
Abstract
We examined motor and tactile-perceptual skills in individuals with high-functioning autism (IHFA) and matched typically developing individuals (TDI) ages 5–21 years. Grip strength, motor speed and coordination were impaired in IHFA compared to matched TDI, and the differences between groups varied with age. Although tactile-perceptual skills of IHFA were impaired compared to TDI on several measures, impairments were significant only for stereognosis. Motor and tactile-perceptual skills should be assessed in children with IHFA and intervention should begin early because these skills are essential to school performance. Impairments in coordination and stereognosis suggest a broad though selective under-development of the circuitry for higher order abilities regardless of domain that is important in the search for the underlying disturbances in neurological development.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Impairments in motor and tactile-perceptual skills are not diagnostic criteria for autism, but they do manifest as delays, deficits and sensitivities in individuals with autism (American Psychiatric Association [APA] 2000 p. 72; Baranek et al. 2005, 2007; Cesaroni and Garber 1991; Grandin 2006; Hochhauser and Engel-Yeger 2010; Jeste 2011; Kanner 1943; Rogers 2009). The same is true for individuals with high-functioning autism (IHFA; Ghaziuddin et al. 1994; Jansiewicz et al. 2006; Mandelbaum et al. 2006; Manjiviona and Prior 1995; Minshew et al. 1995; Noterdaeme et al. 2010; Smith and Bryson 1998; Rumsey and Hamburger 1988; Williams et al. 2006).
Compared to typically developing individuals (TDI), children and adolescents with HFA have greater incoordination (David et al. 2009), reduced grip strength (Hardan et al. 2003; Williams et al. 2006) and mixed results for motor speed, with some studies reporting impaired motor speed in IHFA (Takarae et al. 2004) and some reporting no significant differences (Hardan et al. 2003; Minshew and Goldstein 1998; Williams et al. 2006). Furthermore, many studies have reported incoordination in IHFA compared to TDI across age groups (Dowell et al. 2009; Dziuk et al. 2007; Hardan et al. 2003; Mari et al. 2003; Minshew et al. 1997, Rumsey and Hamburger 1990; Takarae et al. 2004). Despite one study that failed to detect differences between TDI and IHFA (Williams et al. 2006), several studies concluded that movement disturbances or incoordination may be core features of autism spectrum disorder and surrogate indicators of underlying neurological abnormalities.
Tactile-perceptual impairments and other sensory sensitivities in individuals with autism have been documented since the disorder was first described (Kanner 1943). IHFA have reported hypersensitivities to sound and touch (Grandin 2006; Hochhauser and Engel-Yeger 2010) and being overwhelmed and confused when touched by people (Cesaroni and Garber 1991). Minshew et al. (1997) and Williams et al. (2006) examined tactile-perceptual impairments in IHFA. While all measures of tactile-perceptual skills in the Minshew et al. (1997) study failed to discriminate between IHFA and TDI, four of the six measures used by Williams et al. (2006) discriminated between children with high-functioning autism and typically developing children revealing tactile-perceptual impairments in children with high-functioning autism. In another study by Rumsey and Hamburger (1990), men with high-functioning autism made significantly more errors on the fingertip number writing test compared to typically developing men.
What remains unclear from the aforementioned studies, for both motor and tactile-perceptual skills, are the changes that may occur on these skills across different developmental periods. In addition, the characterization and understanding of motor and tactile-perceptual impairments in this population remains limited in part due to variability in study design. For example, none of the reviewed studies examined motor integrities and impairments in children with a mean age less than 10 years, or included samples across a wide range of ages. Some of these studies were not rigorous in identifying IHFA, nor did they control for differences in IQ between IHFA and TDI.
The present study examined motor and tactile-perceptual integrities and impairments in rigorously diagnosed IHFA samples and gender, IQ, socio-economic status, and age-matched TDI samples between 5 and 21 years, the age range typically served by related personnel in public school special education programs. Based on the literature, we hypothesized that IHFA would demonstrate significantly reduced grip strength, motor speed, coordination and tactile-perceptual skills compared to matched TDI, and that these significant differences would exist across different ages.
Methods
We conducted a cross-sectional study using data collected as part of neuropsychological assessment batteries in prior NIH autism research grants (MH40858, NS33355, and U19HD35469). This enabled us to study a broad age range of IHFA and TDI.
Participants
All participants and/or their guardians completed University of Pittsburgh informed consent procedures and documents prior to participation. IHFA met criteria for Autistic Disorder on the Autism Diagnostic Interview- Revised (ADI-R), the Autism Diagnostic Observation Schedule (ADOS), and expert clinical opinion. In addition, all IHFA were required to have a Full-Scale IQ (FS-IQ) and Verbal IQ (V-IQ) of 80 or higher. Exclusion criteria for IHFA were the presence of an identifiable genetic, metabolic, or infectious cause for their autism. IHFA were excluded if there was a history of current seizures, head trauma, or birth injury. Among 230 of initial IHFA in the databases 73 met study criteria.
TDI were healthy volunteers who were recruited through advertisements in neighborhoods with socioeconomic status resembling those of the IHFA families of origin. TDI were excluded if they had a history of learning disability, a neuropsychiatric disorder, any psychological disorder, and if they had a family history of autism or heritable neuropsychiatric disorder with implications for the participant, which was assessed utilizing a screening questionnaire addressing disorders, including autism, in first and second degree relatives. Next we derived a sample of TDI participants who matched the IHFA sample on group characteristics of age, education, and SES (measured with the Hollingshead Index; Hollingshead 1975). Among 224 of initial TDI in the databases 75 met study criteria and comprised the group-matched sample.
Procedures
We utilized data collected for IHFA and TDI with an age range of 5–21 years old for motor (Grip Strength, Finger Tapping Test, and Grooved Pegboard) and tactile-perceptual (Luria-Nebraska tests of Simple Touch, Sharp-Dull Discrimination, Position Sense, and Stereognosis, and Reitan-Kolve tests of Finger Agnosia and Fingertip Number Writing) measures. We included all subjects tested within this age range who completed the motor and tactile- perceptual tests.
Hand dominance for IHFA and TDI was determined with the Lateral Dominance Examination from the Halstead–Reitan Neuropsychological Test Battery (Reitan and Wolfson 1985). All tests were administered by research technicians trained to criterion on the administration and scoring procedures, supervised by a licensed psychologist with provisions for ongoing monitoring of reliability.
Motor Skill Measures
We measured grip strength, motor speed and praxis of the dominant hand. Grip strength was measured with a hand dynamometer using a standardized protocol. Motor speed was measured with the Finger Tapping Test, which requires the tapping of a key that records the number of taps made over five 10 s trials. Coordination was measured with the Grooved Pegboard, which consists of 25 small keyholes, angled in various directions, and requires the insertion and rotation of pegs into the keyholes as quickly as possible.
Tactile-Perceptual Skill Measures
Luria-Nebraska tests of Simple Touch, Sharp-Dull Discrimination, Position Sense, and Stereognosis, and Reitan-Kolve tests of Finger Agnosia and Fingertip Number Writing were used to measure tactile-perceptual skills. For the Reitan-Klove tests, participants identify which of their fingers have been touched, and what number has been written on their fingertip with an empty ballpoint pen with vision occluded. We dichotomized tactile-perceptual scores into “intact—no errors” or “impaired—errors” due to skewed distributions.
Data Analysis
For motor measures, we conducted three analyses of covariance (ANCOVA). The independent variable, group, included two levels: TDI and IHFA. The dependent variables were each of the motor measures (Grip Strength, Motor Speed, and Coordination). The covariate in each analysis was the continuous variable age. Whenever the assumptions of ANOVA were violated, transformation of data was conducted to better fit ANOVA assumptions. We conducted partial eta squared (η 2p ) calculations to assess objectively the magnitude of the observed difference. Effect sizes greater than .04 were considered “practically significant” (Ferguson 2009).
For tactile-perceptual measures we conducted logistic regression analyses, examining associations between group membership (TDI, IHFA) and tactile-perceptual skills controlling for the categorical variable age and the interaction of group by age. To aid interpretation of interaction effects in analyses with a binomial dependent variable, we categorized age into 3 groups based on published developmental milestones in tactile-perception skills (Young = 5–7.99, Middle = 8–11.99, and Older = 12–21). Young and Middle groups were split based on based on previous findings that suggested that age 8 is a critical time point for sensory-motor development in school age children (Ayres 2005). Middle and Older groups were split based on educational level, assuming that primary education concluded at around at age 12, and may represent a critical time point for sensory-motor development (Ayres 2007). We examined odds ratios (OR) to assess the magnitude of effect of significant terms. Odds ratios greater than 1 were considered clinically meaningful.
Results
One hundred forty-eight (n = 148) participants met the inclusion and exclusion criteria, 73 in the IHFA group and 75 in the TDI group. There were no significant differences between IHFA and TDI subject characteristics (Table 1).
Motor Skills
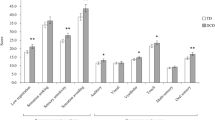
Compared to TDI, IHFA were significantly impaired on all motor measures, grip strength F(1, 145) = 53.93, p < .001, η 2p = 0.27, motor speed F(1, 138) = 6.78, p = .01, η 2p = 0.05, and coordination F(1, 145) = 24.17, p < .001, η 2p = 0.14, after controlling for the continuous variable of age. For measures of grip strength and motor speed, the differences between TDI and IHFA increased with age, while the opposite was observed with coordination (Fig. 1).

Differences between individuals with high-functioning autism (IHFA) and typically-developing individuals (TDI) on grip strength (a), Finger Tapping Test (b), and Grooved Pegboard Test (c)
Tactile-Perceptual Skills
When examining the association between group (TDI, IHFA) and tactile-perceptual skills, IHFA were not anymore likely than TDI to be impaired for Simple Touch (R 2 = 0.09, χ 2(5) = 6.48, p = .26), Sharp/Dull Discrimination (R 2 = 0.10, χ 2(5) = 9.22, p = .10), or Fingertip Number Writing (R 2 = 0.12, χ 2(5) = 10.07, p = .07) after controlling for age category. IHFA were more likely than TDI to be impaired for Stereognosis (R 2 = 0.19, χ 2(5) = 14.35, p = .01), and Finger Recognition (R 2 = 0.25, χ 2(5) = 26.41, p < .001). For stereognosis differences between IHFA and TDI varied across age categories. IHFA in the Older age category were 2.1 times more likely than TDI to demonstrate errors in stereognosis (Fig. 2a). As for Finger Recognition, TDI and IHFA were similar across age categories with the greatest difference in the Middle age group. (Fig. 2b). However, the odds ratios for finger recognition were not clinically meaningful (OR < 1). For Position Sense, due to lack of variability, no further analyses could be run.

Frequencies of No Errors/Errors among the three categories of age for individuals with high-functioning autism (IHFA) and typically-developing individuals (TDI) for stereognosis (a) and finger recognition (b)
Discussion
This study compared the motor and tactile-perceptual skills of IHFA and TDI between 5 and 21 years of age. Several studies have assessed these skills with different age groups, however, to our knowledge, no study has examined motor and tactile-perceptual skills in children, adolescents, and young adults rigorously diagnosed with HFA and an age-matched TDI. Our hypothesis that IHFA would demonstrate lower levels of motor skills than TDI age peers was supported. Our hypothesis that the IHFA group would have lower levels of tactile-perceptual skills compared to TDI age peers was only supported for stereognosis and finger recognition skills.
Our findings regarding grip strength are consistent with previous literature, in part because the studies by Hardan et al. (2003) and Williams et al. (2006) are based on subsets of our data. However, the current study expands our understanding of motor skills in IHFA to a younger age. Weakness in grip strength seems to be apparent from a young age for children with HFA and persists through adolescence and early adulthood. Although considered a simple motor skill, the importance of adequate grip strength cannot be overlooked. In general, grip strength is considered an objective measure of upper extremity functional integrity (Balogun et al. 1991). Fair grip strength is essential for independence in early childhood functional tasks (Amundson 1995; Hager-Ross and Rosblad 2002) as well as in community dwelling older adults (Hyatt et al. 1990). Weaknesses in grip strength in IHFA might be explained by the presence of hypotonia that is evident in some children with autism (Jong et al. 2011; Ming et al. 2007).
Our findings regarding speed and coordination are consistent with previous research, and add to the body of knowledge. Previous research found no significant differences between children with HFA and TD children on simple motor skills (as measured by FTT; Williams et al. 2006), while another study found adults with HFA and TD adults to be significantly different on the same skill (Takarae et al. 2004). Our findings indicated that IHFA performed significantly worse than TDI on motor speed and that the difference increased with age. Likewise, our finding that incoordination in IHFA, as measured by the Grooved Pegboard, is consistent with previous research. For example, a recent study by Jong et al. (2011) found children with autism spectrum disorder demonstrated incoordination when compared to typically developing children. Our results, combined with those of Jong et al. (2011) indicate that motor impairments are evident in both homogeneous and heterogeneous samples, suggesting that motor impairments are an integral aspect of autism spectrum disorders. One of the interesting findings of this study was the pattern of impairments in motor skills, with impairments in grip strength and motor speed increasing with age, compared to TDI, and incoordination decreasing with age. For grip strength and motor speed this is a call for attending to these skills when assessing and intervening with IHFA even at an older age and to acknowledge that the developmental trajectory for IHFA may be different than the trajectory for TDI at different developmental milestones. As for coordination, it could be that developmentally IHFA learn to perform more coordinated movements with age, especially with structured experiences such as the ones provided in school settings, thus the impairments tend to decrease with age, however, not to the point of equivalence with TDI skill level.
The results of the tactile-perceptual measures were conflicting, and yielded rather unexpected results. No group differences between IHFA and TDI were found for simple touch, sharp/dull discrimination, or fingertip number writing, and this finding is inconsistent with previous research (Minshew et al. 1997; Rumsey and Hamburger 1988; Williams et al. 2006). Only finger recognition showed a significant age effect for both IHFA and TDI. Stereognosis skills also showed a surprising pattern with increasing impairments evident in the Middle and Older groups. Stereognosis is considered one of the higher order tactile-perceptual skills, as it relies on higher cognitive functions in addition to intact tactile sensation. Stereognosis, along with other tactile-perceptual skills, discriminated between children with HFA and TD children (κ = 0.44; Williams et al. 2006), however, stereognosis testing does not pass the tolerance test for discriminant analysis for adults with HFA. Our findings are in contrast to these, suggesting that some element of stereognosis impairment may also be evident for older IHFA.
Our findings were in part consistent with the complex information processing disorder model (Minshew and Goldstein 1998). Simple tactile-perceptual skills (such as simple touch, sharp/dull discrimination) were not found to be impaired in IHFA while stereognosis, a complex tactile-perceptual skill, was found to be impaired in our IHFA sample. However, for motor skills, our findings were more extensive that those proposed in this model, because the adolescents/young adults demonstrated impairment on the simple and complex motor skills.
Our examination of the motor system was limited to three parameters—grip strength, motor speed, and coordination. These parameters report on nonspecific elementary motor skills and skilled motor movements relevant to handwriting and other manipulations central to school function. Basal gangliar involvement in the pathophysiology of autism, which is controversial (Enticott et al. 2009; Hardan et al. 2003), may be supported by our findings of reduced coordination. In addition, incoordination, as well as reduced grip strength and motor speed may represent impairments in the integrity of cerebral (Just et al. 2006; Minshew and Williams 2007) and cerebellar (Mostofsky et al. 2009) connections. The tactile-perceptual skills that required the greatest higher cortical circuitry integration were impaired as compared to those based on subcortical elementary tactile abilities. In IHFA, one of the main concerns is the altered development and maturation of cortical systems and particularly the development of connectivity with frontal cortex. The lack of developmental progress in IHFA is mirrored by the lack of maturation in cortical connectivity and in functions dependent on cortical connectivity and maturation (Courchesne and Pierce 2005; Just et al. 2006; Schipul et al. 2011). In conclusion, based on our study and previous research, impairments in motor skills is apparent in IHFA across childhood, and persists through adolescence, and early adulthood and should be of concern to clinical professionals working with this population. Although tactile-perceptual impairments were not as evident in our sample, our findings suggest these skills may be consistent between IHFA and age-matched peers, except for stereognosis.
Clinical Implications
One of the key findings of this study was confirmation of the presence of motor impairments in very young IHFA. This finding has an important implication for practitioners working with IHFA in that assessment and remediation of such skills should begin as early as these impairments can be detected. Grip strength, in specific, holds great promise for change in young children with HFA, because an improvement of grip strength may lead to greater independence in functional activities involving self-care, school tasks, and play. Occupational therapists are trained to address impairments in fine-motor functioning and the factors underlying these impairments. For example, in school settings, occupational therapy provides children exhibiting poor grip strength with an array of preparatory activities that aim to enhance muscle strength and ultimately enable functional tasks in the classroom such as handwriting and use of scissors.
Findings of tactile-perceptual skill impairments also indicate the importance of the assessment of such skills, especially for the higher and more complex tactile processing skills. When complex tactile discrimination is deficient, this reduces the integration of tactile input into the system, thus reducing the capacity for adaptation. The integration of inappropriate and distorted tactile-perceptual skills has been correlated with behavioral rigidities in individuals with autism (Baranek et al. 2005). Occupational therapists can assess a wide array of tactile-perceptual distortions (e.g., body image, letter reversals, spatial relationships for arithmetic) as well as provide interventions to remediate such impairments. Interventions for tactile-perceptual skills include a wide range of sensory training and manipulation games and exercises emphasizing speed, accuracy and total efficiency that are related to and emphasized in school settings. It is important that early detection and continuous reassessment of such skills occur throughout elementary and middle schools years, since our findings indicated that some of these skills may persist through early adulthood.
Limitations, Strengths and Recommendations
As with any study, this study had limitations. One limitation of this study is its cross-sectional design which restricts its generalizability, because the trajectory and exposure to interventions are unknown. A cross-sectional design takes advantage of the capacity to collect data on a large number of subjects in a finite period of time, rather than waiting long periods to collect longitudinal data. The disadvantage is that these are two entirely different groups of subjects. The individuals in the older age group recruited during this time did not have the opportunity for the early interventions that the children recruited during this time frame frequently received. It may also be that the children diagnosed in today’s times had less severe symptoms than the older age group who were diagnosed nearly two decades previously when more severe symptoms were required to attain an autism diagnosis. Ideally, longitudinal studies offer the best methodology to study developmental trajectories as they control for individual variation with different age groups. As with any secondary analysis, we were limited by the variables in the original datasets. This study also had strengths, including a well-defined sample of individuals with high-functioning autism, and a matched sample of typically developing individuals. In addition, we had a wide range of school aged children, and lowered the age range down to children 5 years of age. We recommend the completion of longitudinal studies, especially those focusing on younger children, to ascertain if maturation, interventions, or individual differences yield different outcomes for fine motor skills and tactile-perceptual skills. Additional sensory measures and gross motor measures should also be considered in future studies.
References
American Psychiatric Association [APA]. (2000). Diagnostic and statistical manual of mental disorders, text revision (DSM-IV-TR) (4th ed.). Washington, DC: Author.
Amundson, S. J. (1995). Evaluation tool of children’s handwriting. Homer, Alaska: O.T. Kids.
Ayres, J. (2005). Sensory integration and the child (25th ed.). Los Angeles, CA: Western Psychological Services.
Ayres, J. (2007). Sensory integration and praxis test manual (9th ed.). Los Angeles, CA: Western Psychological Services.
Balogun, J. A., Akomolafe, C. T., & Amusa, L. O. (1991). Grip strength: Effects of testing posture and elbow position. Archives of Physical Medicine and Rehabilitation, 71, 280–283.
Baranek, G. T., Parham, D., & Bodfish, J. W. (2005). Sensory and motor features in autism: Assessment and intervention. In F. R. Volkmar, R. Paul, A. Klin, & D. Cohen (Eds.), Handbook of autism and pervasive developmental disorders (Vol. 2, pp. 831–857). Hoboken, New Jersey: Wiley.
Baranek, G. T., Boyd, B. A., Poe, M. D., David, F. J., & Watson, L. R. (2007). Hyperresponsive sensory patterns in young children with autism, developmental delay, and typical development. American Journal of Mental Retardation, 112, 233–245.
Cesaroni, L., & Garber, M. (1991). Exploring the experience of autism through firsthand accounts. Journal of Autism and Developmental Disorders, 21, 303–313.
Courchesne, E., & Pierce, K. (2005). Why the frontal cortex in autism might be talking only to itself: Local over-connectivity but long-distance disconnection. Current Opinion in Neurobiology, 15, 225–230.
David, F. J., Baranek, G. T., Giuliani, C. A., Mercer, V. S., Poe, M. D., & Thorpe, D. E. (2009). A pilot study: Coordination of precision grip in children and adolescents with high functioning autism. Pediatric Physical Therapy, 21, 205–211.
Dowell, L. R., Mahone, E. M., & Mostofsky, S. H. (2009). Association of postural knowledge and basic motor skill with dyspraxia in autism: Implication for abnormalities in distributed connectivity and motor learning. Neuropsychology, 23, 563–570.
Dziuk, M. A., Larson, J. C. G., Apostu, A., Mahone, E. M., Denckla, M. B., & Mostofsky, S. H. (2007). Dyspraxia in autism: Association with motor, social, and communicative deficits. Developmental Medicine and Child Neurology, 49, 734–739.
Enticott, P. G., Bradshaw, J. L., Iansek, R., Tonge, B. J., & Rinehart, N. J. (2009). Electrophysiological signs of supplementary-motor-area deficits in high-functioning autism but not Asperger syndrome: An examination of internally cued movement-related potentials. Developmental Medicine and Child Neurology, 51, 787–791.
Ferguson, C. J. (2009). An effect size primer: A guide for clinicians and researchers. Professional Psychology: Research and Practice, 40, 532–538.
Ghaziuddin, M., Butler, E., Tsai, L., & Ghaziuddin, N. (1994). Is clumsiness a marker for Asperger syndrome? Journal of Intellectual Disability Research, 38, 519–527.
Grandin, T. (2006). Thinking in pictures: My life with autism. New York, NY: Vintage.
Hager-Ross, C., & Rosblad, B. (2002). Norms for grip strength in children ages 4–16 years. Acta Paediatrica, 91, 617–625.
Hardan, A. Y., Kilpatrick, M., Keshhavan, M. S., & Minshew, N. J. (2003). Motor performance and anatomic magnetic resonance imaging (MRI) of the basal ganglia in autism. Journal of Child Neurology, 18, 317–324.
Hochhauser, M., & Engel-Yeger, B. (2010). Sensory processing abilities and their relation to participation in leisure activities among children with high-functioning autism spectrum disorder. Research in Autism Spectrum Disorders, 4, 746–754.
Hollingshead, A. B. (1975). Four factor index of social issues. New Haven, CT: Yale University Press.
Hyatt, R. H., Whitelaw, M. N., Bhat, A., Scott, S., & Maxwell, J. D. (1990). Association of muscle strength with functional status of elderly people. Age and Ageing, 19, 330–336.
Jansiewicz, E. M., Goldberg, M. C., Newschaffer, C. J., Denckla, M. B., Landa, R., & Mostofsky, S. H. (2006). Motor signs distinguish children with high functioning autism and Asperger’s syndrome from controls. Journal of Autism and Developmental Disorders, 36, 613–621.
Jeste, S. S. (2011). The neurology of autism spectrum disorders. Current Opinion in Neurology, 24, 132–139.
Jong, M. D., Punt, M., Groot, E. D., Minderaa, R. B., & Hadders-Algra, M. (2011). Minor neurological dysfunction in children with autism spectrum disorder. Developmental Medicine and Child Neurology, 53, 641–646.
Just, M. A., Cherkassky, V. L., Keller, T. A., Kana, R. K., & Minshew, N. J. (2006). Functional and anatomical cortical underconnectivity in autism: Evidence from an fMRI study of an executive function task and corpus callosum morphometry. Cerebral Cortex, 17, 951–961.
Kanner, L. (1943). Autistic disturbances of affective contact. Nervous Child, 2, 217–250.
Mandelbaum, D. E., Stevens, M., Rosenberg, E., Wiznitzer, M., Steinschneider, M., Filipek, P., et al. (2006). Sensorimotor performance in school-age children with autism, developmental language disorder, and low IQ. Developmental Medicine and Child Neurology, 48, 33–39.
Manjiviona, J., & Prior, M. (1995). Comparison of Asperger syndrome and high-functioning autistic children on a test of motor impairment. Journal of Autism and Developmental Disorders, 25, 23–39.
Mari, M., Castiello, U., Marks, D., Marraffa, C., & Prior, M. (2003). The reach-to-grasp movement in children with autism spectrum disorder. Philosophical Transactions of the Royal Society of London: Biological Sciences, 358, 393–403.
Ming, X., Brimacombe, M., & Wagner, G. C. (2007). Prevalence of motor impairment in autism spectrum disorders. Brain and Development, 29, 565–570.
Minshew, N. J., & Goldstein, G. (1998). Autism as a disorder of complex information processing. Mental Retardation and Developmental Disabilities, 4, 129–136.
Minshew, N. J., & Williams, D. L. (2007). The new neurobiology of autism: Cortex, connectivity, and neuronal organization. Archives of Neurology, 64, 945–950.
Minshew, N. J., Goldstein, G., & Siegel, D. (1995). Speech and language in high-functioning autistic individuals. Neuropsychology, 9, 255–261.
Minshew, N. J., Goldstein, G., & Siegel, D. J. (1997). Neuropsychological functioning in autism: Profile of complex information processing disorder. Journal of the International Neuropsychological Society, 3, 303–316.
Mostofsky, S. H., Powell, S. K., Simmonds, D. J., Goldberg, M. C., Caffo, B., & Pekar, J. J. (2009). Decreased connectivity and cerebellar activity in autism during motor task performance. Brain, 132, 2413–2425.
Noterdaeme, M., Wriendt, E., & Hohne, C. (2010). Asperger’s syndrome and high-functioning autism: Language, motor and cognitive profiles. European Child and Adolescent Psychiatry, 19, 475–481.
Reitan, R. M., & Wolfson, D. (1985). The Halsted-Reitan neuropsychological test battery. Tuscon, Arizona: Neuropsychology Press.
Rogers, S. J. (2009). What are infant siblings teaching us about autism in infancy? Autism Research, 2, 125–137.
Rumsey, J. M., & Hamburger, S. D. (1988). Neuropsychological findings in high-functioning men with infantile autism, residual state. Journal of Clinical and Experimental Neuropsychology, 10, 201–221.
Rumsey, J. M., & Hamburger, S. D. (1990). Neuropsychological divergence of high-level autism and severe dyslexia. Journal of Autism and Developmental Disorders, 20, 155–168.
Schipul, S. E., Keller, T. A., & Just, M. A. (2011). Inter-regional brain communication and its disturbance in autism. Frontiers in systems neuroscience, 5, 1–11.
Smith, I. M., & Bryson, S. E. (1998). Gesture imitation in autism I: Nonsymbolic postures and sequences. Cognitive Neuropsychology, 15, 747–770.
Takarae, Y., Mishew, N. J., Luna, B., Krisky, C. M., & Sweeney, J. A. (2004). Pursuit eye movement deficits in autism. Brain, 127, 2584–2594.
Williams, D. L., Goldstein, G., & Minshew, N. J. (2006). Neuropsychological functioning in children with autism: Further evidence for disordered complex information-processing. Child Neuropsychology, 12, 279–298.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Abu-Dahab, S.M.N., Skidmore, E.R., Holm, M.B. et al. Motor and Tactile-Perceptual Skill Differences Between Individuals with High-Functioning Autism and Typically Developing Individuals Ages 5–21. J Autism Dev Disord 43, 2241–2248 (2013). https://doi.org/10.1007/s10803-011-1439-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-011-1439-y