
Abstract
This study describes the impact of caregiving on parents of children with autism spectrum disorders (ASDs). Secondly, we investigate construct validation of the care-related quality of life instrument (CarerQol) measuring impact of caregiving. Primary caregivers of children with ASDs were included. Many parents experienced considerable problems combining daily activities with care, had financial problems or suffered from depressive mood. Validity tests showed that a higher impact of caring on the CarerQol was positively associated with higher subjective burden and lower family quality of life. Most of the associations between CarerQol scores and background characteristics confirmed previous research. The CarerQol validly measures the impact of caregiving for children with ASDs on caregivers in our sample. The CarerQol may therefore be useful for including parent outcomes in research on ASDs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Caring for children with autism spectrum disorders (ASDs) is challenging and affects family life. ASDs are neurological complex conditions impairing social interaction and communication, such as difficulties to respond to social interactions or deficits in understanding nonverbal communication. Moreover, persons diagnosed with an ASD have restricted behavioral functions, such as stereotype behavior or inability to adjust to new situations (Strock 2007). Children with ASDs often exhibit more than one of these core ASD symptoms and many also suffer from associated symptoms, such as severe tantrums or sleep problems (Aman 2004; Couturier et al. 2005). Moreover, health in general of these children is lower than that of typically developing children (Gurney et al. 2006; Kuhlthau et al. 2010b, 2013).
Meeting the high care demands of affected children requires much time, effort and patience. This often results in psychological distress, depression, anxiety and other mental or physical health problems among their parents (Bromley et al. 2004; Hamlyn-Wright et al. 2007; Khanna et al. 2011; Kuhlthau et al. 2010a). Moreover, many parents face financial problems, given high out-of-pocket health care expenses, underemployment or employment loss (Bromley et al. 2004; Hamlyn-Wright et al. 2007; Kuhlthau et al. 2005, 2010a, b). Not surprisingly, parents of children with ASDs often feel strained by caregiving (Khanna et al. 2011; Stuart and McGrew 2009).
Given these prolonged and multidimensional care needs of children with ASDs, it is important to accurately measure the impact of caregiving on the lives of the parents of these children. At present, evaluations of ASD treatments are often limited to measurement of effects in children. However, interventions for children with ASDs often require parents’ involvement and also aim to increase parents’ caregiving skills, self-efficacy, knowledge of the disorder, and aim to reduce family stress (McConachie and Diggle 2007). Furthermore, improved well-being of parents could positively influence the effect these interventions have on children with ASDs (Giallo et al. 2013; Osborne et al. 2008). Hence, for fully understanding the effectiveness of ASD interventions it is essential that family outcomes of interventions are also included in evaluation studies (Karst and Van Hecke 2012). Insights from such studies will help develop interventions focusing on the needs of children with ASDs and their family, and facilitate consideration of those in both policy and funding decisions in health care.
Studies in the field of ASD interventions covering parent outcomes often measure parents’ health, in terms of for example, stress, anxiety and mental health (Karst and Van Hecke 2012). A drawback of this approach is the focus on a single aspect of a carers’ quality of life (Qol), i.e. health-related Qol. Other important domains of Qol that can be affected by caring, like social or financial problems, the parent–child relationship or family functioning in general (Karst and Van Hecke 2012) are not considered. In contrast to health related Qol, general Qol considers all domains of Qol (Bobinac et al. 2010; Brouwer et al. 2010). While there is debate in the literature on the definition of general Qol, most definitions consider it as a multi-dimensional concept encompassing subdomains such as physical, material, social and emotional wellbeing (Felce and Perry 1995). In theory, general Qol thus could record all possible effects of caregiving. However, such an outcome might be too broad in the context of informal care because it may be difficult to disentangle the effects of caregiving and other aspects affecting general Qol (Bobinac et al. 2010; van Campen et al. 2013). To overcome the problem of measuring effects that are not directly related to caregiving, an outcome that focuses directly on the caregiving situation could be used. Subjective burden instruments, for example, report the level of caregiving strain felt by caregivers. Many such instruments are available, like the often used Caregiver Strain Index (Robinson 1983) and Zarit Burden Interview (Zarit et al. 1980). Among children with mental, emotional or behavioral problems the Caregiver Strain Questionnaire (Brannan et al. 1997; Khanna et al. 2011; Stuart and McGrew 2009) has also been used. These instruments provide detailed information on problems of caregiving, such as disturbed daily patterns or difficulties communicating with the care recipient (Brouwer et al. 2010; Deeken et al. 2003; Van Durme et al. 2012; Van Exel et al. 2004b). However, although caregivers experience strain of dealing with care problems, they may also derive fulfillment from providing care to a loved one and gain abilities from it, such as developing more positive perspectives on life (Andrén and Elmståhl 2005; Brouwer et al. 2005; Marks et al. 2002; Myers et al. 2009). Hence, some subjective burden instruments incorporate both negative and positive aspects of caregiving, such as the Carer Experience Scale (Al-Janabi et al. 2008) and the Self-rated burden scale (SRB; Van Exel et al. 2004b).
A drawback of using subjective burden instruments in evaluations of interventions for children with ASDs is that they mainly report problems on separate dimensions of burden and lack an overall subjective burden score. However, evaluative research requires such an overall score to appropriately report and compare the impact of caring on caregivers between interventions. Preferably, this score reflects differences in importance of care problems, because the extent to which specific burden dimensions have an impact on Qol differs between caregivers (Van Exel et al. 2004a). Simple aggregation of burden dimensions to reflect total subjective burden without correcting for the severity of problems experienced by caregivers could lead to misleading conclusions.
The care-related quality of life instrument (CarerQol, see Fig. 1) was specifically developed to measure outcomes in caregivers for use in evaluative research, and so to provide the essential information for well-informed policy decisions in health care (Brouwer et al. 2006; Hoefman et al. 2013a). The approach of the CarerQol to measure caregiver outcomes was based on the EuroQol instrument measuring health-related Qol. The CarerQol measures perceived burden in two positive and five negative dimensions, provides a weighted overall subjective burden score and measures general Qol of caregivers (Brouwer et al. 2006). The CarerQol can be administrated in different caregiver populations, because the questions do not refer to a specific care situation. Such a generic instrument might be less sensitive to very specific problems experienced by caregivers in a particular context, such as parents caring for a child with an ASD, and hence less useful in a clinical setting, but it enables comparisons of the impact of caring between different populations of patients and caregivers. Therefore, the CarerQol facilitates descriptive research on the impact of providing care on a caregiver’s life. Moreover, the CarerQol enables comparative research of interventions for children with ASDs including parent outcomes in health care or other sectors, such as education. Finally, interventions directly aimed at parents of children with ASDs, like support programs for caregivers, can be also evaluated with the CarerQol.

CarerQol instrument and descriptive statistics, n = 221
The ability of the CarerQol to measure the impact of caring is supported by several construct validation studies, mostly performed in populations of caregivers for adults (Brouwer et al. 2006; Hoefman et al. 2011b, c, 2013b). To date, one set of validity tests of the CarerQol has been conducted among caregivers for children, in the specific context of children with craniofacial malformations (Payakachat et al. 2011). This study investigated associations between the impact of caregiving and the health of caregivers. Moreover, the SRB was used for construct validation of the CarerQol. Results showed that better scores on the CarerQol instrument were associated with better health and lower SRB among caregivers of children with craniofacial malformations (Payakachat et al. 2011).
Research Objectives
In this study we address two research questions. The first objective of our study is to report the impact on parents of caregiving for a child with an ASD. Given the prolonged and multidimensional nature of the care and attention required by the growing child with an ASD, there is a need to better understand the problems encountered by these parents. The second objective of our study concerns construct validation of the CarerQol instrument in a sample of caregivers of children with ASDs. In other words, we aim to investigate the ability of the CarerQol to measure the impact of providing care on caregivers of children with ASDs. This study is the first to investigate construct validation of the CarerQol among parents of children with ASDs. This study will also add to the knowledge on measurement of the impact of caregiving among caregivers of children in general, by using more elaborate tests than the prior CarerQol validation study among parents (Payakachat et al. 2011); for example, by studying multivariate associations of associates of the CarerQol instrument and performing subgroup analyses among caregivers.
Methods
Data Collection
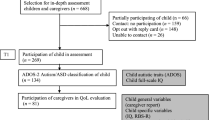
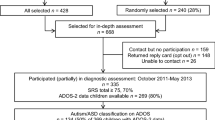
Data were collected from primary caregivers of children with ASDs who participated in clinical registries at two autism treatment network (ATN) sites in the US: Developmental Center, Little Rock, Arkansas and Outpatient Psychiatric Clinic at Columbia University Medical Center, New York. Families of affected children aged 4–17 years were invited to participate in this study by mail. The registry of the ATN site in Arkansas consisted of 247 families. Of these families, 25 did not want to be contacted for research purposes. Two families participated in a pilot survey and were not included in the final survey. The response rate of the final survey was 52.3 % (n = 115). In New York, 179 families were invited to participate in the survey and 109 of these families completed both questionnaires (response rate 60.9 %). In total, 224 families participated in our survey. These families, on average, had two children living in their home with one child having special health care needs and requiring assistance with daily living needs.
The recruitment letter specified that the primary caregiver of the child with an ASD needed to complete two surveys, one as a proxy reporter for the child’s perspective (child health questionnaire), the second from their own perspective as caregiver of a child with an ASD (primary caregiver health questionnaire). Respondents were specifically instructed that the health questions in the child health questionnaire pertained to the health of the child with an ASD and in the primary caregiver health questionnaire to the respondents’ own health. A $25 gift certificate was provided to a family that returned the two completed surveys. The study protocol was approved by the institutional review boards at Columbia University/New York State Psychiatric Institute and University Arkansas for Medical Sciences.
Child Health Questionnaire
The child health questionnaire included information on child age, gender, and whether the child was a first child. Child’s health status was assessed with the Health Utility Index (HUI-3; (Feeny et al. 2002) and Quality of Well-being Scale (QWB-SA; (Seiber et al. 2008). The HUI-3 score ranges from 0 ‘dead’ to 1 ‘best possible health’ based on eight dimensions (vision, hearing, speech, ambulation, dexterity, emotion, cognition and pain). The QWB-SA has a similar range (0 ‘dead’ to 1 ‘full health’) and consists of two parts: (1) questions on mobility, physical activity, social function and (2) a list of 27 symptoms and problem complexes.
Primary Caregiver Health Questionnaire
The primary caregiver questionnaire included questions on characteristics of (1) the caregiver, (2) the informal care situation and (3) the impact of caregiving. First, characteristics of the caregiver included in the questionnaire were age, gender, marital status, highest attained educational level, performing paid work, household income, and health. Caregiver’s health was measured with two generic health utility instruments; the EuroQol descriptive system (EQ-5D; (EuroQol Group 1990) and a six dimensional health state classification, the SF-6D (Brazier and Roberts 2004). The EQ-5D consists of five dimensions of health: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. The SF-6D uses six health dimensions: physical functioning, role limitation, social functioning, pain, energy and mental health. Both instruments result in a total score of health with 0 defined as ‘dead’ and 1 as ‘full health’. In addition, mental health was measured with the Center for Epidemiologic Studies Depression Scale (CES-D; (Radloff 1977). The CES-D measures depressive feelings and behaviors during the past week using 20 items and has a total score that ranges from 0 to 60. A cut-off point of 16 on the CES-D was used to indicate high level of depressive symptoms (Radloff 1977). Second, questions about the care situation concerned the number of hours ‘on call’ for caregiving and the presence of other caregivers for the care of children. Third, the impact of caregiving was measured with the CarerQol, the SRB and the Family Quality of Life scale (FQLS). The CarerQol is comprised of the CarerQol visual analogue scale (CarerQol-VAS) and its descriptive system (CarerQol-7D; (Brouwer et al. 2006), see Fig. 1. The CarerQol-VAS measures general Qol in terms of happiness using a horizontal VAS with defined endpoints of (0) ‘completely unhappy’ and (10) ‘completely happy’ (Brouwer et al. 2006). The CarerQol-7D measures care-related Qol of caregivers and contains seven dimensions of caregiving burden. Five of these dimensions report the negative aspects of caring: (1) relational problems with the care recipient, (2) mental health problems, (3) problems with daily activities, (4) financial problems, and (5) physical health problems. The CarerQol-7D also reports two positive experiences from caring: (6) fulfillment and (7) support. Each of these seven dimensions has three response categories: (1) no, (2) some, and (3) a lot. Answers on the negative dimensions of the CarerQol-7D receive a value of 0 (a lot), 1 (some) and 2 (no). Answers on the positive dimensions receive a value of 0 (no), 1 (some), and 2 (a lot) (Hoefman et al. 2011a). A scoring mechanism is available to calculate a care-related Qol score (Hoefman et al. 2014). These weights, or tariffs, are based on preferences for the positive and negative CarerQol-7D dimensions from the general population in the Netherlands. Applying these tariffs to the CarerQol-7D profiles yields a weighted sum score reflecting a specific part of Qol directly related to caregiving; care-related Qol [more practical issues concerning the calculation of the CarerQol-7D score can be found in the iMTA Valuation of Informal Care Questionnaire (Hoefman et al. 2011a)].
SRB measures subjective burden of informal care and consists of a single horizontal VAS ranging from (0) ‘not straining at all’ to (100) ‘much too straining’ asking respondents how burdensome they feel that caring is at the moment (Van Exel et al. 2004b). The FQLS captures Qol of families with children (Hoffman et al. 2006). It contains 25 items divided into 5 subdomains including family interaction (6 items), parenting (6 items), emotional well-being (4 items), physical/material well-being (5 items), and disability-related support (4 items). A total score is calculated by summing all 25 items (ranging from 25 to 125). Subdomain scores are calculated by summing all items on each subdomain with higher scores representing higher traits. A higher total score refers to higher family Qol.
Statistical Analyses First Research Objective
To answer our first research question on the impact of caregiving on parents of children with ASDs, descriptive statistics in percentages and means (standard deviations; sd) were calculated for the child, parent, and care situation characteristics. Furthermore, the impact of caregiving measured with the CarerQol instrument, the SRB and the FQLS was also presented in percentages and means (SD).
Statistical Analyses Second Research Objective
The second research objective of our study was construct validation of the CarerQol. Here, construct validation was conducted by testing convergent, discriminative and clinical validity of the CarerQol (Streiner and Norman 2003). Convergent validity tests assessed whether the construct of the CarerQol instrument resembled that of other instruments with the same subject of measurement. Discriminative validity tests assessed whether ‘extreme groups’ of respondents had different scores on the CarerQol instrument (Streiner and Norman 2003). Clinical validity tests investigated the extent to which differences in background characteristics were reflected in the scores of the CarerQol instrument. The statistical tests used for the three types of validity will be discussed in the following sub-paragraphs.
Convergent Validity Tests CarerQol
In this study, convergent validity was studied by investigating the association between (1) the two parts of the CarerQol instrument (i.e. the CarerQol-7D and CarerQol-VAS), and (2) between the CarerQol instrument and the other two instruments of the impact of caregiving on parents: the SRB and FQLS. First, the association between the CarerQol-VAS and CarerQol-7D was studied with bivariate and multivariate tests. Spearman’s correlation coefficients were used for testing bivariate associations of CarerQol-VAS and CarerQol-7D. Multivariate association of CarerQol-VAS and CarerQol-7D was studied with ordinary least squares regression (OLS). These multivariate associations were also tested among subgroups of caregivers of children with ASDs. These subgroups experienced either a relatively low or high impact of caregiving: (subgroup 1, n = 120) below average SRB score (subgroup 2, n = 83) equal to or higher than average SRB score (subgroup 3, n = 75) below average FQLS total score, and (subgroup 4, n = 120) equal to or higher than average FQLS total score.
The following hypotheses were formulated for convergent validity tests of the two parts of the CarerQol instrument. We expected that CarerQol-7D dimensions fulfillment and support were positively associated with CarerQol-VAS. The five negative CarerQol-7D dimensions were expected to have a negative association with CarerQol-VAS.
Second, to study associations between the CarerQol and the SRB and FQLS, Spearman’s correlation coefficients were used. For these convergent validity tests the following hypotheses applied. A priori, we hypothesized negative associations of CarerQol-VAS with SRB. Moreover, negative associations were also expected for the positive CarerQol-7D dimensions with SRB. Positive associations were hypothesized for the negative CarerQol-7D dimensions and SRB. Positive associations were expected for CarerQol-VAS and FQLS. Furthermore, we expected that positive CarerQol-7D dimensions would positively correlate with FQLS. Negative CarerQol-7D dimensions were hypothesized to negatively correlate with FQLS. The strength of Spearman’s correlation coefficients of the convergent validity tests was assessed by the following guideline: <0.1 trivial; 0.1–0.3 small; 0.3–0.5 moderate; 0.5–0.7 high; 0.7–0.9 very high; >0.9 nearly perfect (Hopkins 2002).
Discriminative Validity Tests CarerQol
We analyzed discriminative validity of the CarerQol by testing for differences in outcome scores among ‘extreme’ groups of caregivers. These groups of caregivers were constructed using their answers on the seven burden dimensions of the CarerQol-7D. We constructed groups that did, or did not, report fulfillment or support. The same was done for the five negative CarerQol-7D dimensions and groups were constructed with or without problems on the relational, mental health, daily activities, financial or physical health problem dimensions. Among these seven pairs of ‘extreme’ groups we tested for differences in the level of impact of caregiving using three instruments: the CarerQol-VAS, SRB and FQLS. Moreover, we investigated whether caregivers in negative ‘extreme’ groups had lower health status than those in the positive ‘extreme’ groups. The same was done for the health status of the children. Differences in mean scores among the extreme CarerQol-7D groups were analyzed with Student’s t-tests. The following results were expected a priori for the discriminative validity tests of the CarerQol. First, we hypothesized that caregivers deriving fulfillment or receiving support overall had higher CarerQol-VAS and FQLS scores and lower SRB scores. Second, we expected them and their children to be in better health than those without fulfillment or support. A third hypothesis concerned that caregivers experiencing any of the five CarerQol-7D problem dimensions would have lower CarerQol-VAS, FQLS, child health or own health scores and higher SRB scores than those without these care problems.
Clinical Validity Tests CarerQol
To investigate clinical validity, we studied associations between CarerQol-VAS and background characteristics of the child, caregiver and care situation. Bivariate associations were studied with One-way ANOVA tests. Multivariate association between CarerQol-VAS and these characteristics was studied with OLS. We tested several model specifications. We started with the base model of CarerQol-VAS explained by the dimensions of the CarerQol-7D. The child, caregiver and care situation characteristics were added to this base model. We used stepwise backward OLS regression with a cut-off p value > 0.2 to delete insignificant child, caregiver and care situation variables from our model. Categories of background variables were merged if they contained <10 % of our sample. The category with the highest CarerQol-VAS score was used as reference category for dummy variables. All statistical analyses were performed with STATA/SE 12.1 (StataCorp LP, TX, USA).
Results
Sample Characteristics Children and Caregivers
Our sample included 224 parents of children with ASDs (n = 109 ATN site in New York, n = 115 ATN site in Arkansas). The children in our sample were on average 8.4 years (SD 3.5) old (Table 1). The majority of children were male (87 %). Children’s mean HUI-3 score was 0.66 (SD 0.23). Their mean QWB-SA score was 0.59 (SD 0.16).
Caregivers of children with ASDs predominantly were the biological parents (95 %), mostly mothers (89 %) (Table 1). On average, caregivers were 39.4 years (SD 8.3) old. About 60 % had either a college, professional or graduate school degree and many had a paid job. Somewhat more than one-third of families of the children with ASDs had an income of more than $100,000/year. On average, caregivers’ subjective health on a scale from 0 to 100 was 77.6 (SD 15.8), their EQ-5D score was 0.85 (SD 0.14) and their SF-6D score was 0.74 (SD 0.12). Forty percent of caregivers had a CES-D score of 16 or higher, indicating high level of depressive symptoms. Most caregivers were ‘on call’ for care for more than 12 h/day (Table 1). The large majority of caregivers could rely on others to take care of their children.
Research Objective 1: The Impact of Caregiving on Parents of Children with ASDs
Figure 1 presents the CarerQol scores. Almost all caregivers of children with ASDs derived fulfillment from caring for their child (97 %). Many caregivers experienced problems with combining their care tasks with daily activities (61 %). Mental (58 %) and physical (52 %) health problems and financial problems (56 %) were also prevalent. On average, caregivers scored a 7.4 (SD 1.9) on the CarerQol-VAS (Fig. 1). Table 1 shows descriptive statistics of SRB and FQLS. Among caregivers of children with ASDs, the mean SRB score was 36.2 (SD 29.6) and the mean FQLS score was 100.9 (SD 16.1).
Research Objective 2: Construct Validation CarerQol
Convergent Validity: Associations Between CarerQol-VAS and CarerQol-7D
Table 2 presents Spearman’s correlation coefficients of the CarerQol-VAS with the seven burden dimensions of the CarerQol-7D. CarerQol-VAS scores were positively associated with the two positive CarerQol-7D dimensions: fulfillment from caring and support with caring. CarerQol-VAS was negatively associated with the five negative CarerQol-7D dimensions (relational problems, mental health problems, problems with daily activities, financial problems, and physical health problems). These correlation coefficients of the CarerQol-VAS with the CarerQol-7D dimensions had small to high strength of correlation.
Multivariate associations of the CarerQol-VAS and CarerQol-7D show that CarerQol-VAS scores were lower among caregivers who derived no or only some fulfillment from caregiving compared to those who derived a lot (Table 3). CarerQol-VAS scores were also lower among those experiencing physical or mental health problems. Subgroup analysis of the multivariate associations of the CarerQol-VAS and CarerQol-7D showed that fulfillment was associated with CarerQol-VAS among caregivers with high subjective burden and low family Qol. Among subgroups of caregivers with low SRB and those with high FQLS scores, support was associated with CarerQol-VAS. Physical health problems and financial problems were associated with CarerQol-VAS among the subgroup of caregivers with high SRB (Table 3).
Convergent Validity: Associations Between CarerQol and Other Instruments of Impact of Caregiving
Spearman’s correlation coefficients of the CarerQol with subjective burden of caregiving (SRB) and family Qol (FQLS) are displayed in Table 2. First, CarerQol-VAS and CarerQol-7D dimension fulfillment were significantly negatively associated with SRB scores and positively with FQLS domain scores. These correlation coefficients had small to high strength. CarerQol-7D dimension support was significantly associated to four of the five subdomains of FQLS. Relational problems, mental health problems, problems with daily activities, financial problems, and physical health problems of the CarerQol-7D were all positively associated with SRB scores and negatively associated with FQLS domain scores (small to moderate strength of correlation coefficients).
Discriminative Validity
Investigating differences in outcome scores among ‘extreme’ groups of caregivers showed that caregivers of children with ASDs that derived a lot of fulfillment or received a lot of support had higher mean general Qol (CarerQol-VAS) and family Qol (FQLS) (Table 4). Moreover, their child’s and their own health were better compared to caregivers with only some or no fulfillment or support. Furthermore, caregivers with a lot of fulfillment or support had lower subjective burden scores (SRB) compared to others. The same results were found for differences in mean values among caregivers without relational, mental health, daily activities, financial or physical health problems compared to those who did experience problems (Table 4). These differences in mean values were all statistically significant (p < 0.05). The only exception was that no differences were found in the level of the child’s health among caregivers with or without fulfillment.
Clinical Validity
Bivariate associations of the CarerQol-VAS scores and child, caregiver and care situation characteristics are presented in Table 1. The CarerQol-VAS score was higher among caregivers in relatively good physical or mental health. CarerQol-VAS score was also higher among caregivers of children with relatively good health. Concerning the care situation, the CarerQol-VAS score was higher among caregivers that could rely on others for assistance with care. Multivariate regression analysis shows no statistically significant association of the CarerQol-VAS and background characteristics (results not presented).
Discussion
Our study had two research objectives: (1) providing insight in the impact of caregiving on parents of children with ASDs and (2) construct validation of the CarerQol. Concerning the first research objective, as found by others (Gurney et al. 2006; Kuhlthau et al. 2010b, 2013), children with ASDs in our sample had relatively poor overall health, with for example, an average HUI-3 score of 0.7 compared to a HUI-3 score of 0.9 among a healthy control group including many children and adolescents in the US (Pogany et al. 2006). The caregivers of children with ASD in this study predominantly were married mothers in their forties combining care for their child(ren) with a paid job. Thus, given parents’ life phase, they often found it difficult to combine care tasks with daily activities such as work, household activities and family life. Moreover, in line with other findings (Benson 2006; Hamlyn-Wright et al. 2007; Smith et al. 2008), many caregivers of a child with an ASD experienced financial or mental health problems. In our sample, 40 % of parents reported high level of depressive symptoms, which is comparable to levels reported in similar studies of parents of children with ASDs (Benson 2006; Sawyer et al. 2010). By contrast, the prevalence of depressive mood has been reported to be lower amongst parents of children with craniofacial malformations (Payakachat et al. 2011) or among parents of typically developing children (Singer and Floyd 2006).
Despite such difficulties, many parents of children with ASD reported that they derived fulfillment from caring for their child. Moreover, parents described themselves to be fairly happy, scoring more than a 7 on a 0–10 scale of happiness. This result is consistent with previous findings (Brouwer et al. 2006; Hoefman et al. 2011a, b, 2013b; Payakachat et al. 2011).
Before discussing the results of our second research question on construct validation of the CarerQol, we first need to address some study limitations. First, some caution is needed in generalizing our results to all families of children with ASDs given some limitations regarding our study sample and data collection. For example, in our sample of children with ASDs boys were somewhat overrepresented with a boy:girl ratio of 6.7:1 in our data set, while this ratio is 4.6–1 in the United States (Blumberg et al. 2013). Moreover, our sample seems to include relatively many highly educated working mothers. In addition, it should be stressed that our results might have been affected by the use of two specific ATN sites, in Arkansas and New York. In general, these ATN sites differ in terms of the availability of formal and informal care resources given wealth and cultural differences between northern and southern states in the US. Moreover, the ATN site in New York treats children with more severe disorders. Although no differences were detected in the health status of children between ATN sites, we did find that parents from the New York ATN site experienced higher subjective burden of caring (SRB) than parents from the Arkansas’ ATN site. Scores on other outcome variables used in our study did not differ between parents of these two ATN sites. Given our focus on construct validation, we do not consider this finding to be problematic.
Another limitation in our data collection concerned the use of parent-proxy reports. Although these parent-proxy reports are often used in research on children with ASDs due to concerns about the reliability of self-reports from children who often have severe cognitive and communication problems (Kuhlthau et al. 2010a, b), this might have biased our results. However, the impact of this seems relatively small in our study given that our analyses mostly concerned parent variables.
Finally, in this study none of the background characteristics of the child with ASDs, parent or care situation were significantly related to caregivers’ well-being after adjusting for subjective burden dimensions. Given these limitations, it would be interesting in future studies to collect additional characteristics of the children and their disorders, such as clinical assessments of the severity of the disorder, in order to explain the impact of caregiving on their parents more thoroughly. Furthermore, replication of this study in a larger sample from a broader range of ATN sites is advised.
Concerning our second research question on construct validation of the CarerQol, we found that results of convergent and discriminative validity tests showed that well-being, deriving fulfillment and receiving support among caregivers of children with ASDs were all associated with higher family Qol and lower subjective burden of caring. By contrast, having relational, mental health, daily activity, financial or physical health problems were associated with more subjective burden of caring, lower family Qol and lower overall well-being.
When considering the influence of subjective burden dimensions on caregivers’ well-being, we found that especially fulfillment and mental and physical health problems were related to the well-being of parents of children with ASDs. Moreover, subgroup analyses showed interesting insights into the various associations between caregivers’ well-being and subjective burden dimensions. While some aspects of subjective burden, such as mental health, negatively influenced well-being among all subgroups of caregivers, financial problems were especially relevant to the well-being of caregivers experiencing high burden. Additionally, fulfillment especially influenced well-being among caregivers in a relatively bad situation (i.e. high subjective burden or low family Qol), while receiving support was particularly relevant to the well-being of caregivers in a relatively good position (i.e. low subjective burden or high family Qol). Other construct validation tests of the CarerQol instrument also show the diversity of problems that affect well-being among caregivers (Brouwer et al. 2006; Hoefman et al. 2011b, c, 2013b); however, whether the influence of the caring problems we found in this study are only specific for the care situation of children with an ASD, or apply to children with other care needs as well, is not yet clear. Further research into associates of well-being of parents of children suffering from other disorders or illnesses is needed.
Overall, clinical validation results supported the ability of the CarerQol to accurately measure the impact of caregiving, as most background characteristics of caregivers, care recipients and care situations associated with caregivers’ well-being in this study were consistent with findings from previous CarerQol validation studies (Brouwer et al. 2006; Hoefman et al. 2011c, 2013b; Payakachat et al. 2011).
Lastly, a note should be made on the support dimension of the CarerQol. While convergent and discriminative validity tests show inconsistent results in terms of statistical significance, all results seem to imply that support has a positive effect on parents of children with ASDs. This is also found by others (Benson and Karlof 2009; Bromley et al. 2004; Khanna et al. 2011; Sawyer et al. 2010; Stuart and McGrew 2009). However, receiving support also has some downsides. For example, different support resources, such as social networks, professional health care or special educational services, are often used for children with special health needs which require some kind of coordination (Bromley et al. 2004; Kuo et al. 2011). Moreover, support is not always considered as helpful by parents of children with ASDs (Bromley et al. 2004). Hence, support could increase burden when problems arise between caregivers, family and professionals, such as disagreement or communication difficulties (Khanna et al. 2011; Tolkacheva et al. 2011).
Conclusions
This study showed that while many parents in our sample derived fulfillment from providing care for their child with an ASD, this caregiving affected their own lives considerably and in a variety of ways. Parents often experienced problems with combining care with other daily activities, had financial problems or suffered from depressive symptoms. In addition, this study supported construct validity of the CarerQol in a population of caregivers for children with ASDs.
Further research in larger, representative samples of parents providing informal care to children with ASDs or other health problems is needed before these results can be generalized. Notwithstanding, our study showed that the CarerQol can be used to validly assess the impact of caregiving on parents of children with ASDs in our sample. The CarerQol thus seems to provide information that is relevant for evaluations of treatment interventions for children with ASDs or for support interventions for their informal caregivers.
References
Al-Janabi, H., Coast, J., & Flynn, T. N. (2008). What do people value when they provide unpaid care for an older person? A meta-ethnography with interview follow-up. Social Science and Medicine, 67(1), 111–121.
Aman, M. G. (2004). Management of hyperactivity and other acting-out problems in patients with autism spectrum disorder. Seminars in Pediatric Neurology, 11(3), 225–228.
Andrén, S., & Elmståhl, S. (2005). Family caregivers’ subjective experiences of satisfaction in dementia care: Aspects of burden, subjective health and sense of coherence. Scandinavian Journal of Caring Sciences, 19(2), 157–168.
Benson, P. R. (2006). The impact of child symptom severity on depressed mood among parents of children with ASD: The mediating role of stress proliferation. Journal of Autism and Developmental Disorders, 36(5), 685–695.
Benson, P. R., & Karlof, K. L. (2009). Anger, stress proliferation, and depressed mood among parents of children with ASD: A longitudinal replication. Journal of Autism and Developmental Disorders, 39(2), 350–362.
Blumberg, S. J., Bramlett, M. D., Kogan, M. D., Schieve, L. A., Jones, J. R., & Lu, M. C. (2013). Changes in prevalence of parent-reported autism spectrum disorder in school-aged US children: 2007 to 2011–2012. National Health Statistics Reports, 65, 1–12.
Bobinac, A., Van Exel, N. J., Rutten, F. F., & Brouwer, W. B. (2010). Caring for and caring about: Disentangling the caregiver effect and the family effect. Journal of Health Economics, 29(4), 549–556.
Brannan, A. M., Heflinger, C. A., & Bickman, L. (1997). The caregiver strain questionnaire measuring the impact on the family of living with a child with serious emotional disturbance. Journal of Emotional and Behavioral Disorders, 5(4), 212–222.
Brazier, J. E., & Roberts, J. (2004). The estimation of a preference-based measure of health from the SF-12. Medical Care, 42(9), 851–859.
Bromley, J., Hare, D. J., Davison, K., & Emerson, E. (2004). Mothers supporting children with autistic spectrum disorders social support, mental health status and satisfaction with services. Autism, 8(4), 409–423.
Brouwer, W. B. F., Van Exel, N. J. A., & Tilford, M. J. (2010). Incorporating caregiver and family effects in economic evaluations of child health. In W. J. Ungar (Ed.), Economic evaluation in child health. Oxford: Oxford University Press.
Brouwer, W. B., Van Exel, N. J., Van den Berg, B., Van den Bos, G. A., & Koopmanschap, M. A. (2005). Process utility from providing informal care: The benefit of caring. Health Policy, 74(1), 85–99.
Brouwer, W. B., Van Exel, N. J., Van Gorp, B., & Redekop, W. K. (2006). The CarerQol instrument: A new instrument to measure care-related quality of life of informal caregivers for use in economic evaluations. Quality of Life Research, 15(6), 1005–1021. doi:10.1007/s11136-005-5994-6.
Couturier, J. L., Speechley, K. N., Steele, M., Norman, R., Stringer, B., & Nicolson, R. (2005). Parental perception of sleep problems in children of normal intelligence with pervasive developmental disorders: Prevalence, severity, and pattern. Journal of the American Academy of Child and Adolescent Psychiatry, 44(8), 815–822.
Deeken, J. F., Taylor, K. L., Mangan, P., Yabroff, K. R., & Ingham, J. M. (2003). Care for the caregivers: A review of self-report instruments developed to measure the burden, needs, and quality of life of informal caregivers. Journal of Pain and Symptom Management, 26(4), 922–953.
EuroQol Group. (1990). EuroQol—A new facility for the measurement of health-related quality of life. Health Policy, 16(3), 199–208.
Feeny, D., Furlong, W., Torrance, G. W., Goldsmith, C. H., Zhu, Z., DePauw, S., et al. (2002). Multiattribute and single-attribute utility functions for the health utilities index mark 3 system. Medical Care, 40(2), 113–128.
Felce, D., & Perry, J. (1995). Quality of life: Its definition and measurement. Research in Developmental Disabilities, 16(1), 51–74.
Giallo, R., Wood, C. E., Jellett, R., & Porter, R. (2013). Fatigue, wellbeing and parental self-efficacy in mothers of children with an autism spectrum disorder. Autism, 17, 465–480.
Gurney, J. G., McPheeters, M. L., & Davis, M. M. (2006). Parental report of health conditions and health care use among children with and without autism: National survey of children’s health. Archives of Pediatrics and Adolescent Medicine, 160(8), 825.
Hamlyn-Wright, S., Draghi-Lorenz, R., & Ellis, J. (2007). Locus of control fails to mediate between stress and anxiety and depression in parents of children with a developmental disorder. Autism, 11(6), 489–501.
Hoefman, R. J., Van Exel, N. J. A., & Brouwer, W. B. F. (2011a). iVICQ. iMTA valuation of informal care questionnaire. Retrieved 02/12, Version 1.1 (December 2013), from http://www.bmg.eur.nl/english/imta/publications/questionnaires_manuals/ivicq/.
Hoefman, R. J., van Exel, J., & Brouwer, W. (2013a). How to include informal care in economic evaluations. PharmacoEconomics, 31(12), 1105–1119.
Hoefman, R. J., van Exel, J., & Brouwer, W. B. (2013b). Measuring the impact of caregiving on informal carers: A construct validation study of the CarerQol instrument. Health and Quality of Life Outcomes, 11(1), 173.
Hoefman, R. J., van Exel, N. J. A., Foets, M., & Brouwer, W. B. F. (2011b). Sustained informal care: The feasibility, construct validity and test–retest reliability of the CarerQol-instrument to measure the impact of informal care in long-term care. Aging & Mental Health, 15(8), 1018–1027.
Hoefman, R. J., Van Exel, N. J. A., Redekop, W. K., Looren-de Jong, S., & Brouwer, W. B. F. (2011c). A new test of the validity of the CarerQol instrument: Measuring ‘care-related quality of life’ of informal caregivers for use in economic evaluations. Quality of Life Research, 20(6), 875–887.
Hoefman, R. J., Van Exel, N. J. A., Rose, J. M., Lawerman-van de Wetering, E. J., & Brouwer, W. B. F. (2014). A discrete choice experiment to obtain a tariff for valuing informal care situations measured with the CarerQol instrument. Medical Decision Making, 34(1), 84–96.
Hoffman, L., Marquis, J., Poston, D., Summers, J. A., & Turnbull, A. (2006). Assessing family outcomes: Psychometric evaluation of the beach center family quality of life scale. Journal of Marriage and Family, 68(4), 1069–1083.
Hopkins, W. G. (2002). A new view of statistics: Effect magnitudes. Retrieved July 26, 2010, from http://www.sportsci.org/resource/stats/effectmag.html.
Karst, J. S., & Van Hecke, A. V. (2012). Parent and family impact of autism spectrum disorders: A review and proposed model for intervention evaluation. Clinical Child and Family Psychology Review, 15(3), 247–277.
Khanna, R., Madhavan, S. S., Smith, M. J., Patrick, J. H., Tworek, C., & Becker-Cottrill, B. (2011). Assessment of health-related quality of life among primary caregivers of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 41(9), 1214–1227.
Kuhlthau, K., Hill, K. S., Yucel, R., & Perrin, J. M. (2005). Financial burden for families of children with special health care needs. Maternal and Child Health Journal, 9(2), 207–218.
Kuhlthau, K., Kahn, R., Hill, K. S., Gnanasekaran, S., & Ettner, S. L. (2010a). The well-being of parental caregivers of children with activity limitations. Maternal and Child Health Journal, 14(2), 155–163.
Kuhlthau, K., Kovacs, E. A., Hall, T., Clemmons, T., Orlich, F., Delahaye, J., et al. (2013). Health-related quality of life for children with ASD: Associations with behavioral characteristics. Research in Autism Spectrum Disorders, 7(9), 1035–1042.
Kuhlthau, K., Orlich, F., Hall, T. A., Sikora, D., Kovacs, E. A., Delahaye, J., et al. (2010b). Health-related quality of life in children with autism spectrum disorders: Results from the autism treatment network. Journal of Autism and Developmental Disorders, 40(6), 721–729.
Kuo, D. Z., Cohen, E., Agrawal, R., Berry, J. G., & Casey, P. H. (2011). A national profile of caregiver challenges among more medically complex children with special health care needs. Archives of Pediatrics and Adolescent Medicine, 165(11), 1020.
Marks, N. F., Lambert, J. D., & Choi, H. (2002). Transitions to caregiving, gender, and psychological well-being: A prospective US national study. Journal of Marriage and Family, 64(3), 657–667.
McConachie, H., & Diggle, T. (2007). Parent implemented early intervention for young children with autism spectrum disorder: A systematic review. Journal of Evaluation in Clinical Practice, 13(1), 120–129.
Myers, B. J., Mackintosh, V. H., & Goin-Kochel, R. P. (2009). “My greatest joy and my greatest heart ache:” Parents’ own words on how having a child in the autism spectrum has affected their lives and their families’ lives. Research in Autism Spectrum Disorders, 3(3), 670–684.
Osborne, L. A., McHugh, L., Saunders, J., & Reed, P. (2008). Parenting stress reduces the effectiveness of early teaching interventions for autistic spectrum disorders. Journal of Autism and Developmental Disorders, 38(6), 1092–1103.
Payakachat, N., Tilford, J. M., Brouwer, W. B. F., van Exel, N. J., & Grosse, S. D. (2011). Measuring health and well-being effects in family caregivers of children with craniofacial malformations. Quality of Life Research, 20(9), 1485–1495.
Pogany, L., Barr, R. D., Shaw, A., Speechley, K. N., Barrera, M., & Maunsell, E. (2006). Health status in survivors of cancer in childhood and adolescence. Quality of Life Research, 15(1), 143–157.
Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401.
Robinson, B. C. (1983). Validation of a caregiver strain index. Journal of Gerontology, 38(3), 344–348.
Sawyer, M. G., Bittman, M., La Greca, A. M., Crettenden, A. D., Harchak, T. F., & Martin, J. (2010). Time demands of caring for children with autism: What are the implications for maternal mental health? Journal of Autism and Developmental Disorders, 40(5), 620–628.
Seiber, W. J., Groessl, E. J., David, K. M., Ganiats, T. G., & Kaplan, R. M. (2008). Quality of well being self-administered (QWB-SA) scale. San Diego: Health Services Research Center, University of California.
Singer, G. H., & Floyd, F. (2006). Meta-analysis of comparative studies of depression in mothers of children with and without developmental disabilities. American Journal on Mental Retardation, 111(3), 155–169.
Smith, L. E., Seltzer, M. M., Tager-Flusberg, H., Greenberg, J. S., & Carter, A. S. (2008). A comparative analysis of well-being and coping among mothers of toddlers and mothers of adolescents with ASD. Journal of Autism and Developmental Disorders, 38(5), 876–889.
Streiner, D. L., & Norman, G. R. (2003). Health measurement scales: A practical guide to their development and use (3rd ed.). Oxford: Oxford University Press.
Strock, M. (2007). Autism spectrum disorders (pervasive developmental disorders). Bethesda: National Institute of Mental Health (NIMH).
Stuart, M., & McGrew, J. H. (2009). Caregiver burden after receiving a diagnosis of an autism spectrum disorder. Research in Autism Spectrum Disorders, 3(1), 86–97.
Tolkacheva, N., Van Groenou, M. B., De Boer, A., & Van Tilburg, T. (2011). The impact of informal care-giving networks on adult children’s care-giver burden. Ageing and Society, 31(1), 34.
van Campen, C., de Boer, A. H., & Iedema, J. (2013). Are informal caregivers less happy than noncaregivers? Happiness and the intensity of caregiving in combination with paid and voluntary work. Scandinavian Journal of Caring Sciences, 27, 44–50.
Van Durme, T., Macq, J., Jeanmart, C., & Gobert, M. (2012). Tools for measuring the impact of informal caregiving of the elderly: A literature review. International Journal of Nursing Studies, 49(4), 490–504.
Van Exel, N. J., Brouwer, W. B., Van den Berg, B., Koopmanschap, M. A., & Van den Bos, G. A. (2004a). What really matters: An inquiry into the relative importance of dimensions of informal caregiver burden. Clinical Rehabilitation, 18(6), 683–693.
Van Exel, N. J., op Reimer, W. J. S., Brouwer, W. B., Van den Berg, B., Koopmanschap, M. A., & Van den Bos, G. A. (2004b). Instruments for assessing the burden of informal caregiving for stroke patients in clinical practice: A comparison of CSI, CRA, SCQ and self-rated burden. Clinical Rehabilitation, 18(2), 203–214.
Zarit, S. H., Reever, K. E., & Bach-Peterson, J. (1980). Relatives of the impaired elderly: Correlates of feelings of burden. The Gerontologist, 20(6), 649–655.
Acknowledgments
The project was supported by a grant (no. R01MH089466) from the National Institute of Mental Health with JMT and KAK serving as principal investigators. JMT also was supported by the Translational Research Institute (TRI), grant UL1TR000039 through the NIH National Center for Research Resources and National Center for Advancing Translational Sciences. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Mental Health or the National Institutes of Health. The authors acknowledge the members of the ATN for use of the data. The data for the study were collected as part of the ATN, a program of Autism Speaks. Further support came from a cooperative agreement (UA3MC11054) from the U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Research Program, to the Massachusetts General Hospital. The work described in this article represents the independent efforts of the authors with no restrictions from the funding source or the ATN. None of the authors of this study reported a conflict of interest associated with the preparation of the manuscript. Maria Melguizo, Nupur Chowdhury, Rebecca Rieger and Latunja Sockwell provided excellent research assistance.
Conflict of interest
None of the authors of this study reported a conflict of interest associated with the preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hoefman, R., Payakachat, N., van Exel, J. et al. Caring for a Child with Autism Spectrum Disorder and Parents’ Quality of Life: Application of the CarerQol. J Autism Dev Disord 44, 1933–1945 (2014). https://doi.org/10.1007/s10803-014-2066-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-014-2066-1