycles with in vivo matured oocytes (n = 19), a total 149 oocytes were retrieved and 28 of them were matured in vivo. In the 9 natural cycles, a total of 70 immature oocytes were retrieved. There was no significant difference in the rate of in vitro maturation between immature oocytes retrieved from cycles with and without in vivo matured oocytes (67.0 %, 81/121 vs. 70.0 %, 49/70). Significantly higher quality embryos were produced from in vivo matured oocytes than that from sibling in vitro matured oocytes (P < 0.05). However, there were no differences in fertilization and embryo development between immature oocytes retrieved from cycles with and without in vivo matured oocytes (Table 3).
The clinical and implantation rates in the group where at least one embryo produced from an in vivo matured oocyte was transferred were better than those of the group where only embryos produced from in vitro matured oocytes were transferred (30.8 % (4/13), 9.1 % (4/44) vs. 9.1 % (1/11), 3.2 % (1/31)), but the numbers were too small to reach statistical significance (Table 4). A pregnant patient in group 2 had a GV-stage oocyte retrieved from a 16.5 mm DF follicle at collection. Therefore, no in vivo mature oocyte was obtained in this cycle. All pregnancies had a single gestational sac with heart beat and resulted in singleton live births.
Discussion
This study demonstrates that in the presence of a DF the cohort of small follicles can yield immature oocytes capable of generating embryos. However, these embryos generated from the sibling immature oocytes have little effect on clinical outcome.
It has been believed for a long time that oocyte retrieval for IVM program should take place before the development of a DF which affects rest of the cohort to become atretic. The DF can be distinguished from other cohort of follicles by a size >10 mm diameter in humans [14]. Nevertheless, Barnes and Sirard [15] reported that some of the oocytes in early atretic follicles still possess the competence to support embryonic development.
However, this notion has recently been challenged. Chian et al. [16] reported that in the bovine model, the maturational and developmental competence of immature oocytes derived from the small antral follicles was not affected by the presence of a DF or the phase of folliculogenesis. Thornton et al. [17] observed that successful pregnancies can be obtained from immature oocytes retrieved during the mid-cycle aspiration of a DF following hCG priming in unstimulated cycles. In a case series reported by Chian et al. [7] three pregnancies were achieved after the combination of natural cycle IVF/M and transfer of resulting embryos. Lim et al. [10] reported good pregnancy rates after performing natural cycle IVF/M. Based on these studies, Chian and Lim have suggested that developmental competence of immature oocytes is not detrimentally affected by the presence of any size of the DF during the follicular phase and the embryos produced from the immature oocytes could contribute to an increased chance of a pregnancy. However, they did not report on either the embryo development of sibling immature oocytes retrieved from these cycles or how much these embryos contributed to the increase in overall pregnancy rates.
In this study, therefore, we collected data from patients who had the same protocol of natural cycle IVF/M as previously reported [8, 10] and analyzed the embryological and clinical results of natural cycle IVF for women who had normal ovaries. We compared embryos produced from oocytes matured in vivo and in vitro and found that sibling immature oocytes could mature in vitro, fertilize and some of them could develop to good quality embryos similar to the animal model that was reported by Chian [16]. However, when the clinical outcome was assessed in detail depending on the origin of the embryos transferred, a much better pregnancy rate (30.8 %) was obtained in cycles where the transferred embryos were derived from in vivo matured oocytes than in cycles without any embryos produced from in vivo matured oocytes (9.1 %) (Table 4). The pregnant patient in the cycle where only embryos produced from immature oocytes were transferred had only GV-stage oocytes even though they originated from the DF (16.5 mm at collection). Although, we could not verify the origin of the embryo that implanted, it is tempting to speculate that the DF that contained a GV-stage oocyte was not able to suppress the rest of the small follicles. In addition, the three cycles in which only IVM embryos were transferred because no embryos were generated from in vivo matured oocytes due to failed fertilization, did not result in a pregnancy. Our results imply that the clinical outcome most likely relies on the presence of embryos produced from in vivo matured oocytes, similar to that observed in pure natural cycle IVF, and the sibling immature oocytes seem to be adversely affected when a follicle gains dominance (DF > 12 mm) at the time of hCG administration.
It is difficult to make conclusions about the reproductive potential of immature oocytes with only embryological data. From our study, the sibling immature oocytes could not contribute to increased pregnancy outcome. In support of this observation, Lim et al. [9] reported previously that most pregnancies after performing natural cycle IVF/M were achieved from cycles that had in vivo matured oocytes (36.3 %, 33/91). When patients had only in vitro matured oocytes, the pregnancy rate was only 9.4 % (3/32). Although the DF diameter on the day of hCG varied from < 12 to > 17 mm in their study, the clinical outcome is similar to our present study (Table 4). Recently, the same group reported a clinical outcome difference, even though the clinical pregnancy was not different between cycles with and without in vivo matured oocytes (40.1 % vs. 34.9 %), leading to a live birth rate which was significantly higher in the cycles where in vivo matured oocytes were obtained (29.6 % vs. 16.4 %) [11]. However, the authors did not analyze the embryological and clinical outcomes based on the diameter of the DF at the time of hCG administration. In addition, they also did not mention whether they used the same criteria for triggering hCG as their previous study or not. We have previously reported that there were no differences in the rates of clinical pregnancy and implantation between the IVM cycles where embryos were transferred with and without embryos produced from in vivo matured oocytes when hCG priming was administered when the DF reached 10–12 mm, even though the study groups were for women who had polycystic ovaries [18]. Our present data is also consistent with that of Paulson et al. [19], who reported that all pregnancies occurred in the cycles in which one of the embryos was derived from the DF (17 %, 11/66) in unstimulated IVF cycles of women with regular cycles and all of the implantations were singleton. No pregnancy was achieved in the cycles where only IVM embryos were transferred (0 %, 0/10). In their study, the mean DF diameter on day of hCG was about 19 mm.
In conclusion, our data strongly suggest that once a DF is selected (> 12 mm), the embryos generated from the sibling immature oocytes have a poorer reproductive potential, even though they can mature, fertilize and develop. Our results emphasize the concept that the size of the DF at the time of hCG plays an important role in the contribution of the sibling immature oocytes towards achieving a pregnancy in natural IVF cycles. The clinical significance of using immature oocytes in natural cycle IVF needs further evaluation to determine the optimal time to retrieve viable immature oocytes.
References
Steptoe PC, Edwards RG. Birth after the reimplantation of a human embryo. Lancet. 1978;2(8085):366.
MacDougall MJ, Tan SL, Hall V, Balen A, Mason BA, Jacobs HS. Comparison of natural with clomiphene citrate-stimulated cycles in in-vitro fertilization: a prospective, randomized trial. Fertil Steril. 1994;61:1052–7.
Janssens RM, Lambalk CB, Vermeiden JP, Schats R, Bernards JM, et al. In-vitro fertilization in a spontaneous cycle:easy, cheap and realistic. Hum Reprod. 2000;15:314–8.
Johnston I, Lopata A, Speirs A, Hoult I, Kellow G, du Plessis Y. In vitro fertilization: the challenge of the eighties. Fertil Steril. 1981;36:699–706.
Lopata A, Brown JB, Leeton JF, Talbot JM, Wood C. In vitro fertilization of preovulatory oocytes and embryo transfer in infertile patients treatedwith clomiphene and human chorionic gonadotropin. Fertil Steril. 1978;30:27–35.
Edwards RG. IVF, IVM, natural cycle IVF, minimal stimulation IVF – time for a rethink. Reprod Biomed Online. 2007;15:106–19.
Chian RC, Buckett WM, Abdul Jalil AK, Son WY, Sylvestre C, Rao D, et al. Natural-cycle in vitro fertilization combined with in vitro maturation of immature oocytes is a potential approach in infertility treatment. Fertil Steril. 2004;82:1675–8.
Chian RC, Lim JH, Tan SL. State of the art in in-vitro oocyte maturation. Curr Opin Obstet Gynecol. 2004;16:211–9.
Lim JH, Park SY, Yoon SH, Yang SH, Chian RC. Combination of natural cycle IVF with IVM as infertility treatment. In: Tan SL, Chian RC, Buckett WM, editors. In-vitro maturation of human oocytes: basic science to clinical application. London: Informa Healthcare Press; 2007. p. 353–60.
Lim JH, Yang SH, Xu Y, Yoon SH, Chian RC. Selection of patients for natural cycle in vitro fertilization combined with in vitro maturation of immature oocytes. Fertil Steril. 2009;91:1050–5.
Yang SH, Patrizio P, Yoon SH, Lim JH, Chian RC. Comparison of pregnancy outcomes in natural cycle IVF/M treatment with or without mature oocytes retrieved at time of egg collection. Syst Biol Reprod Med. 2012;58:154–9.
Son WY, Tan SL. Laboratory and embryological aspects of hCG-primed in vitro maturation cycles for patients with polycystic ovaries. Hum Reprod Update. 2010;16:675–89.
Hyun CS, Cha JH, Son WY, Yoon SH, Kim KA, Lim JH. Optimal ICSI timing after the first polar body extrusion in in vitro matured human oocytes. Hum Reprod. 2007;22:1991–5.
Ginther OJ, Beg MA, Bergfelt DR, Donadeu FX, Kot K. Follicle selection in monovular species. Biol Reprod. 2001;65:638–47.
Barnes FL, Sirard MA. Oocyte maturation. Semin Reprod Med. 2000;18:123–31.
Chian RC, Chung JT, Downey BR, Tan SL. Maturational and developmental competence of immature oocytes retrieved from bovine ovaries at different phases of folliculogenesis. Reprod Biomed Online. 2002;4:127–32.
Thornton MH, Francis MM, Paulson RJ. Immature oocyte retrieval: lessons from unstimulated IVF cycles. Fertil Steril. 1998;70:647–50.
Son WY, Chung JT, Herrero B, Dean N, Demirtas E, Holzer H, et al. Selection of the optimal day for oocyte retrieval based on the diameter of the dominant follicle in hCG-primed in vitro maturation cycles. Hum Reprod. 2008;23:2680–5.
Paulson RJ, Sauer MV, Francis MM, Macaso T, Lobo RA. Factors affecting pregnancy success of human in-vitro fertilization in unstimulated cycles. Hum Reprod. 1994;9:1571–5.
Financial disclosure
No financial support to disclose
Author information
Authors and Affiliations
Corresponding author
Additional information
Capsule
Although immature oocytes from natural cycle IVF can fertilize normally and can be used to increase the number of embryos available for transfer, the embryos derived from the immature oocytes in natural cycles IVF have a poorer reproductive potential.
Rights and permissions
About this article
Cite this article
Son, WY., Chung, JT., Das, M. et al. Fertilization, embryo development, and clinical outcome of immature oocytes obtained from natural cycle in vitro fertilization. J Assist Reprod Genet 30, 43–47 (2013). https://doi.org/10.1007/s10815-012-9889-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-012-9889-5