
Abstract
Several prospective studies considered the relation between coffee consumption and mortality. Most studies, however, were underpowered to detect an association, since they included relatively few deaths. To obtain quantitative overall estimates, we combined all published data from prospective studies on the relation of coffee with mortality for all causes, all cancers, cardiovascular disease (CVD), coronary/ischemic heart disease (CHD/IHD) and stroke. A bibliography search, updated to January 2013, was carried out in PubMed and Embase to identify prospective observational studies providing quantitative estimates on mortality from all causes, cancer, CVD, CHD/IHD or stroke in relation to coffee consumption. A systematic review and meta-analysis was conducted to estimate overall relative risks (RR) and 95 % confidence intervals (CI) using random-effects models. The pooled RRs of all cause mortality for the study-specific highest versus low (≤1 cup/day) coffee drinking categories were 0.88 (95 % CI 0.84–0.93) based on all the 23 studies, and 0.87 (95 % CI 0.82–0.93) for the 19 smoking adjusting studies. The combined RRs for CVD mortality were 0.89 (95 % CI 0.77–1.02, 17 smoking adjusting studies) for the highest versus low drinking and 0.98 (95 % CI 0.95–1.00, 16 studies) for the increment of 1 cup/day. Compared with low drinking, the RRs for the highest consumption of coffee were 0.95 (95 % CI 0.78–1.15, 12 smoking adjusting studies) for CHD/IHD, 0.95 (95 % CI 0.70–1.29, 6 studies) for stroke, and 1.03 (95 % CI 0.97–1.10, 10 studies) for all cancers. This meta-analysis provides quantitative evidence that coffee intake is inversely related to all cause and, probably, CVD mortality.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Coffee is the second most common beverage in the world after tea. Thus, any health effect of coffee is an important issue of public health. Besides caffeine, coffee contains many bioactive compounds with potential effects on health [1], including minerals and antioxidants, mainly phenolic compounds (such as chlorogenic, caffeic, ferulic and cumaric acids), melanoidins and diterpenes (such as cafestol and kahweol). Coffee has been related with lower incidence of diabetes [2], stroke[3] and cancer at selected sites [4–8].
To date 25 prospective studies considered the quantitative relation between coffee and mortality for all causes [9–33]. Among these, 21 found an inverse or null association (including the most recent paper based on the large NIH-AARP Diet and Health Study[32]), one cohort study of US Seventh-day Adventists found a significant positive association [16], and three studies found a significant increased risk only in men [13, 26, 33].
An estimate of the relation between cardiovascular disease (CVD) mortality and coffee was provided by 22 studies [10, 11, 14–16, 18–22, 25, 27, 29, 30, 32, 34–40]. Most of these found no relation or a moderate inverse association, significant in 4 studies [18–20, 32], while 4 studies found an increased risk [10, 14, 16, 40]. The relation of coffee with mortality for coronary/ischemic heart disease (CHD/IHD) was considered in 17 studies, reporting inconsistent results [10, 11, 14–16, 18, 19, 23, 26, 29, 30, 35–40]. Of the 8 studies considering stroke mortality [10, 20, 26, 29, 30, 32, 39, 40], 5 found no relation [26, 29, 30, 32, 39].
Estimates of the relation between coffee and all cancers mortality have been provided from 13 prospective studies, overall reporting no relation [12, 15, 16, 20, 22, 23, 25, 27, 30–32, 34, 41].
Since most studies included a few deaths and were possibly underpowered to detect an association, we combined all published data on the relation of coffee with mortality from all cause, CVD, CHD/IHD, stroke and all cancers, using a meta-analytic approach.
Methods
Data sources and search
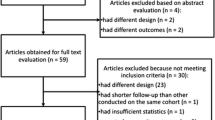
We carried out a PubMed search in January 2013 using the string ‘(prospective OR cohort) AND (fatal OR death OR mortality) AND (hot beverages OR coffee OR caffeine)’, following the Meta Analysis of Observational Studies in Epidemiology (MOOSE) guidelines [42]. A similar strategy was used to search Embase. The searches were limited to human studies written in English. A flow chart of the procedure to select studies is shown in Fig. 1. From the 889 and 2,274 articles retrieved on Pubmed and Embase, three authors (SM, AT, FT) separately selected the studies reporting data on the association between coffee and all cause and/or selected cause-specific mortality, including deaths for CVD, CHD/IHD, stroke and all cancers. Discrepancies between review team members were discussed and resolved.

Flow-chart of the selection of studies included in the meta-analyses. RR relative risk
Study selection
Most studies were not focused on the relation between coffee and mortality, and were no longer considered. Of the 92 publications selected, 58 were not included for at least one of the following reasons: (a) did not report original results from cohort studies; (b) did not provide relative risks (RR) and the corresponding confidence intervals (CI) or information sufficient to calculate them; (c) considered together the disease incidence and mortality; (d) analyzed special populations (e.g. diabetics, people with heart conditions); (e) investigated patients with specific cancers (we included only studies considering total cancer mortality). The reference lists of the remaining 34 articles were checked to obtain other pertinent publications, and 2 additional report was identified [26]. Of the 36 articles selected, 8 were excluded since they reported information on caffeinated drinks [43, 44], or were duplicate reports on the same population [45, 46], or had a number of deaths below 100 [47], or had the upper cutpoint of the reference category too high [10, 12, 34], since for the present analyses we considered as reference category ≤1 cup/day of coffee consumption. No study was excluded a priori for weakness of design or data quality, and we did not assign quality scores to the studies.
Thus, the present analyses were based on 28 prospective studies whose main characteristics are reported in eTable 1 [9, 11, 13–24, 26–33, 35, 37–41]. We summarized decisions and operations on original data for each study in the column “notes”.
Data extraction
We abstracted from the selected studies the following information in a standard format: study design, country, number of subjects (total number of deaths, total cohort size or the number of person-years of follow-up), in general and for each category of coffee consumption, duration of follow-up (years of enrolment and study end, and mean/median duration of follow-up), sex, RR for the categories of coffee intake and the corresponding CIs, type of coffee, outcomes considered and covariates adjusted in the model. Discrepancies between the authors were discussed and resolved.
When a study did not report the RR or the CI, but reported sufficient data to calculate them (i.e. the number of cases and non-cases for each category of coffee consumption), we estimated the RRs and the corresponding 95 % CIs from raw data [9, 11, 23, 26]. When a study reported the adjusted RR but not the corresponding CI, we calculated the CI of the crude RR, and related them to the adjusted RR [14, 18]. If a study provided more than one RR, the one adjusted for the largest number of confounding factors was included in the analysis. When a study reported data on both regular and decaffeinated coffee, data were collected separately [22, 24, 27, 32].
Data synthesis and analysis
All studies reported data on coffee consumption measured in cups/day. As reference category (defined as low drinking) we used either no consumption [17, 18, 21, 22, 25, 26, 30, 32, 37, 38], or the lowest category of coffee consumption considered in each paper, i.e. occasional drinking[20, 23, 27, 33, 40, 41] or drinking up to 1 cup/day [11, 14, 16, 19, 24, 28, 31, 35, 39].
For all cause mortality, we pooled the RRs for the study-specific highest category of coffee consumption versus low drinking, using random-effects models, which consider both within and between study variation. Since smoking is a major confounder of the possible relationship between coffee consumption and mortality for several causes, we excluded from all further analyses studies reporting RRs not adjusted for smoking [9, 11, 23, 26, 35]. Thus, analyses for cause-specific mortality were carried out considering only smoking-adjusting studies.
We selected studies reporting three or more categories of coffee consumption and computed the pooled RRs for an increment of coffee of 1 cup/day. To obtain the information on the dose–response relationship we used the method proposed by Greenland and Longnecker [48], which estimates the study specific RRs for the increment of one unit of consumption by relating the natural logarithm of the RR to the corresponding mean value of intake across exposure categories. This method takes into account that estimates of risk for successive levels of intake are correlated. Open-ended upper categories were considered of the same amplitude as the previous one. The overall RR for an increment of 1 cup/day of coffee was then obtained by pooling the corresponding study-specific RRs with random-effects models.
For all causes and CVD mortality, we computed the pooled RRs for consumption of coffee of ≤3 cups/day (moderate) and >3 cups/day (heavy) versus low drinking. When more than one RR estimate in a study fell in the range considered for moderate or heavy coffee drinking, we first pooled for each study the corresponding estimates using the Hamling et al. method [49]. For all cause and CVD mortality we also computed the pooled RRs including only studies whose highest category of coffee was of at least ≤4 cups/day [13–15, 17–19, 22, 24, 25, 27–29, 31, 32, 37, 39].
Heterogeneity among studies was assessed using the χ2 test, and was defined as a p value <0.10. Moreover, potential heterogeneity was quantified through the I2 statistic, which describes the percentage of total variation across studies due to heterogeneity, rather than chance [50]. Usually low heterogeneity is defined by values of the I2 statistic <25 %, while values of such statistic >75 % are indicative of high heterogeneity.
Publication bias was assessed by funnel plot and by the Begg’s and Mazumdar’s [51], and Egger’s tests [52]. All the statistical analyses were performed using the STATA software (version 11; StataCorp, College Station, TX, USA).
Results
Mortality from all causes
Figure 2 shows the RRs of all cause mortality for the study-specific highest versus low (≤1 cup/day) coffee drinking categories for 23 prospective studies. The pooled RRs were 0.88 (95 % CI 0.84–0.93, p for heterogeneity <0.001, I2 = 68.7 %) for all studies, 0.88 (95 % CI 0.80–0.97) for the 17 studies considering men, and 0.86 (95 % CI 0.82–0.90) for the 13 studies reporting the relation in women.

Total and sex-specific relative risks (RRs) of the relation of all cause mortality with coffee intake. The pooled RRs were calculated using the random-effects models. RR for the study-specific highest coffee drinking category versus low drinking (<1 cup/day) from all the studies combined. *Non smoking adjusting studies
Table 1 shows the combined RRs of all cause mortality for the highest versus low coffee category in strata of selected study characteristics. The pooled RR from the 4 studies with RRs not adjusted for tobacco smoking was 0.91 (95 % CI 0.81–1.01). The corresponding RR for the 19 studies adjusting for tobacco smoking was 0.87 (95 % CI 0.82–0.93), similar in men and women. Among smoking adjusting studies, the pooled RRs were 0.92 (95 % CI 0.85–1.00) for studies conducted in North America, 0.85 (95 % CI 0.76–0.95) for those conducted in Europe, and 0.76 (95 % CI 0.63–0.91) for studies conducted in Japan (p for heterogeneity among RRs in geographic regions = 0.138). The pooled RR was 0.88 (95 % CI 0.83–0.93) for alcohol adjusting papers and 0.81 (95 % CI 0.61–1.08) for those non adjusting for alcohol (p for heterogeneity = 0.577). When we included in the meta-analysis only studies whose reference category was non-drinking, the pooled RR for the highest category of intake was 0.87 (95 % CI 0.83–0.94, p for heterogeneity = 0.42).
There was no evidence of publication bias in the 19 smoking adjusting studies, as tested using Egger’s (p = 0.114) and Begg’s (p = 0.118) tests.
The pooled RR for a consumption increment of 1 cup/day of coffee was 0.97 (95 % CI 0.96–0.98, p for heterogeneity <0.001, I2 = 80.7 %), obtained pooling the RRs of the 17 smoking adjusting studies considering at least three categories of coffee consumption (Fig. 3).

Total and sex specific relative risks (RRs) of the relation of all cause mortality with coffee intake, including only smoking adjusting studies. RR for an increment of coffee drinking of 1 cup/day. The pooled RRs were calculated using the random-effects models
Four studies considered the relation of total mortality with decaffeinated coffee [22, 24, 27, 32]. The pooled RRs for the study-specific highest versus low (≤1 cup/day) decaffeinated coffee intake were 0.90 (95 % CI 0.82–0.99) in both sexes combined, 0.86 (95 % CI 0.80–0.92) in men and 0.83 (95 % CI 0.76–0.91) in women.
Mortality from CVD
The meta-analysis on the relation of overall CVD mortality with coffee included 17 smoking adjusting studies reporting quantitative estimates for CVD and/or CHD/IHD and/or stroke mortality, whose main characteristics are reported in eTable 1. There was no evidence of publication bias overall, as tested using Egger’s (p = 0.963) and Begg’s (p = 0.981) tests.
The combined RR for the study-specific highest versus low (≤1 cup/day) categories of coffee was 0.89 (95 % CI 0.77–1.02, p for heterogeneity <0.001, I2 = 75.7 %) for all subjects, 0.92 in men and 0.84 in women (Fig. 4a). The pooled RR for a consumption increment of 1 cup/day of coffee was 0.98 (95 % CI 0.95–1.00, p for heterogeneity <0.001, I2 = 87.8 %), from 16 studies (Fig. 4b). The corresponding RRs were 0.99 (95 % CI 0.95–1.03) in men, and 0.95 (95 % CI 0.92–0.98) in women.

Total and sex specific relative risks (RRs) of the relation of cardiovascular (CVD) mortality with coffee intake, including only smoking adjusting studies. The pooled RRs were calculated using the random-effects models. a RR for the study-specific highest coffee drinking category versus low drinking (≤1cup/day). b RR for an increment of coffee drinking of 1 cup/day
Table 2 reports the pooled RRs on mortality for CHD/IHD and stroke separately, for the study-specific highest category of coffee drinking compared with low drinking and for an increment of 1 cup/day of coffee. The RRs for CHD/IHD were respectively 0.95 (95 % CI 0.78–1.15, 1.09 in men and 0.77 in women) and 1.00 (95 % CI 0.97–1.04). The corresponding RRs for stroke were 0.95 (95 % CI 0.70–1.29, 0.72 in men and 1.21 in women) and 0.97 (95 % CI 0.94–1.01). The pooled RRs for the study-specific highest category of coffee drinking compared with low drinking were 0.92 (95 % CI 0.73–1.14) for studies conducted in North America, 0.85 (95 % CI 0.73–0.99) for those conducted in Europe, and 0.89 (95 % CI 0.51–1.56) for studies conducted in Japan (p for heterogeneity among RRs in geographic regions = 0.846). The RRs were 0.84 (95 % CI 0.73–0.96) when we pooled the studies adjusting for alcohol intake, and 0.96 (95 % CI 0.77–1.20) among non alcohol adjusting studies (p for heterogeneity = 0.315).
Mortality from all cancers
The meta-analysis on the relation between all cancer mortality and coffee was based on 10 smoking adjusting studies, whose main characteristics are reported in eTable 1. There was small evidence of publication bias overall, as tested using Egger’s (p = 0.067) and Begg’s (p = 0.075) tests.
The pooled RR for the study-specific highest versus low (≤1 cup/day) categories of coffee was 1.03 (95 % CI 0.97–1.10), with no significant heterogeneity among studies (p for heterogeneity = 0.647, I2 = 0 %); the corresponding RRs were 1.07 in men and 0.98 in women (Table 3). Nine studies included three or more categories of coffee intake. Based on these studies, the combined RR for an increment of 1 cup/day of coffee was 1.00 (95 % CI 0.99–1.01), similar in men and women.
The pooled RRs for the study-specific highest versus low coffee intake were 1.05 (95 % CI 0.99–1.13, p for heterogeneity = 0.844) among 4 studies conducted in North America, 0.79 (95 % CI 0.39–1.57, p for heterogeneity = 0.555) among 2 studies conducted in Europe, and 0.94 (95 % CI 0.80–1.09, p for heterogeneity = 0.357) among 4 studies conducted in Japan (p for heterogeneity among RRs in geographic regions = 0.329). We found pooled RRs for the study-specific highest versus low coffee intake of 1.05 (95 % CI 0.98–1.11, p for heterogeneity = 0.968) among 7 studies adjusting for alcohol intake, and 0.84 (95 % CI 0.60–1.16, p for heterogeneity = 0.128) among 3 studies non adjusting for alcohol intake (p for heterogeneity = 0.192).
Additional analyses on the dose-risk relation for all cause and CVD mortality
Based on smoking adjusting studies, compared with low drinking (≤1 cup/day), the pooled RRs for all cause mortality were 0.91 (95 % CI 0.88–0.94) for coffee drinking ≤3 cups/day and 0.87 (95 % CI 0.82–0.92) for drinking >3 cups/day (Table 4). When we selected studies whose highest category of coffee was at least ≤4 cups/day, the pooled RR was 0.87 (95 % CI 0.83–0.91, p for heterogeneity = 0.12) from 14 studies, with no differences between sexes. The corresponding RRs for CVD mortality were 0.87 (95 % CI 0.79–0.96, 0.92 in men and 0.80 in women) for drinking ≤3 cups/day, 0.88 (95 % CI 0.77–1.02, 0.92 in men and 0.80 in women) for drinking >3 cups/day. When we selected studies whose highest category of coffee was at least ≥4 cups/day, the pooled RR was 0.86 (95 % CI 0.77–0.97, 0.90 in men and 0.80 in women).
Discussion
The present meta-analysis, carried out on 23 prospective studies, found a 12 % decreased risk of all cause mortality for the highest coffee intake compared with an intake of up to 1 cup/day among smoking-adjusting studies. The risk was 3 % significantly lower for an increment of consumption of 1 cup/day of coffee, and the inverse association was stronger for heavy than moderate coffee drinking, suggesting a dose-risk relation. Among smoking-adjusting studies, only 4 studies included in the meta-analysis found RR >1 in men [13, 14, 33]. The RRs for the highest versus the lowest category of coffee were below unity, although not significantly, also in the two studies excluded from the meta-analysis because they had a reference category >1 cup/day. In those studies the RRs were 0.95 (95 % CI 0.86–1.05) for drinking ≥7 cups/day compared with ≤2 cups/day [12], and 0.82 (95 % CI 0.48–1.4) in men and 0.61 (95 % CI 0.33–4.15) in women for drinking ≥5 cups/day compared with <5 cups/day[10] Another study, excluded from the meta-analysis since it was based on 162 subjects and 53 deaths, [47] reported a RR of 0.35 (95 % CI 0.20–0.64) for the highest tertile of intake (>2 cups/week) compared to the lowest one (<1 cup/week), with a dose-risk relation.
The exclusion of any study from the analysis did not materially change the summary estimates, and p values from Begg’s and Egger’s tests, together with the absence of significant asymmetry in the funnel plot, indicate that publication bias is unlikely to have appreciably influenced our results. We could not stratify for smoking status, as only 4 papers reported separate estimates for never, former and current smokers [14, 17, 27, 32], and, of these, two studies did not report confidence intervals [14, 17]. The two papers reporting all the information showed a tendency towards a lower RR in never smokers than in current smokers [27, 32]. The existence of an inverse association was further supported by the consistent results of several sensitivity analyses and by the consistency of results across studies conducted in Asia and in North America/Europe, where coffee consumption is higher.
We found an inverse association of borderline significance between coffee and CVD, accordingly with the results of a meta-analysis of fatal and non fatal CHD [53], although the two meta-analyses shared only 7 studies. In fact, differently from the present meta-analysis, the previous one included also studies not adjusting for tobacco smoking and those considering as endpoints also incident for CVD. Moreover, the present meta-analysis included other 10 original studies, [20, 21, 25, 27, 29, 30, 32, 38–40] 8 of which published after the Wu et al. [53] meta-analysis.
For CVD mortality, the favorable effect of coffee appeared similar to that for all cause mortality, although there was no clear dose-risk relation. For fatal stroke, we did not confirm the finding of a protective effect of coffee on stroke incidence reported in a few prospective studies [54–56], though the summary RR was below unity in the present meta-analysis, too.
The effect of coffee on CVD is probably complex and possibly a combination of unfavorable and favorable effects of caffeine and other coffee components on the cardiovascular system. Among unfavorable effects, caffeine has inotropic effect on the heart, and induces a transient increase in blood pressure [57]. However, habitual coffee drinking of >3 cups/day was not associated with an increased risk of hypertension, compared with <1 cup/day [58], and also in hypertensive subjects coffee had no long-term effects and did not increase CVD risk [59]. As for cholesterol levels, coffee has been related to cholesterol increase in Nordic countries [60], but not in other populations [61], and a meta-analysis of 14 clinical trials showed increased serum levels of cholesterol and low density lipoprotein (LDL) only for boiled unfiltered coffee [62]. In fact, diterpenes (such as cafestol and kahweol), responsible for this effect, are mostly bound to coffee filters, and the small amount crossing the filters has no effects on serum lipids [62], including high density lipoproteins (HDL) and triglycerides [63]. Among favorable effects on CVD risk, coffee decreased the risk of diabetes incidence[2] and might decrease CVD risk in diabetic patients [64, 65]. Caffeine has been associated with lower body weight and with decreased platelet aggregation [66]. Coffee has been associated with a lower risk of incident gout [67], higher adiponectin levels in Japanese males [68], inhibition of inflammation in a prospective study of postmenopausal women [22], and beneficial effects on subclinical inflammation in a clinical trial [69]. Moderate doses of coffee have no unfavorable effect on heart failure [70], valvular heart disease [38], and cardiac arrhythmias [71]. Moreover, coffee is very rich in antioxidants[72] which may have a general favorable effect on health.
The favorable effect of coffee on total mortality is however not fully explainable through the effect of coffee on CVD mortality. Favorable effects of coffee on health may also include decreased risk of diabetes mortality [32], and of suicide or injury and accident mortality [17, 32, 73], through its favorable effects on well-feeling and alertness.
In agreement with most evidence, we found no association of coffee with all cancer mortality. In a sensitivity analysis, when considering the 6 studies whose highest category of consumption was at least ≥4 cups/day, we found a RR of 1.04 (95 % CI 0.98–1.11, 1.08 in men and 1.01 in women). An inverse association has been reported by a meta-analysis considering the relation of coffee with incidence of total cancer [74], and by meta-analyses considering incidence of cancer at selected sites, such as cancer at the oral cavity and pharynx [7, 8], liver [4], endometrium [5], which, however, are relatively infrequent. An inverse relation of coffee intake with incidence of colorectal cancer was found in case–control [75], but not in cohort studies [6, 76].
A significant heterogeneity across studies was found. A possible source of heterogeneity is that type of coffee powder, brewing methods, preparation and cup size vary widely in different populations and this may modify the relation, since coffee content of several antioxidants and lipids varies depending on the type of coffee powder (Arabica or Robusta), roasting, and beverage preparation [77]. However, most studies did not report such information. The amount of coffee intake was self-reported. However, recall of coffee drinking has been shown satisfactorily reproducible and valid [78, 79]. Other possible sources of variability are the arbitrary classification of consumption with different cut-points in various studies, and the fact that studies included in these meta-analyses did not consider genetic variants associated with coffee drinking, such as CYP1A2, which is responsible for more than 95 % of caffeine metabolism, and consequently of the effects of caffeine and coffee consumption [80]. However, no heterogeneity emerged in the analyses considering more homogeneous categories of coffee intake, such as non-drinking as reference category or drinking ≥4 cups/day as the highest category, in the absence of material variations of the pooled RRs. With reference to confounding, the major avoidable risk factors for all cause, CVD and cancer mortality also associated with coffee drinking are tobacco smoking and alcohol drinking [81]. Although we excluded from most analyses studies reporting risk estimates not adjusted for tobacco smoking, we cannot exclude residual confounding, which, however, should weaken any inverse association. The pooled RRs were similar in studies adjusting or not for alcohol intake, further suggesting a real inverse relation between coffee intake and total mortality. The lack of adjustment in a few early studies for other relevant confounding factors, such as education, body mass index, or physical activity, might also have somewhat affected our results.
We were unable to consider the relation between caffeine and mortality because most published studies reported only the number of cups of coffee, with no information on total caffeine intake. However, although caffeine intake depends on the variety of raw coffee and the preparation method, and it is also found in cola, energy drinks and several drugs, coffee drinking is its major source and total caffeine intake is strongly correlated with coffee intake in Europe and North America [82]. The inverse association found for decaffeinated coffee with total mortality suggests, however, that substances other than caffeine are responsible of the favorable effect of coffee on mortality. The observation of an inverse relation between decaffeinated coffee and total mortality is based on few studies [22, 24, 27, 32]; moreover, drinkers generally consume low amount of decaffeinated coffee, and in most studies it was not possible to separate drinkers of both regular and decaffeinated coffee from drinkers of decaffeinated coffee only.
A more relevant possible source of bias is reverse causation, since it is possible that healthier people consume more coffee than those with chronic diseases associated with higher mortality rates. However, against this possibility is the fact that the overall estimates were derived only from prospective studies with information collected long time before death, and in most original studies subjects with cancer or CVD at baseline were excluded.
Although bias and confounding were unlikely responsible for the observed association, given the consistent results in different countries, settings and time, the interpretation of the inverse association of coffee with all cause and CVD mortality remains open to discussion, also considering the lack of information on the relation with duration and other time-related factors.
References
Ferruzzi MG. The influence of beverage composition on delivery of phenolic compounds from coffee and tea. Physiol Behav. 2010;100(1):33–41. doi:10.1016/j.physbeh.2010.01.035.
Huxley R, Lee CM, Barzi F, et al. Coffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus: a systematic review with meta-analysis. Arch Intern Med. 2009;169(22):2053–63. doi:10.1001/archinternmed.2009.439.
Larsson SC, Orsini N. Coffee consumption and risk of stroke: a dose-response meta-analysis of prospective studies. Am J Epidemiol. 2011;174(9):993–1001. doi:10.1093/aje/kwr226.
Bravi F, Bosetti C, Tavani A, et al. Coffee drinking and hepatocellular carcinoma risk: a meta-analysis. Hepatology. 2007;46(2):430–5. doi:10.1002/hep.21708.
Bravi F, Scotti L, Bosetti C, et al. Coffee drinking and endometrial cancer risk: a metaanalysis of observational studies. Am J Obstet Gynecol. 2009;200(2):130–5. doi:10.1016/j.ajog.2008.10.032.
Je Y, Liu W, Giovannucci E. Coffee consumption and risk of colorectal cancer: a systematic review and meta-analysis of prospective cohort studies. Int J Cancer. 2009;124(7):1662–8. doi:10.1002/ijc.24124.
Galeone C, Tavani A, Pelucchi C, et al. Coffee and tea intake and risk of head and neck cancer: pooled analysis in the international head and neck cancer epidemiology consortium. Cancer Epidemiol Biomarkers Prev. 2010;19(7):1723–36. doi:10.1158/1055-9965.EPI-10-0191.
Turati F, Galeone C, La Vecchia C, Garavello W, Tavani A. Coffee and cancers of the upper digestive and respiratory tracts: meta-analyses of observational studies. Ann Oncol. 2011;22(3):536–44. doi:10.1093/annonc/mdq603.
Dawber TR, Kannel WB, Gordon T. Coffee and cardiovascular disease. Observations from the framingham study. N Engl J Med. 1974;291(17):871–4. doi:10.1056/NEJM197410242911703.
Heyden S, Tyroler HA, Heiss G, Hames CG, Bartel A. Coffee consumption and mortality. Total mortality, stroke mortality, and coronary heart disease mortality. Arch Intern Med. 1978;138(10):1472–5.
Murray SS, Bjelke E, Gibson RW, Schuman LM. Coffee consumption and mortality from ischemic heart disease and other causes: results from the Lutheran Brotherhood study, 1966-1978. Am J Epidemiol. 1981;113(6):661–7.
Jacobsen BK, Bjelke E, Kvale G, Heuch I. Coffee drinking, mortality, and cancer incidence: results from a Norwegian prospective study. J Natl Cancer Inst. 1986;76(5):823–31.
Vandenbroucke JP, Kok FJ, van ‘t Bosch G, van den Dungen PJ, van der Heide-Wessel C, van der Heide RM. Coffee drinking and mortality in a 25-year follow up. Am J Epidemiol. 1986;123(2):359–61.
LeGrady D, Dyer AR, Shekelle RB, et al. Coffee consumption and mortality in the Chicago Western Electric Company Study. Am J Epidemiol. 1987;126(5):803–12.
Rosengren A, Wilhelmsen L. Coffee, coronary heart disease and mortality in middle-aged Swedish men: findings from the Primary Prevention Study. J Intern Med. 1991;230(1):67–71.
Lindsted KD, Kuzma JW, Anderson JL. Coffee consumption and cause-specific mortality. Association with age at death and compression of mortality. J Clin Epidemiol. 1992;45(7):733–42. doi:10.1016/0895-4356(92)90051-N.
Klatsky AL, Armstrong MA, Friedman GD. Coffee, tea, and mortality. Ann Epidemiol. 1993;3(4):375–81.
Woodward M, Tunstall-Pedoe H. Coffee and tea consumption in the Scottish Heart Health Study follow up: conflicting relations with coronary risk factors, coronary disease, and all cause mortality. J Epidemiol Community Health. 1999;53(8):481–7.
Kleemola P, Jousilahti P, Pietinen P, Vartiainen E, Tuomilehto J. Coffee consumption and the risk of coronary heart disease and death. Arch Intern Med. 2000;160(22):3393–400. doi:10.1001/archinte.160.22.3393.
Iwai N, Ohshiro H, Kurozawa Y, et al. Relationship between coffee and green tea consumption and all-cause mortality in a cohort of a rural Japanese population. J Epidemiol. 2002;12(3):191–8.
Jazbec A, Simic D, Corovic N, Durakovic Z, Pavlovic M. Impact of coffee and other selected factors on general mortality and mortality due to cardiovascular disease in Croatia. J Health Popul Nutr. 2003;21(4):332–40.
Andersen LF, Jacobs DR Jr, Carlsen MH, Blomhoff R. Consumption of coffee is associated with reduced risk of death attributed to inflammatory and cardiovascular diseases in the Iowa Women’s Health Study. Am J Clin Nutr. 2006;83(5):1039–46.
Iso H, Kubota Y. Nutrition and disease in the Japan Collaborative Cohort Study for Evaluation of Cancer (JACC). Asian Pac J Cancer Prev. 2007;8(Suppl):35–80.
Paganini-Hill A, Kawas CH, Corrada MM. Non-alcoholic beverage and caffeine consumption and mortality: the Leisure World Cohort Study. Prev Med. 2007;44(4):305–10. doi:10.1016/j.ypmed.2006.12.011.
Happonen P, Laara E, Hiltunen L, Luukinen H. Coffee consumption and mortality in a 14-year follow-up of an elderly northern Finnish population. Br J Nutr. 2008;99(6):1354–61. doi:10.1017/S0007114507871650.
Laaksonen M, Talala K, Martelin T, et al. Health behaviours as explanations for educational level differences in cardiovascular and all-cause mortality: a follow-up of 60 000 men and women over 23 years. Eur J Public Health. 2008;18(1):38–43. doi:10.1093/eurpub/ckm051.
Lopez-Garcia E, van Dam RM, Li TY, Rodriguez-Artalejo F, Hu FB. The relationship of coffee consumption with mortality. Ann Intern Med. 2008;148(12):904–14. doi:10.7326/0003-4819-148-12-200806170-00003.
Ahmed HN, Levitan EB, Wolk A, Mittleman MA. Coffee consumption and risk of heart failure in men: an analysis from the Cohort of Swedish Men. Am Heart J. 2009;158(4):667–72. doi:10.1016/j.ahj.2009.07.006.
de Koning Gans JM, Uiterwaal CS, van der Schouw YT, et al. Tea and coffee consumption and cardiovascular morbidity and mortality. Arterioscler Thromb Vasc Biol. 2010;30(8):1665–71. doi:10.1161/ATVBAHA.109.201939.
Sugiyama K, Kuriyama S, Akhter M, et al. Coffee consumption and mortality due to all causes, cardiovascular disease, and cancer in Japanese women. J Nutr. 2010;140(5):1007–13. doi:10.3945/jn.109.109314.
Tamakoshi A, Lin Y, Kawado M, Yagyu K, Kikuchi S, Iso H. Effect of coffee consumption on all-cause and total cancer mortality: findings from the JACC study. Eur J Epidemiol. 2011;26(4):285–93. doi:10.1007/s10654-011-9548-7.
Freedman ND, Park Y, Abnet CC, Hollenbeck AR, Sinha R. Association of coffee drinking with total and cause-specific mortality. N Engl J Med. 2012;366(20):1891–904. doi:10.1056/NEJMoa1112010.
Nilsson LM, Winkvist A, Brustad M, et al. A traditional Sami diet score as a determinant of mortality in a general northern Swedish population. Int J Circumpolar Health. 2012;71:1–12. doi:10.3402/ijch.v71i0.18537.
Heyden S, Heyden F, Heiss G, Hames CG. Smoking and coffee consumption in three groups: cancer deaths, cardiovascular deaths and living controls. A prospective study in Evans County, Georgia. J Chronic Dis. 1979;32(9–10):673–7.
Tverdal A, Stensvold I, Solvoll K, Foss OP, Lund-Larsen P, Bjartveit K. Coffee consumption and death from coronary heart disease in middle aged Norwegian men and women. BMJ. 1990;300(6724):566–9.
Stensvold I, Tverdal A, Jacobsen BK. Cohort study of coffee intake and death from coronary heart disease over 12 years. BMJ. 1996;312(7030):544–5.
Hart C, Smith GD. Coffee consumption and coronary heart disease mortality in Scottish men: a 21 year follow up study. J Epidemiol Community Health. 1997;51(4):461–2.
Greenberg JA, Chow G, Ziegelstein RC. Caffeinated coffee consumption, cardiovascular disease, and heart valve disease in the elderly (from the Framingham Study). Am J Cardiol. 2008;102(11):1502–8. doi:10.1016/j.amjcard.2008.07.046.
Leurs LJ, Schouten LJ, Goldbohm RA, van den Brandt PA. Total fluid and specific beverage intake and mortality due to IHD and stroke in the Netherlands Cohort Study. Br J Nutr. 2010;104(8):1212–21. doi:10.1017/S0007114510001923.
Mineharu Y, Koizumi A, Wada Y, et al. Coffee, green tea, black tea and oolong tea consumption and risk of mortality from cardiovascular disease in Japanese men and women. J Epidemiol Community Health. 2011;65(3):230–40. doi:10.1136/jech.2009.097311.
Khan MM, Goto R, Kobayashi K, et al. Dietary habits and cancer mortality among middle aged and older Japanese living in hokkaido, Japan by cancer site and sex. Asian Pac J Cancer Prev. 2004;5(1):58–65.
Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–12. doi:10.1001/jama.283.15.2008.
Greenberg JA, Dunbar CC, Schnoll R, Kokolis R, Kokolis S, Kassotis J. Caffeinated beverage intake and the risk of heart disease mortality in the elderly: a prospective analysis. Am J Clin Nutr. 2007;85(2):392–8.
Paganini-Hill A. Lifestyle practices and cardiovascular disease mortality in the elderly: the leisure world cohort study. Cardiol Res Pract. 2011;2011:983764. doi:10.4061/2011/983764.
Heyden S, Tyroler HA, Cassel JC, Hames CG, Becker C, Heiss G. Coffee consumption and mortality in a community study–Evans Co., Ga. Z Ernahrungswiss. 1976;15(2):143–50.
Snowdon DA, Phillips RL. Coffee consumption and risk of fatal cancers. Am J Public Health. 1984;74(8):820–3.
Fortes C, Forastiere F, Farchi S, Rapiti E, Pastori G, Perucci CA. Diet and overall survival in a cohort of very elderly people. Epidemiology. 2000;11(4):440–5.
Greenland S, Longnecker MP. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am J Epidemiol. 1992;135(11):1301–9.
Hamling J, Lee P, Weitkunat R, Ambuhl M. Facilitating meta-analyses by deriving relative effect and precision estimates for alternative comparisons from a set of estimates presented by exposure level or disease category. Stat Med. 2008;27(7):954–70. doi:10.1002/sim.3013.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60. doi:10.1136/bmj.327.7414.557.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–101.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
Wu JN, Ho SC, Zhou C, et al. Coffee consumption and risk of coronary heart diseases: a meta-analysis of 21 prospective cohort studies. Int J Cardiol. 2009;137(3):216–25. doi:10.1016/j.ijcard.2008.06.051.
Larsson SC, Mannisto S, Virtanen MJ, Kontto J, Albanes D, Virtamo J. Coffee and tea consumption and risk of stroke subtypes in male smokers. Stroke. 2008;39(6):1681–7. doi:10.1161/STROKEAHA.107.504183.
Larsson SC, Virtamo J, Wolk A. Coffee consumption and risk of stroke in women. Stroke. 2011;42(4):908–12. doi:10.1161/STROKEAHA.110.603787.
Lopez-Garcia E, Rodriguez-Artalejo F, Rexrode KM, Logroscino G, Hu FB, van Dam RM. Coffee consumption and risk of stroke in women. Circulation. 2009;119(8):1116–23. doi:10.1161/CIRCULATIONAHA.108.826164.
James JE. Is habitual caffeine use a preventable cardiovascular risk factor? Lancet. 1997;349(9047):279–81. doi:10.1016/S0140-6736(96)04253-5.
Zhang Z, Hu G, Caballero B, Appel L, Chen L. Habitual coffee consumption and risk of hypertension: a systematic review and meta-analysis of prospective observational studies. Am J Clin Nutr. 2011;93(6):1212–9. doi:10.3945/ajcn.110.004044.
Mesas AE, Leon-Munoz LM, Rodriguez-Artalejo F, Lopez-Garcia E. The effect of coffee on blood pressure and cardiovascular disease in hypertensive individuals: a systematic review and meta-analysis. Am J Clin Nutr. 2011;94(4):1113–26. doi:10.3945/ajcn.111.016667.
Thelle DS, Arnesen E, Forde OH. The Tromso heart study. Does coffee raise serum cholesterol? N Engl J Med. 1983;308(24):1454–7. doi:10.1056/NEJM198306163082405.
D’Avanzo B, Santoro L, Nobill A, La Vecchia C. Coffee consumption and serum cholesterol. GISSI-EFRIM Study Group. Prev Med. 1993;22(2):219–24.
Jee SH, He J, Appel LJ, Whelton PK, Suh I, Klag MJ. Coffee consumption and serum lipids: a meta-analysis of randomized controlled clinical trials. Am J Epidemiol. 2001;153(4):353–62.
Cai L, Ma D, Zhang Y, Liu Z, Wang P. The effect of coffee consumption on serum lipids: a meta-analysis of randomized controlled trials. Eur J Clin Nutr. 2012;66(8):872–7. doi:10.1038/ejcn.2012.68.
Zhang W, Lopez-Garcia E, Li TY, Hu FB, van Dam RM. Coffee consumption and risk of cardiovascular diseases and all-cause mortality among men with type 2 diabetes. Diabetes Care. 2009;32(6):1043–5. doi:10.2337/dc08-2251.
Zhang WL, Lopez-Garcia E, Li TY, Hu FB, van Dam RM. Coffee consumption and risk of cardiovascular events and all-cause mortality among women with type 2 diabetes. Diabetologia. 2009;52(5):810–7. doi:10.1007/s00125-009-1311-1.
Montagnana M, Favaloro EJ, Lippi G. Coffee intake and cardiovascular disease: virtue does not take center stage. Semin Thromb Hemost. 2012;38(2):164–77. doi:10.1055/s-0032-1301414.
Choi HK, Willett W, Curhan G. Coffee consumption and risk of incident gout in men: a prospective study. Arthritis Rheum. 2007;56(6):2049–55. doi:10.1002/art.22712.
Imatoh T, Tanihara S, Miyazaki M, Momose Y, Uryu Y, Une H. Coffee consumption but not green tea consumption is associated with adiponectin levels in Japanese males. Eur J Nutr. 2011;50(4):279–84. doi:10.1007/s00394-010-0136-5.
Kempf K, Herder C, Erlund I, et al. Effects of coffee consumption on subclinical inflammation and other risk factors for type 2 diabetes: a clinical trial. Am J Clin Nutr. 2010;91(4):950–7. doi:10.3945/ajcn.2009.28548.
Mostofsky E, Rice MS, Levitan EB, Mittleman MA. Habitual coffee consumption and risk of heart failure: a dose-response meta-analysis. Circ Heart Fail. 2012;5(4):401–5. doi:10.1161/CIRCHEARTFAILURE.112.967299.
Pelchovitz DJ, Goldberger JJ. Caffeine and cardiac arrhythmias: a review of the evidence. Am J Med. 2011;124(4):284–9. doi:10.1016/j.amjmed.2010.10.017.
Svilaas A, Sakhi AK, Andersen LF, et al. Intakes of antioxidants in coffee, wine, and vegetables are correlated with plasma carotenoids in humans. J Nutr. 2004;134(3):562–7.
Kawachi I, Willett WC, Colditz GA, Stampfer MJ, Speizer FE. A prospective study of coffee drinking and suicide in women. Arch Intern Med. 1996;156(5):521–5.
Yu X, Bao Z, Zou J, Dong J. Coffee consumption and risk of cancers: a meta-analysis of cohort studies. BMC Cancer. 2011;11:96. doi:10.1186/1471-2407-11-96.
Galeone C, Turati F, La Vecchia C, Tavani A. Coffee consumption and risk of colorectal cancer: a meta-analysis of case-control studies. Cancer Causes Control. 2010;21(11):1949–59. doi:10.1007/s10552-010-9623-5.
Zhang X, Albanes D, Beeson WL, et al. Risk of colon cancer and coffee, tea, and sugar-sweetened soft drink intake: pooled analysis of prospective cohort studies. J Natl Cancer Inst. 2010;102(11):771–83. doi:10.1093/jnci/djq107.
Viani R. The composition of coffee. In: Garattini S, editor. Caffeine, coffee, and health. New York: Raven Press; 1993. p. 17–41.
D’Avanzo B, La Vecchia C, Katsouyanni K, Negri E, Trichopoulos D. An assessment, and reproducibility of food frequency data provided by hospital controls. Eur J Cancer Prev. 1997;6(3):288–93.
Ferraroni M, Tavani A, Decarli A, et al. Reproducibility and validity of coffee and tea consumption in Italy. Eur J Clin Nutr. 2004;58(4):674–80. doi:10.1038/sj.ejcn.1601864.
Cornelis MC, El-Sohemy A, Kabagambe EK, Campos H. Coffee, CYP1A2 genotype, and risk of myocardial infarction. JAMA. 2006;295(10):1135–41. doi:10.1001/jama.295.10.1135.
Istvan J, Matarazzo JD. Tobacco, alcohol, and caffeine use: a review of their interrelationships. Psychol Bull. 1984;95(2):301–26.
IARC. Coffee, tea, mate, methylxanthines and methylglyoxal. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Lyon, 27 February to 6 March 1990. IARC Monogr Eval Carcinog Risks Hum. 1991;51:1–513.
Acknowledgments
This work was supported by the Italian Association for Cancer Research (AIRC), Milan, Italy, Project No. 10068. SM and FT were supported by a fellowship from the Italian Foundation for Cancer Research (FIRC).
Conflict of interest
The authors declare no conflicts of interest. All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no financial relationships or activities with any organizations that might have an interest with the submitted work in the previous 3 years, no other relationships or activities that could appear to have influenced the submitted work.
Author information
Authors and Affiliations
Corresponding author
Additional information
Alessandra Tavani has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence on a worldwide basis to the BMJ Publishing Group Ltd to permit this article to be published in BMJ editions and any other BMJPGL products and sublicences such use and exploit all subsidiary rights, as set out in our licence.
Statistical codes and datasets available from Malerba or Tavani (stefano.malerba@marionegri.it).
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Malerba, S., Turati, F., Galeone, C. et al. A meta-analysis of prospective studies of coffee consumption and mortality for all causes, cancers and cardiovascular diseases. Eur J Epidemiol 28, 527–539 (2013). https://doi.org/10.1007/s10654-013-9834-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-013-9834-7