
Abstract
This study compares severity of specific depression symptoms in boys with autism spectrum disorder (ASD), attention-deficit hyperactivity disorder (ADHD), or chronic multiple tic disorder (CMTD) and typically developing boys (Controls). Children were evaluated with parent and teacher versions of the Child Symptom Inventory-4 (CSI-4) and a demographic questionnaire. Mothers’ and teachers’ ratings generally indicated the most severe symptoms in boys with ASD ± ADHD. Associations of depression with ASD severity and IQ varied considerably for specific symptoms of depression, ASD functional domain, and informant. Findings provide additional support for the differential influence of neurobehavioral syndromes on co-occurring symptom severity and illustrate how more fine-grained analyses of clinical phenotypes may contribute to a better understanding of etiology and current nosology.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Several decades of research have clearly shown co-morbidity (or co-occurring symptomatology) is a pervasive characteristic of psychiatric syndromes, and more recently investigators have begun to explore its implications for nosology. As we have commented elsewhere (e.g., Guttmann-Steinmetz et al. 2009), one central question is whether co-morbidity alters clinical presentation and management in such a way as to warrant consideration in the classification of mental illnesses. An intuitive reaction is that co-morbidity will generally lead to more severe impairments as a result of the cumulative effects of having more than one disorder. Alternatively, the pathogenic processes that result in co-morbidity may be overlapping but nevertheless unique. In other words, certain combinations of disorders may be qualitatively different from a simple combination of their mono-morbid constituents, both etiologically and clinically. For a variety of reasons, this is often difficult to demonstrate, but one possible strategy is to determine if the pattern of associated co-occurring psychiatric symptoms differs in mono- versus co-morbid conditions both within and between neurobehavioral syndromes. In the case of autism spectrum disorder (ASD) research has been hindered to some extent by nosological preconceptions about co-occurring symptomatology, many of which remain largely unresolved (Gadow et al. 2004a; Sverd 2003).
Perhaps one of the better documented and seemingly more prevalent co-occurring conditions (symptoms) in children with ASD is attention-deficit/hyperactivity disorder (ADHD; reviewed by Rommelse et al. 2010), a disorder that is often associated with chronic multiple tic disorder (CMTD) in both non-ASD (e.g., Comings et al. 1996) and ASD (Gadow et al. 2009) samples. Anxiety has also received much empirical and clinical attention in children with ASD (reviewed by White and Roberson-Nay 2009), but depression, which is also associated with ADHD (reviewed by Daviss 2008) and CMTD (reviewed by Robertson 2006), has not. Although it is clear some children and adolescents with ASD exhibit the behaviors of, or meet diagnostic criteria for, conventional conceptualizations of depression (Gadow et al. 2005; Ghaziuddin et al. 2002; Kim et al. 2000; Lopata et al. 2010; Mandell et al. 2008; Stewart et al. 2006; Sverd 2003; Vickerstaff et al. 2007), little is known about similarities and differences in the clinical presentation of depression in ASD compared with other neurobehavioral syndromes.
Research with non-ASD samples indicates a clear association between global ratings of ASD and depression symptom severity. For example, studies of children referred for outpatient psychiatric evaluation found moderate to high correlations for mothers’ (r = 0.47) and teachers’ (r = 0.59) ratings (Gadow et al. 2004b; Sprafkin et al. 2002a). Comparable results were obtained for mothers’ (r = 0.53) and teachers’ (r = 0.45) ratings of a large, community-based sample (Gadow and Sprafkin 2002). There is also evidence indicating undergraduates with more versus less severe ASD traits have more and less severe depressive features, respectively (Kanne et al. 2009), and youth with diagnosed mood disorder have more severe ASD scores than typically developing peers or patients with diagnosed anxiety disorder (Pine et al. 2008). These studies suggest at least some symptoms of depression and ASD may share common pathogenic processes, which is consistent with findings for monozygotic and dizygotic twins pointing to a modest genetic overlap of combined anxiety and depression symptoms with ASD traits (Hallett et al. 2009). However, investigations of children and adolescents with ASD have found substantially lower correlations between ASD and depression scores. Kim et al. (2000), for example, reported a correlation of r = 0.17 between ASD repetitive behaviors and global depression scores, and Lopata et al. (2010) found a modest association (r = −0.27) between global ASD and depression scores.
To the best of our knowledge, no published studies have examined the differential severity of specific depression symptoms in children with ASD compared with youth who have other types of neurobehavioral syndromes. Moreover, little is known about the relation of specific depression symptoms with core ASD domains (language and social deficits, perseverative behaviors). Such information has potential implications for etiology, nosology, and possibly intervention. To this end, we compared ratings of depression symptoms in (a) three groups of clinic-referred boys with ADHD (ASD + ADHD, CMTD + ADHD, ADHD Only), (b) boys with ASD with and without co-occurring ADHD, and (c) all clinic-referred groups with community controls. We also examined the relation of ASD and IQ with depression symptomatology. Based on prior work (Guttmann-Steinmetz et al. 2010), we expected a greater number of more severe symptoms in clinic-referred boys versus Controls and in co-morbid versus mono-morbid groups, and differences among groups to vary across individual symptoms of depression. Lastly, as research has repeatedly found important discrepancies in mothers’ versus teachers’ ratings of psychiatric symptoms (e.g., Drabick et al. 2007, 2008; Gadow et al. 2006; Guttmann-Steinmetz et al. 2009), we predicted this would also be the case in the present study.
Method
Participants
Clinic Samples
Four groups of clinically referred boys participated in this study (Table 1), all of whom lived in the same geographic area and were evaluated at the same university hospital using identical measures: ASD + ADHD (n = 74), ASD/-ADHD (n = 107), CMTD + ADHD (n = 47), and ADHD Only (n = 59). The two non-ASD samples were recruited for participation in a long-term follow-up study, which included a short-term drug trial for the CMTD + ADHD group (Gadow et al. 2007; Pierre et al. 1999). Participants were recruited from a variety of sources including a child psychiatry outpatient service, community clinics, schools, media advertisements, and parent-support groups. The ASD sample was comprised of consecutive referrals selected from a retrospective chart review (Gadow et al. 2009; Guttmann-Steinmetz et al. 2009, 2010). The research protocol for each study sample was approved by a university Institutional Review Board and appropriate measures were taken to protect patient (and rater) confidentiality. Procedures for recruiting, evaluating, diagnosing, and assessing each group are described in detail in the aforementioned publications.
Children in the two non-ASD samples were excluded from consideration for the study if they were dangerous to self or others, psychotic or had a seizure disorder, or had a major organic brain dysfunction, major medical illness, or ASD. Children were also excluded from the CMTD + ADHD group if their tics were so severe at intake that either the parent or child requested immediate intervention for tics. In all three samples, children were excluded if they were intellectually impaired (IQ < 70) based on full-scale IQ scores (Wechsler or Stanford-Binet).
Control Samples
There were two community-based comparison groups, one each for teacher- and mother-completed ratings, all of whom were evaluated as part of the normative data study for the Child Symptom Inventory-4 (CSI-4; Gadow and Sprafkin 2002) and were living in the same communities as the clinic-referred samples. In the current study we used only teacher ratings of boys who did not receive special education services, and whose teachers’ ratings of ADHD symptoms did not meet criteria for ADHD (based on their CSI-4 Screening cutoff scores described below; n = 173). As was the case for teachers’ ratings, only mothers’ ratings of boys who were not receiving special education services and whose ratings did not meet criteria for ADHD were included in the present study (n = 169).
Measures
Psychiatric Symptoms
The CSI-4 has both parent and teacher versions (Gadow and Sprafkin 1986, 2002). The items bear one-to-one correspondence with DSM-IV symptoms (i.e., high content validity). To determine symptom severity, items are scored (never = 0, sometimes = 1, often = 2, and very often = 3) and summed separately for each subscale (disorder). Subscales used in this study were ADHD, major depressive episode, dysthymia, and ASD. Excluded from the depression symptom matrix was irritability, which is reported elsewhere as it overlaps with generalized anxiety disorder (see Guttmann-Steinmetz et al. 2010) and oppositional defiant disorder (see Guttmann-Steinmetz et al. 2009). The ASD scale generates three subscale scores: Communication Deficits, Social Deficits, and Perseverative Behaviors. Numerous studies indicate the CSI-4 demonstrates satisfactory psychometric properties in community-based normative, clinic-referred non-ASD, and ASD samples (reviewed by Gadow and Sprafkin 2010). Specifically, individual symptom categories evidence satisfactory internal consistency (Cronbach’s alpha), test–retest reliability, and convergent and divergent validity with corresponding scales of other measures. Confirmatory factor analysis supports the internal validity of the DSM-IV model of behavioral syndromes in a large sample (N = 730) of children with diagnosed ASD (Lecavalier et al. 2009). The findings of numerous studies show that CSI-4 scores are minimally correlated with age, gender, IQ, and SES. As with almost all behavior rating scales, mother and teacher ratings evidence modest convergence.
Procedure
Clinic Samples
Procedures for recruiting, evaluating, diagnosing, and assessing each group are described in detail in prior publications (Gadow et al. 2006, 2007; Pierre et al. 1999). Briefly, prior to scheduling the clinic evaluation, mothers of potential patients were mailed a packet of materials including standardized behavior rating scales to be completed by parent and teacher, a background information questionnaire, and a permission for the release of school records. In almost all cases (>90%), parent ratings were completed by the child’s mother.
Clinic evaluations included interviews with the boys and their caregivers, informal observation of parent–child interaction, and review of the aforementioned materials. In addition, the mothers of the boys in the two non-ASD samples were interviewed by trained evaluators using the parent version of the Diagnostic Interview for Children and Adolescents (DICA-P; Reich 2000). The two non-ASD samples were also videotaped for 15 min while completing work assignments in a simulated classroom to assess both ADHD and tics. To be considered ADHD, boys in all three samples had to meet DSM-IIIR (American Psychiatric Association 1987) or DSM-IV (American Psychiatric Association 1994) criteria for ADHD and be above cutoff on at least one mother- and at least one teacher-completed ADHD behavior rating scale. Each child met ADHD symptom criteria in school and home (the “and rule”). The diagnosis of CMTD was based on an extensive battery of tic measures (see Gadow et al. 2007). Almost all (94%) boys met research diagnostic criteria for Tourette syndrome, definite or by history. At least two reliable examiners in different settings witnessed multiple, different motor tics in all patients. For both ADHD samples (±CMTD) evaluations were completed for behavior off medication.
Using DSM-IV criteria, all ASD diagnoses were made by expert clinicians, whose diagnoses were determined to be valid in a related study (Sprafkin et al. 2002b). In all cases, ASD diagnoses were based on (a) comprehensive developmental history of language and social development and inflexible or repetitive behaviors, (b) review of the parent- and teacher-completed CSI-4, which includes a validated ASD subscale (see Measures), and (c) prior evaluations by educators and clinicians. The Autism Diagnostic Observation Schedule (ADOS; Lord et al. 2000), administered by certified reliable examiners, was added to the assessment battery during the course of the study, and this information was used by the clinician to make the diagnosis in approximately 45% of the ASD cases. ADOS- and expert-diagnosed groups did not differ in IQ, demographic characteristics, or severity of any of the 12 DSM-IV ASD symptoms. The distribution of ASD diagnoses by subtype was as follows: autistic disorder (17%), Asperger’s disorder (38%), and PDD-NOS (45%).
Boys in the ASD sample were considered as ASD Only or as ASD + ADHD based on their CSI-4 Screening Cutoff scores. Boys who met criteria for any ADHD symptom category (ADHD:I, ADHD:HI, or ADHD:C) were placed in the ASD + ADHD group. A comparable percentage of boys in each group were receiving psychotropic medication when the rating scales were completed: ASD Only (n = 52; 40%), ASD + ADHD (n = 34; 46%). Mothers’ ratings indicated that both groups evidenced comparable severity for each of the three ASD domains as assessed with the CSI-4. Teachers’ ratings, however, indicated the ASD + ADHD had more severe social deficits (p < 0.001) and perseverative behaviors (p < 0.02).
Control Samples
Teacher CSI-4 ratings were obtained for regular education classes in four public schools. Parent ratings were obtained from three elementary schools and seven pediatric practices. Mothers completed the Checklist for 90% of the boys. Details of the sampling procedure for parent ratings appear elsewhere (Gadow and Sprafkin 2002). Few boys were currently receiving psychotropic medication: parent sample (n = 3), teacher sample (n = 1).
Statistical Analyses
The primary goal of the study was to compare individual symptoms of depression across five different groups of boys: ASD with and without ADHD, CMTD with ADHD, ADHD Only, and Controls. The first step in data analysis was to conduct Chi-square tests and ANOVAs to examine group differences in demographic characteristics. Next, Kruskal–Wallis tests were performed to compare groups for differences in severity ratings of individual CSI-4 items for mothers’ and teachers’ responses separately. Analyses were conducted comparing the three ADHD groups (ADHD only, ASD + ADHD, and CMTD + ADHD) and Controls, followed by a comparison of ASD boys with and without ADHD and Controls. Owing to the exploratory nature of these analyses, we did not employ strategies to control for the number of tests with the exception of a within-measure Bonferroni correction. This procedure is highly conservative for correlated variables (e.g., the symptoms of a specific disease or syndrome) and not well suited for exploratory analyses (see Cohen 1988; Feise 2002; Perneger 1998; Rothman 1990; Zhang et al. 1997). When the Kruskal–Wallis test was significant, follow-up Mann–Whitney U-tests were performed to evaluate pairwise differences among groups, controlling for Type 1 error by using the Bonferroni correction. Only statistically significant results are noted. Lastly, we conducted Spearman rank correlations to examine the association among specific symptoms of depression with IQ and the three core domains of ASD (communication and social deficits, and perseverative behaviors) as assessed with the CSI-4 in the ASD sample. As a rule of thumb for determining the magnitude of correlations, Cohen (1988) suggests the following: r > 0.50 = large, 0.50–0.30 = moderate, and 0.30–0.10 = small.
Results
Background Characteristics
The mean age of the five groups of boys ranged from 8.6 to 9.0 years (Table 1). Groups did not differ in Full-Scale IQ (all group means were within the average intellectual range) or households with a single and/or biological parent, and most were of self-described, European geographic ancestry. There was some variation is SES, and as expected, special education services.
Group Differences Between ADHD Groups and Controls
The two co-morbid groups (ASD + ADHD, CMTD + ADHD) obtained more severe depression symptom ratings than Controls for all symptoms, according to both mothers and teachers (Table 2). However, the ADHD Only group was rated as more severe than Controls for only two mother-rated symptoms (depressed, feels worthless), but most teacher-rated symptoms (ADHD Only > Controls).
Group Comparisons of Boys with ADHD
The largest number of ADHD group differences was between the ASD + ADHD and ADHD Only boys. The ASD + ADHD group was rated more severely for two mother-rated (depressed, little confidence) and two teacher-rated (shows little interest, low energy) symptoms. There were only two instances where the ASD + ADHD and CMTD + ADHD groups differed (teachers’ ratings of shows little interest and low energy). The CMTD + ADHD group had more severe symptoms (shows little interest, things never work out) than the ADHD Only group according to their mothers’ ratings.
Boys with ASD ± ADHD and Controls
The ASD Only group obtained more severe ratings for all depression symptoms from both mothers and teachers than Controls (Table 3) supporting the notion that boys with ASD are at a differentially higher risk for developing depressive symptoms regardless of co-occurring ADHD. Somewhat unexpectedly, the two ASD groups did not differ for any mother-rated symptom, but group differences were significant for two teacher-rated symptoms (shows little interest, low energy), which in both cases were more severe in the ASD + ADHD group.
Association of Depression with ASD and IQ
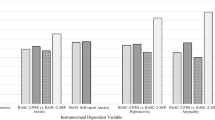
The pattern of Spearman rank correlations (controlling for IQ) between ratings of depression and the three core ASD domains (social and communication deficits, and perseverative behaviors) as assessed with the CSI-4 was mixed and varied as a function of informant, co-morbidity with ADHD, and ASD core domain (Table 4). There were few significant correlations between mother-rated depression and ASD symptoms, and only one symptom was moderately correlated (r = 0.33) with ASD severity (depressed), and this was in the ASD Only group. Conversely, relations were generally stronger for teachers’ ratings. Several symptoms of depression were moderately (r > 0.30) correlated with social deficits and perseverative behaviors in the ASD Only group, whereas most symptoms of depression were moderately correlated with at least one ASD domain score in the ASD + ADHD group.
Severity of depression symptoms was not associated with intellectual ability in boys with ASD + ADHD (Table 5). The magnitude of significant relations was also small for the ASD Only group, but mothers’ ratings of “depressed most of the day” was moderately (r = 0.31) associated with IQ.
Discussion
Findings from a growing number of studies indicate various combinations of disorders are often associated with different or more severe clinical features than either of their mono-morbid constituents separately or combined. Moreover, they are challenging traditional concepts of co-morbidity, nosology, clinical phenotypes, and models of pathogenesis. The present research emanated from a series of prior studies that examined global ratings of co-occurring depression symptoms in various groups of children with neurobehavioral syndromes (e.g., Gadow et al. 2002, 2005, 2009). Compared with typically-developing children, youngsters with ADHD, CMTD, and ASD were found to be at a greater risk for depression symptoms, with the most severe symptoms in children with co-morbid disorder (e.g., CMTD + ADHD, ASD + ADHD). The present study sought to determine if there was an even greater heterogeneity in group differences at the individual symptom level.
All groups of clinically-referred boys evidenced more severe symptoms of depression than Controls, but this was less evident in the ADHD Only group (Table 2). Boys with ASD + ADHD were rated as having more severe depression symptoms than the CMTD + ADHD group, and the two co-morbid ADHD groups had more symptoms than the ADHD Only group, but findings varied as a function of informant and type of depression symptom. It is possible that unique pathogenic processes associated with ASD, ADHD, and CMTD may explain the differential severity of specific symptoms of depression among these groups of boys. Alternatively, differences in relative severity may not translate into qualitative differences in clinical presentation or etiology. For example, it is commonly assumed differences in illness severity simply indicate a more powerful “dose” of the same (or greater number of) pathogenic mechanisms. In the absence of consensus criteria for defining diagnostic constructs whose etiology is not well established, it is difficult to even address this topic. However, two-hit genetic models for various diseases can be interpreted as supporting the notion that differential severity may actually indicate different pathogenic processes (Girirajan et al. 2010). Here, two versus one disease-inducing mutation is associated with a more severe and more complex symptomatology.
Because we previously found that ASD + ADHD was associated with more severe global ratings of depression in children (16% girls) than ASD Only (Gadow et al. 2006), in the current study the ASD sample was subdivided into those with and without co-occurring ADHD symptoms. The two groups of boys were generally similar in the severity of specific depression symptoms based on their mothers’ ratings (Table 3). Teachers, however, rated the co-morbid group as being less interested in pleasurable activities and having less energy than the ASD Only group. The significance of these informant discrepancies should not be underestimated. Approximately 80% of the boys with ASD were receiving special education services, and it is reasonable to assume that in many cases they were in classrooms with peers who had communication or social skills deficits. Although the present study was not designed to examine the bases for informant discrepancies, we offer two possible explanations. Teachers may be more effective evaluators of depression symptom than mothers, at least in terms of CSI-4 ratings, because they have a larger reference group for making such determinations. Alternatively, differences in the demands of school- versus home-environment contribute to contextual variation in child behavior. For example, it is conceivable that more severe ASD social deficits may exacerbate (or more clearly delineate) depression symptoms in the more socially challenging school setting, which may be compounded by co-occurring ADHD. The latter disorder is well-known to be highly sensitive to environmental and task characteristics. Regardless, the notion that ADHD may be a risk factor for depression symptoms in boys with ASD, as it is in nonASD samples, warrants further study.
Relation Between Depression and ASD Symptoms
Owing to the controversy concerning the etiology of co-occurring symptoms that do not define the ASD clinical phenotype, we conducted correlation analyses to determine whether some depression symptoms were more closely associated with specific ASD deficits than others. The results of these analyses indicated divergent findings for mothers’ versus teachers’ ratings and to some extent for boys with ASD ± ADHD, which raise vexing questions about context, informant, and co-morbidity and the comparison of results from different studies. In general, teachers’ and to a lesser extent mothers’ ratings of depression showed a pattern of moderate-strength associations with social deficits, particularly for boys with ASD + ADHD (see Table 4). For one symptom, “shows little interest in pleasurable activities,” which is a defining characteristic of major depressive episode, correlations were r = 0.48 and r = 0.52 for boys with and without co-morbid ADHD, respectively, controlling for IQ. Although it is tempting to interpret this result as simply indicating many children with ASD are expected to lack interest in activities (e.g., making friends) that others consider to be pleasurable, this does not explain the small correlations for mothers’ ratings. Interestingly, ASD communication deficits for the most part were minimally associated with depression. Guttmann-Steinmetz et al. (2010) found a somewhat similar pattern of differential associations for social and communication deficits with anxiety, all of which lends additional support for the Happé and Ronald (2008) fractional-triad model of ASD. The weak associations between depression symptoms and communication deficits also suggests the boys’ verbal ability may not have been a key factor in the informants’ ability to respond to the items, several of which require insight into the boys’ internal state. However, this is a matter of speculation and requires validation with more extensive measures of communication skills. Lastly, the fact that a minimum full-scale IQ of 70 was a subject selection criterion likely impacted this outcome.
Symptom Equivalence and Differential Validity
We do not know whether CSI-4 depression items or DSM-IV depression symptoms are equivalent in ASD versus typically-developing children. For example, ASD pathogenic processes may alter the clinical presentation of specific symptoms of depression or even result in a phenocopy of “true” depression. Unfortunately, although the topic of symptom equivalence has been discussed for decades, there is little programmatic research in this area as it pertains to depression (see Future Directions). A related concern is whether informants were able to make an accurate distinction between ASD and depression symptoms. For example, the ASD + ADHD group had more severe ASD social deficits and perseverative behaviors according to teachers’ ratings than the ASD Only group, and this could have influenced the magnitude of correlations between depression and ASD symptom severity in the ASD + ADHD group (Table 4). However, similarities in correlations between the two ASD groups appear to outweigh differences. Alternatively, co-occurring ADHD may have contributed to the perception of more severe ASD in the school setting, particularly social skills deficits. As the present study was not designed to address let alone resolve these and related issues, they remain topics for future study.
Strengths and Limitations
The present study is exploratory and as such its findings are best conceptualized as hypothesis generating. Major strengths are the size of the samples and their homogeneity with regard to gender, age, intellectual ability, severity of co-occurring ADHD, and geographic region; however, obtained results may not generalize to samples with differing characteristics. Evidence suggests relatively higher rates of depression in adolescents and adults with ASD versus children (Charlot et al. 2008; Ghaziuddin et al. 1998; Hill et al. 2004; Howlin 2000). Whereas the use of an identical measure validated for use with highly divergent samples minimized to some extent group differences resulting from measurement artifact, obtained findings are anchored to some extent to the specific diagnostic and recruitment procedures used in this study. Although we and others (e.g., Lecavalier et al. 2009; Kim et al. 2000) found little relation between IQ or verbal ability and global depression scores in children with ASD (Table 5), it is nevertheless possible the salience of vegetative symptoms in the clinical presentation of depression may be different for individuals with IQ < 70 (cf., Charlot et al. 2008). We did not examine self-report, which is likely to diverge from mother and teacher report (cf., Lopata et al. 2010). Some of the children with ASD were receiving psychotropic medication, which may have influenced caregiver ratings, but there is little controlled research indicating their efficacy for depression in prepubertal children with ASD. Lastly, it is possible referral biases may have impacted obtained findings in spite of the fact that samples were comparable for a number of important variables and were referred primarily for disorders other than depression (see also Schneider et al. 2009).
Future Directions
In spite of excellent sources of information about the identification and clinical management of depression in children with ASD (e.g., Attwood 1998; Ghaziuddin et al. 2002), there are no empirically established, operationalized, consensus criteria for making a clinical diagnosis of depression in this clinical population. Nevertheless, a number of investigators have used one or more accepted procedures for the validation of diagnostic constructs (Feighner et al. 1972; Robins and Guze 1970) to explore potential risk factors and associated clinical features of depression symptoms in ASD (e.g., Barnhill and Smith-Myles 2001; Cook et al. 1994; Gadow et al. 2008; Ghaziuddin et al. 1995; Ghaziuddin and Greden 1998; Hedley and Young 2006; Hill et al. 2004; Kim et al. 2000; Piven and Palmer 1999; Vickerstaff et al. 2007). This remains a pressing area of research not only for depressive disorders but all purported behavioral syndromes within the ASD clinical phenotype.
One concern in the validation of clinical syndromes is evidence of divergence from other similar disorders. Although the interrelation of anxiety and depression is well established, very little is known about their co-occurrence in children with ASD (Charlot et al. 2008; Howlin 2000; Stewart et al. 2006). Evidence from studies of children with ASD indicate somewhat divergent relations of anxiety versus depression with ASD symptom severity (cf., Guttmann-Steinmetz et al. 2010; Pine et al. 2008), biopsychosocial risk factors (Gadow et al. 2008), informant agreement (Lopata et al. 2010), and relative severity compared with controls (Lopata et al. 2010), but mixed results for IQ (cf., Guttmann-Steinmetz et al. 2010; Lecavalier et al. 2009; Sukhodolsky et al. 2008; Weisbrot et al. 2005). In addition, a confirmatory factor analysis of the DSM-IV model of psychiatric syndromes in a large sample (N = 730) of children with ASD supported the distinction between generalized anxiety and depression (Lecavalier et al. 2009). Based on research with non-ASD samples (Moffitt et al. 2007), co-morbid anxiety and depression is likely to be more debilitating than either mono-morbid condition separately and possibly their combined additive effects, but this remains a matter of speculation for children with ASD.
Although the association between specific symptoms of depression and IQ in boys with ASD was modest (Table 5), this may still have clinical implications for certain individuals, especially boys who do not exhibit ADHD behaviors. For example, in community-based samples, higher IQ is usually associated with a stronger potential for adaptive coping strategies to prevent the development of depressive symptoms (Wright et al. 2010). In boys with ASD, however, greater intellectual ability appears to promote greater self-awareness of their own condition, and research indicates this is a risk factor for depressive symptoms (Rieffe et al. 2011; Vickerstaff et al. 2007). Therefore, it is likely treatments aimed at promoting adaptive coping strategies for depression in boys with ASD will need to address this issue.
Summary
Our findings are consistent with prior research showing that diverse neurobehavioral syndromes are associated with differentially greater risk of co-occurring depression symptoms, and extends this observation to boys with ASD. Although the present study is based on the DSM-IV conceptualization of depression, as is the case for almost all related studies in this area, the goal was not to establish research diagnostic criteria. Therefore, future studies will need to identify a valid set of defining characteristics for depression in this clinical population, which also applies to all other behavioral syndromes within the ASD clinical phenotype. Severity of depression symptoms was for the most part comparable for boys with ASD with and without ADHD, which raises a number of interesting questions about pathogenic processes that result in ASD and their role in mood dysregulation as well as criteria for depression in ASD. This having been said, we must bear in mind that the two groups of boys with ASD did appear to differ in teachers’ perceptions of depression symptom severity as well as associations with ASD symptom severity, explanations for which are wanting. It is likely the establishment of valid co-morbid diagnostic constructs will have implications for consensus standards of best clinical practices, evidenced-based interventions, and government-approved indications for pharmaceuticals.
References
American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders, 3rd ed., revised (DSM-III-R). Washington, DC: American Psychiatric Association.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders, 4th ed. (DSM-IV). Washington, DC: American Psychiatric Association.
Attwood, T. (1998). Asperger’s syndrome: A guide for parents and professionals. London: Jessica Kingsley.
Barnhill, G. P., & Smith-Myles, B. (2001). Attributional style and depression in adolescents with Asperger syndrome. Journal of Positive Interventions, 3, 175–190.
Charlot, L., Deutsch, C. K., Albert, A., Hunt, A., Connor, D. F., & McIvane, W. J. (2008). Mood and anxiety symptoms in psychiatric inpatients with autism spectrum disorder and depression. Journal of Mental Health Research in Intellectual Disabilities, 1, 238–253.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Mahwah, NJ: Lawrence Erlbaum.
Comings, D. E., Wu, S., Chiu, C., Ring, R. H., Gade, R., Ahn, C., et al. (1996). Polygenetic inheritance of Tourette syndrome, stuttering, attention deficit hyperactivity, conduct, and oppositional defiant disorder. American Journal of Medical Genetics Part B: Neuropsychiatric Genetics, 67B, 264–288.
Cook, E. H., Jr., Charak, D. A., Arida, J., Spohn, J. A., Roizen, N. J., & Leventhal, B. L. (1994). Depressive and obsessive-compulsive symptoms in hyperserotonemic parents of children with autistic disorder. Psychiatry Research, 52, 25–33.
Daviss, W. B. (2008). A review of co-morbid depression in pediatric ADHD: Etiologies, phenomenology, and treatment. Journal of Child and Adolescent Psychopharmacology, 18, 565–571.
Drabick, D. A. G., Gadow, K. D., & Loney, J. (2007). Source-specific oppositional defiant disorder: Comorbidity and risk factors in referred elementary school boys. Journal of the American Academy of Child and Adolescent Psychiatry, 46, 92–101.
Drabick, D. A. G., Gadow, K. D., & Loney, J. (2008). Co-occurring ODD and GAD symptom groups: Source-specific syndromes and cross-informant comorbidity. Journal of Clinical Child and Adolescent Psychology, 37, 314–326.
Feighner, J. P., Robins, E., Guze, S. B., Woodruff, R. A., Winokur, G., & Munoz, R. (1972). Diagnostic criteria for use in psychiatric research. Archives of General Psychiatry, 26, 57–63.
Feise, R. J. (2002). Do multiple outcome measures require p-value adjustment? BMC Medical Research Methodology, 2.
Gadow, K. D., DeVincent, C. J., & Pomeroy, J. (2006). ADHD symptom subtypes in children with pervasive developmental disorder. Journal of Autism and Developmental Disorders, 36, 271–283.
Gadow, K. D., DeVincent, C. J., Pomeroy, J., & Azizian, A. (2004a). Psychiatric symptoms in preschool children with PDD and clinic and comparison samples. Journal of Autism and Developmental Disorders, 34, 379–393.
Gadow, K. D., DeVincent, C. J., Pomeroy, J., & Azizian, A. (2005). Comparison of DSM-IV symptoms in elementary school-aged children with PDD versus clinic and community samples. Autism, 9, 392–415.
Gadow, K. D., DeVincent, C., & Schneider, J. (2008). Predictors of psychiatric symptoms in children with an autism spectrum disorder. Journal of Autism and Developmental Disorders, 38, 1710–1720.
Gadow, K. D., DeVincent, C. J., & Schneider, J. (2009). Comparative study of children with ADHD Only, autism spectrum disorder + ADHD, and chronic multiple tic disorder + ADHD. Journal of Attention Disorders, 12, 474–485.
Gadow, K. D., Nolan, E. E., Sprafkin, J., & Schwartz, J. (2002). Tics and psychiatric comorbidity in children and adolescents. Developmental Medicine and Child Neurology, 44, 330–338.
Gadow, K. D., & Sprafkin, J. (1986). Stony Brook Child Psychiatric Checklist-3. Stony Brook: Department of Psychiatry, State University of New York.
Gadow, K. D., & Sprafkin, J. (2002). Child symptom inventory-4 screening and norms manual. Stony Brook, NY: Checkmate Plus.
Gadow, K. D., & Sprafkin, J. (2010). The symptom inventories: An annotated bibliography. Available: www.checkmateplus.com [On-line].
Gadow, K. D., Sprafkin, J., Salisbury, H., Schneider, J., & Loney, J. (2004b). Further validity evidence for the teacher version of the Child Symptom Inventory-4. School Psychology Quarterly, 19, 50–71.
Gadow, K. D., Sverd, J., Nolan, E. E., Sprafkin, J., & Schneider, J. (2007). Immediate-release methylphenidate for ADHD in children with comorbid chronic multiple tic disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 46, 840–848.
Ghaziuddin, M., Alessi, N., & Greden, J. (1995). Life events and depression in children with pervasive developmental disorders. Journal of Autism and Developmental Disorders, 25, 495–502.
Ghaziuddin, M., Ghaziuddin, N., & Greden, J. (2002). Depression in persons with autism: Implications for research and clinical care. Journal of Autism and Developmental Disorders, 32, 299–306.
Ghaziuddin, M., & Greden, J. (1998). Depression in children with autism/pervasive developmental disorders: A case-control family history study. Journal of Autism and Developmental Disorders, 28, 111–115.
Ghaziuddin, M., Weidmer-Mikhail, E., & Ghaziuddin, N. (1998). Comorbidity in Asperger’s syndrome. A preliminary research. Journal of Intellectual Disability Research, 42, 279–283.
Girirajan, S., Rosenfeld, J. A., Cooper, G. M., Antonacci, F., Siswara, P., Itsara, A., et al. (2010). A recurrent 16p12.1 microdeletion supports a two-hit model for severe developmental delay. Nature Genetics, 42, 203–210.
Guttmann-Steinmetz, S., Gadow, K. D., & DeVincent, C. J. (2009). Oppositional defiant and conduct disorder behaviors in boys with autism spectrum disorder with and without attention-deficit hyperactivity disorder versus several comparison samples. Journal of Autism and Developmental Disorders, 39, 976–985.
Guttmann-Steinmetz, S., Gadow, K. D., DeVincent, C. J., & Crowell, J. (2010). Anxiety symptoms in boys with autism spectrum disorder, attention-deficit hyperactivity disorder, or chronic multiple tic disorder and community controls. Journal of Autism and Developmental Disorders, 40, 1006–1016.
Hallett, V., Ronald, A., & Happé, F. (2009). Investigating the association between autistic-like and internalizing traits in a community-based twin sample. Journal of the American Academy of Child and Adolescent Psychiatry, 48, 618–627.
Happé, F., & Ronald, A. (2008). The ‘fractionable autism triad’: A review of evidence from behavioural, genetic, cognitive and neural research. Neuropsychology Review, 18, 287–304.
Hedley, D., & Young, R. (2006). Social comparison processes and depressive symptoms in children and adolescents with Asperger syndrome. Autism, 10, 139–153.
Hill, E., Berthoz, S., & Frith, U. (2004). Cognitive processing of own emotions in individuals with autistic spectrum disorder and in their relatives. Journal of Autism and Developmental Disorders, 34, 229–235.
Hollingshead, A. B. (1975). Four factor index of social status. New Haven, CT: Department of Sociology, Yale University.
Howlin, P. (2000). Outcome in adult life for more able individuals with autism or Asperger syndrome. Autism, 4, 63–83.
Kanne, S. M., Christ, S. E., & Reiersen, A. M. (2009). Psychiatric symptoms and psychosocial difficulties in young adults with autistic traits. Journal of Autism and Developmental Disorders, 39, 827–833.
Kim, J. A., Szatmari, P., Bryson, S. E., Streiner, D. L., & Wilson, F. J. (2000). The prevalence of anxiety and mood problems among children with autism and Asperger syndrome. Autism, 4, 117–132.
Lecavalier, L., Gadow, K. D., DeVincent, C. J., & Edwards, M. C. (2009). Validation of DSM-IV model of psychiatric syndromes in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 39, 278–289.
Lopata, C., Toomey, J. A., Fox, J. D., Volker, M. A., Chow, S. Y., Thomeer, M. L., et al. (2010). Anxiety and depression in children with HFASDs: Symptom levels and source differences. Journal of Abnormal Child Psychology, 38, 765–776.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Jr, Leventhal, B. L., DiLavore, P. C., et al. (2000). The autism diagnostic observation schedule-generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30, 205–223.
Mandell, D. S., Morales, K. H., Marcus, S. C., Stahmer, A. C., & Doshi, J. (2008). Psychotropic medication use among Medicaid-enrollled children with autism spectrum disorder. Pediatrics, 121, e441–e448.
Moffitt, T. E., Harrington, H., Caspi, A., Kim-Cohen, J., Goldberg, D., Gregory, A. M., et al. (2007). Depression and generalized anxiety disorder: Cumulative and sequential comorbidity in a birth cohort followed prospectively to age 32 years. Archives of General Psychiatry, 64, 651–660.
Perneger, T. V. (1998). What’s wrong with Bonferroni adjustments. British Medical Journal, 316, 1236–1238.
Pierre, C. B., Nolan, E. E., Gadow, K. D., Sverd, J., & Sprafkin, J. (1999). Comparison of internalizing and externalizing symptoms in children with attention-deficit hyperactivity disorder with and without comorbid tic disorder. Journal of Developmental and Behavioral Pediatrics, 20, 170–176.
Pine, D. S., Guyer, A., Goldwin, M., Towbin, K. A., & Leibenluft, E. (2008). Autism spectrum disorder scale scores in pediatric mood and anxiety disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 47, 652–661.
Piven, J., & Palmer, P. (1999). Psychiatric disorder and the broad autism phenotype: evidence from a family study of multiple-incidence autism families. American Journal of Psychiatry, 156, 557–563.
Reich, W. (2000). Diagnostic Interview for Children and Adolescents (DICA). Journal of the American Academy of Child and Adolescent Psychiatry, 39, 59–66.
Rieffe, C., Oosterveld, P., Meerum Terwogt, M., Mootz, S., Van Leeuwen, E. & Stockmann, A. P. A. M. (2011). Emotion regulation and internalizing symptoms in children with Autism Spectrum Disorders. Autism. doi:10.1177/1362361310366571.
Robertson, M. M. (2006). Mood disorders and Gilles de la Tourette’s syndrome: an update on prevalence, etiology, comorbidity, clinical associations, and implications. Journal of Psychosomatic Research, 61, 349–358.
Robins, E., & Guze, S. B. (1970). Establishment of diagnostic validity in psychiatric illness: Its application to schizophrenia. American Journal of Psychiatry, 126, 983–986.
Rommelse, N. N. J., Franke, B., Geurts, H. M., Hartman, C. A., & Buitelaar, J. K. (2010). Shared heritability of attention-deficit/hyperactivity disorder and autism spectrum disorder. European Child and Adolescent Psychiatry, 19, 281–295.
Rothman, K. (1990). No adjustments are needed for multiple comparisons. Epidemiology, 1, 43–46.
Schneider, J., Gadow, K. D., Crowell, J. A., & Sprafkin, J. (2009). Anxiety in boys with ADHD with and without chronic multiple tic disorder. Journal of Child and Adolescent Psychopharmacology, 19, 1–12. doi:10.1089/cap.2009.0013.
Sprafkin, J., Gadow, K. D., Salisbury, H., Schneider, J., & Loney, J. (2002a). Further evidence of reliability and validity of the Child Symptom Inventory-4: Parent checklist in clinically referred boys. Journal of Clinical Child and Adolescent Psychology, 31, 513–524.
Sprafkin, J., Volpe, R. J., Gadow, K. D., Nolan, E. E., & Kelly, K. (2002b). A DSM-IV-referenced screening instrument for preschool children: The early childhood inventory-4. Journal of the American Academy of Child and Adolescent Psychiatry, 41, 604–612.
Stewart, M. E., Barnard, L., Pearson, J., Hasan, R., & O’Brien, G. (2006). Presentation of depression in autism and Asperger syndrome A review. Autism, 10, 103–116.
Sukhodolsky, D. G., Scahill, L., Gadow, K. D., Eugene, A. L., Aman, M. G., McDougle, C. J., et al. (2008). Parent-rated anxiety symptoms in children with pervasive developmental disorders: Frequency and association with core autism symptoms and cognitive functioning. Journal of Abnormal Child Psychology, 36, 117–128.
Sverd, J. (2003). Psychiatric disorders in individuals with pervasive developmental disorder. Journal of Psychiatric Practice, 9, 111–127.
Vickerstaff, S., Heriot, S., Wong, M., Lopes, A., & Dossetor, D. (2007). Intellectual ability, self-perceived social competence, and depressive symptomatology in children with high-functioning autistic spectrum disorders. Journal of Autism and Developmental Disorders, 37, 1647–1664.
Weisbrot, D. M., Gadow, K. D., DeVincent, C. J., & Pomeroy, J. (2005). The presentation of anxiety in children with pervasive developmental disorders. Journal of Child and Adolescent Psychopharmacology, 15, 477–496.
White, S. W., & Roberson-Nay, R. (2009). Anxiety, social deficits, and loneliness in youth with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 1006–1013.
Wright, M., Banerjee, R., Hoek, W., Rieffe, C., & Novin, S. (2010). Depression and social anxiety in children: Differential links with coping strategies. Journal of Abnormal Child Psychology, 38, 405–419.
Zhang, J., Quan, H., Ng, J., & Stepanavage, M. E. (1997). Some statistical methods for multiple endpoints in clinical trials. Control Clin Trials, 18, 204–221.
Acknowledgments
This study was supported, in part, by grants awarded to Dr. Gadow from the Tourette Syndrome Association, Inc., National Institute of Mental Health (MH 45358), and the Matt and Debra Cody Center for Autism and Developmental Disorders. The authors wish to thank Dr. John Pomeroy, Dr. Joyce Sprafkin, and Dr. Jeff Sverd for their respective roles in the diagnostic evaluations and anonymous reviewers for their helpful comments.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gadow, K.D., Guttmann-Steinmetz, S., Rieffe, C. et al. Depression Symptoms in Boys with Autism Spectrum Disorder and Comparison Samples. J Autism Dev Disord 42, 1353–1363 (2012). https://doi.org/10.1007/s10803-011-1367-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-011-1367-x