
Abstract
This study compared cognitive behavioral therapy (CBT) and treatment-as-usual (TAU) in terms of effects on observed social communication-related autism symptom severity during unstructured play time at school for children with autism spectrum disorders (ASD). Thirteen children with ASD (7–11 years old) were randomly assigned to 32 sessions of CBT or community-based psychosocial treatment (TAU) for 16 weeks. The CBT program is based on the memory retrieval competition model and emphasizes the development of perspective-taking through guided behavioral experimentation supplemented with reflective Socratic discussion and supported by parent training and school consultation to promote generalization of social communication and emotion regulation skills. Trained observers blind to treatment condition observed each child during recess on two separate days at baseline and again at posttreatment, using a structured behavioral observation system that generates frequency scores for observed social communication-related autism symptoms. CBT outperformed TAU at posttreatment on the frequency of self-isolation, the proportion of time spent with peers, the frequency of positive or appropriate interaction with peers, and the frequency of positive or appropriate peer responses to the target child (d effect size range 1.34–1.62). On average, children in CBT were engaged in positive or appropriate social interaction with peers in 68.6 % of observed intervals at posttreatment, compared to 25 % of intervals for children in TAU. Further investigation of this intervention modality with larger samples and follow-up assessments is warranted.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Affecting core autism symptoms through psychosocial treatment has been an elusive goal in the autism literature, particularly for school-age children. Most psychosocial interventions that have been tested in randomized, controlled trials have failed to yield measureable improvement in core autism symptoms among school-aged children (Rao et al. 2008), although recent interventions are beginning to show more promise (e.g., Kasari et al. 2012). The severity of autism spectrum symptoms exhibited during childhood predicts the level of adaptive functioning in later years (e.g., Szatmari et al. 2009), and therefore has important prognostic and treatment implications. Developing treatments that can significantly reduce core autism symptom severity in children is thus a high priority (Spence and Thurm 2010).
Core autism symptoms are wide-ranging and multifaceted, spanning from impaired reciprocal communication and pragmatic language deficits, to limited friendships, to repetitive behaviors such as insistence on nonfunctional routines. The core symptoms tend to be stable over time (Matson and Horovitz 2010; Matson et al. 2010) and resistant even to some intensive interventions (e.g., Dawson et al. 2010). The majority of individuals diagnosed with autism spectrum disorders (ASD) in childhood, even those with high intelligence, have substantial morbidity in adulthood, such as limited employment and social networks (Eaves and Ho 2008; Marriage et al. 2009). However, individuals on the autism spectrum who have categorically lower levels of ASD symptoms have better overall prognoses than those with categorically higher levels of core autism symptoms. For example, Szatmari et al. (2009) found that although all children with ASD demonstrated mixed to poor outcomes, those with Asperger’s disorder as opposed to autistic disorder had relatively better outcomes in adult social relationships and daily living skills. In fact, across the three domains of adaptive functioning in a standardized assessment scale administered during young adulthood, the group difference between Asperger’s disorder and autistic disorder was 20 standard points, even after controlling for IQ. It is likely that interventions for children with ASD will need to substantially reduce the severity of core autism symptoms to improve children’s prognosis and later functioning. A fundamental goal in the field of autism research is the discovery of methods that substantially mitigate the primary symptoms of ASD (e.g., Reichow and Wolery 2009; Spence and Thurm 2010).
While behavioral and talk-based therapies are widely used in community settings for school-aged youth with ASD (Hess et al. 2008), the evidence base for many such treatments is sparse. With the exception of atypical antipsychotic medication, no medical or psychosocial treatments for children with ASD meet American Psychological Association Division 12 (e.g., Chambless and Hollon 1998) guidelines for possible efficacy, and even antipsychotic medication has not yielded improvement in the social communication domain per se. School-aged children with high-functioning ASD have evidenced poor treatment response, in terms of generalization and maintenance, to many extant psychosocial interventions. Many treatments for the elementary school-age-group involve group-based social skills training, but external validity and durability of effects have been poor and efficacy has not been established (e.g., Ferraioli and Harris 2011; Rao et al. 2008). Nonetheless, some promising findings have recently emerged. A social skills group treatment for the 8–12 years old age-group-based on CBT and social learning principles involving parents as social coaches in community settings to address generalization problems found an effect of treatment (vs. waitlist) on parent-reported core autism symptoms (DeRosier et al. 2011). Without independent ratings of outcome, however, the efficacy of this and similar programs remains to be further evaluated.
Second, a promising peer-mediated intervention for school-age children with ASD has also recently been evaluated in a randomized controlled trial, with evidence of greater improvement in observed social engagement with peers on the playground in comparison to a traditional social skill intervention and waiting list conditions (Kasari et al. 2012). Given the use of both independent ratings of outcome as well as the use of an active control group, peer-mediated intervention appears promising. However, many other studies have reported a failure of generalization effects outside of the therapy room for psychosocial and medical interventions for core autism symptoms (McDougle et al. 2005; West et al. 2009).
Cognitive behavioral therapy (CBT) offers one approach that is potentially well-suited to addressing core autism symptoms in higher functioning school-age youth. CBT is among the most successful treatment modalities for many childhood psychiatric disorders, achieving large, clinically significant outcomes in pediatric OCD, anxiety, and disruptive behavior disorders, even in studies with active or placebo control groups. CBT has already been effectively adapted to treat collateral behavioral and emotional problems in school-aged children with ASD (Chalfant et al. 2007; Fujii et al. 2013; Reaven et al. 2012; Sofronoff et al. 2007; Storch et al. 2013; Wood et al. 2009a, b). Children with high-functioning ASD are verbal and have average to above average intellectual abilities (e.g., Loveland and Tunali-Kotoski 2005). Lickel et al. (2012) investigated whether children with high-functioning ASD would have prerequisite skills that might impact receptivity to CBT (e.g., ability to discriminate between thoughts, feelings, and behavior) and generally found no differences in comparison to typically developing children except in the area of emotion discrimination, suggesting no inherent barrier to children’s comprehension of CBT concepts.
A number of CBT-based interventions for core autism symptoms in youth await comprehensive empirical evaluation (see, e.g., Wood et al. 2011). In a randomized, controlled trial of personalized CBT for elementary-aged youth with ASD, 19 children with ASD and concurrent anxiety (ages 7–11 years) were randomized to CBT delivered one-on-one by a therapist, or to a waitlist (Wood et al. 2009b). The modular CBT program consisted of 16 weekly, 90 min sessions emphasizing emotion awareness and regulation, development of theory-of-mind skills, and control of repetitive behaviors. The treatment approach involved an application of cognitive behavioral principles of memory retrieval competition (Brewin 2006) to CBT techniques such as Socratic discussions, rehearsal, and in vivo exposure, which were employed to address each child’s unique constellation of autism symptoms and emotional and behavioral difficulties. There was a statistically significant difference between the CBT group and the waitlist group at posttreatment/postwaitlist on total parent-reported autism symptoms (d = .77), with gains maintained at 3-month follow-up. These findings were then replicated by an independent research group in a sample of 45 children aged 7–11 years randomized to the same personalized CBT program or TAU (Storch et al. 2013). The present study builds from these initial findings.
Contemporary CBT methods explicitly promote the development of mental schemata that guide adaptive appraisals and behavior while suppressing previously learned maladaptive responses (Brewin 2006). Brewin’s model identifies three key strategies for enhancing the retention of adaptive appraisals and behavioral responses and the concurrent suppression of maladaptive appraisals and responses: (1) Patients need to engage in activities that promote deep semantic processing in the context of learning and rehearsing adaptive thoughts and behaviors (as opposed to passive listening) (cf. Anderson et al. 1994). (2) Adaptive appraisals and responses should be practiced in settings, and under conditions, that cue maladaptive appraisals and responses (the encoding specificity principle; Craske et al. 2008; Tulving 1979). (3) There should be positive and reinforcing features associated with memories of adaptive appraisals and responses. A memory with a positive valence is likely to suppress competing memories of appraisals and behavioral responses at recall (Anderson et al. 2000). These three principles of memory retrieval competition have important implications for the implementation of CBT for core autism symptoms (Wood and Schwartzman 2013).
Three core ASD symptoms involve failure to maintain age-appropriate peer relationships, impaired social/emotional reciprocity, and a deficit in sustaining conversations. To remediate conversational and perspective-taking deficits, a memory retrieval competition perspective suggests that skill rehearsal should occur in the actual settings where social deficits are exhibited (e.g., school playground; playdates), rather than in simulated social situations. This perspective also points towards achieving integration of skill-building behavioral tasks (e.g., initiating play with an unknown peer at the park) with guided Socratic discussions held right after the skill rehearsal has occurred to promote deep semantic processing of heretofore abstract or confusing concepts about others’ perspectives and the nature of reciprocity. While therapists are limited in the amount of time they can promote children’s skills in real-world settings, parents and school caregivers can be taught these techniques, once they have been established by the therapist, to extend intervention support to a wide range of relevant real-world situations. There is clear evidence for the value of parent involvement in CBT for children with ASD symptoms (e.g., Puleo and Kendall 2011; Sofronoff et al. 2005).
In summary, the present study goes beyond previous efforts by (1) targeting multiple core autism symptoms within the same treatment model, many of which are unlikely to remit without corresponding improvement in complementary domains (e.g., social engagement and emotion dysregulation, in which the latter tends to impede the former); (2) focusing outcome assessment on a key real-world setting, school, to assess for generalization; and (3) employing a cognitive behavioral model of memory retrieval to enhance treatment efficacy. The original CBT treatment model (Wood et al. 2009a, b) was doubled in length to promote substantial clinical gains in core autism symptoms. Of equal import, an independent evaluator (IE)-administered measure (structured observations of ASD symptoms during school recess) was employed in this study. Measures using IEs blind to treatment condition are considered to be a gold standard for assessing treatment outcome because they mitigate response bias that can interfere with interpretations of checklist measures (e.g., Chambless and Hollon 1998).
Method
Participants
The sample included 13 children, ranging in age from 7 to 11 years (M = 8.77, SD = 1.59), and their primary parent(s), living in the greater Los Angeles area. Children were referred by a medical center-based autism clinic, regional centers, parent support groups, and school personnel such as inclusion specialists and school psychologists. Children met research criteria for ASD and comorbid anxiety, and were part of a study examining the efficacy of an enhanced CBT program for anxiety and social challenges in children with high-functioning autism; details regarding the anxiety-specific outcomes of the children in this study have been previously reported (see Fujii et al. 2013). In contrast, the present paper documents the impact of the intervention on children’s observed social communication-related autism symptom severity, and no outcome measures are shared in common between the two papers. Eligibility criteria included having a clinical diagnosis of ASD confirmed by our research evaluation (see below), an IQ above 70 based on the KBIT-2 (see below), no concurrent psychotic episodes or physical disabilities that would prevent participation in study activities, and an agreement to adhere to restrictions on concurrent treatments during the study: (1) A stable dosage of psychiatric medication, if used at all, was to be maintained for at least 1 month prior to intake and throughout the duration of the trial for all children in the CBT condition; (2) children in the CBT condition were not to receive any concurrent psychotherapy but were permitted to maintain the use of school counseling or other school services such as an aide, speech therapy, occupational therapy, social skills groups that did not assign regular homework, or up to an hour of applied behavior analysis in the home per week [children with ASD often receive many concurrent services of unknown or questionable efficacy (Hess et al. 2008), and it was deemed potentially unethical to require that non-psychotherapy complementary services that had been ongoing and were unlikely to affect study outcomes be dropped simultaneously]. Children in the treatment-as-usual (TAU) condition were allowed to maintain or seek any intervention (and were given community mental health referrals for anxiety treatment) including altering their medication regimen during a 16-week period.
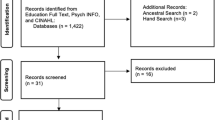
Twenty-two children were assessed for inclusion in the study. Three families did not complete the intake assessment, two families were excluded because the child’s primary mental health diagnosis (other than ASD) was not an anxiety disorder, and one family was excluded because the minimum verbal IQ criterion was not met. Sixteen participants completed the intake assessment and were randomized for inclusion in the study. Three participants within the CBT condition did not complete treatment or their posttreatment assessments due to the family’s inability to consistently attend treatment sessions.
Of the 13 participants included in this study, seven were randomized to the CBT condition and six were randomized to the TAU condition. In contrast to the Fujii et al. (2013) study, one additional participant (in the TAU condition) was included in the present analyses because this child had valid posttreatment observational data, but did not have posttreatment anxiety data available. Table 1 presents descriptive information for participating families. Most children were boys and most primary parents had a college degree. Ethnic/racial groups included Caucasian (n = 9; 69.2 %); Asian (n = 1; 7.7 %); African American (n = 1; 7.7 %); Latino (n = 1; 7.7 %); and mixed race (n = 1; 7.7 %). Groups did not differ significantly on these variables. Seven of the participants were fully included in general education classrooms in regular schools. Three of the participants were fully included in general education classrooms in regular schools with paraprofessional aides. One participant was partially included in a general education classroom in a regular school, and spent part time in a resource room. One participant was in a special day class at a regular school and one participant attended an autism-specific school.
All participants met criteria for one or more anxiety disorder (separation anxiety disorder, social phobia, generalized anxiety disorder, and/or obsessive compulsive disorder; see Fujii et al. 2013). Six CBT participants met criteria for ADHD (one for inattentive-type and five combined-type) with one of the participants with ADHD-combined-type also meeting criteria for oppositional defiant disorder. Four TAU participants met criteria for ADHD (three inattentive-type and one combined-type). In addition, one CBT participant met criteria for post-traumatic stress disorder.
Intervention
CBT Condition
Therapists included six graduate students in clinical or educational psychology and one postdoctoral clinical psychology student. Therapists received a minimum of 8 h of initial training, read the treatment manual, and attended weekly hour-long supervision with the clinical supervisor. Families in the CBT condition received 32 weekly sessions of CBT, with most sessions (except for school-based sessions) taking place at a university clinic or an associated autism community clinic. Sessions lasted 90 min (about 30 min with the child and 60 min with the parents/family), implementing a version of the Building Confidence CBT program (Wood and McLeod 2008) modified by the study authors for use with children with ASD (see Wood et al. 2009a, b). The anxiety-related elements of treatment are described in Fujii et al. (2013) and involve coping skills training followed by in vivo exposure in which a hierarchy is created, delineating feared situations from least to most distressing. Children work their way up the hierarchy and are rewarded as they attempt increasingly fearful activities. In ASD-specific treatment modules, children and parents are taught friendship skills (e.g., giving compliments, acting like a good sport, hosting peer get-togethers successfully, etc.) and children are given social coaching by the therapist, parents, and available school providers on appropriate ways to enter peer interactions and maintain conversations with peers. Social coaching is provided on-site immediately before attempting to join a social activity at school or in the community and is discussed in terms of others’ thoughts and feelings. These skills are practiced in session, at school, and during playdates and are reinforced with a comprehensive reward system that relies on both daily privileges and longer-term incentives. To address the social isolation that many children with ASD experience at school, peer “buddy” and mentoring programs are set up during the school meeting. Two meetings are scheduled at the child’s school to teach the social intervention techniques to relevant school providers (e.g., aides, teachers). Telephone follow-up is offered to teachers on an as-needed basis. All skill development and practice efforts are supported by guided conversations in which the therapist uses Socratic questioning to promote conceptual development and particularly, perspective-taking (e.g., immediately before entering a playground interaction).
Children’s circumscribed interests and stereotypies are incorporated into the intervention in two ways. To enhance rapport, therapeutic concepts (e.g., emotion recognition, cognitive restructuring) are taught using children’s special interests as examples (e.g., for a child primarily interested in a particular cartoon character, the character’s “feelings” and “thoughts” in socially awkward situations could serve as the basis of discussion) and as rewards (e.g., granting access to the preferred stimulus). Later in treatment, a suppression approach is introduced, in which increasing amounts of time per day are devoted to consciously refraining from discussing or engaging in activities related to the circumscribed interest or engaging in stereotypies such as flapping. To help children understand the rationale for suppression, information about social expectations and acceptance is provided during these modules (e.g., that these behaviors are fine in private but tend to confuse peers and get in the way of friendship).
Treatment-as-Usual (TAU) Condition
Families randomized to TAU were given a comprehensive list of community mental health clinics and encouraged to seek evaluation and treatment for their child from one of these resources, or through public/private insurance, or through private practitioners. All children in this condition received a psychosocial intervention in the community during the TAU period. After 16 weeks in the TAU condition, families were given 16 weeks of the same CBT treatment described above.
Treatment Attendance
If a session was missed, it was made up within a week or two so that the allotted number of sessions was completed by all families. The average number of rescheduled treatment sessions was approximately 10 (out of 32 treatment sessions). Treatment sessions were dispersed throughout the calendar year, with start dates varying due to the rolling nature of enrollment in the study. No pattern of differing start dates was seen between the IT and TAU groups.
Therapist Fidelity
Therapists’ adherence to the intervention protocol was monitored through audio recordings of each therapy session. A random selection of three treatment sessions for each CBT participant were coded for fidelity to the treatment manual by trained graduate and undergraduate students with substantial experience. Coders listened to each tape and noted the presence of required topics for each module following a protocol taken from key points within each module developed in the Wood et al. (2009a, b) RCT. Sample items from the checklist were: ‘Planned and/or practiced making phone calls’ (yes/no) and ‘Conducted a social exposure immediately after social coaching discussion’ (yes/no). Results showed that study therapists adhered to 92 % of the required topics, on average.
Measures
ASD Diagnosis and IQ Assessment
All assessments were conducted by IEs blind to treatment condition. ASD diagnoses were assigned using the Autism Diagnosis Interview-Revised (ADI-R; Le Couteur et al. 2003; Lord et al. 1994) and Module 3 of the Autism Diagnostic Observation Schedule (ADOS; Lord et al. 2002). The ADI-R is a 93-item standardized interview that provides a comprehensive autism spectrum diagnostic assessment. Domains assessed by the ADI-R include social, communication, and repetitive behaviors. All ADI-R interviews were conducted with the child’s primary parent. The ADOS is a semi-structured, standardized protocol for observation of social and communicative behavior associated with autism. The ADOS assesses three domains: social, communication, and restricted and repetitive behaviors. Module 3 of the ADOS is designed for verbally fluent children for whom playing with toys is age-appropriate. The validity and reliability of the ADOS cut-off scores have been determined to be robust (Lord et al. 2000). The ADI-R and ADOS were administered by doctoral and post-doctoral students who were research-certified in their use. All children met criteria for ASD based on ADOS scores as well as surpassing the clinical cut-point for at least the social domain of the ADI-R algorithm score. IQ was assessed using the Kaufman Brief Intelligence Test, Second Edition (KBIT-2; Kaufman and Kaufman 2004). The KBIT-2 measures verbal and nonverbal intelligence and has strong reliability and validity (Walters and Weaver 2003).
Observed Social Communication-Related Autism Symptom Severity
This domain was assessed using Bauminger’s (2002) observational measure of social communication behavior during school recess. Each observation lasted 15 min, and two observations were conducted for each participant on different days at each assessment point to attain a broader sample of behavior. Coders observed the target child’s behavior and any peer responses for 40 s intervals followed by 20 s recording periods. Hence, a total of 30 1-min intervals of behavior were coded for each child at each assessment point. Two graduate students familiar with the social interactions of children with autism were trained by the study investigator and practice coding was conducted and feedback provided until 85 % interrater agreement on each code was obtained. Coders maintained close proximity (within ~10 feet) to the target child in order to observe behavior and hear conversations between the child and his or her peers on the playground.
In the coding system, intervals of behavior were initially categorized into four main social communication types based on the actions of the target child: solitary, initiation, response, and interaction. When the child engaged in social behavior with peers, the coder also recorded the peer’s response as either positive (+), neutral (0), or negative (−). For example, positive peer responses were coded when the action of the target child resulted in a clear positive response by the peer, such as an enthusiastic comment, a smile, a high-five, inclusion in an activity, or other behavior that had a distinctly positive quality. Negative responses included ignoring, criticizing, aggression, or active exclusion. A neutral (appropriate) response was coded when the peer’s behavior lacked a specific positive or negative quality. If there was a question as to the nature of the peer’s response due to a lack of sufficient cues, a neutral (appropriate) code was given.
An adaptation was made to Bauminger’s observation system to simplify the coding process. Various types of communication between children were collapsed and divided into two categories on the coding sheet: functional and social communication. Functional communication was solely focused on obtaining information or actions from others while social communication did not have an explicit functional goal and was characterized by chat about a topic of interest (e.g., video games), jokes, stories, and comments about ongoing events in a game (e.g., “she’s fast!”). In addition to coding the behaviors of the target child and their peer’s response, the object of the child’s behavior (peer vs. adult) and the number and gender of the peers the child was interacting with were recorded.
For this study, five summary variables were created, collapsing across one or more codes: Solitary, Any Peer Interaction, Positive or Appropriate Interaction with Peers, Positive or Appropriate Response to Child by Peers, and Negative Behavior. Intervals were coded as Solitary if the child was away from peers and caregivers for the entire interval and this was not a result of playing in a game such as freeze-tag. Any Peer Interaction was coded if the child was engaged in initiation, response, or interaction with a peer, regardless of the content/valence of the interaction. To be coded as a Positive or Appropriate Interaction with Peers, an interval needed to involve at least one of the following elements in the context of initiation, response, or interaction with a peer: affection, greeting, offering help, social communication, functional communication, eye contact, eye contact with a smile, or sharing items. Positive or Appropriate Response to Child by Peers was coded if an interval was coded as Positive or Appropriate Interaction with Peers and the peer’s response to the child’s social behavior was categorized as positive or neutral (appropriate). Intervals were coded as Negative Behavior if the target child engaged in repetitive behaviors, repetitive language, imitating others, avoidant responses (looking or walking away from peers), or verbal or physical aggression. The majority of observations were conducted by one coder. The second coder accompanied the primary coder for five observations to assess for interrater reliability, and 84 % interrater agreement across all codes was obtained. Regular coding meetings were scheduled in order to minimize coder drift and maintain a common set of coding practices/decisions.
Psychiatric Services Assessment
The Service Assessment for Children and Adolescents-Service Use Scale (SACA; Horwitz et al. 2001) was used to track mental health services used by participants during the CBT and TAU conditions. It is a psychometrically sound parent interview about the use of mental health services (supplemented with ASD-specific items as well as an item about change of schools). It was administered at screening and post-CBT and post-TAU assessments.
Procedure
The current study was approved by a university-based IRB and was conducted as approved. Phone contact was initiated by parents referred to the study coordinator, and an initial screening was conducted during this phone call. Parents who remained interested in the study, and whose child appeared to meet basic eligibility criteria gave written informed consent and children gave written assent to participate in the study. Children who completed the intake assessment and met all inclusion/exclusion criteria were block randomized by sex and age to the CBT or TAU condition. The CBT condition entailed 32 weekly sessions, while the TAU condition lasted just 16 weeks. Although this led to an unequal length of time in the two conditions, there is research precedent for this type of design in seminal RCTs (e.g., Kendall 1994; Kendall et al. 1997) and it was deemed ethically preferable to offer families in the TAU condition the opportunity to receive CBT after 16 weeks (a waitlist period with precedent in recent RCTs; e.g., Storch et al. 2013) as compared to 32 weeks. The majority of the CBT treatment was conducted in a clinic setting, though, due to the nature of CBT, some of it was performed in community settings (e.g., parks; shopping malls) and, as described above, several consultations were conducted at the child’s school. During the 16 week TAU condition, families were free to seek any kind of treatment they chose in the community. Post-CBT assessments were completed within one week of termination. Post-TAU assessments were conducted 16 weeks after the baseline assessment, but before initiating CBT. Behavioral observations using the Bauminger (2002) coding system were conducted on two separate days at intake and on two separate days at post-CBT/TAU for all participants. Families received $15 for participating in the assessments.
Results
For the participating sample (N = 13), recruitment began in 8/2008 and ended in 10/2010; posttreatment assessments were completed by 9/2011. There were no statistically significant pretreatment group differences on the demographic variables or ADI-R, ADOS, KBIT, or behavioral observation scores.
Means, standard deviations, and ranges for behavioral observation ratings of social communication-related autism symptom severity are presented in Table 2. Mean scores represent the number of 1-min intervals, out of a total of 30, in which each coded behavior occurred. ANCOVA was used to test group differences at post-CBT/TAU on behavioral observation ratings, with the children’s baseline scores included as covariates. There was a statistically significant group difference on all but one of the behavioral observation summary codes, including Solitary, Any Peer Interaction, Positive or Appropriate Interaction with Peers, and Positive or Appropriate Response to Child by Peers [Fs (1,10) = 8.38, 6.26, 8.86, and 5.95, respectively, ps < .05]. In each case, children in CBT approximately doubled their rate of social interactions (e.g., from 8.86 intervals out of 30 intervals at pretreatment for Positive or Appropriate Interaction with Peers, to 19 intervals out of 30 intervals at posttreatment, on average) and cut their rate of Solitary behavior by more than half from pre- to post-treatment (i.e., declining from 14.71 intervals out of 30 intervals at pretreatment to 6.71 intervals out of 30 intervals at posttreatment, on average). In contrast, for each of these four variables, children’s scores in the TAU group were slightly worse at posttreatment as compared to pretreatment. Hence, posttreatment scores favored CBT over TAU for each of these four variables, with large effect sizes (ds ranged from 1.34 to 1.62; see Figs. 1, 2, 3, 4). No significant treatment effect was found for Negative Behavior (although d = .50, favoring CBT at posttreatment). Because of the small sample in use, a nonparametric version of ANCOVA was employed to test the robustness of the treatment effects. Pre- and post-treatment scores on all observational scales (as noted above and in Table 2) were subjected to rank-order transformation, following convention for robust ANCOVA models (Akritas and Brunner 2003). Then, the ANCOVA tests were rerun, producing an identical pattern of statistically significant effects to those found using classical ANCOVA, described above. These results suggest that extreme scores and outliers on the continuous observational scales within this sample are not likely to have spuriously produced the observed statistically significant findings.

Change in average number of intervals out of 30 that children engaged in solitary behavior from baseline to post-CBT or post-TAU

Change in average number of intervals out of 30 that children engaged in any peer interaction from baseline to post-CBT or post-TAU

Change in average number of intervals out of 30 that children engaged in any proper or appropriate peer interactions from baseline to post-CBT or post-TAU

Change in average number of intervals out of 30 that children received positive or appropriate peer responses to their social initiations from baseline to post-CBT or post-TAU
Service Use
A summary of psychosocial treatment, educational services and psychiatric medication use by treatment condition is presented in Table 3.
TAU Condition
The SACA interview was administered at pre- and post-TAU. At the beginning of the TAU condition, the only services received by TAU participants was psychotropic medication therapy, with four of the six participants receiving such services. Two children were taking antidepressants, one was receiving stimulant medication, and one was taking an antipsychotic. During the TAU condition, all children added at least one psychosocial or educational intervention to their services (see Table 3). TAU Child 1 began services with a behaviorist and maintained a stable dosage of medication. TAU Child 2 began a weekly social skills group, began receiving individual therapy from a school psychologist, and increased his/her dosage of antipsychotic medication. TAU Child 3 began a weekly social skills group at school, and had no changes in psychotropic medication type or dosage. TAU Child 4 received both biweekly individual counseling from a licensed therapist as well as 4 h a week of applied behavioral analysis at home. TAU Child 5 received weekly therapy sessions with a clinical social worker in a community setting, weekly small group occupational therapy, weekly floortime intervention at home, weekly social problem solving treatment during school, and daily assistance from an inclusion specialist during lunch and recess. Child 6 received weekly therapy sessions with a clinical social worker in a community setting.
CBT Condition
At the onset of the study, three of the seven participants in the CBT condition were receiving outside services. Two children were receiving individual therapy from a licensed psychologist, with one of those children also participating in a weekly social skills group. Both children ceased those services before beginning the intervention. Three of the seven children in the CBT condition were receiving stable medication therapy before the start of the intervention. One child was using antipsychotic medication, one was using antidepressant and stimulant medication, and one was using an antidepressant as well as an alpha 2-adrenergic agonist and stimulant medication. One child out of the three using medication changed their dosage during the course of the intervention (he/she increased the dosage of alpha 2-adrenergic agonist medication and reduced the dosage of antidepressant medication). For participants in the CBT condition, the following outside services were received during their 32 weeks of intervention: Three children began receiving a social skills group intervention, with two run by community mental health providers and the third run by a school provider.
Discussion
Children randomized to CBT evidenced a significantly greater improvement in observed social communication-related autism symptom severity as compared to children randomized to TAU. In terms of both positive or appropriate interactions with peers as well as positive or appropriate responses to the child’s social communication bids by peers, children in the CBT group approximately doubled their rate of positive social interactions during recess from pre- to post-treatment, ultimately spending the great majority of their time (77.6 % on average) with others rather than in solitary activities, and the majority of their time (68.6 % on average) engaged in positive or appropriate social interaction with peers. On average, children in the TAU group did not change in their rate of these observed positive behaviors from pre- to post-TAU, ending the TAU condition with notably different frequencies of the same social behaviors when compared to the CBT group (i.e., 45.8 % of intervals observed with others, and only 25 % of intervals engaged in positive or appropriate social interaction with peers). Although the study has a small sample and a number of other limitations, discussed below, these initial results are promising and represent the first objective measurement approach to ascertaining the effects of CBT on children’s core autism symptoms.
As a probe of children’s social communication-related autism symptom severity, blinded observations of participating children at school recess represent a meaningful sample of behavior in a socially-challenging and contextually important daily situation. Numerous studies have illustrated that children with ASD tend to become isolated and disengaged in unstructured social settings such as school recess (e.g., Bauminger et al. 2003; Chamberlain et al. 2007). In these settings, a number of core autism symptoms can be especially pronounced, including a failure to initiate interactions with peers, a lack of appropriate responsiveness to peers’ social initiations, a lack of sustained interaction and play following group entry (sometimes manifested as children quickly disengaging and moving from area to area on the playground yard rather than committing and sticking with a game or conversation; Ingram et al. 2007) and excessive involvement in restricted patterns of interest or behavior (e.g., collecting leaves, walking around drains). For many affected children, the lack of adult direction or other structures (e.g., a requirement to participate in specific social activities), combined with the potentially confusing or unrewarding qualities that some children with ASD attribute to the peer social activities occurring in such settings, likely combine to elicit or magnify deficits in communication and engagement that are core to ASD. While hardly the only relevant context for the expression and impact of autism symptoms among school-age children, behavior during school recess is an important litmus test for intervention effects due to the tendency for autism symptoms to be elicited consistently in this setting (e.g., Kasari et al. 2011).
The participants in the CBT treatment were engaged in a multifaceted range of intervention activities designed to address emotion dysregulation and core autism symptoms. All children in the study had a concurrent anxiety disorder as an entry criterion, which can pose additional barriers to social engagement for children with or without ASD (Bellini 2004; Chang et al. 2012), and most children also met criteria for ADHD. Emotion dysregulation and behavioral problems were addressed using CBT strategies developed for children with ASD (Wood et al. 2009a, b). Both parents and teachers were recruited to help implement both behavioral and cognitive aspects of the intervention to achieve a wraparound effect to the greatest extent possible. Efforts were made to introduce behavioral supports (e.g., reward charts linked to earning daily electronics privileges) synchronized between school and home to maximize the child’s motivation to regulate emotion, comply with caregivers, and engage socially even when initially anxious or disinterested.
With sufficient remission of behavioral symptoms and emotional dysregulation, a treatment focus on core autism symptoms using CBT methods became viable for a majority of children randomized to CBT. In treating core autism symptoms in this sample, it was clinically useful to conceptualize specific social difficulties as emanating partly from at least one of two motivational states: social anxiety or limited social interest. For example, a child who was highly reticent to approach other children due to a perceived likelihood of rejection, but who had exhibited both social interest and sufficient social skill in a limited number of current peer relationships (e.g., friendships established in earlier childhood with parental help; neighbors) was considered to be especially impacted by social anxiety. In contrast, a child who had no evident fearful social cognitions, but expressed disinterest in interacting with peers in many circumstances, was posited to be particularly affected by low social interest/motivation. Children characterized by either or both of these motivational states might or might not also have significant social skill challenges such as limited ability to maintain conversations with peers, a lack of familiarity with basic social entry behavior (e.g., joining in games), or a lack of age-typical play skills (e.g., pretending, board game expertise, handball skill, etc.). The intervention techniques developed for the CBT program under investigation aimed to improve specific skills that were most relevant to rapidly promoting a child’s social engagement within their personal social context, while reducing anxiety and increasing motivation to engage. The modular nature of the intervention required clinicians and supervisors to choose treatment modules that fit the child’s most pressing clinical needs according to an algorithm. In future research, identifying the importance of these two motivational barriers to social engagement to outcomes, and determining which treatment modules are best suited to children with either or both of these barriers would be useful in further personalizing care in CBT treatment.
Exposure and reward strategies were important behavioral techniques used in this CBT program, but an additional element emphasized in this treatment was co-developing (with the child) age-appropriate rationales for specific types of social behavior. In conjunction with experimenting with specific new social behaviors, such as playing with unknown children at the park, or hosting a playdate, Socratic discussions were held to help the child speculate about peers’ perspectives about the child’s social behavior [e.g., “she (child with autism) is making this playdate/game really fun, and I feel happy”] and implications for the future [e.g., “I really want to play with her (child with autism) again; she’s a nice new friend; I hope we have fun like this in the future”]. These discussions were intended to link positive real-world experiences in specific social interactions with theory-of-mind concepts that might generalize to new peer interaction situations. Hence, the social conceptual training embedded in this CBT program, anchored to real-world social successes with peer interactions at home, school, and the community achieved through behavioral means (skills training, exposure, reward), may have been a beneficial element of the overall treatment package.
One distinct element of this treatment was its length: 32 sessions, 90 min per session, with two school visits/consultations. This was a relatively long and intense intervention by the standards of many child CBT programs for anxiety and depression (which often last 8–16 sessions). However, 32 sessions is very brief by the standards of applied behavior analysis, an intensive intervention often used for children with ASD that can last years with many hours per week (e.g., Dawson et al. 2010), particularly if it permitted significantly reduced service use for the child following treatment termination. In general, service use and costs are high for the average school-age child with ASD in the US. Among 6–10 year-olds with mild ASD, the average child uses about seven current services/interventions (e.g., therapies, medications; Green et al. 2006; see also Thomas et al. 2007). Hence, over the course of childhood, even high-functioning children often receive hundreds to thousands of hours of community treatment. Much this treatment is not evidence-based (Hess et al. 2008). A treatment that had the potential to both substantially reduce the need for future service, improve adaptive functioning, and reduce morbidity could be an economical alternative to the actual status quo for the average service recipient. Further research is needed to determine whether the present treatment meets these criteria, or requires further improvement to do so.
The limitations of this study include the small sample size, observations conducted only in school playgrounds, a TAU control group with a 16-week posttreatment assessment, and the lack of a follow-up assessment. While statistically significant intervention effects were obtained, reducing concerns about power, observations in other naturalistic settings such as the home environment would offer more satisfactory generalization probes, though as noted school recess is a uniquely well-suited environment to test the effects of an intervention targeted at social communication with peers. It should be noted that the observational measure summary scores that were used emphasized broad classes of social behaviors (e.g., positive or appropriate initiations) as opposed to discrete communicative acts such as giving compliments, so it is unclear which aspects of peer interactions improved the most in response to CBT. The 16-week posttreatment assessment period was deemed the maximum length of time that would be clinically appropriate to have families wait before offering a structured CBT program (they were given 16 weeks of CBT at that point). An active control group with a credible alternative intervention such as social skills training is likely to be a more stringent test of the specificity of treatment effects and would allow for a 32-week posttreatment assessment. It should also be noted that this CBT program was a multicomponent intervention, and decomposition studies would be needed to determine which elements of treatment are most important for which types of presenting child characteristics.
In summary, core autism symptoms have been a difficult target of treatment in other intervention modalities (cf. Rao et al. 2008), but there is accumulating evidence suggesting that relatively intensive CBT (at least 16 sessions, with significant caregiver involvement) may be a promising approach for reducing the severity of autism symptoms in school-aged children. Accruing evidence points to the relatively better level of adaptation and independence that may be achieved by young adults with qualitatively lower levels of ASD symptom severity, even after controlling for IQ (Szatmari et al. 2009) and hence, such improvements are an important goal for intervention programs. At present, two studies based on parent-reported ASD symptom severity, and one study based on blinded observations of ASD symptoms have found that 16–32 sessions of CBT may yield meaningful reduction in autism symptom severity as compared to a waitlist or TAU comparison group (Storch et al. 2013; Wood et al. 2009b; and the present study). Further research may productively build off this initial pilot trial in exploring the potential of CBT for treating social communication deficits in high-functioning children with ASD. In the meantime, clinicians may find it useful to explore the utility of CBT approaches to addressing presenting problems exhibited by the school-age children with ASD with whom they work.
References
Akritas, M. G., & Brunner, E. (2003). Nonparametric models for ANOVA and ANCOVA: A review. In M. G. Akritas & D. N. Politis (Eds.), Recent advances and trends in nonparametric statistics (pp. 79–92). Amsterdam: Elsevier B.V.
Anderson, M. C., Bjork, R. A., & Bjork, E. L. (1994). Remembering can cause forgetting—retrieval dynamics in long-term-memory. Journal of Experimental Psychology: Learning, Memory, and Cognition, 20, 1063–1087. doi:10.1037/0278-7393.20.5.1063.
Anderson, M. C., Green, C., & McCulloch, K. C. (2000). Similarity and inhibition in long-term memory: Evidence for a two-factor theory. Journal of Experimental Psychology: Learning, Memory, and Cognition, 26, 1141–1159. doi:10.1037/0278-7393.26.5.1141.
Bauminger, N. (2002). The facilitation of social-emotional understanding and social interaction in high-functioning children with autism: Intervention outcomes. Journal of Autism and Developmental Disorders, 32(4), 283–298. doi:10.1023/A:1016378718278.
Bauminger, N., Shulman, C., & Agam, G. (2003). Peer interaction and loneliness in high-functioning children with autism. Journal of Autism and Developmental Disorders, 33(5), 489–507. doi:10.1023/A:1025827427901.
Bellini, S. (2004). Social skill deficits and anxiety in high-functioning adolescents with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 19, 78–86. doi:10.1177/10883576040190020201.
Brewin, C. R. (2006). Understanding cognitive behaviour therapy: A retrieval competition account. Behaviour Research and Therapy, 44, 765–784. doi:10.1016/j.brat.2006.02.005.
Chalfant, A. M., Rapee, R., & Carroll, L. (2007). Treating anxiety disorders in children with high functioning autism spectrum disorders: A controlled trial. Journal of Autism and Developmental Disorders, 37(10), 1842–1857. doi:10.1007/s10803-006-0318-4.
Chamberlain, B., Kasari, C., & Rotheram-Fuller, E. (2007). Involvement or isolation? The social networks of children with autism in regular classrooms. Journal of Autism and Developmental Disorders, 37(2), 230–242. doi:10.1037/0022-006X.66.1.7.
Chambless, D. L., & Hollon, S. D. (1998). Defining empirically supported therapies. Journal of Consulting and Clinical Psychology, 66, 7–18.
Chang, Y., Quan, J., & Wood, J. J. (2012). Effects of anxiety disorder severity on social functioning in children with autism spectrum disorders. Journal of Developmental and Physical Disabilities, 24, 235–245. doi:10.1007/s10882-012-9268-2.
Craske, M. G., Kircanski, K., Zelikowsky, M., Mystkowski, J., Chowdhury, N., & Baker, A. (2008). Optimizing inhibitory learning during exposure therapy. Behaviour Research and Therapy, 46(1), 5–27. doi:10.1016/j.brat.2007.10.003.
Dawson, G., Rogers, S., Munson, J., Smith, M., Winter, J., Greenson, J., et al. (2010). Randomized, controlled trial of an intervention for toddlers with autism: The early start Denver model. Pediatrics, 125(1), e17–e23. doi:10.1542/peds.2009-0958.
DeRosier, M. E., Swick, D. C., Davis, N. O., McMillen, J. S., & Matthews, R. (2011). The efficacy of a social skills group intervention for improving social behaviors in children with high functioning autism spectrum disorders. Journal of Autism and Developmental Disorders, 41(8), 1033–1043. doi:10.1007/s10803-010-1128-2.
Eaves, L. C., & Ho, H. H. (2008). Young adult outcome of autism spectrum disorders. Journal of Autism and Developmental Disorders, 38(4), 739–747. doi:10.1007/s10803-007-0441-x.
Ferraioli, S. J., & Harris, S. L. (2011). Effective educational inclusion of students on the autism spectrum. Journal of Contemporary Psychotherapy, 41(1), 19–28. doi:10.1007/s10879-010-9156-y.
Fujii, C., Renno, P., McLeod, B. D., Lin, C. E., Decker, K., Zielinski, K., et al. (2013). Intensive cognitive behavioral therapy for anxiety disorders in school-aged children with autism: A preliminary comparison with treatment-as-usual. School Mental Health, 5(1), 25–37. doi:10.1007/s12310-012-9090-0.
Green, V. A., Pituch, K. A., Itchon, J., Choi, A., O’Reilly, M., & Sigafoos, J. (2006). Internet survey of treatments used by parents of children with autism. Research in Developmental Disabilities, 27, 70–84. doi:10.1016/j.ridd.2004.12.002.
Hess, K. L., Morrier, M. J., Heflin, L. J., & Ivey, M. L. (2008). Autism treatment survey: Services received by children with autism spectrum disorders in public school classrooms. Journal of Autism and Developmental Disorders, 38(5), 961–971. doi:10.1007/s10803-007-0470-5.
Horwitz, S. M., Hoagwood, K., Stiffman, A. R., Summerfeld, T., Weisz, J. R., Costello, J., et al. (2001). Measuring youth’s use of mental health services: Reliability of the SACA—services assessment for children and adolescents. Psychiatric Services, 52, 1088–1094. doi:10.1176/appi.ps.52.8.1088.
Ingram, D. H., Dickerson Mayes, S., Troxell, L. B., & Calhoun, S. L. (2007). Assessing children with autism, mental retardation, and typical development using the playground observation checklist. Autism, 11(4), 311–319. doi:10.1177/1362361307078129.
Kasari, C., Locke, J., Gulsrud, A., & Rotheram-Fuller, E. (2011). Social networks and friendships at school: Comparing children with and without ASD. Journal of Autism and Developmental Disabilities, 41, 533–544. doi:10.1007/s10803-010-1076-x.
Kasari, C., Rotheram-Fuller, E., Locke, J., & Gulsrud, A. (2012). Making the connection: Randomized controlled trial of social skills at school for children with autism spectrum disorders. Journal of Child Psychology and Psychiatry, 53(4), 431–439. doi:10.1111/j.1469-7610.2011.02493.x.
Kaufman, A. S., & Kaufman, N. L. (2004). Kaufman brief intelligence test (2nd ed.). Circle Pines, MN: American Guidance Service Inc.
Kendall, P. C. (1994). Treating anxiety disorders in children: Results of a randomized clinical trial. Journal of Consulting and Clinical Psychology, 62(1), 100–110. doi:10.1037/0022-006X.62.1.100.
Kendall, P. C., Flannery-Schroeder, E., Panichelli-Mindel, S. M., Southam-Gerow, M., Henin, A., & Warman, M. (1997). Therapy for youths with anxiety disorders: A second randomized clinical trial. Journal of Consulting and Clinical Psychology, 65(3), 366–380. doi:10.1037/0022-006X.65.3.366.
Le Couteur, A., Lord, C., & Rutter, M. (2003). The autism diagnostic interview-revised. Los Angeles: Western Psychological Services.
Lickel, A., MacLean, W. E., Jr., Blakeley-Smith, A., & Hepburn, S. (2012). Assessment of the prerequisite skills for cognitive behavioral therapy in children with and without autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(6), 992–1000. doi:10.1007/s10803-011-1330-x.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Leventhal, B. L., DiLavore, P. C., et al. (2000). The autism diagnostic observation schedule—generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30(3), 205–223. doi:10.1023/A:1005592401947.
Lord, C., Rutter, M., DiLavore, P. C., & Risi, S. (2002). Autism diagnostic observation schedule. Los Angeles: Western Psychological Services.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism diagnostic interview-revised: A revised version of a diagnostic interview for caregivers of individuals with possible developmental disorders. Journal of Autism and Developmental Disorders, 24(5), 659–685. doi:10.1007/BF02172145.
Loveland, K. A., & Tunali-Kotoski, B. (2005). In F. Volkmar, R. Paul, A. Klin, & D. Cohen (Eds.), The school-age child with an autistic spectrum disorder (pp. 247–287). Hoboken, NJ: Wiley.
Marriage, S., Wolverton, A., & Marriage, K. (2009). Autism spectrum disorder grown up: A chart review of adult functioning. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 18(4), 322.
Matson, J. L., Hess, J. A., Neal, D., Mahan, S., & Fodstad, J. C. (2010). Trend of symptoms in children diagnosed with autistic disorder as measured by the autism spectrum disorders-diagnostic for children (ASD-DC). Journal of Developmental and Physical Disabilities, 22(1), 47–56. doi:10.1007/s10882-009-9167-3.
Matson, J. L., & Horovitz, M. (2010). Stability of autism spectrum disorders symptoms over time. Journal of Developmental and Physical Disabilities, 22(4), 331–342. doi:10.1007/s10882-010-9188-y.
McDougle, C. J., Scahill, L., Aman, M. G., McCracken, J. T., Tierney, E., Davies, M., et al. (2005). Risperidone for the core symptom domains of autism: Results from the study by the autism network of the research units on pediatric psychopharmacology. American Journal of Psychiatry, 162(6), 1142–1148. doi:10.1176/appi.ajp.162.6.1142.
Puleo, C. M., & Kendall, P. C. (2011). Anxiety disorders in typically developing youth: Autism spectrum symptoms as a predictor of cognitive-behavioral treatment. Journal of Autism and Developmental Disorders, 41(3), 275–286. doi:10.1007/s10803-010-1047-2.
Rao, P. A., Beidel, B. C., & Murray, M. J. (2008). Social skills interventions for children with Asperger’s syndrome or high-functioning autism: A review and recommendations. Journal of Autism and Developmental Disorders, 38, 353–361. doi:10.1007/s10803-007-0402-4.
Reaven, J., Blakeley-Smith, A., Culhane-Shelburne, K., & Hepburn, S. (2012). Group cognitive behavior therapy for children with high-functioning autism spectrum disorders and anxiety: A randomized trial. Journal of Child Psychology and Psychiatry, 53(4), 410–419. doi:10.1111/j.1469-7610.2011.02486.x.
Reichow, B., & Wolery, M. (2009). Comprehensive synthesis of early intensive behavioral interventions for young children with autism based on the UCLA young autism project model. Journal of Autism and Developmental Disorders, 39(1), 23–41. doi:10.1007/s10803-008-0596-0.
Sofronoff, K., Attwood, T., & Hinton, S. (2005). A randomised controlled trial of a CBT intervention for anxiety in children with Asperger syndrome. Journal of Child Psychology and Psychiatry, 46(11), 1152–1160. doi:10.1111/j.1469-7610.2005.00411.x.
Sofronoff, K., Attwood, T., Hinton, S., & Levin, I. (2007). A randomized controlled trial of a cognitive behavioural intervention for anger management in children diagnosed with Asperger syndrome. Journal of Autism and Developmental Disorders, 37(7), 1203–1214. doi:10.1007/s10803-006-0262-3.
Spence, S. J., & Thurm, A. (2010). Testing autism interventions: Trials and tribulations. The Lancet, 375(9732), 2124–2125. doi:10.1016/S0140-6736(10)60757-X.
Storch, E. A., Arnold, E. B., Lewin, A. B., Nadeau, J. M., Jones, A. M., De Nadai, A. S., et al. (2013). The effect of cognitive-behavioral therapy versus treatment as usual for anxiety in children with autism spectrum disorders: A randomized, controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 52(2), 132–142. doi:10.1016/j.jaac.2012.11.007.
Szatmari, P., Bryson, S., Duku, E., Vaccarella, L., Zwaigenbaum, L., Bennett, T., et al. (2009). Similar developmental trajectories in autism and Asperger syndrome: From early childhood to adolescence. Journal of Child Psychology and Psychiatry, 50(12), 1459–1467. doi:10.1111/j.1469-7610.2009.02123.x.
Thomas, K. C., Morrissey, J. P., & McLaurin, C. (2007). Use of autism-related services by families and children. Journal of Autism and Developmental Disorders, 37(5), 818–829. doi:10.1007/s10803-006-0208-9.
Tulving, E. (1979). Relation between encoding specificity and levels of processing. In L. S. Cermak & F. I. M. Craik (Eds.), Levels of processing in human memory (pp. 405–428). Hillsdale, NJ: Erlbaum.
Walters, S., & Weaver, K. (2003). Relationships between the Kaufman brief intelligence test and the Wechsler adult intelligence scale-third edition. Psychological Reports, 92, 1111–1115. doi:10.2466/pr0.2003.92.3c.1111.
West, L., Waldrop, J., & Brunssen, S. (2009). Pharmacologic treatment for the core deficits and associated symptoms of autism in children. Journal of Pediatric Health Care, 23(2), 75–89. doi:10.1016/j.pedhc.2008.12.001.
Wood, J. J., Drahota, A., Sze, K. M., Har, K., Chiu, A., & Langer, D. (2009a). Cognitive behavioral therapy for anxiety in children with autism spectrum disorders: A randomized, controlled trial. Journal of Child Psychology and Psychiatry, 50, 224–234. doi:10.1111/j.1469-7610.2008.01948.x.
Wood, J. J., Drahota, A., Sze, K., Van Dyke, M., Decker, K., Fujii, C., et al. (2009b). Brief report: Effects of cognitive behavioral therapy on parent-reported autism symptoms in school-age children with high-functioning autism. Journal of Autism and Developmental Disorders, 39(11), 1608–1612. doi:10.1007/s10803-009-0791-7.
Wood, J. J., Fujii, C., & Renno, P. (2011). Cognitive behavioral therapy in high-functioning autism: Review and recommendations for treatment development. In B. Reichow, P. Doehring, D. V. Cicchetti, & F. R. Volkmar (Eds.), Evidence-based practices and treatments for children with autism (pp. 197–230). Berlin: Springer.
Wood, J. J., & McLeod, B. (2008). Child anxiety disorders: A treatment manual for practitioners. New York: Norton.
Wood, J. J., & Schwartzman, B. C. (2013). Cognitive behaviour therapies for youth with autism spectrum disorders. In P. Graham & S. Reynolds (Eds.), Cognitive behaviour therapy for children and families (pp. 189–202). Cambridge, MA: Cambridge University Press.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wood, J.J., Fujii, C., Renno, P. et al. Impact of Cognitive Behavioral Therapy on Observed Autism Symptom Severity During School Recess: A Preliminary Randomized, Controlled Trial. J Autism Dev Disord 44, 2264–2276 (2014). https://doi.org/10.1007/s10803-014-2097-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-014-2097-7