
Abstract
Changes in the Wechsler Intelligence Scales for Children-IV (WISC-IV) may affect the IQ profile characteristic of autism spectrum disorders (ASD). Moreover, the association of particular component cognitive abilities (unlike overall IQ) with symptomatology and adaptive functioning in ASD remains unclear. This archival study characterizes the WISC-IV IQ profile among 56 high-functioning (IQ > 70) children with ASD and correlates WISC-IV performance with ASD and ADHD symptomatology and adaptive functioning. The ASD WISC-IV profile included strengths on Matrix Reasoning and Similarities, weaknesses on Comprehension (which correlated negatively with social symptoms) and the subtests comprising the Processing Speed Index (Coding, Symbol Search). Processing speed task performance correlated negatively with communication symptoms and positively with communication abilities, indicating its importance to functional outcomes in ASD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Intellectual functioning is one of the most widely studied psychological processes among individuals with Autism Spectrum Disorders (ASD). One primary use of IQ measures in this population is the differentiation between high- and low-functioning individuals because of its relevance to school placement. Intellectual functioning is also an important predictor of outcome in ASD (Billstedt et al. 2007; Venter et al. 1992); it is essential for monitoring progress and development (Koegel et al. 1997), and also has been used for the purposes of differential diagnosis (Goldstein et al. 2008). Subscale profile analysis is another common, if controversial (Fiorello et al. 2001; Pfeiffer et al. 2000), use of intelligence measures that is particularly relevant in ASD, which is characterized by unusual variability in performance (Dawson et al. 2007; Goldstein et al. 2008). Of the plethora of intellectual or cognitive ability measures available in the psychologist’s toolkit, the Wechsler scales are the most researched and widely used tests, particularly in ASD populations.
A commonly reported Wechsler profile among school age children with ASD includes lower scores on the Freedom from Distractibility Index (FDI, replaced by the Working Memory Index, or WMI on the Wechsler Intelligence Scale for Children, Fourth Edition [WISC-IV]) and the Processing Speed Index (PSI), when compared with the Verbal Comprehension Index (VCI) and the Perceptual Organization Index (POI; named Perceptual Reasoning Index, or PRI on the WISC-IV) (Mayes and Calhoun 2003, 2008; Nyden et al. 2001; Wechsler 2003). When examining subtest performance at the group level, most studies find relatively high scores on Block Design and low scores on Comprehension and Coding/Digit Symbol (Allen et al. 1991; Asarnow et al. 1987; Dennis et al. 1999; Freeman et al. 1985; Happé 1994; Koyama et al. 2006, 2007; Lincoln et al. 1988; Mayes and Calhoun 2003, 2004; Nyden et al. 2001; Siegel et al. 1996). In fact, Mayes and Calhoun (2004) were able to identify children with high-functioning autism with 73% accuracy based on lower FDI, PSI, and Comprehension subtest scores on the WISC-III. Although this profile has been consistently reported across various age groups and functioning levels, it does not confer diagnostic utility (Siegel et al. 1996).
Because studies of other clinical groups (e.g., children with traumatic brain injury) have shown profile differences when comparing the WISC-IV to older versions of the WISC (e.g., Donders and Jenke 2008), it is important to establish the WISC-IV profile in ASD. Only one of the previously mentioned studies (Mayes and Calhoun 2008) and preliminary data reported in the WISC-IV manual (Wechsler 2003) examine this profile in ASD using the most recent version of the Wechsler scales for children. Their findings are generally consistent with previous findings on the WISC-III, particularly the relative weaknesses on the WMI and PSI (the lowest mean Index score) when compared to the VCI and PRI, although in contrast with the Mayes and Calhoun findings, the WISC-IV normative data indicates solidly average performance on the WMI. WISC-IV subtest analyses reveal relatively low scores in Digit Span, Letter Number Sequencing, Symbol Search, and Coding. It is important to note that processing speed and motor output speed are confounded in the PSI, which is comprised of the motorically demanding Coding subtest and the Symbol Search subtest, which has motor demands as well, though minimized compared to the Coding subtest. Among the subtests that comprise the verbal composite (i.e., VCI), Comprehension is highlighted as the low score, while Similarities is the high score. A relative strength is now reported on the newly added Matrix Reasoning subtest. Indeed, Mayes and Calhoun (2008) find that Matrix Reasoning (followed by Picture Concepts, not Block Design), is the peak subtest score on the PRI, perhaps due to its lack of speed demands and minimal motor planning requirements, when compared with Block Design. Mayes and Calhoun (2008) suggest that this profile reflects strengths in verbal and visual reasoning, and weaknesses in attention, graphomotor, and processing speed in children with high-functioning autism.
Given fairly consistent IQ profiles associated with ASD, one question that arises is how autism symptomatology relates to performance on IQ measures. Joseph et al. (2002) examined the relationship of performance on the Differential Ability Scales (Elliott 1990) with autism symptoms derived from the Autism Diagnostic Observation Schedule (Lord et al. 1999) in a group of children with ASD. They found that, when compared with children with no significant difference between verbal and nonverbal abilities, children with lower verbal abilities (relative to nonverbal abilities) presented more communication and social difficulties while children with discrepantly higher nonverbal cognitive abilities demonstrated more social symptoms. Another recent study (Black et al. 2009) also found that social symptomatology was related to significant differences between Wechsler Verbal and Performance IQs.
In addition to the symptoms comprising the diagnostic criteria of ASD, other co-morbid behaviors are commonly observed in individuals with ASD, such as those associated with Attention Deficit/Hyperactivity Disorder (ADHD). ADHD symptom comorbidity with ASD has been reported to be as high as 59% (Goldstein and Schwebach 2004) to 67.9% (Yoshida and Uchiyama 2004). A third investigation found that approximately 30% of children with high-functioning ASD met full diagnostic criteria for ADHD and up to 55% of them exhibited elevated ADHD symptoms (Leyfer et al. 2006). There is evidence that ADHD in ASD is associated with differences in autism symptomatology, executive functioning (Sinzig et al. 2008), and adaptive behaviors (Yerys et al. 2009), although there are no studies of which we are aware that address the Wechsler IQ profile in ASD plus ADHD. There are, however, prior studies that examined the Wechsler IQ profiles in children with ADHD alone, which find depressed scores on FDI (WISC-III) and PSI, particularly the Coding subtest, but not on the Comprehension subtest (Calhoun and Mayes 2005; Mayes and Calhoun 2003, 2004). On the WISC-IV in particular, ADHD is associated with weaknesses on the WMI and PSI. For example, one study demonstrated that all 118 children with ADHD assessed with the WISC-IV scored lowest on either the WMI or the PSI (Mayes and Calhoun 2006). Furthermore, prior studies have demonstrated an association between ADHD symptoms and weaknesses in both working memory (e.g., Tillman et al. 2011) and processing speed (Chhabildas et al. 2001).
In addition to symptomatology, adaptive behavior, or the ability to function independently in real life (Sparrow et al. 2005), is an important measure of outcome in ASD. Klin et al. (2007) suggest that adaptive abilities, previously under-investigated in high-functioning children and adolescents on the autism spectrum, provide an important indicator of functioning independent from autism symptoms, or disabilities, and a target for intervention that is not captured by IQ. In ASD individuals, those abilities are consistently impaired in most, if not all domains, but particularly in socialization skills (Bolte and Poustka 2002; Carter et al. 1998; Kenworthy et al. 2010). IQ is more predictive of adaptive behavior in ASD with intellectual disability (e.g., Liss et al. 2001; Bolte and Poustka 2002), than in those who are high functioning (Bolte and Poustka 2002; Freeman et al. 1999; Liss et al. 2001; Volkmar et al. 1987; Kenworthy et al. 2005). While Klin et al. (2007) and Kenworthy et al. (2010) find significant correlations between adaptive communication and IQ in three high-functioning ASD samples, adaptive social skills do not appear to have a significant association with intelligence in children with high-functioning ASD (Freeman et al. 1999; Kenworthy et al. 2010). These studies have compared adaptive functioning with scores on several intelligence tests, including the Wechsler scales, but adaptive profiles have not been investigated in relation to the WISC-IV index/subtest profiles.
The purpose of the present study is to examine WISC-IV profiles associated with high-functioning ASD and the relationship of these profiles to ASD and ADHD symptomatology and adaptive functioning. Based on previous research, it is hypothesized that the WISC-IV profile in this sample of high-functioning individuals with ASD will reveal a strength on the Matrix Reasoning subtest, and weaknesses on the Comprehension, Coding, and Symbol Search subtests; and that adaptive communication will be positively related to overall IQ, while adaptive socialization will correlate with the socially-relevant Comprehension subtest score. It is further predicted that ASD social-communication symptoms will correlate negatively with IQ and that ADHD symptoms within this ASD sample will relate negatively with WISC-IV WMI and PSI indices and subtests.
Method
Participants
Participants are a clinically referred sample of 56 consecutive cases of children (46 [82.1%] males) with an autism spectrum disorder diagnosis (high-functioning autism n = 22; Asperger syndrome n = 22; PDD-NOS n = 12) and both complete WISC-IV data and ADOS/ADI data for diagnostic confirmation. All participants were evaluated at the Center for Autism Spectrum Disorders at Children’s National Medical Center in the Washington, DC metropolitan area. Each child received a comprehensive neuropsychological evaluation or a multidisciplinary team evaluation that included a detailed medical and developmental history, an extensive neuropsychological battery, as well as administration of the Autism Diagnostic Interview (ADI; Le Couteur et al. 1989) or the Autism Diagnostic Interview-Revised (ADI-R; Lord, et al. 1994) and the Autism Diagnostic Observation Schedule (ADOS; Lord et al. 1999) by a trained, research reliable clinician. Data were collected as part of a clinical evaluation, thus not all participants received all measures. Parents of children whose clinical data were used in the study were informed via an IRB approved fact sheet for this human subjects IRB approved investigation of de-identified archival data.
Diagnoses were based on DSM-IV criteria and results from the ADI/ADI-R, ADOS, and developmental history. In addition to meeting DSM-IV diagnostic criteria, all participants also met the criteria for a “broad Autism Spectrum Disorder” on the ADI/ADI-R and/or ADOS established by the NICHD/NIDCD Collaborative Programs for Excellence in Autism (Lainhart et al. 2006). Because the ADI/ADI-R and ADOS do not have an algorithm for Asperger syndrome, Lainhart and colleagues developed criteria that include an individual on the broad autism spectrum if they: meet the ADI/ADI-R cut off for autism in the social domain and at least one other domain or meet the ADOS cutoff for the combined social and communication score. All participants also had an IQ standard score of 70 or higher on the WISC-IV VCI or PRI. Sample characteristics, including age, socioeconomic status, raw scores for the ADI/ADI-R and ADOS, as well as standardized Vineland domain scores and ADHD Rating Scale index scores, are presented in Table 1.
Measures
Autism Diagnostic Measures
Children were diagnosed with the Autism Diagnostic Interview (ADI; Le Couteur et al. 1989) and the Autism Diagnostic Interview-Revised (ADI-R; Lord et al. 1994), which are detailed parent or caregiver interviews of developmental history and autism symptoms. Scores are aggregated into symptom clusters that correspond to DSM-IV criteria for a diagnosis of autism. The Autism Diagnostic Observation Schedule (ADOS; Lord et al. 1999) is a structured play and conversational interview that includes a series of social presses and other opportunities to elicit symptoms of an ASD. One of four different ADOS modules is administered depending on the expressive language level and chronological age of the individual. Given the age and functioning level of the participants in this study, only Modules 3 or 4 were administered. Scores for the ADI and ADOS are presented as non-standardized raw scores.
Measures of ASD and ADHD Symptoms
ADOS (see above) Reciprocal Social Interaction and Communication raw scores were used as ASD symptom correlates in all analyses.
The ADHD Rating Scale (DuPaul et al. 1998) is an 18-item parent questionnaire that measures ADHD symptoms (presented as T-scores: mean = 50; standard deviation = 10) in comparison to nationally representative norms (one standard deviation or higher above the mean constitutes significant elevation). This scale is derived from the DSM-IV criteria for a diagnosis of ADHD providing indices of inattention and hyperactivity symptoms separately as well as combined together and it has shown good predictive validity in discriminating children with ADHD from typically developing children (Power et al. 1998).
Adaptive Behavior Measure
The Vineland Adaptive Behavior Scale, Second Edition: Survey Interview Form (Sparrow et al. 2005) is a parent and caregiver interview of adaptive behaviors (presented as standard scores: mean = 100; standard deviation = 15) completed with a clinician. The questions are structured in four main domains: Communication, Daily Living Skills, Socialization, and Motor Skills. Because the Motor domain is not required for individuals 7 years and older, not all data points were available, and therefore, this domain was not used for analysis.
Cognitive Abilities Measure
The Wechsler Intelligence Scale for Children–Fourth Edition (Wechsler 2003) is a measure of intellectual ability and cognitive processing. It has 10 core and five supplemental subtests. The subtests (represented with scaled scores: mean = 10; standard deviation = 3) can be clustered into composite quotients for four indices (represented as standard scores: mean = 100; standard deviation = 15): the Verbal Comprehension Index (VCI), the Perceptual Reasoning Index (PRI), the Working Memory Index (WMI), and the Processing Speed Index (PSI). Because these scores were derived from clinical cases, WMI was not always calculated in the same way; in accordance with the WISC-IV Administration and Scoring Manual (Wechsler 2003) the optional Arithmetic subtest was substituted for Letter Number Sequencing when Letter Number Sequencing was invalidated or if the examiner deemed Arithmetic a preferable substitute (n = 7). In all other cases the standard Digit Span and Letter Number Sequencing combination was used.
Data analytic Plan
Frequencies, means, and standard deviations for IQ index and subtest scores as well as symptom counts and adaptive behavior ratings were calculated and examined for scatter, skewness, and kurtosis before proceeding with analyses. To determine the differences from the normal population mean expectations, data were analyzed initially using one sample t-tests. Repeated measures ANOVAs were used to investigate within group differences among index and subtest scores. After confirming that data were sufficiently normally distributed, Pearson correlations were used to assess the relationship between IQ and both ASD and ADHD symptomatology as well as adaptive functioning. For ASD symptomatology, only the ADOS social and communication scores were utilized because ADI scores are not contemporaneous with IQ assessment (given the assessment of symptoms during a period of prototypical expression [i.e., ages 4–5]) and the ADOS stereotyped behavior scale is not considered a good metric of nonsocial difficulties in ASD because there is a limited window (usually 45–60 min) in which to observe these often highly contextual behaviors.
Results
Descriptive Statistics
Inspection of data did not reveal any problems with skewness, kurtosis, outliers, or the presence of a bimodal distribution. As seen in Table 1, scores on the ADHD Rating Scale were on average at least one standard deviation above the mean. Vineland scores in Communication and Daily Living Skills were on average one standard deviation below the mean. The mean score on the Socialization domain was almost two standard deviations below the mean.
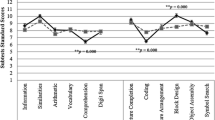
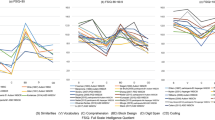
WISC-IV index and subtest scores are summarized in Table 2. Because this is a clinical dataset and not all data points were available for all subjects, Picture Concepts and Letter Number Sequencing subtests were not used for subtest analysis. The only index score that differed significantly from the ‘population mean’ of 100 was PSI (t(55) = −5.64, p < .001). When examining individual differences, 14.3% of individuals with ASD scored two or more standard deviations below the population mean (i.e., a standard score ≤70) on the PSI, and 12.5% scored 70 or lower on the VCI, despite a solidly average mean score on the VCI.
When examining differences from the population mean at the subtest level, Coding (t(55) = −5.49, p < .001), Symbol Search (t(55) = −4.15, p < .001), and Comprehension (t(55) = −4.05, p < .001) scores emerged as significantly lower, while Similarities (t(55) = 3.54, p = .001) and Matrix Reasoning (t(55) = 2.28, p = .03) scores were significantly higher, than the normative sample score of 10. A significant minority of individuals scored two standard deviations or more below the population mean (i.e., a scaled score of 4 or lower) on the Coding (21.4%) and Comprehension (21.4%) subtests.
Within Group Comparisons
Examining within group differences among WISC-IV index scores revealed significant differences (F(3,52) = 18.32, p < .001). Results from post-hoc analyses showed that the PSI was significantly (ps < .01) lower than the PRI (Cohen’s d = −0.89), VCI (Cohen’s d = −0.65), and WMI (Cohen’s d = −0.44). Post-hoc analyses also revealed that PRI was significantly (ps < .03) higher than the WMI (Cohen’s d = 0.57) and VCI (Cohen’s d = 0.31).
Within group differences on subtest performance were also found (F(7,55) = 19.8, p < .001). Post-hoc analyses confirmed that Coding, Comprehension, and Symbol Search were significantly (ps < .01) lower than Block Design, Similarities, Vocabulary, Digit Span, and Matrix Reasoning. Additionally, the Similarities subtest score was significantly (ps < .02) higher than the Block Design and Vocabulary subtest scores while the Digit Span subtest score was significantly (ps < .03) lower than the Matrix Reasoning subtest score but higher than the Symbol Search subtest score. Effect sizes were also calculated and ranged from small (Digit Span and Symbol Search, Cohen’s d = 0.31) to large (Comprehension and Similarities, Cohen’s d = 1.37). All of the significant differences (for both index and subtest score comparisons) reported above survived correction for multiple comparisons using the false discovery rate (q < .05; Benjamini and Hochberg 1995).
Pearson correlations were used to assess the relationship between IQ and adaptive behavior as well as IQ and ASD and ADHD symptomatology scores (see Tables 3, 4). Adaptive communication abilities, as measured by the Vineland, were significantly positively correlated with the WISC-IV VCI, WMI (ps < .01), PRI and PSI (ps < .05). Several significant negative correlations (higher symptom counts associated with lower IQ scores) were also found between the ADOS and the WISC-IV. The ADOS Communication score was negatively correlated (ps < .01) with all WISC-IV verbal subtests (i.e., Vocabulary, Similarities and Comprehension), and therefore, with the VCI. The ADOS Communication score was also negatively associated with scores from the Coding and Symbol Search subtests and therefore the PSI score (ps < .05). Only the Vocabulary and Comprehension subtests (and therefore the VCI) were negatively correlated (ps < .05) with the ADOS Reciprocal Social Interaction score. No significant correlations were found between IQ scores and ADHD Rating Scale scores. It is important to note that even if the sample was constrained to those subjects with ADHD Rating Scale data (n = 45), all of the aforementioned correlational findings remained.
Discussion
This study examined the WISC-IV profile in high-functioning (mean FSIQ = 97) children with ASD, and its relationship to ASD and ADHD symptomatology as well as adaptive abilities. As hypothesized, the ASD WISC-IV profile was generally consistent with previous findings, revealing weaknesses in processing/motor output speed and complex/social language. The Processing Speed Index (PSI) was the greatest area of relative and normative weakness in the ASD group. More than half (55%) of our sample scored at least a full standard deviation below the PSI normative mean score. Furthermore, our data expand on previous reports by demonstrating that performance on the PSI is related to autism communication symptoms and adaptive communication abilities, but not, as we predicted, to ADHD symptoms in this ASD sample. We also found expected strengths on structured, brief, motor-free subtests of the WISC-IV (Similarities and Matrix Reasoning) and weaknesses on a subtest with complex/social language demands (Comprehension). Adaptive behavior was impaired compared to FSIQ, as expected, with the greatest discrepancy between IQ and the Vineland Socialization domain score. Consistent with our predictions, the Vineland Communication domain score was strongly correlated with many WISC-IV subtests, particularly those composing the VCI (i.e., Similarities, Vocabulary, and Comprehension), but Vineland Daily Living and Socialization domain scores were not significantly correlated with any WISC-IV measure (with the exception of the Daily Living Skills and Digit Span correlation). Autism communication symptoms, as measured by the ADOS, were negatively correlated with VCI as well as PSI scores, while ADOS social symptoms were negatively correlated with performance on the VCI, including two of its constituent subtests: Vocabulary and Comprehension. In general, the ASD WISC-IV profile described in the current study is consistent with prior reports (Mayes and Calhoun 2008; Wechsler 2003). We found very clear and consistent deficits in processing speed (whether on the PSI or its constituent subtests) among children with ASD; however, because of task impurity, it is unclear whether this relative weakness reflects actual ‘cognitive’ processing speed, motor speed difficulties, or the two combined. Several recent studies using the inspection time task, a processing speed measure free from motor demands, suggest intact or better processing speed among individuals with ASD. Scheuffgen et al. (2000) found that children with ASD and below average IQ (mean = 82) demonstrated surprisingly fast processing speed, when asked to complete a perceptual discrimination in which the stimuli appeared on the computer screen for a variable amount of time, compared to children with intellectual disabilities. The ASD group’s processing speed was comparable to that of a group of typically developing children with IQ scores 25 points higher, on average. The two most recent studies using the inspection time task extend these results finding comparable processing speed between: (1) a group of relatively high-functioning children with ASD and age and IQ matched typically developing children (Wallace et al. 2009a) and (2) an adult savant with ASD and a control group of neurotypical adults matched on age and verbal ability (Wallace et al. 2009b). This juxtaposition of ASD-related deficits and assets on purported but differing processing speed tasks indicates that there is a significant distinction between processing speed in the context of motor and non-motor tasks, at least among individuals with ASD. More research is needed to reconcile the conflicting findings from investigations using standardized and experimental tasks of processing speed in ASD samples.
Our findings are also consistent with those of Mayes and Calhoun (2008) on the VCI and PRI subtests measuring core verbal and nonverbal concepts and problem solving. We found the expected pattern of higher Similarities, intermediate Vocabulary and low Comprehension scores. Likewise, Matrix Reasoning was the highest score on the PRI. In general, these results indicate that ASD children can show their strengths more consistently when they are asked to provide short verbal responses or complete untimed, motor-free nonverbal tasks.
In contrast to the Mayes and Calhoun findings, but consistent with data reported in the WISC-IV Technical and Interpretive Manual (2003) on 27 children diagnosed with Asperger’s Disorder, we found Working Memory Index (WMI) scores fell in the average range. In the sample described by Mayes and Calhoun (2008) the WMI score was below average, attributed to attention problems by these authors; however, no formal attention measure was administered to confirm this association. In the present study, the hypothesis of attention problems contributing to this or other relationships with IQ was not supported as no correlation was found between ADHD symptoms (measured by the ADHD Rating Scale) and performance on any index or subtest of the WISC-IV. It is important to note, however, that this was a clinical sample with some variability in the way the WMI was calculated. For example, in some cases the Digit Span and Letter Number Sequencing combination was used, while in others the optional Arithmetic subtest was substituted for Letter Number Sequencing. As reported in the Wechsler Technical and Interpretative Manual (Wechsler 2003), there is a relatively lower correlation between Arithmetic and WMI (r = .57) when compared to the correlation between Letter Number Sequencing and WMI (r = .86). Thus, the cognitive demands of those tasks might differ, and might be biased or confounded by extraneous processes, such as mathematical abilities.
Extending prior work, we sought to examine the relationship between specific cognitive abilities and both adaptive functioning and (ASD and ADHD) symptomatology. One of our more provocative findings is that processing speed is not only a relative impairment for children with ASD on WISC-IV measures, but is also correlated positively with their communication abilities and inversely with communication disabilities. Therefore, processing speed, at least as conceptualized by the Wechsler scales, may moderate communication skills and communication deficits in ASD. Historically, there is a link between auditory processing speed and language learning disorders (Tallal 2004), commonly found in ASD, which may be reflected in our findings. Given that the Wechsler processing speed tasks are primarily visuomotor, these correlations may also reflect the dynamic and fast-changing nature of not only verbal, but also nonverbal communication within the context of social interactions.
Surprisingly, we did not find significant correlations between ADHD symptoms and performance on the WISC-IV in this sample of high-functioning children with ASD. Previous studies have shown a similar pattern of lower scores on the PSI and WMI relative to VCI and PRI for both ADHD and ASD groups; however, Comprehension subtest performance distinguishes the groups with ASD children obtaining lower scores (e.g., Calhoun and Mayes 2005; Mayes and Calhoun 2003, 2004). Based on findings from the current study, it is particularly striking that ADHD symptomatology is not associated with poor performance on the PSI subtests among high-functioning children with ASD while ASD symptomatology is. However, another possibility is that our findings join others in the literature demonstrating limited associations between behavioral and neuropsychological measures of attention (e.g., McAuley et al. 2010).
We predicted that only the Communication domain of the Vineland would correlate with all WISC-IV indices, suggesting a strong association between overall IQ and communication skills. Klin et al. (2007) found strong correlations between Vineland Communication scores and Verbal IQ (as measured by the WISC-III) but unlike the present study; no significant correlations were noted with Performance IQ. To our knowledge, the WISC-IV Technical and Interpretative Manual (Wechsler 2003) includes the only data associating WISC-IV Performance scores with adaptive functioning. In that sample of typically developing children, low to moderate correlations were found between the Conceptual composite of the Adaptive Behavior Assessment System-II and all WISC-IV Composites, with WMI and VCI showing the highest correlations (r = .45) and PSI the lowest (r = .25). Other moderate correlations included the Social composite score with VCI and WMI (r = .36 and r = .35, respectively; Wechsler 2003). Taken together, the most consistent link across samples and diagnoses is between verbal ability and adaptive communication skills.
Our finding that ADOS communication symptoms were inversely correlated with verbal abilities is consistent with investigations by Klin et al. (2007) and Black et al. (2009) showing that higher verbal ability is related to fewer communication difficulties. These studies converge to indicate that verbal abilities influence communication disabilities (and/or vice versa) even in high-functioning children with ASD with predominantly intact language.
We also found that the VCI, particularly the Vocabulary and Comprehension subtests, was negatively correlated with social disabilities, as measured by the ADOS Reciprocal Social Interaction score. This finding is consistent with not only the Klin et al. (2007) study, but also a study by Joseph et al. (2002) in which ADOS scores correlated with verbal abilities from the Differential Ability Scales among children with ASD. The correlation between the Comprehension subtest score and the ADOS Reciprocal Social Interaction domain score may reflect, at least in part, their shared reliance on a general understanding of social behavior. The ADOS Reciprocal Social Interaction domain assesses, for example, the ability of a participant to comment on others’ emotions and the participant’s reciprocal social communication during a semi-structured interview, while the Comprehension subtest requires examinees to elaborate on socially-related actions in particular situations, as well as understanding of emotions and knowledge of community and societal norms/rules.
External validity of the present study is limited by the inclusion of only relatively high-functioning children with ASD; these findings may not hold among lower functioning children. Future investigations of the WISC-IV profile in ASD should include children with intellectual impairments to assess their impact upon the profile described here. Furthermore, we have captured cognitive profiles at a single point in time, which could conceivably vary across development due to maturational, intervention, and other effects. Future work should examine these cognitive profiles over time to aid in determining the ontogeny of cognitive peaks and troughs; identify treatment and maturational effects on these profiles; and examine their associations with outcome-related measures, like ASD symptomatology and adaptive functioning. Additionally, increasing the sample size substantially would allow for more sophisticated modeling of the relationships between these cognitive profiles and everyday functioning (i.e., symptomatology and adaptive functioning). It would also create the opportunity to investigate the well-known variability in ASD cognitive performance at the individual as opposed to group level. The inclusion of control groups made up of typically developing children and other clinical groups would be helpful in pinpointing the specificity of the findings documented here.
Conclusions
The current study examined the WISC-IV IQ profile among school-aged children with ASD and how it related to adaptive functioning and both ASD and ADHD symptomatology. We replicate and extend prior work documenting the distinctive IQ profile in ASD. Particularly novel are our findings of processing speed difficulties in ASD that are associated with both communication skills and difficulties, but not with ADHD symptoms. Cognitive profiles in ASD, such as those documented here, could serve as informative endophenotypes, which are key for future genetic investigations. Our findings also have clinical implications. For example, given the impact of processing speed (from the PSI) on FSIQ using the WISC-IV, the General Ability Index might be a better measure of general intellectual functioning than FSIQ among children with ASD. Furthermore, the significant relationship between the Processing Speed Index and communication symptoms and abilities in our sample highlights the importance of assessing and accommodating processing speed/motor output deficits in children with ASD.
References
Allen, M. H., Lincoln, A. J., & Kaufman, A. S. (1991). Sequential and simultaneous processing abilities of high-functioning autistic and language-impaired children. Journal of Autism and Developmental Disorders, 21, 483–502.
Asarnow, R. F., Tanguay, P. E., Bott, L., & Freeman, B. J. (1987). Patterns of intellectual functioning in non-retarded autistic and schizophrenic children. Journal Child Psychology and Psychiatry, 28, 273–280.
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society, Series B (Methodological), 57, 289–300.
Billstedt, E., Gillberg, I. C., & Gillberg, C. (2007). Autism in adults: Symptom patterns and early childhood predictors. Use of the DISCO in a community sample followed from childhood. Journal of Child Psychology and Psychiatry, 48, 1102–1110.
Black, D. O., Wallace, G. L., Sokoloff, J. L., & Kenworthy, L. (2009). Brief report: IQ split predicts social symptoms and communication abilities in high-functioning children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 1613–1619.
Bolte, S., & Poustka, F. (2002). The relation between general cognitive level and adaptive behavior domains in individuals with autism with and without co-morbid mental retardation. Child Psychiatry and Human Development, 33, 165–172.
Calhoun, S. L., & Mayes, S. D. (2005). Processing speed in children with clinical disorders. Psychology in the Schools, 42, 333–343.
Carter, A. S., Volkmar, F. R., Sparrow, S. S., Wang, J., Lord, C., Dawson, G., et al. (1998). The Vineland adaptive behavior scales: Supplementary norms for individuals with autism. Journal of Autism and Developmental Disorders, 28, 287–302.
Chhabildas, N., Pennington, B. F., & Willcutt, E. G. (2001). A comparison of the neuropsychological profiles of the DSM-IV subtypes of ADHD. Journal of Abnormal Child Psychology, 29, 529–540.
Dawson, M., Soulieres, I., Gernsbacher, M. A., & Mottron, L. (2007). Research report: The level and nature of autistic intelligence. Psychological Science, 18, 657–662.
Dennis, M., Lockyer, L., Lazenby, A. L., Donnelly, R. E., Wilkinson, M., & Schoonheyt, W. (1999). Intelligence patterns among children with high-functioning autism, phenylketonuria, and childhood head injury. Journal of Autism and Developmental Disorders, 29, 5–17.
Donders, J., & Jenke, K. (2008). Criterion validity of the Wechsler Intelligence Scale for Children-Fourth Edition after pediatric traumatic brain injury. Journal of the International Neuropsychological Society, 14, 651–655.
DuPaul, G. J., Power, T. J., Anastopoulos, A. D., & Reid, R. (1998). ADHD rating scale- IV: Checklists, norms, and clinical interpretation. New York: The Guilford Press.
Elliott, C. D. (1990). The differential ability scales. Lutz, FL: Psychological Assessment Resources, Inc.
Fiorello, C. A., Hale, J. B., McGrath, M., Ryan, K., & Quinn, S. (2001). IQ interpretation for children with flat and variable test profiles. Learning and Individual Differences, 13, 115–125.
Freeman, B. J., Chapman, L. J., Forness, S. R., & Ritvo, E. R. (1985). Cognitive processing of high functioning autistic children: Comparing the K-ABC and the WISC-R. Journal of Psychoeducational Assessment, 4, 357–362.
Freeman, B. J., Del’Homme, M., Guthrie, D., & Zhang, F. (1999). Vineland adaptive behavior scale scores as a function of age and initial IQ in 210 autistic children. Journal of Autism and Developmental Disorders, 29, 379–384.
Goldstein, G., Allen, D. N., Minshew, N. J., Williams, D. L., Volkmar, F., Klin, A., et al. (2008). The structure of intelligence in children and adults with high functioning autism. Neuropsychology, 22, 301–312.
Goldstein, S., & Schwebach, A. J. (2004). The comorbidity of pervasive developmental disorder and attention deficit hyperactivity disorder: Results of a retrospective chard review. Journal of Autism and Developmental Disorders, 34, 329–339.
Happé, F. G. (1994). Wechsler IQ profile and theory of mind in autism: A research note. Journal of Child Psychology and Psychiatry, 35, 1461–1471.
Hollingshead, A. B. (1975). Four factor index of social status. New Haven: Yale University.
Joseph, R. M., Tager-Flusberg, H., & Lord, C. (2002). Cognitive profiles and social communicative functioning in children with autism spectrum disorder. Journal of Child Psychology and Psychiatry, 46, 807–821.
Kenworthy, L. E., Black, D. O., Wallace, G. L., Ahluvalia, T., Wagner, A. E., & Sirian, L. M. (2005). Disorganization: The forgotten executive dysfunction in high-functioning autism (HFA) spectrum disorders. Developmental Neuropsychology, 28, 809–827.
Kenworthy, L., Case, L., Harms, M. B., Martin, A., & Wallace, G. L. (2010). Adaptive behavior ratings correlate with symptomatology and IQ among individual with high-functioning autism spectrum disorders. Journal of Autism and Developmental Disorders, 40, 416–423.
Klin, A., Saulnier, C. A., Sparrow, S. S., Cicchetti, D. V., Volkmar, F. R., & Lord, C. (2007). Social and communication abilities and disabilities in higher functioning individuals with autism spectrum disorders: The Vineland and the ADOS. Journal of Autism and Developmental Disorders, 37, 748–759.
Koegel, L. K., Koegel, R. L., & Smith, A. (1997). Variables related to differences in standardized test outcomes for children with autism. Journal of Autism and Developmental Disorders, 27, 233–244.
Koyama, T., Tachimori, H., Osada, H., & Kurita, H. (2006). Cognitive and symptom profiles in high functioning pervasive developmental disorder not otherwise specified and attention deficit hyperactivity disorder. Journal of Autism and Developmental Disorders, 36, 373–380.
Koyama, T., Tachimori, H., Osada, H., Takeda, T., & Kurita, H. (2007). Cognitive and symptom profiles in Asperger’s syndrome and high functioning autism. Psychiatry and Clinical Neurosciences, 61, 99–104.
Lainhart, J. E., Bigler, E. D., Bocian, M., Coon, H., Dinh, E., Dawson, G., et al. (2006). Head circumference and height in autism: A study by the collaborative program of excellence in autism. American Journal of Medical Genetics, 140, 2257–2274.
Le Couteur, A., Rutter, M., Lord, C., Rios, P., Robertson, S., Holdgrafer, M., et al. (1989). Autism diagnostic interview: A standardized investigator-based instrument. Journal of Autism and Developmental Disorders, 19, 363–387.
Leyfer, O. T., Folstein, S. E., Bacalman, S., Davis, N. O., Dinh, E., Morgan, J., et al. (2006). Comorbid psychiatric disorders in children with autism: Interview development and rates of disorders. Journal of Autism and Developmental Disorders, 36, 849–861.
Lincoln, A. J., Courchesne, E., Kilman, B. A., Elmasian, R., & Allen, M. (1988). A study of intellectual abilities in high-functioning people with autism. Journal of Autism and Developmental Disorders, 18, 505–524.
Liss, M., Harel, B., Fein, D., Allen, D., Dunn, M., Feinstein, C., et al. (2001). Predictors and correlates of adaptive functioning in children with developmental disorders. Journal of Autism and Developmental Disorders, 31, 219–230.
Lord, C., Rutter, M., DiLavore, P. C., & Risi, S. (1999). Autism Diagnostic Observation Schedule–WPS (ADOS-WPS). Los Angeles, CA: Western Psychological Services.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism diagnostic interview-revised: A revised version of a diagnostic interview for caregivers and individuals with possible developmental disorders. Journal of Autism and Developmental Disorders, 24, 659–685.
Mayes, S. D., & Calhoun, S. L. (2003). Analysis of WISC-III, Stanford-Binet: IV, and academic achievement test scores in children with autism. Journal of Autism and Developmental Disorders, 33, 329–341.
Mayes, S. D., & Calhoun, S. L. (2004). Similarities and differences in Wechsler Intelligence Scale for Children-Third Edition (WISC-III) profiles: Support for subtest analysis in clinical referrals. Clinical Neuropsychologist, 18, 559–572.
Mayes, S. D., & Calhoun, S. L. (2006). WISC-III and WISC-IV profiles in children with ADHD. Journal of Attention Disorders, 9, 486–493.
Mayes, S. D., & Calhoun, S. L. (2008). WISC-IV and WIAT-II profiles in children with high-functioning autism. Journal of Autism and Developmental Disorders, 38, 428–439.
McAuley, T., Chen, S., Goos, L., Schachar, R., & Crosbie, J. (2010). Is the behavior rating inventory of executive function more strongly associated with measures of impairment or executive function? Journal of the International Neuropsychological Society, 16, 495–505.
Nyden, A., Billstedt, E., Hjelmquist, E., & Gillberg, C. (2001). Neurocognitive stability in Asperger syndrome, ADHD, and reading and writing disorder: A pilot study. Developmental Medicine and Child Neurology, 43, 65–171.
Pfeiffer, S., Reddy, L., Kletzel, J., Schmelzler, E., & Boyer, L. (2000). The practitioner’s view of IQ testing and profile analysis. School Psychology Quarterly, 15, 376–385.
Power, T. J., Doherty, B. J., Panichelli-Mindel, S. M., Karustis, J. L., Eiraldi, R. B., Anastopoulos, A. D., et al. (1998). The predictive validity of parent and teacher reports of ADHD symptoms. Journal of Psychopathology and Behavioral Assessment, 20, 57–81.
Scheuffgen, K., Happé, F., Anderson, M., & Frith, U. (2000). High ‘‘intelligence’’, low ‘‘IQ’’? Speed of processing and measured IQ in children with autism. Development and Psychopathology, 12, 83–90.
Siegel, D. J., Minshew, N. J., & Goldstein, G. (1996). Wechsler IQ profiles in diagnosis of high-functioning autism. Journal of Autism and Developmental Disorders, 26, 389–406.
Sinzig, J., Morsch, D., Bruning, N., Schmidt, M. H., & Lehmkuhl, G. (2008). Inhibition, flexibility, working memory and planning in autism spectrum disorders with and without comorbid ADHD-symptoms. Child and Adolescent Psychiatry and Mental Health, 2, 4.
Sparrow, S. S., Cicchetti, D. V., & Balla, D. A. (2005). Vineland adaptive behavior scales: Second edition (Vineland II), survey interview form/caregiver rating form. Livonia, MN: Pearson Assessments.
Tallal, P. (2004). Opinion–improving language and literacy is a matter of time. Nature Reviews Neuroscience, 5, 721–728.
Tillman, C., Eninger, L., Forssman, L., & Bohlin, G. (2011). The relation between working memory components and ADHD symptoms from a developmental perspective. Developmental Neuropsychology, 36, 181–198.
Venter, A., Lord, C., & Schopler, E. (1992). A follow-up-study of high-functioning autistic children. Journal of Child Psychology and Psychiatry, 33, 489–507.
Volkmar, F. R., Sparrow, S. S., Goudreau, D., Cicchetti, D. V., Paul, R., & Cohen, D. J. (1987). Social deficits in autism: An operational approach using the Vineland-adaptive behavior scales. Journal of the American Academy of Child and Adolescent Psychiatry, 26, 156–161.
Wallace, G. L., Anderson, M., & Happé, F. (2009a). Brief report: Information processing speed is intact in autism but not correlated with measured intelligence. Journal of Autism and Developmental Disorders, 39, 809–814.
Wallace, G. L., Happé, F., & Giedd, J. N. (2009b). A case study of a multiply-talented savant with an autism spectrum disorder: Neuropsychological functioning and brain morphometry. Philosophical Transactions of the Royal Society: Section B: Biological Sciences, 364, 1425–1432.
Wechsler, D. (2003). Wechsler intelligence scale for children-fourth edition (WISC-IV). San Antonio, TX: Psychological Corporation.
Yerys, B. E., Wallace, G. L., Sokoloff, J. L., Shook, D. A., James, J. D., & Kenworthy, L. (2009). Attention deficit/hyperactivity disorder symptoms moderate cognition and behavior in children with autism spectrum disorders. Autism Research, 2, 322–333.
Yoshida, Y., & Uchiyama, T. (2004). The clinical necessity for assessing attention deficit/hyperactivity disorder (AD/HD) symptoms in children with high functioning pervasive developmental disorder (PDD). European Child and Adolescent Psychiatry, 13, 307–314.
Acknowledgments
This research was supported by the Intramural Research Program of the NIH, National Institute of Mental Health. We would like to thank the children and families who so kindly gave their time and energy to assist in this research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Oliveras-Rentas, R.E., Kenworthy, L., Roberson, R.B. et al. WISC-IV Profile in High-Functioning Autism Spectrum Disorders: Impaired Processing Speed is Associated with Increased Autism Communication Symptoms and Decreased Adaptive Communication Abilities. J Autism Dev Disord 42, 655–664 (2012). https://doi.org/10.1007/s10803-011-1289-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-011-1289-7