
Abstract
High-dose ionizing radiation is associated with circulatory disease. Risks from lower-dose fractionated exposures, such as from diagnostic radiation procedures, remain unclear. In this study we aimed to ascertain the relationship between fractionated low-to-medium dose radiation exposure and circulatory disease mortality in a cohort of 13,568 tuberculosis patients in Massachusetts, some with fluoroscopy screenings, between 1916 and 1961 and follow-up until the end of 2002. Analysis of mortality was in relation to cumulative thyroid (cerebrovascular) or lung (all other circulatory disease) radiation dose via Poisson regression. Over the full dose range, there was no overall radiation-related excess risk of death from circulatory disease (n = 3221; excess relative risk/Gy −0.023; 95 % CI −0.067, 0.028; p = 0.3574). Risk was somewhat elevated in hypertensive heart disease (n = 89; excess relative risk/Gy 0.357; 95 % CI −0.043, 1.030, p = 0.0907) and slightly decreased in ischemic heart disease (n = 1950; excess relative risk/Gy −0.077; 95 % CI −0.130, −0.012; p = 0.0211). However, under 0.5 Gy, there was a borderline significant increasing trend for all circulatory disease (excess relative risk/Gy 0.345; 95 % CI −0.032, 0.764; p = 0.0743) and for ischemic heart disease (excess relative risk/Gy 0.465; 95 % CI, −0.032, 1.034, p = 0.0682). Pneumolobectomy increased radiation–associated risk (excess relative risk/Gy 0.252; 95 % CI 0.024, 0.579). Fractionation of dose did not modify excess risk. In summary, we found no evidence of radiation-associated excess circulatory death risk overall, but there are indications of excess circulatory death risk at lower doses (<0.5 Gy). Although consistent with other radiation-exposed groups, the indications of higher risk at lower doses are unusual and should be confirmed against other data.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ionizing radiation can cause cancer [1, 2]. Therapeutic doses of ionizing radiation to the heart and large arteries are associated with various types of circulatory disease [3–6]. More recently, and controversially, studies on several groups exposed to low-to-moderate doses of radiation have reported excess mortality and morbidity from circulatory diseases, in particular the Life Span Study (LSS) of Japanese atomic bomb survivors [7] and several occupationally exposed cohorts [8]. There is biological data suggesting there might be a variant response for circulatory disease below vs above about 0.5 Gy [9]. However, the complicated, multifactorial nature of circulatory disease, possible contributions from unmeasured confounders and errors in dose estimates inevitably raise concerns about whether the observed associations are causal [8].
Individuals receiving fluoroscopic X-rays as part of treatment for tuberculosis in Canada and Massachusetts have been studied in relationship to cancer [10–14], but noncancerous diseases have not been so extensively examined. A recent analysis of the Canadian fluoroscopy cohort study indicated small radiation-associated excess relative risks (ERR) of ischemic heart disease (IHD) mortality, with the highest risk for those with the most prolonged period over which the fluoroscopies took place [15]. Radiation-related risks of IHD also decreased significantly with increasing time since first exposure and age at first exposure [15].
We therefore analyzed the Massachusetts tuberculosis fluoroscopy cohort study to assess circulatory disease mortality. We decided a priori to concentrate on the relationship between cumulative lung and thyroid tissue dose (surrogates for dose to the heart and carotid artery, respectively) and death from several circulatory diseases and on possible dose-fractionation associations and modifications by age at exposure and time since exposure. The dose response overall and under 0.5 Gy will be assessed.
Materials and methods
Cohort characteristics and follow-up
The methods used to assemble the Massachusetts tuberculosis fluoroscopy cohort are detailed elsewhere [10, 14, 16]. Briefly, data collected from the medical records of patients with a primary diagnosis of pulmonary tuberculosis between 1915 and 1968 and discharged alive from 12 Massachusetts hospitals were identified, and their medical records were abstracted (Table 1). Cohort entry was defined as the date of admission to one of the participating institutions for treatment of tuberculosis. Of the 13,716 members of the full cohort, 144 were excluded for lack of adequate follow-up information, and another 4 for missing last exposure date, leaving an analysis dataset of 13,568 persons. This dataset is a slightly larger cohort than that considered by Davis et al. [14], because we were more successful at tracing the cohort members originally assembled by Boice [16] and Davis et al. [14]. Data were obtained on pneumothorax treatments, fluoroscopic X-ray exposures (which took place between 1916 and 1961), smoking and alcohol use, and information to assist in locating study subjects. The vital status was determined as of December 31, 2002. Deaths were retrospectively ascertained from the Vital Statistics Offices in the state of last known residence by linking to the mortality files of the Social Security Administration and the National Death Index and by contacting relatives and friends [16]. Vital status was also confirmed through records from the post office, motor vehicle departments, credit bureaus, and other sources [14].
All causes of death on death certificates were coded again using the ninth revision of the International Classification of Diseases (ICD-9). The current analysis describes mortality from all circulatory diseases (ICD-9 codes 390–459), cerebrovascular diseases (CeVD) (ICD-9 430–438), IHD (ICD-9 codes 410–414), hypertensive heart disease (ICD9 401–405), all heart disease (ICD-9 390–429), and other cardiovascular (non-CeVD, non-heart) diseases (ICD-9 439–459) (see Table 1). These endpoints were chosen a priori because they might be radiogenic [8].
Dosimetry
Dosimetry is described elsewhere [14]. Briefly, exposure groups were defined by receipt of air-collapse therapy (pneumothorax/pneumoperitoneum) as indicated on treatment records. Air-collapse therapy was standard treatment for tuberculosis in the 1920s–1940s and involved injecting air into the pleural cavity to force lung tissue away from the chest wall. Typically this procedure was repeated, with the aid of a fluoroscopic examination, 2–3 times per month for over 2 years, and up to 5 years for patients with advanced disease. The radiation dose absorbed by several organs adjacent to the lung and exposed during the fluoroscopic procedures was estimated [17, 18]. This dosimetry method accounted for the number of fluoroscopies, calendar year of exposure, sex, age at treatment (<18, ≥18 years of age), and phantom studies of organ-specific doses using contemporary machine exposure settings to the extent possible.
Cumulative lagged doses to the lung, red bone marrow (RBM) and thyroid were estimated. We regard thyroid dose as a surrogate for dose to the carotid artery, and lung dose as a surrogate for dose to the heart; RBM dose was used because of suggestions of immunologic effects in circulatory disease [19, 20]. Therefore we used thyroid dose to analyze CeVD, and lung dose for all other circulatory disease endpoints, with RBM dose being used for certain sensitivity analyses (Table 6). For most analyses, cumulative dose was lagged by 5 years, as in most previous analyses of these endpoints [8].
Statistical methods
Each patient contributed person-years at risk from 5 years after starting treatment (or entry into the study for those unexposed) to December 31, 2002, or the date of death or last date contacted, whichever occurred earlier. In sensitivity analysis (not shown) we varied the exclusion period from 5 years to between 0 and 10 years. The fitted model assumed that the expected number of deaths in stratum i with cumulative lung/thyroid/RBM dose \( D_{i} \) (in Gy), lung dose rate \( DR_{i} \) (Gy y−1), age at first exposure \( a_{i} \), time since last exposure \( t_{i} \), and associated other covariates \( \left( {X_{ij} } \right)_{j = 1}^{n} \) is given by:
where \( PY_{i} \) is the number of person-years of follow-up. Age at first exposure, years since last exposure and dose rate (defined as the total dose, multiplied by 365.24, and divided by the number of days of irradiation) were centered by subtracting their person-year weighted mean values over the exposed part of the cohort, 26.20, 25.01 years, and 10.44 Gy year−1, respectively. For the purposes of the interaction analysis in Tables 3 and 4 we fitted a slight variant of this model in which for a given factor variable \( X_{m} \) taking values \( 1, \ldots ,M_{m} \) the expected number of deaths is:
It should be emphasized that the models used all incorporated the variables to be used (alcohol consumption, cigarette smoking status, thoracoplasty status, pneumolobectomy status, tuberculous disease status, etc.) in the background model, so that we are testing specifically the adjustment to the radiation dose response. The only exception related to the radiation-specific variables (age at first exposure, years since last exposure, dose rate), which cannot be incorporated in the background model.
Maximum likelihood techniques [21] were used to fit the models with EPICURE [22] and thereby to estimate all the above model parameters, in particular the ERR/Gy, \( \alpha \). All tests were 2-sided with a specified type I error of 0.05, and unless otherwise stated all confidence intervals for risk estimates were derived from the profile likelihood [21]. A forward stepwise procedure [21] determined the form of the model of the underlying risk for each endpoint, in relation to all factors other than radiation dose. Terms were selected for inclusion in the model if a p value of 0.1 or less was achieved by their incorporation. We only evaluated interactions of sex × age and sex × calendar year, and evaluated interactions as groups of variables, namely sex × {ln[age], ln[age]2, …, ln[age]k}, and sex × {year, year2, …, yearm}); the maximal exponents of ln[age], year, namely \( k \), \( m \), were determined by the significance of the associated main effect. The criteria for selection of these groups of interaction variables was the same as for all other variables, namely a p value of 0.1 or less. The results of the analysis of background rates are given in Tables 8, 9, 10, 11, 12, 13 and 14 by endpoint. The forward-stepwise variable selection procedure we used to construct the background rate models was not automated. Automatic variable selection procedures can result in models in which higher polynomial powers of a variable are used, but not all lower order terms, and likewise can add interaction terms without both the associated main effect terms, both of them undesirable features of a model. Certain more automatic forms of the variable selection procedure use a mixture of forward (variable selection) and backward (variable elimination) methods, with different p value thresholds for selection and dropping of variables [23]; the choice of p values requires some care. We have used an alternative fully automatic method, described in “Appendix 2”, using Akaike’s information criterion (AIC) [24, 25] to choose an optimal background model. Minimizing AIC is a standard method of variable selection that avoids over-parameterised (and therefore over-fitted) models. AIC penalises against overfitting by adding 2 × [number of fitted parameters] to the model deviance. The selected variables for each endpoint are given in Table 15. The results of using this automatically selected set of models are shown in Table 16. A mixed forward–backward stepwise procedure was used, implemented in R [26].
We also fitted a simple generalized additive model (GAM) [27], in which the expected number of deaths is:
However, models other than that with the simplest possible radiation effect term, with \( \theta_{1} = \theta_{2} = \theta_{3} = 0 \), proved generally numerically unstable (results not shown). Therefore we present results only for this special case, the constant excess absolute risk (EAR) model:
Inference relates to the EAR coefficient \( \kappa \). Further details are given in Table 17. GAMs were fitted using EPICURE [22] and R [26].
Results
Among persons followed for 5 or more years (345,948 person-years of follow-up), 3221 died of circulatory diseases (Table 1). Overall, radiation had no marked effects on the circulatory system when adjusting for various lifestyle and environmental factors in the background (as per Tables 8, 9, 10, 11, 12, 13 and 14). For all circulatory disease, the ERR/Gy was −0.023 (95 % CI −0.067, 0.028, p = 0.3574, Table 2). There are stronger indications of excess risk for hypertensive heart disease (ERR/Gy = 0.357, 95 % CI −0.043, 1.030, p = 0.0907, Table 2). On the other hand, the dose–response for IHD was negative (ERR/Gy = −0.077, 95 % CI −0.130, −0.012, p = 0.0211, Table 2). The fits of the GAM (Table 17) were also generally non-significant, and some were numerically unstable.
Risk did not change significantly for any endpoint with continuous modification by dose fractionation, age at entry, or time since entry (Table 2). This lack of a marked effect was also the case when factor (grouped) modifications of the temporal and dose rate variables were employed (Table 3).
Cigarette smoking did not significantly modify radiation risk, but the category of alcohol consumption did (p = 0.0075), with statistically significant excess radiation risk in the group whose alcohol consumption was unknown (Table 3).
Thoracoplasty, other surgery, and tuberculosis status did not significantly modify all circulatory disease radiation risk (p > 0.2), but pneumolobectomy did (p = 0.0319), with radiation risk highest (and statistically significant) among those reporting a pneumolobectomy (ERR/Gy = 0.252; 95 % CI 0.024, 0.579; Table 4).
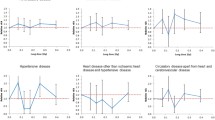
Risk in the low-dose region fluctuated considerably, with indications of excess risk for some endpoints (Fig. 1). If the dose range was restricted to less than 0.5 Gy, borderline significant elevations in ERR were associated with all circulatory disease (ERR/Gy = 0.345; 95 % CI −0.032, 0.764; p = 0.0743), IHD (ERR/Gy = 0.465; 95 % CI −0.032, 1.034; p = 0.0682), and for all heart disease (ERR/Gy = 0.352; 95 % CI −0.067, 0.824; p = 0.1032) (Table 5).

a Dose response for all circulatory disease, and all heart disease, with 95 % CI. b Dose response for cerebrovascular disease, and hypertensive heart disease, with 95 % CI. Lower panel in each graph is low dose (<0.5 Gy) part of upper graph
Different organ doses were associated with a considerable range in risks (Table 6). Risks are particularly large in relation to RBM dose, the use of which increases the ERR/Gy for CeVD more than five-fold (to 0.676, compared with 0.132 for thyroid dose).
The main results used a follow-up period starting 5 years after entry (for those not exposed) or 5 years after last exposure (for those exposed), with cumulative doses lagged by 5 years. The results were essentially unchanged when these exclusion and lagging periods were varied between 0 and 10 years (results not shown). The results of using an automatically selected set of background models, selected to minimize AIC, are shown in Table 16. Comparison of this table with Table 2 indicates that very similar inference results from using this alternative set of background models.
Discussion
We found no strong evidence of radiation-associated excess risks for the all-circulatory disease mortality endpoint. Over the full dose range, there were borderline significant (p ≈ 0.1) indications of an excess risk for hypertensive heart disease. Borderline significant (0.05 < p ≤ 0.10) increasing trends were found for all circulatory disease, IHD, and all heart disease when dose was restricted to <0.5 Gy. Significant excess risk was found for pneumolobectomy. Dose fractionation, age at entry, and time since entry, did not modify radiation risk for circulatory mortality.
The absence of any fractionation effect in the present data contrasts with the inverse fractionation effect observed in the Canadian tuberculosis data [15]. However, the cohorts and analytical methods of these two studies differ in several ways. The significant dose-fractionation effect observed in the Canadian study was estimated for 10-year lagged lung doses, whereas we used 5-year lagged doses. When Canadian data were re-analyzed with the 5-year lag, the dose-fractionation was attenuated and no longer significant [15]. Whereas the Canadian study used time-dependent annual lung doses [15], we relied on cumulative lung and thyroid doses. We also defined dose rate differently. The Canadian study used actual days under treatment and fluoroscopy screening [15], and we defined duration of exposure as the difference between the dates of the first and last fluoroscopy. The two populations also differ, e.g., the Canadian cohort has different calendar times of exposure (1930–1952 vs 1901–1962 in our study). However, risks in the present cohort are entirely consistent with the overall pattern of risk (without adjusting for fractionation) in the Canadian data (Table 7).
Several authors and committees have reviewed evidence for excess risk of circulatory disease in groups exposed to low and moderate doses of radiation (mean dose < 0.5 Gy) [8, 9, 28]. For example, a recent systematic review and meta-analysis [8] documented statistically significant excess risk for three of the four major subtypes of circulatory disease. The risks in the present study, when evaluated over the full dose range or when restricted to less than 0.5 Gy, are similar to results in most other radiation-exposed groups (Table 7).
The candidate biological mechanisms for the circulatory disease effects of radiation have been recently reviewed [9, 28, 29]. At high radiotherapeutic doses (>5 Gy), the cell-killing effect on capillaries and endothelial cells plausibly explains effects on the heart and other parts of the circulatory system [29]. At lower doses (0.5–5 Gy), in humans and in in vivo and in vitro experiments, many inflammatory markers are upregulated long after exposure to radiation, although for exposures less than about 0.5 Gy, the balance shifts toward anti-inflammatory effects [9, 28, 30], implying that the initiating mechanisms for adverse effects in this dose range would not directly result from inflammation. A recent analysis of death from renal failure in the Life Span Study suggests that radiation-induced renal dysfunction may be a factor in increasing the risk of circulatory disease [31], and some experimental data support this suggestion [32].
We used thyroid dose (a surrogate for dose to the carotid artery) to analyze CeVD, and (as in the Canadian tuberculosis analysis [15]) lung dose (a surrogate for heart dose) to analyze all other endpoints. One would expect carotid artery dose to be higher than thyroid dose, but that lung dose is probably lower than heart dose; estimates of both the heart and carotid dose may be wrong by a factor of 2 [33].
Dose-related variations in T cell and B-cell populations in Japanese atomic-bomb survivors suggest that radiation may harm the immune system [34] at doses > 1.5 Gy, implying that whole-body or RBM dose might be the most relevant to the radiation effects of the associated systems. Although other evidence implicates infections and the immune system in cardiovascular disease [19, 35, 36], the negative findings of two randomized-controlled trials of antibiotic administration [37, 38] suggest that bacterial infection is not likely involved in circulatory disease. The somewhat high (albeit non-significant) risks for hypertensive heart disease and CeVD if RBM dose is used (Table 6) (weakly) suggest that dose to this tissue may not be relevant for these endpoints. There is biological data suggesting radiation-associated senescence of monocytes [39], and a somewhat similar mechanism based on monocyte cell killing in the arterial intima suggests that the arterial intima may be causally associated with initiating atheroma in the arterial wall [40] (although there are many other stages between that point and plaque rupture [41, 42]), so that mean arterial dose might be the most relevant organ or tissue dose for studying circulatory disease.
Several recent reviews [8, 9, 28, 43] describe the abundant radiobiological reasons for considering the studies of moderate and low doses separately from studies of high doses. The mechanisms relevant for lower doses are likely to differ from those relevant at higher (e.g., radiotherapeutic) doses. However, risks in studies of medically-exposed groups, with relevant organ doses usually well above 0.5 Gy, are generally consistent with those in populations exposed at the much lower doses and dose rates discussed above [3–6, 44], suggesting that mechanisms operating at high doses and high dose rates may be similar to those at low doses and dose rates. The fact that the IHD risks using mean heart dose in these high-dose/partial-body exposed groups are similar to the risks in the generally uniformly whole-body-exposed groups using whole-body dose discussed above (Table 7) also suggests that mean dose to the heart is the most relevant metric for predicting radiation-associated IHD [44]. In the current analysis, we used lung dose as a surrogate for heart dose.
Epidemiological research has identified specific hereditary and lifestyle risk factors for circulatory disease, including male sex, family history of heart disease, cigarette smoking, diabetes, high blood pressure, obesity, increased low-density lipoprotein cholesterol, and decreased high-density lipoprotein cholesterol plasma concentrations [45–47]. Many studies lack this information on lifestyle factors. Of the studies considered in Table 7 only those of the Japanese atomic-bomb survivors [7, 48], Mayak workers [49, 50], and Canadian fluoroscopy patients [15] had such information. Some lifestyle factors were included in the Nordic breast cancer case–control study [4], and specific medical factors (surgery, thoracoplasty, pneumolobectomy), alcohol consumption, and cigarette smoking were included in the cohort considered here. Cigarette smoking did not modify the dose response in the present cohort, although unknown alcohol consumption and pneumolobectomy did (Tables 3, 4). However, the importance of these findings is unclear, and they may best be interpreted as the effects of chance. In all other radiation-exposed groups with such information there is no evidence that lifestyle factors interacted with radiation risk [4, 7, 48–50].
Strengths of the study include the fact that results are based on a long-term follow-up of a large cohort of subjects of both sexes exposed at different ages. Risks could be evaluated from low-to-moderate radiation doses protracted over time. Dose was evaluated to a number of organs, in particular to the lung, which should be a reasonable surrogate to dose to the heart (as discussed above). The outcome and exposure information are both register-based, so most biases (e.g., due to misclassification of exposure or outcome) are unlikely. As noted above we have information on certain lifestyle and medical variables. A weakness of the study is that there are many other lifestyle and medical risk factors for circulatory disease that we lack information on. These include diabetes, hypertension, and obesity (and related to that exercise). It is possible that these may confound the radiation dose response that we observe. However, as discussed above, there is little information in other studies to suggest interactions of such variables with radiation risk.
The International Commission on Radiological Protection has classified circulatory disease as a tissue reaction effect [51], with a threshold dose of 0.5 Gy. The threshold was derived by fitting a linear model to epidemiologic data and selecting the dose below which there was less than a 1 % chance of an effect. As such this does not represent a true no-effect dose threshold. Schöllnberger et al. [52], analyzing somewhat older Japanese atomic bomb survivor data, concluded that for CeVD and cardiovascular disease, risk estimates are compatible with no risk below threshold doses of 0.62 and 2.19 Gy respectively. However, this analysis is controversial [53]. The analysis of Table 5 suggests that a threshold of the order of 0.5 Gy is marginally inconsistent with the pattern of radiogenic excess risk observed in the Massachusetts tuberculosis fluoroscopy sub-cohort.
In summary, we found no strong evidence of radiation-associated excess risks for the circulatory disease overall. In contrast to the findings in the generally similar (although somewhat larger) Canadian TB fluoroscopy cohort, there was no indication of an inverse fractionation effect. However, borderline significant increasing trends were observed for all circulatory disease, ischemic heart disease, and all heart disease when dose was restricted to <0.5 Gy. The magnitude of the trends both overall and <0.5 Gy are consistent with those in other groups exposed at moderate and low doses. However, the indications of a much steeper low dose slope are unexpected, and should be tested against other data.
References
United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). UNSCEAR 2006 Report. Annex A. Epidemiological Studies of Radiation and Cancer. New York: United Nations; 2008. p. 13–322.
Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation NRC. Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII—Phase 2. Washington, DC: National Academy Press; 2006. p. 1-406.
Little MP, Kleinerman RA, Stovall M, Smith SA, Mabuchi K. Analysis of dose response for circulatory disease after radiotherapy for benign disease. Int J Radiat Oncol Biol Phys. 2012;84(5):1101–9. doi:10.1016/j.ijrobp.2012.01.053.
Darby SC, Ewertz M, McGale P, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368(11):987–98. doi:10.1056/NEJMoa1209825.
Mulrooney DA, Yeazel MW, Kawashima T, et al. Cardiac outcomes in a cohort of adult survivors of childhood and adolescent cancer: retrospective analysis of the Childhood Cancer Survivor Study cohort. BMJ. 2009;339:b4606.
Tukenova M, Guibout C, Oberlin O, et al. Role of cancer treatment in long-term overall and cardiovascular mortality after childhood cancer. J Clin Oncol. 2010;28(8):1308–15. doi:10.1200/JCO.2008.20.2267.
Shimizu Y, Kodama K, Nishi N, et al. Radiation exposure and circulatory disease risk: Hiroshima and Nagasaki atomic bomb survivor data, 1950–2003. BMJ. 2010;340:b5349.
Little MP, Azizova TV, Bazyka D, et al. Systematic review and meta-analysis of circulatory disease from exposure to low-level ionizing radiation and estimates of potential population mortality risks. Environ Health Perspect. 2012;120(11):1503–11. doi:10.1289/ehp.1204982.
McMillan TJ, Bennett MR, Bridges BA, et al. Circulatory disease risk. Report of the independent Advisory Group on Ionising Radiation. Health Protection Agency, Holborn Gate, 330 High Holborn, London; 2010. p. 1–116.
Boice JD Jr, Preston D, Davis FG, Monson RR. Frequent chest X-ray fluoroscopy and breast cancer incidence among tuberculosis patients in Massachusetts. Radiat Res. 1991;125(2):214–22.
Howe GR. Lung cancer mortality between 1950 and 1987 after exposure to fractionated moderate-dose-rate ionizing radiation in the Canadian fluoroscopy cohort study and a comparison with lung cancer mortality in the atomic bomb survivors study. Radiat Res. 1995;142(3):295–304.
Howe GR, McLaughlin J. Breast cancer mortality between 1950 and 1987 after exposure to fractionated moderate-dose-rate ionizing radiation in the Canadian fluoroscopy cohort study and a comparison with breast cancer mortality in the atomic bomb survivors study. Radiat Res. 1996;145(6):694–707.
Little MP, Boice JD Jr. Comparison of breast cancer incidence in the Massachusetts tuberculosis fluoroscopy cohort and in the Japanese atomic bomb survivors. Radiat Res. 1999;151(2):218–24.
Davis FG, Boice JD Jr, Hrubec Z, Monson RR. Cancer mortality in a radiation-exposed cohort of Massachusetts tuberculosis patients. Cancer Res. 1989;49(21):6130–6.
Zablotska LB, Little MP, Cornett RJ. Potential increased risk of ischemic heart disease mortality with significant dose fractionation in the Canadian fluoroscopy cohort study. Am J Epidemiol. 2014;179(1):120–31. doi:10.1093/aje/kwt244.
Boice JD Jr. Follow-up methods to trace women treated for pulmonary tuberculosis, 1930–1954. Am J Epidemiol. 1978;107(2):127–39.
Boice JD Jr, Rosenstein M, Trout ED. Estimation of breast doses and breast cancer risk associated with repeated fluoroscopic chest examinations of women with tuberculosis. Radiat Res. 1978;73(2):373–90.
Boice JD, Monson RR, Rosenstein M. Cancer mortality in women after repeated fluoroscopic examinations of the chest. J Natl Cancer Inst 1981;66(5):863–7.
Ridker PM. Inflammation, infection, and cardiovascular risk: how good is the clinical evidence? Circulation. 1998;97(17):1671–4.
Gura T. Infections: a cause of artery-clogging plaques? Science 1998;281(5373):35–7.
McCullagh P, Nelder JA. Generalized linear models. 2nd edition. Monographs on statistics and applied probability 37. Boca Raton, FL: Chapman and Hall/CRC; 1989. p. 1–526.
Preston DL, Lubin JH, Pierce DA, McConney ME. Epicure release 2.10. Seattle: Hirosoft International; 1998.
Austin PC, Tu JV. Automated variable selection methods for logistic regression produced unstable models for predicting acute myocardial infarction mortality. J Clin Epidemiol. 2004;57(11):1138–46. doi:10.1016/j.jclinepi.2004.04.003.
Akaike H. Information theory and an extension of the maximum likelihood principle. In: Petrov BN, Czáki F, editors. 2nd International symposium on information theory. Budapest: Akadémiai Kiadó; 1973. p. 267–81.
Akaike H. Likelihood of a model and information criteria. J Econ. 1981;16(1):3–14.
R Project. R version 3.1.1 http://www.r-project.org/. 2014.
Hastie T, Tibshirani R. Generalized additive models for medical research. Stat Methods Med Res. 1995;4(3):187–96.
Little MP, Tawn EJ, Tzoulaki I, et al. A systematic review of epidemiological associations between low and moderate doses of ionizing radiation and late cardiovascular effects, and their possible mechanisms. Radiat Res. 2008;169(1):99–109. doi:10.1667/RR1070.1.
Schultz-Hector S, Trott KR. Radiation-induced cardiovascular diseases: is the epidemiologic evidence compatible with the radiobiologic data? Int J Radiat Oncol Biol Phys. 2007;67(1):10–8. doi:10.1016/j.ijrobp.2006.08.071.
Mitchel REJ, Hasu M, Bugden M, et al. Low-dose radiation exposure and atherosclerosis in ApoE −/− mice. Radiat Res. 2011;175(5):665–76. doi:10.1667/RR2176.1.
Adams MJ, Grant EJ, Kodama K, et al. Radiation dose associated with renal failure mortality: a potential pathway to partially explain increased cardiovascular disease mortality observed after whole-body irradiation. Radiat Res. 2012;177(2):220–8. doi:10.1667/RR2746.1.
Lenarczyk M, Lam V, Jensen E, et al. Cardiac injury after 10 Gy total body irradiation: indirect role of effects on abdominal organs. Radiat Res. 2013;180(3):247–58. doi:10.1667/RR3292.1.
Rosenstein M. Personal communication to Mark Little. 2014.
Kusunoki Y, Kyoizumi S, Hirai Y, et al. Flow cytometry measurements of subsets of T, B and NK cells in peripheral blood lymphocytes of atomic bomb survivors. Radiat Res. 1998;150(2):227–36.
Danesh J, Whincup P, Lewington S, et al. Chlamydia pneumoniae IgA titres and coronary heart disease. Prospective study and meta-analysis. Eur Heart J. 2002;23(5):371–5. doi:10.1053/euhj.2001.2801.
Whincup P, Danesh J, Walker M, et al. Prospective study of potentially virulent strains of Helicobacter pylori and coronary heart disease in middle-aged men. Circulation. 2000;101(14):1647–52.
Grayston JT, Kronmal RA, Jackson LA, et al. Azithromycin for the secondary prevention of coronary events. N Engl J Med. 2005;352(16):1637–45. doi:10.1056/NEJMoa043526.
Cannon CP, Braunwald E, McCabe CH, et al. Antibiotic treatment of Chlamydia pneumoniae after acute coronary syndrome. N Engl J Med. 2005;352(16):1646–54. doi:10.1056/NEJMoa043528.
Lowe D, Raj K. Premature aging induced by radiation exhibits pro-atherosclerotic effects mediated by epigenetic activation of CD44 expression. Aging Cell. 2014;13(5):900–10. doi:10.1111/acel.12253.
Little MP, Gola A, Tzoulaki I. A model of cardiovascular disease giving a plausible mechanism for the effect of fractionated low-dose ionizing radiation exposure. PLoS Comput Biol. 2009;5(10):e1000539. doi:10.1371/journal.pcbi.1000539.
Fuster V, Moreno PR, Fayad ZA, Corti R, Badimon JJ. Atherothrombosis and high-risk plaque: part I: evolving concepts. J Am Coll Cardiol. 2005;46(6):937–54. doi:10.1016/j.jacc.2005.03.074.
Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque. J Am Coll Cardiol. 2006;47(8 Suppl):C13–8. doi:10.1016/j.jacc.2005.10.065.
Little MP, Tawn EJ, Tzoulaki I, et al. Review and meta-analysis of epidemiological associations between low/moderate doses of ionizing radiation and circulatory disease risks, and their possible mechanisms. Radiat Environ Biophys. 2010;49(2):139–53. doi:10.1007/s00411-009-0250-z.
Little MP, Zablotska LB, Lipshultz SE. Ischemic heart disease after breast cancer radiotherapy. N Eng J Med. 2013;368(26):2523–4. doi:10.1056/NEJMc1304601#SA1.
Burns DM. Epidemiology of smoking-induced cardiovascular disease. Prog Cardiovasc Dis. 2003;46(1):11–29. doi:10.1016/S0033-0620(03)00079-3.
Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998;97(18):1837–47.
Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–52. doi:10.1016/S0140-6736(04)17018-9.
Yamada M, Wong FL, Fujiwara S, Akahoshi M, Suzuki G. Noncancer disease incidence in atomic bomb survivors, 1958–1998. Radiat Res. 2004;161(6):622–32. doi:10.1667/RR3183
Azizova TV, Muirhead CR, Druzhinina MB, et al. Cardiovascular diseases in the cohort of workers first employed at Mayak PA in 1948–1958. Radiat Res. 2010;174(2):155–68. doi:10.1667/RR1789.1.
Azizova TV, Haylock RGE, Moseeva MB, Bannikova MV, Grigoryeva ES. Cerebrovascular diseases incidence and mortality in an extended Mayak Worker Cohort 1948–1982. Radiat Res. 2014;182(5):529–44. doi:10.1667/RR13680.1.
International Commission on Radiological Protection. ICRP statement on tissue reactions and early and late effects of radiation in normal tissues and organs - threshold doses for tissue reactions in a radiation protection context. ICRP publication 118. Ann. ICRP. 2012;41(1–2):1–322. doi:10.1016/j.icrp.2007.10.003.
Schöllnberger H, Kaiser JC, Jacob P, Walsh L. Dose-responses from multi-model inference for the non-cancer disease mortality of atomic bomb survivors. Radiat Environ Biophys. 2012;51(2):165–78. doi:10.1007/s00411-012-0410-4.
Little MP, Azizova TV, Bazyka D, et al. Comment on “Dose-responses from multi-model inference for the non-cancer disease mortality of atomic bomb survivors” (Radiat. Environ. Biophys (2012) 51:165–178) by Schöllnberger et al. Radiat Environ Biophys 2013;52(1):157–9. doi:10.1007/s00411-012-0453-6.
McGeoghegan D, Binks K, Gillies M, Jones S, Whaley S. The non-cancer mortality experience of male workers at British Nuclear Fuels plc, 1946-2005. Int J Epidemiol. 2008;37(3):506–18. doi:10.1093/ije/dyn018.
Muirhead CR, O’Hagan JA, Haylock RGE, et al. Mortality and cancer incidence following occupational radiation exposure: third analysis of the National Registry for Radiation Workers. Br J Cancer. 2009;100(1):206–12. doi:10.1038/sj.bjc.6604825.
Vrijheid M, Cardis E, Ashmore P, et al. Mortality from diseases other than cancer following low doses of ionizing radiation: results from the 15-Country Study of nuclear industry workers. Int J Epidemiol. 2007;36(5):1126–35. doi:10.1093/ije/dym138.
Krestinina LY, Epifanova S, Silkin S, et al. Chronic low-dose exposure in the Techa River Cohort: risk of mortality from circulatory diseases. Radiat Environ Biophys. 2013;52(1):47–57. doi:10.1007/s00411-012-0438-5.
Grosche B, Lackland DT, Land CE, et al. Mortality from cardiovascular diseases in the Semipalatinsk historical cohort, 1960–1999, and its relationship to radiation exposure. Radiat Res. 2011;176(5):660–9. doi:10.1667/RR2211.1.
Acknowledgments
MPL and AVB were supported by the Intramural Research Program of the National Institutes of Health, the National Cancer Institute (NCI), Division of Cancer Epidemiology and Genetics, and LBZ by NCI grants 5K07CA132918 and 1R03CA188614. The authors are grateful for the detailed and helpful comments of Dr Marvin Rosenstein and a referee.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no financial conflicts of interest.
Appendices
Appendix 1: Background models selected
See Tables 8, 9, 10, 11, 12, 13 and 14.
Appendix 2: Effect of alternative background models selected via minimizing Akaike information criterion
In this appendix we consider an alternative set of explanatory background models for each endpoint, selected via an automatic variable selection process, by minimizing the Akaike information criterion (AIC) [24, 25]. Minimizing AIC is a standard method of variable selection that avoids over-parameterised (and therefore over-fitted) models. AIC penalizes against overfitting by adding 2 × [number of fitted parameters] to the model deviance. We used an iterative mixed-forward–backward stepwise procedure to minimize AIC using models with Poisson error via R [26].
The models used the set of candidate variables listed in Table 15, in which the optimal models chosen are also indicated. We provide the analog of Table 2 using these alternative background models in Table 16.
Appendix 3: Generalized additive models (GAM)
See Table 17.
Rights and permissions
About this article

Cite this article
Little, M.P., Zablotska, L.B., Brenner, A.V. et al. Circulatory disease mortality in the Massachusetts tuberculosis fluoroscopy cohort study. Eur J Epidemiol 31, 287–309 (2016). https://doi.org/10.1007/s10654-015-0075-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-015-0075-9