
Abstract
Parenting a child with autism may differentially affect mothers and fathers. Existing studies of mother–father differences often ignore the interdependence of data within families. We investigated gender differences within-families using multilevel linear modeling. Mothers and fathers of children with autism (161 couples) reported on their own well-being, and their child’s functioning. Mothers reported higher levels of distress compared with fathers, and child behavior problems predicted psychological distress for both mothers and fathers. We found little evidence of child functioning variables affecting mothers and fathers differently. Gender differences in the impact of child autism on parents appear to be robust. More family systems research is required to fully understand these gender differences and the implications for family support.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Parenting a child with an Autism Spectrum Disorder (ASD) has been associated with a range of negative outcomes. Compared to parents of typically developing children, parents of children with an ASD report higher levels of psychological distress (Eisenhower et al. 2005; Schieve et al. 2007; Totsika et al. 2011a). Parents of children with an ASD also report poorer well-being compared to parents of children with Down syndrome (Dabrowska and Pisula 2010; Eisenhower et al. 2005; Griffith et al. 2010; Olsson and Hwang 2003), Fragile X syndrome (Abbeduto et al. 2004), cerebral palsy (Eisenhower et al. 2005), and intellectual disability (ID) alone (Blacher and McIntyre 2006; Totsika et al. 2011b).
Although the majority of research exploring parental adjustment in the field of ASD highlights negative outcomes, there is an emerging body of literature reporting on the positive aspects parents also experience (Bayat 2007; Griffith et al. 2010; Hastings and Taunt 2002). In fact, some researchers have shown no differences in positive perceptions between parents of children with ASD and other parents once key variables such as child behavior problems and family socioeconomic position have been controlled (Totsika et al. 2011a, b).
Family research in the field of ASD traditionally focused on maternal outcomes alone. However, there is a growing literature reporting on both maternal and paternal adjustment. Interest in the different impact on all family members stems from family systems theory (Seligman and Darling 1997). These theories emphasize the dynamic and interdependent nature of the family unit, with the experiences of one member potentially affecting the entire system. For example, a number of researchers have concluded that mothers of children with an ASD experience significantly greater levels of stress than fathers (Dabrowska and Pisula 2010; Herring et al. 2006; Moes et al. 1992; Tehee et al. 2009). Similarly, mothers have also reported higher levels of depression (Hastings et al. 2005; Olsson and Hwang 2001) and anxiety (Hastings 2003; Hastings and Brown 2002) compared to fathers. In the few studies that have compared mothers’ and fathers’ positive perceptions of raising a child with an ASD, mothers have reported more positivity (Hastings et al. 2005; Kayfitz et al. 2010).
Not only does reported well-being apparently differ between mothers and fathers of children with ASD, but researchers have also suggested that maternal and paternal well-being is affected by different variables. Severity of ASD symptoms and related behavior problems have been associated with maternal distress (Beck et al. 2004; Hastings and Johnson 2001; Tobing and Glenwick 2002; Phetrasuwan and Miles 2009), with fewer such associations apparent for fathers (Hastings 2003; Hastings et al. 2005). Similarly, Davis and Carter (2008) reported mothers’ well-being to be associated with their children’s self-regulatory skills, whilst fathers’ well-being was associated more strongly with their children’s externalizing behaviors.
Although a general pattern has emerged from existing research about parental differences in levels of reported well-being, such findings are not altogether consistent in that some studies find no mother-father differences (Davis and Carter 2008; Hastings 2003; Hastings et al. 2005; Rimmerman et al. 2003). There is also a further analytical dimension, which makes it difficult to clearly interpret many of the existing findings. The conventional way to analyze couple data in ASD family research has been to use the general linear model (GLM) framework (e.g., t test, analysis of variance and covariance, and regression analysis). These models (except for related samples t test) assume observations to be independent; an assumption clearly violated within families.
Multiple members within a family form a hierarchical system of individuals nested within a group. Individuals from the same family are likely to be more similar to each other than people from different families because of their shared environment (i.e., there is likely to be considerable dependence). Mother–father data can be correctly modeled as dependent with related samples t tests. However, a number of researchers attempting to identify correlates of paternal and maternal psychological well-being have treated mothers and fathers independently—with paternal and maternal well-being treated as separate outcomes in different regression models (e.g., Hastings and Brown 2002; Hastings et al. 2005; Davis and Carter 2008). When nested data structures are ignored, the estimates of standard errors of important parameters may be biased, thus leading to biased interpretation of the importance of various parameters in accounting for the outcome (Moerbeek et al. 2003). Multilevel linear models (MLM) are an extension of GLM, where the dependence of nested data is explicitly addressed.
Some research data focused on mothers and fathers of individuals with an ASD have been analyzed using MLM, primarily in the form of daily diary studies (repeated measures also equate nested data structures), investigating parents’ typical daily experiences and subsequent subjective well-being (Pottie et al. 2009; Pottie and Ingram 2008; Smith et al. 2010). For example, Pottie et al. (2009) examined contextual factors associated with daily mood in mothers and fathers of children with ASD over 12 weeks and found higher levels of child disruptive behaviors significantly predicted higher levels of daily negative mood/psychological distress, with mothers reporting higher levels of daily negative mood than fathers. Pottie and Ingram (2008) found that severity of ASD symptomatology was not predictive of daily positive or negative mood in mothers or fathers.
In the present study, our aim was to add to the limited literature exploring mother–father differences in ASD family research using MLM. Specifically, we were interested in two questions: (1) Do mothers and fathers report different levels of positive and negative psychological well-being? (2) Is maternal and paternal well-being differentially associated with child characteristics, such as child behavior problems, severity of autism symptoms and adaptive skills, after controlling for other important factors (e.g., family socioeconomic position)? Directional hypotheses were not proposed due to inconsistencies in findings from previous research and methodological limitations in previous research.
Methods
Participants
One hundred and sixty one mother–father couples participated in the research and were drawn from an ASD family study focused on sibling well-being (Petalas et al. 2012). The sample included one adoptive parent couple and one foster parent couple. The remaining couples were biological parents, except for nine couples that included a biological mother and stepfather. The average age of mothers was 41.59 years (SD = 6.59) and fathers 44.02 years (SD = 5.91). Eighty (50 %) fathers and 79 (49 %) mothers were educated to university degree level or higher, with 99 (62 %) mothers and 152 (94 %) fathers in employment at the time of the research. Modal household income in the current sample was £25,000–£35,000 per year (British pounds sterling; approximately $40,000–$55,000 US dollars).
Families’ socio-economic position (SEP) was summarized by categorizing families into one of four possible groups, depending on whether a parent was educated to university degree level (if so, scoring 1), whether at least one parent was currently employed (if so, scoring 1) and whether total annual household income was above the modal value for the sample of £35,000 (if so, scoring 1). Four families (3 %) comprised the lowest possible SEP group, scoring 0 (neither parent educated to university level, neither parent in employment, and annual income below £35,000). Forty nine families (31 %) comprised the second lowest group, scoring 1 point; 49 families (31 %) comprised the second highest group, scoring 2 points; and 57 families (35 %) comprised the highest possible group, scoring 3 points (at least one parent educated to university degree level or higher, at least one parent in employment, and total household income above £35,000).
The majority of participants (95 %) described themselves as being of White British ethnicity. One hundred and sixty couples were cohabiting, and the majority of families (59 %) had two children living in the family home. Ninety-nine (62 %) of the couples’ children had a diagnosis of autism, 61 (38 %) had a diagnosis of Asperger syndrome, and one child had a diagnosis of Pervasive Developmental Disorder–Not Otherwise Specified. One hundred and thirty (81 %) children were male and 31 (19 %) female. Children were on average 10.50 years of age (SD = 2.93), and had received their ASD diagnosis on average 3.81 years (SD = 2.70) previously.
Parental Well-Being Measures
The Hospital Anxiety and Depression Scale (HADS; Zigmond and Snaith 1983) was used to measure parents’ mental health. The HADS was constructed to allow a quick measure of depression and generalized anxiety in hospital settings, but has been widely used in outpatient and community research. It has been used successfully to measure anxiety and depression in parents of children with autism (Rydebrandt 1991; Hastings 2003). The HADS contains 14 items, with seven assessing depression and seven assessing anxiety. Respondents rate items such as “I feel tense or wound up” and “I feel as if I am slowed down” on a four point scale: most of the time, a lot of the time, from time to time, or not at all. Anxiety and depression subscale scores were used in the current study, with good internal consistency displayed for both mothers (Cronbach’s α anxiety: .85, depression: .83) and fathers (Crobach’s α anxiety: .85, depression: .83).
The Parent and Family Problems Subscale of The Questionnaire on Resources and Stress-Short Form (QRS-F; Friedrich et al. 1983) was used to measure general parenting stress associated with the child with ASD. This scale contains 20 items, but we removed five items relating to depression to avoid measurement overlap (Glidden and Floyd 1997). Respondents rate items, including “Our family agrees on important matters” and “There is a lot of anger and resentment in our family”, as either true or false. The QRS-F has previously been used in research with parents of children with autism, and good reliability was obtained (Honey et al. 2005). Internal consistency (Kuder–Richardson coefficient) in the current study was .88 for mothers and .87 for fathers.
The Positive Gain Scale (PGS; Pit-ten Cate 2003) was used to measure parental positive perceptions. The PGS is a 7-item tool, assessing positive experiences related to parenting a child. Parents’ perceived benefits of raising the child and gains made by the family are measured, with respondents choosing whether they strongly agree, agree, not sure, disagree or strongly disagree with statements. Sample items include: “Since having this child I feel I have grown as a person” and “Since having this child, my family has become more tolerant and accepting”. MacDonald, Hastings and Fitzsimons (2010) found good internal consistency (Cronbach’s α .80) for the PGS in a population of fathers of children with ID. The PGS total score was used in the current study (with lower scores indicating higher levels of positive gain). Internal consistency (Cronbach’s α) in the current study was .84 for fathers and .84 for mothers.
Child Measures
The Social Communication Questionnaire (SCQ; Rutter et al. 2003) was used to measure the extent of the child’s autism symptoms. The SCQ is an autism-screening instrument, completed by a carer, and based on international diagnostic criteria (DSM-IV: American Psychiatric Association 2000; ICD-10: World Health Organization 2008). The Current Form of the scale was used for the present research, assessing the child’s behavior and severity of autism symptoms over the preceding 3-month period. The SCQ consists of 40 items, and participants answer yes/no to statements such as: “Is she/he now able to talk using short phrases or sentences?” and “Does she/he play any pretend or make-believe games?” A cut-off score of 15 out of a possible 39 (Item 1 does not have a scoring value as it documents whether or not the child can speak and dictates which of the remaining items to answer) is recommended as an indicator of a possible ASD (Rutter et al. 2003). The mean score in the present study was 20.85 (SD = 7.17), with 133 children (81 %) scoring above the recommended cut-off. In the present study, primary caregivers completed the SCQ, and internal consistency (Kuder–Richardson coefficient) was .83.
The Vineland Adaptive Behavior Scales-2nd Edition (VABS II; Sparrow et al. 2005) was used to measure the level of the child’s adaptive functioning. The VABS II is administered as a semi-structured interview, and was conducted with the child’s primary caregiver over the telephone. The VABS II is composed of items arranged in developmental sequence that measure adaptive behaviors across four domains: socialization, communication, daily living skills, and motor skills (the motor skills domain is only administered to children below the age of 7). An overall adaptive behavior composite standardized score was used in the analyses.
The Strengths and Difficulties Questionnaire (SDQ; Goodman 1997) was used as a measure of children’s behavioral and emotional adjustment, completed by primary caregivers. The 25-item questionnaire measures 4 problem domains: emotional symptoms, conduct problems, hyperactivity, and peer problems; as well as prosocial behavior. Respondents rate statements about their child as not true, somewhat true, or certainly true, based on the child’s behavior over the past 6 months. Example items from each subscale include: “Often unhappy, down-hearted or tearful” (emotional symptoms); “Generally obedient, usually does what adults request” (conduct problems); “Restless, overactive, cannot stay still for long” (hyperactivity); “Rather solitary, tends to play alone” (peer problems); “Helpful if someone is hurt, upset or feeling ill” (prosocial behavior). The SDQ is a well-validated instrument proven to be effective in identifying clinically significant levels of behavioral disturbance in children (Goodman 1997). Good levels of reliability have also been maintained in research with children with autism (Iizuka et al. 2010). The sum of the four problem domains generates a “total difficulties” behavior problem score, which was used in the present study. Internal consistency (Cronbach’s α) obtained in the present study for this scale was .78.
Procedure
The Research Ethics and Governance Committees at Bangor University and The National Autistic Society (NAS) approved the broader family study protocol. The NAS, a UK charity for people with autism and their families, distributed information about the study and invitation letters to 1,000 families registered on their database. Three hundred and five families who met the inclusion criteria, of caring for a child aged 4–16 years who had a formal diagnosis of an ASD, returned the invitation letter, and were mailed consent forms and a questionnaire pack. Two hundred and fifteen families provided written informed consent and returned completed questionnaires. Parents who identified themselves as being the child’s primary carer were then contacted by telephone to complete the VABS II. The present research focused on 161 families where a mother and father both participated.
Data Analysis and Results
The data provided by mother–father dyads formed a two-level hierarchical (multilevel) data structure. Level 1 contains measures at the individual level, representing variation between individuals. Level 2 contains measures shared at the family level, representing variation between families. Level 1 variables in the present research included parent gender, parent age, and parent outcome measures (stress, depression, anxiety, and positive gain). Level 2 variables included family SEP, child age, length of time since receiving diagnosis, family size, child behavior problems (measured with the SDQ), adaptive behaviors (VABS), and severity of autism symptoms (measured with the SCQ).
The MLM framework does not require observations to be independent, models both fixed and random factors, and allows cross-level interactions. Fixed factors are variables where all possible values of interest are measured, and the average effect in the entire population is expressed by the regression coefficient. A factor is random if its units can be regarded as a random sample from a wider population. In the current study, the family unit was modeled as a random factor, with all other variables modeled as fixed. When a multilevel model contains any random effect, a covariance structure needs to be specified. The covariance structure establishes the form of the variance–covariance matrix, and is used to estimate model parameters. For all models in the present research, an unstructured matrix was chosen, which makes no assumptions about the magnitude of the correlation between any two pairs of data. The selection of an unstructured matrix over other alternatives was based on a lack of prior knowledge about the nature of the covariance matrix.
Predictor and control variables were centered around their mean, to add stability to the estimation process and to ease interpretation (Enders and Tofighi 2007). Mean centering does not change the parameters, but does aid the interpretation of the parameters by providing a meaningful value (i.e., the mean) as a reference point for assessing the magnitude of the parameters (Kraemer and Blasey 2004). Statistical analyses were conducted with PASW (SPSS) Statistics 18.0®. Four multilevel models were constructed, to examine each of the parental well-being measures.
First, intercept-only models with no exploratory variables were fitted (unconditional random effects model), to calculate the intraclass correlation (ICC). The ICC represents the within-family and between-family variance. The calculation of the ICC was used to examine whether within-family correlation was large enough to justify the use of MLM as an analysis approach. The unconditional random effects model for each of the four well-being measures suggested that a significant amount of outcome variance was present within-families (stress: 46 %, p < .001; depression: 72 %, p < .001; anxiety: 100 %, p < .001; positive gain: 75 %, p < .001), supporting the decision to model the data using MLM.
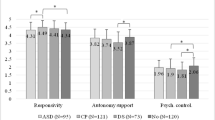
The next step in the analysis introduced parent gender as a fixed effect factor in each model, to address the first research question: whether mothers and fathers report different levels of positive and negative psychological affect. At this stage, gender accounted for 18.25 % (p < .001) of the variance in stress levels; 5.49 % (p = .002) of variance in depression levels; 11.40 % (p < .001) of variance in anxiety levels; and 6.43 % (p = .001) of variance in levels of positive gain. Gender was significantly associated with all outcome measures (father data coded 0, mother data coded 1), with mothers reporting higher levels of stress, anxiety, depression, and positive gain (lower positive gain scale scores represent greater levels of positivity). Table 1 presents mothers’ and fathers’ mean scores on well-being measures, along with the gender coefficients at this stage in the analyses (Table 1).
Subsequently, potentially significant confounding variables (age of carer, age of child, family size, time since receiving ASD diagnosis, and SEP scores) were entered into the models. Adopting a parsimonious approach for the identification of important confounders, only control variables significantly associated with the outcome were retained in the final models.
In the final step of the analyses, we entered child characteristics (autism symptom severity, behavior problems and adaptive functioning) in each model. Child predictor variables (severity of autism symptoms (SCQ total score), level of behavior problems (SDQ total difficulties score), and adaptive behaviors (VABS composite standard score), were all entered into the model to explore their main effects on parental well-being. In addition, interaction terms between each of these child variables and parental gender were included. These interaction terms were included to address our second research question: whether child characteristics are associated differently with maternal and paternal well-being.
The results of the final models for each outcome variable are summarized in Table 2. The final model for parental stress controlled for family SEP (level 2) and child age (level 2). In the final model, parent gender (level 1) and child age were significantly associated with parental stress, with parenting older children related to increased stress. SEP was no longer significantly associated with stress. As a main effect, the level of the child’s behavior problems (level 2) significantly predicted stress. However, no other child variable main effect and none of the interaction terms (parental gender * child characteristics) were significantly associated with parental stress. Therefore, the level of the child’s behavior problems increased parental stress overall, and there was a significant main effect for gender, but there was no differential relationship between child characteristics and stress depending on parent gender.
The final depression model controlled for family SEP (level 2). Gender (level 1) and SEP remained significant in the final model, with lower SEP related to higher levels of depression. As a main effect, the level of the child’s behavior problems (level 2) was the only variable significantly predictive of depression. Overall, the level of the child’s behavior problems was associated with increased parental depression. None of the interaction terms between parental gender and child characteristics were significant, again suggesting that there was no differential relationship between child characteristics and depression depending on parent gender.
The final anxiety model controlled for family SEP (level 2). Parents of lower SEP status reported greater levels of anxiety. As main effects, the level of the child’s behavior problems (level 2) and the level of the child’s adaptive functioning (level 2) were significantly predictive of parental anxiety. Interaction terms also demonstrated that the level of the child’s behavior problems and adaptive functioning were differentially associated with parental anxiety. Mothers’ anxiety was significantly more affected by high levels of the child behavior problems. Mothers’ anxiety was also more affected by the level of the child’ adaptive skills: as adaptive functioning increased, mothers became more anxious.
The final positive gain model controlled for carer age (level 1) and length of time since diagnosis (level 2). When these control variables were introduced, gender was no longer significantly associated with positive perceptions. Carer age remained significant, with younger parents reporting greater levels of positive gain. No child variables were significantly predictive of positive gain, and there was no differential relationship between child characteristics and positive gain depending on parent’s gender.
Discussion
Using an analysis method accounting for the inter-relatedness of data within families, we found that mothers of children with an ASD generally reported higher levels of psychological distress (stress, anxiety, and depression) and higher levels of positive gain compared to fathers. These parent gender differences in stress, depression and anxiety remained statistically significant even after controlling for demographic characteristics and child characteristics. Parental differences for positive gain were less robust and were no longer found once background variables were controlled. We found little evidence of a different pattern of predictors for paternal and maternal well-being, although child behavior problems and adaptive behaviors were more strongly associated with maternal than paternal anxiety. However, these effects were two from a possible 12 interaction effects that could have demonstrated differential impact for mothers and fathers.
In common with previous research (Lecavalier et al. 2006; Osborne and Reed 2009), we found children’s behavior problems emerged as a predictor of parental psychological distress (stress, depression, and anxiety). In contrast, the severity of the child’s autism symptoms and their adaptive skills were not found to be statistically significant predictors of parental well-being (with the exception of adaptive skills predicting parental anxiety). Furthermore, positive gain was not associated with any child characteristics, supporting previous findings that parental positivity may be relatively unaffected by increased behavior problems/symptomatology and reduced adaptive skills (Hastings and Taunt 2002).
Mothers are typically more involved in the care of their children (e.g., Konstantareas and Homatidis 1992), and therefore have greater potential to be affected by their child’s behavior. In the present sample, 156 (97 %) families identified the mother as being the child’s primary caregiver, although we included no measure of parenting responsibilities. A qualitative study by Gray (2003) investigating gender differences when parenting a child with ASD found that mothers’ careers were restricted and often sacrificed to care for the child, and that mothers took on a “disproportionately burdensome role of caring for a disabled child and coping with the problems that the situation produced” (Gray 2003, p. 641). Mothers also often resented the inequality in sacrifice and consequent disproportionate domestic responsibilities. Differing parental responsibilities may well be a salient contributor towards parental well-being, and future research is needed to explore the impact of distribution of responsibilities and sacrifices in explaining parental differences in well-being.
That parental (in particular, maternal) anxiety increased as children’s adaptive functioning improved may appear unexpected. Recent findings from other cultures also suggest higher levels of anxiety in mothers of children with high functioning autism/Asperger syndrome compared to mothers of children with more severe autism (Mori et al. 2009). Higher functioning children are likely to lead more independent lives, which could lead to increased parental anxiety as to their children’s day-to-day safety. Such an association might also be related to increased levels of anxiety in children with high functioning autism (Lecavalier 2006; Sukhodolsky et al. 2008) that could in turn be related to increased anxiety in other family members. Such a pattern of intra-familial psychological distress may be accounted for by Family Systems theory (Seligman and Darling 1997), or by shared genetic effects. In relation to potential family genetic effects, anxiety levels in biological mothers of children with autism have been reported to be higher compared to mothers of other children (Bailey et al. 1998; Micali et al. 2004).
Although paternal and maternal well-being differ significantly, the results suggest these differences are due to factors other than those measured in the current study (child behavior problems, severity of autism symptoms, level of adaptive functioning). In terms of variables explored in previous autism family research, candidate factors include coping strategies and social support (Dabrowska and Pisula 2010; Dunn et al. 2001; Lustig 2002). For example, women have been found to engage in more emotion-focused coping than men (Dabrowska and Pisula 2010), which could be contributing towards mothers’ elevated distress profiles. In future research, a broader range of child, parent, and family variables should be explored so that the root of gender differences in parental distress in families of children with ASD can be elucidated.
It is also important to note that women regularly report increased depression and anxiety compared to men in the general adult population (Bekker and van Mens-Verhulst 2007; Kuehner 2003; McLean and Anderson 2009; Van de Velde et al. 2010). Future research is needed to establish whether the same variables mediate the impact of potential stressors on the well-being of women both generally, and when parenting children with ASD.
The current study had a large sample of 161 mother-father couples, and the nested structure of the data was specifically modeled. Despite these methodological strengths, there are a number of limitations that need to be considered when interpreting the results. It is questionable whether the sample is representative of families of children with an ASD living in the UK. Participants were recruited through a charitable organization’s database, and may represent families who were actively involved/interested in the services the charity had to offer. A further limitation is that primary caregivers (typically mothers) alone completed measures of the child’s autism symptoms and level of adaptive functioning. Therefore, maternal ratings may not accurately represent fathers’ experiences of their child’s behaviors. The current findings need replicating to add to their validity, and also longitudinal designs are needed to explore causal links.
Mothers are clearly at greater risk of experiencing reduced well-being compared to fathers when parenting children with ASDs. Although further research is needed to explain why these gender differences are evident, services need to be aware of potential elevated distress profiles in mothers, and clinical interventions should target improving maternal well-being and reducing their psychological distress.
References
Abbeduto, L., Seltzer, M. M., Shattuck, P., Krauss, M. W., Orsmond, G., & Murphy, M. M. (2004). Psychological well-being and coping in mothers of youths with autism, down syndrome, or fragile X syndrome. American Journal on Mental Retardation, 109(3), 237–254. doi:10.1352/0895-8017(2004)109<237:PWACIM>2.0.CO;2.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.
Bailey, A., Palferman, S., Heavey, L., & Le Couter, A. (1998). Autism: The phenotype in relatives. Journal of Autism and Developmental Disorders, 28(5), 369–392.
Bayat, M. (2007). Evidence of resilience in families of children with autism. Journal of Intellectual Disability Research, 51, 702–714. doi:10.1111/j.1365-2788.2007.00960.x.
Beck, A., Daley, D., Hastings, R. P., & Stevenson, J. (2004). Mothers’ expressed emotion towards children with and without intellectual disabilities. Journal of Intellectual Disability Research, 48, 628–638. doi:10.1111/j.1365-2788.2003.00564.x.
Bekker, M. H. J., & van Mens-Verhulst, J. (2007). Anxiety disorders: Sex differences in prevalence, degree, and background, but gender-neutral treatment. Gender Medicine, 4(B), 178–193.
Blacher, J., & McIntyre, L. L. (2006). Syndrome specificity and behavioural disorders in young adults with intellectual disability: Cultural differences in family impact. Journal of Intellectual Disability Research, 50(3), 184–198. doi:10.1111/j.1365-2788.2005.00768.x.
Dabrowska, A., & Pisula, E. (2010). Parenting stress and coping styles in mothers and fathers of pre-school children with autism and down syndrome. Journal of Intellectual Disability Research, 54(3), 266–280. doi:10.1111/j.1365-2788.2010.01258.x.
Davis, N. O., & Carter, A. S. (2008). Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: Associations with child characteristics. Journal of Autism and Developmental Disorders, 38(7), 1278–1291. doi:10.1007/s10803-007-0512-z.
Dunn, M. E., Burbine, T., Bowers, C. A., & Tantleff-Dunn, S. (2001). Moderators of stress in parents of children with autism. Community Mental Health Journal, 37(1), 39–52. doi:10.1023/A:1026592305436.
Eisenhower, A. S., Baker, B. L., & Blacher, J. (2005). Preschool children with intellectual disability: Syndrome specificity, behaviour problems, and maternal well-being. Journal of Intellectual Disability Research, 49(9), 657–671. doi:10.1111/j.1365-2788.2005.00699.x.
Enders, C. K., & Tofighi, D. (2007). Centering predictor variables in cross- sectional multilevel models: A new look at an old issue. Psychological Methods, 12(2), 121–138. doi:10.1037/1082-989X.12.2.121.
Friedrich, W. N., Greenberg, M. T., & Crnic, K. (1983). A short-form of the questionnaire on resources and stress. American Journal of Mental Deficiency, 88(1), 41–48.
Glidden, L. M., & Floyd, F. J. (1997). Disaggregating parental depression and family stress in assessing families of children with developmental disabilities: A multisample analysis. American Journal on Mental Retardation, 102(3), 250–266. doi:10.1352/0895-8017(1997)102<0250:DPDAFS>2.0.CO;2.
Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Journal of Child Psychology and Psychiatry and Allied Disciplines, 38(5), 581–586. doi:10.1111/j.1469-7610.1997.tb01545.x.
Gray, D. E. (2003). Gender and coping: The parents of children with high functioning autism. Social Science and Medicine, 56(3), 631–642. doi:10.1016/S0277-9536(02)00059-X.
Griffith, G. M., Hastings, R. P., Nash, S., & Hill, C. (2010). Using matched groups to explore child behavior problems and maternal well-being in children with Down syndrome and autism. Journal of Autism and Developmental Disorders, 40, 610–619.
Hastings, R. P. (2003). Child behaviour problems and partner mental health as correlates of stress in mothers and fathers of children with autism. Journal of Intellectual Disability Research, 47, 231–237. doi:10.1046/j.1365-2788.2003.00485.x.
Hastings, R. P., & Brown, T. (2002). Behavior problems of children with autism, parental self-efficacy, and mental health. American Journal on Mental Retardation, 107(3), 222–232. doi:10.1352/0895-8017(2002)107<0222:BPOCWA>2.0.CO;2.
Hastings, R. P., & Johnson, E. (2001). Stress in UK families conducting intensive home-based behavioral intervention for their young child with autism. Journal of Autism and Developmental Disorders, 31(3), 327–336. doi:10.1023/A:1010799320795.
Hastings, R. P., Kovshoff, H., Ward, N. J., Espinosa, F. D., Brown, T., & Remington, B. (2005). Systems analysis of stress and positive perceptions in mothers and fathers of pre-school children with autism. Journal of Autism and Developmental Disorders, 35(5), 635–644. doi:10.1007/s10803-005-0007-8.
Hastings, R. P., & Taunt, H. M. (2002). Positive perceptions in families of children with developmental disabilities. American Journal on Mental Retardation, 107(2), 116–127. doi:10.1352/0895-8017(2002)107<0116:PPIFOC>2.0.CO;2.
Herring, S., Gray, K., Taffe, J., Tonge, B., Sweeney, D., & Einfeld, S. (2006). Behaviour and emotional problems in toddlers with pervasive developmental disorders and developmental delay: Associations with parental mental health and family functioning. Journal of Intellectual Disability Research, 50, 874–882. doi:10.1111/j.1365-2788.2006.00904.x.
Honey, E., Hastings, R. P., & McConachie, H. (2005). Use of the questionnaire on resources and stress (QRS-F) with parents of young children with autism. Autism, 9(3), 246–255. doi:10.1177/1362361305053256.
Iizuka, C., Yamashita, Y., Nagamitsu, S., Yamashita, T., Araki, Y., Ohya, T., et al. (2010). Comparison of the strengths and difficulties questionnaire (SDQ) scores between children with high-functioning autism spectrum disorder (HFASD) and attention-deficit/hyperactivity disorder (AD/HD). Brain & Development, 32(8), 609–612. doi:10.1016/j.braindev.2009.09.009.
Kayfitz, A. D., Gragg, M. N., & Orr, R. R. (2010). Positive experiences of mothers and fathers of children with autism. Journal of Applied Research in Intellectual Disabilities, 23(4), 337–343. doi:10.1111/j.1468-3148.2009.00539.x.
Konstantareas, M. M., & Homatidis, S. (1992). Mothers and fathers self-report of involvement with autistic, mentally delayed, and normal-children. Journal of Marriage and the Family, 54(1), 153–164. doi:10.2307/353283.
Kraemer, H. C., & Blasey, C. M. (2004). Centring in regression analyses: A strategy to prevent errors in statistical inference. International Journal of Methods in Psychiatric Research, 13(3), 141–151. doi:10.1002/mpr.170.
Kuehner, C. (2003). Gender differences in unipolar depression: An update of epidemiological findings and possible explanations. Acta Psychiatra Scandinavia, 108(3), 163–174. doi:10.1034/j.1600-0447.2003.00204.x.
Lecavalier, L. (2006). Behavioral and emotional problems in young people with pervasive developmental disorders: Relative prevalence, effects of subject characteristics, and empirical classification. Journal of Autism and Developmental Disorders, 36(8), 1101–1114. doi:10.1007/s10803-006-0147-5.
Lecavalier, L., Leone, S., & Wiltz, J. (2006). The impact of behaviour problems on caregiver stress in young people with autism spectrum disorders. Journal of Intellectual Disability Research, 50, 172–183. doi:10.1111/j.1365-2788.2005.00732.x.
Lustig, D. C. (2002). Family coping in families with a child with a disability. Education and Training in Mental Retardation and Developmental Disabilities, 37(1), 14–22.
MacDonald, E. E., Hastings, R. P., & Fitzsimons, E. (2010). Psychological acceptance mediates the impact of the behaviour problems of children with intellectual disability on fathers’ psychological adjustment. Journal of Applied Research in Intellectual Disabilities, 23(1), 27–37. doi:10.1111/j.1468-3148.2009.00546.x.
McLean, C. P., & Anderson, E. R. (2009). Brave men and timid women? A review of the gender differences in fear and anxiety. Clinical Psychology Review, 29(6), 496–505.
Micali, N., Chakrabarti, S., & Fombonne, E. (2004). The broad autism phenotype. Autism, 8(1), 21–37.
Moerbeek, M., van Breukelen, G. J. P., & Berger, M. P. (2003). A comparison between traditional methods and multilevel regression for the analysis of multicenter intervention studies. Journal of Clinical Epidemiology, 56(4), 341–350. doi:10.1016/S0895-4356(03)00007-6.
Moes, D., Koegel, R. L., Schreibman, L., & Loos, L. M. (1992). Stress profiles for mothers and fathers of children with autism. Psychological Reports, 71(3), 1272–1274. doi:10.2466/PR0.71.8.1272-1274.
Mori, K., Ujiie, T., Smith, A., & Howlin, P. (2009). Parental stress associated with caring for children with Asperger’s syndrome or autism. Pediatrics International, 51, 364–370. doi:10.1111/j.1442-200X.2008.02728.x.
Olsson, M. B., & Hwang, C. P. (2001). Depression in mothers and fathers of children with intellectual disability. Journal of Intellectual Disability Research, 45(6), 535–543. doi:10.1046/j.1365-2788.2001.00372.x.
Olsson, M. B., & Hwang, P. C. (2003). Influence of macrostructure of society on the life situation of families with a child with intellectual disability: Sweden as an example. Journal of Intellectual Disability Research, 47(4–5), 328–341. doi:10.1046/j.1365-2788.2003.00494.x.
Osborne, L. A., & Reed, P. (2009). The relationship between parenting stress and behavior problems of children with autistic spectrum disorders. Exceptional Children, 76(1), 54–73.
Petalas, M. A., Hastings, R. P., Nash, S., Hall, L. M., Joannidi, H., & Dowey, A. (2012). Psychological adjustment and sibling relationships in siblings of children with autism spectrum disorders: Environmental stressors and the broad autism phenotype. Research in Autism Spectrum Disorders, 6, 546–555.
Phetrasuwan, S., & Miles, M. S. (2009). Parenting stress in mothers of children with autism spectrum disorders. Journal for Specialists in Pediatric Nursing, 14(3), 157–165.
Pit-ten Cate, I. M. (2003 unpublished). Family adjustment to disability and chronic illness in children. Unpublished Doctoral Thesis, University of Southhampton.
Pottie, C. G., Cohen, J., & Ingram, K. M. (2009). Parenting a child with autism: Contextual factors associated with enhanced daily parental mood. Journal of Pediatric Psychology, 34(4), 419–429. doi:10.1093/jpepsy/jsn094.
Pottie, C. G., & Ingram, K. M. (2008). Daily stress, coping, and well-being in parents of children with autism: A multilevel modeling approach. Journal of Family Psychology, 22(6), 855–864. doi:10.1037/a0013604.
Rimmerman, A., Turkel, L., & Crossman, R. (2003). Perception of child development, child-related stress and dyadic adjustment: Pair analysis of married couples of young children with developmental disabilities. Journal of Intellectual & Developmental Disability, 28(2), 188–195. doi:10.1080/1366825031000147111.
Rutter, M., Bailey, A., Lord, C., & Berument, S. K. (2003). Social communication questionnaire. Los Angeles, CA: Western Psychological Services.
Rydebrandt, B. (1991). Defense strategies and anxiety in mothers of disabled-children. European Journal of Personality, 5(5), 367–377. doi:10.1002/per.2410050504.
Schieve, L. A., Blumberg, S. J., Rice, C., Visser, S. N., & Boyle, C. (2007). The relationship between autism and parenting stress. Pediatrics, 119, S114–S121. doi:10.1542/peds.2006-2089Q.
Seligman, M., & Darling, R. B. (1997). Ordinary families: Special children. New York, NY: Guilford Press.
Smith, L. E., Hong, J., Seltzer, M. M., Greenberg, J. S., Almeida, D. M., & Bishop, S. L. (2010). Daily experiences among mothers of adolescents and adults with autism spectrum disorder. Journal of Autism and Developmental Disorders, 40(2), 167–178. doi:10.1007/s10803-009-0844-y.
Sparrow, S. S., Cicchetti, D. V., & Balla, D. A. (2005). Vineland II adaptive behaviour scales. A revision of the Vineland social maturity scale by Edgar A. Doll. Survey interview form. Circle Pines, MN: AGS Publishing.
Sukhodolsky, D. G., Scahill, L., Gadow, K. D., Arnold, L. E., Aman, M. G., McDougle, C. J., et al. (2008). Parent-rated anxiety symptoms in children with pervasive developmental disorders: Frequency and association with core autism symptoms and cognitive functioning. Journal of Abnormal Child Psychology, 36(1), 117–128. doi:10.1007/s10802-007-9165-9.
Tehee, E., Honan, R., & Hevey, D. (2009). Factors contributing to stress in parents of individuals with autistic spectrum disorders. Journal of Applied Research in Intellectual Disabilities, 22(1), 34–42. doi:10.1111/j.1468-3148.2008.00437.x.
Tobing, L. E., & Glenwick, D. S. (2002). Relation of the childhood autism rating scale-parent version to diagnosis, stress, and age. Research in Developmental Disabilities, 23(3), 211–223. doi:10.1016/S0891-4222(02)00099-9.
Totsika, V., Hastings, R. P., Emerson, E., Berridge, D. M., & Lancaster, G. A. (2011a). Behavior problems at 5 years of age and maternal mental health in autism and intellectual disability. Journal of Abnormal Child Psychology, 39(8), 1137–1147. doi:10.1007/s10802-011-9534-2.
Totsika, V., Hastings, R. P., Emerson, E., Lancaster, G. A., & Berridge, D. M. (2011b). A population-based investigation of behavioural and emotional problems and maternal mental health: Associations with autism spectrum disorder and intellectual disability. Journal of Child Psychology and Psychiatry, 52(1), 91–99. doi:10.1111/j.1469-7610.2010.02295.x.
Van de Velde, S., Bracke, P., & Levecque, K. (2010). Gender differences in depression in 23 European countries. Cross-national variation in the gender gap in depression. Social Science and Medicine, 71(2), 305–313.
World Health Organization. (2008). ICD-10: International statistical classification of diseases and related health problems (10th Rev. ed.). New York, NY: Author.
Zigmond, A. S., & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67(6), 361–370. doi:10.1111/j.1600-0447.1983.tb09716.x.
Acknowledgments
The preparation of this manuscript was supported by grant SCS/09/11 from the National Institute for Social Care and Health Research (Wales) to Bangor University. The original research was supported by funding from the European Social Fund, the National Autistic Society, and Bangor University.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jones, L., Totsika, V., Hastings, R.P. et al. Gender Differences When Parenting Children with Autism Spectrum Disorders: A Multilevel Modeling Approach. J Autism Dev Disord 43, 2090–2098 (2013). https://doi.org/10.1007/s10803-012-1756-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-012-1756-9