
Abstract
The main aim of this article was to analyze the relationship of income inequality and government effectiveness with differences in efficiency in the use of health inputs to improve the under-five survival rate (U5SR) in developing countries. Robust Data Envelopment Analysis (DEA) and regression analysis were conducted using data for 47 developing countries for the periods 2000–2004, 2005–2009, and 2010–2012. The estimations show that countries with a more equal income distribution and better government effectiveness (i.e. a more competent bureaucracy and good quality public service delivery) may need fewer health inputs to achieve a specific level of the U5SR than other countries with higher inequality and worse government effectiveness.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
The United Nations’ (UN) Millennium Development Goals (MDGs) provided development priorities and a set of targets to be attained by developing countries in 2015. These goals included commitments to eradicating poverty, improving education and health, and promoting gender equality and sustainable development. This article addresses the specific health-related MDG of the reduction of the under-five mortality rate (U5MR) by two-thirds between 1990 and 2015 (Goal 4, MDG 4). Available data suggest that there has been great progress in improving child survival over the past 25 years: the global U5MR decreased by 53 % and the number of under-five deaths fell from 12.7 million in 1990 to 5.9 million in 2015 [1]. However, despite progress, the global U5MR is remains far from the MDG 4 target; in particular, Sub-Saharan African and Southern Asian countries have to prioritize the reduction of child mortality. Figure 1 shows the evolution of the under-five survival rate (U5SR) since 2000 to illustrate this point. The figure demonstrates that although Sub-Saharan Africa has made great improvements, this region still remains well below the level of progress achieved in other regions.

Under-five survival rate in developing countries by regions (2000–2012)
Developing countries can make progress towards reducing the U5MR either by increasing the resources they allocate to achieving this goal or by enhancing efficiency in the use of their available resources. Some authors have suggested that although spending on health care improves the health status of the population, developing countries can potentially gain more through the more effective and efficient allocation of health resources [2–4]. For example, the WHO has estimated that at least 50 % of medical equipment in developing countries is either partly usable or totally unusable [5]. Moreover, Bokhari et al. have shown that many expensive hospital services in the poorest countries are ineffective in improving health outcomes in the most at-risk population [6]. Thus, the decision to direct these resources to basic primary care with proven effectiveness in reducing child mortality or to more expensive hospital services that may only benefit a small minority of the population will have an effect on health outcomes [7, 8]. In addition, sub-national imbalances in the distribution of resources in some developing countries may produce shortages in rural areas while urban centers are overstaffed, thereby leading to wide spatial inequalities in health and poor performance at the national level [1].
It is a complex task to analyze efficiency at the aggregate level in the production of health outcomes, such as the reduction of child mortality. Although the relevant inputs in this production process include a broad set of discretionary medical care resources, other factors are also of great importance, such as personal factors (e.g. educational level of the population), socio-economic factors (e.g. quality of governance of health institutions), and environmental factors (e.g. prevalence of epidemic diseases) [9]. Regarding socio-economic factors, it has been suggested that mortality tends to decrease faster in countries with a more equal income distribution [10, 11]. It has also been suggested that institutional deficiencies or weak institutional capacity are two of the main reasons for public spending having a low or negligible impact on development outcomes such as health status or education attainmentFootnote 1 (e.g. see [13] and [14]). Based on these suggestions, it could be argued that low mortality may be easier or harder to achieve depending on the politics, economics, and history of any given country [15]. For example, Bangladesh or the Indian state of Kerala, among others, are well-known cases that show how the political, economic, and social characteristics of territories are relevant to achieving low mortality [16]. Bangladesh has overtaken India in a broad range of basic social indicators, including child survival, despite having barely half of India‘s per-capita income [17, 18]. The role of institutions that build trust and cohesion might explain this example of “good health at low cost” [19]. A serious public health problem in many developing countries is that medical personnel are frequently absent from work [20]. Low wages could be a reason for this situation, but it is not always the reason. In Kerala, for example, absenteeism is rare, and this is clearly related with people’s expectations and grass-roots political activism [21]. These are two examples of political (and historical factors) that could explain why, in many ways, “the country you are born in largely determines your life possibilities” as Rodrik claimed [22].
In this context, the main aim of this article was to determine which socio-economic factors are associated with differences in efficiency in converting inputs (physician density and relative total health expenditure) into a specific health outcome (the U5SR) in different countries. This indicator was selected as the target health outcome measure because it is calculated from the U5MR, a UN key indicator for monitoring progress towards MDG 4, which is widely recognized as a bellwether of population health in developing countries.Footnote 2 It should be recognized, however, that there could be differences in the levels of efficiency in the provision of health outputs and health outcomes. In addition, factors influencing efficiency in the provision of health outputs could differ from those affecting the provision of health outcomes [24].Footnote 3 Thus, two main hypotheses were tested at the macro level:
-
There is a direct relationship between the efficiency levels reached by countries in the production of a key health-output, such as child immunization against measles (IAM), and the level of efficiency achieved in producing a basic health-outcome, such as the U5SR.
-
Countries with a more equal income distribution and better government effectiveness tend to be more efficient in the provision of health outcomes, such as the U5SR.
In order to test these hypotheses, two main assumptions were taken into account: that the same health-related inputs are used to produce health outputs and health outcomes; and that a specific country, which could be considered to be highly efficient in the production of a key health output, may not necessarily be efficient in the attainment of health outcomes. After controlling for differences between countries in the operating environment, robust Data Envelopment Analysis (DEA) was implemented to benchmark countries in terms of their relative efficiency in using multiple inputs in the production of selected outputs and outcomes. Subsequently, regression analysis was employed to estimate the cross-sectional associations of IAM efficiency, income inequality, and government effectiveness on the robust efficiency scores estimated for the health outcome (U5MR). The database used in the estimations comprised 47 developing countries with data for the periods 2000–2004, 2005–2009, and 2010–2012 (see Tables 4, 5 and 6 in the Appendix).
Thus, this study adds to the literature by offering an analysis of the association between income inequality and government effectiveness and the level of efficiency reached in the production of this key health outcome. The estimations show that a more equal income distribution and better government effectiveness is associated with higher efficiency in the use of health inputs in reducing the U5MR. Thus, the main challenge in many developing countries is to reduce the U5MR without raising overall health spending by implementing policies directed towards the improvement of government effectiveness and the achievement of a more equal income distribution.
The article is organized as follows. Section 2 reviews the literature on differences in efficiency between developing countries in the use of their current resources to achieve health outputs and outcomes. Section 3 presents the data and the methodology employed in the empirical analysis. Section 4 provides some concluding remarks and a discussion of the implications of the research findings.
2 Health spending efficiency: a review of the literature
Given that the health sector accounts for a sizeable proportion of national expenditures in most countries, an extensive body of literature has addressed the empirical measurement of the efficiency of public expenditure through the estimation of efficiency frontiers. These studies are of two broad types: micro and macro analyses. On the one hand, micro analyses attempt to measure efficiency for particular categories of public spending. These studies have addressed hospitals and health centers, sub-units such as departments, nursing homes, physician practices, district health authorities, and even the costs associated with individual patients [26] in developed and developing countries [27–30]. On the other hand, macro analyses mainly attempt to estimate the efficiency of total public spending at the national level [31–33].
Regarding macro analyses, relatively little empirical research is available on international comparisons of health investment performance through the estimation of efficiency frontiers (e.g. see [2, 31, 34, 35]). However, there is a greater range of empirical literature on the effectiveness of spending directed towards health outcomes. In contrast to previous studies that have suggested that investing in health care sectors has very little impact on improving health outcomes after controlling for the country’s income [3, 36–39], several studies have found evidence that government health expenditures have an impact on outcomes [4, 6, 8, 40–44]. Nevertheless, observed differences in spending on health are insufficient to explain the marked differences in child mortality between countries [8, 39]. The highest fraction of deaths, and in particular child deaths, in developing countries are due to infectious and parasitic diseases [38]. For this reason, vaccine-preventable diseases are seen as global priorities due to their high mortality rate. Given that most vaccinations are inexpensive, immunization is widely recognized as one of the most efficient, successful, and cost-effective health investments and has become a major part of the strategy towards achieving MDG 4 [45–48]. It is also important to take into account that child mortality is not only an indicator of the state of children’s health, but also an indicator of the efficacy of a government’s social policies. The availability of basic health-care services and immunization coverage rates may indicate the extent to which the government is pro-poor [15].
Moreover, in developing countries, appropriate policies, inclusive institutions, and effective instruments should lead to increased efficiency in health expenditure. Empirical and theoretical considerations suggest that greater inequality in income distribution should be associated with worse health status for a given income level [41, 49]. This is explained by the fact that lower income inequality implies that more of the population has significantly higher private income to spend on food, housing, health care, and other basic needs [7]. High income inequality also suggests that economically privileged groups have a greater capacity to influence the political system for their own benefit rather than that of the majority [50]. For example, providing suitable antenatal care in the community (especially in rural areas) may be more effective in reducing the U5MR than providing many of the other high-end inpatient services. In addition, spending on primary health care and health centers tends to benefit the poor more than spending on hospitals. However, these investments are of little direct value to wealthier segments of the population, who use private health care and more specialized forms of public health services [51, 52]. In addition, inequality is socially corrosive and leads to more violence, lower levels of trust, and lower social capital [53]. Thus, inclusive institutions and policies may not only mitigate health inequalities, but also enhance the effectiveness and efficiency of health expenditures in producing basic health outcomes.
The large disparities between the U5MRs of nations with similar rates of development have focused research on identifying the main drivers of U5MR reduction by analyzing the influence of socio-economic and political determinants [54]. In addition to household disposable income level and income distribution, the literature has addressed factors such as geography, environment, ethnicity, maternal education, religion, access to clean water and sanitation, the integration of minorities, political stability, and good governance. It has also been suggested that policy makers should recognize that increases in government health expenditures need to be complementary to, rather than a substitute for, spending in other sectors due to the potential synergetic effects between spending on health and these other sectors, such as utilities, infrastructures, and education [6, 8].
3 Efficiency measurement and its determinants
3.1 Data
As mentioned, the U5MR was selected as the indicator to measure countries’ health outcomes. However, given that DEA has to consider increasing outcomes as the desired objective (more is better), the U5MR has been transformed into the under-five survival rate (U5SR). This variable has been calculated (in percentage) as [(1- (U5MR/1000)) · 100]. In addition, the chosen output indicator is the Proportion of 1-year-old children IAM. Footnote 4 Inputs have to refer to controllable (discretionary) resources employed by countries in the attainment of the health-related outputs and outcomes. Two health inputs were considered: a physical (human) indicator Physician density per 10,000 people (DOC); and a financial indicator Total health expenditure as a percentage of the country’s GDP (THE). An important assumption of the DEA model is that decision-making units (DMUs), countries in our case, operate within homogeneous environments. However, the performance of countries’ health systems is conditioned by factors which may have an impact on the efficiency with which conventional inputs (DOC and THE) are used to produce health outputs and outcomes (IAM and U5MR, respectively). The main global risk factors for deaths in children must be taken into account from among these ‘environmental variables’ that have an impact on the U5SR. The most critical of these risk factors are: non-access to drinkable water; non-access to sanitation facilities; predominant rural population; undernourishment; low educational attainment among women; early pregnancy among adolescents; prevalence of premature babies; and prevalence of HIV in the adult population [56]. All these indicators have been considered to be environmental variables with the exception of the prevalence of HIV and premature babies, which have not been included in the information set due to data availability constraints.
Income inequality (measured by the Gini index) and the competence of the bureaucracy and quality of public service delivery (measured by the Government effectiveness index) are also considered outlying factors that may potentially have an impact on efficiency. Given that the aim of this article was to determine which of these factors are significantly associated with efficiency, both indicators have been included as independent variables in a regression model in which the dependent variable is the robust DEA efficiency scores obtained for U5SR. On the one hand, the Gini index (GINI) is a widely employed indicator to measure inequality in the distribution of income at the country level. Values of GINI range between 0 in the case of “perfect equality” (each individual or household obtains the same income) and 1 in the case of “perfect inequality” (all income belongs to the individual or household with the highest income). Income inequality is a structural socio-economic component of the economies and, to a large extent, is determined by historical, institutional, and cultural factors. On the other hand, governance is a multidimensional concept that, in general, refers to the exercise of political, economic, and administrative capacity [57]. The World Bank’s Worldwide Governance Indicators (WGI) provide aggregate indicators that capture the different dimensions of governance [58]. Specifically, the WGIs provide measures of the quality of governance, on a scale of scores from −2.5 to 2.5, for the six different dimensions considered: control of corruption; government effectiveness; political stability; regulatory quality; rule of law; and voice and accountability. A range of surveys conducted by institutes, non-governmental organizations, and international organizations are employed in the construction of these indexes. Among these indexes, the Government effectiveness index (GE) is employed in this article as the indicator of governance. Among other aspects, it mainly measures perceptions regarding the quality of bureaucracy and public service delivery. This index could be considered a good proxy for the quality of public health service delivery, unlike other institutional quality measures (such as political stability, regulatory quality, rule of law, and voice and accountability) that are expected to have a weaker relationship with health outcomes. Otherwise, the strong correlation between the control of corruption index and government effectiveness index suggests that both variables should not be included in the same regression model.
Table 1 shows the definitions and sources of the variables employed in the empirical analysis. Due to data availability constraints, and given that most of these indicators change slowly, the variables finally included in the analysis were the average values for the periods 2000–2004, 2005–2009, and 2010–2012. Figure 2 shows the variables included and the proposed analytical framework.

Health production model: from health care inputs to outputs and outcomes
3.2 Methodology
Data Envelopment Analysis was used to calculate the technical efficiency of DMUs (countries) relative to a best-practice frontier. The aim of this linear programming (LP) technique is to obtain a convex frontier which “envelops” the entire set of observations [59]. The countries’ levels of efficiency in transforming inputs into outputs and outcomes (i.e. the efficiency scores) are then inferred by estimating how far the data of a given country are from the frontier. Estimated DEA efficiency scores can be either input or output oriented. These two measures provide the same results under constant returns to scale but give different values under variable returns to scale [60]. In this analysis, constant returns to scale were not imposed on an input-oriented specification in the DEA models in order to keep to a minimum a priori restrictions about the shape of the frontier. In this case, the reported efficiency scores can be used to assess by how much discretionary inputs can be reduced without varying the level of outputs.
However, without adequately controlling for the operating environment, DEA estimates will be potentially biased given that a health system’s efficiency in countries characterized by adverse environments will be underestimated and, conversely, the technical efficiency of the health system in countries with favorable environments will be overestimated [61]. This problem may be overcome by the inclusion of environmental variables in the DEA model, which account for the existence of differences in these risk factors, thereby leveling the playing field for all countries by removing the influence of these variables on efficiency [62]. It is also worth noting that in the standard deterministic DEA approach bias may arise when the calculated efficiency scores are used for inference since they lack a probability distribution needed for any regression model. Bootstrapping methods have been proposed to obtain unbiased and consistent DEA efficiency estimates [63].
We used the ‘rDEA’ package in the R statistical software to estimate robust input-oriented DEA technical efficiency measures [64]. This package implements a double bootstrap estimation technique to obtain bias-corrected estimates of the unobserved efficiency measures after adjusting for differences in the environmental variables, as described in Simar and Wilson’s Algorithm #2 [65]. This approach was also used to estimate robust DEA efficiency measures corresponding to the health output (IAM coverage). In this case, the environmental variables considered were: ‘Predominantly urban population prevalence’, ‘Women’s educational attainment’, and ‘Early pregnancy among adolescents’ (see Fig. 2). The ‘rDEA’ program was also used to generate the DEA scores for the standard deterministic model for purposes of comparison.
Thus, after estimating the robust technical efficiency scores, we determined if GINI and GE were significantly associated with efficiency. With this aim, a regression model was specified and estimated to gain insight into the relationship between these factors and the estimated bias-corrected efficiency scores.
3.3 DEA results
Table 2 shows the average values for each region of the variable returns to scale input-orientated bias-corrected DEA scores estimated for the periods 2000–2004, 2005–2009, and 2010–2012 (see Appendix; Tables 4, 5 and 6 showing the individual scores estimated for each country). It is important to note that, on average, the estimated efficiency scores do not substantially change between periods, with the exception of Sub-Saharan Africa (SSA) — and to a lesser extent South Asia (SA) — which underwent significant improvements in average efficiency between 2000 and 2012. These results also suggest that there is room for significant increases in efficiency especially in developing countries in the Middle East and North Africa (MENA), Latin America and the Caribbean (LAC), and Europe and Central Asia (ECA) regions.
For example, Table 2 shows that Moldova had an efficiency score of 0.232 during the last period analyzed, making this country the worst performer in the period 2010–2012. This result implies that Moldova could reduce the use of health inputs by 76.8 % while maintaining the achieved U5SR. It is important to note that, during the period 2010–2012, Moldova spent an average of 11.6 % of the GDP on the health system and had 3.2 physicians per 10,000 people. These figures are in sharp contrast to those of Armenia, for example, which is in the same region and has a similar U5SR (98.3 %); however, Armenia spends 4.3 % of the GDP on health services and has a physician density per 10,000 people (DOC) of 2.8. Other countries from different regions could be mentioned among the low-performing countries. For example, Paraguay and Costa Rica have similar levels of total health expenditure (THE) (9.3 % and 10 % of the GDP, respectively) and DOC (1.2 and 1.1 per 10,000 people, respectively). However, Paraguay has a U5SR of 97.7 % whereas Costa Rica has a U5SR of 99.0 %. In a different region, the case of Jordan is also striking. The U5SR in this country is similar to that of Kazakhstan, but Jordan invests twice the amount of financial resources in the health system. In the period 2010–2012, Jordan expended 8.6 % of the GDP whereas Kazakhstan spent 4.3 %. Most of the inefficiencies detected in these countries could be explained by fragmentation between private and public programs in the case of Jordan [66], and organizational problems with little attention paid to primary health-care services in the case of Paraguay and Moldova [67, 68]. The case of South Africa is also noteworthy. In the period 2010–2012, it spent 8.7 % of the GDP on the health system, achieving a U5SR of 95 %; thus, it has the lowest efficiency score in all periods studied in the Sub-Saharan Africa (SSA) region. The most relevant factors explaining this low level of achievement are social and economic inequalities and the persistently skewed allocation of resources between public and private sectors [69]. Nevertheless, child mortality should undergo further reductions in this country due to the increased prevention of mother-to-child HIV transmission.
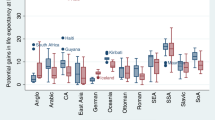
Figure 3 shows the relationship between average efficiency scores estimated for the IAM (the intermediate health output) and the U5SR (the health outcome). As expected, there is a clear positive association between both scores. This association could be due to the fact that, in both cases, the inputs considered are the same. Moreover, this also means that the IAM efficiency scores may be considered strong predictors of the U5SR efficiency scores: if a country is efficient in the delivery of a crucial health-output like IAM, this could suggest that it also efficient in the achievement of health outcomes like U5SR. Although this direct association holds in most cases, there are several countries in which it does not hold, as in the case of two neighboring countries, Costa Rica and Nicaragua, which appear as outliers in the Figure 3. Costa Rica is a regional high performer in terms of the U5SR (99.0 %) and Nicaragua has a U5SR of 97.5 %. Nicaragua and Costa Rica have a THE of 7.6 % and 10 % of the GDP, respectively, and a DOC of 0.8 and 1.1, respectively. As shown in Fig. 4, both countries have similar levels of income inequality (0.43 Nicaragua and 0.49 Costa Rica). However, among other differences, Costa Rica had an average government effectiveness index (GE) of 0.60, whereas Nicaragua had an average GE 0.32 during the period 2000–2012.

Relationship between IAM and U5SR efficiency scores. Averages for the three periods 2000–2004, 2005–2009 and 2010–2012

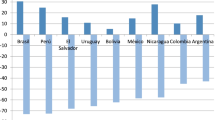
Relationship between income inequality and U5SR efficiency scores. Averages for the three periods 2000–2004, 2005–2009 and 2010–2012
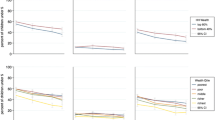
Figures 4 and 5 show that structural socio-economic factors, such as income inequality and government effectiveness, may explain the differences between countries in their estimated robust U5SR efficiency scores. The next section provides insight into which of these outlying factors could be associated with efficiency.

Relationship between government effectiveness and U5SR efficiency scores. Averages for the three periods 2000–2004, 2005–2009 and 2010–2012
3.4 Explaining measured inefficiencies
In the next step, we used the estimated robust DEA efficiency scores to analyze how differences in efficiency across countries could be associated with differences in income inequality and government effectiveness. Table 3 shows the results of the regression models estimated for each period and for pooled data when the dependent variable considered was the estimated bias-corrected U5SR efficiency scores.
The estimations show that countries with a higher GINI have lower U5SR efficiency scores than countries with a more equal income distribution. Specifically, if a country with a GINI of 1 (maximum inequality) attains a GINI of 0 (maximum equality), the resulting efficiency score would change from 0 (minimum efficiency level) to approximately 0.6. In addition, GE had a significant association with U5SR efficiency scores, although this relationship was not significant in the last two periods considered (2005–2012 and 2010–2012). Using pooled data (column 4 in Table 3), estimation results showed that countries in which government effectiveness is higher have higher efficiency scores: a point increase in the GE would increase the health outcome efficiency score by approximately 0.2, all other factors being constant. As expected, the estimations also showed that developing countries with greater efficiency in the provision of IAM have higher U5SR efficiency scores. Thus, when considering efficiency issues in the use of health inputs in the production of basic health outcomes, such as increasing U5SR, the findings suggest that a key role could be played by income distribution and government effectiveness, which are both socio-economic factors that are at least as important as the availability of efficient child immunization programs.
Finally, it worth noting that the estimations include two regional dummies to control for regional idiosyncratic factors that were not included in the model. These variables indicate that, all other factors being constant, the average scores for Middle East and North Africa (MENA) and Europe and Central Asia (ECA) countries are 0.157 and 0.091 less than the overall average, respectively (see Table 3, column 4). These figures suggest that the lower efficiency levels in these countries are explained by factors, not controlled in the model, that differ from those in other countries in different regions. It also noteworthy that the adjusted R-squared was high in all the estimations and that the Ramsey RESET test was not significant in any of the cases. Thus, omitted variable bias was not expected to be an issue in these regressions.
4 Conclusions
The main finding of this article is that income distribution and government effectiveness are associated with efficiency in the provision of health outcomes in developing countries. The results suggest that countries with a more equal income distribution, a more competent bureaucracy, and good quality public service delivery (i.e., better government effectiveness) may need fewer health inputs to achieve a specific level of U5SR than other countries with higher income distribution inequality and low government effectiveness. In other words, although medical outputs could be produced efficiently, they may still only have a limited impact on premature mortality in developing countries if there are high levels of income inequalities and low levels of government effectiveness.
Inequality transcends income and touches on broader dimensions, such as health; for example, higher income inequality appears to be associated with higher mortality, as shown by the clear social gradient in relation to child mortality [70, 71]. Income inequality is a mark of inequity and has profoundly negative social and economic effects in whatever country it occurs. The analysis of equitable progress in health outcomes suggests that when progress is not evenly shared, a persistent within-country inequity reduces the effectiveness and efficiency of the health care system. Furthermore, income inequalities often translate into political inequalities. As a result, privileged groups have a greater ability than that of the majority to influence the political system for their own benefit (i.e. the capture of institutions by powerful groups) [51]. Thus, developing countries with substantial structural inequalities are probably unable to provide equal social benefits to all, even if their governments aspire to do so [72]. Also, inefficient public spending may be a result of poor governance [73]. In fact, impoverishment is perpetuated when the institutions that govern the distribution of public resources are weak, corrupt, or structurally inequitable [12, 14, 74]. In this regard, the findings obtained are supported by those of Hu and Mendoza [44], who found that the general quality of governance, as measured by the control of corruption and the quality of the bureaucracy, plays an important role in helping to reduce infant and child mortality rates. Their main regression results led them to suggest that infant and child mortality rates could be significantly lowered if there was less corruption. Pervasive corruption (fuelled by the “learning through practice” and the belief that “everybody does it”) may have an impact on inequality. At the same time, greater inequality fosters corruption. Thus, this two-way relationship contributes to countries being caught in a vicious circle of inequality and corruption, with corrosive effects on society. To reverse this situation, and achieve virtuous circles in which equity and integrity can become mutually reinforcing, it is crucial to control corruption by means of building stronger institutions leading to better government efficiency and higher quality of the bureaucracy and regulatory framework [75]. Strong and fair inclusive institutions that address the specific structural inequalities that constrain growth and development have to be implemented by fostering sustainable and inclusive economic growth as well as policies with outcomes that are more effective and transparent [76]. Finally, it is important to recall that income distribution and government effectiveness are structural components of economies and, to a large extent, determined by historical, institutional, and cultural factors. For this reason, the inclusion of these indicators as explanatory variables in the regression model can be used to indirectly control a wide range of idiosyncratic factors that could affect efficiency. For example, in developing countries, good governance mainly affects health through its indirect impact on income [77].
A wide sample of developing countries and complete time-series should be analyzed to draw more reliable conclusions. Data availability constrains hindered us from constructing a panel data. Also, further research is needed on the areas explored in this article, and specifically on the barriers that prevent the less developed countries from making progress and significantly reducing the gap that separates them from those with a higher level of efficiency. In any case, the results suggest that the reduction of the disparities identified would require making major changes to institutions, particularly those that have a greater impact on the degree of inequality in income distribution, and overcoming the structural inequalities and political constraints that hinder health achievements.
Notes
It is worth noting the kind of institutions these authors refer to. They consider key public sector institutions, including public service provision, the bureaucracy, and the legal and tax system, sharing the view of Knowles and Owen [12], among others.
The U5MR and Infant Mortality Rate (IMR) are the most used outcome indicators of health achievements in developing countries. However, the U5MR is preferable to the IMR as a measure of survival mainly because the indirect techniques employed to estimate it are less sensitive to assumptions about underlying mortality patterns than are the techniques used to estimate the IMR [23]. In contrast to adult or old-age mortality, child mortality is the one indicator that is based on a comparably large amount of empirical data in low-income and middle-income countries, which makes it unique from a monitoring perspective [1]. In addition, the U5MR has three substantial advantages over life expectancy at birth [7]: under-five deaths are more often due to preventable causes, and thus should be easier to reduce through appropriate policies; the death of a child represents more years of life foregone than does the death of an older person; a new cohort of babies is born every year, so the U5MR is more sensitive than life expectancy to new socioeconomic circumstances and to changes in social service delivery.
Health outcomes refer to the health consequences brought about by the treatment of a health condition or as the result of an interaction with the healthcare system. Thus, health outcomes encompass a wide range of health-related consequences of healthcare interventions and programs (i.e. health outputs) [25].
Three reasons justify the use of this indicator as a measure of health output:
-
Immunization is considered to be a good proxy for the use of basic maternal and infant health services [7], which are strong predictors of the U5MR. In addition, vaccinations are strongly associated with further vaccinations: people who get one are likely to get another [55].
-
Measles is one of the most important causes of child death in poor countries despite the availability of a safe and effective vaccine. In addition, the between-country distribution of alternative indicators, such as DPT (diphtheria, tetanus, and pertussis) vaccination coverage, is similar to that in countries employing measles vaccination coverage.
-
Given the potential of measles vaccination to reduce child mortality and that measles vaccination coverage can be considered to be a marker of access to child health services, routine measles vaccination coverage was also selected as an indicator for monitoring progress towards MDG 4.
-
References
You D, Hug L, Ejdemyr S, Idele P, Hogan D, Mathers C, Gerland P, New J, Alkema L (2015) Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. Lancet Glob Health Collect. doi:10.1016/S0140-6736(15)00120-8
Jayasuriya R, Wodon Q (2003) Development targets and efficiency in improving education and health outcomes in Mexico’s Southern States. World Bank MPRA Paper No. 10577. The World Bank, Washington
Gupta S, Verhoeven M, Tiongson E (2002) The effectiveness of government spending on education and health care in developing and transition economies. Eur J Polit Econ 18(4):717–737
Gupta S, Verhoeven M, Tiongson E (2003) Public spending on health care and the poor. Health Econ 12:685–696
World Health Organization (2010) Health systems financing: the path to universal coverage. WHO, Geneva
Bokhari F, Gai Y, Gottret P (2007) Government health expenditures and health outcomes. Health Econ 16:257–273
McGuire J (2006) Basic health care provision and under-5 mortality: a cross-national study of developing countries. World Dev 34(3):405–425
Farag M, Nandakumar A, Wallack S, Hodgkin D, Gaumer G, Erbil C (2013) Health expenditures, health outcomes and the role of good governance. Int J Health Care Finan Econ 3:33–52
Cutler D, Deaton A, Lleras-Muney A (2006) The determinants of mortality. J Econ Perspect 20(3):97–120
Mehrotra S, Vandemoortele J, Delamonica E (2000) Basic services for all? Public spending and the social dimensions of poverty. Innocenti Research Centre. United Nations Children’s Fund, Florence
Rodgers G (2002) Income and inequality as determinants of mortality: an international cross-section analysis, 1979. Int J Epidemiol 31(3):533–538
Knowles S, Owen D (2010) Which institutions are good for your health? The deep determinants of comparative cross-country health status. J Dev Stud 46(4):701–723
Wagstaff A, Claeson M (2004) The millenium development goals for health: rising to the challenges. The World Bank, Washington
Rajkumar A, Swaroop V (2008) Public spending and outcomes: does governance matter? J Dev Econ 86:96–111
Gauri V, Khaleghian P (2002) Immunization in developing countries: its political and organizational determinants. World Dev 30(12):2109–2132
Ottersen O, Dasgupta J, Blouin C, Buss P et al (2014) The political origins of health inequity: prospects for change. Lancet 383:630–667
Drèze J, Sen A (2011) Putting growth in its place, Outlook
Mushtaque A, Chowdhury R, Bhuiya A, Chowdhury M, Rasheed S, Hussain Z, Chen L (2013) The Bangladesh paradox: exceptional health achievement despite economic poverty. Lancet 382:1734–1745
Rodrik D, Subramanian A (2003) The primacy of institutions (and what this does and dos not mean). Fin Dev 40(2):31–34
Chaudhury N, Hammer J, Kremer M, Muralidharan K, Rogers FH (2006) Missing in action: teacher and health worker absence in developing countries. J Econ Perspect 20(1):91–116
Deaton A (2013) The great escape. Health, wealth, and the origins of inequality. Princeton University Press, Princeton
Rodrik D (2013) The past, present, and future of economic growth. Working Paper 1 Global Citizen Foundation
Ahmad O, Lopez A, Inoue M (2000) The decline in child mortality: a reappraisal. Bull World Health Organ 78:1175–1191
Joumard I, André C, Nicq C (2010) Health care systems: efficiency and Institutions. OECD Economics Department Workings Papers, No. 769. OECD Publishing
Lee A, Leung S (2014) Health outcomes. In: Michalos AC (ed) Encyclopedia of quality of life and well-being research. Springer Reference, Heildelberg
Worthington A (2004) Frontier efficiency measurement in health care: a review of empirical techniques and selected applications. Med Care Res Rev 61(2):135–170
DeLellis N, Ozcan YA (2013) Quality outcomes among efficient and inefficient nursing homes: a national study. Health Care Manag Rev 38(2):156–165
Coppola MN, Ozcan YA, Bogacki R (2003) Evaluation of performance of dental providers on posterior restorations: does experience matter? A data envelopment analysis (DEA) approach. J Med Syst 27(5):445–456
Akazili J, Adjuik M, Jehu-Appiah C, Zere E (2008) Using data envelopment analysis to measure the extent of technical efficiency of public health centres in Ghana. BMC Int Health Human Rights 8:11. doi:10.1186/1472-698X-8-11
Renner A, Kirigia JM, Zere EA, Barry SP, Kirigia DG, Kamara C et al (2005) Technical efficiency of peripheral health units in Pujehun district of Sierra Leone: a DEA application. BMC Health Serv Res 5:5-11
Tandon A (2005) Measuring efficiency of macro systems: an application to millennium development goal attainment. Asian Dev Rev 22(2):108–125
Tanzi V, Schuknecht L (1997) Reconsidering the fiscal role of government: the international perspective. Am Econ Rev 87(2):164–168
Tanzi V, Schuknecht L (2000) Public spending in the 20th century: a global perspective. Cambridge University Press, Cambridge
Adler N, Yazhemsky E, Tarverdyan R (2010) A framework to measure the relative socio-economic performance of developing countries. Socio Econ Plan Sci 44:73–88
Abdelfattah B, Ablanedo-Rosas J, Gemoets L (2011) Developing country efficiency assessment by means of a comprehensive model based on data envelopment analysis. Int J Soc Syst Sci 3(1/2):58–80
Musgrove P (1996) Public and private roles in health: theory and finance patterns. World Bank Discussion Paper No. 339. The World Bank, Washington
Filmer D, Pritchett L (1997) Child mortality and public spending on health: how much does money matter? World Bank Policy Research Working Paper No. 1864. The World Bank, Washington
Filmer D, Hammer J, Pritchett L (1998) Health policy in poor countries: weak links in the chain. World Bank Policy Research Working Paper No.1874. The World Bank, Washington
Filmer D, Pritchett L (1999) The impact of public spending on health: does money matter? Soc Sci Med 49:1309–1323
Anand S, Ravallion M (1993) Human development in poor countries: on the role of private incomes and public services. J Econ Perspect 7(1):133–150
Bidani B, Ravallion M (1997) Decomposing social indicators using distributional data. J Econ 77(1):125–139
Bhalotra S (2007) Spending to save? State health expenditure and infant mortality in India. Health Econ 16:911–928
Farahani M, Subramanian S, Canning D (2010) Effects of state-level public spending on health on the mortality probability in India. Health Econ 19:1361–1376
Hu B, Mendoza R (2013) Public health spending, governance and child health outcomes: revisiting the links. J Human Dev Capabilities 14(2):285–311
Anand S, Bärnighausen T (2007) Health workers and vaccination coverage in developing countries: an econometric analysis. Lancet 369:1277–1285
Hay A (2010) Successes and challenges in global immunization efforts. Trans R Soc Trop Med Hyg 104:87–88
Dietrich S (2011) The politics of health aid: why corrupt governments have incentives to implement aid effectively. World Dev 39(1):55–63
Berkley S (2014) Improving access to vaccines through tiered pricing. Lancet 383:2265–2266
Wilkinson RG, Pickett KE (2006) Income inequality and population health: a review and explanation of the evidence. Soc Sci Med 62:1768–1784
Tandon A (2007) Measuring government inclusiveness: an application to health policy. Asian Dev Rev 24(1):32–48
Ghobarah H, Huth P, Russett B (2004) Comparative public health: the political economy of human misery and well-being. Int Stud Q 48:73–94
Davoodi H, Tiongson E, Asawanuchit S (2010) Benefit incidence of public education and health spending worldwide: evidence from a new database. Poverty Publ Policy 2(2):5–52
Wilkinson RG (2005) The impact of inequality: how to make sick societies healthier. New Press, NY
Feng X, Theodoratou E, Liu L, Chan K, Hipgrave D, Scherpbier R, Brixi H, Guo S, Chunmei W, Chopra M, Black R, Campbell H, Rudan I, Guo Y (2012) Social, economic, political and health system and program determinants of child mortality reduction in China between 1990 and 2006: a systematic analysis. J Global Health 2(1) doi:10.7189/jogh.02.010405
Hall A (2004) Vaccination and child mortality. Lancet 364:2156–2157
Hanf M, Nacher M, Guihenneuc C, Tubert-Bitter P, Chavance M (2013) Global determinants of mortality in under 5 s: 10 year worldwide longitudinal study. BMJ 2013(347):1–8
OECD (2015) Government at a Glance. OECD Publishing, Paris
Kaufmann D, Kraay A, Mastruzzi M (2011) The worldwide governance indicators: methodology and analytical issues. Hague J Rule Law 3:220–246
Charnes A, Cooper W, Rhodes E (1978) Measuring the efficiency of decision making units. Eur J Oper Res 2:429–444
Banker R, Charnes A, Cooper W (1984) Some models for estimating technical and scale inefficiencies in data envelopment analysis. Manag Sci 30:1078–1092
Fried H, Schmidt S, Yaisawarng S (1999) Incorporating the operating environment into a nonparametrtic measure of technical efficiency. J Prod Anal 12:249–267
Ruggiero J (2004) Performance evaluation when non-discretionary factors correlate with technical efficiency. Eur J Oper Res 159:250–257
Simar L, Wilson P (1998) Sensitivity analysis of efficiency scores: how to bootstrap in nonparametric frontier models. Manag Sci 44(1):49–61
Simm J, Besstremyannaya G (2015) Robust Data Envelopment Analysis (DEA) for R version 1.2-2, https://github.com/jaak-s/rDEA
Simar L, Wilson P (2007) Estimation and inference in two-stage, semi-parametric models of production processes. J Econ 136(207):31–64
World Health Organization (2006) Health systems profile-Jordan. Regional Health Systems Observatory-EMRO. Regional Office for the Eastern Mediterranean, WHO, Cairo
Pan American Health Organization (2008) Health systems profile Paraguay. PAHO, Washington
Turcanu G, Domente S, Buga M, Richardson E (2012) Republic of Moldova: health system review. Health Syst Transit 14(7):1–151
Harrison D (2009) An Overview of Health and Health care in South Africa 1994–2010: Priorities, Progress and Prospects for New Gains. A Discussion Document Commissioned by the Henry J. Kaiser Family Foundation to Help Inform the National Health Leaders’ Retreat
Marmot M, Friel S, Bell R, Houweling T, Taylor S (2008) Closing the gap in a generation: health equity through action on the social determinants of health. Lancet 372:1661–1669
McGuire J (2010) Wealth, Health, and Democracy in East Asia and Latin America. Cambridge University Press, Cambridge
Bloom G (2001) Equity in health in unequal societies: meeting health needs in contexts of social change. Health Policy 57:205–224
Makuta I, O’Hare B (2015) Quality of governance, public spending on health and health status in Sub Saharan Africa: a panel data regression analysis. BMC Public Health 15(932):1–11
Gisselquist RM (2012) Good governance as a concept, and why this matters for development policy. UNU-WIDER Working Paper No. 2012/30. World Institute for Development Economics Research, United Nations University, Helsinki
Dobson S, Ramlogan-Dobson C (2012) Why is corruption less harmful to income inequality in Latin America? World Dev 40(8):1534–1545
Marmot M (2005) Social determinants of health inequalities. Lancet 365:1099–1104
Klomp J, De Haan J (2008) Effects of governance on health: a cross-national analysis of 101 countries. Kyklos 61(4):599–614
Acknowledgments
We are grateful for the thoughtful comments from the three anonymous reviewers. We take responsibility for any remaining errors.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Ortega, B., Sanjuán, J. & Casquero, A. Determinants of efficiency in reducing child mortality in developing countries. The role of inequality and government effectiveness. Health Care Manag Sci 20, 500–516 (2017). https://doi.org/10.1007/s10729-016-9367-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10729-016-9367-1