
Abstract
Parents of children with autism spectrum disorder are known to experience more stress than parents of children with any other conditions. The current study describes the parental stress of 118 fathers and 118 mothers at the onset of their children’s Early Intensive Behavioral Intervention program. The objectives of the study were to compare and analyze each parent’s stress and to identify factors that might predict their stress. Results indicated that fathers reported higher levels of stress than mothers. Correlations indicated that the stress levels of both parents were associated with their child’s age, intellectual quotient, severity of autistic symptoms, and adaptive behaviors. Paternal stress, but not maternal stress, was predicted by severity of autistic symptoms and child’s gender. Results are discussed in terms of their implications for services and early interventions.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The period of early childhood is a phase of family life that is likely to cause stress for parents. This is due to several challenges such as the reconciliation of work, couple, family and child care (Koeske and Koeske 1990; Williford et al. 2007). This phase of child development can be especially stressful for families of children with developmental disabilities (DD) such as autism spectrum disorders (ASD), as the characteristics related to these disorders may complicate the overall challenges for families. A considerable number of studies show that parents of children with ASD report higher stress levels than parents of typical children or parents of children with other difficulties (Baker-Ericzen et al. 2005; Blacher and McIntyre 2006; Bouma and Schweitzer 1990; Dumas et al. 1991; Holroyd and McArthur 1976; Mugno et al. 2007; Olsson and Hwang, 2001; Sanders and Morgan 1997; Wolf et al. 1989). Recent data on the issue of stress for families of children with ASD reported mainly about stress as perceived by the mothers (Baker-Ericzen et al. 2005; Griffith et al. 2010; Peters-Scheffer et al. 2012; Phetrasuwan and Miles 2009; Tomanik et al. 2004), from samples of families with children of varying age groups (Baker-Ericzen et al. 2005; Hastings 2003; Ingersoll and Hambrick 2011). Many of these studies focused on a relatively small number of families (Bendixen et al. 2011; Hastings 2003; Rodrigue et al. 1992). While a number of studies have documented factors associated with stress in families of children with ASD, the factors considered are mainly children’s severity of autistic symptoms or level of functioning (Bebko et al. 1987; Benson 2006; Freeman et al. 1991; Hastings and Johnson 2001; Kasari and Sigman 1997; Konstantareas and Homatidis 1989; Szatmari et al. 1994). The present article reports the results of a study investigating the perceived parental stress of 118 families of children with ASD aged 2–5 years, before obtaining Early Intensive Behavioral Intervention (EIBI) services from a public agency. The stress levels perceived by both parents are compared as well as the child and family characteristics and the time delay for services that may influence those stress levels. The article further reports which child, family and services (time on waiting list) characteristics are the best predictors of stress for each parent.
The Evaluation of Stress Perceived by Families of Children with ASD
Studies on parental stress converge on data demonstrating higher stress among families of children with ASD compared to families with typically developing children or children with other DDs (Baker-Ericzen et al. 2005; Dumas et al. 1991). Studies have also reported more depression and lower quality of life in these families compared to those with children with other DDs, physical disabilities, or chronic health conditions (Bouma and Schweitzer 1990; Mugno et al. 2007; Olsson and Hwang 2001; Sanders and Morgan 1997; Wolf et al. 1989). In a recent study by Ingersoll and Hambrick (2011) on 149 parents (136 mothers and 13 fathers) of children with ASD under the age of 18, 85 % reported stress levels reaching a clinically significant threshold. Other studies have reported more modest rates, for example Kayfitz et al. (2010) found that 26 % of parents reported clinically significant stress levels on a parental distress measure. The heterogeneity of results on parental stress may be due to differences in the study methods, including the composition of the participants (e.g. family origin, age of children, number of participants, period in family life cycle) and the tools used to measure stress. Some studies favor the use of a tool subjectively measuring parents perceived stress levels in conjunction with other measures (e.g. Herring et al. 2006); others are based on standardized and validated tools. For the latter, most studies use the Parental Stress Index (PSI; Abidin 1995; e.g. Anthony et al. 2005; Baker-Ericzen et al. 2005; Bendixen et al. 2011; Hall and Graff 2011; Ingersoll and Hambrick 2011; Kayfitz et al. 2010; Lecavalier et al. 2006; Davis and Carter 2008; Strauss et al. 2012). However, even among these studies, the clinical threshold used for determining significant stress levels is not uniform. In addition, the type of data (e.g. continuous or dichotomous, variable cutting point) used to express the measurement may also lead to different results between studies.
Stress in Fathers and Mothers of Children with ASD
Authors of recent studies on parental stress in families of children with ASD reported that few studies have systematically examined stress in fathers and the variables related to their stress levels (notably Bendixen et al. 2011; Flippin and Crais 2011). Davis and Carter (2008) reported that although historically mothers have been the primary informants in studies, fathers are increasingly included in research programs, as researchers recognize the importance of paternal involvement. However, even when included in such studies, fathers mainly represent a smaller proportion than mothers. Most studies that include fathers focus on relatively small and non-equivalent samples, ranging from 11 (Hastings and Johnson 2001) to 61 (Hastings et al. 2005a, b), a fact that makes it difficult to generalize results to all fathers of young children with ASD. More studies are needed on parental stress and paternal stress, in particular, in order to better understand the nature and the predictors of this stress. Moreover, paternal involvement could be a good predictor of a child’s cognitive, emotional, and social development outcomes (Shannon et al. 2002).
That being said, there are a number of studies that compare maternal and paternal stress and well-being. The majority of these studies have reported that more mothers than fathers reach the threshold of significant stress levels (see Hastings 2003; Hastings and Brown 2002; Hastings et al. 2005a, b; Herring et al. 2006; Konstantareas et al. 1992; Milgram and Atzil 1988; Wolf et al. 1989). Baker-Ericzen et al. (2005) conducted a study with a relatively large number of fathers of preschool children with ASD. They compared 27 fathers and 37 mothers of children with ASD to 16 fathers and 23 mothers of typically developing preschoolers. On the PSI, 35 % of fathers and 59 % of mothers in the ASD group reported having significantly high levels of parental stress in the child domain, compared to 13 % of fathers and 17 % of mothers in the typical group. In regard to the parent domain, the study reported significantly higher stress levels for 24 % of mothers and 15 % of fathers of children with ASD compared to 9 % of mothers and 0 % of fathers of children with typical development.
It is important to note that some studies have shown that fathers and mothers of children with ASD reported comparable stress levels (for example, Hastings 2003; Davis and Carter 2008). These studies differ from others in that they included more fathers and also evaluated more equivalent samples of mothers and fathers. For example, Davis and Carter (2008) compared the overall perceived stress among 54 mothers and 54 fathers of young children newly diagnosed with ASD and found that 39 % of mothers scored in the clinical range for parental stress levels, compared to 28 % of fathers. One hypothesis to explain these more similar stress levels between parents in recent studies was that fathers were spending increasingly more time with their child and were more directly involved than the fathers of previous generations were (Pleck and Masciadrelli 2004).
Factors Related to Parental Stress and ASD
The majority of recent studies that focus on the factors associated with parental stress in ASD assessed the relationship between individual characteristics of the children and the parents’ stress. As reported by Hastings (2003), the most studied variables are the severity of the child’s disability (intellectual quotient, functional impairment, difficulty of care) and problem behaviors. Some studies have also documented the relationship between families’ sociodemographic characteristics and parental stress (Ingersoll and Hambrick 2011; Anthony et al. 2005; Hall and Graff 2011). One study documented the relationship between parenting stress and the coping strategies used by both parents. It showed that the stress levels of parents of preschool and school-aged children with ASD were associated with the coping strategies used by the parents and their psychological health (Hastings et al. 2005a, b). Active avoidance strategies for mothers and fathers were associated with more stress, as well as anxiety and depression symptoms. Mothers and fathers could use specific coping strategies, which may have different effects on their stress levels.
To return to the characteristics of children associated with family stress in general, studies of families with young children with DD have indicated that the severity of a child’s impairments are important factors related to parental stress (Tobing and Glenwick 2002). More specific, in the field of ASD, stress and depressive elements reported by families have been found to be related to their reports of their child’s degree of impairment including the severity of cognitive (Baker-Ericzen et al. 2005) and language impairments (Bebko et al. 1987), social deficits (Baker-Ericzen et al. 2005; Davis and Carter 2008), emotional problems and behaviors (Hastings 2003; Hastings et al. 2005a, b; Herring et al. 2006; Lecavalier et al. 2006; Davis and Carter 2008) and overall autism severity (Baker-Ericzen et al. 2005; Bebko et al. 1987; Benson 2006; Freeman et al. 1991; Hastings and Johnson 2001; Ingersoll and Hambrick 2011; Kasari and Sigman 1997; Konstantareas and Homatidis 1989; Szatmari et al. 1994; Tobing and Glenwick 2002). The findings about the relationship between a child’s gender, chronological age, and parental stress are inconsistent. One study has not found any relationship between child’s characteristic and parental stress (Lecavalier et al. 2006). Other authors reported that an earlier diagnosis is associated with greater stress, which does not systematically decline once a diagnosis has been received; while a later diagnosis is related to decreased stress (Osborne et al. 2008).
In terms of variables specifically related to the stress of fathers, Hastings et al. (2005a, b) showed that the stress of fathers who have a preschool child with ASD is more related to the depression of the mothers than to children’ characteristics themselves. Relatedly, Kayfitz et al. (2010) suggested that fathers’ experiences do not occur in isolation of mothers’ mental health, such as stress and depression.
Despite recent advances in the scientific literature on the stress of fathers of children with ASD, studies on the subject are still scarce. In order to be able to provide appropriate services to families, more studies must be conducted to document the issue more thoroughly. These studies should include a larger number of families who have a child with ASD, in the same age range, at the same stage in the family life cycle, with an equal number of fathers and mothers. Furthermore, to the best of our knowledge, no study has examined the effects of waiting times for specialized services on parental stress levels. This variable may have a considerable impact on the levels of stress experienced by parents of young children who have recently received an ASD diagnosis.
Objectives
The objectives of the current study were to (1) describe and compare the perceived stress of fathers and mothers of children with ASD, before they received specialized services (EIBI) from a public agency, (2) analyze the relationships between perceived stress of both parents and the child and family characteristics as well as the waiting delay before access to services., and (3) identify which of these variables that might predict parental stress.
Method
Participants
One hundred and eighteen families (118 fathers and 118 mothers) were recruited at the time of their child’s registration in a public agency offering specialized services to children and adults with developmental delays in Quebec, Canada. This recruiting strategy yielded a study sample that was reasonably homogenous in terms of services to be received (i.e., EIBI), as well as in terms of the step in the intervention process (i.e., following the child’s ASD diagnosis and immediately after beginning intensive behavioural intervention), and stage in the family life cycle (i.e., young children) at which participants were queried.
All participants came from a largely francophone area south of Montreal. The inclusion criteria for the children in the study were that they (a) had received a diagnosis of pervasive developmental delay (PDD), according to the DSM-IV R (American Psychiatric Association 2000), diagnosis that was confirmed by a multidisciplinary evaluation team specialized in autism included a child psychiatrist, (b) were between 2 to 5 years old, and (c) had parental consent to participate in the study. The first inclusion criteria, having a diagnosis of PDD, included autism, Asperger’s syndrome, Pervasive Developmental Disorders-Non Specified (PDD-NOS). Diagnoses of Rett syndrome and Childhood Disintegrative Disorders were not included in this current study. The inclusion criteria for parents were that a) both parents agreed to participate and b) both parents completed all research assessments required. The children (92 boys, 26 girls) were between 2 years, 9 months-old and 5 years, 1 month-old, with an average age of 4 years-old (SD = .61). Demographic information on families, such as parental income, level of education, and occupation are presented in Table 1.
Materials
Severity of Autistic Symptoms
The public agency therapists used the Childhood Autism Rating Scale (CARS; Schopler et al. 1988) to rate the severity of each child’s autistic symptoms. The CARS consists of 15 items assessed on an ordinal scale from 1 to 4 (no problems to severe problems). Scores vary from 15 to 60, with a higher score reflecting a higher severity of autistic symptoms. The internal consistency is excellent (.94). The test–retest reliability (.88), inter-rater reliability (.71) and test validity (.80–.84) are also strong (Schopler et al. 1988).
Intellectual Functioning
The participants’ intellectual functioning was measured using the Wechsler Preschool and Primary Scale of Intelligence (WPPSI-III, Wechsler 2002), for preschool children aged between 2 years, 5 months and 7 years, 3 months. The WPPSI-III provides a verbal intellectual quotient (VIQ), a performance intellectual quotient (PIQ), a full scale intellectual quotient (FSIQ), and a general language composite (GLC). Scores can vary from 40 to 160. The WPPSI-III has demonstrated excellent internal consistency (.86–.97) and test–retest (.84–.92) reliability and validity for both children with and without developmental disabilities (Wechsler 2002).
Adaptive Behaviors
The Adaptive Behavior Assessment System-II (ABAS-II; Harrison and Oakland 2003) measures the adaptive behavior of a person from birth to 89 years old, in various spheres of daily life. In this study, the parent/primary caregiver form (ages 0–5) was used. The tool refers to the three domains recognized by the American Association for Intellectual and Developmental Disabilities (AAIDD American Association on Intellectual and Developmental Disabilities 2011; Schalock et al. 2010) as being necessary to assess adaptive behaviors, which are Conceptual, Social, and Practical, as well as a General Adaptive Composite (GAC). It includes 241 items and between 22 and 27 items in each domain. In order to score an item, the parent or caregiver must assess whether the child currently performs the task independently in daily life on a scale of 4 (0 = unable to 3 = always or almost always able to when needed). The scores vary from 40 to 160. A higher score on the ABAS-II indicates more adaptive behaviors in the child’s repertoire. The internal consistency (.98–.99) and the test–retest reliability (.90) demonstrate the strong reliability of the tool (Harrison and Oakland 2003). When compared to the Vineland Adaptive Behavior Scale (VABS: Sparrow et al. 2005), the correlations between the two tools were relatively high (.70–.84).
Parental Stress
The Parenting Stress Index-Short Form (PSI/SF; Abidin 1995) assesses the perceived stress of parents of children between 3 months and 10 years-old. Both mothers and fathers completed an individual version of the PSI/SF without consulting each other. The short-form version of the PSI is comprised of 36 items divided into 3 subscales: Parental Distress, Parent–Child Dysfunctional Interaction, and Difficult Child. It also includes a total parental stress score. The total score can vary from 36 to 180; subscales vary from 13 to 65. Items are rated in a 5-point Likert scale ranging from strongly disagree to strongly agree, where a higher score means more stress. Abidin (1995) established that a total score of 112 corresponds to the 95th percentile of stress, when compared to parents of typical children. Total Stress is designed to evaluate the overall level of parenting stress that one can experience. The Parental Distress subscale evaluates the distress a parent experiences in his or her role as a parent, such as, “Since having my child, I have been unable to try new and different things”. The Parent–Child Dysfunctional Interaction subscale examines parents’ perceptions about their relationship and interactions with their child, such as, “My child rarely does things for me that make me feel good”. The Difficult Child subscales evaluate parents’ perceptions about their child’s characteristics, such as, “My child gets easily upset over the smallest things”. The internal consistency for the Short version of the PSI (.40–.63) and the test–retest reliability (.68–.85) demonstrate the strong reliability of the tool (PSI/SF; Abidin 1995). Alphas range from .73 to .86 for mothers and .77–.87 for fathers on the three subscales and the total score (PSI/SF; Abidin 1995).
Waiting Times
Information regarding waiting times for services were acquired from the rehabilitation center’s computer database. These data are gathered when the center receives a request for rehabilitation services. This request may originate from the parent or from a professional (e.g. a psychologist or physician). Waiting times are therefore measured from the moment at which the request is made until EIBI services are received.
Procedures
The research protocol was evaluated and approved by the Joint Research Ethics Board for the public developmental service agencies in Quebec.
In order to recruit participants, the researchers met with each of the eligible families before they began receiving services from the public agency. The objective of this initial meeting was to present the research, its objectives, and the parameters of the parents’ and children’s participation. It was made clear that participation in the study was voluntary and that a refusal to participate would not have an influence on the services that their children and family would receive. Every parent that wanted to participate in the study completed a consent form and gave clear informed consent prior to various data collection. Following these consent procedures and prior to obtaining services, an interview with each family was conducted. During the interview, a research assistant completed a sociodemographic questionnaire, the PSI/SF, and the ABAS-II with the parents. When only one parent was present, the questionnaires and an envelope with return address were delivered to the absent parent by the parent that was present, or they were sent by mail. During the completion of the questionnaires, another research assistant performed the WPPSI-III with the child in another room. The CARS was performed after 2 months of services, to enable the public agency therapist to get to know the child better.
Statistical Analysis
Information on the children and their families was computed with descriptive statistics. Paternal and maternal stress levels were compared with t-tests and bivariate analyses were performed. Finally, hierarchical regression analyses were used to identify the child characteristics (age, gender, clinical profile), family characteristics (income, level of education, and length of delay before service) that best predicted paternal and maternal stress distinctively, at the beginning of services. Regression analyses were carried out in four steps. First, the effect of the child’s age, a potential mediator, was tested. Second, the child’s gender was entered in the model. Third, waiting time and maternal education level, contextual variables that were correlated with the dependent variable (i.e., fathers’ and mothers’ stress), were entered. Finally, after accounting for variance explained by the aforementioned variables, the effect of the child’s intellectual functioning and adaptive behaviors, as well as the severity of his or her autistic symptoms, and were entered as predictors of parents’ stress. Furthermore, the mediating effect of the child’s age was tested. The first precept was examined (i.e., a correlation between the independent variables and the identified mediator). Severity of autistic symptoms was related to children’s age (r = −.39**), with younger children displaying more severe autistic symptoms. The mediator variable was not related to intellectual functioning or adaptive behaviors.
Results
Children’s Characteristics
The children’s mean IQ was 74.13 (SD = 22.06), ranging from 42 to 128. On the scale evaluating the severity of autistic symptoms (CARS), the children had a mean of 31.16 (SD = 8.22), with scores ranging from 17 to 51.50, where a higher score corresponds to more severe autistic symptoms. The children’s scores on adaptive behaviors (ABAS-II) were between 42 and 130 (M = 66.20, SD = 15.29), where a child with a higher score would have more adaptive behaviors.
Parental Stress
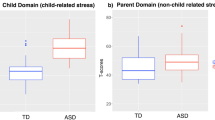
The mean of the parents’ total stress score on the PSI-SF was 116.30 (SD = 20.48). Table 2 presents the paternal and maternal average stress scores for each subscale of the PSI-SF. Fathers reported a significantly higher level of Total Stress than mothers (M of 118.35 and 112.38, respectively), t (117) = −3.83, p < .001. Stress levels reached a clinical score in 60.6 % of fathers and 54.1 % of mothers. Fathers had significantly higher stress scores in all subscales except the Parent–Child Dysfunctional Interaction subscale. The differences between fathers and mothers were statistically significant for Parental Distress, t (117) = −3.02, p < .01, and Difficult Child, t (117) = −4.54, p < .001. Both the paternal and maternal highest stress scores were in the Parental Distress subscale.
Correlates of Stress Levels
Correlations between stress levels and other variables studied revealed that for both fathers and mothers, stress was associated with waiting time for services and maternal education level, as well as with the child’s age, gender, IQ, symptom severity, and adaptive behaviors (Table 3). Fathers’ stress levels (total stress, Parental Distress, and Difficult Child) were associated with the child’s gender and age; fathers’ scores on the Parent–Child Dysfunctional Interaction subscale were associated only with the child’s age. Mothers’ stress levels (total stress and score on all three subscales) were related to the child’s age. Both parents reported higher levels of stress when their child was female or older (i.e., closer to 5 years in age). Regarding contextual variables, fathers’ score on the Difficult Child subscale and mothers’ total stress were associated with waiting times (i.e., longer waiting times were associated with higher stress levels). Fathers’ scores on the Parental Distress subscale were associated with the mother’s education (i.e., lower education levels were associated with higher levels of stress). Fathers’ educational attainment and family income were not significantly associated with stress. Fathers’ total stress (and scores on each of the three subscales) was also associated with variables linked to the child’s clinical profile. Specifically, higher stress levels among fathers were associated with less severe autistic symptoms and more adaptive behaviors. Similar associations were found among mothers (total stress, Difficult Child and Parent–Child Dysfunctional Interaction), although mothers’ Parental Distress scores were only associated with their child’s adaptive behaviors. Finally, scores on the Parent–Child Dysfunctional Interaction subscale were associated with children’s IQ, with higher intellectual functioning being associated with higher stress levels among fathers and mothers.
Regression Analysis
The last objective was to identify the best predictors of parental stress. For this purpose, hierarchical analyses were conducted. The first step of these analyses sought to test the mediating effect of the child’s age. The second step examined the role of the child’s gender. The third step included maternal education level and waiting times for services into the regression model. The last step took into account the child characteristics related to ASD, such as intellectual abilities, severity of autistic symptoms, and adaptive behaviors. Table 4 presents the results for fathers and mothers separately, for the PSI-SF total score and the three subscales.
As shown in Tables 4 and 5, on the first step of the regression, mothers’ total stress and scores on the three subscales were predicted by the child’s age (explaining 13.0, 7, 10 and 14 % of variance, respectively) whereas on the second step, the child’s gender explained fathers’ total stress and score on the Parent–Child Dysfunctional Interaction subscale (explaining 7 and 2 % of variance, respectively). In the third step, waiting times for services and maternal education levels added only to the prediction of mothers’ scores on the Parent–Child Dysfunctional Interaction subscales (3 % of explained variance). The last step added 17 and 10 % of explained variance to the prediction of paternal and maternal total stress; fathers’ total stress was predicted by the child’s adaptive behaviors. Mothers’ total stress was also predicted by the child’s adaptive behaviors and intellectual functioning. The full model explained 28 % of variance in paternal total stress, F (7,117) = 7.66, p < .001, and 24 % in maternal total stress, F (7,117) = 6.59, p < .001. Results on all three subscales are presented in Tables 4 and 5.
The mediating effect of the child’s age was only significant for maternal stress, as measured by the main scale (z = −3.68) and the three subscales (z = −2.17, −3.38, −6.28, respectively), following results obtained from a Sobel test. Children’s age was not a mediator of paternal stress.
Discussion
This study focused on the parental stress of young children with ASD. It targeted both parents and aimed at evaluating fathers’ and mothers’ stress in an equivalent sample. This sample offered the advantages of a large size (118 fathers and 118 mothers), the homogeneity of circumstances (at their entry into EIBI services), the same evaluation conditions for all children and the same period in the life cycle of the families (preschool aged children). The main objectives of this study were to describe and compare fathers’ and mothers’ stress, to identify factors related to parental stress levels, and to identify the best predictors of fathers’ and mothers’ stress separately. This is a key concern since parental stress is an important predictor of both parent and child behaviors and dyadic interaction (Crnic et al. 2005) and has an impact on intervention (Strauss et al. 2012).
Consistent with previous studies (e.g. Baker-Ericzen et al. 2005; Blacher and McIntyre 2006; Bouma and Schweitzer 1990), the results of this study showed that many parents of children with ASD report levels of stress reaching a clinical threshold (cut-off at 95th percentile). The percentage of parents experiencing significant stress levels exceeds that of other studies with comparable families of preschool aged children (e.g. Davis and Carter 2008), despite having chosen a more strict clinical threshold compared to other studies. These results are consistent with Cox et al. (1999) and Davis and Carter (2008) who reported that parents who have just recently received a diagnosis of ASD for their child and who are at the commencement of services, are in a particularly stressful period. This finding demonstrates the importance of providing formal support to families during this critical period, that is, after receiving a diagnosis and while waiting to receive services.
An interesting finding in this study is that mothers and fathers both reported a higher level of stress related to their parental roles (parent domain) rather than to child characteristics or the parent–child relationship (child domain). These findings are different than those of other studies, where parents perceived more stress in the child domain subscales. For example, Baker-Ericzen et al. (2005) reported that 35 % of fathers and 59 % of mothers showed significant stress in the child domain of the PSI/SF, compared to 15 % of fathers and 24 % of mothers in the parent domain. This difference in stress rates in the parent domain between our study and others highlights the fact that parents who have just received a diagnosis for their child and are waiting for early intervention services need to receive support during this time, as they must learn to define their role as a parent of a child with ASD. Parents would benefit from training on different topics related to ASD characteristics, efficient parenting practices for children with ASD, and information on available services.
In this study, fathers reported higher levels of stress than mothers, and more fathers (61 %) than mothers (54 %) scored in the clinical range. Previous studies have shown the inverse, more perceived stress in mothers than fathers (e.g. Baker-Ericzen et al. 2005; Herring et al. 2006). Another study however noted that fathers were more stressed by certain behaviors of children with ASD than the mothers. Davis and Carter (2008) reported that more mothers than fathers scored in the clinical range for parental stress, but the fathers seemed to have more difficulty interacting with their children with autism. Several hypotheses can be made with regard to our data on fathers perceiving more stress than mothers, likewise to the majority of other studies on the subject. First, we must understand why the results of fathers’ stress are higher than those of previous studies in general. As noted in literature, fathers of children with DD have a history of being perceived as the “peripheral parent” (Herbert and Carpenter 1994) or even the “invisible parent” (Ballard et al. 1997) (see MacDonald and Hastings 2010). Research design in the field of parenting in DD is typically framed by the concept of maternal caregiving (MacDonald and Hastings 2010; Marsiglio et al. 2000). Higher stress data among fathers in our study could be explained by the fact that our sample includes a more representative number of fathers compared to previous studies, and thereby paints a more complete picture of the situation. Another possible explanation for our results regarding the difference between mothers’ and fathers’ stress levels may relate to the proportion of time that each parent spends caring for the child and at work. In this study, more fathers than mothers worked full time. Programs and meetings having to do with the child primarily occur during daytime hours and do not accommodate fathers’ professional lives (see MacDonald and Hasting, MacDonald and Hastings 2010). Mothers may therefore be more aware of services and be more likely to participate in appointments with clinical team that provide services. Fathers may thus experience higher levels of stress because they missed important information and discussions regarding the intervention plan for their child.
It is however important to note that significant associations were found between mothers’ and fathers’ stress. As in Kayfitz and colleagues (Kayfitz et al. 2010), maternal and paternal stress was significantly related. Indeed, when fathers reported a higher level of stress, mothers did too. These results confirm the need for a more systematic support, as one parents’ stress is closely linked to that of the other.
Parental stress in our study was associated with the child’s age, intellectual functioning, adaptive behaviors, and severity of autistic symptoms. However, the direction of the associations between those characteristics and parental stress is different than the one found in the scientific literature. Previous studies reported that more severe autistic symptoms lower IQ, and less adaptive behaviors were associated with more parental stress (e.g. Benson 2006; Baker-Ericzen et al. 2005; Hall and Graff 2011; Hastings and Jonhson 2001; Ingersoll and Hambrick 2011; Tobing and Glenwick 2002). In our study, levels of stress were correlated with older children (5 years old compare to 2 years old), with less autistic symptoms, more adaptive behaviors, and better intellectual functioning. These results have to be placed into the context of the current state of public services in Quebec, Canada, to be better understood. Older children from this sample (average of 4 years-old) might start regular school after only 1 year of intervention (at 5 years old) while the younger children might benefit from one to two further years of intervention before the big step to elementary school. The parents of 4 year-olds may feel more stress due to the anticipation of their child’s transition to school in the near future. Also, when children are younger, as in this sample, a lack of adaptive behaviors (e.g. self-care, alimentation) is somehow more easily manageable or seen as less abnormal than when children are older (Hall and Graff 2011). Our hypothesis is that this higher level of stress for parents of older children might be better understood in light of age-expected social-emotional competencies (Briggs-Gowan and Carter 1998). Parents of a child with ASD might experience more stress due to the delays in acquiring such age-expected competencies.
In terms of the inverse relation between parental stress and severity of autistic symptoms and level of adaptive and intellectual functioning that is usually seen in literature, one hypothesis is that when children display more ambiguous autistic symptoms, such as children with higher functioning (i.e., less autistic symptoms, higher intellectual functioning and more adaptive behaviors) parents might be more ambivalent about the diagnoses. Conversely, parents dealing with more symptomatic children might benefit from an earlier diagnosis and therefore more services. In regard to the intervention context in this study, children with a more ambiguous diagnosis or milder symptoms may have possibly been diagnosed later. This could be due to a later request for evaluation by the parents or to the fact that assessment clinics had more reservations about making a diagnosis. It is also possible that the parents, whose children were diagnosed earlier because of more severe symptoms, have been informed that they gone a received more years of intervention from the public intervention center than children with a higher level of functioning. It is thus conceivable that when more amount of time of services are offered, parental stress can slightly decrease compared to those who’s older and will receive less amount of intervention before school. Interestingly, total stress for mothers and Difficult Child for fathers were associated with waiting delay before services, where more delay was associated with more stress. Children with more severe symptoms may be given priority for early intervention, and these shorter waiting times may, in turn, influence parental stress.
In this study, the final model of paternal stress and maternal stress predicted 28 and 24 % of variance, respectively. Paternal and maternal stress were predicted in part by the child’s characteristics. In particular, mothers’ stress (total stress and scores on the three subscales) was predicted by the child’s age, which was identified as a mediating variable for mothers, with mothers of older children displaying higher stress levels. A similar association was found in Tobing and Glenwick (2002), where mothers of older children with PDD-NOS reported higher levels of stress. Children’s age was not found to have a mediating effect on fathers’ stress. Furthermore, the father’s stress (i.e., total stress and score on the Parent–Child Dysfunctional Interaction subscale), but not the mother’s stress, was predicted by the child’s gender, with fathers of girls reporting higher levels of stress. Among the contextual factors examined, only waiting times for services and mothers’ level of education predicted mothers’ scores on Parent–Child Dysfunctional Interaction.
Regarding characteristics related to the child’s clinical profile, a main result of this study was that adaptive behaviors were the most consistent predictors of fathers’ and mothers’ perceived stress (with the exception of fathers’ Parent–Child Dysfunctional Interaction subscale scores). Both parents reported more stress when their child displayed more adaptive behaviors. As discussed earlier, this association between adaptive behaviors and parental stress reports differs from earlier reports, in which parents expressed more stress when their children with ASD presented adaptive difficulties. Again, this may be explained by the fact that the children with milder symptoms have been diagnosed later in life and that their parents were told that they would receive fewer services before entering school. Other studies have found that intellectual abilities were good predictors of maternal stress levels (Baker-Ericzen et al. 2005). In this study, IQ was a good predictor of both mothers’ and fathers’ stress as measured by the Difficult Child subscale, as well as total stress reported by mothers. The severity of children’s autistic symptoms was only a predictor of fathers’ score on the Parent–Child Dysfunctional Interaction subscale. Finally, variables associated with the child’s clinical profile (AB for both parents’ and IQ for mothers only) were the best predictors of total stress, beyond age, gender, and contextual variables (i.e., waiting times and mothers’ education).
The results of this study must be interpreted in light of its methodological limitations. For instance, the instrument used to measure stress only assessed parent’s family-related stress and therefore did not take into account other stressors that could influence a parent’s stress levels. Other information such as social support, which could influence perceived parental stress, were not included in this study. Finally, the correlational design of the present study does not allow the determination of causal relationships between parental stress and children’s characteristics. These relationships should be understood through an bidirectional influences that may exist between the variables of interest.
Conclusion
The results of this study highlight several aspects of stress and the family life-cycle that must be considered when planning services for families of young children with ASD, including: (1) the age of the children (stress can be experienced differently among parents depending on whether the child is very young compared to being older); (2) the point in time a diagnosis has been received (stress may vary according to the steps that parents have had to go through to get the diagnosis and according to their acceptance thereof); (3) the moment when the family will receive services and the types of services they will receive (stress may vary for example if the parent is waiting for EIBI compared to a parent who is receiving services or if services are terminated and the child enters school). Also, different predictors of fathers’ and mothers’ stress underline the distinctive experience for both parents of a child with ASD. Parental stress is an important factor that affects parents and the child, as well as the quality of their relationships. Parental stress is therefore an excellent indicator that should be considered in intervention. At the clinical level, parents of children with higher functioning need support (based on their stress level) as much as parents of children with lower functioning. Parents of a child with ASD should benefit from direct and systematic intervention, distinct from those offered directly to the child. Parents of children with higher functioning should be better supported as they face different challenges than parents of more severely affected children, and those challenges are not necessarily easier. Our results also advocate for a better support for fathers. Interventions should aim to include them and enhance their involvement.
It is an important step in the advancement of knowledge in the field of autism to continue to study the stress of parents of young children with ASD and the related factors in that stress. Parental stress is related to parental involvement in their child’s intervention, their quality of life during intervention, and the family’s quality of life in general. Future studies will provide crucial information on possible support programs that could be implemented for families. Since different child aspects influence fathers and mothers stress, it would be wise to consider the needs of each separately to increase their collaboration and participation through various means.
References
Abidin, R. R. (1995). The parenting stress index (3rd ed.). Odessa, FL: Psychological Assessment Resources.
American Association on Intellectual and Developmental Disabilities. (2011). Intellectual disability: Definition, classification, and systems of supports (11th ed.). Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders—text revision (4th ed.). Washington, DC: Author.
Anthony, L. G., Anthony, B. J., Glanville, D. N., Naiman, D. Q., Waanders, C., & Shaffer, S. (2005). The relationship between parenting stress, parenting behaviour and preschoolers’ social competence and behaviour problems in the classroom. Infant and Child Development, 14(2), 133–154. doi:10.1002/icd.385.
Baker-Ericzen, M. J., Brookman-Frazee, L., & Stahmer, A. (2005). Stress levels and adaptability in parents of toddlers with and without autism spectrum disorders. Research and Practice for Persons with Severe Disabilities, 30(4), 194–204. doi:10.2511/rpsd.30.4.194.
Ballard, K., Bray, A., Shelton, E. J., & Clarkson, J. (1997). Children with disabilities and the education system: The experiences of fifteen fathers. International Journal of Disability, Development and Education, 44(3), 229–241. doi:10.1080/0156655970440305.
Bebko, J. M., Konstantareas, M. M., & Springer, J. (1987). Parent and professional evaluations of family stress associated with characteristics of autism. Journal of Autism and Developmental Disorders, 17(4), 565–576. doi:10.1007/BF01486971.
Bendixen, R. M., Elder, J. H., Donaldson, S., Kairalla, J. A., Valcante, G., & Ferdig, R. E. (2011). Effects of a father-based in-home intervention on perceived stress and family dynamics in parents of children with autism. American Journal of Occupational Therapy, 65(6), 679–687. doi:10.5014/ajot.2011.001271.
Benson, P. R. (2006). The impact of child symptom severity on depressed mood among parents of children with ASD: The mediating role of stress proliferation. Journal of Autism and Developmental Disorder, 36(5), 685–695.
Blacher, J., & McIntyre, L. L. (2006). Syndrome specificity and behavioral disorders in young adults with intellectual disability: Cultural differences in family impact. Journal of Intellectual and Developmental Disability, 50(3), 184–198. doi:10.1111/j.1365-2788.2005.00768.x.
Bouma, R., & Schweitzer, R. (1990). The impact of chronic childhood illness on family stress: A comparison between autism and cystic fibrosis. Journal of Clinical Psychology, 46(6), 722–730. doi:10.1002/1097-4679(199011)46:6<722:AIDJCLP2270460605>3.0.CO;2-6.
Briggs-Gowan, M. J., & Carter, A. S. (1998). Preliminary acceptability and psychometrics of the Infant-Toddler Social Emotional Assessment (ITSEA): A new adult-report questionnaire. Infant Mental Health Journal, 19(4), 422–445. doi:10.1002/(SICI)1097-0355(199824)19:4<422:AID-IMHJ5>3.0.CO;2-U.
Cox, A., Klein, K., Charman, T., Baird, G., Baron-Cohen, S., Swettenham, J., et al. (1999). Autism spectrum disorders at 20 and 42 months of age: Stability of clinical and ADI-R diagnosis. Journal of Child Psychology and Psychiatry, 40(5), 719–732. doi:10.1111/1469-7610.00488.
Crnic, K. A., Gaze, C., & Hoffman, C. (2005). Cumulative parenting stress across the preschool period: Relations to maternal parenting and child behaviour at age 5. Infant and Child Development, 14(2), 117–132. doi:10.1002/icd.384.
Davis, N. O., & Carter, A. S. (2008). Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: Associations with child characteristics. Journal on Autism and Developmental Disorders, 38(7), 1278–1291. doi:10.1007/s10803-007-0512-z.
Dumas, J. E., Wolf, L. C., Fisman, S. N., & Culligan, A. (1991). Parenting stress, child behavior problems, and dysphoria in parents of children with autism, Down syndrome, behavior disorders, and normal development. Exceptionality, 2(2), 97–110. doi:10.1080/09362839109524770.
Flippin, M., & Crais, E. R. (2011). The need for more effective father involvement in early autism intervention: A systematic review and recommendations. Journal of Early Intervention, 33(1), 24–50. doi:10.1177/1053815111400415.
Freeman, N. L., Perry, A., & Factor, D. C. (1991). Child behaviors as stressors: Replicating and extending the use of the CARS as a measure of stress: A research note. Child Psychology & Psychiatry & Allied Disciplines, 32(6), 1025–1030. doi:10.1111/j.1469-7610.1991.tb01927.x.
Griffith, G. M., Hastings, R. P., Nash, S., & Hill, C. (2010). Using matched groups to explore child behaviour problems and maternal well-being in children with Down syndrome and autism. Journal of Autism and Developmental Disorders, 40(5), 610–619. doi:10.1007/s10803-009-0906-1.
Hall, H. R., & Graff, J. C. (2011). The relationships among adaptive behaviors of children with autism, family support, parenting stress, and coping. Issues in Comprehensive Pediatric Nursing, 34(1), 4–25. doi:10.3109/01460862.2011.555270.
Harrison, P. L., & Oakland, T. (2003). Adaptive Behavior Assessment System—Second Edition. San Antonio, TX: The Psychological Corporation.
Hastings, R. P. (2003). Child behaviour problems and partner mental health as correlates of stress in mothers and fathers of children with autism. Journal of Intellectual Disability Research, 47(4–5), 231–237. doi:10.1046/j.1365-2788.2003.00485.x.
Hastings, R. P., & Brown, T. (2002). Behaviour problems of children with autism, parental self-efficacy, and mental health. American Journal on Mental Retardation, 107(3), 222–232. doi:10.1352/0895-8017(2002)107<0222:BPOCWA>2.0.CO;2.
Hastings, R. P., & Johnson, E. (2001). Stress in UK families conducting intensive home-based behavioral intervention for their young child with autism. Journal of Autism and Developmental Disorders, 31(3), 327–336. doi:10.1023/A:1010799320795.
Hastings, R. P., Kovshoff, H., Brown, T., Ward, N. J., degli Espinosa, F., & Remington, B. (2005a). Coping strategies in mothers and fathers of preschool and school-age Children with autism. Autism: The International Journal of Research and Practice, 9(4), 377–391. doi:10.1177/1362361305056078.
Hastings, R. P., Kovshoff, H., Ward, N., degli Espinosa, F., Brown, T., & Remington, B. (2005b). System analysis of stress and positive perceptions in mothers and fathers of pre-school children with autism. Journal of Autism and Developmental Disorders, 35(5), 635–644. doi:10.1007/s10803-005-0007-8.
Herbert, E., & Carpenter, B. (1994). Fathers-the secondary partners: Professional perceptions and a father’s recollections. Children and Society, 8(1), 31–41. doi:10.1111/j.1099-0860.1994.tb00412.x.
Herring, S., Gray, K., Taffe, J., Tonge, B., Swseeney, D., & Einfeld, S. (2006). Behaviour and emotional problems in toddlers with pervasive developmental delay: Associations with parental mental health and family functioning. Journal of Intellectual Disability Research, 50(12), 874–882. doi:10.1111/j.1365-2788.2006.00904.x.
Holroyd, J., & McArthur, D. (1976). Mental retardation and stress on the parents: A contrast between Down’s syndrome and childhood autism. American Journal of Mental Deficiency, 80(4), 431–436.
Ingersoll, B., & Hambrick, D. Z. (2011). The relationship between the broader autism phenotype, child severity, and stress and depression in parents of children with autism spectrum disorders. Research in Autism Spectrum Disorders, 5(1), 337–344. doi:10.1016/j.rasd.2010.04.017.
Kasari, C., & Sigman, M. (1997). Linking parental perceptions to interactions in young children with autism. Journal of Autism and Developmental Disorders, 27(1), 39–57. doi:10.1023/A:1025869105208.
Kayfitz, A. D., Gragg, M. N., & Orr, R. R. (2010). Positive experiences of mothers and fathers of children with autism. Journal of Applied Research in Intellectual Disabilities, 23(4), 337–343. doi:10.1111/j.1468-3148.2009.00539.x.
Koeske, G., & Koeske, R. (1990). The buffering effect of social support on parental stress. American Journal of Orthopsychiatry, 60(3), 440–451. doi:10.1037/h0079164.
Konstantareas, M. M., & Homatidis, S. (1989). Assessing child symptom severity and stress in parents of autistic children. Journal of Child Psychology and Psychiatry, 30(3), 459–470. doi:10.1111/j.1469-7610.1989.tb00259.x.
Konstantareas, M. M., Homatidis, S., & Plowright, C. M. (1992). Assessing resources and stress in parents of severely dysfunctional children through the Clarke modification of Holroyd’s Questionnaire on Resources and Stress. Journal of Autism and Developmental Disorders, 22(2), 217–234. doi:10.1007/BF01058152.
Lecavalier, L., Leone, S., & Wiltz, J. (2006). The impact of behaviour problems on caregiver stress in young people with autism spectrum disorders. Journal on Intellectual Disability Research, 50(3), 172–183. doi:10.1111/j.1365-2788.2005.00732.x.
MacDonald, E. E., & Hastings, R. P. (2010). Fathers of children with developmental disabilities. In M. E. Lamb (Ed.), The role of the father in child development (5th ed., pp. 486–516). New York: Wiley.
Marsiglio, W., Amato, P., Day, R. D., & Lamb, M. E. (2000). Scholarship on fatherhood in the 1990’s and beyond. Journal of Marriage and the Family, 62(4), 1170–1191. doi:10.1111/j.1741-3737.2000.01173.x.
Milgram, N. A., & Atzil, M. (1988). Parenting stress in raising autistic children. Journal of Autism and Developmental Disorders, 18(3), 415–424. doi:10.1007/BF02212196.
Mugno, D., Ruta, L., D’Arrigo, V. G., & Mazzone, L. (2007). Impairment of quality of life in parents of children and adolescents with pervasive developmental disorder. Health and Quality of Life Outcomes, 5, 22. doi:10.1186/1477-7525-5-22.
Olsson, M. B., & Hwang, C. P. (2001). Depression in mothers and fathers with intellectual disability. Journal of Intellectual Disability Research, 45(6), 535–543. doi:10.1046/j.1365-2788.2001.00372.x.
Osborne, L. A., McHugh, L., Saunders, J., & Reid, P. (2008). A possible contra-indication for early diagnosis of Autistic Spectrum Conditions: Impact on parenting stress. Research in Autism Spectrum Disorders, 2(4), 707–715. doi:10.1016/j.rasd.2008.02.005.
Peters-Scheffer, N., Didden, R., & Korzilius, H. (2012). Maternal stress predicted by characteristics of children with autism spectrum disorder and intellectual disability. Research in Autism Spectrum Disorders, 6(2), 696–706. doi:10.1016/j.rasd.2011.10.003.
Phetrasuwan, S., & Miles, M. S. (2009). Parenting stress in mothers of children with autism spectrum disorders. Journal for Specialists in Pediatric Nursing, 14(3), 157–169. doi:10.1111/j.1744-6155.2009.00188.x.
Pleck, J., & Masciadrelli, B. (2004). Paternal involvement in US residential fathers: Levels, sources, and consequences. In M. Lamb (Ed.), The role of the father in child development (4th ed., pp. 222–276). New York, NY: Wiley.
Rodrigue, J. R., Morgan, S. B., & Geffken, G. R. (1992). Psychosocial adaptation of fathers of children with autism, Down syndrome, and normal development. Journal of Autism and Developmental Disorders, 22(2), 249–263.
Sanders, J. L., & Morgan, S. B. (1997). Family stress and adjustment as perceived by parents of children with autism or Down syndrome: Implications for intervention. Child and Family Behavior Therapy, 19(4), 15–32. doi:10.1300/J019v19n04_02.
Schalock, R. L., Luckasson, R. A., Shogren, K. A., Borthwick-Duffy, S., Bradley, V., Buntix, W. H. E., et al. (2010). The renaming of mental retardation: Understanding the change to the term intellectual disability. Intellectual and Developmental Disabilities, 45(2), 116–124.
Schopler, E., Reichler, R. J., & Rochen Renner, B. (1988). The Childhood Autism Rating Scale (CARS). Los Angeles, CA: Western Psychological Services.
Shannon, J. D., Tamis-LeMonda, C. S., London, K., & Cabrera, N. (2002). Beyond rough and tumble: Low-income fathers’ interactions and children’s cognitive development at 24 months. Parenting: Science and Practice, 2(2), 77–104. doi:10.1207/S15327922PAR0202_01.
Sparrow, S. S., Cicchetti, D. V., & Balla, D. A. (2005). Vineland II: A revision of the Vineland Adaptive Behavior Scales: I. Survey/caregiver form. Circle Pines, MN: American Guidance Service.
Strauss, K., Vicari, S., Valeri, G., D’Elia, L., Arima, S., & Fava, L. (2012). Parent inclusion in early intensive behavioral intervention: The influence of parental stress, parent treatment fidelity and parent-mediated generalization of behavior targets on child outcomes. Research in Developmental Disabilities, 33(2), 688–703. doi:10.1016/j.ridd.2011.11.008.
Szatmari, P., Archer, L., Fisman, S., & Steiner, D. L. (1994). Parent and teacher agreement in the assessment of pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24(6), 703–717. doi:10.1007/BF02172281.
Tobing, L. E., & Glenwick, D. S. (2002). Relation of the Childhood Autism Rating Scale-Parent version to diagnosis, stress, and age. Research in Developmental Disabilities, 23(3), 211–223. doi:10.1016/S0891-4222(02)00099-9.
Tomanik, S., Harris, G. E., & Hawkins, J. (2004). The relationship between behaviours exhibited by children with autism and maternal stress. Journal of Intellectual and Developmental Disability, 29(1), 16–29. doi:10.1080/13668250410001662892.
Wechsler, D. (2002). Wechsler preschool and primary scale of intelligence (WPPSI III). San Antonio: Psychological Corp.
Williford, A. P., Calkins, S. D., & Keane, S. P. (2007). Predicting change in parenting stress across early childhood: Child and maternal factors. Journal of Abnormal Child Psychology, 35(2), 251–263. doi:10.1007/s10802-006-9082-3.
Wolf, L., Noh, S., Fisman, S., & Speechley, M. (1989). Brief report: Psychological effects of parenting stress on parents of autistic children. Journal of Autism and Developmental Disorders, 19(1), 157–166. doi:10.1007/BF02212727.
Acknowledgments
We would like to acknowledge the financial support that we received during this research project. This project is part of a larger research project, financed by the Montérégie Health Agency and the Quebec Ministry of Health and Social Services. We want to thank the Centre de réadaptation en déficience intellectuelle et en troubles envahissant du développement Montérégie-Est, Mme Sylvie Gladu, Johanne Gauthier, M. Gilles Lemaire, Mme Caroline Bouffard, Mme Annick LeBeau and Mme Johanne Messier and we extend our gratitude to the children, parents, educators and therapists who participated in this study. We also want to thank Mme Gisela Regli, Mme Kelly Kerr et Mme Catherine Mello for their work on traduction and revision of the article. With regard to competing interests, Amélie Terroux declare to be employees of the Centre de réadaptation déficience intellectuelle et en troubles envahissant du développement Montérégie-Est. Céline Mercier and Claudel Parent-Boursier were under contract for the same agency for the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rivard, M., Terroux, A., Parent-Boursier, C. et al. Determinants of Stress in Parents of Children with Autism Spectrum Disorders. J Autism Dev Disord 44, 1609–1620 (2014). https://doi.org/10.1007/s10803-013-2028-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-013-2028-z