
Abstract
Urothelial bladder carcinoma (UBC) is the most common among urinary bladder neoplasms. We carried out a preliminary study to determine the genetic etiology of UBC in Pakistani population, for this 25 sequence variants from 17 candidate genes were studied in 400 individuals by using polymerase chain reaction-based techniques. Multivariate logistic regression analysis was performed for association analysis of the overall data as well as the data stratified by smoking status, tumor grade and tumor stage. Variants of GSTM1, IGFBP3, LEPR and ACE were found to be associated with altered UBC risk in the overall comparison. CYP1B1 and CDKN1A variants displayed a risk modulation among smokers; IGFBP3 and LEPR variants among nonsmokers while GSTM1 polymorphism exhibited association with both. GSTM1 and LEPR variants conferred an altered susceptibility to low grade UBC; GSTT1, IGFBP3 and PPARG variants to high grade UBC while ACE polymorphism to both grades. GSTM1 and LEPR variants exhibited risk modulation for non-muscle-invasive bladder cancer (NMIBC); GSTT1 and PPARG variants for muscle-invasive bladder cancer (MIBC), and ACE variant for NMIBC as well as MIBC. In general, the susceptibility markers were common for low grade and NMIBC; and distinct from those for high grade and MIBC indicating the distinct pathologies of both groups. In brief, our results conform to reports of previously associated variants in addition to identifying novel potential genetic predictors of UBC susceptibility.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Urinary bladder cancer is the ninth most frequent neoplasm around the globe, affecting approximately 2.7 million people and in 2002 caused 145,000 mortality worldwide [45]. Due to the lack of a national cancer registry in Pakistan, a true age-standardized incidence rate is difficult to ascertain, however, Rafique and Javed [47] reported urinary bladder cancer to be the most common urological cancer in both genders in Pakistan.
Bladder cancer has a multifactorial etiology in which extrinsic risk factors such as cigarette smoking and occupational exposure to carcinogens [55]; as well as genetic variations contribute towards modulation of the incidence risk [23]. These environmental and genetic factors also work interactively, complementing or counteracting each other in modulating the risk of the disease [55].
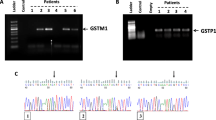
Population-based case control genetic association studies have also been performed in different parts of the world to identify the disease susceptible loci [23]. Some of these genetic factors alter protein activity such as those spanning the coding sequence of gene, e.g. rs1042522 of TP53 [57] and rs1695 of GSTP1 [28]; some affect the transcriptional regulation of target genes, e.g. rs9642880 affects MYC gene expression [61] and rs2854744 of IGFBP3 [17]; while some polymorphisms are responsible for the loss of enzymatic activity, e.g. null gene polymorphisms of GSTT1 and GSTM1 genes [48].
The present investigation was carried out on the most common type of urinary bladder neoplasms, i.e. urothelial bladder carcinoma (UBC) patients and controls of Pakistani origin. To the best of the authors’ knowledge, this is the first extensive report of UBC genetic association study conducted on this population. In this connection, different polymorphic sites were selected based on their biological plausibility and/or information from previously reported studies from other populations.
Since carcinogenesis is a complex and multi-step process that progressively develops from alterations in different cellular pathways [6], therefore genetic variants from some of these pathways were selected in this analysis, including carcinogen metabolism and antioxidant pathways, cell cycle regulation pathway, growth regulation pathway, angiogenesis pathway, folate metabolism pathway, cell signaling pathway, nitric oxide metabolism pathway, inflammatory cytokine and transcription regulation pathway. Previously, we analyzed the association of selected genome-wide association study (GWAS) variants in our population and the results of three common variants from 8q24 region (rs9642880, rs6983267 and rs2294008) have already been published elsewhere [4]. Here the results of 25 common genetic variants (Table 1) are presented.
Materials and methods
Selection criteria for cases and controls
In the present study, unrelated individuals suffering from UBC were recruited from different medical centers in northern Punjab. The cases (N = 200) went through a thorough examination including cystoscopy and trans-urethral resection of bladder tumor. The resected tissue specimens were histopathologically analyzed to determine the type, stage and grade of the tumor in order to classify different sub-groups for comparison. On the basis of tumor stage, two sub-groups were categorized: non-muscle invasive bladder cancer (NMIBC) and muscle-invasive and advanced stages into the group muscle-invasive bladder cancer (MIBC). While the samples based upon tumor grades were divided into two groups as defined by WHO 1973 scheme: papilloma, grade-I and grade-II were combined in the low grade group, while grade-III tumors were placed in the high grade group. Cases of non-Pakistani origin and bladder cancer types other than urothelial were not included in the study in addition to those with a previous history of tumor in an organ other than bladder as well as metastasized cancer.
Age, ethnicity and gender-matched healthy controls free from any malignancy were sampled from the general population.
Blood sampling and genomic DNA extraction
The present investigation conformed to the tenets of 1964 Helsinki Declaration and IRB protocols. The study was approved by the “Ethics Review Board” of the Department of Biosciences of the COMSATS Institute of Information Technology, Islamabad, Pakistan. Genomic DNA was extracted by conventional organic method [54] from peripheral leucocytes. For this study prior informed written consent was obtained from all the study participants.
Genotyping
PCR-based protocols were used for the genotyping of selected polymorphisms (Online Resource 1).
Quality control
In order to authenticate the genotyping methods, 10% selected samples representing all the genotypes were confirmed by Sanger DNA sequencing, in addition another 10% were validated by randomly replicating the PCR-based genotyping. Both the validation approaches gave 100% concordance to the genotypes observed in the first attempt.
Data analysis
Statistical procedures used for data analysis included Student’s t test for the comparison of average age of cases and controls. Hardy–Weinberg Equilibrium (HWE) of genotype frequencies among controls was tested by a goodness-of-fit Chi square (χ2) test. Odds ratio (OR) and 95% confidence interval (CI) were computed by multivariate logistic regression analysis after controlling for age, gender and smoking to determine the association of the variants.
In-silico analysis
The effects of associated nonsynonymous polymorphisms on the three-dimensional structure of respective proteins were predicted through an online tool, Have Your Protein Explained (HOPE; http://www.cmbi.ru.nl/hope/input/).
Results
In the present investigation, 200 UBC and an equal number of control samples were collected. Male:female ratio of the cases was ~3:1 (78.5 and 21.5%), controls were selected in the same proportion (77.5% males and 22.5% females) to match the gender distribution and average age (UBC = 55.5 SD ±13.24 years; controls = 54.3, SD ±9.9 years; t = 1.03, p = 0.31). There were 92 (46%) cigarette smokers among cases and 72 (36%) among controls, while non-smokers were 108 (54%) in cases and 128 (64%) in the controls. Smoking was found to increase UBC susceptibility in men (OR 1.67, 95% CI 1.04–2.7) but not in women.
Overall analysis
Only few polymorphisms were found to modulate UBC susceptibility after adjusting for age, gender and smoking (Table 2). An increase in bladder tumor susceptibility was conferred by GSTM1 null gene variant (M0M0/M1M1 + M1M0 OR 1.9, 95% CI 1.3–2.9); LEPR rs1137101 [(GG/AA OR 1.9, 95% CI 1.1–3.4); log-additive model (LAM) OR 1.4, 95% CI 1.04–1.8] and ACE rs4646994 (DD/II + ID OR 1.9, 95% CI 1.17–3.1). In addition there was a significant protective effect of IGFBP3 rs2854744 [(CA/CC OR 0.6, 95% CI 0.4–0.97); (AA/CC OR 0.5, 95% CI 0.3–0.97)] against bladder tumor risk.
Smoking-status based analysis
This analysis was performed by comparing smoker cases with smoker controls and non-smoker cases with non-smoker controls (Table 2). CYP1B1 rs2567206 was found to be associated with high UBC risk among smokers (TT/CC + CT OR 3.5, 95% CI 1.05–11.5) while CDKN1A rs1801270 conferred protection to them (LAM OR 0.4, 95% CI 0.2–0.7). GSTM1 null gene variant was found to increase the risk among both smokers (M0M0/M1M1 + M1M0 OR 1.96, 95% CI 1.1–3.96) and non-smokers (M0M0/M1M1 + M1M0 OR 1.9, 95% CI 1.1–3.2). In addition, LEPR rs1137101 was found to enhance UBC susceptibility among non-smokers [(GG/AA OR 2.6, 95% CI 1.2–5.4); (LAM OR 1.6, 95% CI 1.1–2.3)] while IGFBP3 rs2854744 was found to play a protective role [(CA/CC OR 0.5, 95% CI 0.3–0.9); (AA/CC OR 0.3, 95% CI 0.14–0.7); (LAM OR 0.6, 95% CI 0.4–0.9)]. All other polymorphisms presented a non-significant relationship with tumor risk with respect to smoking status.
Association with tumor characteristics
With reference to the tumor stage and grade, comparisons were carried out for low grade, high grade, NMIBC and MIBC tumors independently against the control population (Table 3).
PPARG rs1801282 conferred an increased susceptibility towards high grade UBC (GG/CC OR 5.97, 95% CI 1.3–26) and MIBC (GG/CC OR 5.4, 95% CI 1.2–24). GSTT1 null gene polymorphism was found to be associated with an elevated risk of high grade UBC (T0T0/T1T1 + T1T0 OR 2.2, 95% CI 1.1–4.5) and MIBC (T0T0/T1T1 + T1T0 OR 2.7, 95% CI 1.4–5.4) while that of GSTM1 with increased susceptibility of low grade cancer (M0M0/M1M1 + M1M0 OR 2.2, 95% CI 1.4–3.5) and NMIBC (M0M0/M1M1 + M1M0 OR 2.2, 95% CI 1.3–3.5). LEPR rs1137101 was also found to increase the risk of low grade UBC [(GG/AA OR 2.1, 95% CI 1.14–3.9); (LAM OR 1.4, 95% CI 1.1–2)] and NMIBC [(GG/AA OR 2.1, 95% CI 1.1–3.9); (LAM OR 1.4, 95% CI 1.04–2)]. On the other hand, IGFBP3 rs2854744 conferred protection against high grade UBC (CA/CC OR 0.5, 95% CI 0.3–0.98).
Under a recessive model (DD/II + ID), ACE rs4646994 deletion genotype was found to enhance the risk of low grade UBC (OR 1.8, 95% CI 1.07–3.1); high grade UBC (OR 2.07, 95% CI 1.1–4); NMIBC (OR 1.8, 95% CI 1.05–3.1) and MIBC (OR 1.93, 95% CI 1.02–3.7).
Discussion
Urothelial bladder carcinoma is a multifactorial disorder with diverse environmental and genetic etiologies. In the current work, a genetic association study of urothelial bladder carcinogenesis was conducted on a group of UBC cases and controls from Pakistan.
UBC is a disease with a male predominance, the observed gender ratio (~3:1) in the current study is in line with previously reported frequencies of 2–3:1 in Pakistan and other parts of the world [2, 32]. This male-dominated prevalence perhaps is due to the greater exposure of men to environmental carcinogens than women, in addition to hormonal and reproductive factors in the latter [15].
Among the environmental risk factors, cigarette smoking is conventionally considered as one of the biggest known threats [55] and the disease is often referred to as a smoking-related cancer. In agreement with this, the present study too indicated cigarette smoking as one of the risk factors of bladder tumorigenesis. Prevalence of cigarette smoking is 36% in the general male population of Pakistan [3]; while for women, it is considered a taboo. Consequently, we found smoking to be a significant UBC-predisposing factor among men but not in women, as opposed to Karagas et al. [34] who found the risk to equally contribute towards the disease in both genders. However, had a larger number of female smokers been present in the current study, the result would have been more informative.
Among all the selected genetic variants, only few reached a statistical significance to be associated with altered UBC risk and/or its severity. Three of these risk modulators belonged to carcinogen metabolism and antioxidant pathway. Carcinogen exposure and oxidative stress are among the strongest known risk factors for cancer and the tissue has different types of enzymes to deal with these threats. Cytochrome P450 1B1 (encoded by CYP1B1) is a phase-I carcinogen metabolizing enzyme and is involved in the metabolic conversion of several exogenous (e.g., polycyclic aromatic hydrocarbons) and endogenous compounds (e.g., estradiol) into carcinogenic metabolites, which in turn induce carcinogenesis [7]. In the current study, presence of TT genotype of a promoter region polymorphism (rs2567206) of CYP1B1, predisposed smokers to greater risk of the disease, which is plausible given the role of this enzyme in carcinogen metabolism and the higher exposure of smokers to cigarette carcinogens. The present study is the first to report an association of this variant with UBC. In two independent studies to determine the role of this SNP in promoter activity, a strong reduction in promoter activity was seen associated with the ‘C’ allele as compared to ‘T’ by Chakrabarti et al. [11] in a trabecular meshwork (TM3) cell line, while no effect was observed in a human bronchial epithelial cell line [27]. These contrasting effects are possibly due to tissue-specific expression and transcription factors. As currently there are no reports of the expression association of this variant in bladder epithelium therefore, functional characterization of this SNP in this tissue needs further investigation.
Glutathione-sulfo-transferases (GSTs) are a superfamily of phase-II carcinogen metabolizing enzymes involved in the detoxification of reactive carcinogenic metabolites to less reactive and more hydrophilic compounds. Their mechanism of action involves catalysis of the conjugation of glutathione with electrophilic carcinogen metabolites by forming a thioether bond. The resultant products are less hydrophobic and can be easily excreted [29]. GSTT1 (encodes GSTθ) and GSTM1 (encodes GSTµ) are two important members of this superfamily. Each of these harbor a null gene polymorphism (GSTT0 and GSTM0, respectively) causing a loss of enzymatic activity and hence an increased vulnerability to cancer due to inefficient detoxification of carcinogenic metabolites resulting in an increased rate of DNA damage [48]. The role of GSTT1 null polymorphism in bladder carcinogenesis has been found to be inconsistent [1, 34]. In the present study, a non-significant relation of GSTT1 polymorphism with UBC predisposition was observed in overall as well as smoking-status based analysis. GSTM1 polymorphism showed an increased overall risk of UBC and this risk predisposition was irrespective of the smoking-status in agreement with a previously reported meta-analysis [23]. A related possibility is that in addition to tobacco carcinogen metabolism, GSTμ also provides protection against reactive oxygen species, thereby playing a role in smoking- as well as nonsmoking-associated UBC [23]. Upon stratification by tumor grade and stage, GSTT1 polymorphism was found to be significantly associated with advanced disease, i.e., with high grade and MIBC, while GSTM1 polymorphism was associated with low grade and NMIBC. Reason of this differential behavior of the two GSTs in disease severity can be explained by the following observations. GSTT1 null polymorphism is particularly associated with a greater background rate of large-scale genetic alterations such as sister chromatid exchange and formation of micronuclei as compared to GSTM1 [43]. Since the high grade invasive bladder tumors are genetically more unstable and accumulate larger number of genetic alterations than low grade noninvasive UBC [35], therefore GSTT1 deletion is more likely to be deleterious for the more aggressive group as compared to the less aggressive form of the disease.
GSTμ expressed by GSTM is known to inhibit apoptosis via a mechanism independent of its glutathione-conjugating activity; intact GSTμ binds with apoptosis signal-regulating kinase 1 (ASK1) and inhibits its activity [14]. Under stress conditions ASK1 is released from GSTμ and activates kinases that induce apoptosis. Individuals deficient in GSTμ activity have higher ASK1 activity and subsequently greater apoptotic potential than persons with intact GSTμ who have greater chances of proliferation leading to progression [16]. Therefore GSTμ-deficient individuals are less likely to be at an increased risk of developing high grade invasive cancer.
p53 (encoded by TP53) is a tumor suppressor protein that is activated following DNA damage, aberrant growth signals or other stresses on the cell and results in regulation of cell cycle, cell proliferation, DNA repair and apoptosis [60]. Part of p53 functions are mediated by its regulation of the expression of p21 (encoded by CDKN1A), which in turn binds with cyclin-CDK complexes and induces cell cycle arrest, thus regulating cell proliferation [60]. Two nonsynonymous polymorphisms in these genes including rs1042522 (p.Pro72Arg) of TP53 and rs1801270 (p.Ser31Arg) of CDKN1A have been widely studied in relation to their association with bladder cancer [13, 64; Zhang et al. 64]. Pro72 of p53 and/or 31Arg of p21 have been reported to be associated with lower downstream expression of p21 [57]. In a previous study the 31Arg allele was not found to cause a loss of tumor suppressor activity of p21 [12]. In the present analysis no association was found between these variants and UBC risk in an overall as well as stratified analysis. However, a significant protective effect of 31Arg of p21 (‘A’ allele) was observed among smokers. Contrary to this Taghavi et al. [58] have reported an increased risk associated with 31Arg for esophageal squamous cell carcinoma among smokers. Cigarette smoke causes DNA damage [36], which may activate p53/p21 pathway since cigarette smoke has been shown to induce p21 expression in vitro and in animal models [59]. Cigarette smoking and overexpression of p53/p21 have been found to be associated with poor prognosis in non-small cell lung cancer [62]. In addition, p21 triggers replicative senescence [33] and in vitro expression of p21 has been shown to trigger enhanced oxidative stress [38]. Also, p21 has a dual role in carcinogenesis by exhibiting both tumor suppressor as well as oncogenic activities [51]. So the biological roles of p21 are not only diverse but are also ambiguous. Further, they are mediated by different factors including its expression levels, transcriptional control, transcript stability and post-translational regulation [25]. According to HOPE pathogenicity prediction, serine is smaller and polar while arginine is comparatively bigger and positively charged. This change in the size and charge of residue might affect protein function. The intriguing finding in the current study prompts investigation into further trying to understand the association between cigarette smoking and this important pathway in relation to cancer susceptibility.
Another protein participating in cell proliferation regulation is insulin-like growth factor binding protein 3 (IGFBP3), which is a member of a superfamily consisting of at least six well-characterized IGFBPs. IGFBP3 participates in cancer prevention by competitively inhibiting the binding of insulin-like growth factors (IGFs) with their targets and subsequent reduction in IGFs’ mitogenic effects as well as independently by regulating cell multiplication and by inducing apoptosis [21]. Serum levels of IGFBP3 have been shown to be correlated with susceptibility to bladder cancer in an inverse relationship [53, 66]. An IGFBP3 SNP (rs2854744) due to its location near the basal promoter activity element is known to modulate IGFBP3 expression and hence its serum levels; in this SNP the ‘A’ allele results in higher plasma IGFBP3 levels as compared to the ‘C’ allele [17]. This imparts a potential protective role to ‘A’ allele individuals in reducing UBC risk, which was evident in the present study as the ‘A’ allele-harboring individuals were found to have reduced overall UBC susceptibility as well as reduced risk of high-grade tumor. These results are consistent with those of Safarinejad et al. [53] who correlated the genotype results with IGFBP3 serum levels as well and found AA genotype to confer protection. No previous study was found even upon an extensive literature search of correlation of IGFBP3 and cigarette smoking with reference to bladder tumor. Here a protective role of AA and CA genotypes of IGFBP3 is reported for the first time among non-smokers and a loss of protective effect among smokers. Smoking has been found to be associated with reduction in serum IGFBP3 levels in men [49] possibly explaining the non-association among smokers in the current study. Association with high grade tumor could be attributed to the potential role of IGFBP3 in the differentiation of bladder cells. Given its relationship with UBC susceptibility and circulating IGFBP3 levels, rs2854744 can be considered an important potential predictor.
Leptin (encoded by LEP) is a member of a family of adipose tissue-derived hormones called adipocytokines, and exerts its action through receptors such as leptin receptor (encoded by LEPR), which activates specific intracellular pathways. Leptin is primarily involved in energy homeostasis and BMI regulations [31]. Its involvement in carcinogenesis comes from the observation of increased chances of cancer among obese people [10] as well as the role of leptin in cell proliferation, apoptosis, growth regulation and neoangiogenesis [24]. The role of adipocytokines in carcinogenesis has been mainly described through in vitro expression studies and genetic variation analyses are quite scarce [44]. The current study is the first one to determine the possible contribution of two polymorphisms of this pathway in bladder oncogenesis: a promoter SNP (rs7799039) of LEP and a nonsynonymous SNP (rs1137101, p.Gln223Arg) of LEPR. The former affects leptin secretion and its strength of forming complexes with a nuclear protein [30], while the amino acid at 223 position of leptin receptor is a part of its extracellular domain and a substitution of Gln by Arg is known to enhance serum leptin-binding affinity [46]. In the current study, rs7799039 of LEP did not show any association, while a strong association of 223Arg isoform (‘G’ allele) of LEPR with overall UBC susceptibility was observed. As the 223Arg isoform (rs1137101) has a higher affinity for leptin [46], therefore any changes in its structure may act by promoting leptin-mediated growth responses and thus increasing UBC susceptibility. Upon stratified analysis by smoking status, this significant association was only observed among non-smokers which may be explained by the fact that cigarette smoking is associated with lower concentration of leptin [50] thus minimizing the role of rs1137101 among smokers.
We also found rs1137101 to be associated with low grade UBC and NMIBC and no association was observed with high grade or MIBC. Phosphoinositide 3-kinase (PI3K) pathway is frequently activated by mutations in low grade NMIBC and very rarely in high grade MIBC [35]. Leptin is also known to activate PI3K pathway [22], which could be the likely reason behind association of leptin receptor SNP only with low grade and NMIBC.
HOPE analysis predicts an alteration in the charge of residue from neutral (Glu) to positive (Arg) which might affect the binding of ligands. Further the arginine is bigger and might lead to changes in surface geometry of leptin receptor and may affect its interaction with other molecules.
The current novel finding of an association of rs1137101 of LEPR provides a potential candidate for future research and may also help to explore the link between obesity and carcinogenesis.
Angiotensin I-converting enzyme (ACE) is a zinc metalloproteinase that apart from its diverse physiological roles, is also known to promote tumor growth, angiogenesis and metastasis [9]. A 187 bp Alu repeat sequence in intron 16 of ACE has been implicated in the etiology of different cancers [42, 56], which effect has been reported to be achieved by regulating ACE levels. The DD homozygotes have about twofold higher levels of the enzyme as compared to II homozygotes while the I/D heterozygotes have intermediate levels [41]. However, a meta-analysis of different cancers revealed non-association of this polymorphism with cancer risk [65]. To date, no study has been conducted on bladder cancer and ACE I/D polymorphism. In the current study, DD homozygotes were found to confer an increased risk towards overall UBC susceptibility as well as towards low and high grades of cancer and also towards NMIBC and MIBC stages indicating a possible association of ACE activity with underlying mechanisms for different pathological types of UBC.
Peroxisome proliferator activated receptor (PPAR) is a sub-family of nuclear receptors superfamily and includes PPARα, PPARβ/δ and the most widely studied PPARγ [19]. After binding to ligands and coactivators, PPARγ (encoded by PPARG) induces the expression of target genes [39]. rs1801282 (p.Pro12Ala) is the most extensively studied polymorphism of PPARG and 12Ala isoform (‘G’ allele) causes a reduction in receptor activity [18]. Pathogenicity prediction using HOPE suggests a change in protein structure as a result of this substitution. Alanine is smaller in size and might lead to a loss of interactions. In addition, proline induces a special backbone conformation which might be required for this position. Substitution by alanine can disturb this conformation and thus protein activity. Inhibition/reduction of PPARγ activity has been found to be associated with higher grade and advanced stages of bladder cancer [63]. In the present study, the 12Ala isoform was found to significantly enhance tumor severity by correlating with high grade and MIBC. PPARγ mediates several processes such as apoptosis, anti-inflammatory effects, terminal differentiation and subverting of host immune response, which are required for prevention of cancer progression, invasion and metastasis [39]. Therefore, a reduction in its activity due to 12Ala is more likely to affect high grade and MIBC. More specifically, the PPARγ agonists have been shown to play an important role in inducing differentiation of bladder cancer cells by causing an increased expression of adipose-type fatty acid binding proteins (A-FABP) [26]. Therefore, the loss of PPARγ activity has been reportedly associated with UBC progression and severity [39, 63].
In brief, association of SNPs with UBC susceptibility and/or severity was observed in selected genetic variants of CYP1B1, GSTT1 and GSTM1 genes from carcinogen metabolism and antioxidant pathways, CDKN1A from cell cycle regulation pathway, IGFBP3 and LEPR from growth regulation pathway, ACE from angiogenesis pathway and transcription regulator PPARG.
Rest of the selected polymorphisms did not exhibit any statistically significant association in the current investigation, these were GSTP1 and PON1 from carcinogen metabolism and antioxidant pathways, respectively, VEGFA from angiogenesis pathway, MTHFR from folate metabolism pathway, CAV1 from cell signaling pathway, NOS3 from nitric oxide metabolism pathway and inflammatory cytokine TNFA.
Association of variants from different pathways demonstrates the heterogeneous genetic etiology evident not only in the overall UBC susceptibility but also in different histopathological subtypes and in relation to smoking. Non-association of certain variants offers a perspective to explore other candidate factors from these pathways.
Moreover, distinct correlations of clinicopathological subtypes of UBC were also observed. Low grade UBC is frequently known to occur with NMIBC while high grade with MIBC, representing two distinct disease entities with distinct underlying molecular mechanisms and behaviors [35]. Concordant with this, we also found the co-occurrence of low grade with NMIBC (48% of the cases) and of high grade with MIBC (28% of the cases), the rest 24% were either low grade MIBC or high grade NMIBC. Further, the polymorphisms either associated with low grade, NMIBC or with high grade, MIBC with the exception of ACE, which associated with both groups although conferring slightly greater risk for high grade and MIBC (Fig. 1). Thus further studies are required to identify specific sets of prognostic and susceptibility markers for these two groups.

Association of genes (with respect to selected polymorphisms) with increased risk of overall urothelial bladder carcinoma susceptibility, smoking status-based sub-groups and histopathological subtypes; genes with non-associated polymorphism(s) or those conferring protection are not shown
Strengths of the present study are a selection of polymorphisms from multiple pathways based on previous reports as well as predicted involvement and a stratified analysis by smoking status, tumor grade and tumor stage. In addition, this is a preliminary report from Pakistani UBC cases. A major limitation was the sample size due to the relatively low prevalence and/or reporting rate in Pakistan, poor cooperation of indoor patients and a lack of follow-up cases.
Conclusion
The present study is the first attempt to determine an association of selected common variants with UBC in the Pakistani population. In the current study there are a few novel findings and others are a validation of previous ones in different populations. Identification of some putative novel association indicates potential involvement of different pathways in the disease pathology. It also warrants further studies to better understand the molecular mechanisms underlying this multifactorial disorder. Since this was a preliminary study of the Pakistani population, future studies with larger sample size could be helpful to validate these findings and to determine their functional effects. Expression-based studies would be helpful to assess the prognostic significance of some of the variants associated with aggressive tumor and towards personalized therapeutic interventions.
References
Abdel-Rahman SZ, Anwar WA, Abdel-Aal WE, Mostafa HM, Au WW (1998) GSTM1 and GSTT1 genes are potential risk modifiers for bladder cancer. Cancer Detect Prev 22:129–138
Ahmed K, Shahid SM, Jawed M, Islam Z, Hatim F (2006) An evaluation of urinary bladder carcinoma with respect to age, sex, stage and grade. Int J Cancer Res 2:219–223
Ahmed R, Rizwan-ur-Rashid, McDonald PW, Ahmed SW (2008) Prevalence of cigarette smoking among young adults in Pakistan. J Pak Med Assoc 58:597–601
Ali SHB, Younis M, Bangash KS, Rauf A, Anwar K, Khurram R, Khawaja MA, Qureshi AA, Akhter S, Azam M, Kiemeney LA, Qamar R (2013) Common variants at 8q24 confer susceptibility to urothelial bladder cancer in the Pakistani population. Pak J Zool 45:1501–1509
Ayub H, Khan MI, Micheal S, Akhtar F, Ajmal M, Shafique S, Ali SHB, den Hollander AI, Ahmed A, Qamar R (2010) Association of eNOS and HSP70 gene polymorphisms with glaucoma in Pakistani cohorts. Mol Vis 16:18–25
Baba AI, Catoi C (2007) Comparative oncology. The Publishing House of the Romanian Academy, Cornel, Bucharest
Badal S, Delgoda R (2013) CYP1B1: friend or foe? A critical review. BioChemistry 1:8
Bau DT, Chang CH, Tsai RY, Wang HC, Wang RF, Tsai CW, Yao CH, Chen YS, Shyue SK, Huang CY (2011) Significant association of caveolin-1 genotypes with bladder cancer susceptibility in Taiwan. Chin J Physiol 54:153–160
Bauvois B (2004) Transmembrane proteases in cell growth and invasion: New contributors to angiogenesis? Oncogene 23:317–329
Bray GA (2002) The underlying basis for obesity: relationship to cancer. J Nutr 132:3451S–3455S
Chakrabarti S, Ghanekar Y, Kaur K, Kaur I, Mandal AK, Rao KN, Parikh RS, Thomas R, Majumder PP (2010) A polymorphism in the CYP1B1 promoter is functionally associated with primary congenital glaucoma. Hum Mol Genet 19:4083–4090
Chedid M, Michieli P, Lengel C, Huppi K, Givol D (1994) A single nucleotide substitution at codon 31 (Ser/Arg) defines a polymorphism in a highly conserved region of the p53-inducible gene WAF1/CIP1. Oncogene 9:3021–3024
Chen WC, Wu HC, Hsu CD, Chen HY, Tsai FJ (2002) P21 gene codon 31 polymorphism is associated with bladder cancer. Urol Oncol 7:63–66
Cho S, Lee YH, Park HS, Ryoo K, Kang KW, Park J, Eom SJ, Kim MJ, Chang TS, Choi SY, Shim J, Kim Y, Dong MS, Lee MJ, Kim SG, Ichijo H, Choi EJ (2001) Glutathione S-transferase mu modulates the stress-activated signals by suppressing apoptosis signal-regulating kinase 1. J Biol Chem 276:12749–12755
Davis-Dao CA, Henderson KD, Sullivan-Halley J, Ma H, West D, Xiang YB, Gago-Dominguez M, Stern MC, Castelao JE, Conti DV, Pike MC, Bernstein L, Cortessis VK (2011) Lower risk in parous women suggests that hormonal factors are important in bladder cancer etiology. Cancer Epidemiol Biomarkers Prev 20:1156–1170
De Martino M, Klatte T, Schatzl G, Remzi M, Waldert M, Haitel A, Stancik I, Kramer G, Marberger M (2010) Renal cell carcinoma Fuhrman grade and histological subtype correlate with complete polymorphic deletion of glutathione S-transferase m1 gene. J Urol 183:878–883
Deal C, Ma J, Wilkin F, Paquette J, Rozen F, Ge B, Hudson T, Stampfer M, Pollak M (2001) Novel promoter polymorphism in insulin-like growth factor-binding protein-3: correlation with serum levels and interaction with known regulators. J Clin Endocrinol Metab 86:1274–1280
Deeb SS, Fajas L, Nemoto M, Pihlajamaki J, Mykkanen L, Kuusisto J, Laakso M, Fujimoto W, Auwerx J (1998) A Pro12Ala substitution in PPARgamma2 associated with decreased receptor activity, lower body mass index and improved insulin sensitivity. Nat Genet 20:284–287
Desvergne B, Wahli W (1999) Peroxisome proliferator-activated receptors: nuclear control of metabolism. Endocr Rev 20:649–688
Fang DH, Fan CH, Ji Q, Qi BX, Li J, Wang L (2012) Differential effects of paraoxonase 1 (PON1) polymorphisms on cancer risk: evidence from 25 published studies. Mol Biol Rep 39:6801–6809
Firth SM, Baxter RC (2002) Cellular actions of the insulin-like growth factor binding proteins. Endocr Rev 23:824–854
Fruhbeck G (2006) Intracellular signaling pathways activated by leptin. Biochem J 393:7–20
Garcia-Closas M, Malats N, Silverman D, Dosemeci M, Kogevinas M, Hein DW, Tardon A, Serra C, Carrato A, Garcia-Closas R, Lloreta J, Castano-Vinyals G, Yeager M, Welch R, Chanock S, Chatterjee N, Wacholder S, Samanic C, Tora M, Fernandez F, Real FX, Rothman N (2005) NAT2 slow acetylation, GSTM1 null genotype, and risk of bladder cancer: results from the Spanish bladder cancer study and meta-analyses. Lancet 366:649–659
Garofalo C, Surmacz E (2006) Leptin and cancer. J Cell Physiol 207:12–22
Gartel AL, Radhakrishnan SK (2005) Lost in transcription: P21 repression, mechanisms, and consequences. Cancer Res 65:3980–3985
Guan YF, Zhang YH, Breyer RM, Davis L, Breyer MD (1999) Expression of peroxisome proliferator-activated receptor gamma (PPARgamma) in human transitional bladder cancer and its role in inducing cell death. Neoplasia 1:330–339
Han W, Pentecost BT, Spivack SD (2003) Functional evaluation of novel single nucleotide polymorphisms and haplotypes in the promoter regions of CYP1B1 and CYP1A1 genes. Mol Carcinogen 37:158–169
Harries LW, Stubbins MJ, Forman D, Howard GC, Wolf CR (1997) Identification of genetic polymorphisms at the glutathione s-transferase pi locus and association with susceptibility to bladder, testicular and prostate cancer. Carcinogenesis 18:641–644
Hayes JD, Pulford DJ (1995) The glutathione S-transferase supergene family: regulation of GST and the contribution of the isoenzymes to cancer chemoprotection and drug resistance. Crit Rev Biochem Mol Biol 30:445–600
Hoffstedt J, Eriksson P, Mottagui-Tabar S, Arner P (2002) A polymorphism in the leptin promoter region (-2548 G/A) influences gene expression and adipose tissue secretion of leptin. Horm Metab Res 34:355–359
Housa D, Housova J, Vernerova Z, Haluzik M (2006) Adipocytokines and cancer. Physiol Res 55:233–244
Jemal A, Siegel R, Xu J, Ward E (2010) Cancer statistics, 2010. Cancer J Clin 60:277–300
Ju Z, Choudhury AR, Rudolph KL (2007) A dual role of p21 in stem cell aging. Ann NY Acad Sci 1100:333–344
Karagas MR, Park S, Warren A, Hamilton J, Nelson HH, Mott LA, Kelsey KT (2005) Gender, smoking, glutathione-s-transferase variants and bladder cancer incidence: a population-based study. Cancer Lett 219:63–69
Knowles MA, Hurst CD (2015) Molecular biology of bladder cancer: new insights into pathogenesis and clinical diversity. Nat Rev Cancer 15:25–41
Liu X, Conner H, Kobayashi T, Kim H, Wen F, Abe S, Fang Q, Wang X, Hashimoto M, Bitterman P, Rennard SI (2005) Cigarette smoke extract induces DNA damage but not apoptosis in human bronchial epithelial cells. Am J Respir Cell Mol Biol 33:121–129
Lu Y, Ge Y, Shi Y, Yin J, Huang Z (2013) Two polymorphisms (rs699947, rs2010963) in the VEGFA gene and diabetic retinopathy: an updated meta-analysis. BMC Ophthalmol 13:56
Macip S, Igarashi M, Fang L, Chen A, Pan ZQ, Lee SW, Aaronson SA (2002) Inhibition of p21-mediated ROS accumulation can rescue p21-induced senescence. EMBO J 21:2180–2188
Mansure JJ, Nassim R, Kassouf W (2009) Peroxisome proliferator-activated receptor gamma in bladder cancer: a promising therapeutic target. Cancer Biol Ther 8:6–15
Marsh HP, Haldar NA, Bunce M, Marshall SE, le Monier K, Winsey SL, Christodoulos K, Cranston D, Welsh KI, Harris AL (2003) Polymorphisms in tumour necrosis factor (TNF) are associated with risk of bladder cancer and grade of tumour at presentation. Br J Cancer 89:1096–1101
McKenzie CA, Julier C, Forrester T, McFarlane-Anderson N, Keavney B, Lathrop GM, Ratcliffe PJ, Farrall M (1995) Segregation and linkage analysis of serum angiotensin I-converting enzyme levels: evidence for two quantitative-trait loci. Am J Hum Genet 57:1426–1435
Nacak M, Nacak I, Sanli M, Ozkur M, Pektas M, Aynacioglu AS (2010) Association of angiotensin converting enzyme gene insertion/deletion polymorphism with lung cancer in Turkey. Cancer Genet Cytogent 198:22–26
Norppa H (1997) Cytogenetic markers of susceptibility: Influence of polymorphic carcinogen-metabolizing enzymes. Environ Health Perspect 105:829–835
Pechlivanis S, Bermejo JL, Pardini B, Naccarati A, Vodickova L, Novotny J, Hemminki K, Vodicka P, Forsti A (2009) Genetic variation in adipokine genes and risk of colorectal cancer. Eur J Endocrinol 160:933–940
Ploeg M, Aben KKH, Kiemeney LA (2009) The present and future burden of urinary bladder cancer in the world. World J Urol 27:289–293
Quinton ND, Lee AJ, Ross RJ, Eastell R, Blakemore AI (2001) A single nucleotide polymorphism (SNP) in the leptin receptor is associated with BMI, fat mass and leptin levels in postmenopausal Caucasian women. Hum Genet 108:233–236
Rafique M, Javed AA (2004) Role of itravenous urography and transabdominal ultrasonography in the diagnosis of bladder carcinoma. Int Braz J Urol 30:185–191
Rebbeck TR (1997) Molecular epidemiology of the human glutathione s-transferase genotypes GSTM1 and GSTT1 in cancer susceptibility. Cancer Epidemiol Biomarkers Prev 6:733–743
Renehan AG, Atkin WS, O’dwyer ST, Shalet SM (2004) The effect of cigarette smoking use and cessation on serum insulin-like growth factors. Br J Cancer 91:1153–1525
Reseland JE, Mundal HH, Hollung K, Haugen F, Zahid N, Anderssen SA, Drevon CA (2005) Cigarette smoking may reduce plasma leptin concentration via catecholamines. Prostaglandins Leukot Essent Fatty Acids 73:43–49
Roninson IB (2002) Oncogenic functions of tumour suppressor p21(Waf1/Cip1/Sdi1): association with cell senescence and tumour-promoting activities of stromal fibroblasts. Cancer Lett 179:1–14
Safarinejad MR, Shafiei N, Safarinejad S (2012) Methylenetetrahydrofolate reductase (MTHFR) gene C677T, A1298C and G1793A polymorphisms: association with risk for clear cell renal cell carcinoma and tumour behaviour in men. Clin Oncol 24:269–281
Safarinejad MR, Shafiei N, Safarinejad SH (2011) The association between bladder cancer and a single nucleotide polymorphism (rs2854744) in the insulin-like growth factor (IGF)-binding protein-3 (IGFBP-3) gene. Arch Toxicol 85:1209–1218
Sambrook J, Russell DW (2001) Molecular cloning: a laboratory manual, 3rd edn. Cold Spring Harbor Laboratory Press, New York
Silverman DT, Devesa SS, Moore LE, Rothman N (2006) Bladder cancer. In: Schottenfeld D, Fraumeni JF Jr (ed) Cancer epidemiology and prevention, 3rd edn. Oxford University Press, New York, pp 1101–1127
Srivastava K, Srivastava A, Mittal B (2010) Angiotensin I-converting enzyme insertion/deletion polymorphism and increased risk of gall bladder cancer in women. DNA Cell Biol 29:417–422
Su L, Sai Y, Fan R, Thurston SW, Miller DP, Zhou W, Wain JC, Lynch TJ, Liu G, Christiani DC (2003) P53 (codon 72) and P21 (codon 31) polymorphisms alter in vivo mRNA expression of p21. Lung Cancer 40:259–266
Taghavi N, Biramijamal F, Abbaszadegan MR, Khademi H, Sotoudeh M, Khoshbakht S (2010) P21 (waf1/cip1) gene polymorphisms and possible interaction with cigarette smoking in esophageal squamous cell carcinoma in northeastern Iran: a preliminary study. Arch Iran Med 13:235–242
Tomita K, Caramori G, Lim S, Ito K, Hanazawa T, Oates T, Chiselita I, Jazrawi E, Chung KF, Barnes PJ, Adcock IM (2002) Increased p21 (CIP1/WAF1) and B cell lymphoma leukemia-x(L) expression and reduced apoptosis in alveolar macrophages from smokers. Am J Respir Crit Care Med 166:724–731
Vogelstein B, Lane D, Levine AJ (2000) Surfing the p53 network. Nature 408:307–310
Wang M, Wang M, Zhang W, Yuan L, Fu G, Wei Q, Zhang Z (2009) Common genetic variants on 8q24 contribute to susceptibility to bladder cancer in a Chinese population. Carcinogenesis 30:991–996
Xie D, Lan L, Huang K, Chen L, Xu C, Wang R, Shi Y, Wu X, Wang L, Liu Y, Lu B (2014) Association of p53/p21 expression and cigarette smoking with tumor progression and poor prognosis in non-small cell lung cancer patients. Oncol Rep 32:2517–2526
Yoshimura R, Matsuyama M, Segawa Y, Hase T, Mitsuhashi M, Tsuchida K, Wada S, Kawahito Y, Sano H, Nakatani T (2003) Expression of peroxisome proliferator-activated receptors (PPARs) in human urinary bladder carcinoma and growth inhibition by its agonists. Int J Cancer 104:597–602
Zhang R, Chen W, Zhang W, Jiang Q, Liu C, Lin Y, Hu Z, Yu S, Xu G (2011) Genetic polymorphisms of p53 codon 72 and bladder cancer susceptibility: a hospital-based case-control study. Genet Test Mol Biomakers 15:337–341
Zhang Y, He J, Deng Y, Zhang J, Li X, Xiang Z, Huang H, Tian C, Huang J, Fan H (2011) The insertion/deletion (I/D) polymorphism in the angiotensin-converting enzyme gene and cancer risk: a meta-analysis. BMC Med Genet 12:159
Zhao H, Grossman HB, Spitz MR, Lerner SP, Zhang K, Wu X (2003) Plasma levels of insulin-like growth factor-1 and binding protein-3, and their association with bladder cancer risk. J Urol 169:714–717
Acknowledgements
This study was sponsored by Pakistan Academy of Sciences (Grant No. 5-9/PAS awarded to RQ) and Radboud University Medical Center, Nijmegen, The Netherlands.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Ali, S.H.B., Bangash, K.S., Rauf, A. et al. Identification of novel potential genetic predictors of urothelial bladder carcinoma susceptibility in Pakistani population. Familial Cancer 16, 577–594 (2017). https://doi.org/10.1007/s10689-017-9991-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10689-017-9991-z