
Abstract
The purpose of the current study was to test the ability of adolescents and young adults with childhood ADHD to reliably self-report delinquency history. Data were examined from the Pittsburgh ADHD Longitudinal Study (PALS), a follow-up study of children diagnosed with ADHD between 1987 and 1996. Self-report of lifetime delinquency history was compared to concurrent parent-report and to self-report 1 year later. Participants included 313 male probands and 209 demographically similar comparison individuals without ADHD. Results indicated that adolescents and young adults with childhood ADHD were more likely than comparison participants to fail to report delinquent acts reported by a parent and to recant acts they endorsed 1 year earlier. This trend was most apparent for acts of mild to moderate severity. After controlling for several covariates, current ADHD symptom severity and parent-report of the participant’s tendency to lie predicted reporting fewer delinquent acts than one’s parent. Current ADHD symptom severity also predicted more recanting of previously endorsed acts. Based on these findings, several recommendations are made for the assessment of delinquency history in adolescents and young adults with childhood ADHD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Contemporary research on juvenile delinquency typically relies on self-report of offending as the primary measure of delinquency in youth (Loeber et al. 1998; Patterson and Yoerger 1993). This tradition stems from work suggesting that self-report of delinquency is the most valid single source of delinquency history. Official court records provide an objective account of juvenile offending. However, self-report typically identifies significantly more delinquent acts than official records (Kirk 2006). For example, Farrington et al. (2007) found that in a large sample of delinquent adolescents, there were 80 self-reported offenses for every court petitioned offense. Another alternative to self-report is adult informant reporting. One limitation of this approach is that in adolescence, youth spend a decreasing amount of time in the presence of parents and teachers (the most readily available adult informants). As a result, their reports may contain high rates of false negatives and provide an incomplete picture of offending. Delinquency self-report, by contrast, provides more information than any other source and in most cases, possesses adequate test-retest reliability, content validity, and criterion validity (Huizinga and Elliot 1986).
Despite the general conclusion in the antisocial behavior literature that self-report is the most informative source for delinquency history, this approach possesses several noteworthy limitations, even under conditions of assured confidentiality. First, without a gold standard for comparison, it is not possible to assess the validity of self-reported crimes. This is especially true of acts not listed on criminal records or corroborated by an informant. Second, under-reporting of crimes invariably occurs (Huizinga and Elliot 1986), and more frequently in certain groups (Farrington et al. 1996; Hindelang et al. 1981). For example, as most delinquency self-report measures were developed for use with late adolescent males, their items do not adequately assess delinquent acts that are more common in certain sub-populations (Piquero et al. 2002). Also, certain groups may be more likely to misunderstand questionnaires or feel uneasy revealing information.
Individuals with ADHD may be one group at high risk for providing problematic self-report of delinquent behavior. Because delinquent offending is highly prevalent in the ADHD population, delinquency history is an important area of assessment in these individuals (Loeber et al. 2000; Molina et al. 2007a). Whether adolescents and young adults with ADHD are at a higher risk for under-reporting delinquent acts is not yet known. However, a study by Watkins and Melde (2007) provides some evidence that adolescents who are highly impulsive are at a greater risk for under-reporting delinquency. Specifically, in a large middle school sample, the authors reported a significant association between self-report of impulsivity/risk taking and the number of items left unanswered on a delinquency self-report questionnaire. Because low self-control and impulsivity are hallmark symptoms of the ADHD profile (Barkley 2006), it is possible that this finding generalizes to the ADHD population.
In addition to the Watkins and Melde (2007) finding, literature on the assessment of adolescents and young adults with ADHD suggests that this population lacks insight into their own behavior and consequently, often underestimates their symptomatology (Barkley 2006; Wolraich et al. 2005). There are many published studies that explore the inaccuracies of self-report in ADHD samples, though most were conducted with children (for review see Owens et al. 2007). For example, in a study by Loeber et al. (1991a), children with disruptive behavior disorders self-reported significantly lower levels of ADHD symptoms than their parents and teachers. This effect was not present in non-externalizing control participants. In the same study, adult informant reports of ADHD symptoms were more highly correlated with academic outcomes than child reports of ADHD symptoms. These findings suggest that children with ADHD are less valid reporters of symptomatology because they tend to under-report their symptoms (Loeber et al. 1991a, b). Similar findings emerged in several studies of adolescents and young adults with ADHD, suggesting that self-report of externalizing symptoms continues to be problematic in older samples (Barkley et al. 2002; Fischer et al. 1993; for review see Willoughby 2003). This pattern of symptom under-reporting is considered a characteristic self-perception bias possessed by many individuals with ADHD (Owens et al. 2007).
It is important to note that studies of reporting biases in the ADHD population primarily examine domains that require some degree of self-awareness (i.e., ADHD symptoms, functional impairment). The accuracy of these more subjective self-evaluations may differ from reports about factually based material, such as GPA, driving history, and arguably, many delinquent behaviors. For example, some evidence suggests that children and adolescents provide more accurate self-report of Conduct Disorder (CD) symptoms than ADHD symptoms (Hartung et al. 2005; Loeber et al. 1989). Although it should be noted that in clinical populations, children still report conduct problems at lower rates than adult informants (Hart et al. 1994; Rubio-Stipec et al. 2003). The symptoms of CD (e.g., initiating physical fights, lying, stealing) are arguably less subjective than the symptoms of ADHD (e.g., difficulty organizing tasks, difficulty awaiting turn, easily distracted). Thus, it is not clear whether the problematic self-report found in subjective domains is indicative of pervasive self-reporting problems that reach into less subjective areas, such as delinquency.
In addition to biased self perceptions, several other factors also suggest that adolescents and young adults with a history of ADHD may be less accurate reporters of delinquency. Huizinga and Elliot (1986) identified several factors that may lead to delinquency under-reporting. These include several factors that may be associated with ADHD such as deliberate falsification, forgetting events of low salience, difficulty understanding the questionnaire, and social desirability. For example, forgetfulness and carelessness are common symptoms of ADHD and may lead an individual to improperly read instructions or forget acts that were committed (American Psychiatric Association 2000). Additionally, many measures of delinquency are formatted in such a way that respondents “skip out” of sometimes lengthy follow-up questions by failing to endorse an act (Elliot et al. 1985; Shaffer et al. 2000). As a result, highly impulsive individuals with ADHD may choose to deny an act in order to complete the measure more quickly. CD, which includes lying as a symptom, is highly comorbid with ADHD (Barkley 2006). One hypothesis contends that deliberate falsification might occur in an effort to conceal more severe or socially reprehensible acts. These examples differ in their specifics but have the same implication—symptoms of ADHD and related disorders may result in problems with self-report of delinquency.
Given the questionable accuracy of self-report in ADHD samples (Pelham et al. 2005; Wolraich et al. 2005), studies of delinquency in ADHD youth typically rely upon combined parent and self-report of delinquency (Lee and Hinshaw 2004; Molina et al. 2007a). This approach is consistent with the recommendation by Farrington and colleagues (1996), who found that combined self, parent, and teacher report of offending in a highly delinquent sample showed greater convergent validity with court records than self-report alone. While this study was not conducted with an ADHD sample, its findings suggest that in samples that are at risk for problematic self-report, there may be incremental benefit in combining reports of offending. Still undetermined, however, is whether delinquency self-report problems occur more frequently in ADHD samples, and if so, what accounts for these inconsistencies.
To investigate these unanswered questions, this study addressed several aims using data from the Pittsburgh ADHD Longitudinal Study (PALS; Molina et al. 2007b). The PALS is a large follow-up study of children who were diagnosed with ADHD in their elementary school years and who were recontacted for follow-up in adolescence and young adulthood. PALS probands were compared to a demographically similar group of adolescents and young adults without ADHD who were recruited at the start of the follow-up study. We hypothesized that adolescents and young adults with ADHD would be more likely than comparison participants to 1) report less severe delinquency overall than parents and 2) report a lower frequency of delinquent acts than parents. We also compared self-report of lifetime delinquency to self-report of lifetime delinquency 1 year later. We hypothesized that adolescents and young adults with ADHD would be more likely than comparison participants to 1) report less severe lifetime delinquency 1 year later and 2) recant more acts 1 year later. Finally, we conducted an exploratory investigation into factors that contributed to self-report problems in the PALS sample.
Method
Participants
Probands
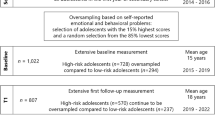
At the start of the follow-up study, 303 male probands were recruited from a pool of 466 study-eligible males previously diagnosed with DSM-III-R or DSM-IV ADHD and treated at the ADD clinic at the Western Psychiatric Institute and Clinic in Pittsburgh, PA from 1987 to 1996 (baseline). Of the 466 study eligible males, 23 could not be located at follow-up and 129 refused or failed to participate. Age at baseline evaluation ranged from 5.0 to 16.83 years (M = 8.92, SD = 1.79). (Females, who were relatively small in number in the PALS, are excluded from the current study).
All probands participated in the Summer Treatment Program (STP) for children with ADHD, an 8-week intervention that included behavioral modification, parent training, and psychoactive medication trials where indicated (Pelham and Hoza 1996). Diagnostic information for the probands was collected at initial referral to the clinic in childhood (baseline) using parent and teacher DSM-III-R and DSM-IV symptom ratings scales (DBD; Pelham et al. 1992a) and a semi-structured diagnostic interview administered to parents by a Ph.D. level clinician. The interview consisted of the DSM-III-R or DSM-IV descriptors for ADHD, ODD, and CD with supplemental probe questions regarding situational and severity factors. It also included queries about other comorbidities to determine whether additional assessment was needed. Following DSM guidelines, diagnoses of ADHD, ODD, and CD were made if a sufficient number of symptoms were endorsed (considering information from both parents and teachers) to result in diagnosis. Two Ph.D. level clinicians independently reviewed all ratings and interviews to confirm DSM diagnoses and when disagreement occurred, a third clinician reviewed the file and the majority decision was used. Exclusion criteria for probands was assessed in childhood (baseline) and included a full-scale IQ < 80, a history of seizures, neurological problems, pervasive developmental disorder, schizophrenia, and/or other psychotic or organic mental disorders.
Probands were recruited for their first follow-up PALS interview as adolescents or as young adults (11–28 years of age; all but three were 25 or younger). Probands were admitted to the follow-up study on a rolling basis between the years 1999–2003 and completed their first follow-up interview immediately upon enrollment. At the time of the first follow-up interview, an average of 8.35 (SD = 2.79) years had elapsed since the probands’ baseline assessment at the ADD clinic. Participants were compared with eligible individuals who did not enroll in the follow-up study on demographic and diagnostic variables collected at baseline. Only one of 14 comparisons was statistically significant at the p < 0.05 significance level. Participants had a slightly lower average CD symptom rating on a four point scale as indicated by a composite of parent and teacher ratings (participants M = 0.43, non-participants M = 0.53).
Comparison Group
Comparison participants were 209 males without ADHD. Comparison participants were recruited for the PALS from the greater Pittsburgh community between 1999 and 2001. These individuals were recruited from several sources including pediatric practices in Allegheny County (40.8%), advertisements in local newspapers (27.5%), local universities and colleges (20.8%), and other methods (10.9%) such as Pittsburgh Public Schools and word of mouth. Like probands, comparison participants were recruited on a rolling basis. Comparison recruitment lagged 3 months behind proband enrollment in order to facilitate efforts to obtain demographic similarity (discussed below). A telephone screening was administered to parents of potential comparison participants to gather basic demographic characteristics, history of diagnosis or treatment for ADHD and other behavior problems, presence of exclusionary criteria as previously listed for probands, and a checklist of ADHD symptoms. Young adults (age 18+) also provided self-report. ADHD symptoms were counted as present if reported by either the parent or by the young adult. Individuals who met DSM-III-R criteria for ADHD, currently or historically, were immediately excluded from the study.
If a potential comparison participant passed the initial phone screen, senior research staff members met to determine whether he was demographically appropriate for the study. Each potential comparison participant was examined with regard to four demographic characteristics: 1) age, 2) gender, 3) race, and 4) parent education level. A comparison participant was deemed study-eligible if his enrollment increased the comparison group’s demographic similarity to the probands. At the end of the recruitment process, the proband and comparison groups were equivalent on the four demographic variables noted above (see Table 1).
Procedure
Follow-up interviews in adolescence and in young adulthood were conducted by post-baccalaureate research staff. All questionnaires (paper or web-based) in the current study were completed privately by participants and parents during the second and third yearly follow-up interviews. During informed consent, all participants were assured of the confidentiality of disclosed materials. In cases where distance prevented participant travel to WPIC, information was collected through a combination of mail, telephone correspondence, and home visits. Participants were permitted to take stimulant medication on the day of the assessment; however a minority of probands (<10%) were currently prescribed stimulant medication during the follow-up years. Age at the second follow-up interview ranged from 12 to 29 years (proband M = 18.68, SD = 3.41; comparison M = 17.97, SD = 3.16).
Measures
Delinquency
Delinquency data were collected with the Self-Reported Delinquency Questionnaire (SRD; Elliott et al. 1985) administered to each participant and his parent(s) during follow-up interviews 2 and 3 (this questionnaire was not administered at the first follow-up interview). Research on the SRD in general populations suggests that the measure possesses adequate validity and test-retest reliability (Huizinga and Elliot 1986). However, these hypotheses have not been tested with an ADHD sample. Participants and their parents were asked whether or not the participant had ever committed 37 delinquent acts (e.g., Have you ever snatched someone’s purse or wallet?). If the act was endorsed, the respondent answered additional follow-up questions, including age at which the act first occurred (e.g., How old were you when you first snatched someone’s purse or wallet?), the setting in which the act was committed (e.g., Did any of these occur at school?), and the value of any damages that resulted (e.g., What was the dollar value?). As a result, participants who denied committing an act skipped answering these follow-up questions. For the purpose of comparison, the sum of acts (out of 37) endorsed in a lifetime was calculated separately for self-report and for parent-report.
Because behavior counts may obscure the severity of behavior (e.g., two occurrences of theft is less severe than a single instance of rape), lifetime severity ratings were coded according to the scheme developed by Wolfgang et al. (1985) and used in the Pittsburgh Youth Study (Loeber et al. 1991b). Severity was coded based on the most serious act a participant or parent reported in the lifetime: 0 = no delinquency; 1 = minor delinquency only at home (e.g., theft of less than $5 or vandalism); 2 = minor delinquency outside the home (e.g., vandalism, cheating someone, shoplifting less than $5); 3 = moderate delinquency (e.g., vandalism, theft of $5 or more, major arson); 4 = serious delinquency (e.g., breaking and entering, attacking someone with the intent to seriously hurt or kill, rape); and 5 = engagement in two or more different level 4 offenses. Because only a small number of youth were coded with only minor delinquency in the home (N = 16), we grouped codes 0 and 1 for data analyses, making a five-level ordinal scale of 1–5.
ADHD Symptom Severity
For participants under the age of 18, ADHD symptom severity was measured at recruitment for the first follow-up interview using the Disruptive Behavior Disorders Rating Scale (DBD; Pelham et al. 1992b). The DBD lists the DSM-III-R and DSM-IV symptoms of ADHD, Oppositional Defiant Disorder (ODD), and CD. Parents and teachers were asked to provide ratings of (0) not at all, (1) just a little, (2) pretty much, or (3) very much for each symptom of ADHD, ODD, and CD. The psychometric properties of the DBD rating scale are very good, with empirical support for distinguishing inattention, hyperactivity/impulsivity, ODD, and CD factors, and internally consistent subscales with alphas above 0.95 (Pelham et al. 1992a, b; Pillow et al. 1998; Wright et al. 2007). ADHD severity scores were obtained by summing the highest ratings for each DSM-IV ADHD symptom reported by parent or teacher and dividing that sum by 18 (total number of ADHD symptoms).
For participants 18 or older, ADHD symptom severity was measured using an unpublished measure (used by permission from R. Barkley). This measure includes items assessing the core symptoms of ADHD in a number of adult-related settings using age appropriate behaviors and wording. Only the items assessing DSM-IV symptoms for ADHD were used in these analyses. Comparable to the DBD, the scores on the adult ADHD scale ranged from 0–3, (0) not at all, (1) just a little, (2) pretty much, or (3) very much. Parents and participants completed this measure and ADHD symptom severity scores were calculated as they were for adolescents. The higher of self or parent rating was utilized as has been done customarily with this sample (Molina et al. 2007b, Wymbs et al. 2008).
Untruthfulness
The measure of untruthfulness used in the current study was the Untruthfulness subscale of the Childhood Psychopathy Scale (CPS; Lynam 1997). The CPS was administered to parents of participants at the first follow-up interview. This 41-item scale assesses various dimensions of psychopathy and is highly reliable (Lynam 1997). Parents indicated the applicability of each item to his/her son using a four point scale that ranged from 1-“never/rarely” to 4-“very often.” The three item Untruthfulness subscale (“Is he open and straightforward?” “Can he be trusted?” “Is he a good liar?”) assessed a participant’s current level of untruthfulness. In the PALS sample, internal reliability for this subscale was acceptable for responses given both by parents of adolescents (0.75) and by parents of young adults (0.82).
Analytic Plan
Differences Between Self and Parent-Report
Because its clinical significance made delinquency severity a variable of principal interest, we began our analyses by exploring agreement between self and parent-report of delinquency severity. For the purposes of this study, agreement was coded into three levels based on whether parent-report indicated more severe lifetime delinquency than self-report (under-reporting), parent and self-report indicated the same severity rating (agreement), or self-report indicated more severe lifetime delinquency than parent-report (parent reports less). To test this question, a 2 (group: ADHD vs. comparison) x 3 (agreement: under-reporting, agreement, parent reports less) Pearson’s chi-square analysis was used with group and agreement of delinquency severity as factors. Agreement between parent and self-report was also examined by comparing group differences for the frequency of acts under-reported (out of 37). For this analysis, we used a nonparametric Mann-Whitney U test (Hollander and Wolfe 1999) given the positively skewed distribution of this variable.
Recanting Previously Reported Delinquency
To establish whether or not participants responded consistently across multiple assessments, we examined the percentage of participants whose responses during follow-up interview 3 indicated less severe lifetime delinquency than indicated by their responses during follow-up interview 2. This index was chosen due to our inability to distinguish newly endorsed acts that were committed between the second and third annual interviews from newly endorsed acts that were not reported at the second annual interview. Participants were coded according to whether or not their lifetime severity rating decreased (0 = no, 1 = yes) and a 2 (group: ADHD vs. comparison) x 2 (severity decrease: yes vs. no). Pearson’s chi-square analysis was used to examine these rates by group. To further explore inconsistent reporting in our sample, the total number of items recanted by a participant was calculated and group differences on this variable were examined using a nonparametric Mann-Whitney U test, because of the positively skewed distribution of this variable.
Item-Level Analyses
We explored items that contributed most to self-reporting problems in order to generate hypotheses about factors contributing to under-reporting and recanting acts. Of the 37 items evaluated in the previous analyses, 14 (37.8%) almost never occurred (endorsed by less than 5% of the sample) and therefore were excluded from the item-level analyses. The remaining 23 items were examined using a series of 2 (group: ADHD vs. comparison) x 2 (consistent: yes vs. no) Pearson’s chi square tests to investigate the propensity for individuals within each group to under-report and recant each separate item. A Bonferroni adjustment was made given the large number of tests (α = 0.002).
Predictors of Self-Report Inconsistencies
Using two multiple regression models, we examined whether ADHD symptom severity and untruthfulness predicted two dependent variables: 1) the number of items a participant under-reported (out of 37) when compared to parent-report and 2) the number of items (out of 37) that were endorsed during follow-up interview 2 and recanted during follow-up interview 3. In these analyses, we used age as a covariate because participants represented a wide age range at follow-up. We also included the total number of delinquent acts endorsed during follow-up interview 2 as a covariate to account for the unavoidable fact that participants committing more delinquent acts have greater opportunities for problematic reporting.
Results
Differences Between Self and Parent-Report
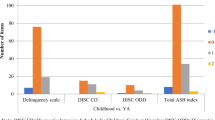
Rates of agreement for delinquency severity obtained via self—versus parent-report differed significantly for probands and controls [Χ 2(2) = 13.74, p < 0.01]. Specifically, probands under-reported the severity of their delinquent activity at higher rates (25.0%) than comparison participants (12.0%, OR = 2.40). Comparison participants (43.3%) were slightly more likely than probands (33.8%, OR = 1.49) to report delinquency that was more severe than that reported by parents (see Fig. 1). Follow-up analyses revealed that most proband under-reporting occurred when self-report indicated no delinquency and parent-report indicated that either mild, moderate, or severe delinquency was present (see Table 2). As expected, data in Table 2 also revealed that a number of probands reported moderate or severe delinquency that went unreported by their parents. Comparison of self and parent-report indicated that probands (Median = 1.00, Range = 0–12, Interquartile Range = 2.50) under-reported significantly more total items than comparison participants (Median = 0.00, Range = 0–15, Interquartile Range = 1.00, U = 21581.00, p < 0.01).

Parent-participant agreement for delinquency severity
Recanting Previously Reported Delinquency
More probands (26.1%) than comparison participants (18.6%) indicated less severe lifetime delinquency at the third follow-up interview than at the second follow-up interview [Χ 2(1) = 3.70, p = 0.06, OR = 1.54]. Probands recanted significantly more acts (Median = 1.00, Range = 0–26, Interquartile Range = 3.00) than comparison participants (Median = 0.00, Range = 0–10, Interquartile Range = 2.00, U = 18132.00, p < 0.01).
Item-Level Analyses
Probands under-reported 4 of the 23 acts at significantly greater rates than comparison participants (p < 0.002) and recanted 4 of 23 acts at significantly greater rates than comparison participants (p < 0.002). Across items, rates of under-reporting ranged from 1.0% to 17.3% in probands and from 0% to 7.7% in comparison participants (see Table 3). Odds ratios indicated that for the four acts with differential rates of under-reporting, probands were 3.62–6.22 times more likely than comparison participants to under-report. Rates of recanting ranged from 2.7% to 18.0% in probands and from 0.5% to 13.3% in comparison participants (see Table 3). Odds ratios indicated that on the four acts with statistically significant group differences, probands were 9.17–11.68 times more likely than comparison participants to recant an item.
Predictors of Self-Report Inconsistencies
The data met all assumptions of multiple regression prior to the analyses (Tabachnick and Fidell 2001). For the prediction of under-reporting compared to parents, the equation was significant [R 2 = 0.20, F(4,497) = 31.49, p < 0.01] and total number of delinquent acts endorsed, untruthfulness, and ADHD symptom severity each uniquely contributed to the prediction (see Table 4). For the prediction of inconsistent reporting across assessments, the equation was also significant [R 2 = 0.24, F(4,421) = 33.13, p < 0.01] and number of delinquent acts endorsed, age at follow-up, and ADHD symptom severity uniquely contributed to the prediction (see Table 5).
Discussion
The purpose of this study was to investigate whether individuals with ADHD are at a higher risk for under-reporting or inconsistently reporting delinquent behaviors and to identify potential contributors to this risk. Several findings emerged. When comparing self-report to parent-report, adolescents and young adults with ADHD were more likely than comparison participants to: 1) report less severe delinquency and 2) report fewer delinquent acts. Regarding inconsistent reporting over time, adolescents and young adults with ADHD were more likely to: 1) rate themselves as less severe offenders than they had a year prior and 2) report lifetime engagement in fewer delinquent acts than they reported a year prior. When investigating contributors to the above noted trends, we found that 1) at the item-level, several acts were specifically problematic for probands, 2) current ADHD symptom severity and parent ratings of untruthfulness predicted the number of acts a participant under-reported and 3) ADHD symptom severity uniquely predicted recanting an act at follow-up interview 3, but untruthfulness did not. Each of these findings is discussed below.
Adolescents and young adults with ADHD were over twice as likely as comparison participants to under-report the severity of their delinquency as compared to parent-report. This finding is particularly concerning as 1) severity classification is a clinically meaningful index and 2) self-report is currently the gold standard in delinquency assessment (Farrington et al. 2007). Using self-report alone, a quarter of adolescents and young adults with ADHD were classified at a delinquency severity level that was lower than parent-report suggested. Given the likelihood that some under-reported delinquent acts occurred unbeknownst to parents (Farrington et al. 1996), this number is probably an underestimate. In most cases of under-reporting (see Table 2), probands reported no lifetime delinquency while parents reported a history of mild, moderate, or even severe delinquent offending. These results suggest that for a subset of young individuals with ADHD, under-reporting resembles outright denial of what, in some cases, is observable moderate or severe delinquent offending. It is important to note that severely offending youth also under-reported minor offenses. However, this under-reporting did not affect the coding of their severity level. Therefore, while our estimate of under-reporting reflects under-reporting at a clinically meaningful level, it is a low estimate of total under-reporting.
To assess inconsistencies in self-report over time, we examined group differences in the tendency to report a lower lifetime severity level than previously reported 1 year earlier. Twenty-six percent of probands and approximately 19% of comparison participants reported less severe lifetime delinquency at follow-up interview 3 than previously reported a year prior. This finding indicates a slightly higher rate of inconsistent responding in the ADHD group. While we know of no study that examines the consistency of severity codes using the method employed in the current study, Huizinga and Elliot (1986) found that approximately 25% of their sample denied at least one previously endorsed delinquent act (as evaluated using the SRD) at 4 weeks follow-up. Although the overall rate of change is similar across our study and the previous one, there were several important methodological differences between the two studies. Our study used a 1 year test-retest period whereas Huizinga and Elliot used 4 weeks. In addition, we evaluated rates of reduced delinquency severity, whereas Huizanga and Elliot evaluated rates of reduced endorsement of any delinquency. As a result, the apparent similarity between the consistency estimates in these two studies may be spurious; had Huizinga and Elliot reported only clinically significant changes, as we did, their estimate would have likely fallen.
To explore potential explanations for the inconsistent reporting detected in the ADHD group, we examined which acts were under-reported and recanted at higher rates in probands than in comparison individuals. Our analyses suggested that specifically problematic items were generally mild to moderate in severity (i.e., skipped class, vandalism, rowdy in public). These items also contain subjective content, suggesting that reporter discrepancies may have stemmed from differential interpretation of these items’ meanings. For example, the wording of many of these items require the respondent to make a subjective judgment about the crime (e.g., “under false pretenses,” “without an excuse,” “with the intent to seriously injure”). It is worth noting that there were some items that displayed high rates of discrepant reporting in both the ADHD and comparison groups, but did not possess significant group differences (i.e. hitting to injure, lying about one’s age, several indices of theft). These items also contained somewhat subjective content. This finding is compatible with findings from the National Youth Study (Huizinga and Elliot 1986) that suggests a high rate of false positives on similar items (i.e., assault, vandalism). It is also consistent with self-perception theory in that individuals with ADHD were most likely to show reporting inconsistencies on items that were somewhat subjective (Owens et al. 2007). Thus, a mother may report that her son has “purposefully” vandalized property because he became angry and broke a chair; however, the participant may not have endorsed this item because he did not feel that such outbursts reflected intentional vandalism.
Several other studies also show that agreement between self-report and official records is lower for milder offenses than for severe ones (Kazemian and Farrington 2005). On the other hand, it is also possible that participant under-reporting on more severe acts was more likely to go undetected due to false negatives reported by parents. For example, severe acts may have occurred unbeknownst to parents or parents may have failed to report severe acts for social desirability reasons. Although self-perception theory would implicate individuals with ADHD as the problematic reporter (Owens et al. 2007), it is also possible that reporting errors made by parents contribute to inconsistencies on subjectively worded items, as well. For example, De Los Reyes and Kazdin (2005) suggest that these discrepancies can stem from cognitive biases possessed by both the participant and the parent (i.e., attributional errors, biased schema-driven memories).
To further explore potential explanations for the inconsistent reporting detected in the ADHD group, we examined the predictive ability of two hypothesized contributors to self-report inaccuracies (untruthfulness and ADHD severity). Interestingly, both behaviors showed evidence of contributing to the prediction of under-reporting as compared to parent-report, even after controlling for the respondent’s age and the number of delinquent acts they endorsed. These findings are consistent with the hypothesis that under-reporting of delinquency may stem from traits associated with ADHD, such as inattention and impulsivity, and the hypothesis that untruthfulness may also contribute to invalid self-report. Additionally, after accounting for the same set of covariates, ADHD symptom severity predicted recanting previously reported delinquent acts, but untruthfulness did not. This finding suggests that ADHD-specific deficits may contribute to the trend of inconsistent reporting across time in the ADHD sample. One must note, however, that it is possible that adolescents and young adults who were untruthful during the second follow-up interview were also untruthful during the third follow-up interview. Thus, repeated under-reporitng is a possible explanation for the non-significance of untruthfulness in this prediction. Age at follow-up was also significant in this equation, indicating that older individuals were more likely to respond inconsistently across time than younger individuals.
Taken together, the findings from this study suggest that delinquency reporting problems in ADHD samples may occur for both deliberate and non-deliberate reasons. Specifically, the association with ADHD symptom severity suggests that some participants denied delinquency because of cognitive limitations (i.e., forgetfulness or carelessness) or impulsivity/poor self-control (i.e., impatience—denying acts to shorten the assessment by skipping out of follow-up questions). The finding that subjectively worded items were especially problematic for ADHD individuals (see Table 3) also suggests that confusion or carelessness may contribute to non-deliberate reporting errors. However, the finding that untruthfulness was also associated with under-reporting suggests that some participants denied delinquency purposefully. Previous research on individuals with ADHD has focused on biased self-perceptions as the principle mechanism behind findings of invalid self-report. Our findings suggest that other factors (i.e., difficulty interpreting an item’s meaning, ADHD symptomatology, untruthfulness) may also contribute to self-report problems in this population, and should be given further attention.
Thus, although self-report is currently the gold standard in the assessment of delinquency, self-report may not be a sufficient source of information when assessing delinquency in adolescents and young adults with ADHD. After conducting our analyses, we estimated that almost half of probands (48.5%) made a clinically significant error in self-report (i.e., self-report indicated less severe delinquency than parent-report or self-report at follow-up interview 3 indicated less severe delinquency than a year prior). These meaningful reporting problems occurred in less than a third of comparison individuals (29.7%). Clearly, there is evidence for the value of self-report of delinquency in ADHD samples, as over half of probands did not display clinically significant problems with self-report and at least one-third of delinquent acts were detected only by self report (see Fig. 1). However, the findings of the current study indicate that combining parent and self-report provide complementary information, suggesting that when assessing delinquency in ADHD samples, data from both informants should be collected (see Fig. 1). Specifically, we recommend using “or” (i.e., aggregating information across informants) rather than “and” combination rules (i.e., examining each report individually). Although some argue that “or” rules may increase the possibility of false positives (Offord et al. 1996), these guidelines safeguard against the type of reporting errors that our results suggest are most likely to occur in the ADHD population (i.e., under-reporting and recanting). This recommendation is consistent with findings from the Pittsburgh Youth Study, which found that combined report possessed greater concurrent validity than self-report alone when compared to court records (Farrington et al. 1996). Our recommendation is also consistent with several studies from the diagnostic literature that suggest that combined report across several informants also provides the most stable estimate of disruptive behavior disorder symptom severity (Bird et al. 1992; Piacentini et al. 1992).
A number of other recommendations can be made based on the results of this study. When assessing delinquency history in an individual with ADHD, it may be advisable to use items with very precise or operationally defined language, as subjectively worded items led to self-reporting problems. Our findings suggest that carelessness or forgetfulness also might contribute to problems with delinquency self-report, and that older participants reported more inconsistently. Thus, it may be helpful to assess delinquency history in shorter intervals (than lifetime) and more frequently (than once a year). In some cases, it may be possible to provide rewards that are contingent upon the careful completion of questionnaires as incentives show evidence of improving cognitive performance in ADHD individuals (Shiels et al. 2008). Further work is needed to determine the utility of the suggestions noted above. Additionally, future research should address which reporter’s account of delinquency history is most predictive of future outcomes. For example, there is some evidence that under-reporting delinquency is predictive of poor outcomes (Ferdinand et al. 2004).
Our study possesses several limitations. First, there was no gold standard available against which to compare the reported delinquency histories, as is typically the case in studies of delinquency (Huizinga and Elliot 1986). Despite the well-documented rates of delinquency in the ADHD population (Molina et al. 2007a) and high correlations between parent-report of child problem behavior and objective measures of impairment (Loeber et al. 1991a, b), it is possible that in some cases, disagreement between participants and parents stemmed from invalid parent reporting. Furthermore, agreement between parents and participants may have stemmed from double under-reporting. Unfortunately, we were unable to examine these possibilities. We were also unable to separately examine the individual symptoms of ADHD (inattention, hyperactivity, and impulsivity) due to high collinearity among these variables. As a result, we did not attempt to pinpoint specific symptoms of ADHD that contribute to the risk of problematic reporting. Although we reported a significant association between untruthfulness and under-reporting in our prediction analyses, it is possible that this association was partially driven by an overlap between the constructs of untruthfulness and under-reporting, both of which relied on parent report. Additionally, probands in the current study were recruited from a clinical population, making it conceivable that the high level of under-reporting found in this sample may not be present in the entire ADHD population (Barker et al. 2007). While our sample was representative of the county in which the study occurred, many of our participants came from middle-class families. As a result, our findings may not extend to exclusively low income or high income samples. Finally, the inclusion of only males in these analyses limits the generalizability of the findings to male populations.
Despite these limitations, we believe that our study offers evidence that due to deficits associated with the ADHD profile, a subset of adolescents and young adults with ADHD display delinquency self-report problems at clinically significant or sub-clinical levels. It appears that inconsistencies in reporting that are specific to an ADHD-related deficit are a pervasive source of assessment error in this population. Thus, it is possible that adolescents and young adults with ADHD will also show problematic reporting in other less subjective domains of interest such as substance dependence, driving skill, or work performance. To safeguard against this possibility, we recommend that clinicians and researchers consider the findings and recommendations in this paper when assessing any domain of functioning in adolescents and young adults with ADHD.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed-TR). Washington, DC: Author.
Barker, E., Bornstein, M., Putnick, D., Hendricks, C., & Suwalsky, J. (2007). Adolescent-mother agreement about adolescent problem behaviors: direction and predictors of disagreement. Journal of Youth and Adolescence, 36, 950–962.
Barkley, R. (2006). Attention-deficit hyperactivity disorder, 3rd ed.: A handbook for diagnosis and treatment. New York: Guilford.
Barkley, R., Fischer, M., Smallish, L., & Fletcher, K. (2002). The persistence of attention deficit hyperactivity disorder into young adulthood as a function of reporting source and definition of disorder. Journal of Abnormal Psychology, 111, 279–289.
Bird, H., Gould, M., & Staghezza, B. (1992). Aggregating data from multiple informants in child psychiatry epidemiological research. Journal of the American Academy of Child & Adolescent Psychiatry, 31, 78–85.
De Los Reyes, A. E., & Kazdin, A. (2005). Informant discrepancies in the assessment of childhood psychopathology: a critical review, theoretical framework, and recommendations for further study. Psychological Bulletin, 131, 483–509.
Elliot, D. Z., Huizinga, D., & Ageton, S. S. (1985). Explaining delinquency and drug use. Beverley Hills: Sage.
Farrington, D. P., Loeber, R., Stouthamer-Loeber, M., Van Kammen, W. B., & Schmidt, L. (1996). Self-reported delinquency and combined delinquency seriousness scale based on boys, mothers, and teachers: concurrent and predictive validity for African-Americans and Caucasians. Criminology, 34, 493–517.
Farrington, D. P., Jolliffe, D., Loeber, R., & Homish, D. L. (2007). How many offenses are really committed per juvenile court offender? Victims and Offenders, 2(3), 227–249.
Ferdinand, R., van der Ende, J., & Verhulst, F. (2004). Parent-adolescent disagreement regarding psychopathology in adolescents from the general population as a risk factor for adverse outcome. Journal of Abnormal Psychology, 113, 198–206.
Fischer, M., Barkley, R., Fletcher, K., & Smallish, L. (1993). The stability of dimensions of behavior in ADHD and normal children over an 8-year followup. Journal of Abnormal Child Psychology, 21, 315–337.
Hart, E., Lahey, B., Loeber, R., & Hanson, K. (1994). Criterion validity of informants in the diagnosis of disruptive behavior disorders in children: a preliminary study. Journal of Consulting and Clinical Psychology, 62, 410–414.
Hartung, C., McCarthy, D., Milich, R., & Martin, C. (2005). Parent-adolescent agreement on disruptive behavior symptoms: a multitrait-multimethod model. Journal of Psychopathology and Behavioral Assessment, 27, 159–168.
Hindelang, M. J., Hirschi, T., & Weis, J. G. (1981). Measuring delinquency. Beverly Hills: Sage.
Hollander, B., & Wolfe, D. (1999). Nonparametric statistical methods (2nd ed.). New York: John Wiley & Sons.
Huizinga, D., & Elliot, D. S. (1986). Reassessing the reliability and validity of self-report delinquent measures. Journal of Quantitative Criminology, 2, 293–327.
Kazemian, L., & Farrington, D. P. (2005). Comparing the validity of prospective, retrospective, and official onset for different offending categories. Journal of Quantitative Criminology, 21(2), 127–147.
Kirk, D. (2006). Examining the divergence across self-report and official data sources on inferences about the adolescent life-course of crime. Journal of Quantitative Criminology, 22, 107–129.
Lee, S. S., & Hinshaw, S. P. (2004). Severity of adolescent delinquency among boys with and without attention deficit hyperactivity disorder: prediction from early antisocial behavior and peer status. Journal of Clinical Child and Adolescent Psychology, 33(4), 705–716.
Loeber, R., Green, S., Lahey, B., & Stouthamer-Loeber, M. (1989). Optimal informants on childhood disruptive behaviors. Development and Psychopathology, 1, 317–337.
Loeber, R., Green, S., Lahey, B., & Stouthamer-Loeber, M. (1991a). Differences and similarities between children, mothers, and teachers as informants on disruptive child behavior. Journal of Abnormal Child Psychology, 19, 75–95.
Loeber, R., Stouthamer-Loeber, M., Van Kammen, W. B., & Farrington, D. P. (1991b). Initiation, escalation and desistance in juvenile offending and their correlates. Journal of Criminal Law and Criminology, 82, 36–82.
Loeber, R., Farrington, D. P., Stouthamer-Loeber, M., & Van Kammen, W. B. (1998). Antisocial behavior and mental health problems. New Jersey: Lawrence Earlbaum & Associates.
Loeber, R., Burke, J. D., Lahey, B. B., Winters, A., & Zera, M. (2000). Oppositional defiant and conduct disorder: a review of the past ten years, Part I. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 1468–1484.
Lynam, D. R. (1997). Pursuing the psychopath: capturing the fledgling psychopath in a nomological net. Journal of Abnormal Psychology, 106(3), 425–438.
Molina, B. S. G., Flory, K., Hinshaw, S. P., Greiner, A. R., Arnold, L. E., Swanson, J. M., et al. (2007a). Delinquent behavior and emerging substance use in the MTA at 36 months: prevalence, course, and treatment effects. Journal of the American Academy of Child and Adolescent Psychiatry, 46(8), 1028–1040.
Molina, B. S. G., Pelham, W. E., Gnagy, E. M., Thompson, A. L., & Marshal, M. P. (2007b). Attention-deficit/hyperactivity disorder risk for heavy drinking and alcohol use disorder is age specific. Alcoholism: Clinical and Experimental Research, 31(4), 643–654.
Offord, D. R., Boyle, M. H., Racine, Y., Szatmari, P., Fleming, J. E., Sanford, M., et al. (1996). Integrating assessment data from multiple informants. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 1078–1085.
Owens, J., Goldfine, M., Evangelista, N., Hoza, B., & Kaiser, N. (2007). A critical review of self-perceptions and the positive illusory bias in children with ADHD. Clinical Child and Family Psychology Review, 10, 335–351.
Patterson, G. R., & Yoerger, K. (1993). Developmental models for delinquent behavior. In S. Hodgins (Ed.), Mental disorder and crime. Newbury Park: Sage.
Pelham, W. E., & Hoza, B. (1996). Intensive treatment: A summer treatment program for children with ADHD. In E. D. Hibbs & P. S. Jensen (Eds.), Psychosocial treatments for child and adolescent disorders: Empirically based strategies for clinical practice. New York: American Psychological Association.
Pelham, W. E., Evans, S. W., Gnagy, E. M., & Greenslade, K. E. (1992a). Teacher ratings of DSM-III-R symptoms for the disruptive behavior disorders: prevalence, factor analyses, and conditional probabilities in a special education sample. School Psychology Review, 21(2), 285–299.
Pelham, W., Gnagy, E., Greenslade, K., & Milich, R. (1992b). Teacher ratings of DSM-III-R symptoms for the disruptive behavior disorders. Journal of the American Academy of Child & Adolescent Psychiatry, 31, 210–218.
Pelham, W. E., Fabiano, G. A., & Massetti, G. M. (2005). Evidence-based assessment of attention-deficit/hyperactivity disorder in children and adolescents. Journal of Clinical Child and Adolescent Psychology, 34, 449–476.
Piacentini, J., Cohen, P., & Cohen, J. (1992). Combining discrepant diagnostic information from multiple sources: are complex algorithms better than simple ones? Journal of Abnormal Child Psychology, 20, 51–63.
Pillow, D. R., Pelham, W. E., Hoza, B., Molina, B. S. G., & Stultz, C. H. (1998). Confirmatory factor analyses examining attention deficit hyperactivity disorder symptoms and other childhood disruptive behaviors. Journal of Abnormal Child Psychology, 26, 293–309.
Piquero, A., Macintosh, R., & Hickman, M. (2002). The validity of a self-reported delinquency scale: comparisons across gender, age, race, and place of residence. Sociological Methods & Research, 30, 492–529.
Rubio-Stipec, M., Fitzmaurice, G., Murphy, J., & Walker, A. (2003). The use of multiple informants in identifying the risk factors of depressive and disruptive disorders: are they interchangeable? Social Psychiatry and Psychiatric Epidemiology, 38, 51–58.
Shaffer, D., Fisher, P., Lucas, C. P., Dulcan, M., & Schwab-Stone, M. (2000). NIMH diagnostic interview schedule for children version IV (NIMH DISC-IV): description, differences from pervious versions, and reliability of some common diagnoses. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 28–38.
Shiels, K., Hawk, L., Lysczek, C., Tannock, R., Pelham, W., Spencer, S., et al. (2008). The effects of incentives on visual-spatial working memory in children with attention-deficit/hyperactivity disorder. Journal of Abnormal Child Psychology, 36, 903–913.
Tabachnick, B. G., & Fidell, L. S. (2001). Using multivariate statistics (4th ed.). Boston: Allyn and Bacon.
Watkins, A., & Melde, C. (2007). The effect of self-control on unit and item nonresponse in an adolescent sample. Journal of Research in Crime and Delinquency, 44, 267–294.
Willoughby, M. (2003). Developmental course of ADHD symptomatology during the transition from childhood to adolescence: a review with recommendations. Journal of Child Psychology and Psychiatry, 44, 88–106.
Wolfgang, M., Figlio, R. M., Tracey, P. E., & Singer, F. I. (1985). The national survey of crime severity. Washington, DC: U.S.
Wolraich, M. L., Wibbelsman, C. J., Brown, T. E., Evans, S. W., Gotlieb, E. M., Knight, J. R., et al. (2005). Attention-deficit/hyperactivity disorder among adolescents: a review of the diagnosis, treatment, and clinical implications. Pediatrics, 115(6), 1734–1746.
Wright, K. D., Waschbusch, D. A., & Frankland, B. W. (2007). Combining data from parent ratings and parent interview when assessing ADHD. Journal of Psychopathology and Behavioral Assessment, 29, 141–148.
Wymbs, B., Pelham, W., Molina, B., Gnagy, E., Wilson, T., & Greenhouse, J. (2008). Rate and predictors of divorce among parents of youths with ADHD. Journal of Consulting and Clinical Psychology, 76, 735–744.
Acknowledgement
This study was supported by grants DA12414, F31 DA017546 from the National Institute on Drug Abuse and additionally, AA11873 from the National Institute of Alcohol Abuse and Alcoholism. Research was also supported in part by AA00202, AA08746, AA12342, and grants from the National Institute on Mental Health (MH12010, MH4815, MH47390, MH45576, MH50467, MH53554, MH069614), the National Institute of Environmental Health Sciences (ES0515-08), and Institute of Education Sciences (IESLO3000665A, IESR324B060045).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sibley, M.H., Pelham, W.E., Molina, B.S.G. et al. Inconsistent Self-Report of Delinquency by Adolescents and Young Adults with ADHD. J Abnorm Child Psychol 38, 645–656 (2010). https://doi.org/10.1007/s10802-010-9404-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-010-9404-3