
Abstract
Purpose
The aim of this study was to compare the distance, intermediate, and near visual performance of a new IOL (ICB00, Eyhance, Tecnis) and classic monofocal IOL (SN60WF IQ AcrySof, Alcon) after unilateral implantation.
Methods
Sixty-three patients were unilaterally implanted with the ICB00 Eyhance IOL (study group) and 65 patients with the SN60WF IQ AcrySof (control group). Visual performance was assessed with monocular corrected distance visual acuity (CDVA) and uncorrected distance visual acuity (UDVA) at 4 m, corrected intermediate visual acuity (CIVA) and uncorrected intermediate visual acuity (UIVA) at 60 cm, and corrected near visual acuity (CNVA) and uncorrected near visual acuity (UNVA) at 40 cm.
Results
CDVA, UDVA, CNVA, and UNVA values did not differ significantly between the study and control groups (0.02 ± 0.02 vs. 0.03 ± 0.02, p = 0.523; 0.05 ± 0.13 vs. 0.05 ± 0.15, p = 0.637; 0.46 ± 0.17 vs. 0.46 ± 0.15, p = 0.821; and 0.47 ± 0.21 vs. 0.49 ± 0.25, p = 0.612; respectively), whereas the study group showed significantly better results for CIVA (0.28 ± 0.12 vs. 0.38 ± 0.13, p = 0.001) and UIVA (0.31 ± 0.16 vs. 0.41 ± 0.12, p = 0.001).
Conclusions
The Eyhance IOL, which features a new optical design based on a continuous power profile, was determined to be superior to a classic monofocal IOL for intermediate visual acuity and not inferior for corrected and uncorrected distance and near visual acuity.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The desire of cataract surgeons and patients alike is for the intraocular lens (IOL) implanted after cataract surgery to provide good vision at far, intermediate, and near distances. New IOLs introduced over the past two decades have come progressively closer to achieving this goal, including multifocal IOLs with diffractive, refractive, and accommodative designs, trifocal IOLs with a greater number of focal points, and extended-depth-of-focus (EDOF) IOLs. However, their inability to provide uninterrupted vision at all distances and the occurrence of positive dysphotopsias such as halo, glare, and starbursts lead to dissatisfaction in some patients [1, 2].
While multifocal IOLs are relatively effective for far, intermediate, and near visual acuity, monofocal IOLs are far from adequate for intermediate and near distances [3]. Important tasks such as using the computer, playing cards, going down stairs or walking on uneven surfaces, various hobbies, and seeing the car dashboard make the need for intermediate vision all the more pressing. A recently introduced monofocal IOL (ICB00, Eyhance, Tecnis) promises to meet the intermediate vision needs of cataract patients who are not candidates for multifocal IOLs, but without causing dysphotopsias such as halo and glare due to the lack of a diffractive or refractive ring.
The structural features of the Eyhance IOL and initial clinical results were shared in a launch meeting held in Frankfurt in February 2019 [4]. According to supplemental material and the first published study [5] provided by the manufacturer, the feature that distinguishes this IOL from other monofocal lenses is that instead of utilizing a spherical aberration-based or zonal design, it has a unique continuous power gradient created by a higher-order asphere. Power maps comparing the Tecnis Eyhance IOL with other Tecnis monofocal lenses demonstrate that they are the same across most of the surface, with the difference appearing only in the central (~ 15%) area [4, 5].
In the present study, we evaluated the visual performance of the new Eyhance monofocal IOL (ICB00, Tecnis) at far, intermediate, and near distances compared to a classic monofocal IOL (SN60WF IQ, AcrySof, Alcon).
Materials and methods
The study included a total of 128 patients who presented with impaired vision due to cataract and underwent uncomplicated cataract surgery with phacoemulsification and in-the-bag implantation of either the Eyhance (ICB00, Tecnis) or AcrySof (SN60WF, Alcon) monofocal IOL by the same surgeon (E.C.) in the Ekol Eye Hospital between September 2019 and January 2020.
In accordance with the Declaration of Helsinki, all patients were informed about the cataract surgery and informed consent was obtained. The study was approved by the Alanya Alaaddin Keykubat University School of Medicine Ethics Committee (no: 16-2/2020).
Inclusion criteria were: age over 40 years, presence of cataract, potential visual acuity of 0.1 LogMAR or better, and preoperative corneal astigmatism less than 1.00 diopter (D). Exclusion criteria were: history of ocular surgery or trauma, dislocated or subluxated lens, presence of uveitis, high myopia or hyperopia, retinal pathologies, glaucoma, and intraocular pressure over 21 mmHg. Patients with intra- or postoperative complications such as anterior capsular tear, posterior capsule rupture, zonular dialysis, and anterior or posterior synechia were also excluded. Refractive error was estimated using an autorefractometer (Topcon KR-8800), followed by manifest refraction to determine corrected distance visual acuity (CDVA). Manifest refraction results were accepted as the patient’s actual refractive error.
The cataract patients were informed about the general features of monofocal IOLs. Of a total of 128 patients, 63 received the ICB00 Eyhance IOL in one eye and were included in the study group, while the other 65 received the SN60WF AcrySof monofocal aspheric IOL in one eye and were classified as the control group.
All operations were performed under topical anesthesia with 0.5% proparacaine hydrochloride (Alcaine, Alcon, Switzerland). In all patients, a main corneal incision of 2.2 mm was made and the anterior chamber was filled with viscoelastic material containing 1.8% sodium hyaluronate. Capsulorhexis was performed manually. Two 1.1-mm side ports were created 90 degrees to the left and right of the main incision. The crystalline lens was emulsified using an Alcon INFINITI® device. After irrigation–aspiration, the anterior chamber was again filled with viscoelastic material and the monofocal IOL was implanted in the bag using its own injector system. After clearing the viscoelastic material from the anterior chamber, the main and side incisions were hydrated without suturing. All patients received an intracameral injection of cefuroxime sodium 1 mg/0.1 ml (Aprokam®, Thea Pharma) for prophylaxis. Postoperative treatment for all patients included a combination of topical netilmicin 0.3% and dexamethasone 0.1% (Netildex®, Teka Corp.) four times a day for 2 weeks and then tapered by 1 drop per week.
Monocular CDVA and uncorrected distance visual acuity (UDVA) were measured under photopic conditions using ETDRS (Early Treatment Diabetic Retinopathy Study) charts at 4 m and 100% contrast (ESV-3000 ETDRS System, Vectorvision, Inc.). Monocular corrected and uncorrected intermediate visual acuities (CIVA, UIVA) were measured using ETDRS near acuity charts (Sloan ETDRS Format Near Vision, Precision Vision) at 60 cm with 100% contrast. Monocular corrected and uncorrected near visual acuities (CNVA, UNVA) were assessed at 40 cm using the same near chart. Visual acuity results were converted to LogMAR values for statistical analysis.
Mean and standard deviation values were calculated, and the normality of the data distributions was analyzed. As the data were normally distributed in both groups, Student’s t test was used for between-group comparisons. IBM SPSS Statistics version 21.0 (IBM Corp., Armonk, NY, USA) package software was used for all statistical analyses. P values < 0.05 were considered statistically significant.
Results
The 63 patients (33 women, 30 men) in the study group (ICB00, Eyhance IOL) had a mean age of 61.3 ± 11.4 (range, 45–80) years, and the 65 patients (34 women, 31 men) in the control group (SN60WF, AcrySof) had a mean age of 60.1 ± 12.5 (range, 44–81) years. There was no difference in sex distribution between the groups (p = 0.718). Preoperative characteristics of patients in the two IOL groups are presented in Table 1. The material and optic features of both IOLs are presented in Table 2.
Mean postoperative follow-up duration was 3.02 ± 1.3 (range, 1–4) months in the study group and 3.1 ± 1.4 (range; 1–4) months in the control group (p = 0.814). Preoperative visual acuity values of the study and control groups were 0.53 ± 0.2 and 0.52 ± 0.2 LogMAR, respectively (p = 0.615).
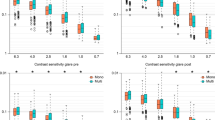
There was no significant difference between the two groups in terms of postoperative spherical equivalent (SE), CDVA, UDVA, CNVA, UNVA values, whereas postoperative CIVA and UIVA values were significantly different. Moreover, a significant difference was detected between the two IOL groups in terms of the amount of hyperopic correction (add plus diopters for near, ADD +) required to allow comfortable reading of the 0.2 LogMAR line at a near distance of 40 cm. Monocular CDVA, UDVA, CIVA, UIVA, CNVA, UNVA, and ADD + results at far (4 m), intermediate (60 cm), and near (40 cm) distances for each group are summarized in Table 3. Figure 1 is a comparative chart showing the CIVA and UIVA values of the two IOL groups with their standard deviations.

Comparative chart showing the mean CIVA and UIVA values of the two IOL groups with their standard deviations. CIVA: corrected intermediate visual acuity, UIVA: uncorrected intermediate visual acuity
Rates of patient satisfaction with spectacle-free distance, intermediate, and near vision were 95.2% (n = 60), 90.4% (n = 57), and 55.5% (n = 35) for the Eyhance IOL and 95.3% (n = 62), 53.8% (n = 35), and 41.5% (n = 27) for the AcrySof IOL, respectively.
In terms of the surgical experience, the ICB00 Eyhance IOL is easily folded, comes out of the injector system with no problem, and is readily manipulated during in-the-bag placement. There was no difference in surgeon comfort during all stages of the operation compared to the classic monofocal IOL (SN60WF, AcrySof).
No patients in either group developed posterior capsule opacification that required neodymium:YAG laser capsulotomy during follow-up. There were no complications resulting in IOL explantation.
Discussion
All technological advances in IOL surface properties (aspheric, spheric), focal properties (bifocal, trifocal, EDOF), and refraction principles (refractive, diffractive, apodized) have aimed to provide maximum improvement in patients’ visual performance at all distances. The aim of this study was to evaluate a new monofocal IOL (ICB00, Eyhance, Tecnis) that improves far visual acuity as effectively as a classical monofocal IOL and also promises better visual acuity at intermediate distances. When we compared corrected and uncorrected visual acuities at far, intermediate, and near distances in 63 patients unilaterally implanted with the Eyhance IOL and 65 patients unilaterally implanted with the AcrySof IOL, there were no significant differences in terms of postoperative SE, CDVA, UDVA, CNVA, or UNVA values, while the eyes with Eyhance IOLs showed significantly better CIVA (0.28 ± 0.12 vs. 0.38 ± 0.13 LogMAR, p = 0.001) and UIVA (0.31 ± 0.16 vs. 0.41 ± 0.12 LogMAR, p = 0.001). Moreover, there was a significant difference between the two monofocal IOLs in terms of the necessary hyperopic correction (ADD + for near) to comfortably read the 0.2 LogMAR line (1.74 ± 0.40 D for Eyhance vs. 2.19 ± 0.37 D for AcrySof, p = 0.003).
The first comparative study of the Eyhance was an unpublished prospective, multicenter, randomized clinical study that evaluated CIVA, CDVA, and UIVA with the Eyhance IOL and the monofocal ZCB00 IOL (Tecnis) [4]. The study analyzed postoperative 6-month outcomes of 67 patients in the Eyhance group (bilateral implantation) and 72 patients in the ZCB00 group (bilateral). In terms of intermediate vision, mean CIVA was significantly better in eyes implanted with the Eyhance IOL compared to those implanted with the ZCB00 IOL, with a difference of 1.1 lines LogMAR. Better UIVA was also reported in the Eyhance group. In terms of distance vision, the Eyhance IOL was reported to provide monocular and binocular distance visual acuity similar to the ZCB00, with a difference in binocular CDVA of 0.4 lines (Snellen equivalent). Therefore, the authors concluded that the Eyhance IOL provided comparable binocular distance vision to the ZCB00 IOL and noted that the frequency of dysphotopsias such as halo, glare, and starbursts was also comparable between the two IOLs. Both the data obtained in the study and feedback from surgeons indicated that the Eyhance IOL has a larger “landing zone” than other monofocal IOLs, which translates to better uncorrected bilateral distance vision outcomes for patients. Indeed, feedback from patients confirmed greater satisfaction with their ability to perform various daily activities without correction [4].
In the first published study examining this new IOL, Mencucci et al. [5] compared far, intermediate (66 cm), and near visual acuity between the ICB00 and another monofocal IOL, the Tecnis ZCB00. They reported that both IOLs provided statistically comparable, high levels of UDVA, CIVA, and CNVA, with the ICB00 group showing significantly better monocular UIVA (0.28 ± 0.11 vs. 0.40 ± 0.10, p < 0.001) and distance-corrected intermediate visual acuity (0.27 ± 0.11 vs. 0.37 ± 0.09, p = 0.023). The monocular CIVA and UIVA values obtained with the ICB00 in the present study (0.28 ± 0.12 and 0.31 ± 0.16 LogMAR, respectively) are similar to those reported by Mencucci et al. They also reported that the two groups did not differ significantly in terms of photopic contrast sensitivity, binocular defocus curve, objective scatter index, Strehl ratio, modulation transfer function cutoff, halo, or glare, and demonstrated that ICB00 IOL provided better spectacle independence than the ZCB00 IOL for intermediate distance [5].
Our study compared the ICB00 IOL with another monofocal SN60WF IOL, with no financial support or other compensation from the manufacturer of the IOL. The CDVA, UDVA, CIVA, UIVA, CNVA, and UNVA values obtained in our study were consistent with those reported in the first ICB00 IOL clinical study [5]. Our results also corroborate the superiority of the ICB00 IOL for intermediate visual acuity (60 cm) with or without correction.
Of the recommended solutions for patients with intermediate vision loss associated with presbyopia, bifocal IOLs have been replaced by trifocal and EDOF IOLs due to their shortcomings at intermediate distances. Hogarty et al. [6] compared 86 eyes implanted with an EDOF IOL (Symfony, Tecnis) and 90 eyes implanted with a monofocal IOL (3-piece ZA9002, Tecnis and ZCT IOL, Tecnis) in terms of visual acuity at two different intermediate distances of 1 m and 63 cm, and showed that the EDOF IOL provided a more substantial increase in visual acuity than the monofocal IOL at both distances. Gil et al. [7] evaluated the visual performance of five different multifocal IOLs (SV25T0, ATLISA 809 M, ATLISA Tri 839MP, ZKB00, ZLB00, and Symfony ZXR00) at far, intermediate (60 cm), and near distances. They determined that the Symfony ZXR00, which had EDOF properties, provided up to +1.73 D of additional power at intermediate distance and was therefore markedly superior to the other IOLs. Pedrotti et al. [8] also compared far, intermediate (60 cm), and near visual acuity with a monofocal IOL (ZCB00, Tecnis), two multifocal IOLs (Restor +3.0 D and +2.50 D, Alcon), and an EDOF IOL (Symfony, ZXR00, Tecnis) and reported that intermediate visual acuity with the EDOF IOL (0.05 ± 0.08 LogMAR) was better than that of the monofocal IOL (0.30 ± 0.08 LogMAR) and +3.00 Restor IOL (0.39 ± 0.06 LogMAR) and comparable to that of the +2.50 Restor IOL (−0.05 ± 0.05 LogMAR). Given that the visual acuity values for EDOF IOLs at intermediate distances (60–70 cm) were 0.18 ± 0.11, 0.021 ± 0.074, and 0.05 ± 0.08 LogMAR in the Hogarty, Gil, and Pedrotti studies, we believe that the visual acuity at 60 cm achieved with the new monofocal ICB00 IOL in the present study (0.28 ± 0.12 LogMAR) is a good result comparable to EDOF IOLs.
Trifocal IOLs offer good vision at intermediate distance, and some of the first of these IOLs to be used were the FineVision Micro F (PhysIOL, Belgium) and AT LISA tri 839MP (Carl Zeiss Meditec, Germany) IOLs. In studies on trifocal IOLs, patients implanted with FineVision Micro F IOL alone had uncorrected visual acuity ranging between −0.05 ± 0.05 and 0.19 ± 0.09 LogMAR at intermediate distances of about 70–80 cm [9,10,11,12]. In studies comparing the FineVision Micro F and AT LISA tri 839MP IOLs, uncorrected visual acuity at an intermediate distance of approximately 66 cm ranged from −0.05 ± 0.12 to 0.32 ± 0.09 LogMAR for both IOLs, with better results for the FineVision Micro F IOL [10, 13, 14]. The rates of spectacle independence in trifocal IOL studies were 92–100%, although dysphotopsias were frequently reported with both IOLs [13,14,15,16,17]. In the present study, corrected (0.28 ± 0.12 LogMAR) and uncorrected (0.31 ± 0.16 LogMAR) intermediate visual acuities were satisfactory and similar to those achieved with trifocal IOLs.
De Medeiros et al. [18] compared 20 patients bilaterally implanted with a trifocal IOL (PanOptix, TNFT00) with 40 patients who received an EDOF IOL (Symfony, ZXR00) in one eye and a bifocal IOL (ZMB00, Tecnis) in the other eye and determined that both groups achieved good intermediate distance vision, with binocular UIVA of 0.14 and 0.2 logMAR, respectively. Alio et al. [19] compared intermediate vision (70 cm) in 17 patients with bilateral bifocal AT LISA 809 M, 15 patients with bilateral trifocal AT LISA 839 M, and 17 patients with bilateral trifocal Restor SN6AD1 IOLs. They reported that despite no significant difference in visual acuity (0.24 ± 0.21, 0.14 ± 0.16, and 0.18 ± 0.17 LogMAR, respectively), patient satisfaction was 88% with the bifocal IOL versus about 94% with the trifocal IOLs. Moreover, dysphotopsias such as halo and glare were observed at substantial rates with all of the IOLs. The intermediate distance vision obtained with ICB00 IOLs in the present study was very similar to that obtained with trifocal and bifocal IOLs in the studies by de Medeiros and Alio.
ICB00 IOL is a monofocal IOL with no diffractive or refractive rings, instead providing intermediate visual gains with a gradual increase in thickness from the periphery to the center, which the manufacturer calls a “continuous power profile” [4, 5]. Due to this continuous power profile, the anterior surface of the ICB00 IOL is that the new design in the center of the IOL compared to other classic monofocal IOLs with the same power without creating the appearance of any zones [4, 5]. Moreover, it is noteworthy that none of the patients implanted with the ICB00 IOL in the present study reported unpleasant photic phenomena such as halo and glare. Considering the reports that dysphotopsias are more frequent with trifocal IOLs [20,21,22], the continuous power profile structure of the ICB00 IOL seems to offer the features of a monofocal IOL while avoiding these disturbing effects.
The ICB00 features a higher-order aspheric optic designed to enhance intermediate vision. Based on simulated visual acuity and the metric proposed by Alarcon et al., defocus curves were calculated for the new lens design and for the standard aspheric monofocal IOL between +0.50 and −2.00 diopters (D) of defocus [23]. The effects of higher-order aberrations (HOAs) on far and intermediate (−1.50 D) simulated visual acuity and the effects of corneal HOAs, pupil size, and decentration were evaluated in computer simulations of realistic eye models [24]. In another study, compared to a standard aspheric monofocal IOL with the same platform, material, and primary spherical aberration, the ICB00-simulated defocus curves showed increased simulated visual acuity in the intermediate range with comparable distance vision, independent of pupil size and corneal HOAs [25]. The ICB00 design provided a gain of approximately 0.1 LogMAR at −1.50 D with a difference of less than 0.05 LogMAR at distance [25]. Both designs also showed similar tolerance to decentration.
The ICB00 lens design is based on a continuous refractive optical surface with a local power change that was optimized to extend the depth of focus while maintaining distance image quality [25]. The purely refractive, continuous aspheric surface design of the ICB00 eliminates the unfavorable effects often associated with noncontinuous surface designs such as diffractive surfaces or zonal refractive designs [26, 27]. Alarcon et al. [25] evaluated photic phenomena using an extended light source and a high dynamic range imaging technique and showed that the ICB00 design performed similarly to aspheric monofocal IOLs that fully compensate for average corneal spherical aberration, without an increase in light scattering.
This study involved a small sample and short follow-up period. Further studies on Eyhance are required to validate our findings with long-term results. Our study focused on visual performance at far, intermediate, and near distances, and we did not investigate the defocus curve, aberrations, or contrast sensitivity. Moreover, our data are the results of monocular implantation, and binocular data are needed. Although we did not compare the ICB00 IOL with the ZCB00 IOL, the SN60WF IOL is comparable in terms of optic and haptic size and material properties. Therefore, we do not believe that this affected the study outcomes.
In brief, the Eyhance (ICB00) is a new IOL that eliminates the shortcomings of monofocal IOLs for intermediate vision during activities such as using a computer and going up or down stairs while avoiding the dysphotopsias that occur with multifocal IOLs. As a standard monofocal IOL that is familiar to surgeons and easy to implant, the Eyhance can be recommended to patients undergoing routine cataract surgery.
References
Bellucci R (2005) Multifocal intraocular lenses. Curr Opin Ophthalmol 16:33–37
Dick HB (2005) Accommodative intraocular lenses: current status. Curr Opin Ophthalmol 16:8–26
Calladine D, Evans JR, Shah S, Leyland M (2012) Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev 9:CD003169
Highlights from the Frankfurt January 2019 Advisory Board Meeting (2018) Material: “Delivering intermediate vision: the new TECNIS eyhance monofocal IOL.” Available at https://www.jjvision.com/ Data on File, Johnson & Johnson Surgical Vision, Inc. DOF2018CT4015
Mencucci R, Cennamo M, Venturi D, Vignapiano R, Favuzza E (2020) Visual outcome, optical quality, and patient satisfaction with a new monofocal IOL, enhanced for intermediate vision: preliminary results. J Cataract Refract Surg 46(3):378–387
Hogarty DT, Russell DJ, Ward BM, Dewhurst N, Burt P (2018) Comparing visual acuity, range of vision and spectacle independence in the extended range of vision and monofocal intraocular lens. Clin Exp Ophthalmol. 46:854–860
Gil MA, Varón C, Cardona G, Buil JA (2020) Visual acuity and defocus curves with six multifocal intraocular lenses. Int Ophthalmol 40(2):393–401
Pedrotti E, Carones F, Aiello F et al (2018) Comparative analysis of visual outcomes with 4 intraocular lenses: monofocal, multifocal, and extended range of vision. J Cataract Refract Surg 44(2):156–167
Carballo-Alvarez J, Vazquez-Molini JM, Sanz-Fernandez JC et al (2015) Visual outcomes after bilateral trifocal diffractive intraocular lens implantation. BMC Ophthalmol. 15:26
Martinez-de-la-Casa JM, Carballo-Alvarez J, Garcia-Bella J et al (2016) Photopic and mesopic performance of 2 different trifocal diffractive intraocular lenses. Eur J Ophthalmol 27:26–30
Vryghem JC, Heireman S (2013) Visual performance after the implantation of a new trifocal intraocular lens. Clin Ophthalmol. 7:1957–1965
Cochener B, Vryghem J, Rozot P et al (2012) Visual and refractive outcomes after implantation of a fully diffractive trifocal lens. Clin Ophthalmol. 6:1421–1427
Marques EF, Ferreira TB (2015) Comparison of visual outcomes of 2 diffractive trifocal intraocular lenses. J Cataract Refract Surg 41:354–363
Bilbao-Calabuig R, Llovet-Rausell A, Ortega-Usobiaga J et al (2017) Visual outcomes following bilateral lmplantation of two diffractive trifocal intraocular lenses in 10 084 eyes. Am J Ophthalmol 179:55–66
Liu X, Xie L, Huang Y (2018) Comparison of the visual performance after implantation of bifocal and trifocal intraocular lenses having an identical platform. J Refract Surg 34:273–280
Mencucci R, Favuzza E, Caporossi O et al (2017) Visual performance, reading ability and patient satisfaction after implantation of a diffractive trifocal intraocular lens. Clin Ophthalmol. 11:1987–1993
Mendicute J, Kapp A, Levy P et al (2016) Evaluation of visual outcomes and patient satisfaction after implantation of a diffractive trifocal intraocular lens. J Cataract Refract Surg 42:203–210
De Medeiros AL, de Araujo Rolim AG, Motta AFP et al (2017) Comparison of visual outcomes after bilateral implantation of a diffractive trifocal intraocular lens and blended implantation of an extended depth of focus intraocular lens with a diffractive bifocal intraocular lens. Clin Ophthalmol. 11:1911–1916
Alio JL, Kaymak H, Breyer D et al (2018) Quality of life related variables measured for three multifocal diffractive intraocular lenses: a prospective randomised clinical trial. Clin Exp Ophthalmol. 46:380–388
Gundersen KG, Potvin R (2017) Trifocal intraocular lenses: a comparison of the visual performance and quality of vision provided by two different lens designs. Clin Ophthalmol. 11:1081–1087
Xu Z, Cao D, Chen X, Wu S, Wang X, Wu Q (2017) Comparison of clinical performance between trifocal and bifocal intraocular lenses: a meta-analysis. PLoS ONE 12(10):e0186522
Cochener B (2016) Prospective clinical comparison of patient outcomes following implantation of trifocal or bifocal intraocular lenses. J Refract Surg 32:146–151
Alarcon A, Canovas C, Rosen R et al (2016) Preclinical metrics to predict through-focus visual acuity for pseudophakic patients. Biomed Opt Express. 7(5):1877–1888
Weeber HA, Featherstone KA, Piers PA (2010) Population-based visual acuity in the presence of defocus well predicted by classical theory. J Biomed Opt 15(4):040509. https://doi.org/10.1117/1.3475956
Alarcon A, Cánovas C, Koopman B, Weeber H, Auffarth GU, Piers PA (2020) Enhancing the intermediate vision of monofocal intraocular lenses using a higher order aspheric optic. J Refract Surg 36(8):520–527
Terwee T, Weeber H, van der Mooren M, Piers P (2008) Visualization of the retinal image in an eye model with spherical and aspheric, diffractive, and refractive multifocal intraocular lenses. J Refract Surg 24(3):223–232
Langeslag MJM, van der Mooren M, Beiko GHH, Piers PA (2014) Impact of intraocular lens material and design on light scatter: in vitro study. J Cataract Refract Surg 40(12):2120–2127
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors have any conflict of interest related to this research.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Approval for the study was obtained from the Alanya Alaaddin Keykubat University Ethics Committee (protocol no. 16-2/2020).
Informed consent
Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Cinar, E., Bolu, H., Erbakan, G. et al. Vision outcomes with a new monofocal IOL. Int Ophthalmol 41, 491–498 (2021). https://doi.org/10.1007/s10792-020-01599-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-020-01599-8