
Abstract
Few research-developed early intervention models have been deployed to and tested in real world preschool programs. In this study, teaching staff implemented a social communication modularized intervention, JASPER, in their daily program. Sixty-six preschool children with autism in twelve classrooms (12 teachers) were randomized to receive immediate JASPER training (IT) or were waitlisted (WL) for 3 months with a 1-month follow up. Measures of core deficits (initiations of joint engagement, joint attention gestures and language, play skills) and standardized cognitive measures were improved for IT over WL children. IT teachers achieved and maintained high fidelity. Teachers can implement evidence-based interventions with significant improvements in core deficits of their children with ASD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The majority of the nearly half million preschool-aged children with autism spectrum disorder (ASD) in the United States are served in public preschools (U.S. Department of Education 2015). Preschool teachers working within US school districts are provided with various commercialized curricula that provide a framework of lessons and strategies to target children’s learning across developmental domains. Often these curricula lack a specific focus on the core social communication challenges experienced by children with ASD which have been the focus of research based intervention studies (Kasari and Smith 2013; Wong and Kasari 2012). These challenges include joint engagement with adults and peers, joint attention gestures and language, and play skills.
Limitations in curricula that address core challenges in autism constitute only one of several gaps between research and practice in early intervention. Another concerns the difficulty in transferring interventions that are delivered one-on-one in research studies to classroom teachers who mostly teach in small groups. Thus, there may be a poor fit between the evidence based practice and the schooling context. Indeed, research-based joint attention interventions that have been transferred to classrooms typically mirror the one-on-one intervention model (Dykstra et al. 2012; Kaale et al. 2012, 2014; Lawton and Kasari 2012; Wong 2013). For example, Kaale et al. (2012) taught nursery school teachers how to implement a joint attention intervention with individual children, and found they were able to increase children’s joint attention skills and duration of time spent in joint engagement. Similarly, Lawton and Kasari (2012) taught teachers a similar joint attention intervention in a one-on-one format and found child improvements in initiating joint attention in the classroom. Although the foregoing studies yield positive results in both teachers and children, it is unclear whether the intervention is feasible and transportable into public preschool programs given that preschool teachers often have to work with small heterogeneous groups of children with ASD.
Additionally, these studies present limited follow up data. Follow up data typically only target the children and do not include the teachers. For example, in a 12-month follow up study, Kaale et al. (2014) demonstrated that children who received the joint attention intervention continued to show more gains in joint attention skills and joint engagement on assessments than children in the control group. It is not clear, however, if these interventions were maintained in the classroom setting, and whether teachers sustained the intervention practice over time.
Another research to practice gap concerns implementation fidelity. Researchers often find poorer implementation fidelity in moving lab based interventions into community settings, and fidelity affects child outcomes (Mandell et al. 2013; Stahmer et al. 2015). Thus, it is not uncommon to find smaller intervention effects in community settings than in controlled laboratory contexts. A factor that can affect fidelity is the complexity of the intervention. Most evidence-based social communication interventions are considered naturalistic, developmental, behavioral interventions (NDBIs; Schreibman et al. 2015). Due to the flexibility and individualization of NDBIs, implementation fidelity of these practices compared to simpler rule-based strategies (e.g., Discrete Trial Teaching; DTT) has been found to be lower and more variable (Stahmer et al. 2015). Therefore, NDBIs may require additional training, coaching, and immediate performance feedback in order for these interventions to be delivered at high enough fidelity to influence the core social communication skills of children with ASD (Stahmer et al. 2015).
Current Study
The present study extends teacher implemented studies by including a larger and more diverse sample of preschool students and teaching professionals in six early childhood programs in a large, urban public school district. Using community-partnered participatory research methods (Wells and Jones 2009), this study is the first examination of the implementation of a modified evidence-based social communication intervention, Joint Attention Symbolic Play Engagement and Regulation (JASPER; Kasari et al. 2006, 2008, 2010, 2014b). In this study JASPER was adapted for delivery using small group instruction by teachers and paraprofessionals in public preschool classrooms. In year 1 of this project we engaged teaching staff and administrators in meetings to determine the goals and procedures of the project, and we adapted the JASPER intervention to fit the needs of the classroom as recommended by the school staff. In this randomized waitlist design, our primary aims were to determine: (a) whether children who received the modified JASPER demonstrated greater improvements in joint attention, joint engagement and play skills over children in the waitlist control group, (b) if children in the modified JASPER condition would demonstrate greater improvements on standardized language and cognitive tests, and (c) if the modified JASPER was feasible in the preschool classrooms and to what degree could teachers deliver the intervention with fidelity. We hypothesized that children receiving the modified JASPER would demonstrate greater social communication, language and cognitive scores over children in the waitlist control group, and that teachers would maintain high levels of implementation fidelity.
Methods
Participants
Children
Participants were recruited from a large, urban public school district. Included children: (a) had a diagnosis of autism spectrum disorder (confirmed by the research team using the Autism Diagnostic Observation Schedule-2 (ADOS-2; Lord et al. 2012), (b) were between 3 and 5 years of age, and (c) were enrolled in one of six autism-specific preschool programs as part of a large urban public school district, all with the same classroom structure and ABA-based curriculum (Verbal Behavior Milestones Assessment and Placement Program). Seventy-eight children met inclusion criteria; however, only 66 children were included in the analyses for the study (See Results for detail). On average the 66 children were 50.26 months old (M = 50.26; SD = 6.38) and 89 % were male. Children ranged in developmental level at study entry (range 11.00–57.67 months; M = 35.41 months: MSEL mental age). Finally, children were of diverse ethnic backgrounds (69 % ethnic minorities) including 31 % Caucasian, 13 % African American, 21 % Hispanic, 16 % Asian, and 19 % Other/Mixed Race (Table 1).
Teaching Professionals
Each of the programs had four adults. Typically, this included the special education teacher, the teaching assistant, the speech and language pathologist assistant, and the behavior consultant. The special education teacher and teaching assistants were the primary target teachers since the other two staff members had a different supervisory structure through the district. The adult:student ratio was 1:2, with 8 children in each classroom (2 classrooms per school program). For the purpose of the study, one teacher and one teaching assistant (hereafter referred to as teachers) were included from each of the six preschool programs, except for one program where we had one teacher and two teaching assistants (n = 13). Included teachers were: (a) employed by the public school district and provided services in the target preschool programs, and (b) available for the intervention.
Randomization and Study Design
Participants were Randomized at the School Level
The school district had autism specific preschool programs at six schools, spaced across the very large school district. Each of these autism programs included two sessions per day (morning and afternoon class) for a total of 12 classrooms. For our purposes, the six schools were matched into three pairs based on the schools’ percentage of students reporting as ethnic minorities, percentage of free and reduced lunch, and percentage of English language learners. Within the matched pair, schools were randomized to immediate JASPER treatment (IT) or to waitlist (WL) who received JASPER 4 months later. Altogether, three programs with six classrooms and including 38 children were randomized to IT and three programs with six classrooms and including 28 children were randomized to WL (See Fig. 1: Flow Chart). Programs that were randomized to IT were taught how to incorporate JASPER strategies into the usual preschool curriculum while the WL classrooms continued with the usual preschool curriculum only.

Flow chart
Intervention
Phase I: JASPER Overview and Target Selection
All six programs were part of the same school district and were intended to be identical in classroom structure and content to make the same program available throughout the district. Therefore, each program had the same center based rotation structure and largely the same toys and materials available within the classrooms. All six programs used the Verbal Behavior Milestones Assessment and Placement Program (VB-MAPP; Sundberg 2008) as their preschool curriculum. They also implemented the same classroom structure including approximately six activity centers each targeting a separate domain of activities/skills including symbolic play, independent play, communication, fine motor, independent activities, and snack. Each activity center was staffed by an adult who would engage students one-on-one or in small groups of 2–3 students. Teachers in the IT group were trained to implement the JASPER intervention (e.g., Kasari et al. 2006, 2008, 2014b) at the pre-existing “play center” where preschool toys were made available for free play, such as a kitchenette, dolls, cars, and blocks. The current study adapted the JASPER model to fit the needs of teachers in a preschool classroom setting who worked with small groups of students as well as those working one-on-one. The primary adaptation included strategic groupings of children based on developmental play level (when possible), appropriate toy selection for the small groups (dependent on children’s play level), environmental seating arrangements that promoted social interactions, and strategies to increase awareness and initiations of peer-to-peer interactions (See “Appendix 1” for more details).
Phase 1: Consultation and Coaching
To begin, two initial 30-min preparation sessions (without the children) were conducted with the target teachers of each classroom. These sessions were conducted in addition to the 8-week in vivo coaching sessions that each individual teacher received as part of the modified JASPER training. These preparation sessions took place in the classroom during the teachers’ preparation time. During the first session, a researcher presented an overview of the basic JASPER strategies via PowerPoint. In the second session, the researcher and the teachers selected developmentally appropriate toys from within the classroom to use during JASPER play sessions. Toy selection was based on information gathered from the student’ entry assessments to determine mastered and target play levels (Shire 2013).
Based on the developmental framework of play introduced to the teachers, Phase 1 of intervention involved categorizing the available materials by play level. In this process, toys that had previously been put away in closets were brought into the play center. Some teachers also made toys for their students when they felt limited by the availability of materials in the classroom. For example, teachers made binoculars and telescopes out of cardboard paper rolls for the children to pretend to be “pirates” within symbolic and thematic play routines. Teachers engineered their play spaces to allow for access to developmentally appropriate toys for each small group, placing other materials out of sight.
Phase 2: In-Vivo Sessions
On site live intervention coaching sessions were provided for 8 weeks for a maximum of 60, 15 min long coaching sessions. The dose of coaching sessions was based on previous parent-mediated JASPER studies that demonstrated effectiveness, which ranged from 24–30 30-min sessions (Kasari et al. 2010, 2014a), and was adapted for feasibility in the context of the classroom. The researchers coached the teachers to use JASPER strategies with their students during the 15-min play center rotation. Coaching included modeling of intervention strategies as well as live feedback and troubleshooting for the teachers as they practiced implementing the strategies with their students. During the first 4 weeks of intervention, each teacher received two 15-min coaching sessions daily. Weekly handouts of specific JASPER strategies were also given to the teachers such that all program content was introduced within these first 4 weeks. For the remaining 4 weeks, coaching frequency was reduced to 2–3 times a week (two 15-min sessions each time per target teacher) and no new topics were introduced. Instead, the sessions focused on practicing the full JASPER module and troubleshooting challenges teachers may have had.
The second phase of the intervention focused on teachers’ active roles and responses to the students during play to foster and maintain joint engagement and build developmentally appropriate play routines. Teachers in this study were very comfortable prompting children and demanding output within their instructional sessions. Within JASPER, teachers were asked to be less directive and to provide structure that allowed the teacher to focus on children’s appropriate and functional initiations of play and social communication. This required teachers to focus on environmental strategies, to talk less (e.g., less verbal prompting of play acts), to become highly responsive to initiations of play and communication from all students, to expand those initiations, and to have knowledge of the next steps in the child’s sequence of development.
Phase 2: JASPER Rotations
The 8-week in vivo JASPER coaching sessions were conducted in the existing play centers within the classroom. Children rotated into the JASPER play centers on 15-min intervals either in small groups of 2–4 children or in a one-on-one format depending on the child’s needs. During these play centers teachers actively interacted with the children while the researchers coached the teachers to use JASPER strategies during these interactions.
The number of children in each group depended on student attendance as well as classroom needs (e.g., behavior management for specific children). The head teacher determined the composition of the small groups and at times this was decided by what teachers wanted to accomplish in their other academic centers aside from the play center. This in turn would affect which children were grouped or placed individually in the play center. Most of the time, children were placed in groups during the play center rotations. For the IT group, prior to intervention, 86 % of the children were in small groups, while the WL group had 84 %. After intervention, IT group had 69 % of the children in small groups and the WL group had 78 % (See Table 3).
Follow-Up Phase
No consultation was provided to the IT group during the 4-week follow up phase. Teachers in the WL group began their Phase 1 Consultation and Coaching one week prior to the IT follow-up data collection. Same as the IT group, the university-based trainers presented the basic JASPER strategies via PowerPoint and selected developmentally-appropriate toys for their students with the WL teachers based on information gathered from children’s assessments. The 1-week Phase 1 preparation ensured that Phase 2 JASPER rotation could begin in a timely manner immediately after the follow-up assessments were completed so that all WL teachers received the same dose of coaching as the IT group within the time limit of the school year.
Measures
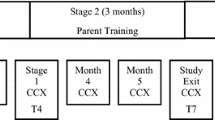
Child and teacher measures were collected at three time points for both the IT and WL group: Entry, Exit (after 2 months), and 1-Month Follow Up (after 3 months for the IT group only).
Child Measures
At study entry, families were asked to complete a demographic form to provide basic information about the characteristics of the child and family (e.g., birthdate, gender, ethnicity, parents’ age and occupations, etc.). The research team administered the Autism Diagnostic Observation Schedule-2 (ADOS-2; Lord et al. 2012) to confirm the children’s autism diagnosis. In addition, the following measures were administered:
The Mullen Scales of Early Learning (MSEL; Mullen 1995) is a standardized test used to measure the child’s cognitive ability. Four cognitive domains were assessed: visual reception, fine motor, receptive and expressive language. Age equivalent scores are available for each subscale. The MSEL was administered at study entry and at the 1-month follow up visit.
Ten-minute teacher-child play interactions (TCX) were taped at study entry, exit, and follow up by research assistants blind to classroom treatment allocation. Following the existing structure set out within the classrooms, the teacher engaged any number of students ranging from one-on-one sessions through groups of students. The TCX was coded for the primary teacher outcome (teachers’ strategy implementation) and primary child outcomes (duration of joint engagement, frequency of initiated joint attention/initiated behavioral regulation, diversity of play skills).
The Early Social-Communication Scales (ESCS: Mundy et al. 1986; Seibert et al. 1982) is a 20–30 min semi-structured assessment used to assess joint attention and behavior regulation skills. The ESCS was delivered at entry, exit, and follow up by a trained assessor in the child’s classroom and videotaped (fidelity of administration M = 86.96, SD = 9.09). Examiners blind to study time point and treatment arm coded the videotapes for the type and frequency of spontaneous joint attention skills (IJA) and spontaneous behavior regulation skills (IBR). Studies have shown ESCS to have good reliability (range = 0.61–0.91) and validity with language measures (Mundy et al. 1994, 1995).
The Structured Play Assessment (SPA; Kasari et al. 2006; Ungerer and Sigman 1981) consists of 5 play sets presented one at a time over a 15–20 min period to measure the child’s spontaneous play acts. Only spontaneous play is recorded, and children are not prompted to engage with toys in any particular way. The assessment is delivered at study entry, exit, and follow up by trained, reliable assessors blind to child treatment allocation (fidelity of administration M = 89.60, SD = 15.41). The SPA is videotaped and later coded by raters who are blind to study time point and treatment arm.
Coding
Graduate students and research assistants who were blind to the study hypothesis, treatment condition, and time points were trained for different coding systems: Engagement, IJA/IBR, play, and teacher implementation strategies. Blind raters were trained on practice videos until reliability was established at 80 %.
Primary Child Outcomes
Joint Engagement: TCX
The teacher-child play interactions were separated into 1-min intervals (total of 10 min) for children’s engagement, play level, and whether the interaction was adult-directed (e.g., teacher redirects the child’s attention to their choice of activity or verbally/physically prompts the child’s to participate; see “Appendix 2” for description of coded variables) or child initiated (e.g., child selects and starts a play routine and the teacher follows). In addition, children’s frequency of IJA (verbal and nonverbal) and IBR (verbal and nonverbal) were coded. For both verbal joint attention and behavioral regulation skills, the number of words used per utterance was coded as “1-word utterance”, “2-word utterance, or “3 or more words utterance”. (See “Appendix 2” for description of coded variables).
IJA/IBR: TCX
Independent raters coded the 10-min teacher-child play interactions for the frequency of spontaneous IJA and IBR including eye contact, gestures (pointing, showing, giving) and language. The overall intra-class coefficient (ICC) for IJA was 0.90 and for IBR 0.95.
IJA & IBR Language
To examine the complexity of language skills in the TCX, the length of the children’s spontaneous utterances to share (IJA) and spontaneous utterances to request (IBR) were coded at three levels: (a) one word, (b) two words, and (c) three or more words. IJA language includes children’s comments and social greetings (e.g., “Let’s play!”). IBR language includes children’s requests to access material, gain information, or get their needs met (e.g., “I want block.”). A spontaneous utterance is defined as a verbal initiation from the child. Only verbal utterances that were clear, appropriate in context (non-repetitive), and directed (to an adult or peer) were counted. All sound effects (e.g., “beep beep”), counting (e.g., “1, 2, 3, 4, 5”), and carrier phrases (e.g., “Ready, set, go”) were counted as one word.
IJA/IBR: ESCS
IJA and IBR from the ESCS were coded using the same coding scheme as the TCX. ICCs for IJA were 0.87 and IBR 0.96.
Play: TCX
The 10-min teacher-child play interactions were split into 1-min intervals (total of 10 intervals). For each interval, coders identified the child’s play level for the majority of the interval. Nine levels of play were coded: Not Playing, Sensory, Simple, Presentation Combination, General Combination, Combination/Pre-Symbolic, Symbolic, Games with Rules, and Thematic. Sensory and simple play were combined to create the category referred to as simple play. Presentation Combination, General Combination, and Combination/Pre-Symbolic were collapsed to form a category functional play. Lastly, symbolic, games with rules, and thematic fantasy play were combined to create the category of symbolic play. Reliability was established with an average accuracy of 0.80.
Play: SPA
The number of unique spontaneous play types and frequency of those acts were coded based on 16 levels of play ranging from indiscriminant to thematic play (Lifter and Bloom 1989). The coding of types and level of play have shown excellent reliability and validity across a range of studies (Kasari et al. 2006; Sigman and Ruskin 1999; Sigman and Ungerer 1984). The 16 levels of play were then divided into four broad categorical types of play: simple, combination, pre-symbolic, and symbolic (See Table 2). The four types of play are based on the developmental sequence of play in child development (Sigman and Ungerer 1984) and were also used to select play targets for the intervention (Shire 2013). Reliability was established for the four types of play: Simple play (α = 0.87–0.96), combination play (α = 0.80–0.99), pre-symbolic play (α = 0.97–0.98), and symbolic play (α = 0.85–0.94). ICCs were calculated for each rater for frequency of play acts including simple play (α = 0.85–0.96), combination play (α = 0.87–0.99), pre-symbolic play (α = 0.95–0.97), and symbolic play (α = 0.87–0.93).
Teacher Outcome
Teachers’ implementation of JASPER strategies was coded from the 10-min teacher-child play interactions (TCX). Teachers’ implementation with all children that they interacted with during the JASPER play rotation was assessed since teachers were not assigned a specific student. The fidelity measure included 31 items targeting the seven main components of the intervention (see “Appendix 1” for JASPER components). Teachers were held to the same standards for implementation as the research clinicians. Each item was rated on a scale of 0–5 where “0” reflected incorrect or lack of implementation of the strategy, a “3” described mixed strategy implementation where up to 50 % of opportunities to use a strategy were missed, and a “5” represented accurate and developmentally appropriate implementation of the strategies at least 80 % of the time. Item scores were summed and divided by the total number of possible points to obtain a total percentage score for strategy implementation. Three reliable raters scored the teachers’ strategy implementation (α = 0.963).
Statistical Analysis
To assess the success of randomization, t tests, Wilcoxon tests, Chi square tests and Fishers exact tests were used to compare characteristics between groups at baseline including child’s developmental skills, joint engagement, social communication skills of IJA and IBR. To model the trajectories of primary and secondary outcomes over treatment and follow up, generalized linear mixed models (GLMM) were applied including main effects of treatment group allocation (IT JASPER and WL), main effects of time, treatment group by time interactions and subject level random intercepts. Separate models were fit for each longitudinal outcome where time was modeled continuously with measurements in months. GLMM account for correlations between repeated measures within subjects, easily allow for both fixed and time-varying covariates and automatically handle missing data, producing unbiased estimates as long as observations are missing at random. Hence, all available observations from each participant were included following an intent-to-treat approach. A “treatment effect” was defined as a significant interaction effect between the IT group and time from baseline to treatment exit. Further, maintenance of the treatment effect was defined as a significant improvement from entry to the 1-month follow-up within the IT group only consistent with waitlist control designs.
Specific to the examination of children’s play skills, symbolic play was examined as a binary process at all time-points where “0” represented children with no symbolic play types and where “1” represented those children with at least one symbolic play type. Symbolic play was not treated as a continuous variable because of the high prevalence of zero symbolic play types at all time points on the SPA. All other outcome variables were continuous.
Results
Preliminary Analysis: Child Characteristics at Study Entry
There were a total of 78 children who consented to participate in the study. However, 12 children consented after the midpoint of the study due to rolling enrollment of children into the preschool programs. These children were excluded from the analysis due to the limited dosage of treatment received. Therefore, 66 children (28 waitlist and 38 immediate treatment) were included in the final analyses evaluating treatment effects.
There were no significant differences in the distribution of gender, chronological age, mental age, receptive language, and expressive language between the treatment groups at entry (see Table 1). The WL group had a slightly higher but non-significant average chronological age. Though mental age was not significantly different between treatment groups, mental age at baseline was included in all regression models to adjust for potential confounding effects of children’s differing skills and abilities. Children’s ethnicity was distributed differentially between treatment groups (p = 0.001) due to school level randomization. Therefore, ethnicity was entered as a parameter in the primary outcome models. Ethnicity was not a significant predictor in any model examining a primary outcome and thus, was omitted from the final models. In addition, site differences and/or clustering effects were reviewed extensively. We evaluated whether there were overall site differences in child characteristics and also site differences in child characteristics within treatment groups. No site differences were found. There were no differences by treatment groups at baseline for all outcome measures: TCX, ESCS, SPA, and Group Size (see Table 3).
Primary Child Outcomes: Joint Engagement, Joint Attention, Requesting and Play
Child-Initiated Joint Engagement
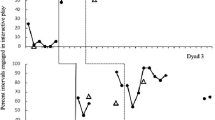
The total time in child-initiated joint engagement with teachers and peers was coded from the TCX. Confirming a priori hypotheses, a significant time by treatment interaction was found, F(1,56) = 5.81, p = 0.019, where children in the IT group spent significantly more time in child-initiated joint engagement than children in WL. In addition, the JASPER IT group maintained the treatment effect at the 1 month follow-up, F(1,65) = 4.83, p < 0.001 (Fig. 2).

Child initiated joint engagement
Initiations of Joint Attention and Requesting
The total number of spontaneous IJA and IBR were coded from two separate contexts, the ESCS and the TCX. There was no significant interaction between treatment group and time on the ESCS for IJA, F(1,59) = 0.27, p = 0.60, or IBR, F(1,59) = 1.34, p = 0.25. There was an overall effect of time for both IJA and IBR, F(1,59) = 7.00, p = 0.01; F(1,59) = 6.11, p = 0.016, respectively. All children improved on IJA and IBR coded from the ESCS over time.
For the TCX, a significant time by treatment interaction was found for both initiations of IJA and IBR, F(1,56) = 5.54, p = 0.022; F(1,56) = 5.94, p = 0.018, respectively, indicating greater growth for children in the IT group. The treatment effect for IJA and IBR was maintained at 1 month follow-up, F(1,65) = 6.94, p = 0.011; F(1,65) = 4.62, p = 0.035 respectively.
IJA Language
A significant time by treatment interaction was found at all three lengths of utterance for IJA language, F(1,56) = 4.47, p = 0.039; F(1,56) = 7.90, p = 0.007; F(1,56) = 7.84, p = 0.007, respectively, with greater gains for those in the IT group. Gains in two word, F(1,65) = 0.14, p = 0.711, and three or more word, F(1,65) = 9.55, p = 0.003, levels were maintained at follow up. Frequency of one-word utterances to share were not significantly different at 1 month follow up, F(1,65) = 18.31, p ≤ 0.001.
IBR Language
A significant time by treatment interaction was found with greater number of one word requests in the IT group, F(1,56) = 8.13, p = 0.006. However, these gains were not maintained at follow-up, F(1,65) = 0.50, p = 0.483. No differences between groups were found for frequency of two or three or more word utterances to request, F(1,56) = 3.18, p = 0.080; F(1,56) = 1.18, p = 0.243, respectively.
Play Level: TCX
Change in the percentage of time spent in the four categorical types of play was examined: simple play, functional play, and symbolic play. There was a significant treatment effect in simple play where children in the IT group and children in the WL group had diverging levels of simple play, F(1,54) = 14.45, p < 0.001. Children in the IT group were significantly decreasing their time spent in simple play during the treatment phase; whereas, children in the WL group were increasing their time spent in simple play. In addition, the treatment effect was maintained at the follow-up where the time spent in simple play was still significantly lower than the time spent in simple play at entry, F(1,64) = 14.8, p < 0.001.
There was a significant treatment effect in functional play where children in the IT group spent significantly more time in functional play compared to the children in the WL group, F(1,55) = 5.19, p = 0.0267, from entry to exit. In addition, the children in the IT group maintained their increase at follow-up, F(1,64) = 19.77, p < 0.001. Lastly, there were no significant treatment effects in symbolic play, F(1,55) = 0.30, p = 0.583.
Spontaneous Unique Play Types: SPA
Three different levels of play on the SPA were evaluated using the SPA for treatment and maintenance effects: simple, combination + pre-symbolic (i.e. functional), and symbolic play. A main effect of time was found for both simple and functional play types from study entry to exit, F(1,57) = 6.71, p = 0.012; F(1,57) = 6.59, p = 0.013, respectively. There was a significant time by treatment interaction where the IT group exhibited greater rate of improvement in simple and functional play types from the start of the treatment to exit as compared to the WL group’s rate of change, F(1,57) = 7.07, p = 0.010; F(1,57) = 8.77, p = 0.0045. The IT group also maintained their treatment effect demonstrating more simple and functional play types at their 1 month follow-up compared to entry, F(1,63) = 25.65, p < 0.001; F(1,63) = 11.65, p = 0.001, respectively. There was no significant effect of treatment for change in symbolic play types, F(1,57) = 2.12, p = 0.151.
Secondary Child Outcome: Standardized Measures of Children’s Language and Cognition
Difference scores (both age equivalency [AE] and T scores) from entry to follow up were calculated for children in the IT and WL group. Two sample t tests assuming unequal variance were applied to the difference scores. A significant difference between groups was found for MSEL mental age, t(58.99) = −3.05, p = 0.003, the visual receptive subscale, t(58.52) = −2.06, p = 0.043, the fine motor subscale, t(53.31) = −2.32, p = 0.024, and the receptive language subscale, t(53.22) = −2.56, p = 0.013, where group means indicate a difference in favor of children in the IT group over WL. However, no significant difference was found for the expressive language subscale, t(58.26) = −0.56, p = 0.58.
Teacher Outcome: Strategy Adoption and Implementation
Overall, a main effect of time was found for all teachers’ strategy implementation, F(1,53) = 10.80, p = 0.002, with a significant treatment by time interaction, F(1,53) = 41.33, p < 0.001. While all teachers improved over time, teachers in the IT group demonstrated greater JASPER strategy adoption and correct implementation compared to those in the waitlist from study entry to exit. The IT group maintained the treatment effect by the 1 month follow-up, F(1,64) = 88.24, p < 0.001 (Fig. 3).

Teacher’s strategy implementation
Discussion
The current study examined the feasibility of adding a brief targeted social communication intervention into public preschool classrooms for children with ASD. In collaboration with school staff, the targeted module was layered into the existing framework of the classroom. The preschools were already applying a commonly used curriculum following applied behavior analytic principles (VB-MAPP: Sundberg 2008). Most of the research on VB-MAPP suggests it is an effective assessment tool and curriculum guide (Gould et al. 2011; Sundberg and Sundberg 2011). However, VB-MAPP lacks the specifics in addressing the social communication and play challenges of children with ASD. Teachers need additional clinical expertise to create and teach lessons to address the social communication challenges of children with ASD. Thus, we adapted JASPER, an evidence-supported modular social communication intervention to fill this need in preschool programs.
This study yielded three main findings. First, teachers and teaching assistants demonstrated high quality JASPER strategy implementation scores comparable to university-based clinicians by the end of the intervention period. Most studies have reported a significant reduction in fidelity when interventions developed in highly controlled laboratory settings are moved into community settings (Mandell et al. 2013). This study suggests that community stakeholders can deliver JASPER with high fidelity as one component of their center based preschool classroom day. High fidelity might be the result of the use of community partnered participatory methods to adapt JASPER for the classroom, as well as the level and sustainment of coaching support. Implementation strategies vary for studies that move interventions into the community. In this study, coaching support was brief (delivered in 15 min periods) but sustained throughout the 2 months of intervention. Coaching support was designed to be more intense up front with fading of support over the course of intervention. Another implementation strategy used was limiting disruption to classroom structures by fitting JASPER into the existing classroom structure (e.g., small groups with peers), and using existing classroom materials. This was a first step into community scale up. A next step would be to look at the extent of support needed in various community contexts for uptake and sustainability of new practices.
Second, although children were similar in their social communication and cognitive/language skills prior to beginning intervention, significant effects were noted for children receiving 2 months of daily JASPER in their classroom. Children who received JASPER demonstrated significant increases in their initiations of joint attention gestures, joint attention language, child-initiated joint engagement and mean length of language with their teachers over children in the waitlist. These effects were noted for spontaneous initiations. Many studies report improvements in joint attention gestures, or language use, but effects are often in prompted responses than in spontaneous initiations (Hardan et al. 2015; Ingersoll and Schreibman 2006). In this study, proximal effects as noted above were significant as were more distal outcomes (e.g., play skills) in standardized test results. Joint attention skills did not generalize from TCX to the ESCS; however, children, overall, did increase their joint attention skills. Joint attention is a core deficit that may require more time for children to use more efficiently and effectively, and to generalize. Rarely have short- term targeted interventions yielded significant change in distal standardized tests over a short, 3-month period of time.
Third, effects were maintained over follow up. Although this study was relatively brief (conducted over 5 months of the school year), testing for maintenance effects after coaching support is removed has been rare in implementation studies in the community for children with ASD. Follow ups are often difficult given the structure of school settings, and the ability to conduct both immediate treatment and wait list interventions in the course of a single school year.
The study results are positive and suggest that several factors may be important in moving targeted, evidence supported interventions into community settings. First, using community partnered participatory methods may lead to better buy-in by community staff and ultimately sustainability (Wells and Jones 2009). Given the short- term nature of this study, however, a future goal would be to follow teacher practices for longer periods of time (e.g., across different school years) to determine the sustained adoption of strategies. Second the social partner is an important factor. Children demonstrated stronger social-communication skills in interactions with their teachers than with unfamiliar testers. Supportive interactive partners may be critical to children being able to initiate communication in play interactions; a future important initiative would be to teach all partners in the child’s environment specific supportive strategies (e.g., parents, other staff).
Finally, the importance of development cannot be under-estimated. Fundamental to most naturalistic developmental behavioral interventions (NDBIs) is the use of the play context for teaching important skills. A unique aspect of JASPER is the careful developmental assessment of children’s play level, and selection of developmentally appropriate toys to build play routines for teaching social communication and language skills. A consideration for small group adaptation of JASPER was the selection of play materials and creation of play routines that fit the developmental play level of all children within the group. Prior to implementing JASPER in the class, teachers had grouped children by their communication or IEP targets rarely their play level. JASPER implementation required teachers to consider toy choice and the match between peer -play level in a center as well.
This skillful scaffolding of play from teachers and teaching assistants may explain the diverging effect in simple play between the IT and WL group. The IT and WL groups were not significantly different in play skills at baseline; however, at the end of intervention, the IT group decreased their overall simple play and increased their functional play in interactions with their teachers. This proximal change in play skill in interactions with their teachers was also noted in the distal testing of play skills on the SPA with an unfamiliar tester. In this context, children in the IT group demonstrated more functional play than children in the WL group.
Strengths, Limitations, and Next Steps
Despite the small number of classrooms (n = 12) in the study, there are clear strengths of this study with positive effects on child outcomes, and high levels of teacher fidelity to the treatment. There are also a number of limitations, not the least of which are due to challenges in implementing interventions into schools (Kasari and Smith 2013). Due to the constraints of the school year timeline, only a brief 1-month follow up period could be conducted. There were also slight decreases in teachers’ strategy implementation and children’s play skills at follow up which indicate a need to examine additional supports to sustain teachers’ continued application of the JASPER intervention strategies.
While we included measures that were both proximal and distal to the intervention focus, other measures would have been useful, including a peer interaction measure, and measures of generalization for both teacher and child behaviors. Future studies may benefit from examining child behavioral change with other partners, such as parents and peers.
Conclusion
Teachers can implement evidence-based interventions with significant improvements in core deficits of their children with ASD. Teachers are also able to achieve and maintain high fidelity in implementing the intervention. Future studies need to explore the intensity and dose of the training to further refine the acceptability and feasibility for scale up interventions.
References
Dykstra, J. R., Boyd, B. A., Watson, L. R., Crais, E. R., & Baranek, G. T. (2012). The impact of the Advancing Social-communication And Play (ASAP) intervention on preschoolers with autism spectrum disorder. Autism, 16(1), 27–44.
Gould, E., Dixon, D. R., Najdowski, A. C., Smith, M. N., & Tarbox, J. (2011). A review of assessments for determining the content of early intensive behavioral intervention programs for autism spectrum disorders. Research in Autism Spectrum Disorders, 5(3), 990–1002.
Hardan, A. Y., Gengoux, G. W., Berquist, K. L., Libove, R. A., Ardel, C. M., Phillips, J., et al. (2015). A randomized controlled trial of Pivotal Response Treatment Group for parents of children with autism. Journal of Child Psychology and Psychiatry, 56, 884–892.
Ingersoll, B., & Schreibman, L. (2006). Teaching reciprocal imitation skills to young children with autism using a naturalistic behavioral approach: Effects on language, pretend play, and joint attention. Journal of Autism and Developmental Disorders, 36(4), 487–505.
Kaale, A., Fagerland, M. W., Martinsen, E. W., & Smith, L. (2014). Preschool-based social communication treatment for children with autism: 12-Month follow-up of a randomized trial. Journal of the American Academy of Child and Adolescent Psychiatry, 53, 188–198.
Kaale, A., Smith, L., & Sponheim, E. (2012). A randomized controlled trial of preschool-based joint attention intervention for children with autism. Journal of Child Psychology and Psychiatry, 53, 97–105.
Kasari, C., Freeman, S., & Paparella, T. (2006). Joint attention and symbolic play in young children with autism: A randomized controlled intervention study. Journal of Child Psychology and Psychiatry, 47(6), 611–620.
Kasari, C., Gulsrud, A. C., Wong, C., Kwon, S., & Locke, J. (2010). A randomized controlled caregiver mediated joint engagement intervention for toddlers with autism. Journal of Autism and Developmental Disorders, 40, 1045–1056.
Kasari, C., Kaiser, A., Goods, K., Nietfeld, J., Mathy, P., Landa, R., … & Almirall, D. (2014a). Communication interventions for minimally verbal children with autism: A sequential multiple assignment randomized trial. Journal of the American Academy of Child & Adolescent Psychiatry, 53(6), 635–646.
Kasari, C., Lawton, K., Shih, W., Barker, T. V., Landa, R., Lord, C., et al. (2014b). Caregiver-mediated intervention for low-resourced preschoolers with autism: An RCT. Pediatrics, 134, e72–e79.
Kasari, C., Paparella, T., Freeman, S., & Jahromi, L. B. (2008). Language outcome in autism: Randomized comparison of joint attention and play interventions. Journal of Consulting and Clinical Psychology, 76, 125–137.
Kasari, C., & Smith, T. (2013). Interventions in schools for children with autism spectrum disorder: Methods and recommendations. Autism, 17(3), 254–267.
Lawton, K., & Kasari, C. (2012). Teacher-implemented joint attention intervention: Pilot randomized controlled study for preschoolers with autism. Journal of Consulting and Clinical Psychology, 80, 687–693.
Lifter, K., & Bloom, L. (1989). Object knowledge and the emergence of language. Infant Behavior and Development, 12(4), 395–423.
Lord, C., Rutter, M., DiLavore, P. C., Risi, S., Gotham, K., & Bishop, S. L. (2012). Autism diagnostic observation schedule, 2nd Edn., (ADOS-2) Manual (Part 1): Modules pp 1–4.
Mandell, D. S., Stahmer, A. C., Shin, S., Xie, M., Reisinger, E., & Marcus, S. C. (2013). The role of treatment fidelity on outcomes during a randomized field trial of an autism intervention. Autism, 17(3), 281–295.
Mullen, E. (1995). Mullen scales of early learning. Circle Pines, MH: American Guidance Service.
Mundy, P., Kasari, C., Sigman, M., & Ruskin, E. (1995). Nonverbal communication and early language acquisition in children with Down syndrome and in normally developing children. Journal of Speech, Language, and Hearing Research, 38(1), 157–167.
Mundy, P., Sigman, M., & Kasari, C. (1994). Joint attention, developmental level, and symptom presentation in autism. Development and Psychopathology, 6(03), 389–401.
Mundy, P., Sigman, M., Ungerer, J., & Sherman, T. (1986). Defining the social deficits of autism: The contribution of non-verbal communication measures. Journal of Child Psychology and Psychiatry, 27(5), 657–669.
Schreibman, L., Dawson, G., Stahmer, A. C., Landa, R., Rogers, S. J., McGee, G. G., et al. (2015). Naturalistic developmental behavioral interventions: Empirically validated treatments for autism spectrum disorder. Journal of Autism and Developmental Disorders, 45, 2411–2418.
Seibert, J. M., Hogan, A. E., & Mundy, P. C. (1982). Assessing interactional competencies: The early social-communication scales. Infant Mental Health Journal, 3(4), 244–258.
Shire, S. Y. (2013). A novel teacher implemented protocol to assess early social communication and play skills in preschool children with Autism. Los Angeles: University of California.
Sigman, M., & Ruskin, E. (1999). Social competence in children with Autism, Down syndrome and other developmental delays: A longitudinal study. Monographs of the Society for Research in Child Development, Serial No. 256, 64(1).
Sigman, M., & Ungerer, J. A. (1984). Cognitive and language skills in autistic, mentally retarded, and normal children. Developmental Psychology, 20(2), 293.
Stahmer, A. C., Rieth, S., Lee, E., Reisinger, E. M., Mandell, D. S., & Connell, J. E. (2015). Training teachers to use evidence-based practices for autism: Examining procedural implementation fidelity. Psychology in the Schools, 52(2), 181–195.
Sundberg, M. L. (2008). Verbal behavior milestones assessment and placement program: The VB-MAPP. Concord, CA: AVB Press.
Sundberg, M. L., & Sundberg, C. A. (2011). Intraverbal behavior and verbal conditional discriminations in typically developing children and children with autism. The Analysis of Verbal Behavior, 27(1), 23.
Ungerer, J. A., & Sigman, M. (1981). Symbolic play and language comprehension in autistic children. American Academy of Child Psychiatry, 20, 318–337.
U.S. Department of Education, National Center for Education Statistics. (2015). Digest of education statistics, 2013 (NCES 2015-011), Chapter 2.
Wells, K., & Jones, L. (2009). “Research” in community-partnered, participatory research. JAMA, 302(3), 320–321.
Wong, C. S. (2013). A play and joint attention intervention for teachers of young children with autism: A randomized controlled pilot study. Autism, 17, 340–357.
Wong, C., & Kasari, C. (2012). Play and joint attention of children with autism in the preschool special education classroom. Journal of Autism and Developmental Disorders, 42(10), 2152–2161.
Acknowledgments
This study was funded by Autism Speaks Grant #7495 (PI: Kasari). We would like to thank the children and families who participated in the study as well as the dedicated teachers, paraprofessionals, and Los Angeles Unified School District for their participation and collaboration on this project. We would also like to thank the team of assessors and coders: Fahad Alnemary, Faisal Alnemary, Kathleen Berry, Michelle Dean, Charlotte DiStefano, Reina Factor, Elizabeth Fuller, Matthew Goodman, Hilary Gould, Clare Harrop, Alison Holbrook, Abbey Hye, Kelsey Johnson, Elizabeth Karp, Kiana Krolik, Jason Lee, Marcella Mattos, Caitlin McCracken, Marina Mladenovic, Jonathan Panganiban, Andrew Schlink, Alyssa Tan, Nicole Tu, and Marta Wirga.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Author Contributions
YC co-coordinated the study, coached the teachers and paraprofessionals, and drafted the manuscript. SS co-coordinated the study, coached the teachers and paraprofessionals, and drafted the manuscript; WS conducted the analyses for the study; CG was the liaison between the community and the university for the project; CK is the principal investigator of the interventional trial and assisted in the drafting of the manuscript.
Conflict of Interest
None.
Rights and permissions
About this article

Cite this article
Chang, YC., Shire, S.Y., Shih, W. et al. Preschool Deployment of Evidence-Based Social Communication Intervention: JASPER in the Classroom. J Autism Dev Disord 46, 2211–2223 (2016). https://doi.org/10.1007/s10803-016-2752-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-016-2752-2