
Abstract
Discernment of possible sex-based variations in presentations of autism spectrum disorder (ASD) symptoms is limited by smaller female samples with ASD and confounds with ASD ascertainment. A large national cohort of individuals with autism, SPARK, allowed parent report data to be leveraged to examine whether intrinsic child characteristics and extrinsic factors differentially impact males and females with ASD. Small but consistent sex differences in individuals with ASD emerged related to both intrinsic and extrinsic factors, with different markers for males and females. Language concerns in males may make discernment of ASD more straightforward, while early motor concerns in females may hamper diagnosis as such delays are not identified within traditional ASD diagnostic criteria.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sex Differences in ASD
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder defined by the presence of social communication impairments and restrictive and repetitive behaviors (American Psychiatric Association, 2013). There is a male bias in the prevalence of ASD, with approximately three to four males to every one female being diagnosed (Loomes et al., 2017). Biological sex and gender differences in ASD are actively being researched, reflecting the concern that the preponderance of males may overshadow the existence of sex and gender differences in the expression of autism symptoms. Some hypothesize that the male prevalence bias is partially perpetuated due to ASD research being predominantly limited to male samples and sampling techniques in prospective and large-scale population-based studies (Lai, Baron-Cohen, et al., 2015; Lai, Lombardo, et al., 2015; Loomes et al., 2017). As the diagnostic criteria for ASD are historically defined by male samples, if females present with different symptom profiles than males, they may be less likely to be recognized and receive an ASD diagnosis, and therefore less represented in research and less understood (Backer van Ommeren et al., 2017; Pisula et al., 2017). However, this may be changing, as some prospective studies provide evidence of increased female recognition over time. Jensen, Steinhausen and Lauritsen, reviewed the ASD sex ratio trajectory from 1995 to 2010 in the Danish National Registry (2014). They documented a reduction in the male majority from 5:1 to 3:1 over the fifteen years. The ratio shift was due to increases in female diagnosis and not reductions in male diagnosis, likely reflecting a growing recognition that autism presents differently across the sexes. Similarly, the male to female ratio was diminished in other prospective and large-scale population-based studies (Lai, Baron-Cohen, et al., 2015; Lai, Lombardo, et al., 2015; Loomes et al., 2017). The observed increase in females diagnosed with autism in population studies underscores the need for more research into defining a female ASD phenotype to improve understanding and recognition.
Several other hypotheses exist to explain the sex bias in ASD, including those that consider potential intrinsic (e.g. biological and inherent individual factors) differences between males and females that impact ASD symptom recognition and those that consider potential extrinsic factors (e.g. external bias in the diagnosis process or environmental factors). Systematic research considering both intrinsic and extrinsic factors is needed (Halladay et al., 2015; Lai, Baron-Cohen, et al., Lai, Baron-Cohen, et al., 2015; Mandy & Lai, 2017). The sexes could vary either in their presentation of ASD symptoms, or vary in which features are recognized and reported by people involved in the referral and diagnostic process (Dworzynski et al., 2012).
Sex Differences in Intrinsic Qualities and the Impact on Measurement and Diagnosis of ASD
Considering intrinsic qualities of the individual, research to date suggests that the male to female ratio in ASD may vary by age, race, or intelligence (Baio, 2012). For example, the magnitude of the male: female diagnostic ratio is reduced in older samples (Estrin et al., 2020; Rutherford et al., 2016), and in samples with co-occurring conditions (Kreiser & White, 2014), but magnified in samples of individuals with higher intelligence (Lai, Baron-Cohen, et al., 2015; Lai, Lombardo, et al., 2015). However, even within the autism field there is a lack of cohesion. Research focused on elucidating the female ASD phenotype has generated mixed, sometimes conflicting, results across developmental domains; including social, communication, cognitive, behavioral, and motor (Ferri et al., 2018). Harrop et al. (2021) found significant sex differences in parent-reported early developmental milestones, with females meeting their language milestones earlier than males, possibly suggesting less early language impairment in females with ASD. However, these milestones did not predict age of diagnosis or age of parental first concern, so the effects of the sex differences are unclear from their sample. Some studies report that females exhibit an increased number and severity of autism symptoms (Frazier & Hardan, 2017). Conversely, others report less severe autism traits and fewer symptoms in females (Backer van Ommeren et al., 2017; Beggiato et al., 2017). Yet other studies have found no sex differences in autism symptomatology (Frazier & Hardan, 2017; Pisula et al., 2017). Reports also conflict as to the types of ASD co-occurring conditions in females, including increased behavioral problems, mood disorders and intellectual disability in females and inconsistent findings in birth defects and sex chromosome-linked genetic conditions (Angell et al., 2021; Baio, 2012; Dworzynski et al., 2012; Kreiser & White, 2014). Such variability in the literature on sex differences prevents clear direction for clinical practice, and may contribute to later diagnosis of females with ASD or females remaining undiagnosed altogether (Begeer et al., 2013; Rutherford et al., 2016).
Further, studies on ASD sex differences considering race and ethnicity are complex to interpret due to confounding influences of systematic racism, access and availability of quality healthcare especially in the United States (Bishop-Fitzpatrick & Kind, 2017). However, a lower proportion of females was found in Spain when compared to wider European samples (Hidalgo, Moreso & Sans, 2021) and the male: female diagnostic ratio varied by racial subgroups in a population-based UK sample (Roman-Urrestarazu et al., 2021). It is important to consider how these intrinsic factors will impact on an individual’s clinical presentation and may also affect the timing of the diagnostic process.
It is not surprising that specifics of a child’s symptom presentation (e.g., severity of ASD symptoms, presence of developmental delays) effects clinical recognition. Rynkiewicz et al. (2016) employed a computerized measurement of nonverbal autism symptoms in children with ASD and no intellectual disability and found that while females used a greater number of gestures than males on the clinician-scored measure (Autism Diagnostic Observation Schedule-2, ADOS-2; Lord et al., 2012) they were impaired when measured by the computerized measure. The authors hypothesized if females appear less impaired than males within clinical assessments, their relative strengths may lead to a missed or later diagnosis.
Addressing this concern within the diagnostic process, Kaat et al. (2021) investigated sex differences on standardized measures of autism symptoms, including the ADOS-2 (Lord Rutter et al., 2012) and the ADI-R (Rutter et al., 2003b). Standardized measures were divided into domains of social communication and repetitive and restricted behavior (RRB) domains. The authors found the addition of child sex significantly improved the predictive model for half of the standardized measure subdomains, across some social communication domains and all but one of the RRB subdomains. However, while specific methods of measurements had variable findings, overall, sex only had a small effect in early childhood, increasing to a moderate effect size in later childhood, which may suggest that children (both males and females) diagnosed younger (e.g. under 4 years) are more similar in symptom profiles and thus more recognizable by diagnostic measures. The mixed findings, even in domains within the same measure, highlight the complexity of distinguishing sex differences and the need to consider several factors of influence. Earlier studies into sex differences on the ADOS-2 and ADI-R and parent reported measures of autism symptoms have found similarly complex results. In their middle childhood sample, Ratto et al., 2018, found no differences in ADOS-severity scores but did find females to be significantly less likely to meet for ASD criteria on the ADI-R, driven by females with higher intelligence scores. However, they also found higher reported autism symptoms on parent questionnaires and greater impairment on parent reported adaptive functioning for females. One possible interpretation of these findings is that the ADI-R has a focus on early childhood, when females with ASD demonstrate fewer classic ASD impairments, or that greater functional impairment drives the identification and recognition of ASD in females. Therefore, females with ASD may have a greater number of co-occurring conditions that are resulting in more noticeable impairment. An additional possible confound in the diagnostic evaluations is the effect of “camouflaging.” In samples without cognitive impairment or co-conditions, females with ASD may actively suppress their symptoms, or camouflage, during a brief clinical observation at a greater rate than males (Dean et al., 2017; Lai, Baron-Cohen, et al., 2015; Lai, Lombardo, et al., 2015). If some females attempt to camouflage their symptoms of autism, clinical impressions may vary, accounting for a proportion of the variance observed in sex differences (Lai et al., 2017). Lastly, clinicians often observe fewer sex differences than are reported in parent or self-report measures (Ferri et al., 2018). This may be due to actual differences in symptom presentation across environments, or common clinic measures may be unable to capture subtle sex differences in autism symptomatology. Therefore, despite being inherent in the individual, intrinsic factors impact on and interact with the extrinsic factors of measurement and the diagnostic process.
Sex Differences in Extrinsic Factors and the Impact on Measurement and Diagnosis of ASD
As discussed, differences in the presentation of autism symptoms likely effects recognition of autism and the diagnostic process. The process of an ASD diagnosis is usually initiated by parental concerns being raised to a general practitioner (GP), making the parent and GP, as the first point of contact, instrumental for achieving an early diagnosis. This process may become additionally complicated when a family is disadvantaged in their access to appropriate care due to geography (rural/urban), or a family’s social-economic status (SES) (Bishop-Fitzpatrick & Kind, 2017). Further, changes in the conception of the autism presentation within the field may not be communicated to the general public as readily, if at all, leading to an elongated diagnostic process, and possibly a missed diagnosis, especially when a child’s presentation of ASD is less severe (Crane et al., 2016). Children from homes with lower SES received a later ASD diagnosis and had less hours of service, compounding the child’s disadvantages(Durkin et al., 2010; Nguyen et al., 2016). In a survey of 1047 United Kingdom families, 92% did not receive a diagnosis at their first consultation, and half were referred to other providers (Crane et al., 2016). Parental concerns that are more associated with ASD in the understanding of the general public may shorten the diagnostic process. In a survey of families with children with ASD, parent first concerns about eye contact, pointing, response to name and delayed speech predicted early diagnosis regardless if the parent or pediatrician first mentioned autism (Becerra-Culqui et al., 2018). Abnormal babbling was significant when it was a pediatrician who first considered ASD as a diagnosis. The likeliness of an early diagnosis increased with the number of developmental concerns, suggesting children with more delays may be easier to recognize. While sex differences were not explored in these models and female representation was variable, findings suggest that the specifics of parental and pediatrician concerns can impact on the age a child is diagnosed. Therefore, if girls with ASD present a different array of symptoms than may be expected for traditional ASD their diagnostic process will be affected.
Importantly, even in those females that are eventually diagnosed, differences in clinical symptom presentation are known to impact the timing of diagnosis, where those with more subtle or less typical forms of ASD receive later ASD diagnoses and subsequently, have later access to supports and services (Kreiser & White, 2014; Lehnhardt et al., 2013). Studies report delayed age of diagnosis in females relative to males, suggesting that females with autism may be more difficult to identify for diagnosis (Harrop et al., 2021; Rutherford et al., 2016; Van Wijngaarden-Cremers et al., 2014).
Current Study
To address the need for a national, comprehensive exploration into possible sex differences in children and adolescents with ASD, we examined a subset of SPARK participants. SPARK is the largest national autism cohort to date and recruits from all regions of the United States (Feliciano et al., 2018). We examined sex differences in those with ASD under 18 years old in this sample via (1) intrinsic factors, including developmental and medical history determinants and ASD symptom presentation, and (2) extrinsic factors related to the ASD diagnostic process. For this study, variables such as parental first concern are considered “extrinsic” as they reflect the parent’s initial perception of concern (and factors related to the parents’ knowledge) rather than directly addressing an observance of delay (e.g., milestones, co-occurring conditions). We focus on factors highlighted by previous literature on sex differences, including where mixed findings across studies has prevented clear clinical action.
We predicted two pathways exist for sex differences to be detected in those with ASD: external factors (e.g., geographical location, family income, and parental first concern) and intrinsic/biological factors (e.g., developmental milestones, intelligence, comorbid medical conditions, and autism symptom severity) will differ between males and females in this SPARK sample. We also hypothesize that these factors will differentially influence age of ASD diagnosis and timing of diagnosis from parental first concern by child sex. The size of the SPARK cohort allows us to consider multiple child, family, and external factors that could influence ASD diagnosis, with an adequate sample of females to make meaningful comparisons to these factors in males.
Method
Recruitment
Recruitment was conducted for the larger SPARK sample by autism centers in the SPARK consortium and via online outlets, thus providing a geographically diverse sample within the United States. For an overview of recruitment and eligibility for participation in SPARK, see (Feliciano et al., 2018).
Sample
We investigated a subset of the full SPARK sample, defined by the following inclusion criteria: the participant must: (1) have a parent reported ASD diagnosis, (2) be under 18 years old. Inclusion criteria resulted in a possible initial analytic sample of 50,505 children under age 18 years with ASD, including 11,104 (21.99%) females. However, sample size varied by data source (Table 1) and amount of missing data so sample sizes are presented by analysis.
Sample Demographics
The sample was predominately urban (87.1%), with married parents (66.4%), white (77.8%; Table 1: Sample size by Demographics and Questionnaire) and described by parents as functioning below age expectation (76.4%). Of those who provided a cognitive test score (n = 7609), 49.6% reported an IQ score of below 90 for their child.
No sex differences were detected in age of enrollment (months) into the SPARK database (male M = 108.94 [8.713 years], female M = 107.89 [8.63 years], p = 0.078).
Within the SPARK database, parents reported on child sex and gender. In this sample, the concordance for male sex and gender was: 99.5% and the concordance for female sex and gender was: 98.3%. The high rates of concordance may be due to the young age of the sample (< 9 years, see Table 1) or potential parent-report bias on this particular item. Due to the high rates of concordance between sex and gender in this sample, and the focus of SPARK as a genetic study of autism, the variable for “sex” defined by biological sex at birth was used for analysis.
Data Sources
The primary sources of data in this investigation included the Individual Data Questionnaire, a Background and History Questionnaire, a Basic Medical Screening Questionnaire and the Social Communication Questionnaire (SCQ; Chandler et al., 2007), described below. All questionnaire data was parent reported to ensure consistency in measurement across ages (Supporting Information for participant flow and questionnaire concordance). However, sample size varied by amount of completed participant data (Table 1). Sample totals are given for each analysis.
Missing data in SPARK denotes the field was not completed by the family or, on scales where totals were generated (e.g., the SCQ), not enough items were completed to obtain a valid score. Missing data was considered by variable. Those individuals with missing data on a variable were not included in the analysis of that variable. Therefore, sample sizes varied and are presented for each variable.
Diagnostic Validity
Inclusion in SPARK is based on a parent reported diagnosis of autism. Use of parent reported diagnostic status was validated in prior research of large online ASD registries (IAN; Daniels et al., 2012). Specifically, in a subset of the larger registry, parent reported ASD status and SCQ scores corresponded with clinician administered diagnostic assessments (Autism Diagnostic Observation Schedule, ADOS; Lord et al., 2000) and ADOS-2 (Lord et al., 2012) scores and the Autism Diagnostic Interview Revised (ADI-R; Lord et al., 1994) and clinical judgment (Lee et al., 2010).
To examine validity of parent reported diagnosis in the current study, participants were classified based on their score on the SCQ (a measure of ASD symptoms described below) meeting the threshold for ASD (scoring 15 and above; Chandler et al., 2007) and those who did not meet threshold for ASD (scoring below 15). Parent report and elevated SCQ (≥ 15) concurred in 82.2% of females, and 86.3% of males in the SPARK sample (n = 17,487). However, for diligence, a full analysis was conducted comparing the SCQ groups by measure. The only difference to emerge was in the developmental milestone of bladder training, in which the analysis of sex differences became insignificant in those scoring < 15 on the SCQ. As such, bladder training is interpreted with caution and the complete sample of those with parent reported ASD, was used in the main analysis. Therefore, parent reported-ASD diagnosis was accepted for determining ASD status and inclusion in our analysis.
Measures
On enrollment in the SPARK cohort, parents are asked to complete online questionnaires about themselves and their dependents, including their child with autism. Our study considers information from the below questionnaires.
Individual Data Questionnaire
Data regarding individual characteristics was obtained during registration, for example, participant relation to the child with autism, child/dependent language level, information about the referral/diagnosis process, and age of child at ASD diagnosis. Time to diagnosis from parent first concern was calculated from the reported “age of first concern” subtracted from child’s reported “age of diagnosis”. Parent reported child IQ scores were reported by point increments (i.e., below 24, 25–39, 40–54, 55–69, 70–79, 80–89, 90–109, 110–119, and 130 and above), but families were not asked for a single/specific number nor asked which measure their child was administered to estimate IQ. The reported brackets were utilized in analyses and bivariate analyses were conducted based on IQ > = 90 and under 89.
Basic Medical Screening
The Basic Medical Screening form is a parent report of child medical complications and psychiatric conditions (coded present /absent by condition). It includes categories of attention, behavior, birth complications, cognitive impairment, developmental and sleep concerns, mood disorders, neurological conditions, genetic conditions, and results from prior genetic testing.
Social Communication Questionnaire Lifetime
The SCQ (Rutter et al., 2003a) is a 40 item, parent report measure of child behaviors symptomatic of ASD, retrospectively measuring symptoms over the individual’s entire developmental history. It has been validated on a population with autism (Chandler et al., 2007), and to confirm ASD status (Lee et al., 2007). Total scores range from 0–39; higher scores indicated more behaviors. Only the total score was used here. Those missing more than three items were excluded per author recommendations.
Background History Questionnaire
The Background History Questionnaire (child version) is a parent reported survey of demographic characteristics (e.g., race, family income) and developmental history of the individual with ASD. Parent reported age of milestone acquisition was collected for: smiling, sitting, crawling, walking, using words, phrases, complex sentences, bladder training, bowel training, and feeding self with a spoon. Family income was indicated with incremental categories (< $20 K, $21–$35, etc.). To determine urban–rural status for each participant, participant zip codes were linked to the National Center of Health Statistics’ Urban and Rural Classification (NCHS) codes, which provides codes indicating population density (Ingram & Franco, 2014). Developmental history included age of developmental milestone achievement, age of first parental concern, and details of: educational history, regression, intervention, and family history of autism.
Results
Interpretation of Significance
Due to the large sample size in the analysis and best practice, significance of sex differences (p < 0.05 level) is presented with effect size to aid interpretation (Levine & Hullet, 2002). Effect size was calculated using eta squared (η2) and partial eta squared (ηp2) as appropriate, with scores of 0.02 interpreted as small effects, scores of 0.13 interpreted as medium effects and scores of 0.26 interpreted as large effect sizes (Bakeman, 2005; Cohen, 1988).
Intrinsic/Biological factors
Milestones
Sex differences in the ages of milestone acquisition were examined with Multivariate Analysis of Covariance (MANCOVA). To control for possible telescoping effects in the MANCOVA of parent reported milestones, the analyses controlled for child age at enrollment in SPARK (Ozonoff et al., 2018). Results were significant for sex differences in age of early developmental milestone acquisition, F(10, 11,506) = 18.56, p < 0.001, η2 = 0.016 (Results: Table 2). Overall, females were more delayed in motor milestones and males were more delayed on language milestones, though sex differences in mean acquisition age were subtle.
Intelligence
Chi Square analyses of parent reported child intelligence score (N = 7609, male = 6130, female = 1658) indicated no significant differences across the categories of IQ (p = 0.399). However, a binary split of average and below average intelligence scores at 90 (≥ 90 = “high”, ≤ 89 = “low”), following both the clinical definition of average and above IQ and the sample’s frequency data (47.3% = high group, 52.7% = low group) resulted in identification of significantly more females in the low intelligence range (X2(1, N=7609) = 6.44, p = 0.011, η2 = 0.028).
Medical Co-Occurring Conditions
Reports of co-occurring medical conditions varied by sex (N = 43,235, male = 34,167, female = 9,068). Sex differences were observed. A greater percentage of parents of females reported: Neurocognitive disorder, Developmental ID, Motor delay, Depression concerns and Sleep conditions. A greater percentage of parents of males reported: ADHD, Language delay or disorder, Articulation issues and Eating problems. Findings, including nonsignificant results, are summarized in Table 3.
Social Communication Questionnaire (SCQ)
On the Total SCQ score (n = 17,899, male = 14,235, female = 3664), females scores were significantly lower (M = 21.70, SD = 7.36), indicating fewer symptoms than males (M = 22.41, SD = 6.95), (F = (1, 17,897) = 29.945, p < 0.01, η2 = 0.002). This statistically significant difference does not have clinical significance as both groups scored well into the affected range. Using the SCQ total score as a dichotomous variable (using ≥ 15 for ASD categorization), significantly more females with reported ASD diagnosis failed to meet the cut-off (17.8%) as compared to males (13.7%), X2(1, N=17,899) = 40.38, p < 0.001, η2 = 0.047).
Extrinsic Factors
Urban and Rural
For the current analysis, participant zip codes were reduced to two levels corresponding to a “rural” or urban” classification (Monz et al., 2019). Chi-square analysis revealed no significant effect of sex by urban–rural geographic status (n = 50,376, male = 39,914, female = 10,462).
Annual Household Income
Significant sex differences in family income were evident (n = 18,049, males = 14,333, female = 3716), such that more females (15.9%) than males (14.0%) were in the $21,000–35,000 bracket and fewer females (9.7%) than males (11.2%) were in the $66,000–80,000 bracket (X2(1, N=18,049) = 25.00, p = 0.002, η2 = 0.037). While the income variable is unrefined by other demographic variables, it suggests families with females with ASD may be over-represented in lower income brackets and may be over-represented in middle class brackets.
Age of Parent First Concern
No sex difference in the age of first parental concern was observed (n = 18,755, male = 14,953, female = 3802). Overall, the mean age of first concern was 21.74 months (SD = 17.10), or 1.82 years.
First Parental Concern
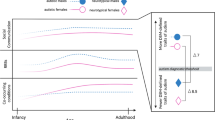
Parent first concern (n = 18,502, male = 14,684, female = 3808) was explored by category of parent response: “late walking”, “mood”, “social”, “repetitive speech”, “something else”, “change or loss” of developmental skill, “late speech” and “repetitive behavior”; Fig. 1. The “change or loss” category captured any developmental regression. Parents of females reported more first concerns than parents of males in the categories of: late walking, mood, social, or something else. Parents of males reported more first concerns than parents of females in the categories of: change or loss, late speech, and repetitive behavior.

First parental concern by child sex. NB Change or loss refers to a change in ability of loss of skill as reported by the parent. Figure of first parental concern by sex
Diagnostic Factors and Impact
Diagnosis Age
Children were excluded if age of diagnosis was < 18 months when the diagnosis may not be reliable (Ozonoff et al., 2015), resulting in a subsample for analysis (n = 18,042, male = 14,334, female = 3,708). Significant sex differences emerged such that males (M = 52.79 months, SD = 31.98) were diagnosed significantly earlier (over 4 months) than females (M = 56.89, SD = 36.42) (F(1,18,040) = 45.63, p < 0.001, η2 = 0.025).
To account for cohort effects and changes in diagnostic practices over time (e.g., shift from DSM fourth to fifth edition), an ANCOVA was conducted controlling for the year of diagnosis. Diagnosis age remained significant, and effect size increased to a medium effect (F(2,47,300) = 5307.10, p < 0.001, η2 = 0.183.
Time to Diagnosis from First Concern
For this analysis, all those with age of diagnosis < 18 months, or with diagnosis age before age of first concern (n = 334) were excluded for data quality. A total sample of 17,605 (male = 13,985, female = 3620) remained. Females (Mage = 35.80, SD = 32.31) have significantly more time elapse between first concern and receiving an ASD diagnosis than did males (over 4 months) but with a small effect size (Mage = 31.66, SD = 28.76; F(1, 17,603) = 56.37, p < 0.001, η2 = 0.003).
Predictors of Age of Diagnosis
To investigate the variables which predict a child’s age at autism diagnosis, a step-wise linear regression model was conducted with selected variables representing both intrinsic and extrinsic variables highlighted from previous literature. Child chronological age was entered as a covariate in step one, followed by child sex and the intrinsic variables of: intelligence and developmental milestones; and extrinsic variables: family income, age of first concern, and child race. The model was significant, [F(14, 1,476) = 53.46, p < 0.001] and predicted 33.7% of the variance (R2 = 0.337). Interestingly, child’s sex was the largest predictor in the model, followed by current age (Table 4). Other significant variables included the intrinsic variables: age of combining phrases, current autism symptoms and intelligence, as well as extrinsic variables, including age of parent’s first concern.
When analyzed independently by sex, the model remained significant for both groups (females: F(13, 316) = 11.36, p < 0.001; and males: F(13,1159) = 48.08, p < 0.001. However, the model predicted 31.8% (R2 = 0.318) and 35.3% (R2 = 0.353) of the variance in the age of diagnosis for females and males, respectively. Predictive variables differed between the sexes. Later age of sitting was predictive of later age of diagnosis in females, but not predictive in males, and, conversely, later age of combining phrases was a significant predictor of earlier age of diagnosis in males but not in females (Table 4).
Predictors of Time Between Parental First Concern and Age of Diagnosis
A step-wise linear regression model was conducted with selected variables representing both intrinsic and extrinsic variables highlighted from previous literature and found to be significant in our analysis. Child chronological age was entered as a covariate in step one, followed by child sex and the intrinsic variables of: intelligence and developmental milestones; and extrinsic variables: family income, age of first concern, and child race. The model was significant, [F(16, 5355) = 83.23, p < 0.001] and predicted 19.7% of the variance (R2 = 0.197) (Table 5).
When analyzed independently by sex, the model remained significant for both groups (females: F(7, 1103) = 56.05, p < 0.001; and males: F(7, 4253) = 131.46, p < 0.001. However, the model predicted 26.2% (R2 = 0.262) and 17.8% (R2 = 0.178) of the variance in the age of diagnosis for females and males, respectively. Predictive variables were similar between the sexes, with chronological age, age of first concern, and age of combing phrases contributing to both models, and age of walking in the female model and annual household income in the male being unique.
Discussion
Despite the longstanding interest to better understand sex differences in autism, findings have been inconsistent and failed to identify specific markers of a female ASD profile. Considering the limitations from previous work, we approached the question of sex differences by considering intrinsic and extrinsic factors in participants from the large, geographically diverse SPARK cohort. This sample affords robust samples of females with ASD. Intrinsic and extrinsic variables, examined together, identify subtle but consistent sex differences.
Sex Differences in Intrinsic Factors
Reported Intelligence, Cognitive Delays, and ID
Differences in intrinsic factors were consistent across multiple variables and questionnaires where parents of females reported lower cognitive test scores (IQ) and more often endorsed cognitive delays and a greater incidence of ID, consistent with other recent findings (Angell et al., 2021; Gabis et al., 2020). While the magnitude of differences was small, the converging evidence across multiple measures of the same construct supports the validity of the findings.
Interestingly, while females on average had lower reported IQ, they had less parent reported autism symptomatology. As a result, clinicians may view females with ASD as having global developmental delays (GDD) rather than noting autism-specific concerns (Gabis et al., 2020). This finding may fit into the larger discussion on sex differences in masking or camouflaging ASD symptoms. Perhaps females generally are better able to camouflage their symptoms independently of cognitive delay (Dworzynski et al., 2012; Estrin et al., 2020; Tierney et al., 2016). In contrast, a meta-analysis of the sex ratio in ASD found it more equal in children with lower intelligence, or Developmental Delay (DD) (Loomes et al., 2017), suggesting females with ASD may be more readily recognized with co-occurring ID, when it is more difficult to camouflage or otherwise mitigate symptom expression (Lai et al., 2017). While intelligence is intrinsic to the child, its implications on symptom presentation may impact on other’s interpretation and recognition of autism symptoms.
Future research should further explore these interpretations, where potential subgroups within IQ and autism symptom presentation could be investigated.
Sex Differences in Extrinsic Factors
Parent Reported First Concerns
Differences in extrinsic factors were also present between males and females with ASD, including the area of parent first concern and the time elapsed from the parent’s first concern to diagnosis and the age of the child at diagnosis.
Parental first concerns were most frequently reported in the language and social domains. However, sex differences emerged within specific developmental domains across measures. Parents of females reported consistent motor concerns, indicating motor delays as a first concern, endorsing more motor delays and indicating greater delays in motor milestones. Likewise, parents of males reported consistent speech and language concerns, indicating speech as their first concern, endorsing more speech concerns, and indicating greater delays in language milestones. It may be that the areas in typical development thought to be strengths for each sex (i.e., motor for males, social/language for females) are more resistant to delay during early development and the comparably weaker areas by sex are more vulnerable to delay (Alexander & Wilcox, 2012).
The different areas of first concern for the sexes also may be relevant to the timing of diagnosis. In our sample, males were more likely to have language delays, a symptom commonly associated with autism in the general public, while females were more likely to have motor delays, a symptom not typically associated with autism specifically (Estrin et al., 2020). Therefore, despite developmental delays being noted in both males and females, concerns specifically for autism may be identified later in females than males (Little et al., 2017). That said, consistent with our findings, recent research has implicated early motor delays as specific to the female ASD phenotype, and suggested that early motor delays should be considered “red flags” for identifying ASD, especially in females (Gabis et al., 2020; Licari et al., 2020). Early motor delays have also been associated with later Restricted and Repetitive Behaviors (RRBs) in children with autism (Uljarevic et al., 2017), but initial research into specific sex profiles suggests the presence and degree of sex differences of RRBs varies by a child’s age and co-occurring conditions (Wodka et al., 2021).
Age of Autism Diagnosis and Time to Diagnosis from Parent First Concern
On average, females were diagnosed four months later than males and sex was the strongest predictor of age of diagnosis. As age of parent first concern did not differ between the sexes, this lag in female diagnosis may reflect delay in the clinical process or family demographics and not from delayed onset of symptoms in females. For example, females with ASD are more likely to be in lower income homes and barriers associated with financial strain may delay the diagnostic assessment process. While small, a four-month delay in diagnosis could impact access to services and early supports during a formative period of child development. Oftentimes, an autism diagnosis may be the only way a family can afford intensive intervention services. Additionally, females are more likely to have cognitive delays, intensifying their need for developmental supports, and the delay of access to intervention could be compounded.
Finally, the factors that predict age of diagnosis and the time between first concern and diagnosis vary between the sexes. While both sexes’ age of diagnosis is significantly predicted by child intelligence and age of parent’s first concern, the specific predictive milestones vary. Following the larger data trend, males’ age of diagnosis was significantly predicted by a language milestone, the age of combining phrases, and females’ age of diagnosis was predicted by a motor milestone, age of sitting. However, more delayed age of sitting in females predicted a later age of ASD diagnosis, while more delayed combining phrases in males predicted earlier ASD diagnosis. Combined with greater cognitive delays, this further suggests that ASD in females may be mistaken for GDD early in development (Dworzynski et al., 2012) or that a female having generalized (e.g., ID) or other specific delays may prompt the initial developmental referral, rather than ASD symptoms alone. An additional factor to consider is the timing of the milestones that predicts a child’s age of diagnosis. Typically, a child can sit independently between 6–8 months, but most do not produce phrase speech until 18–24 months, a time when parents and clinicians are more likely to be considering ASD as a possible explanation for their child’s behavior or delays (Scharf et al., 2016). Therefore, there may be an influence of the developmental timing as well as domain class that predicts when a child is diagnosed with ASD.
Predicting the time between parental first concern and diagnosis is more problematic. Many factors were significant predictors, but only accounted for about 20% of the variance in the sample, implying many more factors of influence are acting. When considered by sex, many factors were the same, with the exception of age of walking in the females, and annual household income in the males. While this may suggest high incomes can streamline the diagnostic process for males (possibly through private insurance and other related factors), the largeness of the unaccounted for variance limits any interpretation.
Limitations
The current report is an important step in identifying sex differences in the intrinsic and extrinsic factors related to timing of autism diagnosis. However, there are limitations. Data were collected within the larger SPARK study, and therefore some variables had large amounts of missing, or incomplete data (> 50% for the IQ report), although the sample remained sufficient for valid analysis. In analyses with notable missing data, findings are interpreted with caution, and we emphasize the need for other reports to validate our findings. Specifically, as IQ was problematic in this regard, further analysis of intelligence in sex differences could be illustrative.
Secondly, our sample is limited to only those diagnosed with autism previously. As some of the sex differences observed in the sample could impact on diagnostic recognition, it is possible there are females with autism that are not diagnosed and therefore excluded from the sample. Our cross-sectional sample cannot address this question, but we feel our large, national sample which also includes individuals through the age of 18 years (providing ample time for ASD identification, including females who may receive a diagnosis later than males), still provides valuable insights into sex differences to inform further research that can address this limitation more fully.
Further, no self-report data was considered. The decision to exclude those over age 18 years maintained continuity in the data sources (all parent report). However, this decision removed the perspective of first-person reporting of those with autism. It additionally removed those diagnosed in adulthood, who may have a less traditional expression of autism and therefore were more difficult to recognize, and it removes anyone diagnosed over 16.5 years ago, which limits any interpretation of changing diagnosis practice from this analysis. A follow up analysis including older ages of participants and self-report data could further expand our findings.
Finally, the data analyzed only contained parent report data. It is possible that some of the sex differences observed reflect a bias in parent reporting rather than actual differences that may be measured in direct observation. For example, reported autism symptoms are measured by the SCQ, reflecting the parents’ perceptions, but sex-specific expectations could influence their observations and interpretations of their child’s behavior. While we controlled for the effect of time (telescoping), to account for recall differences in parent reporting, testing for sex specific assumptions was not possible. Additionally, with only parent report, we cannot determine if the delay in female diagnosis is due to parents’ delay in seeking services, a clinical delay in providing the diagnosis, or a delay elsewhere in the process. Further investigation with multiple reporting sources may elucidate factors pertaining to the influence of sex in diagnostic practices. Addressing some limitations, future analysis could consider cohorts less variable in IQ and age, among other factors. Timing of development may be important in assessing autism, so a prospective longitudinal study of autism symptoms would be informative. It is possible that specific subgroups within the sample may show larger effects, unique associations, or other sex-specific differences. Finally, future studies could consider how the experience of the diagnostic process varies by sex for the child or adolescent with autism.
Conclusion
This study provides an important investigation into two components which impact on sex differences in autism: the extrinsic factors of the diagnosis process and intrinsic factors of the child. Evidence for both was found; with small but consistent differences emerging across domains where language concerns in males may make discernment of ASD more straightforward, while early motor concerns in females may hinder diagnosis as such delays are not identified within traditional ASD diagnostic criteria. We hope to have set the stage for future, more in-depth investigations of subgroups, and possibly investigations of sex differences in adults with ASD.
References
Alexander, G. M., & Wilcox, T. (2012). Sex differences in early infancy. Child Development Perspectives, 6(4), 400–406. https://doi.org/10.1111/j.1750-8606.2012.00247.x
American Psychiatric Association. (2013). DSM-5 diagnostic classification. Diagnostic and Statistical Manual of Mental Disorders. https://doi.org/10.1176/appi.books.9780890425596.x00diagnosticclassification
Angell, A. M., Deavenport-Saman, A., Yin, L., Zou, B., Bai, C., Varma, D., & Solomon, O. (2021). Sex differences in co-occurring conditions among autistic children and youth in Florida: A retrospective cohort study (2012–2019). Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s10803-020-04841-5
Backer van Ommeren, T., Koot, H. M., Scheeren, A. M., & Begeer, S. (2017). Sex differences in the reciprocal behaviour of children with autism. Autism, 21(6), 795–803. https://doi.org/10.1177/1362361316669622
Baio, J. (2012). Prevalence of autism spectrum disorders: Autism and developmental disabilities monitoring network, 14 sites, United States, 2008. Autism Spectrum Disorders: Guidance, Research and Federal Activity, 61(3), 1–19.
Bakeman, R. (2005). Reccomended effect size statistics for repeated measures design. Behavioral Research Methods, 37(3), 379–384. https://doi.org/10.3758/BF03192707
Becerra-Culqui, T. A., Lynch, F. L., Owen-Smith, A. A., Spitzer, J., & Croen, L. A. (2018). Parental first concerns and timing of autism spectrum disorder diagnosis. Journal of Autism and Developmental Disorders, 48(10), 3367–3376. https://doi.org/10.1007/s10803-018-3598-6
Begeer, S., Mandell, D., Wijnker-Holmes, B., Venderbosch, S., Rem, D., Stekelenburg, F., & Koot, H. M. (2013). Sex differences in the timing of identification among children and adults with autism spectrum disorders. Journal of Autism and Developmental Disorders, 43, 1151–1156. https://doi.org/10.1007/s10803-012-1656-z
Beggiato, A., Peyre, H., Maruani, A., Scheid, I., Rastam, M., Amsellem, F., Gillberg, C. I., Leboyer, M., Bourgeron, T., Gillberg, C., & Delorme, R. (2017). Gender differences in autism spectrum disorders Divergence among specific core symptoms. Autism Research, 1014, 680–689. https://doi.org/10.1002/aur.1715
Bishop-Fitzpatrick, L., & Kind, A. J. (2017). A scoping review of health disparities in autism spectrum disorder. Journal of Autism and Developmental Disorders, 47(11), 3380–3391. https://doi.org/10.1007/s10803-017-3251-9
Chandler, S., Charman, T., Baird, G., Simonoff, E., Loucas, T., Meldrum, D., Scott, M., & Pickles, A. (2007). Validation of the Social Communication Questionnaire in a population cohort of children with autism spectrum disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 46(10), 1324–1332. https://doi.org/10.1097/chi.0b013e31812f7d8d
Cohen, J. (1988). Statistical Power of Analysis for the Behavioral Sciences (2nd Edition). Erlbaum.
Crane, L., Chester, J. W., Goddard, L., Henry, L. A., & Hill, E. (2016). Experiences of autism diagnosis: A survey of over 1000 parents in the United Kingdom. Autism, 20(2), 153–162. https://doi.org/10.1177/1362361315573636
Daniels, A. M., Rosenberg, R. E., Anderson, C., Law, J. K., Marvin, A. R., & Law, P. A. (2012). Verification of parent-report of child autism spectrum disorder diagnosis to a web-based autism registry. Journal of Autism and Developmental Disorders, 42, 257–265. https://doi.org/10.1007/s10803-011-1236-7
Dean, M., Harwood, R., & Kasari, C. (2017). The art of camouflage: Gender differences in the social behaviors of girls and boys with autism spectrum disorder. Autism, 21(6), 678–689. https://doi.org/10.1177/1362361316671845
Durkin, M. S., Maenner, M. J., Meaney, F. J., Levy, S. E., DiGuiseppi, C., Nicholas, J. S., Kirby, R. S., Pinto-Martin, J. A., & Schieve, L. A. (2010). Socioeconomic inequality in the prevalence of autism spectrum disorder: evidence from a US cross-sectional study. PLoS ONE, 5(7), e11551.
Dworzynski, K., Ronald, A., Bolton, P., & Happé, F. (2012). How different are girls and boys above and below the diagnostic threshold for autism spectrum disorders? Journal of the American Academy of Child and Adolescent Psychiatry, 51(8), 788–797. https://doi.org/10.1016/j.jaac.2012.05.018
Estrin, G. L., Milner, V., Spain, D., Happé, F., & Colvert, E. (2020). Barriers to autism spectrum disorder diagnosis for young women and girls: A systematic review. Review Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s40489-020-00225-8
Feliciano, P., Daniels, A. M., Green Snyder, L. A., Beaumont, A., Camba, A., Esler, A., Gulsrud, A. G., Mason, A., Gutierrez, A., Nicholson, A., Paolicelli, A. M., McKenzie, A. P., Rachubinski, A. L., Stephens, A. N., Simon, A. R., Stedman, A., Shocklee, A. D., Swanson, A., Finucane, B., & Chung, W. K. (2018). SPARK: A US Cohort of 50,000 families to accelerate autism research. Neuron, 89(3), 488–493. https://doi.org/10.1016/j.neuron.2018.01.015
Ferri, S. L., Abel, T., & Brodkin, E. S. (2018). Sex differences in autism spectrum disorder: a review. Current Psychiatry Reports. https://doi.org/10.1007/s11920-018-0874-2
Frazier, T. W., & Hardan, A. Y. (2017). Equivalence of symptom dimensions in females and males with autism. Autism, 21(6), 749–759. https://doi.org/10.1177/1362361316660066
Gabis, L. V., Attia, O. L., Roth-Hanania, R., & Foss-Feig, J. (2020). Motor delay- An Early and more common “red flag” in girls rather than boys with autism spectrum disorder. Research in Developmental Disabilities. https://doi.org/10.1016/j.ridd.2020.103702
Halladay, A. K., Bishop, S., Constantino, J. N., Daniels, A. M., Koenig, K., Palmer, K., Messinger, D., Pelphrey, K., Sanders, S. J., Singer, A. T., Taylor, J. L., & Szatmari, P. (2015). Sex and gender differences in autism spectrum disorder: Summarizing evidence gaps and identifying emerging areas of priority. Molecular Autism. https://doi.org/10.1186/s13229-015-0019-y
Harrop, C., Libsack, E., Bernier, R., Dapretto, M., Jack, A., McPartland, J. C., Van Horn, J.D., Webb, S.J., Pelphrey, K., & GENDAAR Consortium. (2021). Do Biological Sex and Early Developmental Milestones Predict the Age of First Concerns and Eventual Diagnosis in Autism Spectrum Disorder? Autism Research, 14(1), 156–168.
Ingram, D. D., & Franco, S. J. (2014). 2013 NCHS urban-rural classification scheme for counties. Vital and Health Statistics, Series 2: Data Evaluation and Methods Research.
Jensen, C. M., Steinhausen, H. C., & Lauritsen, M. B. (2014). Time trends over 16 years in incidence-rates of autism spectrum disorders across the lifespan based on nationwide Danish register data. Journal of Autism and Developmental Disorders, 44, 1808–1818. https://doi.org/10.1007/s10803-014-2053-6
Kaat, A. J., Shui, A. M., Ghods, S. S., Farmer, C. A., Esler, A. N., Thurm, A., & Georgiades, S. (2021). Sex differences in scores on standardized measaures of autism symptoms: A Multisite integrative data analysis. The Journal of Child Psychology and Psychiatry, 62(1), 97–106. https://doi.org/10.1111/jcpp.13242
Kreiser, N. L., & White, S. W. (2014). ASD in females: are we overstating the gender difference in diagnosis? Clinical Child and Family Psychology Review, 17, 67–84. https://doi.org/10.1007/s10567-013-0148-9
Lai, M. C., Baron-Cohen, S., & Buxbaum, J. D. (2015). Understanding autism in the light of sex/gender. Molecular Autism. https://doi.org/10.1186/s13229-015-0021-4
Lai, M. C., Lombardo, M. V., Auyeung, B., Chakrabarti, B., & Baron-Cohen, S. (2015). Sex/gender differences and autism: setting the scene for future research. Journal of the American Academy of Child and Adolescent Psychiatry, 54(1), 11–24. https://doi.org/10.1016/j.jaac.2014.10.003
Lai, M. C., Lombardo, M. V., Ruigrok, A. N. V., Chakrabarti, B., Auyeung, B., Szatmari, P., Happé, F., & Baron-Cohen, S. (2017). Quantifying and exploring camouflaging in men and women with autism. Autism, 21(6), 690–702. https://doi.org/10.1177/1362361316671012
Lee, L. C., David, A. B., Rusyniak, J., Landa, R., & Newschaffer, C. J. (2007). Performance of the social communication questionnaire in children receiving preschool special education services. Research in Autism Spectrum Disorders, 1(2), 126–138. https://doi.org/10.1016/j.rasd.2006.08.004
Lee, H., Marvin, A. R., Watson, T., Piggot, J., Law, J. K., Law, P. A., Constantino, J. N., & Nelson, S. F. (2010). Accuracy of phenotyping of autistic children based on internet implemented parent report. American Journal of Medical Genetics, Part b: Neuropsychiatric Genetics, 153B(6), 1119–1126. https://doi.org/10.1002/ajmg.b.31103
Lehnhardt, F.-G., Gawronski, A., Pfeiffer, K., Kockler, H., Schilbach, L., & Vogeley, K. (2013). The investigation and differential diagnosis of asperger syndrome in adults. Deutsches Aerzteblatt Online., 110(45), 755–763. https://doi.org/10.3238/arztebl.2013.0755
Levine, T. R., & Hullett, C. R. (2002). Eta squared, partial eta squared, and misreporting of effect size in communication research. Human Communication Research, 28(4), 612–625.
Licari, M. K., Alvares, G. A., Varcin, K., Evans, K. L., Cleary, D., Reid, S. L., & Whitehouse, A. J. (2020). Prevalence of motor difficulties in autism spectrum disorder: Analysis of a population-based cohort. Autism Research, 13(2), 298–306. https://doi.org/10.1002/aur.2230
Little, L. M., Wallisch, A., Salley, B., & Jamison, R. (2017). Do early caregiver concerns differ for girls with autism spectrum disorders? Autism, 21(6), 728–732. https://doi.org/10.1177/1362361316664188
Loomes, R., Hull, L., & Mandy, W. P. L. (2017). What is the male-to-female ratio in autism spectrum disorder? A systematic review and Meta-analysis. Journal of the American Academy of Child and Adolescent Psychiatry, 56(6), 466–474. https://doi.org/10.1016/j.jaac.2017.03.013
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24, 659–685. https://doi.org/10.1007/BF02172145
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Leventhal, B. L., Dilavore, P. C., Pickles, A., & Rutter, M. (2000). The Autism Diagnostic Observation Schedule-Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30, 205–223. https://doi.org/10.1023/A:1005592401947
Lord, C., Rutter, M., DiLavore, P., Risi, S., Gotham, K., & Bishop, S. (2012). Autism Diagnostic Observation Schedule, (ADOS-2) Modules 1–4. Western Psychology Publishing.
Mandy, W., & Lai, M. C. (2017). Towards sex- and gender-informed autism research. Autism, 21(6), 643–645. https://doi.org/10.1177/1362361317706904
Monz, B. U., Houghton, R., Law, K., & Loss, G. (2019). Treatment patterns in children with autism in the United States. Autism Research, 12(3), 517–526. https://doi.org/10.1002/aur.2070
Nguyen, C. T., Krakowiak, P., Hansen, R., Hertz-Picciotto, I., & Angkustsiri, K. (2016). Sociodemographic disparities in intervention service utilization in families of children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 46(12), 3729–3738.
Ozonoff, S., Young, G. S., Landa, R. J., Brian, J., Bryson, S., Charman, T., Chawarska, K., Macari, S. L., Messinger, D., Stone, W. L., Zwaigenbaum, L., & Iosif, A. M. (2015). Diagnostic stability in young children at risk for autism spectrum disorder: A baby siblings research consortium study. Journal of Child Psychology and Psychiatry, 56(9), 988–998. https://doi.org/10.1111/jcpp.12421
Ozonoff, S., Li, D., Deprey, L., Hanzel, E. P., & Iosif, A. M. (2018). Reliability of parent recall of symptom onset and timing in autism spectrum disorder. Autism, 22(7), 891–896. https://doi.org/10.1177/1362361317710798
Pisula, E., Pudło, M., Słowińska, M., Kawa, R., Strząska, M., Banasiak, A., & Wolańczyk, T. (2017). Behavioral and emotional problems in high-functioning girls and boys with autism spectrum disorders: Parents’ reports and adolescents’ self-reports. Autism, 21(6), 738–748. https://doi.org/10.1177/1362361316675119
Ratto, A. B., Kenworthy, L., Yerys, B. E., Bascom, J., Wieckowski, A. T., White, S. W., & Anthony, L. G. (2018). What about the girls? Sex-based differences in autistic traits and adaptive skills. Journal of Autism and Developmental Disorders, 48(5), 1698–1711. https://doi.org/10.1007/s10803-017-3413-9
Roman-Urrestarazu, A., van Kessel, R., Allison, C., Matthews, F. E., Brayne, C., & Baron-Cohen, S. (2021). Association of race/ethnicity and social disadvantage with autism prevalence in 7 million school children in England. JAMA Pediatrics, 175, 210–2100.
Rutherford, M., McKenzie, K., Johnson, T., Catchpole, C., O’Hare, A., McClure, I., Forsyth, K., McCartney, D., & Murray, A. (2016). Gender ratio in a clinical population sample, age of diagnosis and duration of assessment in children and adults with autism spectrum disorder. Autism, 20(5), 628–634. https://doi.org/10.1177/1362361315617879
Rutter, M., Le Couteur, A., & Lord, C. (2003a). Autism Diagnostic Interview-Revised (ADI-R). Los Angeles: Western Psychological Services.
Rutter Bailey, A., Lord, C., & M. (2003b). Manual of the Social Communication Questionnaire. Western Psychology Publishing.
Rynkiewicz, A., Schuller, B., Marchi, E., Piana, S., Camurri, A., Lassalle, A., & Baron-Cohen, S. (2016). An investigation of the “female camouflage effect” in autism using a computerized ADOS-2 and a test of sex/gender differences. Molecular Autism. https://doi.org/10.1186/s13229-016-0073-0
Scharf, R. J., Scharf, G. J., & Stroustrup, A. (2016). Developmental milestones. Pediatrics in Review. https://doi.org/10.1542/pir.2014-0103
Tierney, S., Burns, J., & Kilbey, E. (2016). Looking behind the mask: Social coping strategies of girls on the autistic spectrum. Research in Autism Spectrum Disorders, 23, 73–83. https://doi.org/10.1016/j.rasd.2015.11.013
Uljarević, M., Hedley, D., Alvares, G. A., Varcin, K. J., & Whitehouse, A. J. (2017). Relationship between early motor milestones and severity of restricted and repetitive behaviors in children and adolescents with autism spectrum disorder. Autism Research, 10(6), 1163–1168. https://doi.org/10.1002/aur.1763
Van Wijngaarden-Cremers, P. J. M., Van Eeten, E., Groen, W. B., Van Deurzen, P. A., Oosterling, I. J., & Van Der Gaag, R. J. (2014). Gender and age differences in the core triad of impairments in autism spectrum disorders: A systematic review and meta-analysis. Journal of Autism and Developmental Disorders, 44, 627–635. https://doi.org/10.1007/s10803-013-1913-9
Wodka, E. L., Parish-Morris, J., Annett, R. D., Carpenter, L., Dillon, E., Michaelson, J., Kim, S.H., Landa, R.J., the Spark Consortium & Kanne, S. (2021). Co-occurring attention-deficit/hyperactivity disorder and anxiety disorders differentially affect males and females with autism. The Clinical Neuropsychologist. https://doi.org/10.1080/13854046.2021.1942554
Acknowledgements
We gratefully acknowledge the families who participated in SPARK and the aid and support of the Simon’s Foundation. We have no other contributors to mention here, nor any funding to report.
Funding
Funding for the Senior Author: SPARK: Simons Foundation Powering Autism Research for Knowledge, Simons Foundation (SPARK #534041, ELW).
Author information
Authors and Affiliations
Consortia
Contributions
All authors contributed to the study conception and design. Material preparation and secondary data analysis were performed by EW and ED. The first draft of the manuscript was written by ED and EW; SK and RL provided input into data analyses and editing initial drafts. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest or completing interest.
Ethical Approval
The study was completed within the Ethical Guidelines of the institutions. Further questions regarding declarations may be directed to the corresponding author.
Informed Consent
Informed consent was obtained from legal guardians of all participants in the SPARK database.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dillon, E.F., Kanne, S., Landa, R.J. et al. Sex Differences in Autism: Examining Intrinsic and Extrinsic Factors in Children and Adolescents Enrolled in a National ASD Cohort. J Autism Dev Disord 53, 1305–1318 (2023). https://doi.org/10.1007/s10803-021-05385-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-021-05385-y