
Summary
Purpose: The integrin αvβ3 is an adhesion molecule expressed by proliferating endothelial cells and antibodies blocking this integrin inhibit angiogenesis in preclinical models. MEDI-522 is a second generation humanized anti-αvβ3 antibody designed for antiangiogenic therapy. The purpose of this study was to examine potential effects of this agent on blood vessels.
Experimental design: In a phase I dose escalation study, MEDI-522 was administered by weekly infusions to 25 adult patients with advanced solid organ malignancies. As a surrogate angiogenesis assay, a wound was created by punch biopsy of the arm skin. This wound site was re-biopsied after a 7-day interval. Dual-label immunofluorescence experiments followed by computer-assisted image analysis were conducted to analyze the vasculature.
Results: Sequential pretreatment and 4-week treatment skin biopsy pairs were available on 4 patients, who had received 6 or 10 mg/kg of MEDI-522. MEDI-522 was detected in the dermal blood vessels as well as the dermal interstitium both in intact and wounded skin sites following treatment. No statistically significant difference was found between pretreatment and treatment samples of skin for vascular area, endothelial cell proliferation and apoptosis, or β3 integrin levels. Phosphorylated focal adhesion kinase (pFAK) was significantly diminished in skin wound vessels during MEDI-522 treatment compared to the pretreatment samples.
Conclusions: MEDI-522 was detectable both in quiescent and in angiogenically active skin blood vessels as well as in the dermal interstitial space. The levels of pFAK were reduced during MEDI-522 treatment, suggesting a modulating effect on this signaling molecule.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The development of new blood vessels (angiogenesis) is believed to be necessary for tumor growth and development. Therefore, targeting genetically normal host vessels presents itself as an attractive treatment strategy, particularly in advanced, therapy-resistant neoplasms. Angiogenically active endothelial cells specifically upregulate the αvββ3 integrin [1]. This cell adhesion receptor is important for cell migration, growth and survival. In preclinical models, the inhibition of αvβ3 integrin with monoclonal antibody LM609 results in the suppression of angiogenesis and tumor growth [2]. A humanized version of this antibody (Vitaxin, Applied Molecular Evolution, San Diego, CA) has been proven safe for therapeutic use, but had limited efficacy in patients with advanced malignancies [3, 4]. The affinity of this antibody for the αvβ3 integrin heterodimer was further increased using stepwise maturation with phage expression libraries [5]. The resulting MEDI-522 antibody was recently evaluated at the University of Wisconsin Comprehensive Cancer Center in a phase I dose escalation trial. The pharmakokinetic and clinical observations from this study have recently been reported [6]. Briefly, no major adverse events were observed. Dynamic CT imaging revealed a significant increase in the mean blood transit time, suggesting a decreased microvascular blood flow within tumors. There were no objective responses but three patients with metastatic renal cell carcinoma experienced prolonged stable disease. In fact, one patient remains on study with stable disease after 3 years of MEDI-522 treatment at a dose of 2 mg/kg. Monitoring of antiangiogenic therapy effects is a challenging task. With current technology, tissue examination may offer the best opportunity for analyzing signaling events in endothelial cells. Since tumor tissue is often difficult to obtain and shows a high degree of interpatient variability, we applied a skin wounding assay as surrogate angiogenesis test. This method and similar approaches have previously been used by us and other investigators to evaluate the efficacy of different antiangiogenic agents in vivo [7, 8]. In a limited number of patient volunteers, experimental skin wound sites were biopsied before and during MEDI-522 therapy. A series of staining experiments were performed to analyze parameters related to the distribution of MEDI-522, vascular density, endothelial cell turnover, and signaling events down-stream of the αvβ3 integrin.
Materials and methods
Patients and study design
Adult patients (age >18 years) with lymphomas or other solid tumors, which were refractory to standard therapies were eligible for this study. The study protocol had been reviewed and approved by the Institutional Review Board of the University of Wisconsin, and all patients gave written informed consent. In this phase I dose escalation trial, MEDI-522 was administered by weekly intravenous infusion at doses ranging from 2 to 10 mg/kg body weight. Details about the study design and the patient population have been reported [6].
Biopsies
Two pairs of sequential skin biopsies were performed at the University of Wisconsin General Clinical Research Center (GCRC) with a 4-mm punch biopsy device (Acuderm, Fort Lauderdale, FL) in the same location on the upper arm, to assess blood vessel formation in wound sites. The purpose of the first biopsy was to create a wound, whereas the second biopsy 7 days later captured the wound tissue. The first biopsy pair was taken prior to treatment (weeks–2 and −1), the second biopsy pair 4 weeks after the initiation of MEDI-522 infusions (weeks 4 and 5). In one patient, pretreatment (week −1) and treatment (week 4) samples from a superficial tumor were obtained by needle core biopsy. Both skin punch biopsy cylinders and tumor biopsies were embedded in OCT compound, snap-frozen and stored at −70°C.
Immunocytochemistry
For MEDI-522 localization, 8-μm-thick frozen sections were fixed in 4% paraformaldehyde for 10 min. After blocking, the sections were incubated with goat-anti-MEDI-522 antibody (20 μg/ml; gift from Medimmune) and mouse anti-von Willebrand Factor (vWF) antibody (Neomarkers) at a dilution of 1:150 in PBS plus bovine serum albumine (1% w/v) for 60 min. For integrin localization, the frozen sections were fixed in cold acetone for 10 min, blocked and stained with mouse anti-integrin β3 monoclonal antibody (Chemicon international, Temecula, CA) at 25 μg/ml and rabbit anti-vWF antibody at a dilution of 1:2000 (Dako, Carpinteria, CA). For the detection of phosphorylated focal adhesion kinase (pFAK), the frozen sections were fixed as for integrin detection. A rabbit (polyclonal) anti-FAK-[pY397] phosphospecific antibody (Cell Signaling Technology, Beverly, MA; 1:40) was combined with a mouse anti-vWF antibody. Ki67 labeling was performed using a monoclonal antibody (clone 7B11; Zymed Laboratories, San Francisco, CA) at a 1:25 dilution and rabbit anti-vWF antibody as described. The primary antibody incubations were followed by appropriate Alexa488 and Alexa568-conjugated secondary antibodies at a 1:400 dilution (Molecular Probes, Eugene OR).
Analysis of endothelial cell apoptosis
Endothelial cell apoptosis was detected by dual labeling of tissues with the TUNEL procedure and with anti-vWF antibodies. Apoptotic cells were identified using the In Situ Cell Death Detection, Fluorescein kit (Roche-Boehringer Mannheim, Indianapolis, IN), according to the manufacturer's instructions but omitting the signal conversion reaction.
Image acquisition and analysis
A minimum of three images were acquired from each dual-labeled tissue section with an Olympus BX50 microscope equipped for epifluorescence and fitted with a cooled charge-coupled device camera (Diagnostic Instruments, Sterling Heights, MI). To analyze fluorescence intensity in blood vessels, the vWF-positive areas were outlined using the “magic wand” tool within the Photoshop program (Adobe, San Jose, CA). A mask, identifying the vWF positive areas was superimposed on the corresponding image of the marker of interest (e.g. MEDI-522). The average fluorescence intensity within the vascular areas was measured with ImageJ software (NIH; public domain; http://rsb.info.nih.gov/ij/). Figure 1 illustrates the analysis method.

Schematic illustration of computer-assisted analysis of fluorescence intensity in blood vessels: A section of skin wound tissue was labeled with antibodies to the endothelial cell marker vWF (red channel) and to MEDI-522 (green channel). (A) Red channel grey scale image highlighting vWF-positive blood vessels. (B) Mask, created by thresholding the vWF-positive area with the “magic wand” tool in Adobe Photoshop. (C) Green channel grey scale image depicting MEDI-522 distribution and intensity. (D) Green channel grey scale image depicting MEDI-522 distribution and intensity after applying vWF mask and thus eliminating all non-vessel areas. (E) Three-dimensional display of MEDI-522 fluorescence intensity in vWF-positive areas. Original magnification: 400×
Statistical analysis
All values were expressed as mean±SEM. Statistical analysis was performed by paired t-test. Values were considered significantly different at P< 0.05.
Results
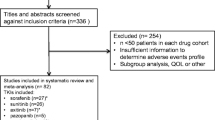
Skin and tumor biopsies were performed on patient volunteers. Wound healing was not delayed during treatment compared to pretreatment biopsies. Nine patients consented to skin biopsies. Complete sets of pretreatment and treatment skin biopsy samples were obtained from four patients, who had received MEDI-522 at the highest two dose levels (one patient on 6 mg/kg and three patients on 10 mg/kg). Pretreatment and treatment tumor biopsies were only available from one patient with a renal cell carcinoma metastatic to the neck area.
The initial goal of our staining experiments was to determine whether MEDI-522 reaches angiogenically active blood vessels, its intended target. A specific antibody detected abundant MEDI-522 in skin vessels (Fig. 2). Surprisingly, MEDI-522 accumulated in dermal vessels of both normal and wounded skin to a similar extent. MEDI-522 was also detected in the dermal interstitium of intact and wounded skin, indicating significant extravasation of this agent even from quiescent vessels. The quantified MEDI-522 blood vessel staining results are shown in Fig. 3(A). Similarly, in the tumor biopsy, MEDI-522 localized to blood vessels and tumor cells (Fig. 2(E, F)). Since only a single tumor biopsy pair was available, we restricted subsequent analyses to the skin samples.

Localization of MEDI-522 in tissue sections: Tissue sections were incubated with anti-MEDI-522 and anti-vWF antibodies as described in Materials and Methods. Secondary Alexa488 (green fluorescence) and Alexa568 (red fluorescence) conjugated antibodies were used for the detection of MEDI-522 and vWF respectively. DAPI was added to the mounting medium to highlight nuclei. (A) Intact skin before initiation of treatment. Dermal blood vessels (“V”) are present and are enlarged in the inset. Background staining with the anti-MEDI-522 antibody is low; E= Epidermis. (B) Intact skin 30 days after initiation of weekly infusions of MEDI-522 (6 mg/kg). MEDI-522 is deposited in dermal vessels (“V” and inset) and in the dermal interstitium. (C) The site from the punch biopsy shown in “A” was rebiopsied after a 7-day interval but prior to initiation of MEDI-522 treatment. Abundant microvessels (“V” and inset) are present within the wound site granulation tissue. (D) The site from the punch biopsy shown in “B” was rebiopsied after a 7-day interval and 37 days after initiation of MEDI-522 treatment. MEDI-522 co-localizes with microvessels (“V” and inset) within the wound site granulation tissue and has been deposited in the dermal connective tissue. The wound is partially re-epithelialized with a thickened epidermis (“E”). (E) Needle core biopsy of metastatic renal cell carcinoma prior to MEDI-522 infusions. (F) Same metastasis 31 days after initiation of MEDI-522 treatment. Original magnification: 200 × (A-D); 400 × (E,F)

Quantitative analysis of skin vessel parameters: (A) The mean MEDI-522 fluorescence signal in blood vessels (defined as vWF-positive tissue regions) was quantified with the ImageJ program as described in Materials and Methods. As expected, the MEDI-522 signal was stronger during treatment (p=0.0005 and 0.0006, respectively) but there was no significant difference between intact and wounded skin. (B) Vascularity was expressed as the ratio of the vWF-positive area in the tissue of interest and the vWF-positive area in the non-wounded pretreatment skin sections. (C) The mean fluorescence intensity for β3 integrin subunit was measured as described in “A”. There was no significant difference between intact and wounded skin or pretreatment and treatment skin samples respectively. (D) The mean fluorescence intensity for tyrosine-397 phosphorylated FAK (p-FAK-Y-397) was measured as described in “A”. Pretreatment and treatment samples of intact skin did not differ significantly, but the p-FAK signal in wounded skin during MEDI-522 treatment was significantly lower compared to the pretreatment biopsies (P=0.03). All values represent the mean of four samples from individual patients and at least three images per biopsy sample. The error bars indicate the standard error of mean. (E) pFAK staining intensity in skin wound vessels before and during MEDI-522 treatment for all four patients

Detection of β3 integrin subunit and phosphorylated FAK in skin wound tissue: (A) β3 integrin subunit (green channel) localizes to endothelial cells in blood vessel (“V”). (B) and (C) Anti-FAK-Y397 phospho-specific antibody detects a signal in dermal blood vessels (“V”). Original magnification: 400 × (A), 400 × (B, C)
As potential readouts for MEDI-522 antiangiogenic activity, we evaluated vessel area fraction, endothelial cell proliferation and apoptosis in the skin biopsy samples. As expected, the vessel area fraction was significantly elevated in wounded tissues compared to uninjured skin (Fig. 3(B)). However, this parameter did not differ significantly between pretreatment and treatment samples. Proliferating (Ki67-positive) and apoptotic (TUNEL-positive) endothelial cells were rare in all skin biopsies, precluding a quantitative comparison (not shown).
One possible consequence of integrin αvβ3 ligation by MEDI-522 would be the down-regulation of this adhesion receptor. This possibility was examined by probing the skin tissue sections with an antibody directed against an epitope on the β3 integrin subunit, which is distinct from the LM609/MEDI-522-binding domain. The β3 integrin signal was slightly higher in wound tissue than in uninjured skin, but this difference did not reach statistical significance (p=0.085; Fig. 3(C)). Blood vessel β3 integrin staining in wound sites decreased in two of the four patients during MEDI-522 treatment, but the mean staining intensity of all four patients was not significantly different between pretreatment and treatment samples (p=0.27).
Despite the lack of an intrinsic kinase domain, integrin ligation by extracellular matrix constituents triggers multiple signaling events, which culminate in the reorganization of the cytoskeleton and migration. One of the key signal relay molecules in the integrin adhesion complex is FAK, which not only possesses tyrosine kinase activity but also contains multiple auto- and transphosphorylation sites [9]. Upon integrin ligation, FAK is autophosphorylated at a tyrosine in the 397-position, creating a binding site for src kinase. Conversely, blocking of integrin ligation with an antibody would be expected to reduce phosphorylation of FAK-Y397. An antibody specifically reacting with pFAK-Y397 detected a signal predominantly in blood vessel endothelial cells. A strong signal was detected in blood vessels of uninjured skin and pretreatment and treatment samples did not differ significantly (Fig. 3(D)). It is likely that FAK phosphorylation in uninjured vessel endothelial cells is induced by integrins other than αvβ3. In contrast, the mean pFAK397 signal was significantly lower in skin wounds during MEDI-522 treatment compared to pretreatment samples (p=0.03; Fig. 3(D), Fig. 4). pFAK was diminished in three of the four patients (Fig. 3(E)). Among these three patients were the two patients who had experienced a drop in β3 integrin levels. There was no relationship between pFAK reduction and MEDI-522 dose, as the single patient with unchanged pFAK was on the highest dose of 10 mg/kg. This result suggests a suppression of FAK activation by MEDI-522, although a decrease in total FAK cannot be excluded. We were unable to detect total FAK protein in the skin sections with commercially available antibodies.
Discussion
In a phase I dose escalation trial, the anti-αvβ3 integrin antibody MEDI-522 was administered to patients with therapy-resistant, advanced solid organ malignancies [6]. Paired pretreatment and treatment skin wound biopsies provided the opportunity to study the localization of MEDI-522 to angiogenically active blood vessels and to evaluate downstream effects.
No complete or partial responses were observed during MEDI-522 treatment and healing of the experimental skin wound sites was not recognizably delayed. In keeping with these clinical observations, MEDI-522 did not induce a decrease in granulation tissue vascularity. Also, in contrast to several preclinical studies with antibody LM609 [10], we failed to detect an induction of endothelial cell apoptosis during MEDI-522 administration. One reason for this apparent lack of efficacy might be pharmacokinetic obstacles preventing the drug from reaching its target sites. However, we identified abundant MEDI-522 in blood vessels and the interstitium of skin and one tumor sample. To our knowledge, this is the first analysis of MEDI-522 tissue distribution at the microscopic level. Since the immunofluorescence detection method is qualitative rather than quantitative, we cannot conclude with certainty that the tissue drug levels are sufficient to block the αvβ3 receptors. However, pharmacokinetic data from this trial, in keeping with prior trials indicate that MEDI-522 trough levels at a dose of 10 mg/kg consistently exceed 30 μg/ml; a concentration sufficient for in vitro and in vivo preclinical activity [4, 6].
Data from antibody and peptide inhibition experiments are consistent with the hypothesis that αvβ3 integrin is required for angiogenesis [1]. Recent observations with integrin subunit-deficient mice have called this conclusion into question. Mice deficient in β3 integrin subunit are viable and display an enhanced pathological angiogenesis [11, 12]. Mice lacking αv integrin subunit are remarkable for excessive angiogenesis preceding their premature death due to cerebral defects [13]. The inconsistencies between these different experimental models prompted Hynes to propose that αvβ3 integrin may have antiangiogenic activity and that LM609 and related antibodies may activate rather than inhibit this adhesion receptor [14]. Cheresh favors an alternative model, where αvβ3 physiologically ligated by extracellular matrix (ECM) molecules conveys a survival signal, whereas unoccupied or antibody-blocked αvβ3 integrin triggers apoptosis [15]. In summary, the exact role of αvβ3 integrin in angiogenesis is presently a matter of controversy [16].
Interestingly, the only MEDI-522-associated effect on blood vessels observed in this study was a reduction in pFAK-Y397. However, more patients would need to be studied to confirm this finding. Whether the modest decrease in pFAK seen in these patients is physiologically relevant is not clear. FAK is a key molecule in cellular signaling, which integrates and amplifies signals received from integrin cell adhesion and growth factor receptors [17]. Binding of the FAK N-terminal domain to β-integrin subunits leads to Y-397 autophosphorylation and subsequent activation and docking steps (reviewed in [18]). FAK-Y397 is also required for growth factor receptor signal transduction, since blocking of integrin signaling by placing cells in suspension abrogates, and a constitutively active FAK mutant rescues mitogen-induced activation of the raf-MEK-Erk cascade [19, 20]. Genetically FAK-deficient animals provide key evidence on the importance of FAK in angiogenesis. Embryos of FAK knockout mice show early lethality due to severe mesoderm abnormalities and cardiovascular defects [21]. FAK-deficient endothelial cells lack the ability to form vascular networks in collagen gels and animals with a conditional deletion of FAK in endothelial cells are characterized by defective angiogenesis during late embryogenesis [22, 23].
There is currently no recommended gold standard for the monitoring of antiangiogenic therapy effects. Recent progress in radiologic imaging techniques has made the analysis of tumor perfusion parameters during antiangiogenic trials possible [6, 24]. Probing signaling pathways in endothelial cells by examining tissue samples provides complementary information and may reveal more subtle treatment effects.
References
Brooks PC, Clark RA, Cheresh DA (1994) Requirement of vascular integrin alpha v beta 3 for angiogenesis. Science 264:569–571
Brooks PC, Stromblad S, Klemke R, Visscher D, Sarkar FH, Cheresh DA (1995) Antiintegrin alpha v beta 3 blocks human breast cancer growth and angiogenesis in human skin. J Clin Invest 96:1815–1822
Patel SR, Jenkins J, Papadopolous N, Burgess MA, Plager C, Gutterman J, Benjamin RS (2001) Pilot study of vitaxin—an angiogenesis inhibitor-in patients with advanced leiomyosarcomas. Cancer 92:1347–1348
Gutheil JC, Campbell TN, Pierce PR, Watkins JD, Huse WD, Bodkin DJ, Cheresh DA (2000) Targeted antiangiogenic therapy for cancer using Vitaxin: a humanized monoclonal antibody to the integrin alphavbeta3. Clin Cancer Res 6:3056–3061
Wu H, Beuerlein G, Nie Y, Smith H, Lee BA, Hensler M, Huse WD, Watkins JD (1998) Stepwise in vitro affinity maturation of Vitaxin, an alphav beta3-specific humanized mAb. Proc Natl Acad Sci USA 95:6037–6042
McNeel DG, Eickhoff J, Lee FT, King DM, Alberti D, Thomas JP, Friedl A, Kolesar J, Marnocha R, Volkman J, Zhang J, Hammershaimb L, Zwiebel JA, Wilding G (2005) Phase I trial of a monoclonal antibody specific for {alpha}v{beta}3 integrin (MEDI-522) in patients with advanced malignancies, including an assessment of effect on tumor perfusion. Clin Cancer Res 11:7851–7860
Lockhart AC, Braun RD, Yu D, Ross JR, Dewhirst MW, Humphrey JS, Thompson S, Williams KM, Klitzman B, Yuan F, Grichnik JM, Proia AD, Conway DA, Hurwitz HI (2003) Reduction of wound angiogenesis in patients treated with BMS-275291, a broad spectrum matrix metalloproteinase inhibitor. Clin Cancer Res 9:586–593
Mundhenke C, Thomas JP, Wilding G, Lee FT, Kelzc F, Chappell R, Neider R, Sebree LA, Friedl A (2001) Tissue examination to monitor antiangiogenic therapy: a phase I clinical trial with endostatin. Clin Cancer Res 7:3366–3374
Mitra SK, Hanson DA, Schlaepfer DD (2005) Focal adhesion kinase: in command and control of cell motility. Nat Rev Mol Cell Biol 6:56–68
Brooks PC, Montgomery AM, Rosenfeld M, Reisfeld RA, Hu T, Klier G, Cheresh DA (1994) Integrin alpha v beta 3 antagonists promote tumor regression by inducing apoptosis of angiogenic blood vessels. Cell 79:1157–1164
Hodivala-Dilke KM, McHugh KP, Tsakiris DA, Rayburn H, Crowley D, Ullman-Cullere M, Ross FP, Coller BS, Teitelbaum S, Hynes RO (1999) Beta3-integrin-deficient mice are a model for Glanzmann thrombasthenia showing placental defects and reduced survival. J Clin Invest 103:229–238
Reynolds LE, Wyder L, Lively JC, Taverna D, Robinson SD, Huang X, Sheppard D, Hynes RO, Hodivala-Dilke KM (2002) Enhanced pathological angiogenesis in mice lacking beta3 integrin or beta3 and beta5 integrins. Nat Med 8:27–34
Bader BL, Rayburn H, Crowley D, Hynes RO (1998) Extensive vasculogenesis, angiogenesis, and organogenesis precede lethality in mice lacking all alpha v integrins. Cell 95:507–519
Hynes RO (2002) A reevaluation of integrins as regulators of angiogenesis. Nat Med 8:918–921
Cheresh DA, Stupack DG (2002) Integrin-mediated death: an explanation of the integrin-knockout phenotype? Nat Med 8:193–194
Carmeliet P (2002) Integrin indecision. Nat Med 8:14–16
Sieg DJ, Hauck CR, Ilic D, Klingbeil CK, Schaefer E, Damsky CH, Schlaepfer DD (2000) FAK integrates growth-factor and integrin signals to promote cell migration. Nat Cell Biol 2:249–256
Parsons JT (2003) Focal adhesion kinase: the first ten years. J Cell Sci 116:1409–1416
Renshaw MW, Price LS, Schwartz MA (1999) Focal adhesion kinase mediates the integrin signaling requirement for growth factor activation of MAP kinase. J Cell Biol 147:611–618
Aplin AE, Short SM, Juliano RL (1999) Anchorage-dependent regulation of the mitogen-activated protein kinase cascade by growth factors is supported by a variety of integrin alpha chains. J Biol Chem 274:31223–31228
Ilic D, Furuta Y, Kanazawa S, Takeda N, Sobue K, Nakatsuji N, Nomura S, Fujimoto J, Okada M, Yamamoto T (1995) Reduced cell motility and enhanced focal adhesion contact formation in cells from FAK-deficient mice. Nature 377:539–544
Ilic D, Kovacic B, McDonagh S, Jin F, Baumbusch C, Gardner DG, Damsky CH (2003) Focal adhesion kinase is required for blood vessel morphogenesis. Circ Res 92:300–307
Shen TL, Park AY, Alcaraz A, Peng X, Jang I, Koni P, Flavell RA, Gu H, Guan JL (2005) Conditional knockout of focal adhesion kinase in endothelial cells reveals its role in angiogenesis and vascular development in late embryogenesis. J Cell Biol 169:941–952
Miles KA, Charnsangavej C, Lee FT, Fishman EK, Horton K, Lee TY (2000) Application of CT in the investigation of angiogenesis in oncology. Acad Radiol 7:840–850
Acknowledgments
Work supported by the National Cancer Institute, UO1 CA62491 (G. Wilding, PI) and NO2-CO-124001 (22XS082A; G. Wilding, PI) and by National Center for Research Resources, MO1 RR03186 (P.M. Farrell, PI).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhang, D., Pier, T., McNeel, D.G. et al. Effects of a monoclonal anti-αvβ3 integrin antibody on blood vessels—A pharmacodynamic study. Invest New Drugs 25, 49–55 (2007). https://doi.org/10.1007/s10637-006-9013-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10637-006-9013-8