
Abstract
Despite consistent and substantive research documenting a large male to female ratio in Autism Spectrum Disorder (ASD), only a modest body of research exists examining sex differences in characteristics. This study examined sex differences in developmental functioning and early social communication in children with ASD as compared to children with typical development. Sex differences in adaptive behavior and autism symptoms were also examined in children with ASD. Participants (n = 511) were recruited from the Florida State University FIRST WORDS® Project and University of Michigan Autism and Communication Disorders Center. Analyses did not reveal significant effects of sex or a diagnostic group by sex interaction, suggesting a similar phenotype in males and females early in development. Further research is needed to examine sex differences across development.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is characterized by social communication impairments and the presence of fixated interests and repetitive behaviors (American Psychiatric Association 2013; Volkmar et al. 2005). ASD affects approximately 1 in 68 children in the United States and is diagnosed more frequently in males (1 in 42) than females (1 in 189; CDC 2014). Children are receiving diagnoses of ASD and entering intervention at increasingly earlier ages—a trend influenced by theories from developmental neuroscience, based on the hypothesis that neuroplasticity allows interventions to have a greater impact when delivered during infancy and early childhood than at later ages (Dawson 2008; Yirmiya and Ozonoff 2007). Clinical practice guidelines of the American Academy of Pediatrics recommend that all children be screened for ASD at 18 and 24 months of age (Johnson et al. 2007), which has contributed to an emphasis on early diagnosis. Additionally, the recent development of diagnostic tools attuned to the presentation of ASD in toddlers (Luyster et al. 2009; Robins et al. 2001) has allowed for the provision of more stable diagnoses at younger ages (Chawarska et al. 2009; Lord et al. 2012). Despite consistent sex differences in rate of diagnosis (CDC 2012), little research examining sex differences in early diagnostic features of ASD is available. Research examining sex differences in the presentation of ASD in toddlers is important to inform screening and diagnosis and to improve access to early intervention.
Most research focusing on sex differences have concentrated on reporting the large male-to-female ratio in rates of the disorder. Wing and Gould (1979) examined the prevalence of autism in children with special needs and found that males were 15 times more likely than females to carry a diagnosis of ASD. Prevalence studies have also documented differences presently and historically in age of diagnosis, with ASD frequently diagnosed later in females (Kopp and Gillberg 1992; Giarelli et al. 2010). An epidemiological study found that both less and more able females were diagnosed later than males, and more able females were diagnosed significantly later than both less able females and more able males (Shattuck et al. 2009). This high male-to-female ratio may reflect a true difference in prevalence or it may suggest that females with ASD are under-diagnosed (Koenig and Tsatsanis 2005). Since the DSM-IV-TR diagnostic criteria were developed and tested with an overwhelmingly male sample (Volkmar et al. 1994), it is possible that the diagnostic criteria used in previous investigations of sex differences is not sensitive to posited sex differences in the manifestation and presentation of ASD. Kim et al. (2011) conducted a large-scale prevalence study screening all 7–12-year-old children for ASD in a South Korean community. The study found a 5.1:1 male to female ratio in the high-risk group (children receiving special education services or children with an identified disability) and a much lower 2.5:1 ratio in the general population. This study is unique in that the research team screened all eight-year-old children in the population, likely allowing for the identification of ASD cases in females with less severe symptoms who may not have been referred for evaluation. On the other hand, the presence or extent of impairment was not documented in these ASD cases making it difficult to interpret these findings (Lord 2011).
The earliest studies of sex differences in children with ASD documented much higher rates of severe cognitive and developmental delays in females than males (Lord et al. 1982), although IQ distributions and the magnitude of differences have varied between studies. A review of medical records for a population cohort of 8-year-old children born in 1992 and 1994 found that females were more likely to have an intelligence quotient (IQ) below 70 (72.7 vs. 56.4 %) and that the sex ratio varied significantly between IQ levels. At very low levels of IQ (IQ < 34), the sex ratio was 1:1 (Male: Female) and in the range of intellectual disability (ID; IQ < 70), the ratio was 2.4:1 (Nicholas et al. 2008). However, at the highest level of functioning the sex ratio was much greater (4.9:1). It is important to note that this sample had a higher proportion of less able children than most epidemiological studies with the majority of the sample (60.4 %) within the range of ID (<70). Little consensus exists on the prevalence of ID in children with ASD, and epidemiological studies have yielded conflicting estimates of 25 % (Chakrabarti and Fombonne 2001), 55 % (Baird et al. 2006), 44.6 % (ADDM 2007), and 38 % (CDC 2012) of children with ASD and concurrent ID. The results of epidemiological studies over time suggest that more children without ID are being diagnosed with ASD.
Results of recent studies documenting sex differences in intellectual functioning contrast with previous studies of older cohorts. Carter et al. (2007) examined sex differences in developmental functioning in a sample of toddlers with ASD (n = 22 females) between 18 and 33 months. They reported significantly higher nonverbal cognitive scores (Mullen Scales of Early Learning Visual Reception) in the female group after controlling for language level but lower overall language and motor scores. Another study examining toddlers between 18 and 47 months (n = 42 females) did not reveal significant sex differences in verbal or nonverbal developmental functioning using the Mullen Scales of Early Learning (MSEL; Mullen 1995; Hartley and Sikora 2009). It is surprising that the Carter et al. and Hartley and Sikora studies yielded disparate results given the similar ages and measures used within both studies, suggesting that further research examining sex differences using younger samples is necessary. Zwaigenbaum et al. (2012) examined sex differences in a sample of 3-year-old, high-risk younger siblings of children with ASD with and without documented ASD diagnoses and low-risk controls. This study found that females in all three groups showed more developed socialization and daily living skills as measured by the Vineland Adaptive Behavior Scales (VABS; Sparrow et al. 2004) and higher fine motor scores as measured by the MSEL but did not find significant differences in language functioning or visual reception scores.
Similar to the results of recent studies examining developmental functioning, current studies examining sex differences in ASD symptoms have yielded conflicting findings. Some studies have found that females show fewer repetitive behaviors (Nicholas et al. 2008; Hartley and Sikora 2009) and fewer social communication symptoms (Zwaigenbaum et al. 2012) while other studies have failed to find significant differences in diagnostic features (Carter et al. 2007; Holtman et al. 2007). Using review of medical records, Nicholas et al. (2008) examined ASD symptoms in a population cohort of 8-year-old children with ASD and found that females were less likely to present with preoccupation with parts of objects and repetitive routines and rituals. Comparing males and females within a mixed sample of young children at high and low risk for ASD, Zwaigenbaum et al. found that females evidenced slightly fewer symptoms of ASD using the Autism Diagnostic Observation Scale (ADOS; Lord et al. 1999) Calibrated Severity Scores (Gotham et al. 2009) as well as fewer social and communication symptoms on the Autism Diagnostic Interview-Revised (ADI-R; Lord et al. 1994).
There is some evidence from the existing literature that the detection of sex differences in developmental functioning and diagnostic features is affected by sample characteristics and the manner in which ASD symptomatology is measured and analyzed. A larger number of studies have documented sex differences using the ADI-R, a semi-structured parent interview as compared to the ADOS, a structured clinical observation. This difference is apparent particularly with respect to repetitive behaviors. In contrast to the ADOS, the ADI-R has a greater number of items measuring both social communication and repetitive behavior features, which may make it more sensitive to detect sex differences. However, it is also possible that the differences detected by studies using the ADI-R and other parent report measures are influenced by a bias that results from parents reporting on the atypicality of their child’s behavior in comparison to typically-developing same sex peers. In fact, one study demonstrated that although males and females with ASD did not differ with regard to social communication and restricted and repetitive behaviors as measured by the ADOS, parents of females with ASD reported much lower levels of social competence (Carter et al. 2007). Using a sample of older children, Holtman et al. (2007) also found that while females did not differ significantly from males with ASD on core ASD symptoms, parents reported significantly more behavioral and emotional difficulties in females with ASD.
The research literature that has examined the development of communication and language in typically developing infants and toddlers may inform investigations of sex differences in children with ASD. Small differences have been documented favoring females in a number of early communication domains including the development of nonverbal communication (Clarke-Stewart 1973; Fenson et al. 1994), vocabulary acquisition (Fenson et al. 1994; Huttenlocher et al. 1991), frequency of social initiations (Klein and Durfee 1978), and a lower likelihood of early language delay (Dale et al. 2003). Fenson et al. (1994) examined the development of early communication with a large sample of typically developing infants and toddlers and documented small yet significant differences, favoring females in the rate of gestural development and receptive and expressive vocabulary between 8 and 18 months of age. Interestingly, Fenson et al. found a stronger role of sex on gesture production for two subscales measuring gestures acquired through observational learning with a great deal of cultural content—‘pretending to be a parent’ for females and ‘imitating adult actions’ for males. Females also combined words earlier than males and produced longer and more complex utterances at earlier ages (Fenson et al. 1994). However, it is particularly important to note that all of the sex differences found in this study were small, accounting for approximately 1–2 % of the variance.
In addition, early social experiences with caregivers have been found to facilitate the acquisition of skills needed for language learning, including joint attention, imitation, and gesture development (Akhtar and Tomasello 2000; Snow 1989) in children with typical development, and the research literature suggests that adults interact with infant males and females differently (Stern and Karraker 1989). It is theorized that parents’ differential socialization strategies used with males and females provide an environment more supportive of social communication development for females (Bussey and Bandura 1999; Huttenlocher et al. 1991; Leaper et al. 1998; Malatesta and Haviland 1982), possibly contributing to observed differences between sexes in typical development and serving as a protective factor against social communication difficulties.
While subtle differences favoring females have been observed in the development of early communication and language in typically developing children, studies examining sex differences in ASD populations have rarely included typically developing comparison groups. Research examining how the early social communication skills of males and females diagnosed with ASD differ from typically developing males and females may provide important implications for early identification (Koenig and Tsatsanis 2005). The present study examined sex differences in early social communication and developmental functioning in children with ASD and typical development (TD) and adaptive behavior and autism symptoms in children with ASD. In contrast to previous studies, the present study used a larger, well-characterized community based sample of young children who completed a communication evaluation early in development and a follow-up diagnostic or developmental evaluation approximately 1 year later.
Based on studies suggesting differential socialization practices within typically developing children, it was predicted that on measures of early social communication, females with ASD would demonstrate more developed symbolic communication skills than males with ASD on the CSBS. Consistent with literature documenting sex differences in the early development of typically developing children, it was hypothesized that both females with ASD and TD would exhibit slightly higher verbal skills and lower nonverbal skills than their male counterparts on the MSEL. Finally, based on existing literature (Nicholas et al. 2008; Hartley and Sikora 2009; Zwaigenbaum et al. 2012) it was hypothesized that the females with ASD would demonstrate fewer restricted and repetitive behaviors on the ADOS and comparable social communication features.
Methods
Participants
Participant Recruitment
All children included in the current study were recruited from the FIRST WORDS® Project (Wetherby et al. 2008) at the Florida State University Autism Institute (FSUAI) and the University of Michigan Autism and Communication Disorders Center (UMACC). Participants were recruited from community screening in pediatrician offices, younger siblings of children with ASD, and children who were referred to the project because of concerns about development or suspected autism. Children recruited from the general pediatric sample (n = 14,334; 48 % female) were screened using the CSBS Infant-Toddler Checklist (Wetherby and Prizant 2002). Of these children, 2,579 (39 % female) completed an early communication evaluation that consisted of the CSBS Behavior Sample before 24 months of age. Children who showed red flags for ASD during the communication evaluation were invited to participate in an additional diagnostic evaluation. Children who did not show red flags for ASD also completed an additional evaluation at approximately 24–36 months of age that consisted of the MSEL.
Parents of all participants provided written informed consent prior to any testing and the study was approved by the Florida State University Institutional Review Board and the University of Michigan Institutional Review Board. A detailed description of inclusion criteria for the FIRST WORDS® Project can be found in Wetherby et al. (2008).
ASD Group
To determine diagnostic status, all children who completed a communication evaluation and displayed red flags of ASD were invited to participate in a diagnostic evaluation (M = 28.09 months, SD = 12.30) that examined the child’s autism symptoms with the Autism Diagnostic Observation Schedule (ADOS; Lord et al. 1999), developmental functioning with the Mullen Scales of Early Learning (MSEL; Mullen 1995), and adaptive behavior with the Vineland Adaptive Behavior Scales (VABS; Sparrow et al. 2004). Information gathered from parent report, clinician observation, and standardized measures were used to formulate a best-estimate clinical diagnosis. Children who received a best-estimate diagnosis of ASD and evidenced a nonverbal developmental level of at least 12 months as measured by the MSEL were included in the ASD group. For children who completed multiple diagnostic batteries, the battery closest to 36 months of age was selected for data analysis. The final ASD sample consisted of 288 participants (54 female) who received best-estimate diagnoses of ASD. Table 1 presents information on the demographic and ethnic composition of the sample.
TD Group
Children were included in the TD group if they did not show red flags of ASD, did not have delayed development based on the CSBS and MSEL, were judged to be typically developing by an experienced clinician and if caregivers did not express concerns about the child’s development. During recruitment of children in the TD group, an effort was made to recruit males and females in similar proportions to the ASD group; therefore, males with TD were oversampled, yielding a sample of 59 females and 164 males. Additionally, an ADOS was completed on 30 % (n = 65) of the TD group and all scored below the algorithm cutoff for ASD (Social Affect + Restricted Repetitive Behavior M = 3.94, SD = 2.85).
Measures
Communication and Symbolic Behavior Scales Developmental Profile
The CSBS is a standardized tool for the assessment of early social communication abilities. The CSBS Behavior Sample consists of a standardized set of procedures and activities administered by a trained examiner that are designed to encourage spontaneous communicative behavior from very young children up to 24 months of age. The Behavior Sample includes a series of communicative temptations, books, and play activities to entice spontaneous communication and symbolic play and probes to examine response to joint attention and understanding of words. It consists of six distinct activities; social communication skills are scored throughout the observation. The Behavior Sample is recorded and scored from video by a trained clinician. The CSBS Behavior Sample yields 20 items that form 3 composite scores (Social, Speech, and Symbolic) and 7 cluster scores (Emotion and Eye Gaze, Communication, Gestures, Sounds, Words, Understanding and Object Use). The Behavior Sample has been found to have high internal consistency (α coefficients ranging from .86 to .92), good inter-rater and test–retest reliability, and support for construct, concurrent, and predictive validity (Wetherby et al. 2002; Wetherby and Prizant 2002). Inter-rater reliability for the Behavior Sample was calculated using generalizability (g) coefficients for pairs of seven independent raters on randomly selected videotapes for at least 10 % of the samples scored by each rater. All g coefficients were over .60, which is considered acceptable for demonstrating inter-rater reliability (Mitchell, 1979) with an average of .88 for the items, .92 for the composites, and .96 for the total, indicating high inter-rater reliability.
Mullen Scales of Early Learning
The MSEL is a measure of cognitive functioning used in infants and children up to 66 months of age. The MSEL consists of four cognitive scales yielding T scores for each: Visual Reception, Fine Motor, Receptive Language, and Expressive Language. Ratio developmental quotients (DQ) were calculated based on age equivalent scores divided by chronological age for Visual Reception and Fine Motor to reflect children’s nonverbal DQ (NVDQ) and Receptive and Expressive Language to reflect verbal DQ (VDQ).
Vineland Adaptive Behavior Scales, Second Edition
The VABS is a standardized parent interview used to assess adaptive behavior in four domains: Communication, Daily Living Skills, Socialization, and Motor Skills.
Autism Diagnostic Observation Schedule
Modules 1, 2, 3 or the Toddler Module (ADOS-T; Luyster et al. 2009) of the ADOS were completed by a trained experimenter and used to confirm participant’s diagnosis at the follow-up diagnostic evaluation. Social affect and restricted and repetitive behavior totals were calculated using the revised algorithms for Modules 1, 2 and 3 (Gotham et al. 2007). The ADOS is a semi-structured, standardized assessment that has been found to have good reliability and high sensitivity and specificity in identifying characteristics of ASD (Lord et al. 2000; Gotham et al. 2007; Luyster et al. 2009).
Results
Preliminary Data and Power Analysis
Prior to analyses, data were screened for skewness, kurtosis, and the presence of univariate and multivariate outliers. Scatterplots for each pair of variables were examined separately for each group to identify non-linear relationships and did not reveal any obvious evidence of non-linearity. A power analysis was conducted using the GPower computer program (Faul et al. 2009). Specifying 0.8 power, the available sample size and a 2 × 2 ANOVA analysis including main effects and interactions, analyses estimated a minimally detectable effect size of Hedge’s g = 0.27 which indicates that this study had sufficient power to detect educationally meaningful effects (Rosenthal 1991). In order to maximize the probability of detecting any existing differences, no corrections for the number of analyses conducted were used.
Site Differences
A series of independent sample t-tests was conducted to examine sample differences between TD and ASD participants at FSU and UMACC on the ADOS algorithm totals, CSBS cluster scores, and MSEL and VABS subscales. Within participants with ASD, analyses revealed significant differences with regard to the CSBS Object Use cluster t (286) = −4.09, p < 0.001, indicating that ASD participants from FSU had significantly higher object use scores (Cohen’s d = 0.69). Additionally, ASD participants from FSU demonstrated significantly higher motor scores on the VABS, t (223) = −1.66, p = 0.047, Cohen’s d = 0.42. No significant differences were detected between TD participants recruited from FSU and UMACC.
Early Social Communication Skills
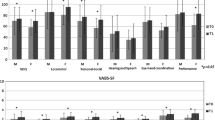
To examine sex differences in early communication skills, seven 2 × 2 ANOVAs were conducted using Welch corrections for violations of the assumption of homogeneity of variance. Specifically, males and females with TD and ASD were compared on CSBS Behavior Sample cluster scores (see Table 2). Analyses revealed significant differences between children with ASD and TD on all seven cluster scores with children with TD demonstrating significantly higher scores (see Table 3). Analyses revealed a significant difference between males and females on the CSBS Words Cluster, F (1,168.72) = 4.68, p < 0.05, as well as a significant diagnostic status × sex interaction, F (1,168.72) = 5.20, p < 0.05. Welch-corrected contrasts using Tukey HSD to control for type I error revealed significant differences between males and females in the TD group with females achieving significantly higher scores on the CSBS Words Cluster, F(1,92.25) = 7.82, p < 0.05. Males and females in the ASD group were not significantly different with regard to the CSBS Words Cluster score, F (1, 84.61) = 0.01, p = 0.92.
Developmental Level
Before conducting six 2 × 2 (Diagnostic Status × Gender) ANOVAs on the developmental level variables, we first inspected the groups to see if they met the assumption of homogeneity of variance. Results of Levene’s Test of Equality of Variances indicated significant violation of the homogeneity of variance assumption (all p < 0.05) for all six measures. To address this, the 2 × 2 ANOVAs and any potential contrasts were modeled using Welch corrections. Specifically, males and females with TD and ASD were compared on MSEL T-Scores as well as NVDQ and VDQ. Descriptive statistics for each MSEL subscale, NVDQ, and VDQ are presented in Table 4.
Analyses revealed significant main effects of diagnostic group. As expected, follow-up analyses revealed that children with ASD demonstrated significantly lower scores than children in the TD group on all subscales of the MSEL as well as NVDQ and VDQ (see Table 5). Analyses did not reveal a significant effect of sex or a significant diagnostic group × sex interaction. For these and all subsequent analyses, Hedges g was calculated to quantify the magnitude of differences using pooled variance to account for unequal sample sizes, noting that in the two-group case for the main effects, Cohen’s d and Hedges’ g are equivalent (see Table 5). Comparing by sex within the ASD group, small effect sizes were observed for all of the MSEL subscales. Hedge’s g calculations documented small to negligible effect sizes for diagnostic group × sex interactions (see Table 5). Follow-up contrasts were conducted to examine differences in specific areas of developmental functioning using Tukey HSD to control for Type I error due to multiple comparisons and Welch corrections to address violated homogeneity of variance. Analyses revealed that females in the TD group demonstrated significantly higher Receptive Language T-Scores than males, F (1,104.41) = 12.74, p < 0.05, and the magnitude of this difference was medium (Hedges’ g = 0.54). Comparing by sex within the TD group, small effect sizes were observed for Visual Reception, Fine Motor, and Expressive Language subscales as well as NVDQ and VDQ (Cohen’s d ≤ 0.3) with females evidencing higher scores.
Adaptive Behavior
To examine sex differences in adaptive behavior, a series of one-way ANOVA analyses were conducted. Specifically, males and females with ASD were compared on the four subscales of the VABS (Communication, Socialization, Daily Living, and Motor Skills) and the VABS Composite. Analyses did not reveal a significant difference between males and females with ASD in any areas of adaptive functioning. The magnitude of the differences in means for males and females on VABS subscales as measured by Hedge’s g were trivial (<0.10).
Autism Symptoms
As expected, the ADOS total score was correlated with MSEL NVDQ (r = −0.51, p < 0.001), and therefore NVDQ was included in the model as a covariate. To examine sex differences on a measure of autism symptoms, two one-way ANCOVA analyses were conducted. Males and females with ASD were compared on the ADOS domain scores (Social Affect and Restricted and Repetitive Behaviors; see Table 6). Analyses did not reveal significant sex differences, and effect sizes were negligible to small (see Table 6).
Discussion
The present study examined sex differences in early social communication skills developmental functioning, adaptive behavior and autism symptoms, using a large sample of young children with ASD and TD. Post-hoc power analyses indicated that the current study had sufficient power to detect meaningful effects. As expected, the TD group showed better early communication skills as well as higher overall developmental functioning when compared to the ASD group. Analysis of the TD group revealed that females with TD showed significantly better receptive language skills on the MSEL and use of words for communication on the CSBS when compared to males with TD. However, males and females with ASD in this sample evidenced no significant differences on measures of developmental functioning and early social communication skills.
Within our sample, TD females evidenced more developed skills in the ability to use words to communicate as well as better receptive language abilities. These findings are consistent with existing literature that documents a slight female advantage in the development of early language and communication (Fenson et al. 1994; Galsworthy et al. 2000). In contrast to the TD group, significant sex differences in communication skills were not observed within the ASD group. Although both the ASD and TD groups completed the CSBS and MSEL at similar chronological ages, the ASD group evidenced significantly lower levels of nonverbal and verbal development. It is possible that sex differences in language and communication would be more apparent as children with ASD acquire more language skills. It is also possible that we may have missed some more able children during screening, although it is important to note that in this ASD sample, 67 % achieved nonverbal developmental quotients above 70 which is comparable to rate documented in a recent CDC prevalance study (62 %; CDC, 2012).
This study did not find any significant differences between males and females in the ASD group on measures of adaptive functioning and autism symptoms, contributing to the seemingly disparate research findings on sex differences in individuals with ASD. This study has several unique attributes that contribute to the growing body of literature examining sex differences in ASD including the use of a relatively large sample of children with ASD, a sizeable typically developing comparison group, and well-established measures of early social communication skills, autism symptoms, and developmental functioning.
The lack of demonstrated sex differences in the present study may be due to limitations that should be acknowledged. This study included 511 children (288 of whom were diagnosed with ASD), but only 54 females with ASD were included. It is possible that the lack of sex differences found in this study and other studies of young children may be explained by ASD unfolding more slowly in females than males or parents and clinicians being less likely to express concern about more able females (Giarelli et al. 2010; Shattuck et al. 2009), although the average developmental level within this sample was comparable to other studies of older children with ASD. While all children included in the TD group were assessed by an experienced clinician, only 30 % of the TD group completed a comprehensive autism diagnostic evaluation. A wide range of developmental functioning was documented in our ASD sample, which is frequently observed in ASD research but may have affected our ability to detect differences in ASD symptoms and early social communication skills. Examination of sex differences in these areas in a larger, more homogeneous sub-sample of children with ASD may reveal different results.
Additionally, this study measured autism symptomatology using the ADOS, a direct observation measure. The ADOS was developed primarily as a diagnostic tool rather than a metric of symptom severity, and it may have limitations in documenting sex differences in characteristics. ADOS algorithms include the items that are most informative in a diagnostic context but may not provide an adequate sample of ASD features, or alternatively, it may be that ADOS algorithm items are not sensitive to sex differences in ASD symptoms. The combination of direct clinical observation and parent report has been demonstrated to yield a more accurate representation of a child’s ASD phenotype (Kim and Lord 2012; Risi et al. 2006). It is possible that our conclusions regarding sex differences in autism symptoms are limited due to the method in which autism symptoms were assessed; although research suggests that parent report measures of social-communication functioning may be biased by parent’s perceptions of their child’s behavior in comparison to typically developing same sex peers (Carter et al. 2007; Holtman et al. 2007).
In conclusion, no sex differences were found in early social communication skills, verbal and nonverbal developmental level, adaptive skills, and autism symptoms in our sample of preschool children diagnosed with ASD. This study provides several directions for future research. For example, it is possible that sex differences in children with ASD are more apparent as children age and research that systematically examines the ASD phenotype in males and females across age and developmental level is necessary.
References
Akhtar, N., & Tomasello, M. (2000). The social nature of words and word learning. In R. Golinkoff & K. Hirsh-Pasek (Eds.), Becoming a word learner: A debate on lexical acquisition. Oxford: Oxford University Press.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (Vol. 5). Washington, DC: American Psychiatric Association.
Baird, G., Simonoff, E., Pickles, A., Chandler, S., Loucas, T., Meldrum, D., et al. (2006). Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: The Special Needs and Autism Project (SNAP). The Lancet, 368(9531), 210–215.
Bussey, K., & Bandura, A. (1999). Social cognitive theory of gender development and differentiation. Psychological Review, 106(4), 676–713.
Carter, A. S., Black, D., Tewani, S., Connolly, C., Kadlec, M. B., & Tager-Flusberg, H. (2007). Sex differences in toddlers with autism spectrum disorders. Journal of Autism and Developmental Disorders,. doi:10.1007/s10803-006-0331-7.
Centers for Disease Control and Prevention. (2014). Prevalence of autism spectrum disorder—Autism and developmental disability monitoring network, 11 sites, United States, 2010. In Surveillance Summary (pp. 1–21). 28, March, 2014. Morbidity and Mortality Weekly Report, 63.
Chakrabarti, S., & Fombonne, E. (2001). Pervasive developmental disorders in preschool children. Journal of the American Medical Association, 285, 3093–3099.
Chawarska, K., Klin, A., Paul, R., Macari, S., & Volkmar, F. (2009). A prospective study of toddlers with ASD: Short-term diagnostic and cognitive outcomes. Journal of Child Psychology and Psychiatry, 50, 1235–1245.
Clarke-Stewart, K. A. (1973). Interactions between mothers and their young children: Characteristics and consequences. Monographs of the Society for Research in Child Development, 38 (6–7, Serial No. 153).
Dale, P. S., Price, T. S., Bishop, D. V. M., & Plomin, R. (2003). Outcomes of early language delay: I. Predicting persistent and transient language difficulties at 3 and 4 years. Journal of Speech, Language, and Hearing Research, 46(3), 544–560.
Dawson, G. (2008). Early behavioral intervention, brain plasticity, and the prevention of autism spectrum disorder. Development and Psychopathology, 20, 775–803.
Faul, F., Erdfelder, E., Buchner, A., & Lang, A. G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41, 1149–1160.
Fenson, L., Dale, P. S., Reznick, J. S., Bates, E., Thal, D. J., & Pethick, S. J. (1994). Variability in early communicative development. Monographs of the Society for Research in Child Development, 59 (1, Serial No. 242).
Galsworthy, M. J., Dionne, G., Dale, P. S., & Plomin, R. (2000). Sex differences in early verbal and non-verbal cognitive development. Developmental Science, 3, 206–215.
Giarelli, E., Wiggins, L. D., Rice, C. E., Levy, S. E., Kirby, R. S., Pinto-Martin, J., et al. (2010). Sex differences in the evaluation and diagnosis of autism spectrum disorders among children. Disability and Health Journal, 3(2), 107–116.
Gotham, K., Pickles, A., & Lord, C. (2009). Standardizing ADOS scores for a measure of severity in autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 693–705.
Gotham, K., Risi, S., Pickles, A., & Lord, C. (2007). The Autism diagnostic observation schedule: Revised algorithms for improved diagnostic validity. Journal of Autism and Developmental Disorders, 37, 613–627.
Hartley, S. L., & Sikora, D. S. (2009). Sex differences in autism spectrum disorders: An examination of developmental functioning, autism symptoms and coexisting behavior problems in toddlers. Journal of Autism and Developmental Disorders, 39, 1715–1722.
Holtman, M., Bolte, S., & Poustka, F. (2007). Autism spectrum disorders: Sex differences in autistic behaviour domains and coexisting psychopathology. Developmental Medicine and Child Neurology, 49, 361–366.
Huttenlocher, J., Haight, W., Bryk, A., Seltzer, M., & Lyons, T. (1991). Early vocabulary growth: Relation to language input and gender. Developmental Psychology, 27, 236–248.
Johnson, C. P., Myers, S. M., & The Council on Children with Disabilities. (2007). Identification and evaluation of children with autism spectrum disorders. Pediatrics, 120(4), 1183–1215.
Kim, Y. S., Leventhal, B. L., Koh, Y. J., Fombonne, E., Laska, E., Lim, E. C., et al. (2011). Prevalence of autism spectrum disorders in a total population sample. [published online May 9, 2011]. American Journal of Psychiatry. doi:10.1176/appi.ajp.2011.10101532.
Kim, S. H., & Lord, C. (2012). Combining information from multiple sources for the diagnosis of autism spectrum disorders for toddlers and young preschoolers from 12 to 47 months of age. Journal of Child Psychology and Psychiatry, 53, 143–151.
Klein, R. P., & Durfee, J. T. (1978). Effects of sex and birth order on infant social behavior. Infant Behavior and Development, 1, 106–117.
Koenig, K., & Tsatsanis, K. (2005). Pervasive developmental disorders in girls. In D. J. Bell, S. L. Foster, & E. J. Mash (Eds.), Handbook of behavioral and emotional problems in girls. New York: Springer.
Kopp, S., & Gillberg, C. (1992). Girls with social deficits and learning problems: Autism, atypical Asperger syndrome or a variant of these conditions. European Child and Adolescent Psychiatry, 1, 89–99.
Leaper, C., Anderson, K. J., & Sanders, P. (1998). Moderators of gender effects on parents’ talk to their children: A meta-analysis. Developmental Psychology, 34, 3–27.
Lord, C. (2011). How common is autism. Nature, 474, 166–168.
Lord, C., Luyster, R., Guthrie, W., & Pickles, A. (2012). Patterns of developmental trajectories in toddlers with autism spectrum disorder. Journal of Consulting and Clinical Psychology, 80(3), 477.
Lord, C., Risi, S., Lambrecht, L., Cook Jr, E. H., Leventhal, B. L., DiLavore, P. C., et al. (2000). The autism diagnostic observation schedule—generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of autism and developmental disorders, 30(3), 205–223.
Lord, C., Rutter, M., DiLavore, P., & Risi, S. (1999). Autism diagnostic observation schedule-generic. Los Angeles, CA: Western Psychological Services.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism diagnostic interview-revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24, 659–685.
Lord, C., Schopler, E., & Revicki, D. (1982). Sex differences in autism. Journal of Autism and Developmental Disorders, 12, 317–330.
Luyster, R., Gotham, K., Guthrie, W., Coffing, W., Petrack, R., et al. (2009). The autism diagnostic observation schedule—toddler module: A new module of a standardized diagnostic measure for autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 1305–1320.
Malatesta, C. Z., & Haviland, J. M. (1982). Learning display rules: The socialization of emotional expression in infancy. Child Development, 53, 991–1003.
Mitchell, S. K. (1979). Interobserver agreement, reliability, and generalizability of data collected in observational studies. Psychological Bulletin, 86(2), 376.
Mullen, E. M. (1995). Mullen scales of early learning (AGS (Edition ed.). Circle Pines: American Guidance Service Inc.
Nicholas, J. S., Charles, J. M., Carpenter, L. A., King, L. B., Jenner, W., & Spratt, E. G. (2008). Prevalence and characteristics of children with autism-spectrum disorders. Annals of Epidemiology, 18, 130–136.
Risi, S., Lord, C., Gotham, K., Corsello, C., Chrysler, C., Szatmari, P., et al. (2006). Combining information from multiple sources in the diagnosis of autism spectrum disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 45, 1094–1103.
Robins, D., Fein, D., Barton, M., & Green, J. (2001). The modified-checklist for autism in toddlers (M-CHAT): An initial investigation in the early detection of autism and Pervasive Developmental Disorders. Journal of Autism and Developmental Disorders, 31, 131–144.
Rosenthal, R. (1991). Meta-analytic procedures for social research (Vol. 6). New Delhi: Sage.
Shattuck, P., Durkin, M., Maenner, M., Newschaffer, C., Mandell, D., Wiggins, L., et al. (2009). Timing of identification among children with an autism spectrum disorder: Findings from a population-based surveillance study. Journal of American Academy of Child & Adolescent Psychiatry, 48(5), 474–483.
Snow, C. E. (1989). Understanding social interaction and language acquisition: Sentences are not enough. In M. H. Bornstein & J. S. Bruner (Eds.), Interaction in human development. Hillsdale, NJ: Erlbaum.
Sparrow, S. S., Cichetti, D. V., & Balla, D. A. (2004). Vineland Adaptive Behavior Scales-Second Edition (Vineland–II). Bloomington, MN: Pearson Assessment.
Stern, M., & Karraker, K. (1989). Modifying the prematurity stereotype: Impact of providing varied information. Journal of Clinical and Social Psychology, 8, 1–13.
Volkmar, F. R., Chawarska, K., & Klin, A. (2005). Autism in infancy and early childhood. Annual Review of Psychology, 6, 315–336.
Volkmar, F. R., Klin, A., Siegel, B., Szatmari, P., Lord, C., Campbell, M., et al. (1994). Field trial for autistic disorder in DSM-IV. American Journal of Psychiatry, 151, 1361–1367.
Wetherby, A. M., Allen, L., Cleary, J., Kublin, K., & Goldstein, H. (2002). Validity and reliability of the Communication and Symbolic Behavior Scales Developmental Profile with very young children. Journal of Speech, Language and Hearing Research, 45, 1202–1218.
Wetherby, A. M., Brosnan-Maddox, S., Peace, V., & Newton, L. (2008). Validation of the Infant-Toddler Checklist as a broadband screener for autism spectrum disorders from 9 to 24 months of age. Autism, 12, 487–511.
Wetherby, A. M., & Prizant, B. (2002). Communication and symbolic behavior scales developmental profile-first (normed ed.). Baltimore, MD: Paul H. Brookes.
Wing, L., & Gould, J. (1979). Severe impairments of social interaction and associated abnormalities in children: Epidemiology and classification. Journal of Autism and Developmental Disorders, 9, 11–29.
Yirmiya, N., & Ozonoff, S. (2007). The very early phenotype of autism. Journal of Autism and Developmental Disorders, 37, 1–11.
Zwaigenbaum, L., Bryson, S., Szatmari, P., Brian, J., Smith, I.M., Roberts, W. et al. (2012). Sex differences in children with autism spectrum disorder identified within a high-risk infant cohort. Journal of Autism and Developmental Disorders, 2. doi:10.1007/s10803-012-1515-y.
Acknowledgments
This research was supported in part by NICHD R01HD065272, NIDCD R01DC007462, and CDC U01DD000304 awarded to Amy M. Wetherby. Vanessa P. Reinhardt was supported in part by grant UA3 MC 11055 AIR-B from the Maternal and Child Health Research Program, Maternal and Child Health Bureau (Combating Autism Act Initiative), Health Resources and Services Administration, Department of Health and Human Services. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NICHD, NIDCD, the NIH, or the CDC. This paper was based on Vanessa Reinhardt’s Masters thesis.
Conflict of interest
Amy M. Wetherby receives royalties for the CSBS. Catherine Lord receives royalties for the ADOS and ADOS-T from Western Psychological Services.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Reinhardt, V.P., Wetherby, A.M., Schatschneider, C. et al. Examination of Sex Differences in a Large Sample of Young Children with Autism Spectrum Disorder and Typical Development. J Autism Dev Disord 45, 697–706 (2015). https://doi.org/10.1007/s10803-014-2223-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-014-2223-6