
Abstract
The results of over a decade of research at Victoria University on the effectiveness of various smoke alarm signals for awakening sleeping people are presented and compared. The results show that the signal level (sound volume, light intensity, etc.) and the type of sound or signal affect the probability of people being woken up by an alarm. The 520 Hz square wave sound was the most effective of the sounds tested, waking most (often all) of the participants. The smoke alarms currently used in Australia and the USA emit sounds of about 3,100 Hz. Many participants did not wake up to such tones even when very loud at the pillow (95 dBA). In all groups tested the high-pitched sound was the worst and in most, notably children, young adults (sober and 0.05 BAC) and older adults, it was much worse than the 520 Hz square wave signal. In adults with hearing loss it was more than seven times as effective as the current signal and more effective than the bed and pillow shakers. Strobe lights were found to have very poor waking effectiveness. A voice alarm was quite effective for younger age groups but not for older adults. The voice alarm was also found to have real problems in waking participants with limited English. It is recommended that the 520 Hz square wave sound in the T-3 pattern be adopted as a replacement for the current smoke alarm sound.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
1 Introduction
This paper primarily draws together and examines the results of more than a decade of research at Victoria University (VU) on the effectiveness of various smoke alarm signals for awakening sleeping people. We present the available results for the range of sounds and other signals that have been tested, and compare the results of the various studies. We identify important cases that have not yet been examined, and discuss limitations of the available research and the conclusions that can be drawn from it.
Smoke alarms in dwellings are intended to warn occupants of the presence of a fire, presumably with the expectation that, so warned, they are:
-
Less likely to be injured or killed by the fire or its effects
-
More likely to extinguish the fire while it is small, thus lessening the damage
No specific purpose is stated in AS 3786, the Australian Standard for smoke alarms [1] or in NFPA 72 [2]. NFPA 72 does state that a household fire alarm system produces an alarm signal … for … notifying the occupants of the presence of a fire so that they will evacuate the premises. Presumably this applies to smoke alarms. Smoke alarms may be of some value when occupants are awake, but their greatest value is when the occupants are asleep and are thus less likely to notice the fire or its effects with sufficient time to avoid harm [3].
Smoke alarms consist of two primary components in a single unit [1]. The first component, a smoke detector, is required to reliably sense the presence of smoke from a developing fire. There are two aspects to smoke detector reliability [3] although only the first of these is addressed in AS 3786 [1]. The smoke detector must have a very high probability of:
-
Sensing smoke when it is present even at low concentrations
-
Not being triggered by non-fire related phenomena (because of the detrimental effect false alarms may have on occupant behaviour e.g. disabling and/or ignoring an alarm)
The smoke detector is used to activate the second component, an alarm sounding device [1]. The alarm sounding device must reliably warn occupants of the likely presence of a fire, must be heard by them and they must recognise it as an urgent alarm [3]. There are four aspects to the reliability of the alarm sounding device. The device must have a very high probability that it will:
-
Sound when activated
-
Sound with the required signal at the required sound level for the required duration
-
Not make any noise when not activated (to avoid annoyance to occupants)
-
Not sound unless activated by the smoke detector (for the same reason)
It is normally assumed that early detection is beneficial, and thus that smoke alarms can only be very effective for their intended purpose if they quickly detect the fires that harm people and then quickly warn the people who are most often harmed by those fires [3]. Ideally, on this basis, the smoke detector is in or near the locations of the fire starts and the alarm sounding device is in or near the locations of relevant people (those most often harmed and those who care for occupants who cannot reliably respond or respond appropriately to an alarm, e.g. very young children, very old people, and physically or mentally handicapped people).
If the smoke detector is located far from the relevant fire start locations then it is likely that greater time will elapse before the detector is triggered, and the probability that it may not trigger at all is greater. If the alarm sounding device is located far from the occupants likely to be harmed (or the people who care for them) then the probability that those occupants will not hear or respond to the alarm is greater, as is the probability that they will take longer to respond to it. In both cases, the more remote the device, the more it is likely that doors, walls, furniture etc will delay and/or reduce the probability that the alarm is effective.
If the fire start location and the occupants likely to be harmed (or the people who care for them) are always in the same vicinity there is no difficulty in locating smoke alarms. However, if they are not (which appears to often be the case), a compromise is required when determining the location of smoke alarm units. When an alarm close to a fire sounds, the sound level near occupants located elsewhere may be considerably attenuated. Alternatively, there may be a considerable delay in detection of a fire by smoke alarms close to the occupants but not close to the fire. But if the smoke alarms are interconnected this situation is resolved. Interconnected here is taken to mean that with interconnected smoke alarms there is a smoke detector and alarm sounding device at each location and the activation of one leads to all of the smoke alarms being activated [1]. The likelihood of occurrence of false (sometimes called nuisance) alarms increases with the number and interconnection of smoke alarms, as does the total cost of the smoke alarm system. It is notable that in the USA NFPA has required alarms in bedrooms since 1993 and interconnected alarms since 1989 [2, 4]. In Australia, the Building Code of Australia (BCA) [5] even now (2008) does not have these requirements.
The effectiveness of smoke alarms in achieving their intended purpose is affected by factors such as the type of smoke detector and the sound emitted by the alarm sounding device [3]. There are a variety of smoke detection technologies that vary in their sensitivity to various types of smoke [6, 7] and therefore may activate the alarm sounding device at different times after ignition even if they are in the same location. This aspect will not be considered further in this paper.
The sound emitted by the alarm sounding device must be very effective in awakening sleeping people, particularly those people whose characteristics make them most at risk of being killed and injured in dwelling fires [3], and it has now been established that there are several aspects of the sound that influence this effectiveness [8–22]. We will show below that our studies over the last 10 years demonstrate that the current (high-pitched) sounds used in smoke alarms in Australia and the USA are substantially less effective in waking sleeping people than other tested sounds. This research has also demonstrated that increasing the sound output level increases the proportion of the people who wake up. Thus it is apparent that the type of sound emitted by a smoke alarm and the level of that sound affect the risk to the occupants associated with fire. These considerations can be restated as follows: the particular sound emitted by a smoke alarm, the level (loudness) of the sound emitted, the recommended locations of smoke alarms and whether the smoke alarms are interconnected, directly effect the injury and fatality rates in dwelling fires, provided that it is assumed that some people would not awaken in response to the other cues created by the fire (sounds, smells, heat, flickering light, etc.).
Smoke alarms can only be very effective in reducing fire casualties (fatalities and injuries) if they awaken sleeping people who would not otherwise awaken to the cues of a smouldering or flaming fire. In some countries a minimum sound level at the pillow of 75 dBA is specified for smoke alarms [2]. (A hallway alarm typically results in a pillow volume of 55–65 dBA with the door open.) However most unimpaired adults will normally awaken quickly to their smoke alarm sounding, even at levels well below 75 dBA [8, 9, 12]. But there are many vulnerable (or at-risk) people within the population (including children, adults impaired with alcohol, adults over 65 years and people who are hard of hearing) who are much less likely to awaken to such a signal. For over a decade we have tested the waking effectiveness of different signals, normally presented during deep sleep, among such at-risk people.
Sleep is classified as REM (rapid eye movement) sleep and non-REM sleep with the latter being divided into four stages (Stage 1–Stage 4) of increasing depth [23]. A person is drowsy rather than fully asleep in Stage 1 and is more difficult to wake up from Stages 3 and 4 (deep sleep) than from REM and Stage 2 sleep. The deeper stages of sleep occur early in the night which is also the time when many residential fire fatalities occur [24, 25].
The Temporal 3 (T-3) pattern of sound now specified in many countries for emergency evacuation signals specifies only the pattern of sound: one cycle is signal on for 0.5 s, off for 0.5 s on for 0.5 s, off for 0.5 s, on for 0.05 s and off for 1.5 s. Other characteristics of the signal (pitch, sound level, etc) are not specified. It was first specified by ISO in 1987 [26] and was first adopted in Canada in 1995, the USA in 1996 [27] and Australia in 2004 [28].
In 2001 Bruck [13] drew together the then available research on the ability of smoke alarms to wake sleeping people and the sleep research on arousal thresholds and concluded that people in many groups in the population would not awaken to a 75 dBA (at the pillow) high-pitched alarm. This review was expanded and updated by Bruck and Ball [28] Other research since 2001 has produced relevant findings. Proulx and Laroche [27] found that the T-3 sound was rarely identified as a fire alarm or evacuation signal and did not convey the need for an urgent response. Du Bois et al. [29] found that 96% of adults woke to a high-pitched (∼3,100 Hz) alarm sound when presented in the T-3 pattern for two minutes at 75 dBA at the pillow during Stage 4, Stage 2 and REM sleep. However, only 57% of people whose hearing ability was reduced by 20–90 dBA over the range 250–8,000 Hz awoke to the same signal [29]. In 2006, Smith et al. [30] reported that in stage 4 sleep twenty-four 6–10-year-old children responded better to 100 dBA mother’s voice alarms (96% woke up) than the high pitched alarm also at 100 dBA (only 58% woke up).
Other early studies investigated the effectiveness of strobe lights for waking people but most did not control for sleep stage. Bowman et al. [31] did control for sleep stage and reported that only one third of their normal hearing female participants woke up from deep sleep to a strobe of more than 75 cd and that just less than half were woken from REM sleep. Du Bois et al. [29] in the 2005 study mentioned above reported that just over half of the deaf participants were woken up by a 110 cd, 1 Hz strobe light but only a third of hard of hearing and normal hearing participants were woken up.
2 Early Research at VU
The early smoke alarm studies at VU utilised a variety of signals presented at one signal strength and tested normal people as well as some at-risk people.
The initial objective was to understand and estimate the response of normal people to smoke alarms [8]. In this first study, undertaken in 1995, 24 sleeping young adults aged 18-24 years were exposed twice to a 60 dBA smoke alarm sound (a recording of the continuous beeping of an ∼3,100 Hz sound of a widely used Australian smoke alarm) in a sleep laboratory. The first presentation was unexpected (naive) but no significant difference was noted in the response between the first and second presentation (which was obviously not unexpected). The sleep stage was monitored and the alarm was presented in Stage 4, Stage 2 or REM sleep. Five participants did not awaken to one or both presentations, a total of seven non-awakenings in the 48 presentations (∼15%). Non-awakenings occurred in all stages of sleep and were retrospectively related to reported lack of sleep on the night prior to the test (sleep deprivation). Awakening was generally quick with awakening in 65% of presentations occurring within 30 s of the alarm, gradually rising to 85% during the entire 10 min alarm sound presentation (Figure 1).

Cumulative percentage woken up by a 60 dBA (at the pillow) smoke alarm sound in young adults (age 18–24 years, n = 24) as a function of time
In considering this and the following studies it is worthwhile noting the proportion of the participants who did not respond, as it is people not responding who are most likely to be killed or injured. In this study, as shown in Figure 1, 35% did not respond within the first 30 s, and even after 10 min of the alarm sounding at 60 dBA a very significant 15% remained asleep.
The next study tested waking to an Australian smoke alarm sound at ∼60 dBA at the pillow of children and their parents in their own homes [9]. Thirty-six participants aged between 6 and 59 years participated with all of the participants self-reporting normal hearing and sleep, no chronic illness and no ongoing medications affecting sleep/wake behaviour. Each subject wore an Actigraph (set to record movement at 32 s intervals) on their wrist to monitor sleep/wake behaviour. The smoke alarm sounded for 3 min, 1 h prior to the midpoint and 1 h after the midpoint of sleep of the shortest sleeper in the household. All of the adults awoke (100%), but only 23% of the children awoke to the smoke alarm sound, even fewer (14%) if only <16 year olds are considered. All of the adults woke during the first 32 s (Figure 2). Of the children 17% awoke within the first 32 s of the alarm beginning to sound, and all who awoke did so within 64 s. Thus, while all of the adults responded quickly, a very disturbing 83% of the children did not respond within the first 32 s and this only fell to 77% by the end of the 3 min alarm period.

Cumulative percentage woken up by a 60 dBA (at pillow) smoke alarm sound in adults (age 30–59 years, n = 16) and children (age 6–17 years, n = 20) as a function of time period
It is often assumed that all sleeping people have a high risk of becoming a fire fatality. However, fire brigade statistics indicate that most people wake to signs of fire as most occupants avoid injury and death when a reported fire occurs, even at night [12]. This suggests that vigilance continues during sleep. The next VU project tested the hypothesis that the majority of unimpaired adults would wake to minimal cues during a fire [12]. Low level cues designed to mimic the early presence of a fire were presented in their own homes to 33 adult volunteers aged 25–55 years, who self-reported normal sleep and normal responsiveness of the senses (auditory, visual and olfactory), plus 16 of their partners. Their ability to awaken to two different sounds (≤48 dBA) and a flickering light (≤5 lux) four hours after going to bed was tested. A second experiment in a sleep laboratory tested the responsiveness of 17 young adults aged 18–26 years to a 10-min exposure to an increasing level of a smoke odour during an afternoon nap (sleep stage: 2). There was a high rate of arousal to the sound cues (91% to a crackling sound and 83% to a shuffling sound), but only 59% awoke to the odour and 49% to the flickering light. In Figure 3 it can be seen that the majority of the subjects who woke to the sounds (shuffle and crackle) did so within the first 30 s but the response to the light was both lower and slower.

Cumulative percentage of adults (age 25–55 years, n = 33) woken up by low level simulated fire sounds and light as a function of time period
These findings indicate that most people will wake up to low-level auditory cues during a fire and around half will awaken to a low level flickering light or a smell. Extensive statistical modelling based on this data found that females have a significantly higher probability of waking to these cues than males. In addition, their response time was consistently shorter, though the difference was not statistically significant [32].
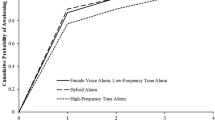
The effectiveness of various sounds for waking sleeping children has remained of great interest and was the subject of further study. One study [14], investigated the awakening of sleeping children aged 6–10 years using four different signals (all 89 dBA at the pillow). Two of the alarm sounds were voice recordings, one the voice of the child’s mother, the other the voice of a female actor. Both were intended to sound urgent, with the mother’s message including the child’s name several times and the actor’s message referring to fire and danger. The third signal was a 520 Hz square wave sound in the T-3 pattern [26]. The fourth signal was the high frequency (∼3,100 Hz) beep produced by a popular Australian smoke alarm and was a subset of data presented in Figure 2 [11]. Only children in the 6–10 years age group from that study are included here. The presentation was at 1 am (and also at 3 am in the case of the 520 Hz square wave and smoke alarm sounds). The children all woke up to the mother’s voice (100%), all but one woke up to the actor’s voice (94%) and the 520 Hz square wave signal (96%), but only 57% awoke to the smoke alarm sound. There was no significant difference in the results for the first three signals but there was a clearly significant difference between them and the Australian smoke alarm sound. Not only did many fewer children wake to the smoke alarm sound, most took longer to wake up (Figures 4, 5).

Cumulative percentage of children (age 6–10 years, n = 19 for voices, n = 27 for 520 Hz square wave, n = 22 for Australian smoke alarm) woken up at 89 dBA as a function of time period

Cumulative percentage woken up as a function of auditory arousal threshold for older adults (age 65–83 years, n = 42) [18]
Reviewing the studies presented above (Figures 1–4) there is a great deal of consistency in the results. Many young children did not wake up to the beeping ∼3,100 Hz Australian alarm sounds, even at ∼89 dBA, and many of those who did took longer to wake up. In comparison, most adults woke up to the same alarm at 60 dBA and, perhaps more importantly, woke up to fire-like sounds at ≤48 dBA. But they were much less likely to wake up to a smoke-like odour or low level flickering light.
3 More Recent Studies at VU
The more recent smoke alarm studies at VU involved testing of adults who may be considered to be at-risk. All used a similar experimental methodology called repeated measures to allow a direct comparison of the effectiveness of various signals (sounds, light, etc.) for waking people. The repeated measures technique tests the response of every participant to each signal. Thus each participant acts as their own control and differences in response are more readily apparent (compared with comparisons between groups made up of different people). Care should be taken in the comparisons of the results across different studies as there are some small differences in the presentation of the signals that may affect comparisons, as noted below.
3.1 Experimental Method
In these studies the signals were presented during deep sleep at increasing intensities or levels and waking was determined using brain wave patterns (EEG). The duration of each level was 30 s except for the highest level, which was longer. In the initial studies of this type, only sound was used, and there were no pauses between the levels. These cases are noted in the descriptions of the studies below. The remaining studies, with increasing intensity levels, presented sounds, pillow and bed shakers and strobe lights. Comparisons between these signals are facilitated by the use of a waking score which is shown in Table 1, which gives details of signal duration and level for each waking score. In these studies there was a pause or silence between the levels, as shown in Table 1.
The presentation order of all signals was counterbalanced in all studies with increasing intensity levels. The sounds used in these studies included the ∼3,100 Hz sound of a current US smoke alarm, a 520 Hz square wave sound, pure tones and various other sounds as noted in the descriptions below. The current smoke alarm signals used in Australia and the USA are a relatively high frequency sound easily generated at high volume using a small inexpensive piezoelectric siren. The current alarm signal (used in all of the studies below, except [14, 15]) is the high pitched T-3 sound [26] recorded from a current US smoke alarm (Kidde) and has a single dominant frequency of ∼3,100 Hz. The 520 Hz square wave signal is a mixed frequency sound with a dominant low frequency (520 Hz) and peaks at the 3rd, 5th, 7th, etc. harmonics.
There was some variation in the procedures used in these studies. In the studies incorporating strobes and/or shakers (shown in Figures 6 and 8), the sound level (measured at the pillow) commenced at 55 dBA and was incremented by 10 dBA, as shown in Table 1. In these studies comparison between the signals has been accomplished by using the waking score (Table 1) and a benchmark level for each signal. The sounds and other signals were presented in the T-3 pattern at five levels with a pause (no signal) between each level.
The benchmark level for all sounds is 75 dBA and for the pillow and bed shakers it is the standard intensity as purchased. For the strobe light the benchmark level is a single strobe light of 177 cd (considerably brighter than the intensity of 110 cd required by the National Fire Protection Association as an emergency notification signal when mounted more than 610 mm below the ceiling). The strobes were mounted at the foot of the bed, directed towards the pillow, with the three different strobe levels achieved by having one (177 cd), two (310 cd) or three strobes (420 cd) flashing simultaneously. The waking score (a number from 1 to 12) simply numbers the successive signal presentations and pauses (Table 1). Full details of the rationale behind the waking score and experimental procedure used in each study can be found in the original publications [15, 18, 19, 20].
In the other studies with increasing intensity (shown in Figures 5, 7, 9, 10), the sound level commenced at 35 dBA and was incremented by 5 dBA every 30 s until the 95 dBA level. It was maintained at 95 dBA for 210 s if the participant did not wake up.
3.2 Research Findings
The results of these studies are presented below in terms of the cumulative percentage awakened to allow comparison of the effectiveness of the signals at the various signal strengths tested (Figures 5–10). Each of these graphs has the benchmark level indicated by a vertical line to facilitate comparison of the signals at the benchmark level.

Cumulative percentage woken up for adults (age 18–77 years, n = 38) with mild to moderately severe hearing loss as a function of waking score [19]

Cumulative percentage awakened for sober young adults (age 18–26 years, n = 14) as a function of sound level [15]

Cumulative percentage woken up for young adults (aged 18–26 years, n = 32) with 0.05 Blood Alcohol Content as a function of waking score [20]

Cumulative percentage woken up for young adults (age 18–26 years, n = 14) with 0.05 Blood Alcohol Content as a function of sound level [15]

Cumulative percentage woken up for young adults (age 18–26 years, n = 14) with 0.08 Blood Alcohol Content as a function of sound level [15]
As noted above, caution should be exercised if comparing waking rates across studies as in Figure 5 (older adults), Figure 7 (sober young adults), Figure 9 (young adults at 0.05 BAC) and Figure 10 (young adults at 0.08 BAC) there were no pauses between different intensity levels, while pauses were inserted between signals in studies shown in Figure 6 (adults with hearing loss) and Figure 8 (young adults at 0.05 BAC). Based on these results it is noted that sounds commencing from silence had slightly greater waking effectiveness than the same sounds with no silence between increments. Thus, due to the design of the studies, comparisons within each study are more meaningful than comparisons across the studies. Nevertheless some across study observations are sufficiently strong that they are noteworthy.
3.2.1 Older adults
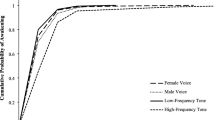
Forty-two adults aged from 65 to 83 years were presented with two signals per night over two nights while in Stage 3 sleep (Figure 5) [18]. The sample was screened to exclude people whose hearing thresholds fell into the lowest 16% for their age. The signals were the ∼3,100 Hz smoke alarm sound, the 520 Hz square wave, a male voice (saying danger, fire, wake up) and a 500 Hz pure tone, all in the T-3 pattern. A male voice was used in this study in preference to a female voice as, in a pilot study, it was found that the response to the male voice was considerably better than to the female voice [18]. There were no silences between the sound levels in this study. The most important findings were that the older adults needed a lower volume to wake to the 520 Hz square wave sound (median = 45 dBA) than to the other three signals and the ∼3,100 Hz alarm sound needed the highest volume (median = 65 dBA). Individual responses from three participants of non-English speaking background suggested a voice alarm in English would not be suitable for them.
At 75 dBA, the 520 Hz square wave can be said to be over three times better (at waking older adults) than the other signals as, at this sound level, less than 5% of participants did not respond compared with 14–18% for the other signals tested. The comparison is also in favour of the 520 Hz square wave at other sound levels.
3.2.2 Adults with mild to moderately severe hearing loss: [19]
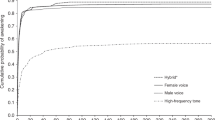
There are more than 34 million people in the US who are hard of hearing. In this study 38 adults (aged 18–77 years) with hearing loss averaging between 25 and 70 dB in each ear (i.e. mild to moderately severe hearing loss, but not deaf), each received three signals per night on two non-consecutive nights (Figure 6) [19]. The signals activated during Stages 3 or 4 sleep were a 400 Hz square wave, a 520 Hz square wave, the ∼3,100 Hz smoke alarm, a bed shaker (under mattress) and a pillow shaker (all in the T-3 pattern), and a strobe light in a modified T-3 pattern. Each signal was presented for the levels and durations shown in Table 1 until the participant was awake or the full range of intensities had been presented.
Under the testing conditions the 520 Hz square wave sound was the single most effective signal (Figure 6b), awakening 92% of hard of hearing participants when presented at or below 75 dBA and awakening 100% at or below 95 dBA. Both the 520 Hz and 400 Hz square waves were significantly more effective than the ∼3,100 Hz smoke alarm sound, which awoke 56% at or below 75 dBA. The bed shaker and pillow shaker devices, presented alone, awoke 80–83% of the hard of hearing participants at the intensity level as purchased (vibrating in intermittent pulses). The strobe lights were not an effective means of waking this population with only 27% waking to the lowest strobe light intensity and less than 60% waking to the strongest signal, which was very much stronger than the NFPA required ceiling or wall strobe.
At the benchmark level (waking score = 5) the strobe light is clearly the worst performer, not waking 77% of participants, with the ∼3,100 Hz smoke alarm sound being nearly as bad by not waking 56%. In contrast the 520 Hz square wave woke all but 8% of participants, between 7 and 10 times better. The 400 Hz square wave and the bed and pillow shakers were not quite as effective as the 520 Hz square wave but were much better than the ∼3,100 Hz smoke alarm sound and the strobes.
3.2.3 Sober young adults
Fourteen adults aged 18–26 years (self declared deep sleepers) received three signals on one night to explore the arousal threshold of deep sleeping young adults in Stage 4 sleep to three signals: a female voice alarm, a high pitch beeping smoke alarm common in Australian homes and the 520 Hz square wave T-3 alarm [15]. There were no silences between the sounds in this study. The female voice and the 520 Hz square wave consistently resulted in responses at lower sound levels than the Australian smoke alarm (see Figure 7).
Thus for sober young adults at the benchmark sound level (75 dBA) the 520 Hz square wave was about six times better than the Australian smoke alarm (7% did not respond compared with 43% non-response for the smoke alarm).
3.2.4 Young Adults with 0.05 Blood Alcohol Content (BAC)
The 32 participants consumed vodka and juice to become moderately alcohol impaired immediately before going to bed [20]. Six signals were presented across two non-consecutive nights to investigate their responsiveness during Stage 4 sleep to a 400 Hz square wave, 520 Hz square wave, 500 Hz pure tone, ∼3,100 Hz smoke alarm sound, bed shaker (under mattress) and a pillow shaker (all in T-3 pattern) and a strobe light in a modified T-3 pattern, all presented as shown in Table 1. This study found that the 400 Hz and 520 Hz square wave sounds were significantly more effective than the ∼3,100 Hz smoke alarm sound (93–100% of participants woke up at 75 dBA or less in contrast to only 62%, Figure 8). The bed and pillow shakers were not particularly effective (only 58–65% woke up at the intensity level as purchased), and the strobe lights were also not effective with only 24% of the young adults waking to the benchmark strobe light intensity and less than 70% at the highest intensity.
The 520 Hz square wave woke up all of the young adults with 0.05 BAC, making it much more effective than the strobe, pillow and bed shakers, and the ∼3,100 Hz smoke alarm sound (76%, 42%, 35% and 38%, respectively did not respond).
An earlier study [15], exploring the arousal threshold of deep sleeping young adults with 0.05 BAC in Stage 4 sleep to three alarm signals (female voice alarm, Australian smoke alarm and 520 Hz square wave T-3 alarm, all with no silences between sound levels), produced results that were consistent in terms of the differences in waking effectiveness of the beeping smoke alarm compared to the 520 Hz square wave, but different in that less awoke at comparable volumes (Figure 9).
3.2.5 Young adults with 0.08 BAC
Results from the same study but with 0.08 BAC were similar: the female voice and 520 Hz square wave T-3 alarm consistently resulted in faster response times than the Australian alarm signal (Figure 10) [15].
In summary, the more recent research studies have consistently shown that in the tested groups the 520 Hz square wave signal was much more effective than the current USA and Australian smoke alarm signals. The strobes were not effective, but the pillow and bed shakers were much more effective, but not as effective as the 520 Hz. Square wave sound.
4 Discussion
All of the people involved in these studies (except initially in the first [8]) were primed—they had knowledge of the alarm signals being tested and they knew they would be subjected to a signal. These factors were likely to lead to a better waking response than when the signal was completely unexpected. In addition, the people tested in these studies were not among those in the population most severely affected by their age, disability or condition. The older people who participated were, by virtue of the selection criteria, among the more active older people and had relatively good hearing amongst people of the same age. The hard of hearing participants were not subject to severe hearing loss, and the alcohol-affected people were young, not severely alcohol affected and did not have other disabilities. Therefore the results of these studies are likely to under-estimate the proportion of the population who will not respond to these signals from deep sleep in an unprimed, unscreened population.
There remain many vulnerable groups not yet tested. Such groups include people using sleeping tablets, people using other drugs that might affect sleep or response to signals during sleep, the deaf, and people with other physical or mental disabilities that might affect their response to a smoke alarm.
It is obvious from the results presented that the signal level and the type of sound or signal affected the probability that the participants did not respond. In our opinion it is likely that the response of other people to these signals will be similar and that it is therefore appropriate to seriously consider improved smoke alarm notification for the whole population based on this data.
Examination of Figures 5–10 indicates that it is necessary for the ∼3,100 Hz sound to be ∼20 dBA louder than the 520 Hz square wave sound for their effectiveness in waking people to be approximately equal. Three main possibilities for improved occupant response are apparent:
-
Replace the current 85 dBA smoke alarm sound with the 520 Hz square wave sound at 85 dBA
-
Retain the current sound but increase the sound level to 105 dBA
-
Require smoke alarms (current sound and level) in every room (perhaps excluding kitchens and bathrooms) and require interconnection
The first option is favoured by the authors based on the results of these studies. The second and third options are included above as they have been suggested in discussions in various forums.
The third option would be less effective than the other two as in many situations it would be likely to only increase the sound level at the pillow by ∼10 dBA.
The 520 Hz square wave sound is preferred by the authors as its effectiveness is less likely to be adversely affected as the population ages (as is happening in Australia, the USA and many other countries at present) compared with the ∼3,100 Hz smoke alarm sound, given that high frequency hearing loss is part of normal aging but is not recognised by many people until quite severe [33].
Of course, if the 520 Hz square wave sound was adopted the effectiveness of smoke alarms could be further enhanced by increasing the sound level to 95 or even 105 dBA.
As noted above the 520 Hz square wave has multiple peaks and several of these are within the speech frequency range where our hearing is most sensitive. The 520 Hz square wave peaks are more than a critical bandwidth apart so this increases the perceived loudness (although this is not reflected in the sound level measured by a sound meter). The perceived increase occurs because the different frequencies activate different parts of the basilar membrane [34]. In addition, the multiple frequency peaks are less likely to be masked by ambient noise than a single frequency sound and lower frequencies penetrate walls and doors better than higher frequencies [28].
It would be very beneficial to be able to estimate directly the overall effect on the frequency of fatalities of changes in smoke alarm requirements. The limitations mentioned above mean that there is great difficulty in generalising the current results to the whole population. Nevertheless, it is clear that when the smoke alarm signal level and other signal characteristics are set (in codes, etc.) effectively the overall fire fatality rate is being set, or at least strongly influenced. The reason it is not possible to accurately estimate the overall fatality rate is that needed information is missing: the missing information includes the proportion of the population in each vulnerable or at-risk group, the rate of fire starts for each of these groups (the rate of fire starts might vary considerably from the average over the whole population for some of the groups of at-risk people), the effectiveness of the current and alternative alarm signals in awakening sleeping people for all people in each at-risk group and the current fatality rates for each group. Research to obtain this missing data should be undertaken to facilitate possible further improvements in smoke alarms, and smoke alarm usage and effectiveness.
5 Conclusions and Recommendations
The 520 Hz square wave sound has consistently been found to be the most effective of the sounds tested in waking sleeping people. In all of the groups tested the 520 Hz square wave has resulted in waking most (generally all) of the people tested who did not awaken to very loud (95 dBA at the pillow) emissions of the current Australian and USA smoke alarm sounds. There is no reason to believe that this result would not apply to the entire population. Thus it appears that adoption of the 520 Hz square wave sound in the T-3 pattern as the standard smoke alarm sound would further reduce the rate of fatalities among sleeping people in fires (assuming current alarms have resulted in a reduction in domestic fire fatalities).
Among children and young adults (the latter both sober and at 0.05 BAC) the 520 Hz square wave signal reduced, by a factor of 6–10, the proportion of people not woken by the current signal. For adults with hearing loss this factor was six. In this group and the 0.05 BAC group the 520 Hz square wave sound was more effective than the bed and pillow shakers. When strobe lights were tested they were found to have very poor waking effectiveness, even though the highest intensity level tested was over three times higher than those required for strobes in the USA. A voice alarm was quite effective in the younger groups tested but much less so in the older adults. The voice alarm was also found to have real problems in waking participants with limited English.
It is therefore recommended that the 520 Hz square wave sound in the T-3 pattern be adopted to replace the current smoke alarm sounds as the alarm signal for all smoke alarms and that consideration also be given to increasing the required sound level, the required alarm locations and the interconnection of all smoke alarms.
References
AS 3786-1993, Smoke Alarms, Standards Australia, Sydney
NFPA 72 (2002) National fire alarm code. National Fire Protection Association, Quincy, MA
Thomas I, Ball M (2007) Consideration of domestic smoke alarms as a system, 10th suppression and detection research and applications conference (SUPDET2007). Retrieved 10th October 2007 from http://www.nfpa.org/assets/files//PDF/Proceedings/Consideration_of_Domestic_Smoke_Alarms_as_a_Sytsem_-_I.Thoma.pdf
Lee A (2005) The audibility of smoke alarms in residential homes, CPSC-ES-0503. US Consumer Product Safety Commission, Bethesda, MD. Retrieved 12th November 2007 from http://www.cpsc.gov/LIBRARY/FOIA/foia05/os/audibility.pdf
ABCB (2008) Building code of Australia volumes 1 and 2, Class 2. Australian Building Codes Board, Canberra
Ball M, Watts-Hampton T, Thomas I (2007) Domestic smoke alarms, which is best and how effective are they? A literature and statistics study. Centre for Environmental Safety and Risk Engineering, Victoria University, Melbourne, March (prepared for the Bushfire Cooperative Research Centre)
Peacock RD, Averill JD, Bukowski RW, Reneke PA. (2005) Home smoke alarm project, manufactured home tests. Retrieved 3/02/2006 from http://www.smokealarm.nist.gov/Series1.htm
Bruck D, Horasan M (1995) Non-arousal and non-action of normal sleepers in response to a smoke detector alarm. Fire Safety J 25:125–139
Bruck D (1998) Arousal from sleep with a smoke detector in children and adults technical report FCRC-TR 98-04. Fire Code Reform Centre, Sydney
Bruck D (1999) Non-awakening in children in response to a smoke detector alarm. Fire Safety J 32:369–376
Bruck D, Bliss RA (2000) Sleeping children and smoke alarms. In: Proceedings of the 4th Asia-Oceania symposium on fire science and technology. Asia-Oceania Association for Fire and Technology, Tokyo, pp 602–613
Bruck D, Brennan P (2001) Recognition of fire cues during sleep. In: Proceedings of the 2nd international symposium on human behaviour in fire. London, Interscience Communications, pp 241–252
Bruck D (2001) The who, what, where and why of waking to fire alarms: a review. Fire Safety J 36(7):623–639
Bruck D, Reid S, Kouzma J, Ball M (2004) The effectiveness of different alarms in waking sleeping children. In: Proceedings of the third human behaviour in fire conference. Belfast, 1–3 October, Interscience Communications, London, pp 279–290
Ball M, Bruck D (2004a) The effect of alcohol upon response to fire alarm signals in sleeping young adults. In: Shields J (ed.) In: Proceedings of the third human behaviour in fire conference. Belfast, 1–3 October, Interscience Communications, London, pp 291–302
Ball M, Bruck D (2004b) The salience of fire alarm signals for sleeping individuals: a novel approach to signal design. In: Shields J (ed) In: Proceedings of the third human behaviour in fire conference. Belfast, 1–3 October, Interscience Communications, London pp 303–314
Bruck D, Ball M (2005) Sleep and fire: who is at risk and can the risk be reduced? In: Proceedings of the 8th international symposium of the international association for fire safety science. Beijing
Bruck D, Thomas I (2006) Reducing fire deaths in older adults: investigation of auditory arousal with different alarm signals in sleeping older adults. Report for the Fire Protection Research Foundation. Retrieved 10th October 2007 from http://www.nfpa.org/assets/files//PDF/Research/Investigation_of_Auditory_Arousal.pdf
Bruck D, Thomas I (2007) Waking effectiveness of alarms (auditory, visual and tactile) for adults who are hard of hearing. Report for the Fire Protection Research Foundation. Retrieved 10th October 2007 from http://www.nfpa.org/assets/files//PDF/Research/hardofhearing&alarms.pdf
Bruck D, Thomas I, Ball M (2007) Waking effectiveness of alarms (auditory, visual and tactile) for the alcohol impaired. Report for the Fire Protection Research Foundation. Retrieved 10th October 2007 from http://www.nfpa.org/assets/files//PDF/Research/alcohol&alarmsreport.pdf
Bruck D, Thomas I (2007) A different smoke alarm signal will awaken many people more effectively. Sleep Biol Rhythms 5:A3
Ball M (2007) Cognitive processing during sleep: the role of signal significance and participant characteristics, PhD Thesis. Victoria University, Melbourne, Australia, Ch 6
Zepelin H, McDonald CC, Zammit GK (1984) The effects of age on auditory awakening. J Gerontol 39(3):294–300
Thomas IR, Verghese D (2001) CESARE-RISK: a summary report, Victoria University and Fire Code Reform Centre Ltd., Melbourne
Thomas IR, Brennan P (2002) Injuries and fatalities in apartment building fires. International association for fire safety science—proceedings of the seventh international symposium, pp 1085–1096
ISO 8201 (1987) Acoustics—Audible Emergency Evacuation Signal, International Standards Organisation, Geneva, Switzerland
Proulx G, Laroche C (2003) Recollection, identification and perceived urgency of the temporal-three evacuation signal. J Fire Prot Eng 13:67–82
Bruck D, Ball M (2007) Optimizing emergency awakening to audible smoke alarms: an update. Human Factors 49(4):585–601
Du Bois J, Ashley E, Klassen M, Roby R (2005) Waking effectiveness of audible, visual and vibratory emergency alarms on people of all hearing levels, In: Proceedings of the accessible emergency notification and communication: state of the science conference. Gallaudet University, Washington, DC, 2–3 Nov. Retrieved on 27th August 2006 from http://www.tap.gallaudet.edu/EmergencyConf/Papers/Du%20Bois.htm
Smith G, Splaingard M, Hayes J, Xiang H (2006) Comparison of a personalised parent voice smoke alarm with conventional residential tone smoke alarm for awakening children. Pediatrics 118:1623–1632
Bowman SK, Jamieson DG, Ogilvie RD (1995) Waking effectiveness of visual alerting signals. J Rehabil Res Dev 32:43–62
Hasofer AM, Bruck D (2004) Statistical analysis of response to fire cues. J Fire Safety 39:663–688
Cruickshanks KJ, Wiley T, Tweed T, Klein B, Klein R, Mares-Perlman JA et al (1998) Prevalence of hearing loss in older adults in Beaver Dam, Wisconsin: the epidemiology of hearing loss. Am J Epidemiol 148:879–886
Zwicker E, Flottorp G, Stevens SS (1957) Critical band widths in loudness summation. J Acoust Soc Am 29:548–557
Acknowledgement
These studies were financially supported by the Fire Protection Research Foundation, Australian Research Council, OneSteel and Umo Lai. Results in [15] are from the PhD research of Michelle Ball.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Thomas, I., Bruck, D. Awakening of Sleeping People: A Decade of Research. Fire Technol 46, 743–761 (2010). https://doi.org/10.1007/s10694-008-0065-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10694-008-0065-5