
Abstract
Non-suicidal self-injury (NSSI) is a self-destructive behavior of common prevalence in adolescence and young adulthood. Engagement in NSSI has been consistently linked in the literature with perceptions of one’s parent–child relationships as negative or invalidating. However, the potential for multiple combinations of such relational characteristics to be associated with varying cognitive and behavioral manifestations of NSSI remains uninvestigated. In the current study, a person-centered approach to studying perceived parent–child relationship quality and NSSI was adopted; functions and behavioral severity of NSSI were then compared across the different relational profiles created. A latent profile analysis in a sample of 264 self-injuring university students (205 females; mage = 19.37 years, sd = 1.50) revealed four distinct profiles, two characterized by negative parent–child perceptions and two by positive parent–child perceptions. The perceived relational dimensions of these profiles were unique compared to a parallel group of 264 non-self-injurers (207 females; mage = 19.27 years, sd = 1.33). Participants reporting negative parent–child relationships endorsed more severe NSSI, and engaged in NSSI to regulate aggressive emotions. In contrast, individuals reporting positive parent–child relationships engaged in less extreme manifestations of NSSI overall, suggesting lower psychological deficits. Findings suggest that, although not all self-injurers perceive their relationships with parents negatively, variation in the perception of relational quality is implicated in behavioral and cognitive variation in NSSI engagement.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Non-suicidal self-injury (NSSI) involves deliberate, self-inflicted destruction of body tissue (Nixon and Heath 2009); these acts are performed without suicidal intent, and using methods that are not socially sanctioned, commonly including self-cutting or burning of skin. Originally believed to be a symptom underlying psychiatric diagnoses of borderline personality disorder (BPD) or depression, researchers and clinicians now concede that NSSI is more prevalent than previously conceived of within non-psychiatric, community-based populations. Recent research shows that between 13 and 17% of nonclinical samples of adolescents and young adults report NSSI behavior (Swannell et al. 2014). According to Marsha Linehan’s biosocial theory (1993) of the development of self-harm in BPD patients – which has also been applied to NSSI external to BPD diagnosis -- experiencing an invalidating family environment during childhood limits an individual’s capacity to appropriately regulate distressing emotion, thus increasing the likelihood of engaging in NSSI. Indeed, researchers have well established that negative or invalidating parent–child relationships are linked with NSSI (e.g., Adrian, Zeman, Erdley, Lisa, and Sim 2011; Bureau et al. 2010a; Claes, Vandereycken, and Vertommen 2004; Crowell et al. 2008).
To date researchers in this field have primarily applied variable-centered approaches to studying relational correlates of NSSI. As such researchers have typically identified individual relational characteristics associated with NSSI engagement or frequency. In contrast, the use of a person-centered approach places the individual as the unit of interest, and establishes organizational patterns of responses on key variables to create profiles of individuals similar to one another on the variables of interest, but different from people assigned to the other identified profiles (Bergman and Trost 2006). This approach is often recommended for use in developmental psychopathology research (see von Eye and Bergman 2003) to account for diversity within groups of similarly diagnosed individuals, and to compare these groups based on the degree of risk demonstrated within their particular clinical behavior.
The existing literature’s emphasis on variable-centered approaches, particularly with regard to research concerning interpersonal correlates of NSSI, does not adequately account for diversity of relational qualities that may be reported within groups of self-injurers. Overlooking this possible diversity further limits our knowledge regarding NSSI. Though evidence suggests that varying risk factors have distinct influences on features of NSSI (Barrocas, Giletta, Hankin, Prinstein, and Abela 2014; Hamza and Willoughby 2014; Klonsky and Olino 2008; Lundh, Wångby-Lundh, and Ulander 2009; Whitlock, Muehlenkamp, and Eckenrode 2008), the potential for differential impacts of parent–child relationships on cognitive (e.g., functions of NSSI) and behavioral manifestations of NSSI (e.g., age of onset, frequency, number of methods) remain uninvestigated. The current study aimed to alleviate these limitations through its use of a person-centered approach to establish profiles of self-injurers based on parent–child relationship quality, and comparing these profiles across characteristics of NSSI.
Existing Evidence from Person-centered Approaches
Only one research group has previously conducted a person-centered approach to the study of interpersonal characteristics and NSSI. Lundh et al. (2009) identified profiles of female middle school students based on self-reported quality of emotional tone in both parent and peer relationships. Five profiles were apparent, two of which were characterized by poor emotional tone with parents but differed from one another in regards to reported quality of peer relationships. Individuals who reported poor parent–child emotional tone reported greater frequency of NSSI, regardless of the quality of peer relationships.
Although Lundh et al. (2009) provided a first step in adopting a person-centered approach to studying NSSI and interpersonal relationships, their study is limited by the inclusion of both self-injurers and non-self-injurers, as the findings may overlook additional diversity in the reported quality of parent–child relational characteristics evident for self-injurers alone. Further, the use of a single assessment of relationship quality (emotional tone) limits the detail that can be obtained regarding how different aspects of parent–child relationships may form varying typologies of self-injuring youth. Relationships are multifaceted, and can be characterized by many different features, and thus multiple indicators of relationship quality should be considered.
Common Indicators of Parent–child Relationship Quality
Linehan’s suggests in her biosocial theory (1993) regarding the development of NSSI that relationships with parents in which the individual’s emotions are negated or ignored contribute to deficits in emotion regulating capacities, which correspond with increases in the chance of engaging in NSSI. Such environments may feature parent–child relationships in which there is a lack of care and excessive control (e.g., Bureau et al. 2010a; Gratz 2006), limited trust and communication (Hilt, Nock, Lloyd-Richardson, and Prinstein 2008), and where the child ultimately feels alienated from the parent (Bureau et al. 2010a; Yates, Tracy, and Luthar 2008). These relational features represent a general lack of intimacy or care within the parent–child relationship, rather than more extreme relational trauma. Relational trauma results from highly insensitive or inadequate caregiving and, in extreme cases, from child maltreatment (e.g., Bureau et al. 2010b). Perceptions of relational trauma from one’s family environment are likely elevated in self-injurers given the theoretical and empirical associations between NSSI and maltreatment (see Yates 2009).
Indeed Bureau et al. (2010a) found that university students engaging in recent NSSI reported greater relational trauma than non-self-injuring participants. Likewise, West, Rose, Spreng, and Adam (2000) found that adolescents demonstrating suicidal behavior (commonly comorbid with NSSI) reported more relational trauma than a non-suicidal comparison group. Although limited in number, these findings indicate that relational dimensions associated with maladaptive or disturbed parent–child relationships are associated with NSSI in young adults as suggested by earlier theoretical models (Linehan 1993). Given that relationships are multifaceted, it is likely that these common indicators of relational quality combine in heterogeneous patterns to form different parent–child relational profiles of self-injuring young adults.
Variation in NSSI Manifestation
One can further anticipate individuals with differing perceptions of parent–child relationship quality to also vary in the manifestation of their NSSI behavior. For example, self-injurers who report having overly controlling parents versus those with more relationally traumatic backgrounds may differ in their reasons for engaging in NSSI or in the severity of their behavior. Our investigation provided an opportunity to empirically move beyond a general understanding that negative or invalidating family environments are associated with NSSI, and permitted further analysis of the influences of specific relational characteristics on the manifestation of NSSI in young adults.
Variation in the Functions of NSSI
Klonsky (2007) compiled a comprehensive review of the reported motivations for engaging in NSSI, and extracted seven super-ordinate functions from the past literature. Emotion regulating functions are the most empirically supported functions of NSSI, through which individuals use NSSI to relieve extreme negative or aversive emotions. Klonsky also indicated anti-dissociation, anti-suicide, social influence, self-punishment, and sensation seeking functions at lesser frequencies throughout the literature. In the only study to directly assess the influence of parent–child relationship characteristics on NSSI functions (Kaess et al. 2013), researchers showed that adverse relational experiences (i.e., maternal antipathy and neglect) corresponded with increases in NSSI’s use to regulate emotional distress, but with either slight decreases or no change in reports of engaging in NSSI for social or interpersonal reasons.
Variation in the Severity of NSSI
NSSI severity is commonly indicated by behavioral characteristics such as number of methods used, age of onset, and frequency of NSSI (see Lundh et al. 2009; Whitlock et al. 2008). Researchers have shown that self-injurers engaging in more severe NSSI also report experiencing physical, sexual, and emotional abuses more often than those engaging in NSSI of lesser severity (Whitlock et al. 2008). Non-abusive characteristics of family environments also predict increased severity and frequency of NSSI in some investigations (Di Pierro, Sarno, Perego, Gallucci, and Madeddu 2012; Lundh et al. 2009), but not in others (Kaess et al. 2013), suggesting a need for further research in this regard.
Objectives & Hypotheses
The current study was guided by two main objectives. The first objective was to establish profiles of self-injurers based on individuals’ perceptions of characteristics underlying their relationships with parents. This objective was comprised of two hypotheses. First, we expected that multiple profiles would be obtained, with all profiles differing on some combination of parent–child relational dimensions, based on the argument that it is unlikely for all individuals to report the same types of experiences and relationships with parents. Second, we hypothesized that some profiles would report relationships with parents that were characterized by especially damaging or negative features (e.g., alienating, relationally traumatic), while other profiles would describe features deemed to be less damaging or traumatic in nature (e.g., overprotective, controlling). In particular, we expected to find variation in the degree to which relational dimensions were reported by the obtained profiles of self-injurers when compared to the average levels of these dimensions reported by a non-self-injuring control group.
The second objective aimed to determine how self-injurers reporting different relational characteristics varied in cognitive (i.e., functions) and behavioral (i.e., severity) manifestations of NSSI. Based on the literature reviewed above, we predicted that individuals belonging to profiles characterized by particularly poor or damaging parent–child relationships would endorse NSSI functions to a greater degree. It was further expected that emotion-regulating functions, reflecting a greater psychological deficit than the other functions assessed, and with particular relevance to the parent–child relationship as described above, would be especially over-reported by individuals in these negatively characterized profiles. Finally, we also expected that profiles reporting especially traumatizing parent–child relationships would report earlier age of NSSI onset, more frequent engagement, and more NSSI methods than participants reporting less problematic parent–child relationships.
Method
Participants
Individuals were selected from a sample of 3990 undergraduate students between 17 and 25 (3076 females; Mage = 19.39 years, SD = 1.50) who had participated in an ongoing study. Two subsamples were drawn from the larger group: 264 participants (205 females; mage = 19.37 years, sd = 1.53) were selected based on endorsing at least one NSSI behavior in the prior 6 months, and comprised the NSSI subsample. These findings reflect a 6.6% prevalence rate of NSSI within the overall sample. An additional 264 participants who had never engaged in NSSI (207 females; mage = 19.27 years, sd = 1.33) were randomly selected from the larger group to serve as a comparison group for parent–child relationship quality.
The majority of the NSSI group was Caucasian (76.3%), with some representation of Black (6.5%), Asian (5.7%) and Middle Eastern (4.2%) backgrounds. A majority of the sample (57.8%) lived in accommodations other than with their parents. The comparison group did not differ significantly from the NSSI group on key demographics, nor did either the comparison or NSSI group differ from the remaining participants who were unselected from the overall sample.
NSSI Subsample Characteristics
On average, participants in the NSSI group reported initiating NSSI at 14.97 years of age (sd = 2.61). Most individuals had engaged in NSSI one to five times in the past 6 months (76.1%), though some did endorse monthly (12.1%), weekly (8.3%), and daily (3.4%) NSSI. Participants most commonly reported engaging in cutting (55.5%), burning (31.3%), and hitting (34.5%) as methods of self-injury.
Procedure
Participants were registered in introductory psychology courses at a Canadian university and selected the current study from a list of available investigations in which they could participate for course credit. Questionnaires were hosted through an online survey tool, and were completed via a secure web address. An information sheet informed participants that consent was implied through completion of the questionnaires. All participants were assigned an anonymous five digit identification code by the computerized system, which was used to label their data, and no other identifying information was collected. Participants were treated in accordance with the ethical guidelines of the institution and the American Psychological Association, and study procedures were approved by the institution’s ethics board.
Measures
Non-Suicidal Self-Injury
The Ottawa Self-Injury Inventory (OSI; Martin et al. 2013) assessed the occurrence of NSSI behavior as well as cognitive and behavioral characteristics of NSSI. Occurrence of NSSI was determined by answers to: how often in the past 6 months have you actually injured yourself without the intention to kill yourself? Responses were rated on a 5- point scale (not at all, 1 to 5 times, monthly, weekly, daily). Categories were collapsed to create a three category variable, with not at all ratings reflecting a no NSSI category, 1 to 5 times remaining as is, and monthly, weekly, and daily responses combined to form a more than 5 times category to represent frequency of NSSI.
Functions of NSSI were determined by the degree to which participants rated each of twenty-four listed reasons for engaging in NSSI. Each reason was rated on a 5-point scale ranging from never a reason (0) to always a reason (4). The four subscales established by Martin et al. (2013) were calculated to reflect the following functions: internal emotion regulation (ER; 8 items reflecting the need to regulate an internal emotion or feeling, e.g., to relieve feelings of sadness or feeling down; to stop me from thinking about/acting on thoughts to kill myself), social influence (nine items reflecting the need to regulate/manage one’s social environment, e.g., to avoid getting in trouble for something I did), external ER (three items reflecting the need to express a challenging emotion, e.g., to release unbearable tension), and sensation seeking (four items, e.g., to experience a high like a drug high). Internal consistencies for the subscales ranged between poor and excellent in the current research, internal ER, α = 0.86; social influence, α = 0.74; external ER: α = 0.81; sensation seeking: α = 0.64. Given the poor internal consistency of the sensation seeking function, it was eliminated from analyses.
Three OSI items assessed the severity of NSSI. First, participants were presented a checklist of seventeen methods and were asked to select all that apply to their behavior to assess the number of NSSI methods used. The list of methods (cutting, scratching, interfering with wound healing, burning, biting, hitting, piercing skin with sharp pointy objects, trying to break bones, head-banging) was summed to represent the total number of methods used. Age of onset of NSSI was indicated via numerical response to the question: how old were you when you started to self-injure? Finally, frequency of recent NSSI was measured as described above.
Parent–Child Relational Dimensions
Seven indicators of parent–child relationship quality were measured, namely, maternal lack of care, maternal control, paternal lack of care, paternal control, trust in parent–child relationships, feeling alienated from parents, and relational trauma.
The Parental Bonding Index (PBI; Parker, Tupling, and Brown 1979) assessed the degree to which participants perceived their mother and their father as caring or controlling. The PBI was presented as two 25-item 4-point Likert-type scales (responses from 1 to 4) asking about mother and father separately, with higher scores reflecting poor parental bonding. Internal consistencies of the four scales were strong in the current sample, with Cronbach’s α ranging between 0.85 and 0.93.
The parent items of the Inventory of Parent and Peer Attachment (IPPA; Armsden and Greenberg 1987) were used to measure the degree to which participants perceived relationships with their parents as characterized by trust, good communication, and alienation. The IPPA-parent is a 28-item self-report measure rated on a 5-point scale (responses from 1 to 5), with higher scores indicating higher levels of each subscale. Cronbach’s alpha coefficients were strong for both trust, α = 0.84, and alienation subscales, α = 0.87,, but poor for the communication dimension, α = 0.60, which was ultimately removed from the current analyses.
The Adolescent Unresolved Attachment Questionnaire (AUAQ; West et al. 2000) is a 10-item self-report scale rated on a 5-point scale (responses from 1 to 5) measuring one’s current perceptions regarding the degree to which early relationships were characterized by relational trauma resulting from continued feelings of failed protection, anger towards parents, and fear of abandonment. Higher scores indicated greater relational trauma. A total score representing relational trauma was used, and internal consistency was strong, α = 0.89.
Demographic Variables
All participants also completed a standard sociodemographic questionnaire. Items assessing sex, age, and current living arrangements (e.g., do you currently live with your parents?) were explored as potential covariates.
Data Analyses
All data used in this study were first screened for assumptions underlying parametric statistics. The first objective was analyzed in three steps. First, a latent profile analysis (LPA) in LatentGOLD version 4.5 (Vermunt and Magidson 2005) was used to identify profiles of self-injurers based on their self-reported perceptions of parent–child relational quality. LPA applies EM algorithms of parameter estimation to identify profiles comprised of participants who resemble one another, but who can be differentiated from individuals in other profiles, on the basis of a given set of indicators, Second, a MANOVA comparing the relational dimensions between profiles was conducted to describe and label the obtained profiles. Third, a series of one-sample t-tests comparing the mean of each relational dimension within each obtained profile to the mean of each relational dimension calculated for a non-self-injuring control group tested the hypothesis that individuals in the self-injury profiles reported relational dimensions which distinguished them from non-self-injurers.
The second objective was also tested in three analyses. Two separate MAN (C) OVAs compared the reported functions and severity of NSSI (age of onset, number of methods) across profiles. MAN (C) OVAs were followed up with planned contrasts such that the most negative profile obtained was compared with each other obtained profile. Given that the contrasts for this analysis were planned, they were performed in lieu of multivariate and univariate omnibus significance tests (see Tabachnick and Fidell 2007). However, post-hoc Tukey’s lowest significant difference (LSD) tests comparing all other possible pairwise difference were only conducted when univariate effects were significant. Lastly, a Pearson chi-square analysis tested the prediction that frequency of NSSI (indicator of severity) would vary across the profiles. All analyses other than the LPA were conducted in SPSS version 20 (IBM Corporation, 2011).
Results
Preliminary Analyses
Missing Data Analysis & Exploration of Assumptions
Individual items assessing NSSI characteristics (excluding frequency) were missing between 13.6 and 54.3% of data. A missing value analysis showed that data were missing at random across profiles, Little’s MCAR tests: Profile 1: χ 2 (58) = 71.66, p = 0.11; Profile 2: χ 2 (38) = 44.68, p = 0.21; Profile 3: χ 2 (11) = 19.68, p = 0.06; Profile 4: χ 2 (4) = 2.46, p = 0.65. While such a high proportion of missing data at first seems in excess it is not necessarily unexpected as research has shown that many self-injuring individuals are willing to admit to having engaged in the behavior, but are often less likely to divulge additional information regarding the details of their experiences with NSSI (see Klineberg, Kelly, Stansfeld, and Bhui 2013). Thus, only those individuals who reported full information for functions of NSSI and NSSI severity (n = 139) were used for analyses using these variables.
Variables were further screened to ensure suitability for multivariate statistics. Univariate outliers were replaced by scores within three standard deviations from the mean (see Tabachnick and Fidell 2007) for the following: mother care (one outlier), mother control (one), father control (one), trust (one), relational trauma (two), social influence function (one), external ER function (one). The social influence function and number of NSSI methods each demonstrated positively skewed distributions; a square root transformation normalized social influence function, a logarithmic transformation normalized number of methods. Two multivariate outliers were removed from analyses (one among reasons for engaging in NSSI, one among indicators of NSSI severity).
Potential Covariates for Multivariate Analyses
Age, sex, and current living arrangements were analyzed as potential covariates. Age was significantly correlated with number of NSSI methods used, r = 0.17, p < 0.01. Current living arrangements was associated with social influence functions, t (137) = −2.06, p < 0.05, such that individuals currently living with their parents reported more social influence functions for NSSI, m = 0.70, than those who did not currently live with parents, m = 0.53. No other significant associations were found. Age was included as a covariate in analyses regarding NSSI methods, as was current living arrangement in analyses of NSSI functions.
Identification of Parent–Child Relationship Profiles
The first hypothesis was that multiple patterns of parent–child relational dimensions would be identified within the sample of self-injurers. Multiple fit indices provided by the LPA were used to determine the best fitting classification model, including the Akaike Information Criterion (AIC), the Consistent Akaike Information Criterion (CAIC), the Bayesian Information Criterion (BIC), entropy, and Wald statistics. A four profile solution was ultimately selected (see Table 1), as BIC, AIC and CAIC values reached a low point at the four profile solution before increasing at the five profile model, suggesting improved model fit in the four profile solution (Vermunt and Magidson 2005). Entropy and Wald statistics were also maximized compared to models with fewer or more profiles, further supporting the four profile solution (Ramaswamy et al. 1993).
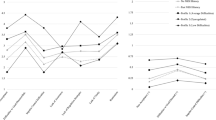
Profile Descriptions
Two profiles (profiles 2 and 3) were characterized by positive perceptions of parent–child relationships overall, while the remaining two (profiles 1 and 4) featured overall reports of negative relational patterns (see Table 2). The first profile (n = 112) was labeled the Negative-invalidating group. Compared to other profiles (excluding profile 4) these individuals reported more negative relational features. The second profile, deemed the Positive-moderate group (n = 95) rated relationships with parents positively, though not excessively so. In contrast, the third profile (n = 35) was characterized by Positive-idealistic perceptions of parent–child relationships; across all indicators, individuals within this profile reported highly positive relational quality. The fourth profile was entitled Negative-disturbed (n = 22); participants within this final profile reported significantly less trust and care from mothers, and significantly more relational trauma and alienation than all other groups.
Comparing Relational Quality Between Non-Self-Injurers and Self-Injurer Profiles
We further hypothesized that the obtained profiles of self-injurers would meaningfully differ from non-self-injurers in their reports of parent–child relational characteristics. Indeed, participants in both Negative-invalidating and Negative-disturbed profiles rated relationships with parents less positively (lower perceptions of mother care, father care and trust) and more negatively (higher perceptions of mother control, relational trauma and alienation) than the comparison group; members of the Negative-invalidating profile also had higher perceptions of father control than the comparison group (see Table 3).
Results also emphasized the excessively idealistic relational perceptions reported by self-injuring participants in the Positive-idealistic profile, such that participants in this profile reported higher scores for all positive indicators and lower scores for all negative indicators (marginal differences for relational trauma) even when compared to the non-self-injuring group. The Positive-moderate group most closely resembled the perceptions of relationship quality reported by non-self-injurers, but nonetheless self-injurers within this profile perceived relationships with parents as characterized by more alienation, and marginally less care from fathers than their non-self-injuring counterparts.
Profile Differences in ER Functions
We predicted that profiles characterized by more disrupted, traumatic parent–child relational dimensions would endorse functions of NSSI to a higher degree, particularly for ER functions (see Table 4 for multivariate, univariate and post-hoc details). Planned contrasts demonstrated that the Negative-disturbed profile reported more internal ER functions than the Positive-idealistic profile, t (32) = −2.73, p < 0.01, marginally more than the Positive-moderate, t (66) = −1.86, p = 0.06, but no different from the Negative-invalidating profiles, t (70) = −1.14, p = 0.24. In contrast, the Negative-disturbed profile showed greater endorsement of external ER functions compared to each of the Positive-moderate, t (66) = −2.68, p < 0.01), Positive-idealistic, t (32) = −3.41, p < 0.01, and Negative-invalidating, t (70) = −1.97, p < 0.05 groups. Social influence functions did not differ between the Negative-disturbed and remaining profiles, t’s between −1.31 and 0.13, p’s between 0.19 and 0.90. Additional pairwise comparisons (Tukey’s LSD tests) were conducted only for external ER due to lack of univariate significance for the other functions (see Table 4). Post-hoc results showed that participants in the Negative-invalidating profile also endorsed external ER functions to a greater degree than those in the Positive-idealistic profile. No other pairwise differences were found.
Profile Differences NSSI Severity
It was hypothesized that profiles featuring more disrupted, traumatic parent–child relationships would report more severe NSSI (see Table 4). Planned comparisons showed that the Negative-disturbed group reported using significantly more NSSI methods than the Positive-idealistic group, t (28) = −2.75, p < 0.05, marginally more than the Positive-moderate profile, t (56) = −1.18, p = 0.08, but resembled the Negative-invalidating group, t (69) = −1.50, p = 0.12. Moreover, age of onset was earlier in the Negative-disturbed group than in the Positive-moderate profile, t (56) = 2.31, p < 0.05, marginally earlier than the Positive-idealistic profile, t (28) = 1.75, p = 0.08, but no different than the Negative-invalidating, t (69) = 1.34, p = 0.18 profiles. No post-hoc tests were performed due to lack of univariate significance.
The frequency of recent NSSI also varied across profiles, χ 2 (3, n = 264) = 11.99, p < 0.01 (see Table 5). Individuals in the Positive-moderate profile were less likely than expected to engage in NSSI more than five times in the past 6 months, while participants in the Negative-disturbed profile were more likely to have engaged in NSSI more than five times during the same timeframe.
Discussion
In line with the primary hypothesis, the present findings from a person-centered approach demonstrate that self-injurers are heterogeneous in their perceptions of the quality of parent–child relationships. Of note, not all of these perceptions are inherently negative, as prior research would lead one to believe, and the perceptions reported by individuals in each profile differed meaningfully from comparisons with a non-self-injuring control group.
The largest profile (Negative-invalidating) most closely resembles what Linehan (1993) described as invalidating family environments (e.g., limited parental care and trust, reports of relational trauma and moderate alienation), and was perhaps the most anticipated based on past theoretical and empirical work (e.g., Adrian et al. 2011; Bureau et al. 2010a; Gratz 2006). The Negative-disturbed profile presented highly adverse family environments, confirming that NSSI may develop as a consequence of extremely damaging interpersonal experiences as suggested by theoretical models (see Yates 2009). Moreover, individuals in both negatively valenced profiles reported significantly poorer relational features compared to non-self-injuring participants, further supporting the well-established notion that many self-injurers perceive their relationships with parents as characterized by negative relational characteristics.
Interestingly, the remaining two profiles were comprised of individuals reporting positive relational features. The Positive-moderate profile featured reports of positive relational dimensions which were not exceptionally high; in fact alienation was the only relational indication that was greater in this profile (and marginally lower father care) than in non-self-injurers. This suggests that NSSI engagement for these individuals may be associated with specific aspects of invalidating family environments (i.e., feelings of alienation), or with experiences external to family background, such as poor peer interactions (Hasking, Andrews, and Martin 2013), extra-familial sexual or physical violence (Levesque, Lafontaine, Bureau, Cloutier, and Dandurand 2010), psychological symptoms (Hasking, Momeni, Swannell, and Chia 2008), or other distressing life events (Hasking et al. 2013), each of which are linked to the likelihood of engaging in NSSI. Future research should examine if individuals reporting positive parent–child relationships have also experienced one or more of these additional risk factors.
Finally, individuals in the Positive-idealistic profile boasted exceptionally positive relationships with parents compared to both other self-injurers and non-self-injurers. Although it may seem conceptually counterintuitive that individuals engaging in NSSI would perceive such highly positive childhood family relationships, findings may suggest that these individuals feel great pressure to live up to parents’ expectations, which may result in greater stress in adolescence, and higher probability of NSSI behavior (see Claes, Soenons, Vansteenkiste, and Vandereycken 2012 for a discussion of perfectionism and NSSI). It is also possible, as with the Positive-moderate profile, that NSSI engagement in the Positive-idealistic group was triggered following experiences or life events occurring external from the family context.
A potential counter explanation for the Positive-idealistic profile stems from attachment theory. A portion of adults demonstrate dismissing states of mind regarding early attachment experiences (see Main, Hesse, and Goldwyn 2008) by describing parents in a positive light, but failing to support these descriptions with specific episodic memories. Dismissing states of mind are believed to result from an unconscious disconnection from attachment related memories, a defence mechanism of deactivation discussed by Bowlby (1969), perhaps in order to repudiate having felt rejected by their parents during childhood. Following this logic, individuals in the Positive-idealistic profile may have suppressed negative feelings regarding rejecting or invalidating relationships with parents, and may have been incapable of reporting such experiences in this study given the self-report assessments of relational quality, which are subject to the conscious availability of information to the individual. Unfortunately, the current methodology did not permit verification of this hypothesis; additional research is warranted.
Profile Differences in the Manifestation of NSSI
As hypothesized, the Negative-disturbed in particular tended to present more severe cognitive and behavioral manifestations of NSSI compared to the two positive profiles. This finding is complementary to prior work showing strong associations between severe NSSI and particularly disrupted or disturbed parent–child relationships (Di Pierro et al. 2012; Hamza and Willoughby 2014), and to additional findings that positive experiences with parents may protect against engaging in severe NSSI (Williams and Hasking 2009).
Individuals in the negative family background profiles reported using NSSI for emotion regulating purposes to a high degree. Specifically, individuals in the Negative-disturbed group endorsed internal ER functions to a higher degree than the Positive-idealizing profile, and more external ER functions than all of the other profiles. Further, the Negative-invalidating profile demonstrated more external ER deficits compared to the Positive-idealistic profile. The lack of significant differences for social influence functions, suggests that ER functions of NSSI may be particularly influenced by one’s prior experiences with parents as was hypothesized. These findings are congruent with existing theory and research (Adrian et al. 2011; Kaess et al. 2013; Linehan 1993) indicating that damaging parent–child relationships are associated with deficits in emotion regulation in self-injuring youth. Given that adequate emotion regulating skills develop in part through high quality parent–child interactions (see Thompson 1994), individuals reporting disrupted or invalidating relationships with parents are more likely to demonstrate emotion regulation deficits, evidenced in this instance through their use of NSSI to regulate aversive emotion. Thus we would expect that individuals reporting positive relationships with parents would perceive no such deficit.
Interestingly, profile differences were notable for external ER functions, suggesting that the use of NSSI for external ER purposes may reflect the greatest psychological deficit compared even to internal ER. In this investigation, internal ER was assessed by items requiring the individual to identify having experienced a specific emotion or lack thereof before engaging in NSSI (e.g., to relieve feelings of sadness). The ability to correctly label emotional experiences when responding to this item can be considered indicative of rudimentary emotion regulation (see Thompson 1994). In contrast, items reflecting the external ER function reflected the use of NSSI to alleviate negative arousal in general (e.g., to release frustration (or) unbearable tension), rather than a particular labelled emotion. Higher endorsement of the external ER items may require very basic emotion regulating capacity as opposed to the precise labelling of emotional experiences required of the internal ER function scale. It is possible that the two affect regulation functions depict varying deficits in emotion regulation. Alternatively, it is also possible that the external ER items are simply broader in the scope of emotional experiences covered, and were thus more highly endorsed for this reason. Such explanation would account for the higher means of external ER compared to internal ER reported across profiles. Additional research to further substantiate either argument, and to understand possible mechanisms served by NSSI as a regulator of different types of emotions, is necessary.
We also predicted that the behavioral severity of NSSI would vary across the obtained profiles. Indeed, individuals in the Negative-disturbed profile reported earlier age of onset than the Positive-moderate profile (marginal for Positive-idealistic), used more NSSI methods than participants in the Positive-idealistic profile (marginal for Positive-moderate), and were more likely to have engaged in frequent NSSI (more than 5 times in the last 6 months), while the Positive-moderate profile was correspondingly less likely to engage in frequent NSSI. Each of these findings is in line with past research. Earlier age of onset of NSSI has previously been related to lack of parental care (Saldias, Power, Gillanders, Campbell, and Blake 2013). Researchers have also suggested that individuals with damaging family relationships may engage in more severe NSSI in general (Di Pierro et al. 2012; Hamza and Willoughby 2014), and may use NSSI more frequently in particular (Lundh et al. 2009).
Such findings suggest that increasingly traumatizing or disrupted interactions with parents are associated with greater pathology of NSSI behavior, and may place the individual at risk for prolonged, chronic engagement in potentially higher risk self-harm (see also Whitlock et al. 2008). For instance, individuals with disrupted parent–child relationships are likely to experience corresponding deficits in regulatory capacities (Adrian et al. 2011; Linehan 1993). The use of a greater number of self-harming methods and more frequent NSSI engagement in the Negative-disturbed profile in particular may reflect greater deficits in self-regulatory capacities, and a corresponding heightened need to adopt additional ways to self-injure or more frequent self-injury in order to achieve relief or release.
The two positive profiles resembled one another to a greater extent than the two negative groups, despite marked differences in perceived relational quality. Again, this is consistent with past research suggesting that positive parent–child relationships protect against severe NSSI behavior (Williams and Hasking 2009), and with the work of previous researchers who have identified subtypes of self-injurers who engage in superficial or low to moderate severity NSSI (Barrocas et al. 2014; Klonsky and Olino 2008; Whitlock et al. 2008). These individuals seem to test the waters of NSSI behavior, but present with a reduced risk for chronic abuse of the behavior, and may have different reasons for initiating the behavior than a fundamental lack of emotional self-regulatory capacity evident in self-injurers reporting negative relationships.
While this explanation is certainly plausible for the Positive-moderate profile in particular, it is perhaps more challenging to accept for the Positive-idealistic profile, as it fails to address the extreme nature of the positive relationships reported by these individuals when compared to non-self-injuring counterparts. Assuming our previous conjecture regarding dismissing defensive mechanisms of these individuals to be true, this begs the question of whether one can trust the characteristics of NSSI reported by these participants. In other words, is it possible that the defensive strategy employed to deny past relational issues may extend to a similar denial of symptomatic distress or psychological need, despite admitting to engaging in pathological behavior (see Shedler, Mayman, and Manis 1993). Indeed individuals adopting dismissing strategies under-report personal distress via self-report questionnaires compared to information obtained from peer reports (Larose and Bernier 2001). Thus, it is strongly suggested that future researchers focus on identifying self-injurers who do not report negative experiences with parents, and to collect multi-informant data regarding the individuals’ NSSI behavior, as well as corresponding risk factors, in order to further examine the nature of their self-harm.
Limitations
Despite the importance of the current findings, they are not without limitation. Primarily, the generalizability of results to community populations of late adolescents and young adults may be limited as these data come from a university student sample, comprised of mostly female students. Findings pertaining to characteristics of NSSI (functions, age of onset, number of methods) should be interpreted cautiously as they represent a restricted portion of the overall sample of due to the large amount of missing data for these items. As previously discussed, this amount of missing data may reflect individuals’ willingness to endorse engagement in NSSI generally, but to remain hesitant to disclose such experiences in detail, even through questionnaire format (see Klineberg et al. 2013). The use of self-report measures of parent–child relationship quality may yield modified and subjective perceptions of actual events and experiences, and, given the cross-sectional nature of the assessments, it is unclear whether relationship characteristics preceded NSSI. Finally, we were unable to account for the potential influences of extraneous variables (i.e., peer relationship quality, psychological symptoms) in the current study, which may have had relevance to the obtained profiles and to variation in NSSI.
Clinical Implications & Conclusions
The present study furthers our knowledge of parent–child relational influences in association with NSSI. In particular the current findings suggest that clinicians, teachers, frontline workers and counselors alike should not assume that only young adults reporting child abuse or neglect are at risk for engaging in NSSI, and that some self-injuring youth may even claim to have highly positive interaction with parents. Although individuals engaging in self-injury report both positive and negative family backgrounds, the present study nonetheless suggests that those with especially disrupted family experiences may be at increased risk for engaging in especially severe, prolonged NSSI. In conclusion, the current findings extend reigning social theory of the development of NSSI (Linehan 1993), and emphasize the need for additional rigorous research focused on understanding the nature of NSSI particularly within individuals who do not report experiencing the classic interpersonal risk factors. Nonetheless, therapies focusing on improving the quality of family relationships, or on changing the individual’s perceptions of relationship quality, may be particularly useful in the treatment and prevention of NSSI for many individuals.
References
Adrian, M., Zeman, J., Erdley, C., Lisa, L., & Sim, L. (2011). Emotional dysregulation and interpersonal difficulties as risk factors for non-suicidal self-injury in adolescent girls. Journal of Abnormal Child Psychology, 39, 389–400. doi:10.1007/s10802-010-9465-3.
Armsden, G. C., & Greenberg, M. T. (1987). The inventory of parent and peer attachment: Individual differences and their relationship to psychological well-being in adolescence. Journal of Youth and Adolescence, 16, 427–454. doi:10.1007/BF02202939.
Barrocas, A. L., Giletta, M., Hankin, B. L., Prinstein, M. J., & Abela, J. R. Z. (2014). Nonsuicidal self-injury in adolescence: longitudinal course, trajectories, and intrapersonal predictors. Journal of Abnormal Child Psychology, 43, 369–380. doi:10.1007/s10802-014-9895-4.
Bergman, L. R., & Trost, K. (2006). The person-oriented versus the variable-oriented approach: are they complementary, opposites, or exploring different worlds. Merrill-Palmer Quarterly, 52, 601–632. doi:10.1353/mpq.2006.0023.
Bowlby, J. (1969). Attachment and loss (Vol. I: Attachment). New York City: Basic Books.
Bureau, J.-F., Martin, J., Freynet, N., Poirier, A. A., Lafontaine, M.-F., & Cloutier, P. F. (2010a). Perceived dimensions of parenting and non-suicidal self-injury in young adults. Journal of Youth and Adolescence, 5, 484–494. doi:10.1007/s10964-009-9470-4.
Bureau, J.-F., Martin, J., & Lyons-Ruth, K. (2010b). Attachment dysregulation as hidden trauma in infancy: Early stress, maternal buffering, and psychiatric morbidity in adolescence. In R. Lanius, E. Vermetten, & C. Pain (Eds.), The hidden epidemic: The impact of early life trauma on health and disease (pp. 48–56). New York City: Cambridge University Press.
Claes, L., Vandereycken, W., & Vertommen, H. (2004). Family environment of eating disordered patients with and without self-injurious behaviors. European Psychiatry, 19, 494–498. doi:10.1016/j.eurpsy.2004.09.001.
Claes, L., Soenons, B., Vansteenkiste, M., & Vandereycken, W. (2012). The scars of the inner critic: perfectionism and nonsuicidal self-injury in eating disorders. European Eating Disorders Review, 20, 196–202. doi:10.1002/erv.1158.
Crowell, S. E., Beauchaine, T. P., McCauley, E., Smith, C. J., Vasilev, C. A., & Stevens, A. L. (2008). Parent–child interactions, peripheral serotonin, and self-inflicted injury in adolescents. Journal of Consulting and Clinical Psychology, 76, 15–21. doi:10.1037/0022-006X.76.1.15.
Di Pierro, R., Sarno, I., Perego, S., Gallucci, M., & Madeddu, F. (2012). Adolescent nonsuicidal self-injury: the effects of personality traits, family relationships and maltreatment on the presence and severity of behaviors. European Child and Adolescent Psychiatry, 21, 511–520. doi:10.1007/s00787-012-0289-2.
Gratz, K. L. (2006). Risk factors for deliberate self-harm among female college students: the role and interaction of childhood maltreatment, emotional inexpressivity, and affect intensity/reactivity. American Journal of Orthopsychiatry, 76, 238–250. doi:10.1037/0002-9432.76.2.238.
Hamza, C. A., & Willoughby, T. (2014). A longitudinal person-centered examination of nonsuicidal self-injury among university students. Journal of Youth and Adolescence, 43, 671–685. doi:10.1007/s10964-013-9991-8.
Hasking, P., Momeni, R., Swannell, S., & Chia, S. (2008). The nature and extent of non-suicidal self-injury in a non-clinical sample of young adults. Archives of Suicide Research, 12, 208–218. doi:10.1080/13811110802100957.
Hasking, P., Andrews, T., & Martin, G. (2013). The role of exposure to self-injury among peers in predicting later self-injury. Journal of Youth and Adolescence, 42, 1543–1556. doi:10.1007/s10964-013-9931-7.
Hilt, L. M., Nock, M. K., Lloyd-Richardson, E. E., & Prinstein, M. J. (2008). Longitudinal study of non-suicidal self-injury among young adolescents: Rates, correlates and preliminary test of an interpersonal model. Journal of Early Adolescence, 28, 455–469. doi:10.1177/0272431608316604.
IBM Corp Released. (2011). IBM SPSS statistics for windows, version 20.0. Armonk, NY: IBM Corp.
Kaess, M., Parzer, P., Mattern, M., Plener, P. L., Bifulco, A., Rusch, F., & Brunner, R. (2013). Adverse childhood experiences and their impact on frequency, severity and the individual function of nonsuicidal self-injury in youth. Psychiatry Research, 206, 265–272. doi:10.1016/j.psychres.2012.10.012.
Klineberg, E., Kelly, M. J., Stansfeld, S. A., & Bhui, K. S. (2013). How do adolescents talk about self-harm: a qualitative study of disclosure in an ethnically diverse urban population in England. BMC Public Health, 13, 572–582. doi:10.1186/1471-2458-13-572.
Klonsky, E. D. (2007). The functions of deliberate self-injury: a review of the evidence. Clinical Psychology Review, 27, 226–239. doi:10.1016/j.cpr.2006.08.002.
Klonsky, E. D., & Olino, T. M. (2008). Identifying clinically distinct subgroups of self-injurers among young adults: a latent class analysis. Journal of Consulting and Clinical Psychology, 76, 22–27. doi:10.1037/0022-006X.76.1.22.
Larose, S., & Bernier, A. (2001). Social support processes: mediators of attachment state of mind and adjustment in late adolescence. Attachment & Human Development, 3, 96–120. doi:10.1080/14616730010024762.
Levesque, C., Lafontaine, M.-F., Bureau, J.-F., Cloutier, P. F., & Dandurand, C. (2010). The influence of romantic relationships and intimate partner violence on non-suicidal self-injury in young adults. Journal of Youth and Adolescence, 39, 474–483. doi:10.1007/s10964-009-9471-3.
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. New York City: Guilford Press.
Lundh, L.-G., Wångby-Lundh, M., & Ulander, J. (2009). Emotional tone in young adolescents’ close relationships and its association with deliberate self-harm. Interpersona, 3, 111–138. Retrieved from http://interpersona.org/
Main, M., Hesse, E., & Goldwyn, R. (2008). Studying differences in language usage in recounting attachment history: an introduction to the AAI. In H. Steele & M. Steele (Eds.), Clinical applications of the adult attachment interview (pp. 31–68). New York City: The Guilford Press.
Martin, J., Cloutier, P. F., Levesque, C., Bureau, J.-F., Lafontaine, M.-F., & Nixon, M. K. (2013). Psychometric properties of the functions and addictive features scales of the Ottawa self-injury inventory: a preliminary investigation using a university sample. Psychological Assessment, 25, 1013–1018. doi:10.1037/a0032575.
Nixon, M.-K., & Heath, N. (2009). Introduction to non-suicidal self-injury in adolescents. In M.-K. Nixon & N. Heath (Eds.), Self-injury in youth: the essential guide to assessment and intervention (pp. 1–6). New York City: Routledge Press.
Parker, G., Tupling, H., & Brown, L. B. (1979). A parental bonding instrument. British Journal of Psychiatry, 52, 1–10. doi:10.1111/j.2044-8341.1979.tb02487.x.
Ramaswamy, V., Desarbo, W. S., Reibstein, D. J., & Robinson, W. T. (1993). An empirical pooling approach for estimating marketing mix elasticities with PIMS data. Marketing Science, 12, 103–124. doi:10.1287/mksc.12.1.103.
Saldias, A., Power, K., Gillanders, D. T., Campbell, C. W., & Blake, R. A. (2013). The mediatory role of maladaptive schema modes between parental care and non-suicidal self-injury. Cognitive Behavior Therapy. doi:10.1080/16506073.2013.781671.
Shedler, J., Mayman, M., & Manis, M. (1993). The illusion of mental health. American Psychologist, 48, 1117–1131. doi:10.1037//0003-066X.48.11.1117.
Swannell, S. V., Martin, G. E., Page, A., Hasking, P., & St. John, N. J. (2014). Prevalence of non-suicidal self-injury in nonclinical samples: systematic review, meta-analysis, and meta-regression. Suicide & Life-Threatening Behavior, 44, 273–303. doi:10.1111/sltb.12070.
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics (5th ed.). Boston: Pearson Education Inc.
Thompson, R. A. (1994). Emotion regulation: a theme in search of definition. In N. A. Fox & J. J. Campos (Eds.), The development of emotion regulation: biological and behavioral considerations. Chicago: University of Chicago Press.
Vermunt, J. K., & Magidson, J. (2005). Technical guide for LatentGOLD 4.0: basic and advanced. Belmont: Statistical Innovations Inc.
von Eye, A., & Bergman, L. R. (2003). Research strategies in developmental psychopathology: dimensional identity and the person-oriented approach. Development and Psychopathology, 15, 553–580. doi:10.1017.S0954579403000294.
West, M., Rose, S., Spreng, S., & Adam, K. (2000). The adolescent unresolved attachment questionnaire: the assessment of perceptions of parental abdication of caregiving behavior. The Journal of Genetic Psychology, 161, 493–503. doi:10.1080/00221320009596727.
Whitlock, J. L., Muehlenkamp, J. J., & Eckenrode, J. E. (2008). Variation in non-suicidal self-injury: identification and features of latent classes in a college population of emerging adults. Journal of Clinical Child & Adolescent Psychology, 37, 725–735. doi:10.1080/15374410802359734.
Williams, F., & Hasking, P. (2009). Emotion regulation, coping and alcohol use as moderators in the relationship between non-suicidal self-injury and psychological distress. Prevention Science, 11, 33–41. doi:10.1007/s11121-009-0147-8.
Yates, T. (2009). Developmental pathways from child maltreatment to non-suicidal self-injury. In M. K. Nock (Ed.), Understanding Non-suicidal self-injury: origins, assessment and treatment (pp. 117–138). Washington: American Psychological Association.
Yates, T. M., Tracy, A. J., & Luthar, S. S. (2008). Nonsuicidal self-injury in “privileged” youth: longitudinal and cross-sectional approaches to developmental process. Journal of Consulting and Clinical Psychology, 76, 52–62. doi:10.1037/0022-006X.76.1.52.
Acknowledgments
The authors would like to thank Drs. Annie Bernier, and Jane Ledingham for their feedback on an early version of this manuscript.
Conflicts of Interest
The authors have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Martin, J., Bureau, JF., Yurkowski, K. et al. Heterogeneity of Relational Backgrounds is Associated With Variation in Non-Suicidal Self-Injurious Behavior. J Abnorm Child Psychol 44, 511–522 (2016). https://doi.org/10.1007/s10802-015-0048-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-015-0048-1