
Abstract
Research suggests a protective effect of religious service attendance on various health outcomes. However, most research has been done in religious societies, raising the question of whether these associations are also prominent in secular cultures. Here we examine mortality and hospitalisations by religious service attendance among men and women in a secular society. We performed a cohort study including 2987 Danes aged 40+ interviewed in SHARE from 2004 to 2007 and followed up in the Danish registries until 2018. We used Cox regressions and negative binomial regressions to examine associations, including interactions with sex and adjusting for age, wave, socioeconomic factors, lifestyle factors, body mass index, and history of diseases. Overall, 5.0% of men and 6.6% of women reported that they had taken part in a religious organisation within the last month. Among 848 deaths, we found lower mortality for people who attended religious services (hazard ratio (HR) 0.70; 95% CI 0.50–0.99). There was evidence for an association among women (HR 0.56; 95% CI 0.35–0.89), but not among men (HR 0.95; 95% CI 0.59–1.53). In contrast, regarding hospital admissions (n = 12,010), we found lower hospitalisation rates among men who attended religious services (incidence rate ratio (IRR) 0.67; 95% CI 0.45–0.98), whereas no association was found among women (IRR 0.95; 95% CI 0.70–1.29). Sensitivity analyses with E-values were moderately robust. Our results contribute to the limited literature on possible health benefits of religious service attendance in secular societies, demonstrating lower mortality among women and fewer hospitalisations among men.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Religiosity seems to be an important pathway to human well-being [1]. Religiosity, often measured as attending religious services, is associated with better physical health and longevity and potential explanations include a healthier lifestyle, increased social support, and more positive emotions [2, 3]. Across most of the world, women live longer than men despite reporting worse health—the so-called male–female health survival paradox [4]. Also, women are in general more religious than men. This is also the case in Denmark—a country often being considered one of the least religious societies in the world [5, 6]. There have been indications in the research literature, at least from mortality studies [7], that protective associations between religion and health may be most substantial in more religious societies, where a higher proportion of people regularly participate in a religious organisation. Studies from the United States show that mortality is the health outcome for which the evidence on religious service attendance is most substantial [1, 8,9,10,11,12]. Evidence from Europe is sparse, but previous research from longitudinal mortality studies, including 734 and 1080 persons from Denmark [13] and Finland [14], respectively, suggested a protective association of religious service attendance on mortality among women, but not among men.
Although evidence on religiousness and health from Europe is limited [15], previous studies from 10 European countries participating in the Survey of Health, Ageing and Retirement in Europe (SHARE) have demonstrated protective associations with health from various forms of religious participation. Specifically, evidence was found regarding participation in a religious organisation and lower odds of cancer [16], activity limitations [17], and depression [17, 18], as well as lower odds of negative lifestyle habits including smoking, alcohol consumption, physical activity, and sleep problems [19]. Recently, Herold et al. confirmed the association between religious service attendance and a healthier lifestyle in a secular Danish setting [20]. Nevertheless, due to many participants with unknown vital status in SHARE [21], mortality is one outcome that no previous SHARE studies have investigated.
To fill this knowledge gap, this study aims to investigate mortality and hospitalisation by religious service attendance among middle-aged and older Danes participating in the Danish SHARE survey, which is linked to Danish nationwide registers. We hypothesise that people who attend religious services have lower mortality and hospitalisation rates than those who do not attend religious services. Based on previous evidence, we expect the most protective associations regarding mortality among women. However, although the effect on mortality may be less strong in men, it might be that the effect of religiousness could protect men from more severe illnesses, reflected in fewer hospitalisations among those attending religious services.
Methods
Data source and study population
SHARE is an interview-based survey providing high-quality survey data on the ageing population in Europe, including health, economic, and social factors among Europeans aged 50 and older and their spouses or partners at any age [22]. These data were collected in biannual interview waves starting in 2004–2005. SHARE collects data according to strict quality standards and with ex-ante harmonised interviews. If possible, SHARE interviews the same people in each wave (the longitudinal sample), but refreshment samples are also drawn regularly to compensate for attrition and to maintain a representation of the younger age cohorts [22]. As part of the REGLINK-SHAREDK project, the Danish SHARE data have been linked to Danish register data from Statistics Denmark. This individually linked database allows a unique data source, merging subjective information from interviews with more objective register data [23].
We performed a longitudinal study including Danish men and women aged 40 years and older who participated in at least one SHARE interview in waves 1 (2004–2005) or 2 (2006–2007). The household response rates in Denmark in SHARE waves 1 and 2 were 67.1% and 65.2%, respectively [24]. We included participants at first intake, i.e., the first time they took part in one of the waves. We excluded individuals below age 40 (n = 2), those with missing values on religious service attendance (n = 54), individuals with no linkage to the Danish registers (n = 29), and one person with an invalid interview date, leaving 2987 individuals in the study population.
Hospitalisation and mortality
The Danish SHARE data were linked to national health registers through a unique 10-digit personal identification number (a CPR number), which has been assigned to all persons alive and living in Denmark since April 2, 1968 [25]. We used the Danish Civil Registration System [26] for information on birth date, the Causes of Death Registry for information on deaths [27], and the National Patient Register [28] for information on hospitalisations.
Religious service attendance
Data on religious service attendance came from the personal interview in SHARE, where the participants in waves 1 and 2 were asked ‘‘Have you done any of these activities in the last month?’’ This question had seven answer categories, including ‘‘Taken part in a religious organisation (church, synagogue, mosque, etc.)’’ to which the participants could answer “yes” or “no”. In this study, we consider participating in a religious organisation as effectively being analogous to religious service attendance.
Socio-demographic variables
Socio-demographic variables included sex, age at interview (in years), wave, education, marital status, wealth, history of diseases, current smoking, alcohol intake, and body mass index (BMI). The age of participants was grouped into 5-year age groups from age 40 to age 79 with an open-ended category from age 80+. Education was measured with the International Standard Classification of Education (ISCED), grouped into lower (ISCED 0–2), medium (ISCED 3–4) and higher (ISCED 5–6). Marital status was categorised into married/registered partnership, unmarried/divorced, and widowed. Wealth was calculated based on an average of the imputations provided in each wave of SHARE, which compensates for nonresponse and is the sum of household net financial assets and household real assets [29]. Information about the history of diseases was reported in response to the question: “Has a doctor ever told you that you had/do currently have one of the following conditions?” (High cholesterol, stroke, diabetes, lung disease, and cancer). Smokers were people reporting that they were currently smoking cigarettes, cigars, or pipes. Alcohol consumption was defined by the intake of any alcoholic beverages (such as beer, cider, wine, spirits, or cocktails) daily or almost every day during the previous six (wave 1) or three (wave 2) months preceding the survey. Body mass index (BMI) was divided into three groups < 25, 25–29.9 and 30+. The proportion of missing values was low (0.5% for education, 0.1% for smoking, and 1.6% for BMI). For the other variables, there were no missing values (Table 1).
Statistical analyses
We estimated the overall mortality (40–98 years) for men and women, respectively, using Kaplan–Meier estimation, and we tested the differences between the curves using a log-rank test. In addition, we estimated hazard ratios (HRs) and 95% confidence intervals (CIs) for the differences in mortality between those attending religious service and those who did not through a Cox proportional hazards analysis. We tested the Cox proportional hazards assumptions using the log–log plot of the Kaplan–Meier survival function and by Schoenfeld residuals, and the assumptions were met. Hospitalisation was measured as admission to a hospital as an inpatient. Due to signs of overdispersion in the Poisson regression, negative binomial regression was used to estimate the frequency of hospitalisations calculated by the incidence rate ratios (IRRs) with 95% CIs. This method allowed us to consider repeated hospitalisations for each person. Follow-up started at the interview and continued until death or the end of follow-up (December 31, 2018), whichever came first.
We fitted five models for mortality and hospitalisations. In model 1, we adjusted for age and wave as well as for sex in the combined model. In model 2, we further adjusted for education, marital status, and wealth. In model 3, we added history of diseases including high cholesterol, stroke, diabetes, and lung disease, and in model 4, we included smoking, alcohol consumption and BMI on top of the other covariates. Moreover, we added a model 5 by using a logistic regression model, in which possible confounders were taken into account by estimating propensity scores. They were used to estimate the Cox regression and the negative binomial regression models, respectively including robust standard errors. Moreover, as a sensitivity analysis we added cancer in models 3 and 4. When investigating mortality, cancer was included with the possibility for a time-varying HR to fulfil the Cox proportional hazards assumptions (Supplementary Table 1).
In the overall models, sex was included as a basic covariate. In the stratified models, we included a multiplicative interaction term between religious service attendance and sex in all regression models, resulting in estimates for each sex separately and in p-values for the possible effect modification by sex. Moreover, we investigated possible additive interactions by the additive Aalen model for mortality and by robust regression models for hospitalisations.
For sensitivity analyses, we calculated the E-value for both the effect sizes (E-value) and the lower limits of CIs in model 4 (E-valueCI) using the package “E-value” in Stata [30]. The E-value is a proposed measure of the sensitivity of effect sizes in longitudinal studies [31]. The E-value is the minimum strength of association on the risk ratio scale that an unmeasured confounder would need to have with both the exposure and the outcome, conditional on the measured covariates, to fully explain away a specific exposure-outcome association. Consequently, an unmeasured confounder with associations higher than or equal to the E-value could be able to explain away the measured effect. However, any unmeasured confounder with a weaker association could not. Estimating E-valueCI determines the minimum confounding that would suffice to shift the CI to include the null [32].
We used Stata (version 17.0) for all analyses, though the additive interactions for mortality were performed via R version 4.0.3. The significance level was set to be 5% (α = 0.05).
Results
In total, 1348 (45.1%) men and 1639 (54.9%) women were included in the study. The sample’s mean age was 62.6 years (standard deviation (SD) = 10.7 years). A total of 5.0% of men and 6.6% of women reported that they had taken part in a religious organisation within the last month (Table 1). Overall, 848 (28.4%) deaths were observed during the 14-year follow-up period: 36 deaths (20.5%) among people attending religious services (18 (26.5%) among men and 18 (16.7%) among women) and 812 (28.9%) among those not attending (389 (30.4%) among men and 423 (27.6%) among women). Hospitalisation rates were 254/1000 person-years for those attending services (237 among men and 264 among women) and 268/1000 person-years for those not attending (294 among men and 247 among women). When we compared the baseline characteristics, we found a lower proportion of smokers among people who attended religious services (49.4% vs. 63.0%, p < 0.001). Compared with people not attending religious services, a tendency was found towards less alcohol consumption, higher education and higher wealth among people attending religious services, though non-significant (Table 1).
Differences in mortality for Danes who attended religious services versus those who did not are demonstrated by Kaplan–Meier curves showing better survival for those who attended religious services in the total sample (Fig. 1A); however, when stratified by sex, the differences between the curves were only significant among women (Fig. 1B, C).

Kaplan–Meier curves for all-cause mortality from age 40 years for the total study population (A) and for Danish men (B) and women (C) who had taken part in a religious organisation within the last month vs those who did not
The Cox regression models adjusted for age and wave showed that religious service attendance was associated with lower mortality in the overall model (HR 0.56; 95% CI 0.40–0.78). When investigating the associations stratified by sex, no significant association was found among men (HR 0.76; 95% CI 0.47–1.22), whereas the association persisted among women (HR 0.44; 95% CI 0.28–0.71). After further adjustments for socioeconomic characteristics, history of diseases, and lifestyle factors, the associations attenuated but remained significant in the total sample (HR 0.70; 95% CI 0.50–0.99) (Fig. 2A, Table 2). In the sex-specific analyses, the significant association persisted among women (HR 0.56; 95% CI 0.35–0.89) but not among men (HR 0.95; 95% CI 0.59–1.53) (Fig. 2A, Table 2). There was not, however, definitive evidence for neither multiplicative nor additive interactions between religious service attendance and sex (Table 2). When including cancer, the results were similar to those from the main models, except that the association with mortality in the total sample in model 4 became borderline significant (HR 0.72; 95% CI 0.52–1.01) (Supplementary Table 1). When examining the E-values, we found an E-value of 2.21 for the total sample indicating that an unmeasured confounder that was associated 2.21-fold with both the exposure and the outcome, conditional on the measured covariates, could suffice to explain away the effect, but weaker joint confounder association could not; however, the analogous associations for the CI lower limit were only at 1.11-fold (E-valueCI = 1.11). We found this effect in women more robust than for the total sample with an E-value of 2.97 (E-valueCI = 1.50) (Table 2). Results from the propensity score model confirmed that religious service attendance was associated with lower mortality among women (HR 0.64; 95% CI 0.43–0.97) (Fig. 2A, Table 2).

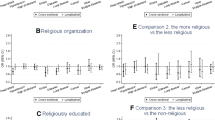
Hazard ratios with 95% confidence intervals (CIs) for all-cause mortality (A) and incidence rate ratios with 95% CIs for all-cause hospitalisations (B) overall and stratified by sex among Danes participating in SHARE waves 1 and 2 who had taken part in a religious organisation within the last month vs those who did not. Model 1: Adjusted for age and wave. Model 2: Adjusted for age, wave, education, marital status, and wealth. Model 3: Adjusted for age, wave, education, marital status, wealth, and history of diseases including high cholesterol, stroke, diabetes, and lung disease. Model 4: Adjusted for age, wave, education, marital status, wealth, history of diseases including high cholesterol, stroke, diabetes, and lung disease, smoking, alcohol consumption, and body mass index. Model 5: Based on propensity score models adjusted for age, wave, education, marital status, wealth, history of diseases including high cholesterol, stroke, diabetes, lung disease, and cancer, smoking, alcohol consumption, and body mass index
Among 12,010 inpatient hospitalisations, we found fewer hospitalisations for people who had taken part in a religious organisation (IRR 0.78; 95% CI 0.61–1.00). In addition, a lower risk of hospitalisation was found among men (IRR 0.61; 95% CI 0.41–0.91) but not among women (IRR 0.88; 95% CI 0.66–1.22). After further adjustments, the association remained for men (IRR 0.67; 95% CI 0.45–0.98) but became borderline significant for the entire sample (Fig. 2B, Table 2). However, given the limited sample size, there was again no definitive evidence for neither multiplicative nor additive interactions between religious service attendance and sex (Table 2). When we included cancer in the model, the results were similar to the main model (Supplementary Table 1). When investigating the E-values, we found that for men, an unmeasured confounder would have to be associated 2.35-fold (E-value) and at minimum 1.17-fold (E-valueCI = 1.17) with both the exposure and the outcome to explain away the reported effect (Table 2). Results from the propensity score model confirmed the significant association between religious service attendance and fewer hospitalisations among men (IRR 0.58; 95% CI 0.41–0.80) (Fig. 2B, Table 2). A borderline significant interaction with sex was found (p = 0.05) indicating a stronger association among men than among women (Table 2).
Discussion
Our results demonstrated that religious service attendance is associated with lower mortality (around 30%). When stratifying by sex, the association was found among women (around 44%) but not among men. In addition, a borderline significant overall association was found between religious service attendance and fewer hospitalisations in the entire sample, and with a significant association persisting among men (around 33%). Our results from Denmark—one of the least religious societies in the world—confirm the well-known health benefits of religious service attendance demonstrated in more religious nations such as the US [3, 33,34,35,36,37,38,39]. They are also in line with previous research from Denmark [13] and Finland [14], supporting already available evidence for a protective effect of religious service attendance on mortality among women.
In line with previous evidence regarding sex differences in religiousness [6], we found an indication that Danish women reported religious service attendance slightly more frequently than did men (6.6% vs. 5.0%). Strawbridge et al. reported a relatively strong protective effect of weekly religious attendance on survival for women but a weaker effect for men. For women, the protective effect of weekly religious attendance was of the same magnitude as other health behaviours, whereas for men, it was more modest [40]. In agreement, we found a 44% reduced risk of all-cause mortality for women who participated in a religious organisation, even when taking several potential confounders into account. In contrast, the association with hospitalisations was only significant among men in the main models, with a decreased risk of hospital admissions of 33% in the fully adjusted model, still with moderately strong robustness. A proposed interpretation of the reduced hospitalisation rate for men despite no protection against mortality could perhaps be related to religious organisations supporting their members in time of illness and perhaps especially around the time of death. Religious and cultural aspects might play a role in the decisions regarding dying at home [41]. Thus, if men who participated in religious organisations were more inclined to want to die at home compared with men not participating in religious organisations, this could perhaps explain some of the effect.
While it has been previously proposed that the protective effect of religious attendance is mainly mediated by, e.g., the positive impact of belonging to a social community or having a healthier lifestyle, current studies on mediation analyses have not been able to entirely explain the health effects of religious attendance through physical, psychological, or social processes [2]. Whether some of the protective effect could be mediated by spiritual experience is beyond what natural sciences can account for today. However, with reference to Popper’s “critical rationalism” [42], we argue that rigorous scientific thought should be open for the importance of such experience. More research is needed to understand which factors mediate the protective effects of religious service attendance on health.
The evidence reported in the present study raises interesting questions for public health agencies in secular cultures. People might consider it controversial to encourage religious service attendance as a public health driver, because there are no studies documenting that going from no to frequent religious attendance with the sole motivation of living longer actually works. However, more definitive knowledge of the specific driving factors in the protective effect of religiosity on health could perhaps guide public health initiatives that could support the utilisation of more extensive and broadly understood existential, spiritual, or religious health resources. Efforts to promote community participation for those who already positively self-identify with a religious tradition might also be considered reasonable [43]. Further, needs related to such constructs may also arise in the non-religious patient when confronted with severe illnesses or other life crises. Knowledge about this could enhance the ability of the healthcare system to provide spiritual care for such needs [44, 45].
The strength of this study is information on religiousness from survey interviews linked to Danish registers with almost complete and unselected information on mortality and hospital admissions. The prospective study design with information on religiousness preceding the outcomes and adjustment for several baseline variables, including age, socioeconomic status, marital status, lifestyle variables, and history of diseases, reduces the risk of reverse causation [15]. Adjustment of baseline health is critical in research examining associations between religion and health outcomes since it may be that only those who are relatively healthy can attend religious services [15]. Despite the attempt to adjust for baseline health in the present study, residual confounding cannot be excluded and could, at least to some degree, explain the observed associations. However, to determine the robustness of the results, we applied both classical covariate-adjusted models as well as propensity score models with overall similar results, hence strengthening the interpretation that our results are not a result of residual confounding.
The main limitation in the present study was the limited sample size of approximately 3000 participants, with only 5.9% who attended religious services during the previous month. Consequently, it was impossible to investigate cause-specific mortality and hospitalisations, and the sample size limited the power to detect significant interactions between religious service attendance and sex. Moreover, we were not able to investigate a potential dose–response association because the question only concerned “taking part in a religious organisation within the last month” as a binary variable. Although this question does not specify the type of activity individuals are involved in, we considered it similar to religious service attendance in this study. Thus, religious service attendance was only measured at one time point and may have changed subsequently, which we could not consider in this study. Future studies with the capacity to make such inferences are currently on their way, for instance the EXICODE study by Stripp et al. [46].
Conclusions
This longitudinal Danish cohort study demonstrated that religious service attendance was associated with lower mortality, though mainly among women. Moreover, we found fewer hospitalisations among men who attended religious services. Our results contribute to the limited literature regarding the impact of religiousness on health in a secular society, confirming that the findings from more religious societies also persist in Denmark. However, further research is needed to replicate these findings in a larger sample with the possibility of investigating cause-specific mortality and hospitalisations. In addition, future studies should examine whether certain aspects of religious activity are accountable for the protective effect on mortality and hospitalisations as well as how spiritual needs might become clinically important. These findings could have potential importance for public health policies.
Data availability
SHARE data is free of charge for scientific use globally http://www.share-project.org/data-access.html.
Code availability
Not applicable.
References
Koenig HG, King DE, Carson VB. Handbook of religion and health. Oxford: Oxford University Press; 2012. p. 317.
Kim ES, VanderWeele TJ. Mediators of the association between religious service attendance and mortality. Am J Epidemiol. 2019;188(1):96–101.
Chen Y, Kim ES, VanderWeele TJ. Religious-service attendance and subsequent health and well-being throughout adulthood: evidence from three prospective cohorts. Int J Epidemiol. 2021;49(6):2030–40.
Oksuzyan A, Juel K, Vaupel JW, Christensen K. Men: good health and high mortality. Sex differences in health and aging. Aging Clin Exp Res. 2008;20(2):91–102.
Zuckerman P. Society without God: what the least religious nations can tell us about contentment. New York: New York University Press; 2008.
Hvidtjorn D, Hjelmborg J, Skytthe A, Christensen K, Hvidt NC. Religiousness and religious coping in a secular society: the gender perspective. J Relig Health. 2014;53(5):1329–41.
Olga S. Religion, self-rated health, and mortality: whether religiosity delays death depends on the cultural context. Soc Psychol Personal Sci. 2015;6(8):911–22.
Musick MA, House JS, Williams DR. Attendance at religious services and mortality in a national sample. J Health Soc Behav. 2004;45(2):198–213.
Hummer RA, Rogers RG, Nam CB, Ellison CG. Religious involvement and U.S. adult mortality. Demography. 1999;36(2):273–85.
Strawbridge WJ, Cohen RD, Shema SJ, Kaplan GA. Frequent attendance at religious services and mortality over 28 years. Am J Public Health. 1997;87(6):957–61.
Chida Y, Steptoe A, Powell LH. Religiosity/spirituality and mortality. A systematic quantitative review. Psychother Psychosom. 2009;78(2):81–90.
Li S, Stampfer MJ, Williams DR, VanderWeele TJ. Association of religious service attendance with mortality among women. JAMA Intern Med. 2016;176(6):777–85.
La Cour P, Avlund K, Schultz-Larsen K. Religion and survival in a secular region. A twenty year follow-up of 734 Danish adults born in 1914. Soc Sci Med (1982). 2006;62(1):157–64.
Teinonen T, Vahlberg T, Isoaho R, Kivela SL. Religious attendance and 12-year survival in older persons. Age Ageing. 2005;34(4):406–9.
VanderWeele TJ. Religion and health in Europe: cultures, countries, context. Eur J Epidemiol. 2017;32(10):857–61.
Ahrenfeldt LJ, Hvidt NC, Kjøller ST, Möller S, Lindahl-Jacobsen R. Religiousness and diseases in Europe: findings from SHARE. J Relig Health. 2019;58(6):1925–37.
Ahrenfeldt LJ, Möller S, Andersen-Ranberg K, Vitved AR, Lindahl-Jacobsen R, Hvidt NC. Religiousness and health in Europe. Eur J Epidemiol. 2017;32:1–9.
Opsahl T, Ahrenfeldt LJ, Moller S, Hvidt NC. Religiousness and depressive symptoms in Europeans: findings from the survey of health, ageing, and retirement in Europe. Public Health. 2019;175:111–9.
Ahrenfeldt LJ, Moller S, Hvidt NC, Lindahl-Jacobsen R. Religiousness and lifestyle among Europeans in SHARE. Public Health. 2018;165:74–81.
Herold SC, Hvidt NC, Möller S, Christensen K, Ahrenfeldt LJ. Is religiousness associated with better lifestyle and health among Danes? Findings from SHARE. J Relig Health. 2020;61:1621.
Ahrenfeldt LJ, Scheel-Hincke LL, Kjaergaard S, Moller S, Christensen K, Lindahl-Jacobsen R. Gender differences in cognitive function and grip strength: a cross-national comparison of four European regions. Eur J Pub Health. 2019;29(4):667–74.
Borsch-Supan A, Brandt M, Hunkler C, Kneip T, Korbmacher J, Malter F, et al. Data resource profile: the survey of health, ageing and retirement in Europe (SHARE). Int J Epidemiol. 2013;42(4):992–1001.
SHARE. REGLINK-SHAREDK 2021. http://www.share-project.org/special-data-sets/record-linkage-project/reglink-sharedk.html
Bergmann M, Kneip T, Luca GD, Scherpenzeel A. Survey participation in the Survey of Health, Ageing and Retirement in Europe (SHARE), Wave 1–7. Based on Release 7.0.0. 2019.
Thygesen LC, Daasnes C, Thaulow I, Bronnum-Hansen H. Introduction to Danish (nationwide) registers on health and social issues: structure, access, legislation, and archiving. Scand J Pub Health. 2011;39(7 Suppl):12–6.
Pedersen CB. The Danish civil registration system. Scand J Pub Health. 2011;39(7 Suppl):22–5.
Helweg-Larsen K. The Danish register of causes of death. Scand J Pub Health. 2011;39(7 Suppl):26–9.
Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish national patient registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–90.
SHARE. Survey of Health, Ageing and Retirement in Europe. Release guide 7.1.0. http://www.share-project.org/fileadmin/pdf_documentation/SHARE_release_guide_7-1-1.pdf; 2020
Ariel L, Maya BM, Tyler JV. EVALUE: Stata module for conducting sensitivity analyses for unmeasured confounding in observational studies. S458592 ed: Boston College Department of Economics; 2019.
VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann Intern Med. 2017;167(4):268–74.
VanderWeele TJ, Mathur MB, Chen Y. Outcome-Wide Longitudinal Designs for Causal Inference: A New Template for Empirical Studies. Stat Sci. 2020;35(3):437–66.
Ransome Y. Is investing in religious institutions a viable pathway to reduce mortality in the population? Soc Sci Med. 1982;2020(262):113106.
Pawlikowski J, Bialowolski P, Weziak-Bialowolska D, VanderWeele TJ. Religious service attendance, health behaviors and well-being-an outcome-wide longitudinal analysis. Eur J Public Health. 2019;29(6):1177–83.
Chen Y, Koh HK, Kawachi I, Botticelli M, VanderWeele TJ. Religious service attendance and deaths related to drugs, alcohol, and suicide among US Health Care professionals. JAMA Psychiat. 2020;77(7):737–44.
Spence ND, Farvid MS, Warner ET, VanderWeele TJ, Tworoger SS, Argentieri MA, et al. Religious service attendance, religious coping, and risk of hypertension in women participating in the nurses’ health study II. Am J Epidemiol. 2020;189(3):193–203.
Pawlikowski J, Bialowolski P, Weziak-Bialowolska D, VanderWeele TJ. Religious service attendance, health behaviors and well-being-an outcome-wide longitudinal analysis. Eur J Pub Health. 2019;29:1177.
VanderWeele TJ, Yu J, Cozier YC, Wise L, Argentieri MA, Rosenberg L, et al. Attendance at religious services, prayer, religious coping, and religious/spiritual identity as predictors of all-cause mortality in the black women’s health study. Am J Epidemiol. 2017;185(7):515–22.
VanderWeele TJ, Li S, Tsai AC, Kawachi I. Association between religious service attendance and lower suicide rates among US women. JAMA Psychiat. 2016;73(8):845–51.
Strawbridge WJ, Cohen RD, Shema SJ. Comparative strength of association between religious attendance and survival. Int J Psychiatry Med. 2000;30(4):299–308.
Boussarsar M, Bouchoucha S. Dying at home: cultural and religious preferences. Intensive Care Med. 2006;32(11):1917–8.
Popper KR. The logic of scientific discovery. Hutchinson; 1959.
VanderWeele TJ, Balboni TA, Koh HK. Invited commentary: religious service attendance and implications for clinical care, community participation, and public health. Am J Epidemiol. 2022;191(1):31–5.
Stripp TK, Büssing A, Wehberg S, Andersen HS, Kørup AK, Pedersen HF, et al. Measuring spiritual needs in a secular society: validation and clinimetric properties of the Danish 20-item spiritual needs questionnaire. J Relig Health. 2022;61:3542.
Hvidt NC, Nielsen KT, Korup AK, Prinds C, Hansen DG, Viftrup DT, et al. What is spiritual care? Professional perspectives on the concept of spiritual care identified through group concept mapping. BMJ Open. 2020;10(12):e042142.
Stripp TK, Wehberg S, Büssing A, Andersen-Ranberg K, Jensen LH, Henriksen FL, et al. Protocol for EXICODE: the EXIstential health COhort DEnmark—a register and survey study of adult Danes. BMJ Open. 2022;12(6):e058257.
Acknowledgements
This paper uses data from SHARE Waves 1 and 2 (DOIs: https://doi.org/10.6103/SHARE.w1.600, https://doi.org/10.6103/SHARE.w2.600); see Börsch-Supan et al. for methodological details [22]. The European Commission has funded the SHARE data collection, DG RTD through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782, SHARE-COVID19: GA N°101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, and VS 2020/0313. Furthermore, additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C, RAG052527A) and from various national funding sources is gratefully acknowledged (see www.share-project.org).
Funding
This research was funded by Demography of Sex Differences in Health and Survival, grant number P01 AG031719 (LJA).
Author information
Authors and Affiliations
Contributions
LJA: Conceptualisation, Formal analysis, Investigation, Methodology, Project administration, Visualisation, Roles/Writing—original draft. SM: Formal analysis, Methodology NCH: Supervision TJV: Supervision TKS: Roles/Writing—editing and revisions, Formal analysis, Conceptualisation, Supervision.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
Ethics approval was handled by SHARE (Survey of Health, Aging, and retirement in Europe). See: A., Jürges, Hendrik. The Survey of Health, Aging, and Retirement in Europe – Methodology. MEA, 2005.
Consent to participate
Consent was obtained by SHARE (Survey of Health, Aging, and retirement in Europe). See: Börsch-Supan, A., Jürges, Hendrik. The Survey of Health, Aging, and Retirement in Europe – Methodology. MEA, 2005.
Consent for publication
Consent was obtained by SHARE (Survey of Health, Aging, and retirement in Europe). See: Börsch-Supan, A., Jürges, Hendrik. The Survey of Health, Aging, and Retirement in Europe – Methodology. MEA, 2005.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ahrenfeldt, L.J., Möller, S., Hvidt, N.C. et al. Effect of religious service attendance on mortality and hospitalisations among Danish men and women: longitudinal findings from REGLINK-SHAREDK. Eur J Epidemiol 38, 281–289 (2023). https://doi.org/10.1007/s10654-023-00964-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-023-00964-y