
Abstract
Relatively few studies have examined gender differences in infants and toddlers, and most focus on clinically referred samples or high-risk infant cohorts. The current study aimed to examine gender differences in early autism manifestations and cognitive development in a community-ascertained sample. In total, 46 males and 21 females with ASD were seen at approximately 24 and 48 months of age. No significant gender differences were observed on overall cognitive ability, verbal skills, non-verbal skills, overall autism severity, or restricted repetitive behaviours. However, females were found to exhibit more social communication impairments than males. These findings may indicate that female toddlers with less severe or different, social communication impairments may be more likely to be missed during routine surveillance during toddlerhood.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Gender estimates have remained stable in autism spectrum disorder (ASD), ranging between 3 and 4 males for every female (Baio 2012; Fombonne 2009; Bryson and Smith 1998; Baxter et al. 2015; Lotter 1966; Wing 1981). However, the gender ratio has been noted to be different among those with an intellectual disability (1.31–1.95:1) versus those with average intelligence (4.4–5.5:1) (Fombonne 2005; Tsai and Beisler 1983). Due to the large disparity in prevalence between the genders, differences between males and females with ASD have long been of interest. However, most of the older studies examining gender difference in ASD have focused on school-aged children who were traditionally diagnosed during their childhood years (Lord et al. 1982; Solomon et al. 2012; Volkmar et al. 1993; McLennan et al. 1993; Mandy et al. 2012; Banach et al. 2008). Advances in understanding the early autism phenotype has meant that children can now be successfully identified and diagnosed in toddlerhood (Barbaro and Dissanayake 2009, 2013; Clifford and Dissanayake 2008; Landa and Garrett-Mayer 2006; Osterling et al. 2002; Ozonoff et al. 2010; Young et al. 2003), with diagnoses remaining stable over time (Barbaro and Dissanayake 2016; Clark et al. 2017). However, despite progress in understanding the early manifestations of autism, few studies to date have investigated gender differences in infants and toddlers.
Carter et al. (2007) were amongst the first to investigate gender differences in cognitive abilities and autism manifestations in toddlers with ASD. In a clinical sample of 68 males [M (SD) = 28.4 (3.5) months] and 22 females [M (SD) = 28.1 (3.9) months], they found lower scores in females than males in motor development, adaptive behaviour, and emotional development. However, females had better visual reception abilities than males, contrary to findings among older age groups (Lord et al. 1982; Volkmar et al. 1993). It is important to note, nonetheless, that these gender differences were minimal, with no other differences in cognition. Subsequent research examining cognition in toddlers with ASD has found no difference in the developmental profile of males and females in clinical (Sipes et al. 2011; Hartley and Sikora 2009) or community samples (Westman-Andersson et al. 2013).
The findings regarding gender differences in core autism symptoms in toddlers are more varied. Carter et al. (2007) found no significant gender differences in these symptoms in their clinical sample of toddlers with ASD, using the Autism Diagnostic Observation Schedule (ADOS; Lord et al. 2000) and the Autism Diagnostic Interview-Revised (ADI-R; Lord et al. 1994a). Similarly, Westman-Andersson et al. (2013) found no gender differences in autism manifestations in a smaller community sample of toddlers (20 males, 20 females, 21–45 months) matched on age and cognition, using the ADOS. A recent study by Reinhardt et al. (2015) also reported no difference in core autism symptoms in a large sample of young children with ASD ascertained through paediatric community screening, younger siblings of children with ASD, and other children referred due to developmental concerns [234 males, 54 females; M (SD) = 28.09 (12.30) months].
Some studies have reported gender differences in autism symptoms in their young samples. Hartley and Sikora (2009) found that young males with ASD within a clinical sample [n = 157, M (SD) = 35.51 (7.09) months] had significantly more RRBs than females [n = 42, M (SD) = 35.98 (7.29) months], while females showed better social communication skills. Similarly, Sipes et al. (2011) also found that males with ASD within a clinical sample exhibited more RRBs compared to females with ASD. These mixed findings may be a result of studies examining gender differences in young children with ASD across broad age ranges whereby gender differences may be confounded by developmental effects.
To date two studies have utilised high-risk infant cohorts to examine gender differences among young children with an older sibling with ASD. The high-risk infant cohort model allows the investigation of the development of ASD among infants at a higher risk of developing ASD. Chawarska et al. (2016) investigated gender differences in social attention in sample of 101 “high-risk” siblings (71 males and 31 females) and 61 low risk infants (32 males and 29 females). Social attention was assessed at 6 and 12 months of age. It was observed that the female infants spent significantly more time than their male counterparts attending to social scenes and faces. Moreover, the high-risk females also spent more time attending to social stimuli than their low risk female counterparts. Increased attention to social stimuli was also associated with fewer ASD symptoms at 24 months among the high-risk group for both genders. Similarly, Zwaigenbaum et al. (2012) observed a female advantage in social and communication scores measured by the ADI-R, and on the socialisation and daily living skills subscales on the Vineland Adaptive Behaviour Scales when examining a sample of high and low risk children at 3 years of age [M (SD) = 38.1 (2.5) months]. It was also found that females in all three groups (high risk ASD, high-risk non-ASD, and low risk) had lower scores on the ADOS severity metric compared to their male counterparts. The results from these two studies illustrate that females with ASD may exhibit superior social skills compared to their male counterparts, which in turn may result in fewer ASD symptoms. However, there is growing evidence that the genetic mechanisms underlying multiplex and simplex ASD are different (Sebat et al. 2007; Campbell et al. 2006; Christian et al. 2008; Itsara et al. 2010). Therefore, results attained from high-risk infant cohort studies may not provide results reflective of the entire ASD spectrum.
One study has examined gender differences longitudinally in a clinically referred sample of 30 male and female children with ASD, aged between 2 and 5 years, across two time points (Posterino et al. 2015). No gender differences were found in core autism manifestations at either point in time. At the initial assessment, females had significantly lower cognition scores compared to males, but both genders improved over time with no significant difference between genders at follow-up. However, as Postorino et al. (2015) examined a clinically referred sample, it is difficult to draw conclusions regarding general population with ASD .
Methods of recruitment can have a significant impact on the generalisability of results between studies. A recent study conducted by Sacrey et al. (2017) examined differences between children recruited through a high-risk sibling study and those recruited through a community referral programme. It was found that those in the high-risk sibling cohort had better adaptive behaviour and less severe social-communication impairments compared to the community referral group. This result illustrates the importance of considering sampling bias when recruiting participants. The advantage of utilising a sample of children ascertained via prospectively identified, low-risk, community-based screening is that these samples are not subject to the biases inherent in high-risk and clinical cohorts. Therefore, the examination of these community-based cohorts allows for better extrapolation of findings to the general ASD population. Furthermore, limited longitudinal research has been conducted examining the early developmental trajectories of males and females with ASD, and no studies have examined these trajectories within a community-based sample.
The aim in the current study was to examine gender differences in early autism manifestations and cognitive development in a community-ascertained sample of children with ASD from 24 to 48 months of age. Based on the existing literature, we predicted no significant differences in the cognitive profiles between males and females with ASD over time, but expected both groups to improve in cognition between the two time points based on the expected receipt of early intervention (Vivanti and Dissanayake 2016; Vivanti et al. 2014; Anderson et al. 2007). Based on the mixed findings to date on gender differences in autism symptoms (Charman et al. 2005; Gotham et al. 2012; Lord et al. 2012a), no directional hypothesis was proposed. However, it was expected that autism severity would remain stable over time (Shumway et al. 2012; Gotham et al. 2012).
Method
Participants
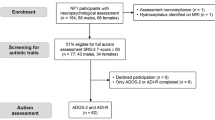
Participants were drawn from a larger, community-based study known as the Social Attention and Communication Study (SACS; Barbaro and Dissanayake 2010), in which children were referred for a developmental assessment by their Maternal and Child Health (MCH) nurse, following identification of early markers of ASD. All children were seen and followed-up by the SACS team at the Child Development Unit (CDU), La Trobe University. The clinicians were trained to research reliability on both the ADOS and ADI-R. Participants were initially seen for a diagnostic assessment during toddlerhood at approximately 24-months of age. A diagnostic decision was made based on information obtained from the ADOS and ADI-R in combination with clinical judgement. Participants were invited to attend a follow-up assessment approximately 24 months later. In total, 46 males and 21 females with ASD were seen at both baseline, during toddlerhood, and pre-school age. However, as it was not possible to complete the non-verbal cognitive scales for one female at follow-up, due to behavioural difficulties during the assessment, the analyses examining non-verbal cognitive development included only 20 females.
Measures
Mullen Scales of Early Learning (MSEL; Mullen 1995)
Four of the MSEL subscales were administered to each participant: fine motor, visual reception, receptive language, and expressive language. Developmental quotients (DQ) were calculated for each subscale by dividing the participant’s chronological age by their estimated age equivalent on each subscale. Verbal and Non-verbal DQs were calculated by averaging the two individual verbal and nonverbal DQs. An overall developmental quotient was also calculated by averaging the four individual developmental quotients.
Autism Diagnostic Observation Schedule-Generic (Ados-G; Lord et al. 2000) and Autism Diagnostic Observation Schedule-2 (Ados-2; Lord et al. 2012b)
Both the ADOS-G and ADOS-2 are semi-structured, standardised assessments of social interaction, communication, play, and imaginative use of materials, administered to individuals suspected of having ASD. As participants that comprise the sample were seen across a number of years, they were assessed in the clinic using a mixture of the ADOS-G and ADOS-2. To enable comparison of symptom severity across the differing ADOS versions and modules, Gotham et al. (2006) revised “Social Affect” (SA) and “Restricted and Repetitive Behaviours” (RRB) algorithm scores were calculated. These total scores were then converted into comparison scores for the both the individual SA and RRB domains, based on algorithms by Hus et al. (2014). A total severity score was also calculated based on the comparison score matrices by Gotham et al. (2009).
Procedure
Ethical approval for the study was obtained from the La Trobe University Human Ethics Committee, and all parents provided informed consent to participate in the project. Parents attended the CDU where the ADOS-G/ADOS-2 and MSEL were administered by trained clinicians with research reliability. Parents were also interviewed using the ADI-R (Lord et al. 1994b) by an experienced clinician. Diagnostic decisions were determined using these tools in combination with clinical judgement. Parents were recontacted and invited to participate in a follow-up assessment, which involved the administration of the same assessment tools at preschool age.
Results
At the baseline assessment, children were aged between 23 and 33 months of age [males: M (SD) = 25.1 (1.8) months; females: M (SD) = 26.2 (2.7) months]; they were between 36 and 59 months of age at the follow-up assessment [males: M (SD) = 49.3 (4.2) months; females: M (SD) = 48.7 (4.0) months]. Independent samples t tests indicated no significant differences between the males and females on chronological age at baseline, t (28.2) = − 1.69, p = .102, or follow-up, t (65) = .562, p = .576. The average amount of time between the two assessments was 23.6 months, with no difference between the genders, t (65) = 1.38, p = .173.
Exploratory bivariate correlation analyses were conducted to examine the relationships between cognition and autism severity at each age within the male and female samples. Values above .33 were considered meaningful, regardless of significance, which accounts for 10% of the variance. Table 1 presents the results from this analysis with the baseline data presented above the line and the follow up data below the line.
A slightly different pattern for the two genders emerges when examining the relationship between cognition and autism manifestations. At the initial assessment, cognition and autism manifestations were not strongly related among either males or females. However, at the follow-up assessment, there were moderate to strong negative associations between all ADOS and MSEL variables among the male participants. For the female participants, the only meaningful association was between SA and verbal DQ (r = − .381).
The cocor package for statistical comparison of dependent correlations (Diedenhofen and Musch 2015)was used to calculate if there was a significant difference in the correlation between autism severity and overall cognition at baseline compared to follow-up within each gender. Among males, the association between autism severity and overall cognition was significantly stronger at follow-up compared to baseline (z = 2.25, p = .025). There was no significant difference between baseline and follow-up for females (z = .976, p = .329).
Cognitive Development
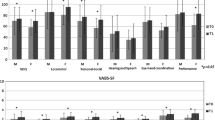
A 2 (Gender) × 2 (Time) repeated measures ANOVA conducted on overall DQ showed no differences between males and females, F (1, 64) = .335, p = .565, η2 = .005 (Fig. 1).There was a significant main effect of Time, such that both groups improved in their overall DQ from baseline to follow-up, F (1, 64) = 14.70, p < .001, η2 = .187, and the interaction was not significant, F (1, 64) = .121, p = .729, η2 = .002.

Developmental quotients (DQ) from the Mullen Scales of Early Learning (MSEL) presented by gender and time point
Two 2 (Gender) × 2 (Time) repeated measures ANOVAs were conducted to examine whether there were any significant differences between male and female participants on their verbal or non-verbal DQs. There was no main effect of Gender on non-verbal DQ, F (1, 64) = .351, p = .556, η2 = .005, or verbal DQ, F (1, 65) = .180, p = .673, η2 = .003. In addition, there was no change between the two time points for non-verbal DQ, F (1, 64) = .001, p = .973, η2 < .001. However, there was a significant increase in verbal DQ between the two time points, F (1, 65) = 48.51, p < .001, η2 = .427, such that verbal DQ was higher at follow up compared to the initial assessment. The interaction effects between Time and Gender was not significant for either non-verbal DQ, F (1, 64) = .051, p = .822, η2 = .001, or verbal DQ, F (1, 65) = .263, p = .610, η2 = .004.
Autism Manifestations
The repeated measures ANOVA on autism severity revealed no reliable difference between the genders, F (1, 65) = 3.01, p = .088, η2 = .044, although there was a slight trend toward females having higher severity scores than males (Fig. 2). There was a significant change in autism severity between the two time points, F (1, 65) = 14.03, p < .001, η2 = .178, such that autism severity decreased at the follow-up assessment compared to baseline. The interaction effect was not significant, F (1, 65) = .045, p = .832, η2 = .001.

Autism Diagnostic Observation Schedule (ADOS) comparison scores presented by gender and time point
The individual ADOS subscales were also analysed for gender differences using two repeated measures ANOVAs. There was a significant gender difference with a medium effect size on the SA subscale, F (1, 65) = 4.61, p = .036, η2 = .066, but not the RRB scale, F (1, 65) = .001, p = .970, η2 < .001. As apparent in Table 1, females had more SA symptoms compared to males. Both the SA and RRB scores were significantly lower at the follow up assessment compared to baseline, F (1, 65) = 7.22, p = .009, η2 = .100 and F (1, 65) = 6.81, p = .011, η2 = .095 respectively. There was no significant interaction effect for either SA, F (1, 65) = .150, p = .700, η2 = .002, or RRB scores, F (1, 65) = 2.79, p = .099, η2 = .041.
Discussion
The aim in this study was examine gender differences in cognition and autism manifestations among young children with ASD from 24 to 48 months of age who had been ascertained from a community-based sample. This is the first study to examine gender differences across time in a community-based cohort. Consistent with the previous literature (Solomon et al. 2012; Hartley and Sikora 2009; Sipes et al. 2011; Westman-Andersson et al. 2013) and the study hypothesis, no significant gender differences were observed on overall cognitive ability, or on verbal and non-verbal ability.
In line with Postorino et al. (2015) and our hypothesis, both male and female children improved in their overall cognition from baseline (24-months) to follow-up (48-months), with this change over time appearing to be largely driven by an improvement in verbal ability. No change was seen in the groups between the two time points on non-verbal ability. For both genders, verbal ability was lower at both time points than non-verbal ability, consistent with previous findings (Hartley and Sikora 2009; Carter et al. 2007). The improvement in verbal skills across the two time-points supports previous literature that has found improvements over time among children with ASD in receipt of early intervention, which tends to have marked effects on verbal ability in particular (Vivanti and Dissanayake 2016; Vivanti et al. 2014; Anderson et al. 2007).
In regards to autism manifestations, no significant difference was found between males and females on overall autism severity or on RRBs, as measured by the ADOS. This finding contradicts some previous research reporting that males have significantly higher levels of RRBs compared to females. However, most of the research conducted in this area has examined older children with ASD (Lord et al. 1982; Mandy et al. 2012; McLennan et al. 1993; Solomon et al. 2012; Supekar and Menon 2015). To date only two studies have found higher RRBs among male toddlers with ASD (Hartley and Sikora 2009; Sipes et al. 2011). The current finding is supported by four previous studies that also noted no differences in RRBs between male and female toddlers with ASD (Carter et al. 2007; Reinhardt et al. 2015; Postorino et al. 2015). Interestingly a meta-analysis found that the gender difference in RRBs does not become apparent until 6 years of age (Van Wijngaarden-Cremers et al. 2014), suggesting that the children in the current study may be too young to observe any gender difference in the manifestations of RRBs. In addition, it has been argued that females with ASD may experience RRBs outside the realm of what is captured by the diagnostic criteria, which is mainly based on research conducted on males with ASD (Mandy et al. 2012; Hull et al. 2016; Hiller et al. 2014, 2016; Sutherland et al. 2017).
The young female children with ASD in the current study exhibited more deficits in social affect compared to their male counterparts. This finding is consistent with those of McLennan et al. (1993) and Banach et al. (2008) who both observed more communication difficulties among school-aged females with ASD. However, the literature examining young children with ASD is more varied. Some studies found no gender difference in social communication (Carter et al. 2007; Westman-Andersson et al. 2013; Reinhardt et al. 2015; Sipes et al. 2011), two found that females had superior social communication skills (Hartley and Sikora 2009; Zwaigenbaum et al. 2012), and one showed enhanced social attention among high-risk female toddlers (Chawarska et al. 2016).
Children were referred to the current study by their Maternal and Child Health nurse, following routine surveillance and identified as “at risk” on the SACS tool (Barbaro and Dissanayake 2010, 2013). It is possible that this referral process may have been subject to a gender bias. Previous research has identified that females with ASD are often diagnosed later than males (Begeer et al. 2013; Rivet and Matson 2011; Holtmann et al. 2007), and tend to be referred for other comorbid conditions rather than an ASD assessment (Holtmann et al. 2007; Mandy and Tchanturia 2015; Kopp and Gillberg 1992). Therefore, it is possible that the female toddlers in the current study were those that presented with more severe social communication difficulties, which are typically considered consistent with a diagnosis of ASD.
The finding that females with ASD were more impaired in their social communication skills in this community-based sample is consistent with the theory that females with ASD might exhibit social camouflaging skills and thus are less readily identified by standard assessment techniques. The social camouflage theory was proposed to help explain the large gender ratio in ASD diagnosis of 3–4:1 (Wing 1981; Attwood 2007). Research examining this theory has found school aged females are more likely to integrate their verbal and non-verbal behaviours (Hiller et al. 2014), use gestures to facilitate their communication (Rynkiewicz et al. 2016), and engage in a reciprocal conversation (Hiller et al. 2014). Adolescent females with ASD are also more likely to have better friendships than males (Head et al. 2014), and adult females show fewer autism features in social contexts (Lai et al. 2011). One study examining pre-diagnosis concerns also found that caregivers reported that females aged between 6 and 17 years were able to engage in complex imitation and presented with different restricted interests compared to males (Hiller et al. 2016). It is unlikely however, that toddler females with ASD would have the necessary social skills to engage in social camouflage. However, it is interesting to note that Chawarska et al. (2016) recently found that ‘high risk sibling’ females exhibit more attention to socially related stimuli than their male counterpart within the first year of life. Taken together, the results from the current study may suggest that females with more social communication difficulties are more readily identified through community surveillance prior to 24 months of age, although this cannot be conclusively determined without follow-up studies comparing the genders through different sampling methods.
This is the first study to find that toddler females with ASD exhibit more social communication impairments than males with ASD. A strength of this study is that the community-based cohort was recruited through ongoing surveillance of their social attention and communication behaviours by trained nurses (Barbaro and Dissanayake 2010; Barbaro et al. 2011). This is also the first study to investigate gender differences across time within a community sample. The current finding that the greater severity in social affect among females remains from toddlerhood to preschool age is one that requires further investigation and replication across different sampling methods.
Indeed, the change in autism symptoms overtime runs counter to our hypothesis that these would remain stable over time. That is, the overall severity score on the ADOS was significantly lower at the follow-up assessment compared to baseline for both genders. This same pattern was also observed for each of the individual social affect and RRB subscales, suggesting an improvement in autism severity over time. This finding contrasts with Postorino et al. (2015), who found no difference across time in autism severity on the ADOS. However, the ages of the children examined by Postorino et al. (2015) ranged from 2 to 5 years at baseline and were a clinically referred sample whereas the current study utilized a community-based sample diagnosed with ASD by 2-years of age. The observed improvement in ADOS scores may suggest that early identification, in facilitating access to early intervention, significantly influenced the core autism manifestations, as was the case for cognition. Together with the improvements in verbal cognition over time, these findings provide support for the benefit of early identification for both males and females with ASD. However, as the current study did not aim to investigate the impact of early intervention, this discussion must remain tentative.
Consistent with previous research, an inverse relationship was found between cognitive ability and autism symptoms (Skuse et al. 2009). However, it is of interest that this association was not significant among males or females when they were 2-years of age. By preschool age, this relationship was evident between all the cognition and autism variables in males. Among females, only the SA subscale was meaningfully associated with verbal ability at follow-up. Thus in both genders, the inverse association between cognition and autism severity became stronger over time, despite improved cognition and symptom severity at follow-up. This finding supports the suggestion that social communication deficits early in development impacts input from the environment, affecting learning and subsequent cognitive development (Vivanti et al. 2013). Further, it appears that this association is stronger among males than females, although the smaller sample size of females may have influenced this finding, which calls for replication.
It is important to acknowledge the limitations in the current study. In a recent meta-analysis, Hull et al. (2016) argued that in order to accurately assess gender difference in ASD it is necessary to also examine a group of typically developing children. Inclusion of this latter group allows researchers to tease apart the difference between ‘typical’ gender differences and gender differences specifically associated with ASD. As the current study did not include a matched typically developing sample, we are unable to comment on the whether the difference between the genders found here are typical of those observed among children without ASD. Further research is required to accurately characterise the developmental pathways of males and females with ASD and without ASD.
An additional limitation was the relatively small sample of participants, particularly for the females, which was then amplified due to attrition at follow-up. In the only other follow-up study of gender differences to date, Postorino et al. (2015) had a slightly larger sample of 30 females with ASD from baseline to follow-up. However, as noted earlier, the ages of the children in their study ranged between 2 and 5 years of age at baseline. The current study examined longitudinal gender differences in a sample of 48 males and 21 females who were within a narrow age range at both baseline and follow-up. Nevertheless, replication of the current findings in a larger longitudinal sample is important.
The current study only focused on gender differences in cognition and autism manifestations during toddlerhood and preschool age. It is important to consider that differences may exist between genders on variables not considered in this study (e.g., adaptive functioning). Indeed, the meta-analysis by Hull et al. (2016) also found gender differences among individuals with ASD in internalising and externalising behaviours as well as in executive functions. Future research should investigate the presence of these differences in toddlerhood and the development of this wider range of behaviours over time.
In conclusion, the only gender difference found in our very young community-based sample of children with ASD was in their social communication impairments, where females exhibited more impairments than males with ASD, which were maintained over time. No differences were found between the genders in cognition or on RRBs. The findings may indicate that toddler females with fewer, or different, social attention and communication impairments may be more difficult to identify early, and are thus not referred for an ASD assessment prior to 24 months of age. Importantly, improvements in both verbal ability and autism manifestations were noted from toddlerhood to preschool age, with both males and females showing the same developmental changes over time. Combined, these findings support the importance of early identification and intervention in children with ASD. Further, it is apparent that a greater focus is needed on the identification of toddler females, who may be more likely to be missed during routine surveillance and screening.
References
Anderson, D. K., Lord, C., Risi, S., DiLavore, P. S., Shulman, C., Thurm, A., et al. (2007). Patterns of growth in verbal abilities among children with autism spectrum disorder. Journal of Consulting and Clinical Psychology, 75(4), 594–604. https://doi.org/10.1037/0022-006X.75.4.594.
Attwood, T. (2007). The complete guide to Asperger’s syndrome. London: Jessica Kingsley.
Baio, J. (2012). Prevalence of autism spectrum disorders: Autism and Developmental Disabilities Monitoring Network, 14 Sites, United States, 2008. Morbidity and Mortality Weekly Report. Surveillance Summaries. Vol. 61, No. 3. Centers for Disease Control and Prevention.
Banach, R., Thompson, A., Szatmari, P., Goldberg, J., Tuff, L., Zwaigenbaum, L., et al. (2008). Brief report: Relationship between non-verbal IQ and gender in autism. Journal of Autism and Developmental Disorders, 39(1), 188. https://doi.org/10.1007/s10803-008-0612-4.
Barbaro, J., & Dissanayake, C. (2009). Autism spectrum disorders in infancy and toddlerhood: A review of the evidence on early signs, early identification tools, and early diagnosis. Journal of Developmental & Behavioral Pediatrics, 30(5), 447–459. https://doi.org/10.1097/DBP.0b013e3181ba0f9f.
Barbaro, J., & Dissanayake, C. (2010). Prospective identification of autism spectrum disorders in infancy and toddlerhood using developmental surveillance: The Social Attention and Communication Study. Journal of Developmental & Behavioral Pediatrics, 31(5), 376–385. https://doi.org/10.1097/DBP.0b013e3181df7f3c.
Barbaro, J., & Dissanayake, C. (2013). Early markers of autism spectrum disorders in infants and toddlers prospectively identified in the Social Attention and Communication Study. Autism, 17(1), 64–86. https://doi.org/10.1177/1362361312442597.
Barbaro, J., & Dissanayake, C. (2016). Diagnostic stability of autism spectrum disorder in toddlers prospectively identified in a community-based setting: Behavioural characteristics and predictors of change over time. Autism. https://doi.org/10.1177/1362361316654084.
Barbaro, J., Ridgway, L., & Dissanayake, C. (2011). Developmental surveillance of infants and toddlers by maternal and child health nurses in an Australian community-based setting: Promoting the early identification of autism spectrum disorders. Journal of Pediatric Nursing, 26(4), 334–347. https://doi.org/10.1016/j.pedn.2010.04.007.
Baxter, A. J., Brugha, T. S., Erskine, H. E., Scheurer, R. W., Vos, T., & Scott, J. G. (2015). The epidemiology and global burden of autism spectrum disorders. Psychological Medicine, 45(3), 601–613. https://doi.org/10.1017/S003329171400172X.
Begeer, S., Mandell, D., Wijnker-Holmes, B., Venderbosch, S., Rem, D., Stekelenburg, F., et al. (2013). Sex differences in the timing of identification among children and adults with autism spectrum disorders. Journal of Autism and Developmental Disorders, 43(5), 1151–1156. https://doi.org/10.1007/s10803-012-1656-z.
Bryson, S. E., & Smith, I. M. (1998). Epidemiology of autism: Prevalence, associated characteristics, and implications for research and service delivery. Mental Retardation and Developmental Disabilities Research Reviews, 4(2), 97–103.
Campbell, D. B., Sutcliffe, J. S., Ebert, P. J., Militerni, R., Bravaccio, C., Trillo, S., et al. (2006). A genetic variant that disrupts MET transcription is associated with autism. Proceedings of the National Academy of Sciences, 103(45), 16834–16839, https://doi.org/10.1073/pnas.0605296103.
Carter, A. S., Black, D. O., Tewani, S., Connolly, C. E., Kadlec, M. B., & Tager-Flusberg, H. (2007). Sex differences in toddlers with autism spectrum disorders. Journal of Autism and Developmental Disorders, 37(1), 86–97. https://doi.org/10.1007/s10803-006-0331-7.
Charman, T., Taylor, E., Drew, A., Cockerill, H., Brown, J.-A., & Baird, G. (2005). Outcome at 7 years of children diagnosed with autism at age 2: Predictive validity of assessments conducted at 2 and 3 years of age and pattern of symptom change over time. Journal of Child Psychology and Psychiatry, 46(5), 500–513. https://doi.org/10.1111/j.1469-7610.2004.00377.x.
Chawarska, K., Macari, S., Powell, K., DiNicola, L., & Shic, F. (2016). Enhanced social attention in female infant siblings at risk for autism. Journal of the American Academy of Child & Adolescent Psychiatry, 55(3), 188–195. https://doi.org/10.1016/j.jaac.2015.11.016.
Christian, S. L., Brune, C. W., Sudi, J., Kumar, R. A., Liu, S., Karamohamed, S., et al. (2008). Novel submicroscopic chromosomal abnormalities detected in autism spectrum disorder. Biological Psychiatry, 63(12), 1111–1117. https://doi.org/10.1016/j.biopsych.2008.01.009.
Clark, M. L. E., Barbaro, J., & Dissanayake, C. (2017). Continuity and change in cognition and autism severity from toddlerhood to school age. Journal of Autism and Developmental Disorders, 47(2), 328–339. https://doi.org/10.1007/s10803-016-2954-7.
Clifford, S. M., & Dissanayake, C. (2008). The early development of joint attention in infants with autistic disorder using home video observations and parental interview. Journal of Autism and Developmental Disorders, 38(5), 791–805. https://doi.org/10.1007/s10803-007-0444-7.
Diedenhofen, B., & Musch, J. (2015). cocor: A comprehensive solution for the statistical comparison of correlations. PLoS ONE, 10(4), e0121945. https://doi.org/10.1371/journal.pone.0121945.
Fombonne, E. (2005). Epidemiological studies of pervasive developmental disorders. In F. R. Volkmar, R. Paul, A. Klin & D. Cohen (Eds.), Handbook of autism and pervasive developmental disorders: Diagnosis, development, neurobiology, and behavior (Vol. 1, 3rd ed, pp. 42–69). Hoboken, NJ: Wiley.
Fombonne, E. (2009). Epidemiology of pervasive developmental disorders. Pediatric Research, 65(6), 591–598.
Gotham, K., Pickles, A., & Lord, C. (2009). Standardizing ADOS Scores for a measure of severity in autism spectrum disorders. Journal of Autism and Developmental Disorders, 39(5), 693–705. https://doi.org/10.1007/s10803-008-0674-3.
Gotham, K., Pickles, A., & Lord, C. (2012). Trajectories of autism severity in children using standardized ADOS Scores. Pediatrics, 130(5), e1278–e1284. https://doi.org/10.1542/peds.2011-3668.
Gotham, K., Risi, S., Pickles, A., & Lord, C. (2006). The autism diagnostic observation schedule: Revised algorithms for improved diagnostic validity. Journal of Autism and Developmental Disorders, 37(4), 613. https://doi.org/10.1007/s10803-006-0280-1.
Hartley, S. L., & Sikora, D. M. (2009). Sex differences in autism spectrum disorder: An examination of developmental functioning, autistic symptoms, and coexisting behavior problems in toddlers. Journal of Autism and Developmental Disorders, 39(12), 1715. https://doi.org/10.1007/s10803-009-0810-8.
Head, A. M., McGillivray, J. A., & Stokes, M. A. (2014). Gender differences in emotionality and sociability in children with autism spectrum disorders. Molecular Autism, 5(1), 19. https://doi.org/10.1186/2040-2392-5-19.
Hiller, R. M., Young, R. L., & Weber, N. (2014). Sex differences in autism spectrum disorder based on DSM-5 criteria: Evidence from clinician and teacher reporting. Journal of Abnormal Child Psychology, 42(8), 1381–1393. https://doi.org/10.1007/s10802-014-9881-x.
Hiller, R. M., Young, R. L., & Weber, N. (2016). Sex differences in pre-diagnosis concerns for children later diagnosed with autism spectrum disorder. Autism, 20(1), 75–84. https://doi.org/10.1177/1362361314568899.
Holtmann, M., Bölte, S., & Poustka, F. (2007). Autism spectrum disorders: Sex differences in autistic behaviour domains and coexisting psychopathology. Developmental Medicine & Child Neurology, 49(5), 361–366. https://doi.org/10.1111/j.1469-8749.2007.00361.x.
Hull, L., Mandy, W., & Petrides, K. (2016). Behavioural and cognitive sex/gender differences in autism spectrum condition and typically developing males and females. Autism. https://doi.org/10.1177/1362361316669087.
Hus, V., Gotham, K., & Lord, C. (2014). Standardizing ADOS domain scores: Separating severity of social affect and restricted and repetitive behaviors. Journal of Autism and Developmental Disorders, 44(10), 2400–2412. https://doi.org/10.1007/s10803-012-1719-1.
Itsara, A., Wu, H., Smith, J. D., Nickerson, D. A., Romieu, I., London, S. J., et al. (2010). De novo rates and selection of large copy number variation. Genome Research, 20(11), 1469–1481. https://doi.org/10.1101/gr.107680.110.
Kopp, S., & Gillberg, C. (1992). Girls with social deficits and learning problems: Autism, atypical Asperger syndrome or a variant of these conditions. European Child & Adolescent Psychiatry, 1(2), 89–99. https://doi.org/10.1007/bf02091791.
Lai, M.-C., Lombardo, M. V., Pasco, G., Ruigrok, A. N. V., Wheelwright, S. J., Sadek, S. A., et al. (2011). A Behavioral Comparison of Male and Female Adults with High Functioning Autism Spectrum Conditions. PLoS ONE, 6(6), e20835. https://doi.org/10.1371/journal.pone.0020835.
Landa, R., & Garrett-Mayer, E. (2006). Development in infants with autism spectrum disorders: A prospective study. Journal of Child Psychology and Psychiatry, 47(6), 629–638. https://doi.org/10.1111/j.1469-7610.2006.01531.x.
Lord, C., Luyster, R., Guthrie, W., & Pickles, A. (2012a). Patterns of developmental trajectories in toddlers with autism spectrum disorder. Journal of Consulting and Clinical Psychology, 80(3), 477–489. https://doi.org/10.1037/a0027214.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Leventhal, B. L., DiLavore, P. C., et al. (2000). The autism diagnostic observation schedule—generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30(3), 205–223. https://doi.org/10.1023/a:1005592401947.
Lord, C., Rutter, M., & Couteur, A. (1994a). Autism diagnostic interview-revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders. https://doi.org/10.1007/bf02172145.
Lord, C., Rutter, M., Dilavore, P., Risi, S., Gotham, K., & Bishop, S. (2012b). Autism diagnostic observation schedule. Torrance: Western Psychological Services.
Lord, C., Rutter, M., & Le Couteur, A. (1994b). Autism diagnostic interview-revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24(5), 659–685. https://doi.org/10.1007/bf02172145.
Lord, C., Schopler, E., & Revicki, D. (1982). Sex differences in autism. Journal of Autism and Developmental Disorders, 12(4), 317–330. https://doi.org/10.1007/bf01538320.
Lotter, V. (1966). Epidemiology of autistic conditions in young children. Social Psychiatry, 1(3), 124–135. https://doi.org/10.1007/bf00584048.
Mandy, W., Chilvers, R., Chowdhury, U., Salter, G., Seigal, A., & Skuse, D. (2012). Sex differences in autism spectrum disorder: Evidence from a large sample of children and adolescents. Journal of Autism and Developmental Disorders, 42(7), 1304–1313. https://doi.org/10.1007/s10803-011-1356-0.
Mandy, W., & Tchanturia, K. (2015). Do women with eating disorders who have social and flexibility difficulties really have autism? A case series. Molecular Autism, 6(1), 6. https://doi.org/10.1186/2040-2392-6-6.
McLennan, J. D., Lord, C., & Schopler, E. (1993). Sex differences in higher functioning people with autism. Journal of Autism and Developmental Disorders, 23(2), 217–227. https://doi.org/10.1007/bf01046216.
Mullen, E. M. (1995). Mullen scales of early learning. Circle Pines, MN: AGS.
Osterling, J. A., Dawson, G., & Munson, J. A. (2002). Early recognition of 1-year-old infants with autism spectrum disorder versus mental retardation. Development and Psychopathology, 14(2), 239–251. https://doi.org/10.1017/S0954579402002031.
Ozonoff, S., Iosif, A.-M., Baguio, F., Cook, I. C., Hill, M. M., Hutman, T., et al. (2010). A prospective study of the emergence of early behavioral signs of autism. Journal of the American Academy of Child & Adolescent Psychiatry, 49(3), 256–266. https://doi.org/10.1016/j.jaac.2009.11.009.
Postorino, V., Fatta, L. M., De Peppo, L., Giovagnoli, G., Armando, M., Vicari, S., et al. (2015). Longitudinal comparison between male and female preschool children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(7), 2046–2055. https://doi.org/10.1007/s10803-015-2366-0.
Reinhardt, V. P., Wetherby, A. M., Schatschneider, C., & Lord, C. (2015). Examination of sex differences in a large sample of young children with autism spectrum disorder and typical development. Journal of Autism and Developmental Disorders, 45(3), 697–706. https://doi.org/10.1007/s10803-014-2223-6.
Rivet, T. T., & Matson, J. L. (2011). Review of gender differences in core symptomatology in autism spectrum disorders. Research in Autism Spectrum Disorders, 5(3), 957–976. https://doi.org/10.1016/j.rasd.2010.12.003.
Rynkiewicz, A., Schuller, B., Marchi, E., Piana, S., Camurri, A., Lassalle, A., et al. (2016). An investigation of the ‘female camouflage effect’ in autism using a computerized ADOS-2 and a test of sex/gender differences. Molecular Autism, 7(1), 10. https://doi.org/10.1186/s13229-016-0073-0.
Sacrey, L.-A. R., Zwaigenbaum, L., Szatmari, P., Bryson, S., Georgiades, S., Brian, J., et al. (2017). Brief report: Characteristics of preschool children with ASD vary by ascertainment. Journal of Autism and Developmental Disorders, 47(5), 1542–1550. https://doi.org/10.1007/s10803-017-3062-z.
Sebat, J., Lakshmi, B., Malhotra, D., Troge, J., Lese-Martin, C., Walsh, T., et al. (2007). Strong association of de novo copy number mutations with autism. Science, 316(5823), 445–449. https://doi.org/10.1126/science.1138659.
Shumway, S., Farmer, C., Thurm, A., Joseph, L., Black, D., & Golden, C. (2012). The ADOS calibrated severity Score: Relationship to phenotypic variables and stability over time. Autism Research, 5(4), 267–276. https://doi.org/10.1002/aur.1238.
Sipes, M., Matson, J. L., Worley, J. A., & Kozlowski, A. M. (2011). Gender differences in symptoms of autism spectrum disorders in toddlers. Research in Autism Spectrum Disorders, 5(4), 1465–1470. https://doi.org/10.1016/j.rasd.2011.02.007.
Skuse, D. H., Mandy, W., Steer, C., Miller, L. L., Goodman, R., Lawrence, K., et al. (2009). Social communication competence and functional adaptation in a general population of children: Preliminary evidence for sex-by-verbal IQ differential risk. Journal of the American Academy of Child & Adolescent Psychiatry, 48(2), 128–137. https://doi.org/10.1097/CHI.0b013e31819176b8.
Solomon, M., Miller, M., Taylor, S. L., Hinshaw, S. P., & Carter, C. S. (2012). Autism symptoms and internalizing psychopathology in girls and boys with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(1), 48–59. https://doi.org/10.1007/s10803-011-1215-z.
Supekar, K., & Menon, V. (2015). Sex differences in structural organization of motor systems and their dissociable links with repetitive/restricted behaviors in children with autism. Molecular Autism, 6(1), 50. https://doi.org/10.1186/s13229-015-0042-z.
Sutherland, R., Hodge, A., Bruck, S., Costley, D., & Klieve, H. (2017). Parent-reported differences between school-aged girls and boys on the autism spectrum. Autism. https://doi.org/10.1177/1362361316668653.
Tsai, L. Y., & Beisler, J. M. (1983). The development of sex differences in infantile autism. The British Journal of Psychiatry, 142(4), 373–378. https://doi.org/10.1192/bjp.142.4.373.
Van Wijngaarden-Cremers, P. J. M., van Eeten, E., Groen, W. B., Van Deurzen, P. A., Oosterling, I. J., & Van der Gaag, R. J. (2014). Gender and age differences in the core triad of impairments in autism spectrum disorders: A systematic review and meta-analysis. Journal of Autism and Developmental Disorders, 44(3), 627–635. https://doi.org/10.1007/s10803-013-1913-9.
Vivanti, G., Barbaro, J., Hudry, K., Dissanayake, C., & Prior, M. (2013). Intellectual development in autism spectrum disorders: New insights from longitudinal studies. Frontiers in Human Neuroscience, 7, 354.
Vivanti, G., & Dissanayake, C. (2016). Outcome for children receiving the early start denver model before and after 48 months. Journal of Autism and Developmental Disorders, 46(7), 2441–2449. https://doi.org/10.1007/s10803-016-2777-6.
Vivanti, G., Paynter, J., Duncan, E., Fothergill, H., Dissanayake, C., & Rogers, S. J. (2014). Effectiveness and feasibility of the early start denver model implemented in a group-based community childcare setting. Journal of Autism and Developmental Disorders, 44(12), 3140–3153. https://doi.org/10.1007/s10803-014-2168-9.
Volkmar, F. R., Szatmari, P., & Sparrow, S. S. (1993). Sex differences in pervasive developmental disorders. Journal of Autism and Developmental Disorders, 23(4), 579–591. https://doi.org/10.1007/bf01046103.
Westman-Andersson, G., Gillberg, C., & Miniscalco, C. (2013). Pre-school children with suspected autism spectrum disorders: Do girls and boys have the same profiles? Research in Developmental Disabilities, 34(1), 413–422. https://doi.org/10.1016/j.ridd.2012.08.025.
Wing, L. (1981). Sex ratios in early childhood autism and related conditions. Psychiatry Research, 5(2), 129–137. https://doi.org/10.1016/0165-1781(81)90043-3.
Young, R. L., Brewer, N., & Pattison, C. (2003). Parental identification of early behavioural abnormalities in children with autistic disorder. Autism, 7(2), 125–143. https://doi.org/10.1177/1362361303007002002. doi.
Zwaigenbaum, L., Bryson, S. E., Szatmari, P., Brian, J., Smith, I. M., Roberts, W., et al. (2012). Sex differences in children with autism spectrum disorder identified within a high-risk infant cohort. Journal of Autism and Developmental Disorders, 42(12), 2585–2596. https://doi.org/10.1007/s10803-012-1515-y.
Acknowledgments
The authors would like to acknowledge the Research Focus Area Understanding Disease at La Trobe University for providing a Write-up Award that facilitated the preparation of this manuscript. LPL is funded by the Cooperative Research Centre for Living with Autism (Autism CRC). The authors are also extremely grateful to all the study participants and their families for contributing to the project.
Author information
Authors and Affiliations
Contributions
RJ, JB, and CD conceived and designed the study. JB and LPL assisted in the data collection. LPL obtained funding to facilitate the preparation of the manuscript, conducted the data analyses, and drafted the manuscript. RJ, JB, and CD critically revised the manuscript and provided feedback. All authors read and approved the final manuscript.
Corresponding author
Rights and permissions
About this article

Cite this article
Lawson, L.P., Joshi, R., Barbaro, J. et al. Gender Differences During Toddlerhood in Autism Spectrum Disorder: A Prospective Community-Based Longitudinal Follow-Up Study. J Autism Dev Disord 48, 2619–2628 (2018). https://doi.org/10.1007/s10803-018-3516-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-018-3516-y