
Abstract
Negative interpersonal events have been consistently identified as both antecedents and sequalae of adolescent depressive symptoms. However, little is known about the relative contributions of specific domains of interpersonal events (parents, peers or teachers) to the maintenance of depressive symptoms during early adolescence or whether a lack of positive interpersonal interactions plays a direct role in maintaining depressive symptoms. Further, few studies have examined whether positive interpersonal events moderate associations between negative events and adolescents’ depressive symptoms. This study combined stress generation and exposure models to evaluate the contribution of daily events to the maintenance of depressive symptoms in a sample of 132 adolescents (53 % female) followed from ages 13 to 15. Daily phone diaries collected at age 14 assessed adolescents’ negative and positive interactions with parents, teachers, and peers in a sample of adolescents from economically disadvantaged families. Negative peer events uniquely accounted for the maintenance of depressive symptoms over the 2 years period. Results did not differ by gender; however, positive parent events buffered the effects of negative parent events for females but not for males. Findings highlight the significance of peer relationships during a period of vulnerability for depressive symptoms.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Depressive symptoms that emerge during adolescence often follow a chronic and recurrent course (Tram and Cole 2006). An extensive literature has demonstrated reciprocal, or bidirectional, relations between negative interpersonal events and depressive symptoms (Carter et al. 2006; Clements et al. 2008; Moberly and Watkins 2008). Stress generation models view depression as predicting subsequent negative interpersonal events, whereas stress exposure models view negative interpersonal events as predicting subsequent depressive symptoms. These two models have been combined to account for the maintenance of depressive symptoms over time (Rudolph et al. 2009). In spite of an extensive literature on stress generation and stress exposure models of depressive symptoms, few studies have considered the discrete domains of negative interpersonal events (e.g., interactions involving parents, teachers, or peers) or the potential direct and moderating roles of positive interactions. The current study used an intensive diary assessment that differentiated between daily negative and positive interactions with parents, teachers, and peers. We then tested particular domains of interpersonal events as mechanisms that maintain depressive symptoms over a 2 years period among a sample of economically disadvantaged adolescents who are at increased risk for experiencing negative interpersonal events and depressive symptoms (Eamon 2001; Tracy et al. 2008).
Stress Exposure and Stress Generation Models of Depression
Over two decades of research support the stress exposure model of adolescents’ depressive symptoms (e.g., Compas et al. 1989). Initial support for this model came from studies based on self-reports of negative events or daily hassles (e.g., Sim 2000). Single assessments of daily hassles (i.e., negative events that occur over the course of a typical day, such as an argument with a parent) were found to be more robust predictors of depressive symptoms than major life events (DeLongis et al. 1982). The stress generation model provides an alternative account of the association between stress and depressive symptoms. This model acknowledges that children and adolescents actively contribute to their experiences and that individuals with depressive symptoms generate stressful events, particularly in how they interact with others (Rudolph et al. 2000). Studies of the stress generation model show that depressive symptoms are more likely to generate dependent events that are influenced by the individual’s affect and behavior (e.g., an argument with a parent or peer) than independent events that occur outside the individual’s control (e.g., death of a relative) (Rudolph et al. 2000; Rudolph 2008). Support for the stress generation model typically comes from studies that use context-based interview methods in which the “stressfulness” of events is determined by the evaluator to reduce risks associated with self-report measures (Hammen 2006).
The transactional model of stress and depression recognizes that depressive symptoms are influenced by the dynamic interplay between an individual and his/her environment (Sameroff and Mackenzie 2003). This model points to how the stress exposure and stress generation models are compatible with each other, with stressful interpersonal events serving as both antecedents and sequalae of depressive symptoms. When combined, stress exposure and stress generation models can account for the continuity of depression over time (Rudolph et al. 2009). Rudolph et al. (2009) integrated the stress generation and stress exposure models in a single mediation model. They found that stressful interpersonal events mediated increases in adolescent depressive symptoms over a 2 years time period for females from an at-risk community sample (the study oversampled adolescents higher in depressive symptoms). Longitudinal designs that include three or more time points allow for the examination of transactional processes by extending models to include more than just single unidirectional pathways.
Distinguishing Context and Valence of Interpersonal Events
Negative interpersonal events have been linked to the development and maintenance of adolescents’ depressive symptoms (e.g., Rudolph et al. 2009). Parent-child relations play a prominent role in the development of adolescent depressive symptoms (Sheeber et al. 2001). Both the mother-child relationship and the father-adolescent relationship have been implicated in adolescent depression (Sheeber et al. 2007). High levels of parent-adolescent conflict have been consistently associated with depression in community samples (Laursen and Collins 1994; Schneiders et al. 2007). In addition, negative peer events such as arguments with peers may contribute to low self-esteem and hopelessness about maintaining positive and trusting relationships (Storch and Ledley 2005). Further, negative interactions with teachers have been linked to adolescent risk behaviors (Kobak et al. 2012), whereas high-quality relationships with teachers protect children from experiencing chronically high levels of internalizing problems (O’Connor et al. 2011). Although negative interactions with parents, teachers, and peers have all been associated with adolescents’ depressive symptoms, much less is known about the relative contributions of these interpersonal domains to the maintenance of adolescents’ depressive symptoms.
A lack of positive interpersonal interactions may also play a direct role in maintaining depressive symptoms. Lewinsohn and colleagues (e.g., Lewinsohn and Graf 1973; Lewinsohn and Libet 1972) were among the first researchers to show that a lack of positive events is associated with depression. One study of loneliness in a community sample indicated that painful experiences of rejection or abandonment as well as a lack of pleasurable interpersonal engagement were both related to the onset and maintenance of depressive symptoms (Joiner et al. 2002). In addition, Joiner et al. (1996) found that lack of pleasurable engagement was a better predictor of adolescent depression than painful disconnection, which suggests that positive interpersonal experiences are as important in depression as negative interpersonal experiences. Previous findings also suggest differential effects for positive parent and peer events in terms of the impact of social support across interpersonal domains (Stice et al. 2004). Stice and colleagues found that a lack of parental support but not peer support predicted future increases in depressive symptoms, while depressive symptoms predicted future decreases in peer support but not parental support.
Some studies suggest that positive interpersonal events protect adolescents from risk associated with negative interpersonal events. The moderating effect of positive events has been shown in studies with adults. For example, Nezlek and Plesko (2003) found that positive events moderated the effects of negative events on daily self-esteem and depressogenic thinking in a community sample of adults. Given that adolescents look to their parents as a source of security and safety (Kobak et al. 2007), positive parent events may be particularly important in buffering the effects of negative events during this time period. Adolescents’ sex may also moderate the effects of interpersonal events on depressive symptoms. Ge et al. (1994) showed that using observer ratings of positive parent behaviors in a community sample of adolescents, maternal warmth and support protected females from adverse effects of life stress on depressive symptoms. Stadler et al. (2010) also found that parental support protected female middle school students against the effects of peer-victimization on mental health status.
Although research suggests there are no gender differences in the stability of depressive symptoms (e.g., Tram and Cole 2006), interpersonal events may be a more salient source of stress that maintain depressive symptoms for females (Rudolph et al. 2009). In a large longitudinal study, Hankin et al. (2007) examined adolescent gender as a moderator of the unique effects of different types of events in generation and exposure models. They found that sex differences in depression were partially explained by girls reporting higher rates of negative interpersonal events. Other research, however, suggests that in urban minority populations, the relationship between interpersonal stress and depression does not differ for males and females due to higher levels of stress reported by boys in this population (Carlson and Grant 2008; Grant et al. 2004).
Stress generation models have relied on contextual-based life events interviews, which have become the gold standard for documenting stressful life events (Liu and Alloy 2010). Whereas self-report measures rely on a priori decisions about the stressfulness of an event, contextual-based interviews include assessment of the circumstances surrounding the event so that “objective” ratings regarding the level of threat can later be assessed (Hammen 2006). Contextual-based interview methods have advantages over traditional self-report measures (e.g., life-events checklists; see Kessler 1997 for a review) in that they take into account the personal meaning of an event (e.g., its level of “stressfulness” from the point of view of the individual) and are less subject to mood-congruent cognitive bias (Hammen 2006). However, both traditional self-report and interview methods may not be sensitive to daily interpersonal interactions.
Structured diary measures are an alternative method of measuring stressful events that are relatively underutilized and offer advantages to both traditional self-report measures and contextual-based interviews. Diary methods are considered ecologically valid in that they assess every-day experiences in real world situations (Bolger et al. 2003). In contrast to traditional self-report measures that assess the occurrence of events over longer time periods, diary measures assess experiences as they unfold over a brief time interval, increasing accuracy in the recollection of events. Further, repeated diary measures afford a relatively large sample of behavior, providing more reliable estimates of an individual’s typical experiences (Bolger et al. 2003; Iida et al. 2012). Averaging across daily reports captures an individual’s typical experiences while reducing problems associated with retrospective reports. Finally, diary methods allow for the measurement of different types of events that may be distinguished by both valence and relationship domains.
The Current Study
The goal of this study was to examine how domains of daily interpersonal events (parents, teachers, or peers) contribute to the maintenance of depressive symptoms. In modeling the maintenance of depressive symptoms, we first examined the generation pathway in which depressive symptoms at age 13 were tested as predictors of increased exposure to daily interpersonal events at age 14. We then tested the exposure pathway in which interpersonal events at age 14 were tested as predictors of age 15 depressive symptoms. Finally, we tested both generation and exposure paths in a single model to examine different types of events as mechanisms that maintain depressive symptoms. We also tested whether positive events moderated the effects of negative events on depressive symptoms (Ge et al. 1994) and whether there were gender differences in the models. The sample was restricted to disadvantaged adolescents to extend prior work on depression to a low-income sample and to examine variability within a group at increased risk for exposure to negative events and depressive symptoms (Eamon 2001; Tracy et al. 2008).
Method
Participants
One hundred thirty-two adolescents (53 % female) were recruited from the first cohort of a two-cohort sample of 225 low-income families participating in a larger longitudinal study. Adolescents completed 2 weeks of diaries for which they received $75. Funding for this study enabled us to conduct daily phone diaries for only a portion of the original sample. The average annual family income for the sample ranged from 0 to > $200,000 (M = $25,500; SD = $26,000; Mdn = $20,500; Lower Quartile = $7,500; Upper Quartile = $37,000). Seventy-six percent of the sample identified themselves as African American, 21 % Caucasian, and 3 % Hispanic.
Procedures
The age 13 and age 15 assessments took place in the adolescents’ homes and schools. At age 14, adolescents and their caregivers were interviewed by phone on 8 weekday evenings (Monday through Thursday). Daily diaries were collected at age 14 with phone interviews that took place over the course of two consecutive weeks between the hours of 6 p.m. and 10 p.m. Interviews were conducted only on weekday evenings to allow participants to report on events that occurred in the school context and to maximize the likelihood of reaching participants at a consistent time each day. Phone interviews lasted approximately 15 min and were administered by trained undergraduate research assistants. If a participant was unable to be reached on a particular evening, research assistants continued to call them on subsequent evenings until they completed all eight interviews. On average, participants completed the eight phone interviews within 15 days (SD = 8 days). Forty-four percent of participants completed all phone interviews consecutively (in 11 days).
Measures of Depression
Depressive Symptoms
The Children’s Depression Inventory (CDI; Kovacs 1985) was administered when the subjects were approximately 13 years old. The CDI is a 27-item self-report questionnaire that assesses depressive symptoms in children. Each of the items consists of three statements scored from 0 to 2, in order of increasing severity. Cronbach’s alpha for the CDI was 0.82 in this study. The Center for the Epidemiological Study of Depression Scale (CES-D; Radloff 1977) was administered when the subjects were 15. The CES-D is a 20-item measure that asks the participant to rate how often over the past week they experienced symptoms associated with depression, such as restless sleep, poor appetite, and feeling lonely. Response options ranged from 0 (Rarely or none of the time) to 3 (Most or almost all the time).
Self-Esteem
The Rosenberg Self-Esteem Scale (Rosenberg 1965) is a widely used measure of self-value and self-respect that has good construct, convergent, and discriminant validity (Crandal 1973). The scale’s ten items are rated from 1 (Strongly Disagree) to 9 (Strongly Agree) and a total scale score was computed by averaging across items. Internal consistency for the sample (measured by Cronbach’s alpha) is 0.85.
Hopelessness
The 17-item Hopelessness scale (Kazdin et al. 1986) was administered to measure the degree to which an individual feels hopeless. Respondents may answer “True” or “False” to the items, and a total scale score is computed by averaging all item scores. The scale demonstrates good reliability (Cronbach’s alpha of 0.77 in the present sample) and good predictive validity (as a predictor of depressive symptoms and suicidality; Kazdin et al. 1986).
Diary Measures
Daily Event Scale
Participants indicated the extent to which events occurred during the past day on a 1 (not at all) to 4 (a lot) scale. The events scale was an expanded version used in previous studies (Little and Kobak 2003; Esposito et al. 2005). Similar daily event measures, such as the Daily Events Survey (DES; Butler et al. 1994), have been successfully used in daily diary studies with adults, though our study differed from the DES in that we did not ask participants to report on the subjective importance of the events. The 38 daily event items were subjected to principal axis factoring with Promax rotation. Ten factors were initially identified. In order to focus on general parent, teacher, and peer events, items measuring aggression (4 items), romantic interactions (2 items), positive achievement events (3 items), and parental involvement/monitoring (3 items) were excluded, as well as 4 items with loadings less than 0.40 (e.g., Did you go somewhere with one of your parents?). Five factors consisting of the remaining items were then subjected to multilevel factor analysis in MPLUS. The scale that resulted in optimal model fit consisted of 17 items: 4 positive parent events (Your parent showed affection to you; You showed affection to your parent; You shared something about your day with your parent; Your parents let you know they were pleased with something you did; α = 0.77); 4 negative parent events (You talked back to a parent; You were yelled at by a parent; You argued with a parent; Your parent cursed at you; α = 0.76); 2 positive peer events (You talked with your friends; You joked around with your friends; α = 0.61); 3 negative peer events (You got into a fight with another kid; You argued with another kid; Another kid disrespected you; α = 0.74); and 4 negative teacher events (You got in trouble with a teacher; You received a detention; A teacher got mad at you; You got a warning from a teacher; α = 0.76).
Control Measures
Daily Negative Affect
Four items (sad, blue, downhearted, and alone) from the Sadness subscale of the Positive and Negative Affect Schedule (PANAS; Watson and Clark 1992) assessed children’s daily negative affect on a 1 (strongly disagree) to 5 (strongly agree) scale regarding how they felt that day, and item scores were averaged to calculate a daily negative affect score. These scores were then aggregated across the eight diary days to measure the participants’ typical level of negative affect at the time of the diary assessment. The negative affect scale showed good internal consistency in the present study (α = 0.84).
Family Income-to-Needs Ratio
The income-to-needs ratio reflected per capita family income divided by the per capita figure constituting the federal poverty standard for the assessment year. At the age 13 assessment wave, caregivers provided estimates of total household income earned from employment of all residents and income derived from other sources (i.e., disability, child support, public assistance, retirement, etc.). A ratio of 1.0 represents the poverty line and 2.0 represents the threshold for economic disadvantage. The mean was 1.27 (SD = 0.99) and the median was 1.15. Forty-four percent had ratios below the poverty line.
Family Risk Index
The family risk index (Ackerman and Brown 2006) reflected caregiver responses at the age 13 assessment wave to questions about five markers of family risk experienced in the previous 2 years. For each marker, we coded affirmative answers 1 and negative answers 0 and summed the scores to form an index. The markers reflected mother reports about (a) whether she experienced any changes in intimate residential partners (32 %); (b) whether the household experienced any change in residence (36 %); (c) whether any adult member of the household had police contact for criminal behavior (15 %); (d) whether any adult member of the household was under psychiatric treatment (20 %); and (e) whether any adult member of the household experienced drug or alcohol dependence or abuse (17 %). The index mean was 1.17 (SD = 1.06). Among these markers, only change in residence and change in mother’s intimate residential partners correlated significantly (r = 0.24, p < 0.01).
Results
Data Analytic Plan
After examining descriptive statistics and zero-order correlations among the observed predictor, outcome, and family variables, a measurement model tested the structure and gender invariance of depressive symptoms at ages 13 and 15. Structural equation modeling was then used to address the main study aims. Analyses were conducted in Mplus Version 6.0 (Muthén and Muthén 1998–2010). The form of estimation was maximum likelihood (ML). Maintenance of depressive symptoms was determined by the presence of a significant A path (events regressed on age 13 depressive symptoms), a significant B path (age 15 depressive symptoms regressed on events), and a significant indirect path (A and B paths). Because we were interested in examining factors that maintain adolescent depressive symptoms, we did not control for previous levels of depressive symptoms in our models.
Presence of a significant indirect path through aggregated levels of daily events was calculated using bootstrapping procedures (MacKinnon et al. 2002; Shrout and Bolger 2002) that take multiple random samples of observations (we chose 1,000) from the original sample, with replacement, and provides a distribution of parameter estimates. This procedure is considered more powerful than the conventional Sobel test, especially with small samples (Little et al. 2007). Distributions of parameter estimates tend to be skewed (MacKinnon et al. 2002); therefore, bias-corrected confidence intervals were computed (Efron and Tibshirani 1993; MacKinnon et al. 2004). An effect is significantly different from zero if zero is not included in the bootstrapped confidence interval. For testing our hypotheses, we relied on the conventional 5 % alpha significance level. However, in addition to the corresponding 95 % confidence intervals (CIs), we also report 99 % CIs to explore the effects of controlling potential Type I error inflation.
Model fit was assessed using the Comparative Fit Index (CFI; Bentler 1990), the Root Mean Square Error of Approximation (RMSEA; Browne and Cudeck 1993), and the Standardized Root Mean Square Residual (SRMR; Bentler 1995), in addition to a chi-square test. The CFI is considered acceptable if above 0.9, but values above 0.95 are considered indicative of good fit (Kaplan 2000). RMSEA and SRMR values below 0.05 are considered acceptable, values between 0.05 and 0.08 are considered indicative of fair fit, and values between 0.08 and 0.10 are considered an indication of mediocre fit (Kaplan 2000). Nested models were compared using Χ 2 difference tests.
Preliminary Analyses
Zero-Order Correlations
Descriptive statistics and zero-order correlations among the observed variables are shown in Tables 1 and 2. Examination of distributional statistics indicated that many of the variables were skewed, and as a result, Log 10 transformations were used to establish normal distributions prior to subsequent analyses. For the most part, adolescents’ gender was not associated with differences in symptoms or diary measures. However, by age 15, females reported slightly higher levels of depressive symptoms and lower levels of self-esteem than males. The family demographic variables were not correlated with the other study variables. Given the lack of relations between the demographic variables and other study variables, we did not include the demographic variables as covariates in subsequent analyses.
CFA of the Depressive Symptoms
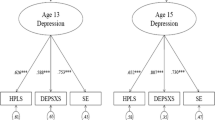
Because a different depression scale was used at the age 13 and age 15 assessments, this study used a latent variable that combined scores from the depression scales with scores from the Hopelessness Scale and Rosenberg’s Self-Esteem Scale. The estimated factor represented Beck’s negative cognitive triad (Beck 1967), which includes negative views of the self (low self-esteem), the world (general depressive symptoms), and the future (hopelessness). The model depicted in Fig. 1 shows the confirmatory factor analysis that evaluated depression, low self-esteem and hopelessness as multiple indicators of depressive symptoms at ages 13 and 15. Hopelessness was chosen as the reference variable and its unstandardized factor loading was constrained to 1. Error terms for the repeated measures (hopelessness and self-esteem) were allowed to covary (Cole et al. 2007), as depicted by the curved double-headed arrows between the smaller circles in the figure. Chi-square tests and other goodness-of-fit indices indicated that the model had adequate fit to the data (Χ 2 (6) = 1.596, p = 0.95; RMSEA = 0.000; CFI = 1.000; SRMR = 0.019). The latent depressive symptoms variables were significantly correlated (r = 0.59, p < 0.001), providing further evidence that reports of depressive symptoms were stable across ages 13 to 15. Paired samples t-tests provided further evidence of the stability of depressive symptoms: the means for the hopelessness (t (95) = 0.114, p > 0.05) and self-esteem variables (t (95) = 0.28, p > 0.05) did not significantly differ across the two time points. Given the lack of variance in growth of depression, the effect of events on changes in depression was not evaluated.

Standardized parameter estimates for the measurement of latent depression variables
To examine measurement invariance across male and female adolescents, we first performed single-group analyses for each gender group. The two-factor model had adequate fit for both males (Χ 2 (6) = 4.210, p = 0.6482; RMSEA = 0.000; CFI = 1.000; SRMR = 0.040) and females (Χ 2 (6) = 3.627, p = 0.7270; RMSEA = 0.000; CFI = 1.000; SRMR = 0.038). We then performed a multiple group analysis to examine measurement invariance across the two groups by comparing a series of nested models using chi-square difference tests. The first model tested the equality of the overall structure (configural invariance). The nested models included constraints across gender groups of equal factor loadings (factor loading invariance) and item intercepts (intercept invariance). Results indicated configural (Χ 2 (12) = 7.838, p = 0.7977; RMSEA = 0.000; CFI = 1.000; SRMR = 0.039), factor loading (ΔΧ2 (Δdf = 4) = 1.104, p = 0.8936), and intercept invariance (ΔΧ2 (Δdf = 4) = 4.405, p = 0.3540) in indicators of depressive symptoms across males and females.
The Generation Model
The initial analyses tested whether depressive symptoms at age 13 predicted interpersonal events at age 14 (the generation model). The hypothesis was that depressive symptoms at age 13 would predict increased exposure to negative interpersonal events and decreased exposure to positive interpersonal events. We explored unique effects of event type by differentiating the events by their valence (i.e., positive vs. negative) and interpersonal context (i.e., whether the events involved parents, teachers, or peers). Age 13 depressive symptoms significantly predicted negative parent events (B = 0.473, p < 0.001), negative teacher events (B = 0.442, p < 0.001), negative peer events (B = 0.468, p < 0.001), and positive parent events (B = −0.369, p < 0.001) in the hypothesized directions. The path to positive peer events was not significant (B = −0.160, n.s.).
The Exposure Model
The second set of analyses tested whether interpersonal events at age 14, in turn, predicted depressive symptoms at age 15 (the exposure model). The hypothesis was that heightened negative events and decreased positive events, in turn, would predict age 15 depressive symptoms. All five event variables were entered as simultaneous predictors to assess the unique effect of each variable while controlling for overlapping variance of the predictors. The effects of negative peer events (B = 0.361, p < 0.01) and positive peer events (B = −0.271, p < 0.05) were both significant. When negative affect was entered into the model (to account for possible bias due to mood-congruent reporting), negative and positive peer events remained significant predictors. We tested for multicollinearity using the variance inflation factor (VIF). Successive calculations with different combinations of variables indicated VIFs well below the typical cutoff (VIF = 10). Thus, the lack of significant findings for all but the peer events variables was not due to a problem with multicollinearity.
Maintenance of Depressive Symptoms
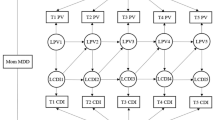
The final analyses combined the generation and exposure models to examine whether negative or positive interpersonal events at age 14 maintained depressive symptoms across ages 13 and 15 (see Fig. 2). All five event variables were entered simultaneously as maintenance variables between age 13 and age 15 depressive symptoms. The hypothesis was that heightened exposure to negative events and reduced exposure to positive events would maintain depressive symptoms. The events variables were allowed to correlate with each other. The model had adequate fit to the data (Χ 2 (28) = 34.264, p = 0.1923; RMSEA = 0.041; CFI = 0.983; SRMR = 0.065). Standardized path coefficients are shown in Fig. 2 and confidence intervals are summarized in Table 3. Bootstrapping results supported the indirect effect of negative peer events (95 % CI: 0.053–0.395) indicating that heightened exposure to negative peer events contributed to the maintenance of depressive symptoms. None of the other age 14 interpersonal events variables produced a significant indirect effect. The indirect effect for negative peer events remained significant when controlling for NA at age 14.

The combined model in which average daily negative and positive events maintain depressive symptoms across ages 13 to 15. Correlations among the negative events variables and between the negative events variable and positive events variables were included but not depicted in the figure
Gender and Positive Events as Moderators
Gender was tested as a moderator of the association between events and depressive symptoms in the combined model. Single group analyses of males and females suggested that the model fit was better for females (Χ 2 (28) = 20.495, p = 0.8457; RMSEA = 0.000; CFI = 1.000; SRMR = 0.064) than for males (Χ 2 (28) = 45.577, p = 0.0193; RMSEA = 0.101; CFI = 0.896; SRMR = 0.098). To determine whether the difference in model fit was statistically significant, multiple group analyses compared a model in which paths were free to vary for males and females (i.e., the baseline model; Χ 2 (64) = 71.986, p = 0.2306; RMSEA = 0.043; CFI = 0.978; SRMR = 0.086) to a model in which cross-group equality constraints were imposed on all of the regression paths (Χ 2 (74) = 73.606, p = 0.4911; RMSEA = 0.000; CFI = 1.000; SRMR = 0.087). Comparison of model fit did not reveal significant gender differences in the model (ΔΧ2 (10) = 1.62, p = 0.9985).
We also tested whether positive events buffered the effects of negative events on depressive symptoms. We tested a series of exposure models in MPLUS that included a negative events variable, a positive events variable, and their interaction (the product of the mean centered negative and positive events variables created using the DEFINE command) as predictors of the age 15 latent depressive symptoms variable. None of the interactions were significant; however, when males and females were examined separately, positive parent events significantly moderated the effects of negative parent events for females (B = −0.010, p = 0.048) but not for males (B = 0.008, p > 0.05) (ΔΧ2 (1) = 5.665, p < 0.05). Females who reported more positive parent interactions reported weaker effects of negative parent events in maintaining depressive symptoms (see Fig. 3 for graphical representation). The relationship between negative parent events and depressive symptoms for males was consistent across all levels of positive parent events.

Moderating effect of positive parent events. The lines represent the relationships between negative parent events and age 15 depressive symptoms for female subjects who were 1.5 SD below the mean (low positive parent events) and those who were 1.5 SD above the mean (high positive parent events)
Discussion
The findings build upon and extend previous studies of stress generation and stress exposure models of depressive symptoms (Hankin et al. 2007; Rudolph et al. 2009). Although negative interpersonal events have been an integral component of exposure and generation models, relatively little is known about how discrete domains of negative events maintain adolescents’ depressive symptoms. The current findings indicate that negative interactions with peers make unique contributions to maintaining adolescents’ depressive symptoms. The focus on maintenance of depressive symptoms required that negative peer events be both predicted by age 13 depressive symptoms (the generation model) and also that these events predicted depressive symptoms at age 15 (the exposure model). In support of the generation model, depressive symptoms at age 13 predicted more frequent negative parent, teacher, and peer events and fewer positive parent events at age 14. The results also indicated that negative peer events and a lack of positive peer events uniquely predicted depressive symptoms at age 15 in support of the exposure model. However, in more stringent tests of mechanisms that maintained depressive symptoms between ages 13 and 15, only negative peer events accounted for the maintenance of depressive symptoms over the two-year period. Adding controls for negative affect to the model indicated that associations between events and depressive symptoms were not inflated due to mood-bias.
Although both negative and positive peer events at age 14 predicted depressive symptoms at age 15, only negative peer events contributed to the maintenance of depressive symptoms from ages 13 to 15. This finding extends prior findings on negative peer events and depression (e.g., Hankin et al. 2007) by indicating that negative experiences with peers play an important role in maintaining depressive symptoms. Because daily negative peer events were defined in terms of aggression and victimization experiences (e.g., “Got into a fight with another kid.”), it is possible that this association reflects comorbid depressive and externalizing symptoms. Links between aggressive behavior/peer victimization and depressive symptoms are well established (Sweeting et al. 2006; Vitaro et al. 2002) and have been attributed to increased peer relationship problems that occur for some adolescents (Dodge et al. 1997; Poulin and Boivin 2000a; Poulin and Boivin 2000b).
Previous studies have reported that females, but not males, benefit from maternal warmth and support as a stress buffer (e.g., Ge et al. 1994; Stadler et al. 2010). The results extended these findings by showing that girls’ daily positive parent events served to reduce the influence of negative parent events on depressive symptoms. In other words, negative interactions with parents increased risk of depressive symptoms for females who reported a low frequency of positive parent interactions, but depressive symptoms were not affected by frequency of negative parent events for females who reported higher levels of positive parent events. Thus, the adolescent girls in our sample were particularly sensitive to positive aspects of relationships with parents in ways that reduced their risk of depressive symptoms. This suggests that prevention/intervention efforts should be aimed at increasing positive parent interactions for female adolescents.
The diary design provided information about adolescents’ rates of exposure to events with parents, peers, and teachers. Adolescents in the current study reported higher mean levels of both negative and positive peer events compared to parent and teacher events. Both types of events at age 14 predicted depressive symptoms at age 15. These findings suggest that heightened sensitivity to peer interactions, specifically, may play a role in the development and maintenance of depressive symptoms in early adolescence. Neural developmental changes in the brain’s social information processing network (SIPN), which is involved in emotional attributes applied to social stimuli, has been implicated in the development of mood disorders during adolescence (Nelson et al. 2005). The SIPN model proposes that adolescents experience heightened sensitivity to interpersonal events, which, in turn, increases their risk for depression. Thus, with the increased importance of peers during this time period, peer events begin to serve a primary role in the development of adolescents’ depressive symptoms.
The daily diary methodology provided an alternative to the retrospective self-report and interview methods commonly used in the stress/depression literature. By aggregating daily reports, this methodology provided a more ecologically sensitive measure of youth’s interpersonal experiences and decreased the influence of retrospective memory bias found in measures that require adolescents to report events over a period of weeks or months. Additionally, the diary design allowed us to measure and control for concurrent mood states, decreasing the risk of mood congruent memory bias.
Limitations
There were several limitations to the study. The sample consisted of adolescents from economically disadvantaged families. We do not know whether the findings would hold for adolescents across a wider range of socioeconomic circumstances. The study was designed to examine daily interpersonal events as factors that maintain depressive symptoms in early adolescence. The design did not allow us to rule out the possibility that concurrent associations between depressive symptoms and events explain significant paths linking depressive symptoms and events across time. Because we did not control for depressive symptoms at ages 13 or 14 (we were interested in the maintenance of depressive symptoms rather than growth in symptoms), relations between events and depressive symptoms at age 14 may explain the predictive associations across time. However, controlling for NA at age 14 accounted for the associations between depression and events at age 14 to some extent. In addition, the daily diary measures were limited to self-report. It is possible that the use of other informants, such as teachers and parents would have produced different results. Future studies should include multiple methods for measuring emotional reactivity and depressive symptoms in order to avoid possible bias associated with lack of method variance. Further, the diary measure of daily events was constructed for this study (based on prior models) and does not have a validation history, although factor analysis and tests of reliability provide initial support for the validity of the measure. Finally, the study design cannot account for unmeasured third variables. For example, relations between disruptive behavior problems and depressive symptoms are well established (Loeber et al. 1994; Patterson et al. 1992). Given that negative peer interactions include aggressive behavior as well as victimization experiences, comorbid disruptive behavior problems may partially account for the observed relationships.
Adolescents’ gender did not moderate the direct paths between depressive symptoms and daily interpersonal interactions. The current sample was restricted to a relatively small nonclinical sample of young adolescents (only 10 % of the current sample reported symptoms above the clinical cutoff score of 19 for the CDI; Kovacs 1985). One possible explanation for the lack of gender differences is that the majority of studies documenting gender differences in the association between depression and daily events were conducted in samples of older adolescents with higher levels of depressive symptoms (e.g., Hankin et al. 2007). Although most research shows that economically disadvantaged minority adolescents are at increased risk for exposure to negative interpersonal events (e.g., Evans 2004) and depressive symptoms (Tracy et al. 2008), some studies found that African American children actually report fewer depressive symptoms than Caucasian and Latino children (e.g., Twenge and Nolen-Hoeksema 2002). Further, studies suggest that gender differences in stress models of depression may be minimized in low income, urban minority samples (Carlson and Grant 2008; Grant et al. 2004).
The latent depressive symptoms variables used in the study were constructed from scales measuring aspects of depression consistent with Beck’s cognitive triad: negative thoughts about the future, self, and world. A potential limitation of the current study is that once these scale composites were pooled with hopelessness and self-esteem scales, the latent variables largely represented cognitive aspects of depression (negative thoughts and beliefs) even though the general depression scales measured multiple types of depressive symptoms. It is possible that negative daily experiences relate differently to other types of depressive symptoms, including mood and behavioral symptoms.
The study has several implications for understanding, preventing and treating depressive symptoms during early adolescence. Given the importance of negative peer events in maintaining depressive symptoms, programs designed to reduce negative peer interactions may prevent the development and maintenance of depressive symptoms during this time period. Classroom or school wide programs intended to reduce peer victimization during early adolescence may contribute to reductions in depressive symptoms. The results also suggest that clinical interventions such as those with a social skills component (e.g., interpersonal therapy for adolescent depression) could benefit by helping adolescents to cope with negative peer interactions and develop interpersonal skills that reduce exposure to negative events. Finally, the results suggest that girls are more sensitive to positive interactions with family members. Interventions designed to increase positive/warm parent-adolescent interactions may be particularly effective for girls who experience higher levels of family conflict.
The current study extends the literature on daily events and depressive symptoms (e.g., Carter et al. 2006; Clements et al. 2008) by identifying unique effects of negative peer events in maintaining adolescent depressive symptoms across ages 13 to 15. This study highlights the importance of peer interactions during this time period. Future studies could differentiate among interactions with close friends, romantic partners, and more distal members of the peer network.
References
Ackerman, B. P., & Brown, E. D. (2006). Income poverty, poverty co-factors, and the adjustment of children in school. In R. V. Kail (Ed.), Advances in child development and behavior, 34 (pp. 91–129). Oxford: Elsevier.
Beck, A. T. (1967). Depression: Clinical, experimental, and theoretical aspects. New York: Harper & Row.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107, 238–246.
Bentler, P. M. (1995). EQS structural equations program manual. Encino: Multivariate Software.
Bolger, N., Davis, A., & Rafaeli, E. (2003). Diary methods: capturing live as it is lived. Annual Review of Psychology, 54, 579–616.
Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & J. S. Long (Eds.), Testing structural equation models (pp. 136–162). Beverly Hills: Sage.
Butler, A. C., Hokanson, J. E., & Flynn, H. A. (1994). A comparison of self-esteem lability and low trait self-esteem as vulnerability factors for depression. Journal of Personality and Social Psychology, 66, 166–177.
Carlson, G. A., & Grant, K. E. (2008). Adolescents risk for psychopathology among African American urban adolescents. Journal of Early Adolescence. doi:10.1177/0272431608314663.
Carter, J. S., Garber, J., Ciesla, J. A., & Cole, D. A. (2006). Modeling relations between hassles and internalizing and externalizing symptoms in adolescents: a four-year prospective study. Journal of Abnormal Psychology, 115, 428–442.
Clements, M., Aber, J. L., & Seidman, E. (2008). The dynamics of life stressors and depressive symptoms in early adolescence: a test of six theoretical models. Child Development, 79, 1168–1182.
Cole, D. A., Ciesla, J., & Steiger, J. H. (2007). The insidious effects of completely justifiable correlated residuals in latent variable covariance structure analysis. Psychological Methods, 12, 381–398.
Compas, B. E., Howell, D. C., Phares, V., Williams, R. A., & Ledoux, N. (1989). Parent and child stress and symptoms: an integrative analysis. Developmental Psychology, 25, 550–559.
Crandal, R. (1973). The measurement of self-esteem and related constructs. In J. P. Robinson & P. R. Shaver (Eds.), Measures of social psychological attitudes (pp. 80–82). Ann Arbor: ISR.
DeLongis, A., Coyne, J. C., Dakof, G., Folkman, S., & Lazarus, R. S. (1982). Relationship of daily hassles, uplifts, and major life events to health status. Health Psychology, 1, 119–136.
Dodge, K. A., Lochman, J. E., Harnish, J. D., & Bates, J. E. (1997). Reactive and proactive aggression in school children and psychiatrically impaired chronically assaultive youth. Journal of Abnormal Psychology, 106, 37–51.
Eamon, M. K. (2001). The effects of poverty on children’s socioemotional development: an ecological systems approach. Social Work, 46, 256–266.
Efron, B., & Tibshirani, R. J. (1993). An introduction to the bootstrap. Chapman & Hall.
Esposito, A. J., Kobak, R., & Little, M. (2005). Aggression and self-esteem: a diary study of children’s reactivity to negative interpersonal events. Journal of Personality, 73, 887–906.
Evans, G. W. (2004). The environment of childhood poverty. American Psychologist, 59, 77–92.
Ge, X., Lorenz, F. O., Conger, R. D., Elder, G. H., & Simons, R. L. (1994). Trajectories of stressful life events and depressive symptoms during adolescence. Developmental Psychology, 30, 467–483.
Grant, K. E., Lyons, A. L., Finkelstein, J. S., Conway, K. M., Reynolds, L. K., & O’Koon, J. H. (2004). Gender differences in rates of depressive symptoms among low-income, urban, African American youth: a test of two mediational hypotheses. Journal of Youth and Adolescence, 33, 523–533.
Hammen, C. (2006). Stress generation in depression: reflections on origins, research, and future directions. Journal of Clinical Psychology, 62, 1065–1082.
Hankin, B. L., Mermelstein, R., & Roesch, L. (2007). Sex differences in adolescent depression: stress exposure and reactivity models. Child Development, 78, 279–295.
Iida, M., Shrout, P. E., Laurenceau, J.-P., & Bolger, N. (2012). Using diary methods in psychological research. In H. Cooper, P. M. Camic, D. L. Long, A. T. Panter, D. Rindskopf, & K. J. Sher (Eds.), APA handbook of research methods in psychology, Vol 1: Foundations, planning, measures, and psychometrics (pp. 277–305). Washington: American Psychological Association.
Joiner, T. E., Jr., Catanzaro, S. J., & Laurent, J. (1996). The tripartite structure of positive and negative affect, depression, and anxiety in child and adolescent psychiatric inpatients. Journal of Abnormal Psychology, 105, 401–409.
Joiner, T. E., Lewinsohn, P. M., & Seeley, J. R. (2002). The core of loneliness: lack of pleasurable engagement–more so than painful disconnection–predicts social impairment, depression onset, and recovery from depressive disorders among adolescents. Journal of Personality Assessment, 79, 472–491.
Kaplan, D. (2000). Structural equation modeling: Foundations and extensions. Thousand Oaks: Sage.
Kazdin, A. E., Rodgers, A., & Colbus, D. (1986). The hopelessness scale for children: psychometric characteristics and concurrent validity. Journal of Consulting and Clinical Psychology, 54, 241–245.
Kessler, R. C. (1997). The effects of stressful life events on depression. Annual Review Psychology, 48, 191–214.
Kobak, R., Rosenthal, N., Zajac, K., & Madsen, S. (2007). Adolescent attachment hierarchies and the search for an adult pair bond. New Directions in Child Development Adolescent Attachment, 2007, 57–72.
Kobak, R., Herres, J., Gaskins, C., Gaskins, C., & Laurenceau, J.-P. (2012). Teacher-student interactions and adolescent states of mind as predictors of early romantic attachments and risky sexual behaviors. Attachment and Human Development, 14, 289–303.
Kovacs, M. (1985). The children’s depression inventory (CDI). Psychopharmacology Bulletin, 21, 995–998.
Laursen, B., & Collins, W. A. (1994). Interpersonal conflict during adolescence. Psychological Bulletin, 115, 1970–209.
Lewinsohn, P. M., & Graf, M. (1973). Pleasant activities and depression. Journal of Consulting and Clinical Psychology, 41, 261–268.
Lewinsohn, P. M., & Libet, J. (1972). Pleasant events, activity schedules, and depressions. Journal of Abnormal Psychology, 79, 291–295.
Little, M., & Kobak, R. (2003). Emotional security with teachers and children’s stress reactivity: a comparison of special-education and regular-education classrooms. Journal of Clinical Child and Adolescent Psychology, 32, 127–138.
Little, T. D., Preacher, K. J., Selig, J. P., & Card, N. A. (2007). New developments in latent variable panel analyses of longitudinal data. International Journal of Behavioral Development, 31, 357–365.
Liu, R. T., & Alloy, L. B. (2010). Stress generation in depression: a systematic review of the empirical literature and recommendations for future study. Clinical Psychology Review, 30, 582–593.
Loeber, R., Russo, M. F., Stouthamer-Loeber, M., & Lahey, B. B. (1994). Internalizing problems and their relation to the development of disruptive behaviors in adolescence. Journal of Research on Adolescence, 4, 615–637.
MacKinnon, D. P., Lockwood, C. M., Hoffman, J. M., West, S. G., & Sheets, V. (2002). A comparison of methods to test mediation and other intervening variable effects. Psychological Methods, 7, 83–104.
MacKinnon, D. P., Lockwood, C. M., & Williams, J. (2004). Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behavioral Research, 39, 99–128.
Moberly, N. J., & Watkins, E. R. (2008). Ruminative self-focus and negative affect: an experience sampling study. Journal of Abnormal Psychology, 117, 314–323.
Muthén, L. K., & Muthén, B. O. (1998). Mplus user’s guide (6th ed.). Los Angeles: Muthén & Muthén.
Nelson, E. E., Leibenluft, E., McClure, E. B., & Pine, D. S. (2005). The social re-orientation of adolescence: a neuroscience perspective on the process and its relation to psychopathology. Psychological Medicine, 35, 163–174.
Nezlek, J. B., & Plesko, R. M. (2003). Affect- and self-based models of relationships between daily events and daily well-being. Personality and Social Psychology Bulletin, 29, 584–596.
O'Connor, E. E., Dearing, E., & Collins, B. A. (2011). Teacher-child relationship and behavior problem trajectories in elementary school. American Educational Research Journal, 48, 120–162.
Patterson, G. R., Reid, J. B., & Dishion, T. J. (1992). A social interactional approach: Antisocial boys. Eugene: Castalia Publishing Company.
Poulin, F., & Boivin, M. (2000a). Reactive and proactive aggression: evidence of a two-factor model. Psychological Assessment, 12, 115–122.
Poulin, F., & Boivin, M. (2000b). The role of proactive and reactive aggression in the formation and development of friendships in boys. Developmental Psychology, 36, 1–8.
Radloff, L. S. (1977). The CES-D scale: a self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401.
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton: Princeton University Press.
Rudolph, K. D. (2008). Developmental influences on interpersonal stress generation in depressed youth. Journal of Abnormal Psychology, 117, 673–679.
Rudolph, K. D., Hammen, C., Burge, D., Lindberg, N., Herzberg, D., & Daley, S. E. (2000). Toward an interpersonal life-stress model of depression: the developmental context of stress generation. Development and Psychopathology, 12, 215–234.
Rudolph, K. D., Flynn, M., Abaied, J., Groot, A., & Thompson, R. (2009). Why is past depression the best predictor of future depression? Stress generation as a mechanism of depression continuity in girls. Journal of Child Clinical and Adolescent Psychology, 38, 473–485.
Sameroff, A. J., & Mackenzie, M. J. (2003). Research strategies for capturing transactional models of development: the limits of the possible. Developmental Psychopathology, 15, 613–640.
Schneiders, J., Nicolson, N. A., Berkhof, J., Feron, F. J., de Vries, M. W., & van Os, J. (2007). Mood in daily contexts: relationship with risk for early adolescence. Journal of Research on Adolescence, 17, 697–722.
Sheeber, L., Hops, H., & Davis, B. (2001). Family processes in adolescent depression. Clinical Child and Family Psychology Review, 4, 19–35.
Sheeber, L. B., Davis, B., Leve, C., Hops, H., & Tildesley, E. (2007). Adolescents’ relationships with their mothers and fathers: associations with depressive disorder and subdiagnostic symptomatology. Journal of Abnormal Psychology, 116, 144–154. doi:10.1037/0021-843X.116.1.144.
Shrout, P. E., & Bolger, N. (2002). Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychological Methods, 7(4), 422–445.
Sim, H. (2000). Relationship of daily hassles and social support to depression and antisocial behavior among early adolescents. Journal of Youth and Adolescence, 29, 647–659.
Stadler, C., Feifel, J., Rohrmann, S., Vermeiren, R., & Poustka, F. (2010). Peer-victimization and mental health problems in adolescents: are parental and school support protective? Child Psychiatry and Human Development, 41, 371–386.
Stice, E., Ragan, J., & Randall, P. (2004). Prospective relations between social support and depression: differential direction of effects for parent and peer support? Journal of Abnormal Psychology, 113, 155–159.
Storch, E. A., & Ledley, D. R. (2005). Peer victimization and psychosocial adjustment in children: current knowledge and future directions. Clinical Pediatrics, 44, 29–38.
Sweeting, H., Young, R., West, P., & Der, G. (2006). Peer victimization and depression in early-mid adolescence: a longitudinal study. British Journal of Educational Psychology, 76, 577–594.
Tracy, M., Zimmerman, F. J., Galea, S., McCauley, E., & Vander Stoep, A. (2008). What explains the relation between family poverty and childhood depressive symptoms? Journal of Psychiatric Research, 42, 1163–1175.
Tram, J. M., & Cole, D. A. (2006). A multimethod examination of the stability of depressive symptoms in childhood and adolescence. Journal of Abnormal Psychology, 115, 674–686.
Twenge, J. M., & Nolen-Hoeksema, S. (2002). Age, gender, race, socioeconomic status, and birth cohort differences on the children’s depression inventory: a meta-analysis. Journal of Abnormal Psychology, 111, 578–588.
Vitaro, F., Brendgen, M., & Tremblay, R. E. (2002). Reactively and proactively aggressive children: antecedent and subsequent characteristics. Journal of Child Psychology and Psychiatry, 43, 495–505.
Watson, D., & Clark, L. A. (1992). On traits and temperament: general and specific factors of emotional experience and their relation to the five-factor model. Journal of Personality, 60, 441–476.
Conflict of Interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
This research was supported by a grant from the National Institute of Mental Health (RO1-MH59670, to Roger Kobak).
Rights and permissions
About this article

Cite this article
Herres, J., Kobak, R. The Role of Parent, Teacher, and Peer Events in Maintaining Depressive Symptoms during Early Adolescence. J Abnorm Child Psychol 43, 325–337 (2015). https://doi.org/10.1007/s10802-014-9896-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-014-9896-3