
Abstract
To test whether alarms that are effective in awakening children and prompting their escape are also effective among older adults 60 to 84 years old. These two age groups are at highest risk of residential fire-related death. Using a randomized, non-blinded, repeated measures design, 31 older adults were exposed during the N2 or N3 sleep stages to four different smoke alarms signals: female voice, low-frequency tone, female voice combined with low-frequency tone (hybrid alarm), and high-frequency tone. The median age of study subjects was 62.0 years and 87.1% were female. All (n = 31) subjects awakened and performed the escape procedure to all four alarms; The median time-to-awaken was 1.0 s for all four alarms and the median time-to-escape was 4.0 s for the female voice alarm and 5.0 s for the other three alarms. Pairwise comparisons among all four alarms did not show any significant differences in the probability functions for time-to-awaken or time-to-escape. Older adult participants rapidly awakened and performed the escape procedure to all the alarm types tested. Study results suggest that smoke alarms that were developed for the unique developmental requirements of sleeping children are also effective among sleeping older adults. The findings of this study contribute to identification of smoke alarm signals that are effective for individuals of all ages.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Residential fires are an important cause of injury and death in the United States (US) and smoke alarms represent a core prevention strategy. When residential alarms were initially developed, the focus was on detection technologies for smoke or heat, with little attention directed towards effectiveness of the alerting signal, including during sleep [1]. However, arousing sleeping individuals and alerting them to a residential fire emergency is important because the rate of apartment fire-related mortality is three times higher during the sleep period of 1:00 to 7:00 a.m. than other times [2]. Although the high-frequency tone alarms found in many households awaken most adults, they are not effective in awakening children [3,4,5,6,7,8,9,10]. Smith and colleagues previously demonstrated that 96% of children 6 to 12 years old awoke and 83% performed an escape procedure in response to an alarm using their mother’s voice, which was significantly better than their response to a high-frequency tone alarm [9]. Based on the success of this maternal voice alarm, they subsequently embarked on a series of studies to determine which characteristics of the alarm signal were critical for its effectiveness [6,7,8]. Smith et al. [7, 8] showed that personalizing the voice alarm signal with the child’s first name or mother’s voice did not increase alarm effectiveness. They then demonstrated that a low-frequency tone alarm and a female voice alarm each performed better than comparator alarm signals [8]. Additionally, they showed that alarms using a male voice, female voice, or a combination of a female voice and a low-frequency tone were each significantly more effective than a high-frequency tone alarm, but that there were no significant pairwise differences in effectiveness when those three alarms were compared with each other [6]. These findings among sleeping children are generally consistent with those of Bruck and colleagues but using different study methods [11,12,13]. Because it is impractical to have separate alarms for children and adults in a household, Smith et al. then tested the low-frequency tone and female and male voice alarms, which were effective among sleeping children, among sleeping adults 20 to 49 years old and demonstrated that they were also highly effective in the adult population [14].
It is important that smoke alarms developed for the unique developmental requirements of sleeping children also be evaluated among sleeping older adults. Residential fire fatality rates increase rapidly during the later years of life. Based on 2011 to 2015 annual averages, individuals 65 to 74 years old have a residential fire fatality rate almost twice that of the overall population, and those 75 to 84 years old have a rate that is more than two-and-a-half times higher than the overall national average [15]. In 2015, adults 65 years and older represented 15% of the US population but accounted for 40% of fire deaths [16]. In addition, the US population is aging. In 2000, individuals 65 years and older accounted for 12% of the population and by 2050, they are projected to represent 21% of the US population [17]. A number of factors place older adults at higher risk for residential fire-related injury and death, including diminished sensory and mental abilities, increased prevalence of disability and poor health, and poverty [17]. These factors increase the risk of fire occurrence, limit an individual’s ability to detect a fire and escape, and impede recovery from fire-related injury.
Bruck and colleagues is the only research team that previously has conducted a study comparing different types of alarms among sleeping older adults [1, 18]. They tested three alarms, including a male voice alarm, among 42 subjects and concluded that voice alarms should not be used for adult populations. Therefore, given this conclusion, testing the voice alarms that Smith et al. found to be effective among children in the older adult population was especially important.
The objective of this study was to test smoke alarms among sleeping older adults that Smith and colleagues had previously shown to be effective among sleeping children 5 to 12 years old. The study tested whether older adults would awaken and perform an escape procedure in response to a smoke alarm that uses a female voice, low-frequency tone, or a combination of the female voice and low-frequency tone (hybrid alarm); a comparator high-frequency tone alarm was also included in the study. The findings of this study contribute to identification of smoke alarm signals that are effective for individuals of all ages. This study promotes the goal of reducing residential fire-related injuries and deaths among children old enough to perform self-rescue and among older individuals in the household.
2 Methods
2.1 Study Population and Definitions of Sleep Stages
The study population consisted of older adults, who were recruited via study announcements using institution-wide emails in a large academic children’s hospital and the hospital’s Facebook page. Individuals were eligible to enroll in the study if they (1) were 60 to 84 years old, (2) did not have a medical condition and were not taking a medication that might affect sleep, arousal, or their ability to perform the study’s escape procedure, (3) did not have a hearing impairment, (4) did not have an acute illness at the time of the study, and (5) spoke English. To participate in the study, participants had to pass a pure-tone hearing screening test on the first night of the study using a Maico MA25 portable audiometer and had to successfully respond to all tested frequencies of 500, 1000, 2000, and 4000 Hertz (Hz) at ≤ 55 decibels (dB) in both ears. This study was approved by the institutional review board of the authors’ institution. Written informed consent was obtained from study participants. Participants were compensated monetarily for their time.
Sleep consists of three non-rapid eye movement stages (N1, N2, and N3) followed by a rapid eye movement (REM) stage that cycle throughout the night with each person experiencing 4 to 5 sleep cycles per night. Each consecutive non-REM sleep stage is characterized by progressive slowing of the electroencephalography (EEG) wave patterns. The N2 and N3 sleep stages are the ones relevant to this study. N2 sleep is defined as occurring (in absence of criteria for N3) if either or both of the following occur during the first half of a 30-s EEG/polysomnography (PSG) epoch or the last half of the previous epoch: (1) one or more K complexes unassociated with arousals, and (2) one or more sleep spindles [19]. N3 sleep is defined as high voltage (> 75 microvolts peak-to-peak amplitude), slow wave (0.5 to 2 Hz) EEG activity accounting for ≥ 20% of a 30-s epoch, measured over the frontal regions [19]. N3 sleep was formerly separated into stage 3 sleep (S3S) and stage 4 sleep (S4S) under an older nomenclature, in which N3 began with S3S and then progressed into S4S, which is characterized by the slow wave, high voltage (delta wave) activity accounting for > 50% of a 30-s EEG/PSG epoch [20].
This study was conducted separately for the ≥ 60-year-old age group because of the lower prevalence of N3 sleep and greater prevalence of hearing loss among older adults, as well as modifications needed in the escape procedure to ensure participant safety. In previous studies, the escape procedure consisted of the subject getting out of bed after being awakened by an alarm, walking to the bedroom door, and exiting. However, there was concern that this may present a fall risk to older individuals in an unfamiliar environment who may experience transient confusion associated with sleep inertia upon awakening. The escape procedure in this study consisted of the participant sitting up in bed and pushing a one-inch-in-diameter glowing button mounted on the wall by the bed upon being awakened by an alarm. The button was positioned so that the participant would need to sit up to reach it.
2.2 Study Design
This study used a randomized, non-blinded, repeated measures design to evaluate the ability of the study alarms to awaken individuals and prompt their performance of an escape procedure. Participants were each exposed during the N2 or N3 sleep stage of separate sleep cycles to these four smoke alarm signals: female voice, low-frequency tone, female voice combined with low-frequency tone (hybrid alarm), and high-frequency tone. The voice message used in the female voice and hybrid alarms was “Fire! Fire! Wake up! Get out of bed! Leave the room!” An auditory arousal threshold (AAT) is the intensity level in decibels (dB) of an auditory stimulus required to awaken an individual from sleep. The repeated measures design used by this study avoids potential confounding due to variation of AATs among individuals (inter-subject variability can be high) and takes advantage of the stability of AATs for an individual across sleep cycles (intra-subject variability is low) [21,22,23].
The female voice, low-frequency tone, and hybrid alarms used in this study have been shown to effectively awaken children 5 to 12 years old from S4S and prompt their performance of an escape procedure upon awakening [6, 8]. In addition, the female voice and low-frequency tone alarms have each separately been demonstrated to do the same for adults 20 to 49 years old in S4S [14]. Although the low-frequency tone alarm was adopted in 2014 as the United States standard for commercial sleeping areas, such as in hotels and motels, it is not the standard for residential sleeping areas unless being provided voluntarily for individuals with hearing loss [24]. A high-frequency (approximately 3200 Hz) tone alarm was also included in this study because it is the alarm type currently found in many homes. The low-frequency (500 Hz square wave) alarm employed in this study was a Simplex 1996, 4100 Fire Alarm and is the same alarm previously used in studies by Proulx and Laroche [25], Bruck et al. [26], and Smith et al. [8, 14]. The hybrid alarm was developed because a previous study had showed that the low-frequency tone was marginally better at awakening children 5 to 12 years old but had a somewhat longer time-to-escape than the female voice alarm [8]. Therefore, it was hypothesized that there may be advantages to combining these signals into one alarm and that the voice message may provide valuable instructions and urgency regarding life-saving escape behaviors during the period of confusion associated with sleep inertia upon awakening that could shorten the time-to-escape [27, 28]. This hybrid alarm performed well among children but has not been tested among older adults, and therefore merits investigation [6]. In addition, inclusion of a hybrid alarm is novel because only one other study has evaluated an alarm that uses a shift pattern among sleeping individuals and that study did not include older adults [29].
Based on the Latin Square shown in Table 1, four sequences of alarm signals were used to minimize the possibility of a sequence effect. Block randomization (in blocks of four) of these sequences was performed and then placed in sequentially numbered sealed envelopes by a research assistant, who was not involved with study enrollment or conducting the study. Study participants received the next available envelope upon arrival for their first study night, and only study staff knew the assigned alarm sequence after the envelope was opened. Alarm signals were amplified through small, smoke alarm-size speakers in the study bedrooms, which provided consistent signals at 85 dB when measured at the pillow. This is louder than required by the National Fire Alarm and Signaling Code (NFPA 72) and the UL 217 Standard for Smoke Alarms, which is 85 dB at 10 feet [25, 30]. Study rooms were comfortably decorated to resemble a typical residential setting.
Subjects were taught the escape procedure on the night of the study prior to going to sleep. Sleep stage was monitored to ensure that alarms were all triggered during the N2 or N3 sleep stages, which minimized the potential for comparisons among alarm signals to be influenced by the sleep stage variability of AATs. After bedroom lights were turned off, continuous EEG, electro-oculography, and chin electromyography via telemetry with synchronized low-light video monitoring were conducted by a PSG technician. The EEG montage consisted of F3, F4, C3, C4, O1, O2, M1, and M2 electrodes.
2.3 Testing Protocol and Measurements
The goal was to trigger the alarm during N3 sleep because N3 is the sleep stage with the highest AAT and therefore the most refractory to arousal [10]. The alarm was triggered after a subject was in N3 sleep for 2 min or in S4S for 30 s, whichever occurred first. However, N3 and especially S4S occur less often among older adults and may not occur at all for some individuals in this age group [31]; therefore, the alarm was triggered for subjects who were still in N2 after 30 min in that sleep stage. “Time-to-awaken” is the interval from the triggering of the alarm to the initiation of at least a 3-s arousal associated with movement and subsequent awake EEG. The interval from when the alarm was triggered until the study participant pushed the “escape button” on the wall by the bed is the “time-to-escape.” This procedure was conducted during the first and second sleep cycles on two separate study nights at least 6 days apart, resulting in each subject being exposed to four different alarm signals (two different signals each night). Testing on consecutive nights was not done to avoid the possibility of confounding effects attributable to sleep deprivation and altered sleep architecture. A senior certified PSG technician determined the “time-to-awaken” from the EEG-video recordings. The sleep stage during which an alarm was triggered and the “time-to-awaken” interval were later reviewed and verified by one of the authors, who is a physician board-certified in sleep medicine, while blinded to the alarm used. No discrepancies were identified during this review.
2.4 Statistical Analysis
Statistical analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC). The Kaplan–Meier estimator was used to estimate the probability functions for time-to-awaken and time-to-escape. The generalized Wilcoxon test was used to assess the overall equality and pairwise comparisons of time-to-awaken and time-to-escape probability functions. Hazard ratios (HRs) with Wald’s 95% confidence intervals (CIs) were calculated for each pair of alarms. The hazard ratio is a comparison between the probability of events (in this case, awakenings or escapes) in one treatment group compared with the probability of events in another group. A hazard ratio of 1 means that both groups are experiencing an equal number of events at any point in time [32]. Statistical significance was determined at p < 0.05.
3 Results
Among the 31 study subjects, the median age was 62.0 years (interquartile range [IQR]: 61.0 to 65.0) and 27 (87.1%) were female. Twenty-two participants (71.0%) were awakened from N3 sleep, including 8 subjects (25.8%) from S3S and 14 (45.2%) from S4S; 9 subjects (29.0%) were awakened from N2 sleep. All subjects awoke and successfully performed the escape procedure in response to all four alarms. The median time-to-awaken from N2 sleep and S4S was 1.0 s, while the median time-to-awaken from S3S was 1.1 s. In addition, the median time-to-escape from N2 sleep and S4S was 4.3 s, while the median time-to-escape from S3S was 5.3 s. The median time-to-awaken and time-to-escape by type of alarm and sex are shown in Table 2.
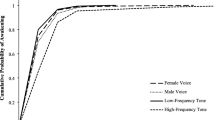
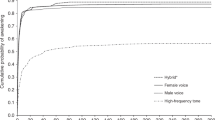
The cumulative probabilities of awakening and escaping for the four alarms are shown in Figs. 1 and 2, respectively. Overall, there were no significant differences in the probability functions for time-to-awaken (Wilcoxon, p = 0.43) or time-to-escape (Wilcoxon, p = 0.75) among the alarms (Table 3). The median time-to-awaken was 1.0 s for each of the alarms (Table 2). Pairwise comparisons among the four alarms did not show any significant differences in the probability functions for time-to-awaken (Table 3). The median time-to-escape was 4.0 s for the female voice alarm and 5.0 s for the other three alarms (Table 2). Pairwise comparisons among the four alarms did not show any significant differences in the probability functions for time-to-escape (Table 3). The median time-to-awaken and time-to-escape varied by no more than 0.5 s by sex among the four alarm types (Table 2).

Cumulative probability of awakening by type of alarm

Cumulative probability of escape by type of alarm
4 Discussion
All alarms in this study consistently and rapidly awoke older adults and prompted performance of the escape procedure, regardless of whether they were in N2 or N3 sleep. Unlike previous studies by Smith et al. this study did not show any significant differences in time-to-awaken or time-to-escape among the different types of alarms [6,7,8,9, 14]. This is unlikely to be simply attributable to sample size because the median time-to-awaken (1 s) and median time-to-escape (4 to 5 s) were uniformly exceedingly short for each type of alarm. In contrast, previous studies among children 5 to 12 years old demonstrated that the performance of the high-frequency tone alarm was clearly inferior to that of the other types of alarms (Tables 4 and 5) [6,7,8,9]. These results suggest that the female voice, low-frequency tone, and hybrid alarms, which are effective in awakening and prompting escape among sleeping children, are also effective among sleeping older adults. This is important because it is impractical to have separate alarms for individuals of different ages in a household.
Smoke alarms should be able to awaken sleeping individuals across the age range, including children, and prompt their escape in the event of a residential fire. Children 5 to 12 years old have a higher residential fire fatality rate than teenagers and adults up to age 35 years [15], and although they are potentially capable of self-rescue in a residential fire, they are unlikely to awaken to the high-frequency tone smoke alarm found in many homes [4, 7, 10]. This study and previous smoke alarm research with children by Smith, et al. have contributed to the relatively small literature on this topic [11,12,13, 26, 33] and employed improvements in study methodology, such as monitoring and controlling for sleep stage, using a repeated measures design to mitigate the potential effects of inter-subject variation in AATs [22, 23], and including an escape procedure. Inclusion of an escape procedure is important because a person not only needs to awaken, but also needs to escape in a fire emergency.
Voice smoke alarms have the potential benefit of being able to provide emotional and instructional content that may facilitate a quicker escape, especially during the sleep inertia-associated confusion experienced upon awakening [27]. Previous studies by Smith and colleagues have demonstrated that voice alarms do not have to be personalized for effectiveness, such as using a voice message that includes the child’s first name or the mother’s voice. This is important because smoke alarms that use a generic recorded message can be manufactured at a lower cost and can be installed without the effort of personalization by consumers. The decreased cost and increased ease of installation increases the likelihood that the alarms will be used and installed correctly [34]. However, the only other study that has evaluated smoke alarms among sleeping older adults concluded that “the option of a voice alarm should no longer be considered for adult populations” [1]. The findings of the current study do not support that conclusion. This is likely attributable, in part, to the use of different study methods; the most important being the use of different outcome measures based on the sound delivery procedure used. Bruck et al. delivered the signal for each alarm at escalating volume levels, starting at 35 dB (at the pillow) and increasing by 5 dB every 30 s until awaking occurred, with a maximum volume of 95 dB. AATs for each alarm type were compared during data analysis [18]. In contrast, the current study delivered alarm signals at a constant level of 85 dB at the pillow and compared the frequencies of awakening and escaping and the times-to-awaken and -escape among alarms. We prefer our alarm delivery method because we have had many child study subjects with times-to-awaken that were greater than 30 s, which means that some individuals required more than a 30-s window (as used by Bruck and colleagues) for awakening at a constant alarm volume level. The presentation of an alarm signal in escalating volume increments also does not mimic real-world emergency fire alarm conditions, in which a signal is presented at a single volume and the times-to-awaken and -escape are directly relevant to survival.
Another difference in methods between the study by Bruck, et al. and the current study is that researchers in the previous study waited for subjects to be in N3 sleep for 90 s before triggering the alarm, while the criteria used in the current study were 2 min in N3, 30 s in S4S, or 30 min in N2 [18]. Sleep stage at the time of alarm initiation was not related to awakening or escaping in the current study; therefore, this methodological difference between studies is unlikely to have influenced conclusions. Additionally, the median age of subjects in the current study was 62 years and the mean age in the previous study was 73.1 years; this age difference may have influenced study findings [18]. However, all participants in the current study quickly awakened and performed the escape procedure to all alarm types tested, demonstrating no influence of age on response. In addition, conclusions of the previous study may be over-generalized from a male voice alarm to all voice alarms and from older adults to all “adult populations.” They also stated that “the voice alarm was also found to have real problems in waking participants with limited English;” however, there were only three non-native speakers in the study and their degree of English fluency was not documented [35]. The current study did not assess the effect of English fluency on voice alarm performance.
The high-frequency tone alarm may perform less effectively among the general population of older adults than in this study, especially when the smoke alarm is located outside of a closed bedroom. There are two reasons for this. First, this study was conducted among a select group of older adults, excluding those with hearing impairments. High-frequency hearing loss, presbycusis, is a part of normal aging and may limit the effectiveness of alarms using high-frequency signals in the older population [36]. Second, high-frequency sounds are not transmitted as well as low-frequency sounds through closed doors and walls in the home. Energy from a 500 Hz smoke alarm signal is better transmitted through these barriers, while more of the energy from a 3200 Hz alarm signal is reflected [37,38,39]. The NFPA 72, National Fire Alarm and Signaling Code recommends that smoke alarms be installed inside every sleep room in addition to outside those rooms and on each level of a home [24]. Consistent with these national recommendations, study alarms were positioned inside the sleep rooms. Although smoke alarms, especially high-frequency alarms, located outside of a closed bedroom in the real world may not awaken sleeping individuals as well, the number of adverse outcomes attributable to decreased notification of a fire because of a closed bedroom door are considered to be relatively small [38].
4.1 Study Limitations
This study had some limitations. It was conducted among healthy older adults without any hearing problems or medication use that could affect sleep; therefore, results may not be generalizable to the entire older adult population. The alarm intensity was 85 dB at the pillow, which is louder than required by the National Fire Alarm and Signaling Code (NFPA 72) and the UL 217 Standard for Smoke Alarms. This study had a relatively small sample size; however, it is similar in size to the only other study of the effectiveness of different smoke alarms among older adults (n = 42); in addition, it is unlikely that a larger study sample would change the conclusions of the study because the median time-to-awaken (1 s) and median time-to-escape (4 to 5 s) were uniformly and exceedingly short for each type of alarm. This is consistent with previous research showing that older individuals awaken more easily than younger people, especially children [4, 23]. The study did not include an adaptation night, which is often employed to avoid a “first night effect.” However, such an effect was minimized by the repeated measures study design and by waking study participants from N2 or N3 sleep; these deeper stages of sleep are least influenced by potential confounders because of decreased cortical arousability [21]. To reduce the potential for falls among the older adult participants, the escape procedure in this study was limited to sitting up in bed and pushing a button rather than getting out of bed, walking to the bedroom door and exiting, which was done in previous studies among younger individuals by Smith et al. In addition, participants rehearsed the escape procedure immediately before falling asleep, which may have affected the time-to-escape; however, escape times were very short and demonstrated little variability among these older adult subjects.
5 Conclusions
Older adult participants rapidly awakened and performed the escape procedure to all the alarm types tested. The objective of this study was to test smoke alarms among sleeping older adults that had previously been shown to be effective among sleeping children 5 to 12 years old. Study results suggest that the female voice, low-frequency tone, and hybrid alarms, which are effective in awakening and prompting escape among sleeping children, are also effective among sleeping older adults. The findings of this study contribute to identification of smoke alarm signals that are effective for individuals of all ages. This study promotes the goal of reducing residential fire-related injuries and deaths among children old enough to perform self-rescue and among older individuals in the household.
Data Availability
The dataset analyzed during the current study is available from the corresponding author on reasonable request for research purposes following completion of publication of findings based on this dataset.
Abbreviations
- AAT:
-
Auditory arousal threshold
- CI:
-
Confidence interval
- dB:
-
Decibel
- EEG:
-
Electroencephalography
- HR:
-
Hazard ratio
- Hz:
-
Hertz
- IQR:
-
Interquartile range
- PSG:
-
Polysomnography
- REM:
-
Rapid eye movement
- S3S:
-
Stage 3 sleep
- S4S:
-
Stage 4 sleep
References
Geiman JA, Gottuk DT (2006) Reducing fire deaths in older adults: optimizing the smoke alarm signal research project; summary technical report. The fire protection research foundation, Quincy, MA. https://www.sustainable-design.ie/fire/NFPA_Summary-Report_2006_Fire-Older-Auditory-Arousal.pdf. Accessed December 14, 2020.
Bruck D, Ball M (2007) Optimizing emergency awakening to audible smoke alarms: an update. Hum Factors 49(4):585–601
Bruck D, Horasan M (1996) Non-arousal and non-action of normal sleepers in response to a smoke detector alarm. Fire Saf J 25:125–139
Busby KA, Mercier L, Pivik RT (1994) Ontogenetic variations in auditory arousal threshold during sleep. Psychophysiology 31(2):182–188
Nober EH, Pierce H, Well A (1981) Waking effectiveness of household smoke and fire detection devices. Fire J 75:86–130
Smith GA, Chounthirath T, Splaingard M (2020) Comparison of the effectiveness of female voice, male voice, and hybrid voice-tone smoke alarms for sleeping children. Pediatr Res 88(5):769–775
Smith GA, Chounthirath T, Splaingard M (2019) Effectiveness of a voice smoke alarm using the child’s name for sleeping children: a randomized trial. J Pediatr 205:250–256
Smith GA, Chounthirath T, Splaingard M (2020) Do sleeping children respond better to a smoke alarm that uses their mother’s voice? Acad Pediatr 20(3):319–326
Smith GA, Splaingard M, Hayes JR, Xiang H (2006) Comparison of a personalized parent voice smoke alarm with a conventional residential tone smoke alarm for awakening children. Pediatrics 118(4):1623–1632
Underwriters laboratories, smoke alarm STP research group (2003) Report from the UL smoke alarm STP research group on childhood awakening in response to smoke alarms. Underwriters Laboratories, Northbrook, IL
Bruck D (1999) Non-awakening in children in response to a smoke detector alarm. Fire Saf J 32(4):369–376
Bruck D, Bliss RA (2000) Sleeping children and smoke alarms. In: Yamada T (ed) Proceedings of the fourth Asia-Oceania symposium on fire science and technology. Tokyo, Japan: Asia-Oceania symposium on fire science and technology 602–613
Bruck D, Reid S, Kouzma J, Ball M (2004) The effectiveness of different alarms in waking sleeping children. Proceedings from the 3rd international symposium on human behaviour in fire; Belfast, Ireland 279–289
Smith GA, Kistamgari S, Splaingard M (2020) Optimizing smoke alarm signals: testing the effectiveness of children’s smoke alarms for sleeping adults. Inj Epidemiol 7:51
Ahrens M (2018) Home fire victims by age and gender. National fire protection association, Quincy, MA. https://www.nfpa.org//-/media/Files/News-and-Research/Fire-statistics-and-reports/Building-and-life-safety/oshomevictims.pdf. Accessed December 14, 2020
United states fire administration (2020) Fire safety outreach materials for older adults. United States fire administration, federal emergency management agency, department of homeland security, Washington DC; https://www.usfa.fema.gov/prevention/outreach/older_adults.html Accessed December 14, 2020
United states fire administration (2006) Fire and the older adult. FA-300. United States fire administration, national fire data center. Federal emergency management agency, department of homeland security, Washington DC. https://www.usfa.fema.gov/downloads/pdf/statistics/fa-300.pdf. Accessed December 14, 2020
Bruck D, Thomas I (2008) Comparison of the effectiveness of different fire notification signals in sleeping older adults. Fire Technol 44(1):15–38
Berry RB, Brooks R, Gamaldo CE et al (2016) The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. American Academy of Sleep Medicine, Darien, IL
Rechtschaffen A, Kales A (1968) A manual of standardized terminology, techniques and scoring systems for sleep stages of human subjects. US Government Printing Office, Washington, DC
Bonnet MH, Johnson LC, Webb WB (1978) The reliability of arousal threshold during sleep. Psychophysiology 15(5):412–416
Bruck D (2001) The who, what, where and why of waking to fire alarms: a review. Fire Saf J 36(7):623–639
Zepelin H, McDonald CS, Zammit GK (1984) Effects of age on auditory awakening thresholds. J Gerontol 39(3):294–300
National fire protection association (2019) NFPA 72: national fire alarm and signaling code. National Fire Protection Association, Quincy, MA
Proulx G, Laroche C (2003) Recollection, identification and perceived urgency of the temporal-three evacuation signal. J Fire Prot Eng 13(1):67–82
Bruck D (1998) Technical report FCRC-TR 98–04: arousal from sleep with a smoke detector alarm in children and adults. http://www.abcb.gov.au/-/media/Files/Resources/Research/FCRC-TR-98-04-Arousal-from-sleep-smoke-detector-in-children-and-adults.pdf. Accessed May 22, 2020
Hellier E, Edworthy J, Weedon B, Walters K, Adams A (2002) The perceived urgency of speech warnings: semantics versus acoustics. Hum Factors 44(1):1–17
Smith JJ, Wogalter MS (2007) Perceived effectiveness of warning messages for use as vocal warnings in residential fire alarms. Proc Hum Factors Ergo Soc Annu Meet 51(20):1398–1402
Ball M, Bruck D (2004) The salience of fire alarm signals for sleeping individuals: a novel approach to signal design. In proceedings of the 3rd international symposium on human behaviour in fire. Belfast, Ireland. 303–314
Laboratories Underwriter (2020) UL 217 Standard for smoke alarms, Edition 9. Underwriters Laboratories, Northbrook, IL
Dement WC (2016) Normal human sleep. In: Kryger MH, Roth T, Dement WC (eds) Principles and Practice of Sleep Medicine, 6th edn. Elsevier
Glen S (2021) Hazard ratio: definition, examples and log of the hazard. In StatisticsHowTo.com. Elementary statistics for the rest of us! www.statisticshowto.com/hazard-ratio/. Accessed May 21, 2021
Bruck D, Thomas IR (2012) Community-based research on the effectiveness of the home smoke alarm in waking up children. Fire Mater 36(5–6):339–348
Baker SP (1981) Childhood injuries: the community approach to prevention. J Public Health Policy 2(3):235–246
Thomas I, Bruck D (2010) Awakening of sleeping people: a decade of research. Fire Technol 46:743–761
Cruickshanks KJ, Wiley TL, Tweed TS et al (1998) Prevalence of hearing loss in older adults in Beaver Dam, Wisconsin. The epidemiology of hearing loss study. Am J Epidemiol 148(9):879–886
Dinaburg JB (2020) Audible alarm signal waking effectiveness: literature review. Report number FPRF-2020–04. Quincy, MA: fire protection research foundation, national fire protection association
Olenick SM, Boehmer H, Klassen MS (2019) Door messaging strategies: implications for detection and notification. Report number FPRF-2019–12. Quincy, MA: fire protection research foundation, national fire protection association
Quirt JD (1987) Sound transmission through building components. Noise control in buildings: proceedings of building science insight. Institute for research in construction, national research council of Canada. Canada. 23–38. https://nrc-publications.canada.ca/eng/view/object/?id=86fc10e0-885c-41c5-8608-aef1933bd77d. Accessed December 14, 2020
Funding
This research was supported by a grant from the National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (grant # R49CE002106; principal investigator: Gary A. Smith). The interpretations and conclusions in this article do not necessarily represent those of the funding organization. The funding organization was not involved in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
GS contributed substantially to the conception and design of the study, acquisition of data, and analysis and interpretation of data; he drafted the article, approved the final version to be published, and agrees to be accountable for all aspects of the work. SK conducted data analyses and contributed substantially to interpretation of data; she revised the article critically for important intellectual content, approved the final version to be published, and agrees to be accountable for all aspects of the work. MS contributed substantially to the conception and design of the study, acquisition of data, and interpretation of data; he revised the article critically for important intellectual content, approved the final version to be published, and agrees to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of interest
The authors do not have any conflicts of interest/competing interests to disclose.
Ethical Approval
This study was approved by the institutional review board of the authors’ institution.
Consent to Participate
Written informed consent was obtained from study participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Smith, G.A., Kistamgari, S. & Splaingard, M. Optimizing Smoke Alarm Signals for Those at Highest Risk for Residential Fire-Related Death: Testing the Effectiveness of Children’s Smoke Alarms for Sleeping Older Adults. Fire Technol 58, 311–326 (2022). https://doi.org/10.1007/s10694-021-01147-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10694-021-01147-5